Back to Journals » Journal of Pain Research » Volume 14
Effectiveness of Pregabalin Treatment for Neuropathic Pain in Patients with Spine Diseases: A Pooled Analysis of Two Multicenter Observational Studies in Japan
Authors Taguchi T, Nakano S, Nozawa K
Received 27 November 2020
Accepted for publication 18 February 2021
Published 16 March 2021 Volume 2021:14 Pages 757—771
DOI https://doi.org/10.2147/JPR.S293556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Toshihiko Taguchi,1 Shogo Nakano,2 Kazutaka Nozawa2
1Japan Organization of Occupational Health and Safety, Yamaguchi Rosai Hospital, Sanyo-Onoda, Yamaguchi, Japan; 2Pfizer Japan, Inc., Tokyo, Japan
Correspondence: Kazutaka Nozawa Email [email protected]
Purpose: Neuropathic pain (NeP) is common among patients with chronic pain associated with spine diseases. Practical effectiveness of pregabalin, one of the first-line treatments for NeP, has not been evaluated in an entire population of patients with spine diseases, including various pathophysiological conditions. This pooled analysis aimed to evaluate the therapeutic value of pregabalin for chronic pain with NeP component in patients with spine diseases in routine primary care settings.
Patients and Methods: We pooled data from two 8-week prospective observational cohort studies for patients with chronic low back pain with accompanying lower limb pain (NeP component), and patients with chronic cervical pain and accompanying upper limb radiating pain (NeP component) in routine primary care settings in Japan. For both studies, patients were treated for 8 weeks with pregabalin (alone/with other analgesics) or usual care with conventional analgesics (eg, non-steroidal anti-inflammatory drugs). Changes in pain numerical rating scale (NRS), Pain-Related Sleep Interference Scale (PRSIS), and EuroQol 5-dimension 5-level (EQ-5D-5L) scores from baseline to week 8 were summarized and compared between the pregabalin and usual care groups, and also for subgroups of primary diagnosis. Safety was evaluated by adverse events (AEs) in the pregabalin group.
Results: The pooled dataset comprised 700 patients (pregabalin group: 302; usual care group: 398). All patient-reported outcomes (PRO) scores significantly improved from baseline to week 8 in the pregabalin than in the usual care group (NRS: P< 0.0001; PRSIS: P< 0.0001, and EQ-5D-5L: P=0.0006). Overall, all three PRO measures showed greater improvement in the pregabalin than in the usual care group, irrespective of the primary diagnosis. AEs were reported in 36.1% of the pregabalin group.
Conclusion: This analysis suggested multi-faceted effectiveness of treatment with pregabalin from the patient’s perspectives under a “real-world” practice in all patients with chronic NeP from various spine diseases.
Keywords: neuropathic pain, chronic pain, spine diseases, pregabalin, pooled analysis
Introduction
Low back pain and cervical pain are common health problems in developed countries. About 83% of the population in Japan experience low back pain at some point in their lives,1 and 48.3% of adults have neck or shoulder pain each year.2 Neuropathic pain (NeP), defined as “pain caused by a lesion or disease of the somatosensory nervous system”3 is caused by various etiologies including spine diseases, such as radiculopathy and cauda equina lesions,4 and cervical spondylotic myelopathy.5 NeP from these spine diseases is often experienced as low back pain and cervical pain with pain radiating down to the legs and arms, respectively.
According to an Internet-based survey in Japan, the prevalence of NeP was estimated to be 6.4% among the general population.6 NeP is common among patients with chronic pain associated with spine diseases, with a reported prevalence as high as 53.3%.5 Involvement of NeP further increases the burden of chronic pain in patients, including pain intensity,7–9 quality of life (QOL),8–11 and sleep interference,9,10 and interference with daily activities,10 when compared to chronic pain without an NeP component. Considering the indirect effect of pain on QOL (T Taguchi, personal unpublished data),12,13 pain relief with pharmacological treatment is a cornerstone for NeP management to reduce the multifaceted burdens.14
Pregabalin, a ligand of α2-δ subunits of voltage-gated calcium channels,15 reduces plasma membrane expression of calcium channels and calcium influx as well as inhibits the release of neurotransmitters, such as glutamate.16,17 Activation of descending noradrenergic and serotonergic pathways also contributes to the analgesic effects of pregabalin.18,19 Pregabalin was approved for NeP and pain associated with fibromyalgia in Japan20 and has also been recommended as one of the first-line pharmacological treatments for NeP14 in some other countries.21,22 Several randomized controlled trials (RCTs) have shown that pregabalin reduces pain intensity and improves sleep, health status, or other patient-reported outcomes (PROs) in patients with various types of NeP.23–29 Recently, however, some RCTs demonstrated that pregabalin was not more effective than placebo in reducing pain and other relevant PROs in patients with sciatica,30 lumbosacral radiculopathy,31 and lumbar spinal stenosis with neurogenic claudication,32 partially because of the high placebo response and possible involvement of the nociceptive component of pain, or unlikely or little involvement of NeP component of the target conditions of these studies.
To evaluate the effectiveness of pregabalin in chronic NeP from spine diseases, reflecting pain management in Japanese routine clinical practice, we previously conducted non-interventional studies in patients with chronic low back pain (CLBP) with accompanying lower limb pain below the knee (NeP component) (CLBP with NeP component, hereinafter)33 or chronic cervical pain accompanying upper limb radiating pain (NeP component) (chronic cervical pain with NeP component, hereinafter).34 In both studies, pain and pain-related sleep interference, function, and health status significantly improved in patients treated with pregabalin (alone or in combination with other analgesics) than in those with usual care, using conventional analgesics.33,34 Generally, pregabalin was well tolerated in both studies.33,34 These results provided clinically important information on the effectiveness and benefits of treatment using pregabalin in routine clinical practice.
At the same time, our previous observational studies revealed that ≥90% of the patients were treated with non-steroidal anti-inflammatory drugs (NSAIDs), and not treated with the first-line NeP treatments, that is, pregabalin, duloxetine, and tricyclic antidepressive agents,14 despite the involvement of the neuropathic component in the “real-world” setting.33,34 Evidence in an entire population of patients encompassing different diagnoses of spine diseases may help to guide better treatment strategies. However, to date, most of the observational studies have targeted patients with specific diagnoses (eg, cervical, lumbar, or lumbosacral radiculopathy),35–37 or pain location (back or low back);38,39 no study has investigated the practical effectiveness of pregabalin in an entire population of patients with spine diseases, including various pathophysiological conditions, a common NeP population encountered in daily clinical practice.
Therefore, this study aimed to obtain a comprehensive picture of therapeutic values of pregabalin for chronic pain with NeP component in patients with spine diseases from the patient’s perspective. In this analysis, using the pooled dataset of our previous studies in patients with CLBP with NeP component33 and chronic cervical pain with NeP component34 in routine primary care settings in Japan, we evaluated the effectiveness of pregabalin on PRO measures. Moreover, we conducted sub-group analyses to further explore patient profiles associated with treatment response.
Patients and Methods
Study Overview
This was a retrospective, pooled analysis of two prospective observational cohort studies conducted in Japan, with similar study design and methods, with one major difference in target pain site: the low back (Study A0081333, referred to as Study 1333, hereinafter)33 and cervical region (Study A0081354, referred to as Study 1354, hereinafter)34 (Table 1).
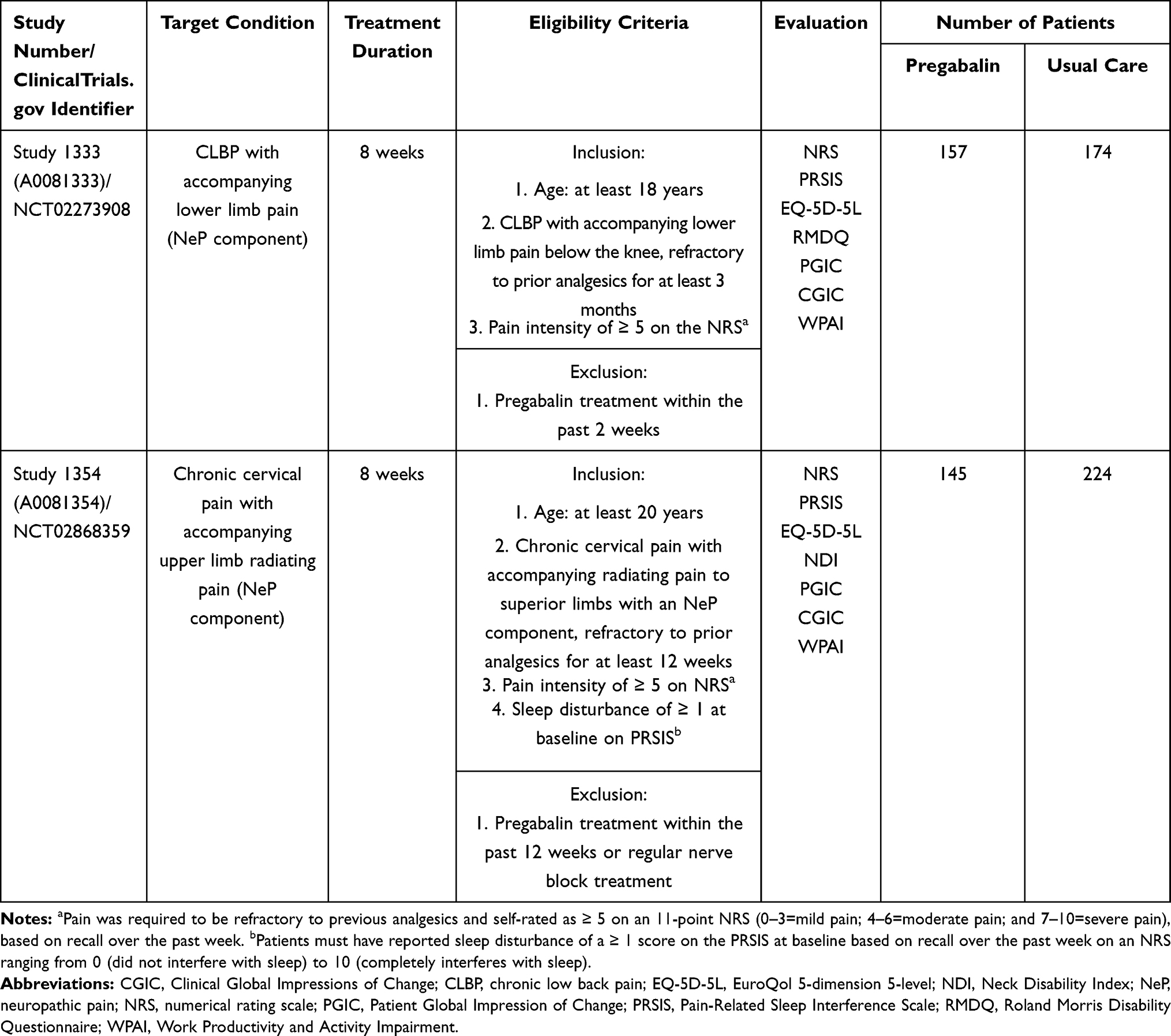 |
Table 1 Summary of the Studies Included in the Pooled Analysis |
Individual studies included in this analysis were registered with clinicaltrials.gov (Study 1333: NCT02273908; Study 1354: NCT02868359), approved by the Byoin-Godo Ethical Review Board, and conducted in accordance with the Declaration of Helsinki. All patients included in both studies provided written informed consent.
Study Design
Detailed methods have been published previously.33,34 Individual studies were 8-week, multicenter, prospective, observational studies that evaluated the effectiveness of pregabalin for the treatment of CLBP with NeP component (Study 1333)33 or chronic cervical pain with NeP component (Study 1354)34 in primary care settings under routine clinical practice (Table 1). Study 1333 was conducted in 2014, while Study 1354 was conducted between October 2016 and October 2017.
The inclusion and exclusion criteria for individual studies were generally similar (Table 1). Briefly, Study 1333 included patients aged ≥18 years who had CLBP with accompanying lower limb pain below the knee, and with pain that was refractory to prior analgesics for at least 3 months with an intensity rating of ≥5 on a numerical rating scale (NRS). Study 1354 included patients aged ≥20 years who had chronic cervical pain with accompanying radiating pain to the upper limbs with an NeP component, with pain that was refractory to previous analgesics for at least 12 weeks, and had an intensity of ≥5 on the NRS. In study 1354, patients were also required to have sleep interference by pain, rated ≥1 on Pain-Related Sleep Interference Scale (PRSIS), a detailed description of which is provided in the section below.
To reduce selection bias, both studies consecutively enrolled all patients who met the eligibility criteria during the enrollment period of individual studies at each site. Study sites were screened and selected based only on feasibility from the medical institutions that had contracted with a site management organization and had accepted support by clinical research coordinators across Japan.
For both studies, enrolled patients were treated for 8 weeks with pregabalin (alone or in combination with other analgesics) or usual care with conventional analgesics, such as paracetamol (acetaminophen), NSAIDs, antidepressants, other antiepileptic agents, and opioids. Selection of these treatments and their dose was solely rested on the physician’s best clinical judgment based on the package insert in the original studies to investigate the effectiveness of treatment with pregabalin under the settings reflecting the Japanese routine clinical practice. For the same reason, treatment compliance was not assessed in the original studies and the participants were not included or excluded based on a particular dose or compliance level.
Outcome Measures
In both studies, effectiveness was evaluated by PRO measures, including NRS, PRSIS, and EuroQol 5-dimension 5-level (EQ-5D-5L), administered at baseline, week 4, and week 8 (or at discontinuation). These three measures were included in the present analysis as PRO measures of treatment effectiveness.
NRS, an 11-point pain rating scale (ranging from 0 to 10), was used to evaluate average pain intensity over the past week. An NRS score of 0–3 was considered mild, 4–6 as moderate, and 7–10 as severe pain.34 PRSIS, a patient-completed measure, is used to evaluate the extent to which pain interferes with a patient’s sleep over the past week on an NRS (ranging from 0 [did not interfere with sleep] to 10 [completely interfered with sleep]). It is derived from the Pain Interference with Sleep item of the Brief Pain Inventory – Short Form.40 EQ-5D-5L, a standardized, self-administered questionnaire, consists of five-dimension descriptive system (ie, mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and visual analog scale. Each dimension has five levels of severity (ie, no problems, slight problems, moderate problems, severe problems, and extreme problems).41 The severity level against each dimension is combined to calculate a single utility index value. The index score for the Japanese population ranged from −0.025 to 1.00 (1 denotes “perfect health” and 0 “death”).42 For this analysis, only the data from the EQ-5D-5L index score were used to assess health status.
Moreover, at baseline, all enrolled patients underwent the self-reported Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS)43 after a physical examination; however, it was later not used for diagnosis.
Safety was evaluated by reports of adverse events (AEs). AEs were considered treatment-related when there was a reasonable possibility of a causal relationship between the treatment and AE. Any AEs in patients administered with pregabalin of any dose that met the following conditions were considered serious: resulted in death; life-threatening; required inpatient hospitalization or prolongation of hospitalization; resulted in persistent or significant disability/incapacity (substantial disruption of the ability to perform normal life functions); or resulted in congenital anomaly/birth defect.
Statistical Analyses
A dataset of patients with chronic pain with an NeP component from spine diseases was created by pooling data from individual studies (Study 1333 and Study 1354) and were grouped according to the treatment received (pregabalin or usual care group). All patients who received at least one dose of pregabalin or usual care were included in the dataset, and baseline characteristics were summarized for these patients.
Analysis of PROs was conducted on the full analysis set (FAS), which comprised all pooled patients who received at least one dose of pregabalin or usual care and had at least one post-baseline evaluable PRO assessment. Changes in PRO scores from baseline at weeks 4 and 8 were summarized and compared between pregabalin and usual care groups, using the mixed effect model for repeated measurements, including fixed categorical effects of treatment, visit, and treatment-by-visit interaction as well as a fixed continuous effect of baseline value. A shift in the pain intensity level, based on the NRS score, from baseline to week 8 was described in patients with NRS data at week 8 available. The proportion of patients reporting pain intensity level as mild, moderate, or severe, based on the NRS score at week 8, was summarized by baseline pain intensity level (moderate or severe) for each treatment group. PRO score changes were also summarized for subgroups of patients stratified by primary diagnosis.
To explore patient profiles associated with treatment response, treatment response state was summarized for subgroups of patients stratified by whether their main pain was perceived as radiating, and by pain duration. Treatment responder was defined by an NRS reduction of ≥30%. Patients’ perception of whether their main pain was radiating or not was defined, according to areas on the S-LANSS body maps the patients marked (Supplementary Figure 1). Patients in Study 1333 were considered to perceive their main pain radiating if they marked on ipsilateral adjacent areas of the lower half of the body; those in Study 1354 were considered as such when they marked the ipsilateral adjacent areas of the upper half of the body. Patients who did not perceive their main pain radiating had other patterns, including marks on a single area, multiple distant areas, and bilateral or contralateral areas, for both studies. We assessed the association between perception of radiating main pain and treatment responder state by using logistic regression analysis, adjusted for sex, age, and NRS at baseline, and calculated adjusted odds ratio (OR) of the responder state and its 95% confidence interval (CI). The logistic regression analysis included patients with NRS data available at week 8.
For safety analysis, AEs reported were summarized in the safety analysis set. The safety analysis set included all patients who received at least one dose of pregabalin.
P < 0.05 was considered statistically significant for the overall population. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Baseline Characteristics
In this study, pooled data comprised of 331 patients from Study 1333 and 369 patients from Study 1354. In total, 700 patients were treated with pregabalin (pregabalin group, n = 302) or usual care (usual care group, n = 398). Of these, excluding 24 and 9 patients without post-baseline evaluable PRO assessment data from the pregabalin and usual care groups, respectively, 667 patients (pregabalin group, n = 278 and usual care group, n = 389) were included in the FAS. All 302 patients in the pregabalin group were included in the safety analysis set.
Baseline characteristics of the pooled patients are provided by the treatment group in Table 2. In the pregabalin group, male and female proportions were almost similar (female: 53.0%), whereas in the usual care group, females accounted for a larger proportion (65.8%). Mean (standard deviation [SD]) age was slightly higher in the usual care group than in the pregabalin group (68.3 [14.4] years vs 63.9 [15.9] years). The distribution pattern of primary diagnosis was mostly similar between both treatment groups, and the most common diagnosis was cervical spondylotic radiculopathy (28.1% for pregabalin and 27.9% for usual care). Mean pain duration was slightly shorter in the pregabalin group than in the usual care group (50.4 months vs 56.7 months). At baseline, most of the patients in both treatment groups had received NSAIDs (95.0% for pregabalin and 92.0% for usual care). At baseline, the mean (SD) NRS and PRSIS were higher in the pregabalin group than in the usual care group (NRS: 6.2 [1.2] vs 5.8 [1.1]; PRSIS: 3.2 [2.5] vs 2.8 [2.2]), while the mean (SD) EQ-5D-5L scores were comparable between both treatment groups (pregabalin: 56.9 [18.1]; usual care: 57.0 [15.6]). During the study period, the median (min–max) pregabalin dose administered per patient was 50 mg/day (25–300 mg/day).
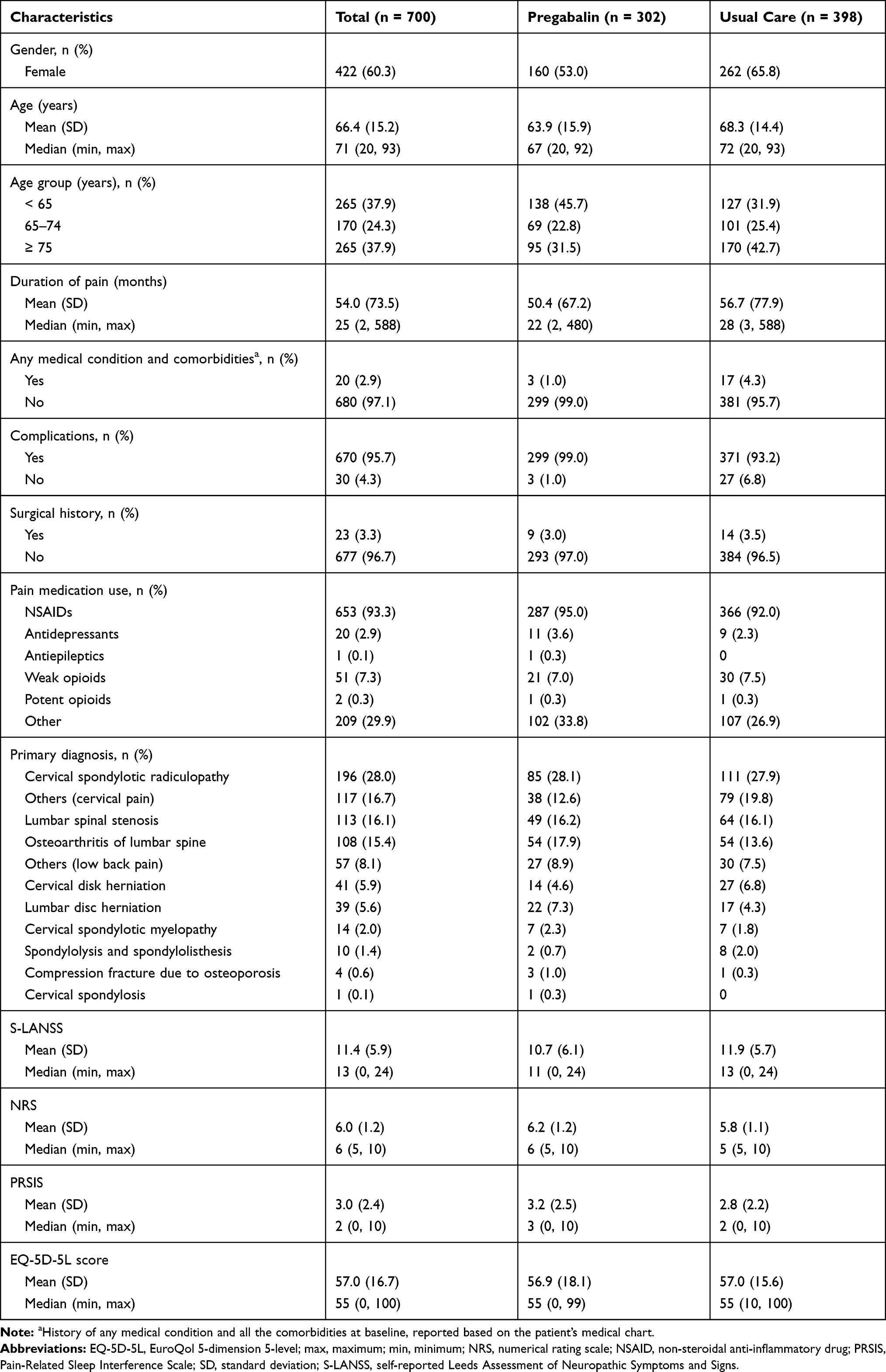 |
Table 2 Baseline Characteristics of Studies Included in the Pooled Analysis |
Effectiveness Based on PRO Measures
Least squares (LS) mean change (95% CI) in NRS scores continued to decrease from baseline through week 8 in both treatment groups (pregabalin: −1.50 [95% CI: −1.71, −1.29] at week 4 and −2.21 [95% CI: −2.44, −1.98] at week 8; usual care: −0.77 [95% CI: −0.94, −0.60] at week 4 and −1.15 [95% CI: −1.34. −0.96] at week 8) (Figure 1A). The improvement was significantly greater in the pregabalin group than in the usual care group (between-treatment difference in LS mean from baseline) both at week 4 (−0.73 [95% CI: −1.00, −0.46]; P < 0.0001) and at week 8 (−1.06 [95% CI: −1.36. −0.76]; P < 0.0001).
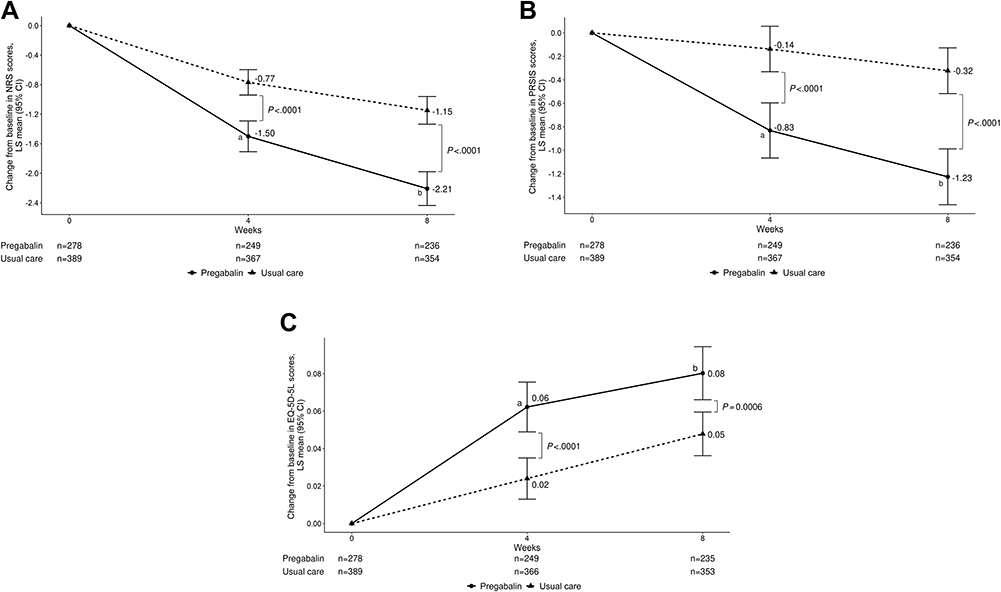 |
Figure 1 Least-squares mean change in NRS scores (A), PRSIS scores (B), and EQ-5D-5L scores (C) from baseline at week 4 and week 8.Notes: Data from the FAS are presented. LS mean (95% CI) treatment difference (pregabalin vs usual care) in (A) aWeek 4: -0.73 (-1.00, -0.46); bWeek 8: -1.06 (-1.36, -0.76), (B) aWeek 4: -0.69 (-1.00, -0.39); bWeek 8: -0.90 (-1.21, -0.60), (C) aWeek 4: 0.04 (0.02, 0.06); bWeek 8: 0.03 (0.01, 0.05).Abbreviations: CI, confidence interval; EQ-5D-5L, EuroQol 5-dimension 5-level; FAS, full analysis set; LS, least-squares; NRS, numerical rating scale; PRSIS, Pain-Related Sleep Interference Scale. |
Figure 2 summarizes the shift in the pain intensity level from baseline to week 8. The proportion of patients who continued to have the same pain intensity level from baseline at week 8 was smaller in the pregabalin group than in the usual care group (moderate pain: 49.7% vs 69.3% (Figure 2A); severe pain: 21.3% vs 42.5% (Figure 2B)). Correspondingly, the proportion of patients who had a shift in the pain intensity level towards lower severity was higher in the pregabalin group than in the usual care group (shift from moderate to mild: 44.7% [72/161 patients] vs 23.0% [63/274 patients]; shift from severe to moderate or mild: 78.7% [59/75 patients] vs 57.5% [46/80 patients]).
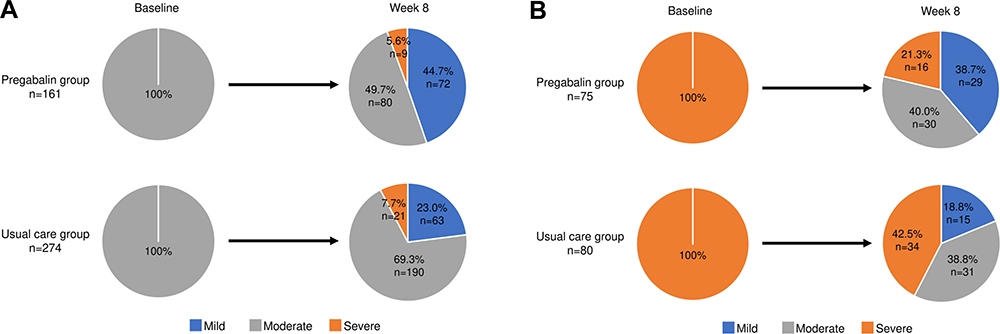 |
Figure 2 Shift in the pain intensity level from baseline to week 8 by intensity level at baseline (A) moderate and (B) severe.Note: Pain intensity level was based on NRS: mild (0–3), moderate (4–6), and severe (7–10). Patients included were those with available NRS data at Week 8.Abbreviation: NRS, numerical rating scale. |
LS mean change (95% CI) in PRSIS scores from baseline decreased at both week 4 and week 8 in the pregabalin group, while there was not much change observed in the usual care group during the same time period (pregabalin: −0.83 [95% CI: −1.07, −0.60] at week 4 and −1.23 [95% CI: −1.46, −0.99] at week 8; usual care: −0.14 [95% CI: −0.33, 0.06] at week 4 and −0.32 [95% CI: −0.52, −0.13] at week 8) (Figure 1B). Significantly greater improvement in PRSIS scores was observed in the pregabalin group than in the usual care group (LS mean treatment difference: −0.69 [95% CI: −1.00, −0.39; P < 0.0001] at week 4 and −0.90 [95% CI: −1.21, −0.60; P < 0.0001] at week 8).
LS mean change (95% CI) in EQ-5D-5L scores continued to improve from baseline through week 8 in both treatment groups (pregabalin: 0.06 [95% CI: 0.05, 0.08] at week 4 and 0.08 [95% CI: 0.07, 0.09] at week 8; usual care: 0.02 [95% CI: 0.01, 0.03] at week 4 and 0.05 [95% CI: 0.04, 0.06] at week 8) (Figure 1C). However, the improvement was significantly greater in the pregabalin group than in the usual care group (LS mean treatment difference: 0.04 [95% CI: 0.02, 0.06; P < 0.0001] at week 4 and 0.03 [95% CI: 0.01, 0.05; P = 0.0006] at week 8).
Subgroup Analysis by Primary Diagnosis
Stratification by primary diagnosis yielded a small number of patients for each diagnosis subgroup (Figure 3A–C). Although the change in NRS (Figure 3A), PRSIS (Figure 3B), and EQ-5D-5L scores (Figure 3C) from baseline at week 8 varied by each diagnosis, the overall trend was greater improvement across all three PRO measures in the pregabalin group compared with the usual care group, irrespective of the primary diagnosis. Changes in PRO scores from baseline at week 8 favoring usual care over pregabalin tended to be seen in very small diagnosis subgroups.
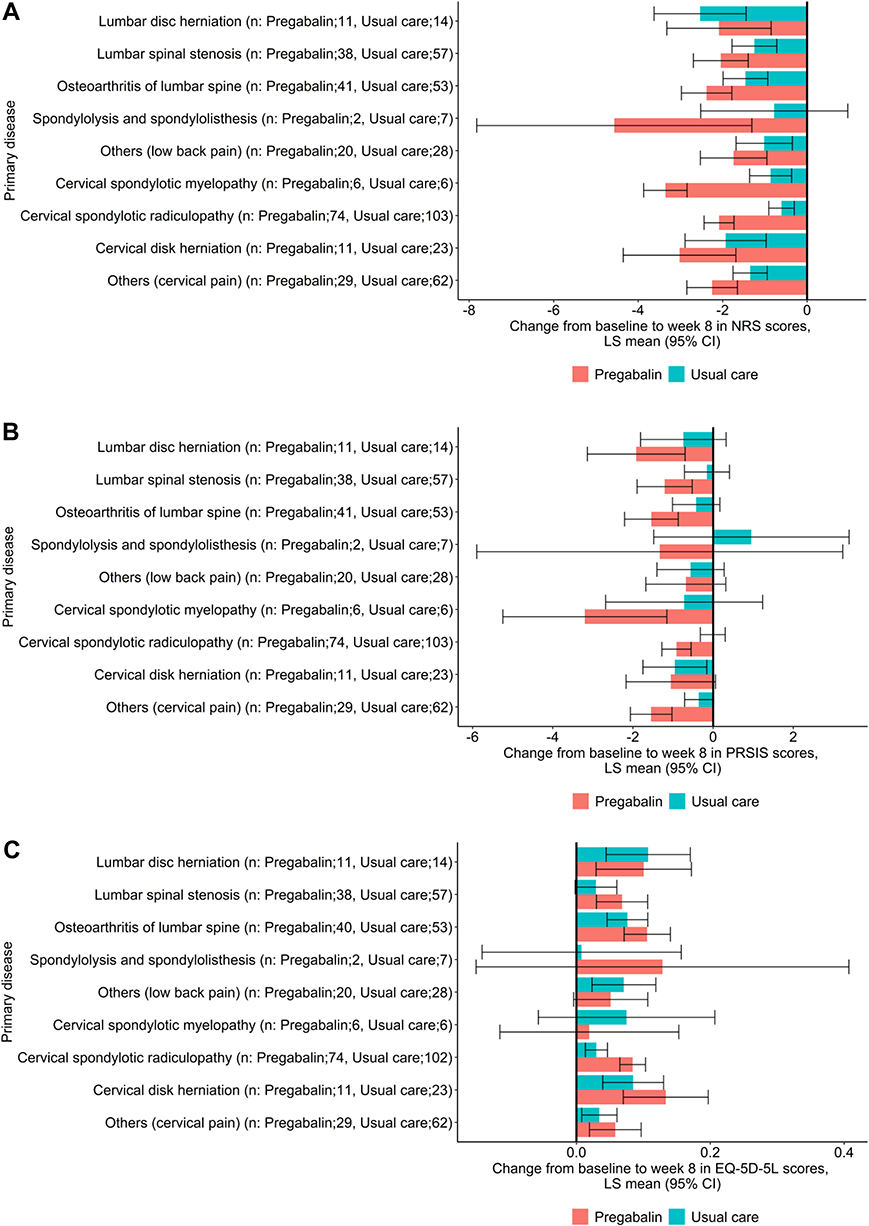 |
Figure 3 Change in NRS scores (A), PRSIS scores (B), and EQ-5D-5L scores (C) from baseline by primary diagnosis at week 8.Notes: Data from the FAS are presented. The number of patients diagnosed with compression fracture due to osteoporosis or cervical spondylosis was too small to estimate the treatment effects in the model, and thus these subgroups were not included in this analysis.Abbreviations: CI, confidence interval; EQ-5D-5L, EuroQol 5-dimension 5-level; FAS, full analysis set; LS, least-squares; NRS, numerical rating scale; PRSIS, Pain-Related Sleep Interference Scale. |
Responder Analysis
Slightly over half of the patients in the pregabalin group achieved “responder” status for pain relief (ie, ≥30% reduction in NRS), irrespective of whether or not the patients perceived their main pain radiating (55.5% vs 55.9% (Table 3); OR: 0.976 [95% CI: 0.59, 1.61]). In the usual care group, the proportion of patients who achieved “responder” status tended to be slightly lower in those who perceived their main pain radiating than those who did not (26.0% vs 34.8%; OR: 0.653 [95% CI: 0.42, 1.03]).
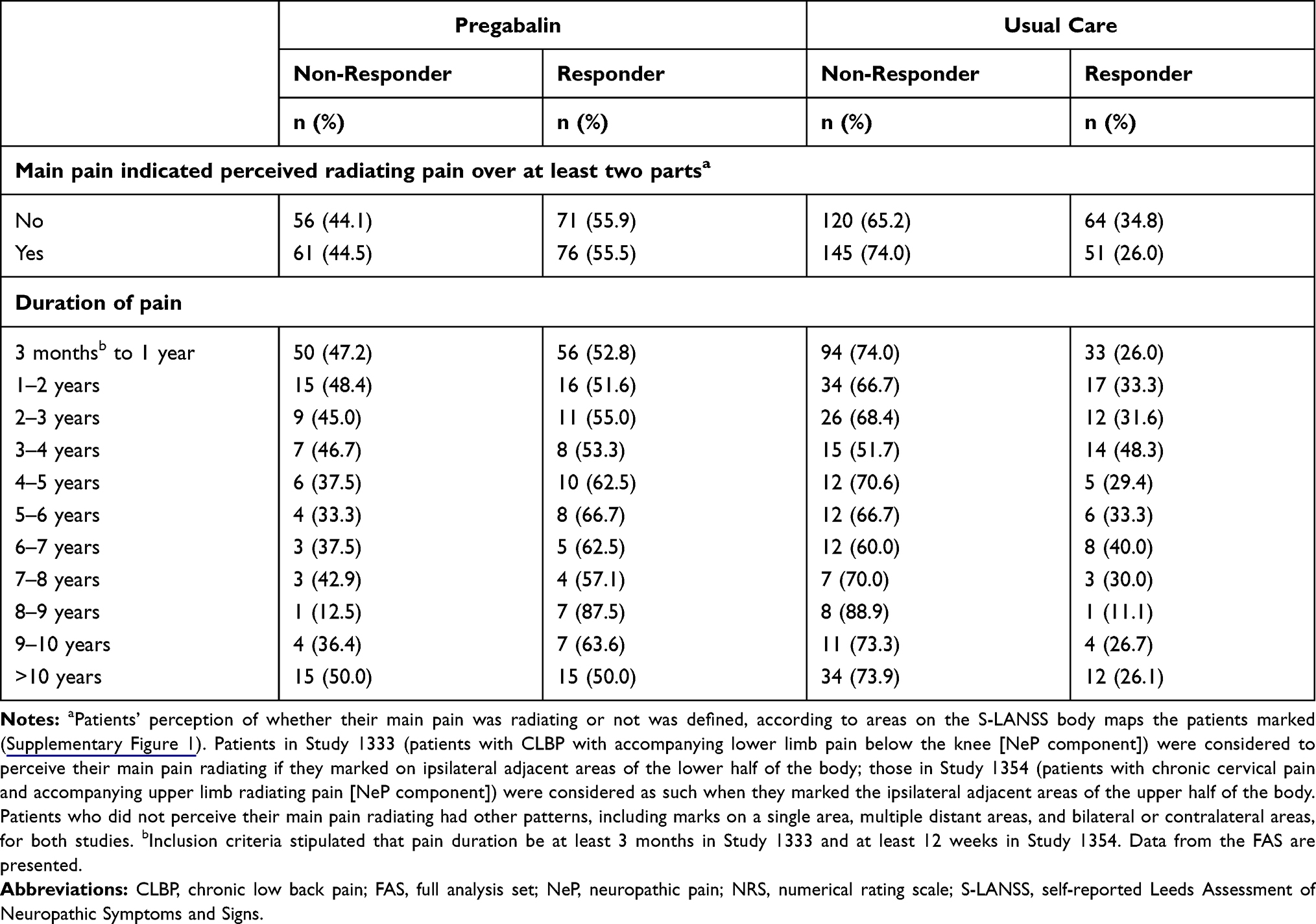 |
Table 3 Responder Analysis (≥30% Reduction in NRS) by Patient Characteristics |
In the pregabalin group, more than 50% of patients achieved “responder” status for pain relief, irrespective of pain duration (Table 3). In the usual care group, a majority of patients were “non-responders”, irrespective of pain duration. No linear increase or decrease in the trend was observed for responder rate by pain duration in either treatment group.
Safety
In the safety analysis set patients (pregabalin group), 36.1% reported AEs (Table 4). AEs reported in 20.9% of the patients were considered treatment-related and none was serious. Treatment-related AEs led to discontinuation in 7.0% of the patients. The most common treatment-related AEs in the pregabalin group were dizziness (10.3%) and somnolence (8.9%). Other treatment-related AEs were reported in less than 1% of patients in the pregabalin group.
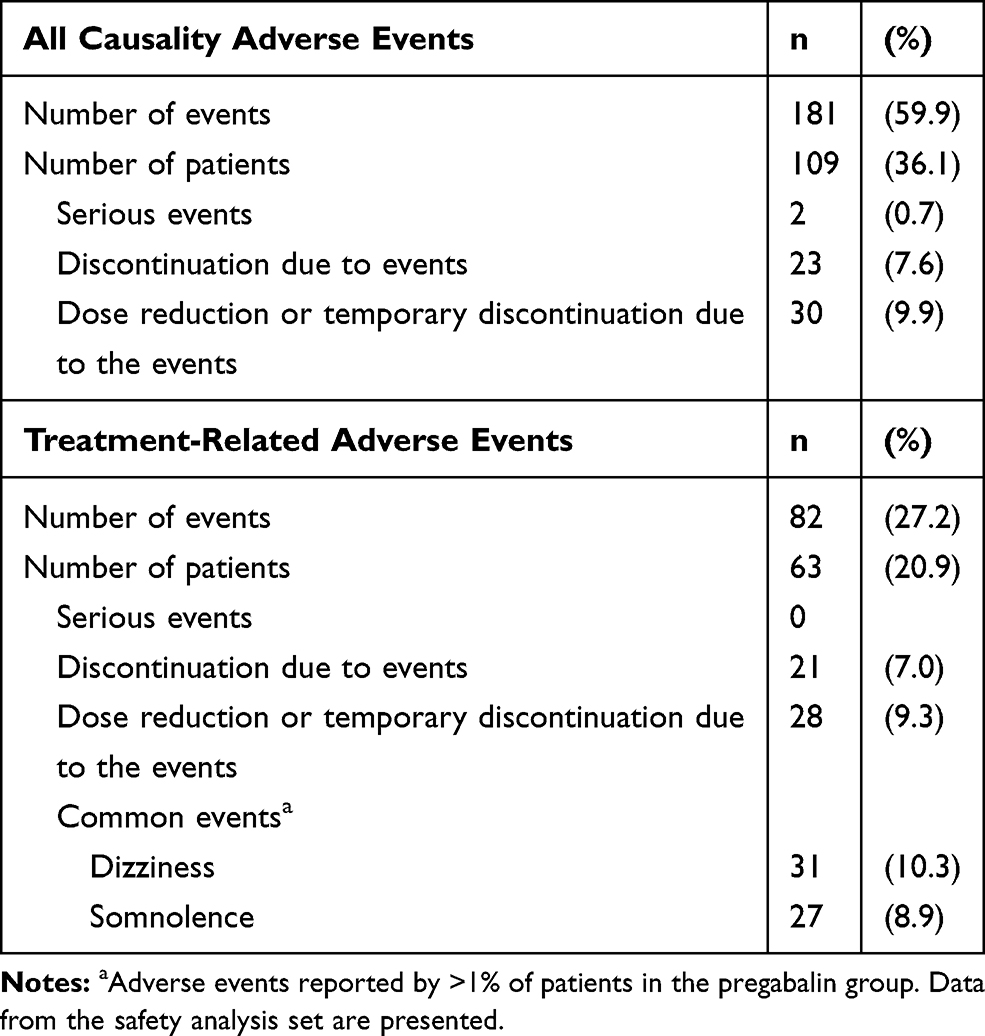 |
Table 4 Adverse Events Reported in the Pregabalin Group in the Pooled Analysis (n = 302) |
Discussion
In this pooled analysis, we aimed to obtain a comprehensive picture of therapeutic values of pregabalin for chronic pain with NeP component in patients with spine diseases. All the PROs, pain intensity, pain-related sleep interference, and health status significantly improved from baseline through week 8 in the pregabalin group (alone or in combination with other analgesics), compared with the usual care group. Multi-dimensional effectiveness of treatment using pregabalin, previously separately demonstrated in the original observational studies,33,34 was shown to be evident in the entire population of patients with chronic pain with NeP component from spine diseases in routine primary care settings.
The goal of NeP treatment is not only to reduce pain, but also to improve daily living and QOL, rather than to eliminate the pain since a cure for the condition has not yet been established.14 When interpreted in reference to the minimal important difference (MID) and clinically meaningful improvement previously reported,44–48 the degree of improvement in all PRO measures in the present analysis suggests that patients may have achieved not only statistically significant but also clinically meaningful improvement in pain and various aspects of their lives after 8 weeks of pregabalin treatment. NRS scores improved at week 8 by −2.21 in the pregabalin group and by −1.15 in the usual care group. The pregabalin group exceeded 2.0, reported as the clinically important difference associated with much improvement or greater on Patient Global Impression of Change (PGIC) in patients with chronic pain44 and as the value associated with much better improvement in chronic musculoskeletal pain,45 and was also determined as a key threshold score, associated with improvement or much improvement on PGIC, in treatment for Japanese patients with CLBP.46 Similarly, improvement in PRSIS by −1.23 and EQ-5D-5L scores by 0.08 at week 8 in the pregabalin group exceeded the MID of 1–247 and 0.061,48 respectively, but not in the usual care group (PRISIS and EQ-5D-5L score improvement from baseline: −0.32 and 0.05, respectively). It should be noted that the MID for PRSIS referred to Daily Sleep Interference Scale, similar to PRSIS with an 11-point NRS of sleep interference by pain, except for a recall period of the past 24 h.47 Even though the data were not utilized in the present pooled analysis, the original studies33,34 reported functional improvement measured by the Roland-Morris Disability Questionnaire and Neck Disability Index both exceeded the MID (3.549 and 8.5,50 respectively). The present and original study results suggest the effectiveness of pregabalin treatment not only for pain relief but also for improvement in various aspects, including pain-related sleep interference, function, and QOL. Furthermore, the pathway by which pain, pain-related sleep interference, and function influence QOL was clarified in another study using data from the pregabalin group patients from the same original studies.33,34 It was demonstrated that the impact of pain reduction on QOL improvement achieved after treatment with pregabalin consisted of direct and indirect effects, but with greater contribution of indirect impact via functional improvement (Unpublished data, Taguchi et al 2020). Therefore, treatment with pregabalin may play an important role, not only from the perspective of pain relief but also QOL, to achieve a treatment goal of NeP to reduce the multi-faceted burdens of patients beyond pain itself.
Focusing on pain relief, one of the essentials of NeP treatment, pain was alleviated to a lower level for more patients in the pregabalin group than in the usual care group, regardless of whether it was moderate or severe at baseline. This trend is consistent with observations from pooled analysis of RCTs in Japanese patients with postherpetic neuralgia, diabetic neuropathy, and spinal cord injury.51 Improvement in persistent pain that had not been relieved with other analgesics for at least 3 months after 8-week treatment with pregabalin, without unknown or any major safety concerns may be promising for patients.
Greater improvement in all the PRO measures in pregabalin than in the usual care group was also generally demonstrated across different primary diagnoses by subgroup analysis (Figure 3). Minor variations in the trend in some subgroups may largely be attributed to the small number of patients included in the subgroup. In addition, considering the greater burden associated with chronic NeP than those without an NeP component,7–11 the degree of involvement of NeP may also contribute to the variations. When comparing the results of the original studies, more patients with CLBP with an NeP component responded to usual care33 than those with chronic cervical pain with an NeP component.34 It was suggested that more patients in Study 1333 had CLBP of greater involvement of nociceptive and less of NeP, while more patients in Study 1354 had cervical pain with greater involvement of NeP and less nociceptive pain. Therefore, the degree of burden and responses to treatment may be different, relative to chronic cervical pain.
To explore who can benefit from treatment with pregabalin, we further conducted a responder analysis by stratifying patients according to their perceptions of whether the main pain was radiating or not, and their pain duration (Table 3). Based on the trend described, it is inferred that more than half of the patients may be able to equally benefit from treatment using pregabalin, regardless of whether their main pain was radiating or not, or regardless of how many years they had been suffering from the pain. In contrast, the majority of patients in all the subgroups did not seem to respond to usual care; even in patients who considered that their main pain was not radiating, only 34.8% of patients achieved ≥30% pain relief. Considering varying etiologies of NeP and characteristics of each patient, the finding that practical effectiveness of pregabalin across diverse diagnoses of spine diseases, pain, and patient characteristics may provide useful information for the use of pregabalin, one of the first-line treatment for NeP, in daily clinical practice.
Based on the accumulated evidence in various conditions associated with an NeP component, such as postherpetic neuralgia,23–26 diabetic neuropathy,27,28,52,53 spinal cord injury,29 and painful lumbar or cervical radiculopathy,35–37 pregabalin is recommended as one of the first-line treatments for NeP.14,21,22 However, in some RCTs in patients with NeP associated with spine diseases, the efficacy of pregabalin was not shown to be greater than that obtained in the placebo group,30–32 partially due to a high placebo response. For example, the RCT in patients with acute or chronic sciatica, reported pain intensity was reduced by about 50% from baseline to week 8 in both the pregabalin and placebo groups, and nearly two-thirds of both groups were satisfied with their treatments.30 Their study population comprised mostly of acute cases (pain < 3 months in 80.2%).30 Considering that the sciatica pain resolves early (2 weeks in 36% and 12 weeks in 73%) without surgery,54 these improvements in both groups may have reflected spontaneous recovery. Moreover, in an RCT in patients with chronic lumbosacral radiculopathy,31 pain relief during the single-blinded pregabalin treatment phase may have been carried over to the following double-blind treatment phase, leading to a lack of separation of treatment effect by pregabalin from those by placebo. Furthermore, the possible involvement of the nociceptive component of the target conditions (sciatica,30 lumbosacral radiculopathy,31 and lumbar spinal stenosis32) may have affected the treatment response. For example, in an RCT in patients with sciatica, the baseline PainDETECT score suggested that most of the patients were likely to have had predominantly nociceptive pain or unlikely/uncertain neuropathic pain component.30 Taken together, the possibility of pregabalin’s effectiveness for chronic pain with an NeP component from spine diseases may not be completely excluded, and may require further consideration.
Adverse events reported were consistent with the known safety profile of pregabalin in the Japanese patient population.55 However, prescriptions should be made based on careful consideration of overall benefits and risks. Less-than recommended dose of pregabalin administered during the study period (150–600 mg/day)33,34 suggests that physicians may have carefully adjusted the pregabalin dose according to each patient based on the renal function because the included study population was relatively old (mean age: 66.4 years), and most of them were concomitantly prescribed other analgesics, such as NSAIDs.
This study has some limitations. First, inclusion criteria of moderate to severe cases refractory to analgesics may limit the generalizability of the dataset. Nevertheless, pain resolves without the need for pharmacological intervention for some patients, while for others, it is not until NeP becomes chronic that treatment with pregabalin is successfully introduced. Second, the potential for bias in treatment selection because the decision rested on the physician’s discretion, but at the same time, this approach reflects “real-world” treatment practice, which does not necessarily endorse balanced treatment strategies. Third, this study may not conclude the effectiveness solely attributed to pregabalin, since other analgesics were permitted to be used in combination with pregabalin. In Studies 133333 and 1354,34 most of the patients received concomitant medications at baseline and during study periods (pregabalin group: at least 91% in Study 1333 and at least 72% in Study 1354, respectively; usual care group: at least 99% in both studies), most of which were NSAIDs34 (data of Study 1333 not shown). Lastly, whether the main pain was perceived radiating or not was identified when the marks of the worst pain site made by a patient were spreading to the adjacent areas. On the other hand, diagnosis of radiating pain by physicians may be different, as it usually follows a specific dermatome. There may remain a possibility that our definition underestimates patients who could not recognize their main pain radiating.
Conclusions
This pooled analysis suggests multi-faceted effectiveness of treatment with pregabalin, alone or in combination with other analgesics, from the patient’s perspectives under a “real-world” practice in all patients with chronic NeP from spine diseases, a common but previously under-appreciated population. The trends observed across the subgroups may suggest that patients with various diagnoses and profiles (irrespective of whether the main pain was perceived as radiating, or how long the pain had persisted) possibly benefit from treatment with pregabalin. These findings suggest important therapeutic values of pregabalin as one of the first-line treatments for chronic pain with an NeP component in patients with spine diseases.
Abbreviations
AEs, adverse events; CI, confidence interval; CLBP, chronic low back pain; EQ-5D-5L, EuroQol 5-dimension 5-level; FAS, full analysis set; LS, least squares; MID, minimal important difference; NeP, neuropathic pain; NRS, numerical rating scale; NSAIDs, non-steroidal anti-inflammatory drugs; OR, odds ratio; PGIC, Patient Global Impression of Change; PRO, patient-reported outcome; PRSIS, Pain-Related Sleep Interference Scale; QOL, quality of life; RCT, randomized controlled trial; SD, standard deviation; S LANSS, self-reported Leeds Assessment of Neuropathic Symptoms and Signs.
Data Sharing Statement
Upon request, and subject to certain criteria, conditions and exceptions (see https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information), Pfizer will provide access to individual de-identified participant data from Pfizer-sponsored global interventional clinical studies conducted for medicines, vaccines and medical devices (1) for indications that have been approved in the US and/or EU or (2) in programs that have been terminated (ie, development for all indications has been discontinued). Pfizer will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data may be requested from Pfizer trials 24 months after study completion. The de-identified participant data will be made available to researchers whose proposals meet the research criteria and other conditions, and for which an exception does not apply, via a secure portal. To gain access, data requestors must enter into a data access agreement with Pfizer.
Acknowledgments
Statistical analysis support was provided by Ryozo Wakabayashi at Clinical Study Support, Inc. (Nagoya, Japan), and medical writing support was provided by Emiko Sato at Clinical Study Support, Inc. (Nagoya, Japan) and funded by Pfizer.
Funding
This research was sponsored by Pfizer. The funder was involved in the manuscript writing, editing, and approval, and decision to publication.
Disclosure
Shogo Nakano and Kazutaka Nozawa were employees of Pfizer Japan, Inc. at the time of study conduct and manuscript development. Toshihiko Taguchi was not financially compensated for their collaboration in this project or for the development of this manuscript, although Toshihiko Taguchi has received honorarium from Pfizer Japan Inc. outside of this work. The authors report no other conflicts of interest relevant to this work.
References
1. Fujii T, Matsudaira K. Prevalence of low back pain and factors associated with chronic disabling back pain in Japan. Eur Spine J. 2013;22(2):432–438. doi:10.1007/s00586-012-2439-0
2. Takasawa E, Yamamoto A, Kobayashi T, et al. Characteristics of neck and shoulder pain in the Japanese general population. J Orthop Sci. 2015;20(2):403–409. doi:10.1007/s00776-014-0676-2
3. International Association for the Study of Pain [homepage on the Internet]. Washington, D.C.: IASP Terminology; 2017. Available from: https://www.iasp-pain.org/terminology?navItemNumber=576#Neuropathicpain.
4. Ogawa S, Komatsu M, Ohno S, Yamane H, Hayakawa K. Pregabalin (Lyrica) Shiyou seiseki chousa: chukan kaiseki houkokusho [Interim report of drug use investigations of pregabalin (Lyrica)]. Prog Med. 2013;33(10):2159–2171.
5. Yamashita T, Takahashi K, Yonenobu K, Kikuchi S. Prevalence of neuropathic pain in cases with chronic pain related to spinal disorders. J Orthop Sci. 2014;19(1):15–21. doi:10.1007/s00776-013-0496-9
6. Ogawa S, Iseki M, Kikuchi S. A large-scale survey on chronic pain and neuropathic pain in Japan. J Jpn Clin Orthop Assoc. 2012;47(6):565–574.
7. Torrance N, Smith BH, Bennett MI, Lee AJ. The epidemiology of chronic pain of predominantly neuropathic origin. Results from a general population survey. J Pain. 2006;7(4):281–289. doi:10.1016/j.jpain.2005.11.008
8. Hiyama A, Watanabe M, Katoh H, Sato M, Sakai D, Mochida J. Evaluation of quality of life and neuropathic pain in patients with low back pain using the Japanese orthopedic association back pain evaluation questionnaire. Eur Spine J. 2015;24(3):503–512. doi:10.1007/s00586-014-3723-y
9. Inoue S, Taguchi T, Yamashita T, Nakamura M, Ushida T. The prevalence and impact of chronic neuropathic pain on daily and social life: a nationwide study in a Japanese population. Eur J Pain. 2017;21(4):727–737. doi:10.1002/ejp.977
10. Kim JH, Hong JT, Lee CS, et al. Prevalence of neuropathic pain and patient-reported outcomes in Korean adults with chronic low back pain resulting from neuropathic low back pain. Asian Spine J. 2017;11(6):917–927. doi:10.4184/asj.2017.11.6.917
11. Smith BH, Torrance N, Bennett MI, Lee AJ. Health and quality of life associated with chronic pain of predominantly neuropathic origin in the community. Clin J Pain. 2007;23(2):143–149. doi:10.1097/01.ajp.0000210956.31997.89
12. Wong WS, Chan ST, Fung VB, Fielding R. The differential mediating effects of pain and depression on the physical and mental dimension of quality of life in Hong Kong Chinese adults. Health Qual Life Outcomes. 2010;8(1):1. doi:10.1186/1477-7525-8-1
13. Gunnarsdottir S, Ward SE, Serlin RC. A population based study of the prevalence of pain in Iceland. Scand J Pain. 2010;1(3):151–157. doi:10.1016/j.sjpain.2010.05.028
14. Japanese Society of Pain Clinicians [homepage on the Internet]. Tokyo: guidelines for the pharmacologic management of neuropathic pain. Second edition; 2016. Available from: http://minds4.jcqhc.or.jp/minds/Pharmacologic-management-of-neuropathic-pain/Pharmacologic-Management-of-Neuropathic-pain-ENGver.pdf.
15. Field MJ, Cox PJ, Stott E, et al. Identification of the alpha2-delta-1 subunit of voltage-dependent calcium channels as a molecular target for pain mediating the analgesic actions of pregabalin. Proc Natl Acad Sci U S A. 2006;103(46):17537–17542. doi:10.1073/pnas.0409066103
16. Fink K, Dooley DJ, Meder WP, et al. Inhibition of neuronal Ca2+ influx by gabapentin and pregabalin in the human neocortex. Neuropharmacology. 2002;42(2):229–236. doi:10.1016/S0028-3908(01)00172-1
17. Maneuf YP, Hughes J, McKnight AT. Gabapentin inhibits the substance P-facilitated K(+)-evoked release of [(3)H]glutamate from rat caudial trigeminal nucleus slices. Pain. 2001;93(2):191–196. doi:10.1016/S0304-3959(01)00316-5
18. Tanabe M, Takasu K, Takeuchi Y, Ono H. Pain relief by gabapentin and pregabalin via supraspinal mechanisms after peripheral nerve injury. J Neurosci Res. 2008;86(15):3258–3264. doi:10.1002/jnr.21786
19. Bee LA, Dickenson AH. Descending facilitation from the brainstem determines behavioural and neuronal hypersensitivity following nerve injury and efficacy of pregabalin. Pain. 2008;140(1):209–223. doi:10.1016/j.pain.2008.08.008
20. Pfizer Inc, Eisai [homepage on the Internet]. Lyrica® capsules approved in Japan for additional indication of pain associated with fibromyalgia; 2012. Available from: https://www.eisai.com/news/pdf/enews201236pdf.pdf.
21. National Institute for Health and Clinical Excellence [homepage on the Internet]. Neuropathic pain – pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist settings. NICE; 2013. Available from: http://www.nice.org.uk/guidance/cg173/chapter/1-recommendations.
22. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/S1474-4422(14)70251-0
23. Sabatowski R, Galvez R, Cherry DA, et al. Pregabalin reduces pain and improves sleep and mood disturbances in patients with post-herpetic neuralgia: results of a randomised, placebo-controlled clinical trial. Pain. 2004;109(1–2):26–35. doi:10.1016/j.pain.2004.01.001
24. van Seventer R, Feister HA, Young JP
25. Dworkin RH, Corbin AE, Young JP
26. Ogawa S, Suzuki M, Arakawa A, Araki S, Yoshiyama T. efficacy and tolerability of pregabalin for postherpetic neuralgia: a multicenter, randomized, double-blind, placebo-controlled clinical trial. J Jpn Soc Pain Clinicians. 2010;17(2):141–152.
27. Rosenstock J, Tuchman M, LaMoreaux L, Sharma U. Pregabalin for the treatment of painful diabetic peripheral neuropathy: a double-blind, placebo-controlled trial. Pain. 2004;110(3):628–638. doi:10.1016/j.pain.2004.05.001
28. Lesser H, Sharma U, LaMoreaux L, Poole RM. Pregabalin relieves symptoms of painful diabetic neuropathy: a randomized controlled trial. Neurology. 2004;63(11):2104–2110. doi:10.1212/01.WNL.0000145767.36287.A1
29. Cardenas DD, Nieshoff EC, Suda K, et al. A randomized trial of pregabalin in patients with neuropathic pain due to spinal cord injury. Neurology. 2013;80(6):533–539. doi:10.1212/WNL.0b013e318281546b
30. Mathieson S, Maher CG, McLachlan AJ, et al. Trial of pregabalin for acute and chronic sciatica. N Engl J Med. 2017;376(12):1111–1120. doi:10.1056/NEJMoa1614292
31. Baron R, Freynhagen R, Tolle TR, et al. The efficacy and safety of pregabalin in the treatment of neuropathic pain associated with chronic lumbosacral radiculopathy. Pain. 2010;150(3):420–427. doi:10.1016/j.pain.2010.04.013
32. Markman JD, Frazer ME, Rast SA, et al. Double-blind, randomized, controlled, crossover trial of pregabalin for neurogenic claudication. Neurology. 2015;84(3):265–272. doi:10.1212/WNL.0000000000001168
33. Taguchi T, Igarashi A, Watt S, et al. Effectiveness of pregabalin for the treatment of chronic low back pain with accompanying lower limb pain (neuropathic component): a non-interventional study in Japan. J Pain Res. 2015;8:487–497. doi:10.2147/JPR.S88642
34. Taguchi T, Nozawa K, Parsons B, et al. Effectiveness of pregabalin for treatment of chronic cervical radiculopathy with upper limb radiating pain: an 8-week, multicenter prospective observational study in Japanese primary care settings. J Pain Res. 2019;12:1411–1424. doi:10.2147/JPR.S191906
35. Flórez-García M, Ceberio-Balda F, Morera-Domínguez C, Masramón X, Pérez M. Effect of pregabalin in the treatment of refractory neck pain: cost and clinical evidence from medical practice in orthopedic surgery and rehabilitation clinics. Pain Pract. 2011;11(4):369–380. doi:10.1111/j.1533-2500.2010.00430.x
36. Morera-Domínguez C, Ceberio-Balda F, Flórez-García M, Masramón X, López-Gómez V. A cost-consequence analysis of pregabalin versus usual care in the symptomatic treatment of refractory low back pain: sub-analysis of observational trial data from orthopaedic surgery and rehabilitation clinics. Clin Drug Investig. 2010;30(8):517–531. doi:10.2165/11536280-000000000-00000
37. Saldana MT, Navarro A, Perez C, Masramon X, Rejas J. Patient-reported-outcomes in subjects with painful lumbar or cervical radiculopathy treated with pregabalin: evidence from medical practice in primary care settings. Rheumatol Int. 2010;30(8):1005–1015. doi:10.1007/s00296-009-1086-1
38. Toelle TR, Varvara R, Nimour M, Emir B, Brasser M. Pregabalin in neuropathic pain related to DPN, cancer and back pain analysis of a 6-week observational study. Open Pain J. 2012;5(1):1–11. doi:10.2174/1876386301205010001
39. Sakai Y, Ito K, Hida T, Ito S, Harada A. Neuropathic pain in elderly patients with chronic low back pain and effects of pregabalin: a preliminary study. Asian Spine J. 2015;9(2):254–262. doi:10.4184/asj.2015.9.2.254
40. Cleeland CS, Ryan KM. Pain assessment: global use of the brief pain inventory. Ann Acad Med Singapore. 1994;23(2):129–138.
41. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
42. Ikeda S, Shiroiwa T, Igarashi A, et al. Developing a Japanese version of the EQ-5D-5L value set. J Natl Inst Public Health. 2015;64:47–55.
43. Bennett MI, Smith BH, Torrance N, Potter J. The S-LANSS score for identifying pain of predominantly neuropathic origin: validation for use in clinical and postal research. J Pain. 2005;6(3):149–158. doi:10.1016/j.jpain.2004.11.007
44. Farrar JT, Young JP
45. Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J Pain. 2004;8(4):283–291. doi:10.1016/j.ejpain.2003.09.004
46. Suzuki H, Aono S, Inoue S, et al. Clinically significant changes in pain along the pain intensity numerical rating scale in patients with chronic low back pain. PLoS One. 2020;15(3):e0229228. doi:10.1371/journal.pone.0229228
47. Vernon MK, Brandenburg NA, Alvir JM, Griesing T, Revicki DA. Reliability, validity, and responsiveness of the daily sleep interference scale among diabetic peripheral neuropathy and postherpetic neuralgia patients. J Pain Symptom Manage. 2008;36(1):54–68. doi:10.1016/j.jpainsymman.2007.09.016
48. Shiroiwa T, Fukuda T, Ikeda S, et al. Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Qual Life Res. 2016;25(3):707–719. doi:10.1007/s11136-015-1108-2
49. Ostelo RW, de Vet HC. Clinically important outcomes in low back pain. Best Pract Res Clin Rheumatol. 2005;19(4):593–607. doi:10.1016/j.berh.2005.03.003
50. Young IA, Cleland JA, Michener LA, Brown C. Reliability, construct validity, and responsiveness of the neck disability index, patient-specific functional scale, and numeric pain rating scale in patients with cervical radiculopathy. Am J Phys Med Rehabil. 2010;89(10):831–839. doi:10.1097/PHM.0b013e3181ec98e6
51. Parsons B, Fujii K, Nozawa K, Yoshiyama T, Ortiz M, Whalen E. The efficacy of pregabalin for the treatment of neuropathic pain in Japanese subjects with moderate or severe baseline pain. J Pain Res. 2019;12:1061–1068. doi:10.2147/JPR.S181729
52. Richter RW, Portenoy R, Sharma U, Lamoreaux L, Bockbrader H, Knapp LE. Relief of painful diabetic peripheral neuropathy with pregabalin: a randomized, placebo-controlled trial. J Pain. 2005;6(4):253–260. doi:10.1016/j.jpain.2004.12.007
53. Satoh J, Yagihashi S, Baba M, et al. Efficacy and safety of pregabalin for treating neuropathic pain associated with diabetic peripheral neuropathy: a 14 week, randomized, double-blind, placebo-controlled trial. Diabet Med. 2011;28(1):109–116. doi:10.1111/j.1464-5491.2010.03152.x
54. Vroomen PC, de Krom MC, Knottnerus JA. Predicting the outcome of sciatica at short-term follow-up. Br J Gen Pract. 2002;52(475):119–123.
55. Onouchi K, Koga H, Yokoyama K, Yoshiyama T. An open-label, long-term study examining the safety and tolerability of pregabalin in Japanese patients with central neuropathic pain. J Pain Res. 2014;7:439–447. doi:10.2147/JPR.S63028
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.