Back to Journals » Journal of Pain Research » Volume 18
Effectiveness of Non-Pharmacological Interventions for Pain Management After Laparoscopic Cholecystectomy: A Systematic Review and Network Meta-Analysis
Authors Lei T, Peng Y, Liu Y, Xie Y, Wang J
Received 8 September 2025
Accepted for publication 9 December 2025
Published 20 December 2025 Volume 2025:18 Pages 6933—6946
DOI https://doi.org/10.2147/JPR.S566145
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Houman Danesh
Ting Lei,1 Yanqiong Peng,2 Yuanjun Liu,1 Yaping Xie,3 Junjie Wang1
1Department of Hepato-Biliary-Pancreatic Surgery, Suining Central Hospital, Suining, Sichuan Province, People’s Republic of China; 2Department of Nursing, Suining Central Hospital, Suining, Sichuan Province, People’s Republic of China; 3Nursing Department, the Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian Province, 362000, People’s Republic of China
Correspondence: Yanqiong Peng, Department of Nursing, Suining Central Hospital, Suining, Sichuan Province, People’s Republic of China, Email [email protected] Ting Lei, Department of Hepato-Biliary-Pancreatic Surgery, Suining Central Hospital, Suining, Sichuan Province, People’s Republic of China, Email [email protected]
Background: Although non-pharmacological interventions are widely utilized for postoperative pain management, their comparative effectiveness remains unclear. This network meta-analysis (NMA) aimed to comprehensively evaluate the effects of various non-pharmacological interventions on postoperative pain and anxiety after LC, and to identify the optimal intervention through ranking analysis.
Methods: A literature search was executed to identify relevant randomized controlled trials (RCTs) that investigated non-pharmacological interventions for alleviating pain after laparoscopic cholecystectomy (LC). This search encompassed the electronic databases PubMed, Web of Science, Embase, CINAHL, and the Cochrane Library, with the coverage spanning from the inception of each database to January 2025. Two independent reviewers performed literature search, study selection, quality assessment, and data extraction. The Cochrane Risk of Bias 2.0 tool was employed for bias assessment. A Bayesian NMA was conducted, with surface under the cumulative ranking curve (SUCRA) values used to rank intervention effectiveness.
Results: The review identified 15 types of non-pharmacological interventions. The most common among these were acupressure (n=5), massage (n=4), and transcutaneous electrical nerve stimulation (TENS, n=2). The NMA demonstrated that ear acupressure, aromatherapy, and foot baths ranked as the top three interventions for alleviating postoperative pain after LC. Compared with standard care, all three interventions significantly improved pain scores: ear acupressure (standardized mean difference [SMD] = − 3.61, 95% credible interval [CrI] − 5.71 to − 1.50), essential oil therapy (SMD = − 2.59, 95% CrI − 4.93 to − 0.27), and foot baths (SMD = − 2.42, 95% CrI − 4.67 to − 0.19). SUCRA rankings revealed ear acupressure (93.93%) as the most effective intervention, followed by essential oil therapy (80.97%) and foot baths (78.46%). None of the evaluated non-pharmacological interventions demonstrated statistically significant effects on anxiety reduction.
Conclusion: Multiple non-pharmacological interventions can effectively alleviate postoperative pain after LC. However, none of the evaluated interventions produced statistically significant reductions in postoperative anxiety.
Keywords: LC, network meta-analysis, analgesia, non-pharmacological interventions, pain management
Introduction
Laparoscopic cholecystectomy (LC) is the gold standard surgical treatment for benign gallbladder diseases, being widely utilized due to its minimally invasive nature and rapid recovery profile.1 Although LC significantly reduces postoperative pain compared with conventional open surgery,2 studies indicate that 17–41% of patients continue to experience substantial pain following LC, with 3.4–7.0% developing persistent pain.3 The sources of postoperative pain include somatic pain from trocar-related incisions, visceral pain caused by peritoneal distention, and diaphragmatic irritation triggered by elevated intra-abdominal pressure and carbon dioxide insufflation.4,5 The mechanism of shoulder pain following laparoscopic procedures remains incompletely understood,6 although residual carbon dioxide between the liver and right diaphragm is considered a contributor to diaphragmatic irritation that may lead to referred shoulder pain.4 Additional explanations include phrenic nerve stimulation caused by carbonic acid generated intraperitoneally from retained carbon dioxide,6 and some investigators emphasize that visceral pain associated with tissue trauma during cholecystectomy may represent the major component of postoperative discomfort.7 Without adequate pain management, LC may result in considerable patient discomfort, limited mobility, and impaired respiratory function including restricted deep breathing and coughing. These complications not only compromise early postoperative recovery but may also extend hospitalization duration and increase healthcare costs.3,8 Effective pain management has been demonstrated to promote early mobilization, improve patient comfort and satisfaction, reduce hospital length of stay, and decrease overall healthcare expenditure.9 Therefore, optimal postoperative pain control is both a fundamental component of clinical care and a cornerstone of Enhanced Recovery After Surgery (ERAS) protocols, warranting high priority in perioperative management.
Conventional pharmacological approaches, including non-steroidal anti-inflammatory drugs (NSAIDs) and opioids, are the cornerstone of postoperative pain management. However, opioids, even at therapeutic dosages, frequently produce adverse effects including nausea,10 vomiting,10 somnolence;11 severe cases may result in respiratory depression.12,13 These adverse effects not only increase patient discomfort and treatment complexity—often requiring additional medications to manage side effects—but may also impede recovery. Non-pharmacological interventions provide notable analgesic benefits and offer advantages such as procedural simplicity, affordability, and favorable safety profiles,14,15 with high acceptance and satisfaction among patients and caregivers.16,17 Consequently, investigating effective non-pharmacological analgesic interventions as adjuncts or alternatives to pharmacotherapy holds significant clinical importance in optimizing postoperative pain management strategies for LC. The primary objective of non-pharmacological analgesia is to directly reduce pain intensity while empowering patients with enhanced pain control, thereby improving the overall pain experience.18 Additionally, these interventions are commonly integrated into multimodal analgesic protocols in combination with pharmacological treatments to achieve synergistic effects, optimize overall pain control, and potentially reduce opioid requirements.19,20 Identifying effective and safe non-pharmacological analgesic interventions has therefore become a crucial direction in advancing postoperative pain management.
Established non-pharmacological analgesic modalities include ear acupressure,21 essential oil therapy,22 foot baths,23 acupressure,21 massage therapy,24 and transcutaneous electrical nerve stimulation (TENS).25 These interventions have demonstrated positive effects in alleviating postoperative pain, reducing medication dependence, and enhancing overall surgical recovery outcomes, A systematic review and meta-analysis also reported that non-pharmacological strategies effectively relieve pain in cardiac surgery patients while maintaining procedural simplicity and a low incidence of adverse effects.26 However, current clinical guidelines lack specific recommendations for optimal non-pharmacological approaches to postoperative analgesia following LC. Furthermore, no studies have systematically compared the efficacy and safety of these interventions for LC-related postoperative pain management, creating substantial uncertainty and challenges in clinical practice.
This study utilized a network meta-analysis (NMA) to evaluate the effects of various non-pharmacological interventions on postoperative pain and anxiety following LC. The primary outcome of this study was the pain score. The secondary outcomes included patient anxiety scores. This study aimed to elucidate the clinical efficacy of non-pharmacological approaches in LC pain management. Additionally, we sought to provide evidence-based guidance for developing non-pharmacological analgesic protocols.
Methods
This study was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for NMA (PRISMA-NMA) guidelines,27,28 with complete details provided in Supplementary Table S1. The search strategy and analytical protocol for this systematic review and NMA were prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42025634377.
Literature Search Strategy
A comprehensive literature search was conducted across five major databases (PubMed, Web of Science, Embase, CINAHL, and the Cochrane Library). The search aimed to identify clinical studies investigating non-pharmacological interventions for postoperative pain relief following LC. The search encompassed all available literature from database inception through January 2025. Both Medical Subject Headings (MeSH) terms and free-text words were employed, for example: (((“preemptive” OR “preoperative” OR “perioperative”) AND (“analgesia*” OR “pain” OR “analgesic*”)) OR (“preemptive analgesia” OR “preoperative analgesia” OR “perioperative analgesia”)) AND (“Laparoscopic Cholecystectomy”). Reference lists of relevant systematic reviews were manually searched to identify additional eligible studies. The complete search strategy is detailed in Supplementary Table S2.
Study Selection
Literature management was performed using EndNote software. Two independent reviewers (Ting Lei and Yaping Xie) conducted study screening and data extraction according to predefined inclusion and exclusion criteria. Discrepancies were resolved through discussion with a third investigator (Junjie Wang). Screening was not blinded to authors, institutions, or journals. Inclusion criteria were established based on the PICOS framework: (1) Population (P): adult inpatients aged ≥18 years undergoing elective LC; (2) Intervention (I): non-pharmacological analgesic interventions including ear acupressure, essential oil therapy, massage therapy, acupressure, foot baths, and TENS; (3) Comparator (C): standard care; (4) Outcomes (O): postoperative pain assessed using Visual Analogue Scale (VAS) or Numerical Rating Scale (NRS), and postoperative anxiety evaluated using State-Trait Anxiety Inventory (STAI), or Beck Anxiety Inventory; (5) Study design (S): Only randomized controlled trials (RCTs) were considered for inclusion in this network meta-analysis.
Exclusion criteria comprised: (1) patients with chronic pain history (excluding gallstone-related pain); (2) patients requiring conversion from LC to open cholecystectomy; (3) pregnant or lactating women; (4) duplicate publications; (5) conference abstracts or study protocols; (6) studies with inaccessible full text despite author contact attempts.
Risk of Bias Assessment
Two reviewers (Ting Lei and Yaping Xie) independently evaluated risk of bias using the Cochrane Risk of Bias tool version 2.0 (ROB 2.0). This approach follows recommendations from the Cochrane Handbook version 5.1.0. Assessment domains included bias arising from randomization process, deviations from intended interventions (effect of assignment to intervention), deviations from intended interventions (effect of adhering to intervention), missing outcome data, measurement of outcomes, selective reporting of results, and other sources of bias. Each domain was classified as “high risk,” “some concerns,” or “low risk.” Results were cross-verified, with disagreements resolved through discussion with Junjie Wang.
Data Extraction
Two reviewers (Ting Lei and Junjie Wang) independently extracted key data elements, followed by cross-verification. Discrepancies were resolved through consultation with a third reviewer (Yaping Xie). Extracted information included first author, country, publication year, study design, participant characteristics (age, sample size, gender distribution), detailed intervention descriptions, and outcome measures (pain and anxiety scores). All outcome measures represented the difference between pre- and post-intervention NRS or VAS scores. Pain was assessed using numeric rating scales (NRS) or visual analogue scales (VAS), with higher scores indicating more severe pain. Anxiety was assessed using the State-Trait Anxiety Inventory (STAI), where higher scores reflect more severe anxiety. When differences were not reported in the original studies, they were calculated using formulas specified in the Cochrane Handbook.29 If key summary data were missing, we tried to reconstruct standard deviations from other reported dispersion statistics (such as standard errors, 95% confidence intervals, or interquartile ranges) using standard formulas. If this still could not be reliably reconstructed, we attempted to contact the corresponding authors. Studies with missing dispersion data were retained in the qualitative synthesis but excluded from the quantitative analysis for that specific outcome.
Data Synthesis
A Bayesian NMA was performed using the gemtc package in R software (version 4.4.3). Continuous variables (pain and anxiety scores) were pooled as standardized mean differences (SMDs) with 95% credible intervals (CrIs). Between-study heterogeneity was evaluated using the between-study variance (τ2) and the I2 statistic from random-effects models. I2 values of approximately 25%, 50%, and 75% were interpreted as indicating low, moderate, and high heterogeneity, respectively. Network diagrams were constructed to provide visual representation of available evidence across intervention comparisons. For networks containing closed loops, inconsistency was evaluated using node-splitting methodology, comparing direct and indirect evidence; P-values >0.05 indicated acceptable consistency. Random-effects models were fitted using Markov chain Monte Carlo (MCMC) algorithms with 10,000 burn-in iterations, 50,000 sampling iterations, and thinning interval of 10. Model convergence was confirmed when Gelman-Rubin statistics for all four independent chains were <1.01. To further explore potential sources of heterogeneity and assess the robustness of the findings, we conducted sensitivity analyses excluding trials judged to be of lower methodological quality (ie, with a high overall risk of bias) and performed a predefined subgroup analysis stratified by the presence versus absence of background pharmacological analgesia across trial arms. Results were presented in league tables showing pairwise comparisons between interventions. We used surface under the cumulative ranking curve (SUCRA) values to quantify ranking probabilities, where values range from 0–100% with higher values indicating greater probability of optimal effectiveness.
Results
Literature Selection Process and Results
The systematic search strategy yielded 5,724 potentially relevant records, comprising 891 from PubMed, 1,275 from Embase, 2,790 from the Cochrane Library, 377 from Web of Science, and 391 from CINAHL. After removing 1,781 duplicates using EndNote, 3,943 unique studies remained for screening. After screening titles and abstracts, 3,818 studies were excluded, and 125 proceeded to full-text review. During full-text screening, we excluded 98 studies for the following reasons: ineligible populations (n=8), inappropriate interventions (n=22), incompatible outcomes (n=35), and unsuitable study designs (n=33). Ultimately, 21 RCTs involving 2,695 patients undergoing LC were included for analysis (Figure 1).30–50
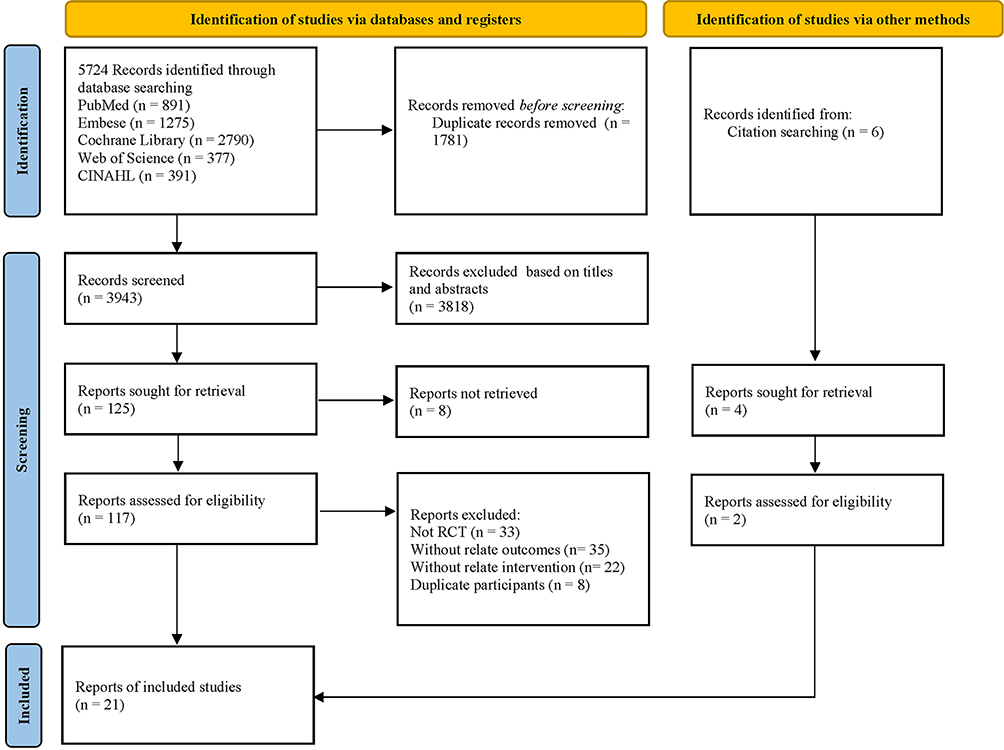 |
Figure 1 Literature selection flowchart. |
Characteristics of Included Studies
All 21 included studies were RCTs evaluating pain outcomes (n = 19) and anxiety outcomes (n = 7). A total of 2,695 patients were randomized to intervention groups (n = 1,719) or control groups (n = 1,047). The included studies exhibited a broad geographical distribution, encompassing multiple countries. Specifically, Turkey contributed the largest number of studies (n=10), followed by Iran (n=6). Single studies were identified from Russia, Brazil, Denmark, South Korea, and China. All control groups received standard care. Participant ages ranged from 40 to 60 years. These studies evaluated 15 distinct non-pharmacological analgesic interventions for postoperative pain management following LC. Among these, six studies (28.57%, n = 621 participants) investigated acupressure, while four studies (19.05%, n = 621 participants) examined massage therapy. The included trials spanned from 2008 to 2024. Pain assessment was the most frequently evaluated outcome (19 studies; n = 2,162 participants), followed by anxiety assessment (7 studies; n = 784 participants). Detailed baseline characteristics of the included studies are presented in Table 1 and Table S3.
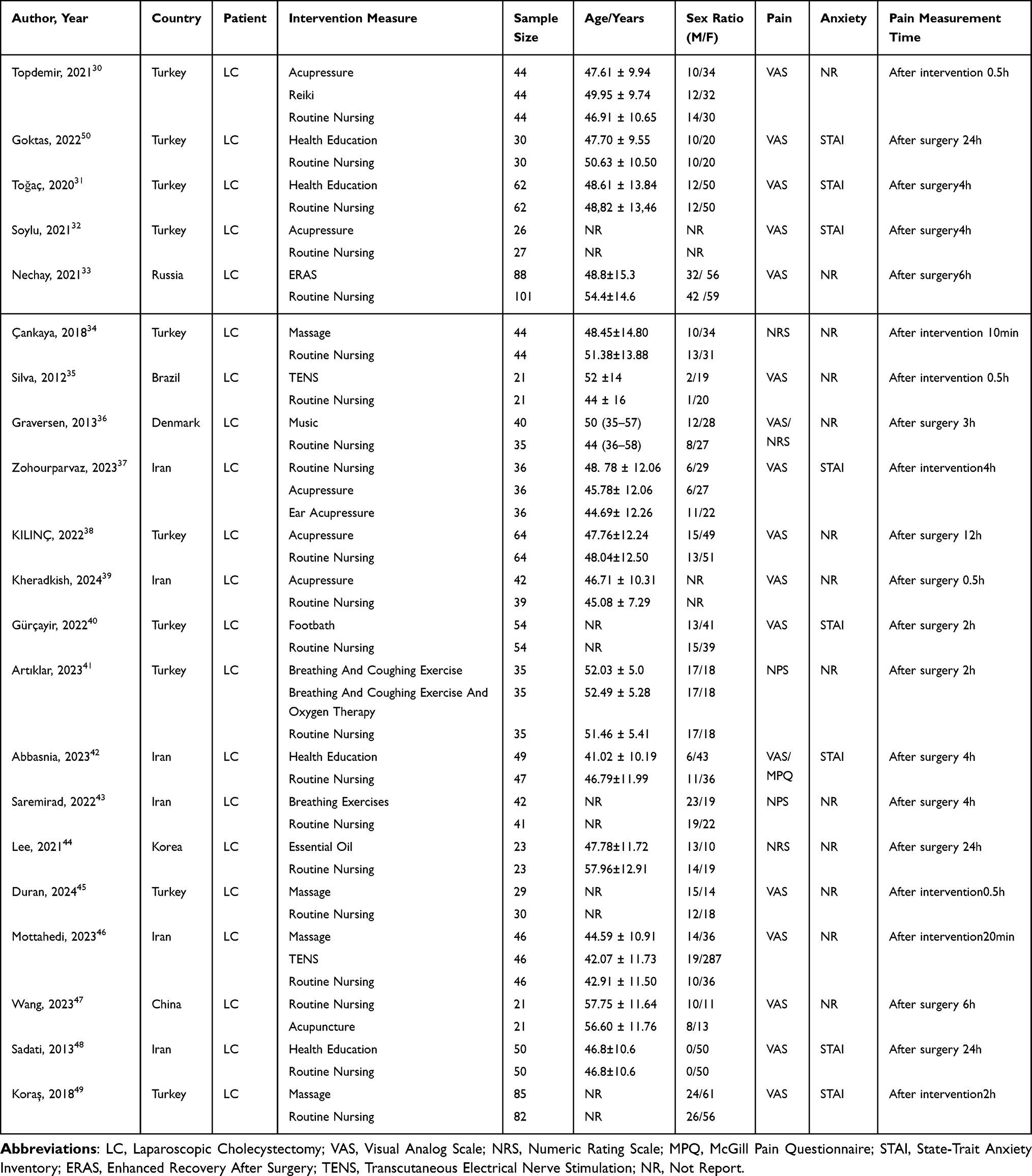 |
Table 1 Characteristics and Quality Assessments of the Included Studies |
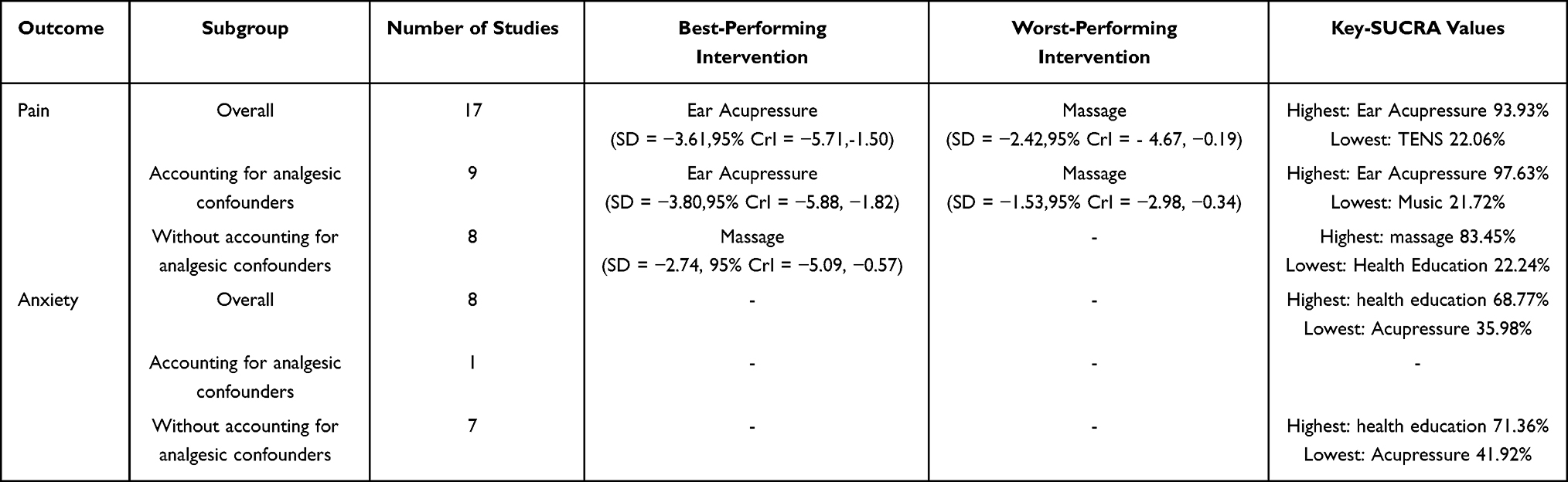 |
Table 2 Subgroup Analysis results |
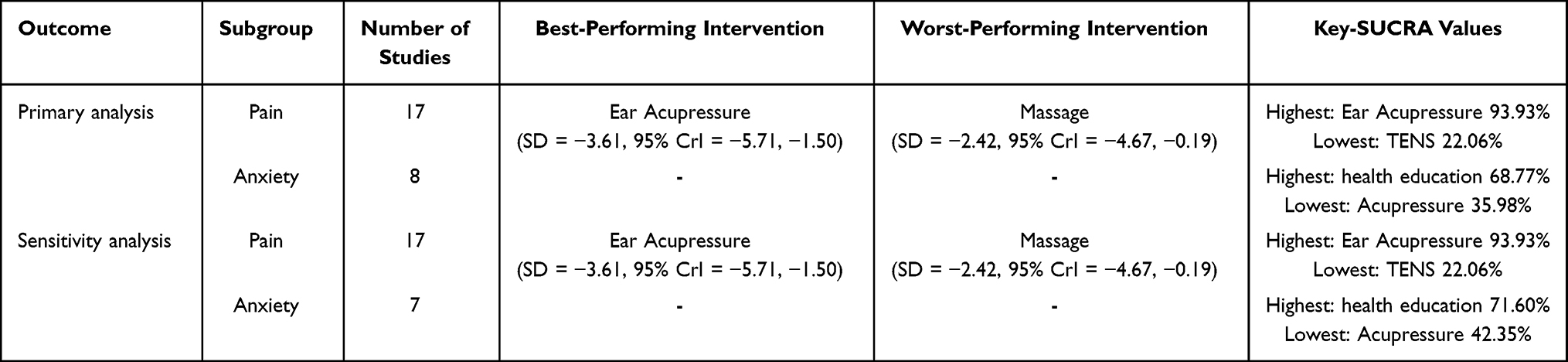 |
Table 3 Results of Sensitivity Analysis |
Risk of Bias Assessment
Study quality was evaluated using the ROB 2.0 tool. The bias assessment revealed that 19.47% of studies (4 trial) raised some concerns, 76.19% (19 trials) demonstrated low risk of bias, and 4.76% (1 trial) exhibited high risk of bias (Supplementary Figure S1).
NMA of Pain Outcomes
Twenty-one trials incorporating 15 interventions were included in the NMA of pain outcomes. The network diagram for pain outcomes is presented in Figure 2A. Given the presence of closed loops, inconsistency testing was conducted, revealing no significant inconsistency (Supplementary Figure S2). The forest plot of relative effects (Figure 2B) demonstrated significant pain improvement with three interventions compared with standard care. Ear acupressure showed the largest effect (SMD = −3.61, 95% CrI −5.71 to −1.50), followed by essential oil therapy (SMD = −2.59, 95% CrI −4.93 to −0.27) and foot baths (SMD = −2.42, 95% CrI −4.67 to −0.19). SUCRA rankings indicated that ear acupressure achieved the highest probability of being the most effective intervention for pain reduction (SUCRA = 93.93%), followed by essential oil therapy (SUCRA = 80.97%) and foot baths (SUCRA = 78.46%). Comprehensive pairwise comparison results are provided in Supplementary Table S4. No statistically significant differences were observed between Reiki and massage therapy, music therapy, foot baths, or breathing exercises.
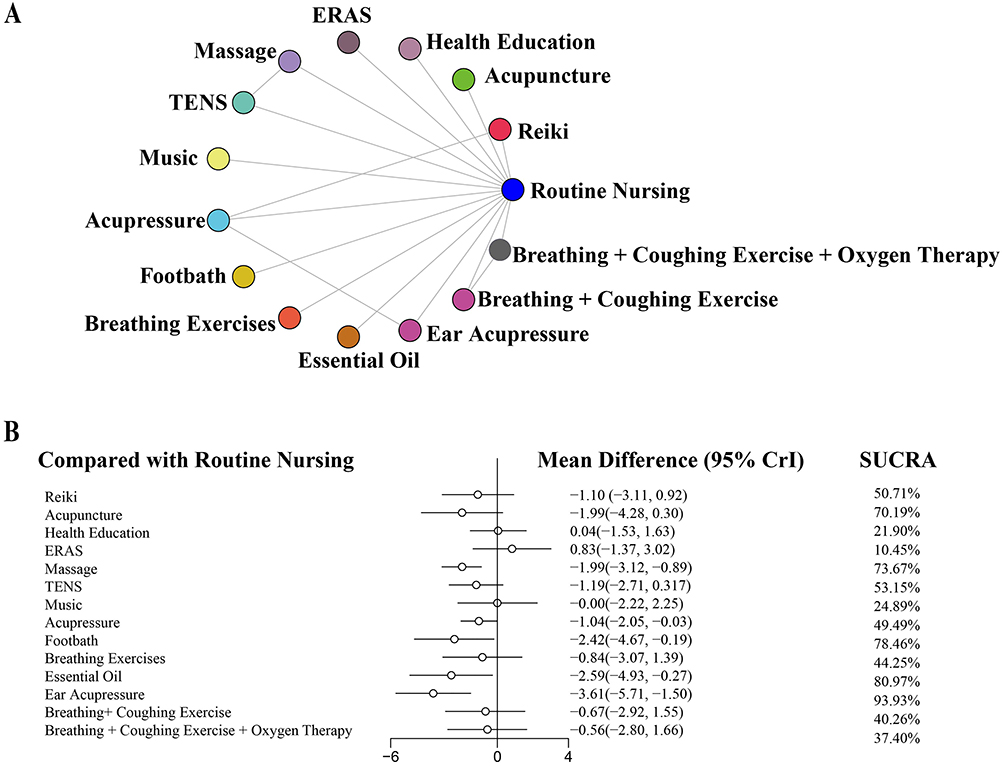 |
Figure 2 (A) Network geometry of non-pharmacological interventions for postoperative pain; (B) Forest plots and SUCRA rankings of non-pharmacological interventions for postoperative pain. Abbreviations: ERAS, Enhanced Recovery After Surgery; TENS, Transcutaneous Electrical Nerve Stimulation; CrI, Credible Interval; SUCRA, Surface Under The Cumulative Ranking Curve. |
NMA of Anxiety Outcomes
Seven trials involving four interventions were included in the NMA of anxiety outcomes. The network diagram for anxiety is shown in Figure 3A, with no closed loops identified. The forest plot of relative effects (Figure 3B) revealed that, compared with standard care, acupressure, health education, foot baths, massage therapy, and meditation did not demonstrate statistically significant improvements in anxiety scores. Detailed pairwise comparison results are presented in Supplementary Table S5.
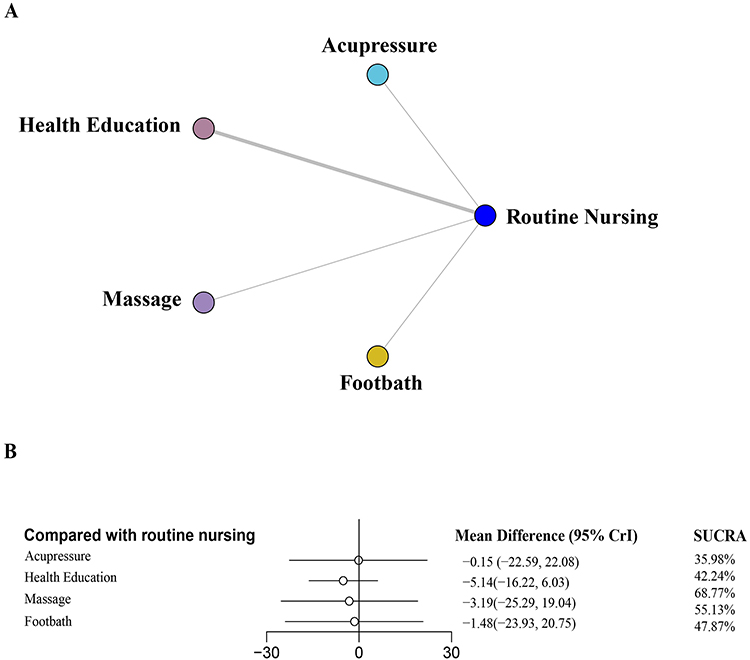 |
Figure 3 (A) Network geometry of non-pharmacological interventions for anxiety; (B) Forest plots and SUCRA rankings of non-pharmacological interventions for anxiety. Abbreviations: CrI, Credible Interval; SUCRAc, Surface Under The Cumulative Ranking Curve. |
Subgroup Analyses
Subgroup analyses were conducted to determine whether background analgesic use influenced pain and anxiety outcomes (Table 2). The main analysis (n = 17) identified ear acupressure as the most effective intervention overall (SUCRA = 93.93%). In the nine studies without interference from background analgesics, ear acupressure maintained its therapeutic superiority, with a SUCRA value of 97.63%. In the eight studies where this confounder was not controlled and ear acupressure was not included, massage ranked as the most effective intervention (SUCRA = 83.45%). For anxiety outcomes, both the main analysis (n = 8) and the subgroup without background analgesic influence (n = 7) suggested that health education may be the most effective approach.
Sensitivity Analyses
Sensitivity analyses supported the robustness of the findings (Table 3). For both pain and anxiety outcomes, the relative ranking of interventions remained stable Minor fluctuations in point estimates were observed for anxiety but did not alter the overall conclusions, confirming the reliability of the network meta-analysis.
Discussion
This systematic review and NMA evaluated 15 non-pharmacological interventions for alleviating postoperative pain following LC, with primary focus on short-term changes in pain intensity. The NMA results demonstrated that ear acupressure, essential oil therapy, and foot baths exhibited the most significant analgesic effects following LC. These findings align with a previous meta-analysis confirming the overall analgesic value of non-pharmacological interventions in surgical populations51 and with evidence from a systematic review showing their efficacy in cardiac surgery patients.26 Furthermore, the pronounced efficacy of auricular therapy is consistent with a specific study demonstrating that auricular acupuncture significantly reduced ibuprofen requirement after ambulatory knee surgery compared to a control procedure.52
Acupressure, originating from traditional Chinese medicine, involves applying gentle finger pressure to specific meridian points on the body to stimulate physiological regulatory processes. Therapeutic effects are achieved through sustained pressure application to the same acupoint.53 This technique is a non-invasive, cost-effective intervention that avoids skin damage, infection, or bleeding while effectively controlling pain symptoms without significant complications.54,55 The ear contains numerous meridian connections that converge at key therapeutic points, and stimulation of these auricular points can activate regulatory mechanisms and provide analgesic effects.56 Zohourparvaz et al37 demonstrated that both acupressure and ear acupressure effectively reduced shoulder pain following LC, with ear acupressure providing superior and more rapid pain relief. Arumugam et al57 conducted a meta-analysis of five RCTs involving 451 participants, showing that ear acupressure significantly reduced labor pain compared with standard care. However, research specifically examining ear acupressure for LC-related postoperative pain remains limited, and these findings require cautious interpretation. Additional high-quality RCTs are needed to validate the efficacy of ear acupressure in managing postoperative pain after LC.58 Consistent with our findings, ear acupressure has been shown to improve heart rate variability, thereby reducing sympathetic nervous system activity, decreasing adrenaline and cortisol secretion, and enhancing relaxation responses, which collectively reduce pain, stress, and anxiety levels.59 The analgesic mechanisms of acupressure are believed to involve two primary pathways: first, blocking pain signal transmission through neural pathways to the spinal cord and brain; second, stimulating endorphin release, which contributes to pain reduction.60
Essential oil therapy uses plant-derived essential oils administered through various routes, including inhalation, topical application, massage, or foot baths. These approaches can alleviate stress, reduce pain, and improve sleep quality. Lee et al44 investigated essential oil therapy effects on postoperative pain in LC patients, revealing significant differences among intervention, placebo, and control groups. The intervention group demonstrated markedly lower pain scores and required fewer additional pain control measures beyond standard analgesics within 48 hours postoperatively. Bagheri et al61 reported concordant findings, with intervention group patients inhaling four drops of 2% lavender essential oil in oxygen for 20 minutes, while controls received oxygen alone. Postoperative pain was assessed immediately upon surgical ward transfer and at 2, 6, and 24 hours post-surgery using visual analogue scales. Pain severity was significantly reduced in the intervention group at all four measurement points compared with controls. However, the aromatic properties of essential oils preclude patient blinding, potentially introducing placebo effects that warrant cautious result interpretation. To establish the analgesic efficacy of inhaled essential oil therapy, future research should investigate various essential oil types, different concentration ratios, and multiple outcome measures to determine optimal pain management protocols.
Foot baths represent an effective, cost-efficient, and easily implementable non-pharmacological intervention. Nursing staff can administer this treatment to alleviate postoperative pain, reduce anxiety and stress, promote muscle relaxation, and improve sleep quality.62 Consistent with our findings, existing literature demonstrates that patients undergoing abdominal surgery experience statistically significant pain reduction following foot bathing compared with control groups.23,63,64 In a study by Soonyoung and Myoungjin,65 patients in the experimental group who received warm foot baths following hand replantation demonstrated marked decreases in pain intensity. Similarly, Gurccayir et al40 reported that foot baths effectively reduced both pain and anxiety levels in patients following LC. The analgesic mechanisms of warm foot baths are believed to involve two primary pathways: first, reduction of muscle spasms and metabolic rate coupled with enhanced blood circulation; second, interruption of pain transmission pathways, thereby attenuating pain perception.66–68
The subgroup analyses revealed an important pattern in evidence quality. Ear acupressure emerged as the most effective intervention based entirely on high-quality studies that controlled for background analgesic use, strengthening confidence in its observed efficacy. In contrast, massage was ranked most effective only in studies lacking adequate control of confounding, suggesting possible overestimation of its benefits. This contrast highlights the superior methodological rigor underpinning the evidence supporting ear acupressure. Clinically, these findings indicate that non-pharmacological analgesic recommendations should prioritize interventions supported by higher-quality evidence, positioning ear acupressure as a preferred strategy after LC.
This study provides two major innovations. First, it establishes the most comprehensive evidence-integration framework to date by incorporating all available RCTs into a unified NMA, allowing simultaneous comparison of fifteen non-pharmacological interventions and providing a global efficacy ranking. Second, the use of SUCRA values enhances the interpretability of findings by estimating the probability that each intervention represents the optimal choice, offering more clinically actionable insights than traditional meta-analyses.
This study has several notable strengths. First, this is the inaugural application of NMA methodology to comprehensively compare the effectiveness of 15 non-pharmacological interventions for postoperative pain management following LC, providing novel evidence-based insights into this important clinical challenge. Second, we incorporated a comprehensive range of commonly utilized non-pharmacological interventions, facilitating thorough comparative analysis to guide postoperative analgesic strategy selection for LC. Third, we conducted systematic and extensive literature searches across five major databases, spanning from database inception through January 2025, to maximize identification of all relevant research. Furthermore, a notable strength of our analysis is the broad geographical representation of the included studies, which encompassed research from a wide range of countries and regions, including Turkey, Iran, Russia, Brazil, Denmark, South Korea, and China. This diversity enhances the external validity and generalizability of our findings. It suggests that the efficacy of the evaluated non-pharmacological interventions for post-operative pain may be robust across different healthcare settings and patient populations. Moreover, the inclusion of studies from various cultural contexts hints at the potential cross-cultural acceptability of these modalities, which is a particularly valuable attribute for managing a universal experience like pain.
Several limitations warrant acknowledgment. First, due to limited study availability, we did not differentiate between specific acupoint combinations in acupressure and massage interventions, precluding determination of relative efficacy and safety among different acupoint protocols. Second, inclusion was restricted to English-language publications, potentially introducing language bias through exclusion of non-English studies. Third, several included studies featured small sample sizes and brief follow-up periods, potentially limiting assessment of long-term clinical outcomes. Fourth, most included studies were single-center investigations, which may introduce bias and limit generalizability of findings. Fifth, pain was assessed at varying timepoints across trials, creating methodological heterogeneity and limiting precise comparison of analgesic onset and duration. Differences in the intervention sets included in various subgroups further constrained direct comparison under identical conditions, although these differences accurately reflect the stratified evidence levels that currently exist among non-pharmacological modalities.
Conclusions
This network meta-analysis confirmed that auricular therapy, essential oil therapy, and foot baths are effective non-pharmacological options for relieving postoperative pain after laparoscopic cholecystectomy (LC). Auricular therapy demonstrated the strongest overall analgesic effect and may be considered a preferred non-pharmacological component of multimodal analgesia after LC.
Clinical Significance and Practical Value
These findings provide clear evidence-based foundation to guide clinical practice. Incorporating auricular therapy and other non-pharmacological modalities into multimodal analgesia strategies following LC offers patients a safe, effective, and well-accepted analgesic option. This approach not only effectively alleviates patient pain and enhances patient safety, but also reduces opioid consumption, thereby minimizing the incidence of opioid-related adverse effects such as nausea, vomiting, and constipation. These benefits directly contribute to accelerated patient recovery and improved overall quality of care.
Future Research Perspectives
Although this study confirms the overall efficacy of these interventions, key treatment parameters including optimal acupoint combinations, stimulation intensity, frequency, and treatment duration remain unstandardized. Establishing these parameters is critical for advancing the intervention from “effective” to “optimal.” Future research could employ factorial or optimization trial designs to systematically analyze and establish best practice protocols. Large-scale, high-quality multicenter randomized controlled trials are urgently needed to further validate the impact of these therapies on long-term functional recovery, patient satisfaction, and economic benefits, thereby providing high-level evidence to inform clinical guideline development. We also recommend standardizing pain assessment timepoints in future studies to facilitate objective comparisons of intervention onset time and duration of effect across different modalities.
In summary, this study establishes the superior position of auricular therapy within non-pharmacological pain management after LC, providing essential theoretical foundation and practical direction for developing safer, more efficient, and patient-centered perioperative analgesic strategies.
Data Sharing Statement
All data generated or analysed during this study are included in this published article and its Supplementary Information Files.
Acknowledgments
The authors acknowledge individuals and institutions that contributed to this study but did not meet authorship criteria.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Ting Lei contributed to study conception and design, literature search, bias risk assessment, data extraction and analysis, and manuscript drafting. Yanqiong Peng contributed to study conception and design and provided critical manuscript revision. Ting Lei and Yaping Xie contributed to literature search and bias risk assessment. Ting Lei and Junjie Wang contributed to data extraction. Yuanjun Liu contributed to study conception and design. All authors contributed to data interpretation and provided critical manuscript review for publication.
Funding
This study was supported by the Sichuan Nursing Association Research Project Program (Grant No. H24073).
Disclosure
The authors have no conflict of interest to declare.
References
1. Mansour NO, Boraii S, Elnaem MH. et al. Evaluation of preoperative duloxetine use for postoperative analgesia following laparoscopic cholecystectomy: a randomized controlled trial. Front Pharmacol. 2022;13:944392. doi:10.3389/fphar.2022.944392
2. Cao L, Yang T, Hou Y, Yong S, Zhou N. Efficacy and Safety of Different Preemptive Analgesia Measures in Pain Management after Laparoscopic Cholecystectomy: a Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Pain Ther. 2024;13(6):1471–1497. doi:10.1007/s40122-024-00647-w
3. Jain S, Nazir N, Mustafi SM. Preemptive low-dose intravenous ketamine in the management of acute and chronic postoperative pain following laparoscopic cholecystectomy: a prospective randomized control study. Med Gas Res. 2022;12(4):141–145. doi:10.4103/2045-9912.337995
4. Gurusamy KS, Vaughan J, Toon CD, et al. Pharmacological interventions for prevention or treatment of postoperative pain in people undergoing laparoscopic cholecystectomy. Cochrane Database Syst Rev. 2014;2014(3):CD008261. doi:10.1002/14651858.CD008261
5. D M, Udayakumar GS, Sivakumar SK, Ms R, Narayanan V. Comparison of Ultrasound-Guided Erector Spinae Plane Block and Oblique Subcostal Transversus Abdominis Plane Block for Postoperative Analgesia After Laparoscopic Cholecystectomies: a Prospective Randomized Controlled Trial. Cureus. 2025;17(9):e93364. doi:10.7759/cureus.93364
6. Kietpeerakool C, Rattanakanokchai S, Yantapant A, et al. Pulmonary Recruitment Maneuver for Reducing Shoulder Pain after Laparoscopic Gynecologic Surgery: a Network Meta-Analysis of Randomized Controlled Trials. Minim Invasive Surg. 2020;2020:7154612. doi:10.1155/2020/7154612
7. Ekstein P, Szold A, Sagie B, Werbin N, Klausner JM, Weinbroum AA. Laparoscopic surgery may be associated with severe pain and high analgesia requirements in the immediate postoperative period. Ann Surg. 2006;243(1):41–46. doi:10.1097/01.sla.0000193806.81428.6f
8. Abuelzein MLA, Baghdadi MA, Abbdelhady WA, et al. A prospective randomized controlled study on the role of restoring liver diaphragm surface tension and pain control at port sites in optimizing pain management following laparoscopic cholecystectomy. Ann Gastroenterol Surg. 2022;7(1):131–137. doi:10.1002/ags3.12602
9. Tsai CS, Tung HH, Fang CJ, Chen CT. Effectiveness of non-pharmacological interventions for pain reduction following chest tube removal: a systematic review and network meta-analysis. Intensive Crit Care Nurs. 2025;87:103909. doi:10.1016/j.iccn.2024.103909
10. Artawan IM, Ratu K, Adang GPT, Riwu M. Comparison of the Effectiveness of Paracetamol and Ibuprofen Combination With Paracetamol and Ketorolac for Postoperative Analgesia in Cesarean Section: a Single Blind Randomized Clinical Trial. Asian J Anesthesiol. 2024;62(4):187–195. doi:10.6859/aja.202412_62(4).0002
11. Hasegawa T, Okuyama T, Suzuki N, et al. Efficacy and safety of combining low-dose methadone with ongoing opioid treatment for uncontrolled cancer pain: an open-label single-arm study. Oncologist. 2025;30(9):215. doi:10.1093/oncolo/oyaf215
12. Zhang X, Qiao S, Pan H. Insidious opioid-induced respiratory depression following abdominal steel pipe perforation injury: a case report. Medicine. 2025;104(43):e45435. doi:10.1097/md.0000000000045435
13. Pogatzki-Zahn EM, Segelcke D, Schug SA. Postoperative pain-from mechanisms to treatment. Pain Rep. 2017;2(2):e588. doi:10.1097/pr9.0000000000000588
14. Boateng EA, Kumi LO, Diji AK. Nurses and midwives’ experiences of using non-pharmacological interventions for labour pain management: a qualitative study in Ghana. BMC Pregnancy Childbirth. 2019;19(1):168. doi:10.1186/s12884-019-2311-x
15. Zhang Z, Lin Y, Wang Z, Qian D. The effect of non-pharmacological intervention on the pain relief in patients with liver neoplasm after transcatheter arterial chemoembolization: a network meta-analysis. Journal of Interventional Radiology. 2025;34(05):518–524. doi:10.3969/j.issn.1008-794X.2025.05.014
16. Fan L, Zeng J, Ran L, et al. Virtual reality in managing dental pain and anxiety: a comprehensive review. Front Med Lausanne. 2023;10:1285142. doi:10.3389/fmed.2023.1285142
17. Soysal GE, Demir Erbas S. Factors influencing pain, anxiety, and comfort in patients undergoing coronary angiography: a prospective observational study. Saudi Med J. 2025;46(6):679–687. doi:10.15537/smj.2025.46.6.20240158
18. Mwanza E, Gwisai RD, Munemo C. Knowledge on Nonpharmacological Methods of Pain Management among Nurses at Bindura Hospital, Zimbabwe. Pain Res Treat. 2019;2019:2703579. doi:10.1155/2019/2703579
19. Friesner SA, Curry DM, Moddeman GR. Comparison of two pain-management strategies during chest tube removal: relaxation exercise with opioids and opioids alone. Heart Lung. 2006;35(4):269–276. doi:10.1016/j.hrtlng.2005.10.005
20. Hsu KC, Chen LF, Hsiep PH. Effect of music intervention on burn patients’ pain and anxiety during dressing changes. Burns. 2016;42(8):1789–1796. doi:10.1016/j.burns.2016.05.006
21. Ghanbari F, Rejeh N, Bahrami T, Yahyazadeh H, Saatchi K. Comparative Effectiveness of Ear and Body Acupressure for Postoperative Pain in Elderly Women Following Knee Arthroplasty: a Randomized Trial. J Integr Complement Med. 2025;31(11):987–996. doi:10.1177/27683605251377400
22. Nouira M, Souayeh N, Kanzari SA, et al. Aromatherapy Using Lavender Oil Effectiveness on Pain and Anxiety After C-Section: A Randomized Controlled Trial. J Epidemiol Glob Health. J Epidemiol Glob Health. 2024;14(4):1536–1544. doi:10.1007/s44197-024-00305-6
23. Uslu Y, Akbayrak H, Kuytak Ortahisar B, Barak TH. The effect of lavender foot baths on postoperative pain and sleep quality in comparison with foot baths with warm water only-A prospective randomized controlled study. Explore (NY). 2024;20(3):385–391. doi:10.1016/j.explore.2023.10.003
24. J Brilhadori, CD Marinho-Junior, IM Correia, et al. Effects of Massage Therapy on Anxiety, Depression, Stress, Pain, Quality of Life, and Immune Aspects in People Living With HIV: a Systematic Review and Meta-Analysis. J Assoc Nurses AIDS Care. 2025;36(6):e29–e30. doi:10.1097/jnc.0000000000000597
25. Khubzan W, Alharbi L, Alharbi L, et al. The effectiveness of transcutaneous electrical nerve stimulation (TENS) for postoperative pain after laparoscopic cholecystectomy: a systematic review and meta-analysis. Saudi J Anaesth. 2025;19(4):607–613. doi:10.4103/sja.sja_450_25
26. Yıldız T, Oyuktaş M, Avcu Ç. The effect of non-pharmacological methods on pain in patients undergoing open heart surgery: a systematic review and meta-analysis. Turk Gogus Kalp Damar Cerrahisi Derg. 2024;32(3):291–306. doi:10.5606/tgkdc.dergisi.2024.25603
27. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
28. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
29. Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019; 10(10):ED000142. doi:10.1002/14651858
30. Topdemir EA, Saritas S. The effect of Acupressure and Reiki application on Patient’s pain and comfort level after laparoscopic cholecystectomy: a randomized controlled trial. Complement Ther Clin Pract. 2021;43:101385. doi:10.1016/j.ctcp.2021.101385
31. Toğaç HK, Yılmaz E. Effects of preoperative individualized audiovisual education on anxiety and comfort in patients undergoing laparoscopic cholecystectomy: randomised controlled study. Patient Educ Couns. 2021;104(3):603–610. doi:10.1016/j.pec.2020.08.026
32. Soylu D, Tekinsoy Kartın P. The effect on gastrointestinal system functions, pain and anxiety of acupressure applied following laparoscopic cholecystectomy operation: a randomised, placebo-controlled study. Complement Ther Clin Pract. 2021;43:101304. doi:10.1016/j.ctcp.2021.101304
33. Nechay T, Titkova S, Tyagunov A, Anurov M, Sazhin A. Modified enhanced recovery after surgery protocol in patients with acute cholecystitis: efficacy, safety and feasibility. Multicenter randomized control study. Updates Surg. 2021;73(4):1407–1417. doi:10.1007/s13304-021-01031-5
34. Çankaya A, Saritaş S. Effect of Classic Foot Massage on Vital Signs, Pain, and Nausea/Vomiting Symptoms After Laparoscopic Cholecystectomy. Surg Laparosc Endosc Percutan Tech. 2018;28(6):359–365. doi:10.1097/sle.0000000000000586
35. Silva MB, de Melo PR, de Oliveira NM, Crema E, Fernandes LF. Analgesic effect of transcutaneous electrical nerve stimulation after laparoscopic cholecystectomy. Am J Phys Med Rehabil. 2012;91(8):652–657. doi:10.1097/PHM.0b013e318246638f
36. Graversen M, Sommer T. Perioperative music may reduce pain and fatigue in patients undergoing laparoscopic cholecystectomy. Acta Anaesthesiol Scand. 2013;57(8):1010–1016. doi:10.1111/aas.12100
37. Zohourparvaz MS, Taghanaki HB, Moghadam MG, et al. Comparison of the effects of body acupressure and ear acupressure on shoulder pain in Iranian patients undergoing laparoscopic cholecystectomy: a randomized controlled trial. Trad Integr Med. 2023; 8(4):370–378. doi:10.18502/tim.v8i4.14485
38. Kilinç T, Karaman Özlü Z. Effect of acupressure application on patients’ nausea, vomiting, pain, and sleep quality after laparoscopic cholecystectomy: a randomized placebo-controlled study. Explore (NY). 2024;20(1):44–52. doi:10.1016/j.explore.2022.11.004
39. Kheradkish F, Valiani M, Amini Rarani S, Hashemi M. The effect of acupressure on pain levels and physiologic indicator in patients undergoing laparoscopic cholecystectomy: a double-blind, randomized clinical trial. Complement Ther Clin Pract. 2024;57:101868. doi:10.1016/j.ctcp.2024.101868
40. Gürçayir D, Karabulut N. Effects of Footbath on Pain, Anxiety, Sleep, and Comfort Levels in Patients With Postlaparoscopic Cholecystectomy: a Randomized Controlled Study. Surg Laparosc Endosc Percutan Tech. 2024;34(5):452–458. doi:10.1097/sle.0000000000001306
41. Artıklar T, Erden S. The Effect of Breathing and Coughing Exercises and Oxygen Therapy on Shoulder Pain and Analgesic Consumption After Laparoscopic Cholecystectomy: a Randomized Controlled Study. J Perianesth Nurs. 2024;39(4):540–546. doi:10.1016/j.jopan.2023.10.008
42. Abbasnia F, Aghebati N, Miri HH, Etezadpour M. Effects of Patient Education and Distraction Approaches Using Virtual Reality on Pre-operative Anxiety and Post-operative Pain in Patients Undergoing Laparoscopic Cholecystectomy. Pain Manag Nurs. 2023;24(3):280–288. doi:10.1016/j.pmn.2022.12.006
43. Saremirad M, Yazdimoghaddam H, Dalili A, Rastaghi S. The Impact of Incentive Spirometry on Shoulder Tip Pain in Laparoscopic Cholecystectomy: a Randomized Clinical Trial. Surg Laparosc Endosc Percutan Tech. 2021;32(1):14–20. doi:10.1097/sle.0000000000001012
44. Lee J, Hur MH. The Effects of Aroma Essential Oil Inhalation on Stress, Pain, and Sleep Quality in Laparoscopic Cholecystectomy Patients: a Randomized Controlled Trial. Asian Nurs Res. 2022;16(1):1–8. doi:10.1016/j.anr.2021.11.002
45. Duran MK, Öztürk Ş. The effect of shoulder massage on shoulder pain and sleep quality in patients after laparoscopic cholecystectomy: a randomized controlled trial. BMC Nurs. 2024;23(1):618. doi:10.1186/s12912-024-02264-6
46. Mottahedi M, Shamsi M, Babani SF, Goli S, Rizevandi P. Comparing the effect of transcutaneous electrical nerve stimulation and massage therapy on post laparoscopic shoulder pain: a randomized clinical trial. BMC Musculoskelet Disord. 2023;24(1):764. doi:10.1186/s12891-023-06905-w
47. Wang F, Peng P, Zheng Y, Cheng S, Chen Y. Effect of Acupuncture on Postoperative Pain in Patients after Laparoscopic Cholecystectomy: a Randomized Clinical Trial. Evid Based Complement Alternat Med. 2023;2023:3697223. doi:10.1155/2023/3697223
48. Sadati L, Pazouki A, Mehdizadeh A, Shoar S, Tamannaie Z, Chaichian S. Effect of preoperative nursing visit on preoperative anxiety and postoperative complications in candidates for laparoscopic cholecystectomy: a randomized clinical trial. Scand J Caring Sci. 2013;27(4):994–998. doi:10.1111/scs.12022
49. Koraş K, Karabulut N. The Effect of Foot Massage on Postoperative Pain and Anxiety Levels in Laparoscopic Cholecystectomy Surgery: a Randomized Controlled Experimental Study. J Perianesth Nurs. 2019;34(3):551–558. doi:10.1016/j.jopan.2018.07.006
50. Goktas S, Tosun Y, Gezginci E, Onuk E, Keğin M. Preoperative educational package in cholecystectomy patients on anxiety and return to normal activity—A randomized controlled clinical trial. Indian J Surg. 2022;84(Suppl 1):139–146. doi:10.1007/s12262-021-02983-z
51. Ding L, Hua H, Zhu H, et al. Effects of virtual reality on relieving postoperative pain in surgical patients: a systematic review and meta-analysis. Int J Surg. 2020;82:87–94. doi:10.1016/j.ijsu.2020.08.033
52. Usichenko TI, Kuchling S, Witstruck T, et al. Auricular acupuncture for pain relief after ambulatory knee surgery: a randomized trial. Cmaj. 2007;176(2):179–183. doi:10.1503/cmaj.060875
53. Abbasoğlu A, Cabıoğlu MT, Tuğcu AU, et al. Acupressure at BL60 and K3 Points Before Heel Lancing in Preterm Infants. Explore (NY) Sep-Oct. 2015;11(5):363–366. doi:10.1016/j.explore.2015.07.005
54. Barker R, Kober A, Hoerauf K, et al. Out-of-hospital auricular acupressure in elder patients with hip fracture: a randomized double-blinded trial. Acad Emerg Med. 2016;13(1):19–23. doi:10.1197/j.aem.2005.07.014
55. Monson E, Arney D, Benham B, et al. Beyond Pills: acupressure Impact on Self-Rated Pain and Anxiety Scores. J Altern Complement Med. 2019;25(5):517–521. doi:10.1089/acm.2018.0422
56. Hou PW, Hsu HC, Lin YW, Tang NY, Cheng CY, Hsieh CL. The History, Mechanism, and Clinical Application of Auricular Therapy in Traditional Chinese Medicine. Evid Based Complement Alternat Med. 2015;2015:495684. doi:10.1155/2015/495684
57. Arumugam V, Balakrishnan A, Venugopal V, et al. Auriculotherapy for Labour Pain Management: a Systematic Review and Meta-Analysis. J Acupunct Meridian Stud. 2024;17(5):158–164. doi:10.51507/j.jams.2024.17.5.158
58. Hu N, Soh KL, Japar S, Li T. Ear-Marking Relief: a Meta-Analysis on the Efficacy of Auricular Acupressure in Alleviating Anxiety Disorders. Complement Med Res. 2024;31(3):266–277. doi:10.1159/000537734
59. Trinh DT, Nguyen NC, Tran AH, Bui MP, Vuong NL. Enhancing Vagal Tone, Modulating Heart Rate Variability with Auricular Acupressure at Point Zero: a Randomized Controlled Trial. Med Acupunct. 2024;36(4):203–214. doi:10.1089/acu.2024.0001
60. Luo D, Wang X, He J. A comparison between acute pressure block of the sciatic nerve and acupressure: methodology, analgesia, and mechanism involved. J Pain Res. 2013;6:589–593. doi:10.2147/jpr.S47693
61. Bagheri H, Salmani T, Nourian J, et al. The Effects of Inhalation Aromatherapy Using Lavender Essential Oil on Postoperative Pain of Inguinal Hernia: a Randomized Controlled Trial. J Perianesth Nurs. 2020;35(6):642–648. doi:10.1016/j.jopan.2020.03.003
62. Uslu Y, Akbayrak H, Kuytak OB, et al. The effect of lavender foot baths on postoperative pain and sleep quality in comparison with foot baths with warm water only-A prospective randomized controlled study. Explore (NY). 2024;20(3):385–391. doi:10.1016/j.explore.2023.10.003
63. Ünver S, Çolakoğlu Ü, Akıncı AT, et al. Effects of Footbath on Postoperative Pain and Sleep Quality in Patients With Lumbar Degenerative Disc Disease: A Randomized Controlled Study. J Neurosci Nurs. 2023;55(4):125–130. doi:10.1097/JNN.0000000000000709
64. Cal E, Cakiroglu B, Kurt AN, Hartiningsih SS, Dane S. The Potential Beneficial Effects Of Hand And Foot Bathing On Vital Signs In Women With Caesarean Section. Clin Invest Med. 2016;39(6):27508.
65. Yoon S, Kwon M. The effect of foot bath therapy on post-operation pain, stress, HRV in hand replantation patients. Korean J Occupational Health Nursing. 2011;2011:105–112.
66. Liao WC, Landis CA, Lentz MJ, Chiu MJ. Effect of foot bathing on distal-proximal skin temperature gradient in elders. Int J Nurs Stud. 2005;42(7):717–722. doi:10.1016/j.ijnurstu.2004.11.011
67. Saeki Y, Nagai N, Hishinuma M. Effects of footbathing on autonomic nerve and immune function. Complement Ther Clin Pract. 2007;13(3):158–165. doi:10.1016/j.ctcp.2006.12.006
68. Chandler A, Preece J, Lister S. Using heat therapy for pain management. Nurs Stand. 2002;17(9):40–42. doi:10.7748/ns2002.11.17.9.40.c3297
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Peripheral Nerve Blocks After Arthroscopic Shoulder Surgery: A Systematic Review and Network Meta-Analysis
Gao Y, Huang J, Liu Z, Hu Z, Yan W, Ren D
Journal of Pain Research 2026, 19:589046
Published Date: 21 April 2026
Effectiveness of Non-Pharmacological Interventions on Postoperative Pain in Gastric Cancer: A Systematic Review and NMA Protocol
Lei S, Tian H, Qi H
Journal of Pain Research 2026, 19:604748
Published Date: 20 May 2026