Back to Journals » Journal of Pain Research » Volume 19
Effectiveness of Jaw Exercises Applied in Addition to Cervical Stabilization Exercises in Individuals with Chronic Neck Pain: A Randomized Controlled Trial
Authors Canli M ![]() , Özüdoğru A
, Özüdoğru A ![]() , Alkan H, Cigdem-Karacay B
, Alkan H, Cigdem-Karacay B
Received 5 December 2025
Accepted for publication 1 February 2026
Published 18 February 2026 Volume 2026:19 584088
DOI https://doi.org/10.2147/JPR.S584088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Mehmet Canli,1 Anıl Özüdoğru,1 Halil Alkan,2 Basak Cigdem-Karacay3
1Department of Physiotherapy, Kırşehir Ahi Evran University, School of Physical Therapy and Rehabilitation, Kırşehir, Turkey; 2Department of Physiotherapy Rehabilitation, Muş Alparslan University, Faculty of Health Sciences, Muş, Turkey; 3Department of Physical Medicine and Rehabilitation Faculty of Medicine, Kırşehir Ahi Evran University, Kırşehir, Turkey
Correspondence: Mehmet Canli, Department of Physiotherapy, Kırşehir Ahi Evran University, School of Physical Therapy and Rehabilitation, Kırşehir, Turkey, Tel +90 541 550 13 46, Email [email protected]
Purpose: Chronic neck pain (CNP), defined as pain localized to the cervical spine region persisting for more than three months, represents a major global health problem with a steadily increasing prevalence worldwide. This randomized controlled trial aimed to investigate the effectiveness of adding jaw exercises to cervical stabilization exercises on pain, sensorimotor function, and functional outcomes in individuals with CNP.
Patients and Methods: A total of 62 individuals aged 18– 65 years with cervical spine pain lasting longer than three months and a pain intensity of ≥ 3 cm on the Visual Analogue Scale (VAS) were included. Participants were randomly allocated to the Rocabado group (RG, n=31) or the control group (CG, n=31). The CG performed cervical stabilization exercises (CSE), while the RG performed Rocabado exercises in addition to CSE for 6 weeks. Pain intensity (VAS), pressure pain threshold and tolerance, balance, cervical range of motion, muscle endurance, Neck Disability Index (NDI), and cervical proprioception were assessed at baseline and post-treatment. Sample size was calculated based on the NDI as the primary outcome.
Results: Both groups demonstrated significant improvements in pain intensity, cervical range of motion, muscle endurance, disability, balance, and proprioception after 6 weeks (p< 0.05). Compared with the control group, the Rocabado group showed significantly greater improvements in pressure pain threshold and tolerance (η2 = 0.29– 0.41), cervical propriosepsiyon (η2 = 0.14– 0.19), and static and dynamic balance parameters (η2 = 0.27– 0.46), indicating moderate to large group-by-time effects (p< 0.05).
Conclusion: Adding Rocabado exercises to cervical stabilization exercises provides superior improvements in sensorimotor function and pain-related outcomes in individuals with chronic neck pain. These findings suggest that integrating jaw-focused exercises into cervical rehabilitation programs may offer clinically meaningful benefits.
Trial Registration: This clinical trial was registered at http://clinicaltrials.gov (Number: NCT05887349, registration date: 05/23/2023).
Keywords: pain, neck pain, jaw, exercise
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Das has been published for this article.
Introduction
Chronic neck pain (CNP) is known as neck pain (NP) that lasts longer than 3 months.1 CNP negatively affects the quality of life, physical and mental functions of individuals. It is reported that approximately 67% of individuals worldwide will experience NP at least once in their lifetime, and approximately 20% of these individuals will develop CNP.2 Recent Global Burden of Disease data indicate that chronic neck pain affects over 200 million people worldwide and represents a substantial and growing contributor to global disability.3 Individuals with CNP have pain, migraine, muscle function imbalances, and abnormal breathing patterns.4
There are studies reporting that individuals with NP may have temporomandibular joint (TMJ) disorder due to the anatomical and biomechanical relationship between the TMJ and the structures forming the cervical region, or vice versa, TMJ disorder (TMJD) may lead to painful sensations in the neck.5 In addition, some studies have reported that patients with TMJD often have symptoms of NP.6 The reason for the relationship between TMJD and neck symptoms is that jaw movements consist of simultaneous movements of the mandible, head and neck.7 Another relationship between the TMJ and the cervical region is the trigeminocervical nucleus caudalis, which is the common afferent between the two regions.8 Previous biomechanical studies suggest that mandibular position and jaw movements can influence cervical proprioception and postural control through shared neuromuscular and sensory pathways. Given the coordinated movement of the jaw, head, and cervical spine, exercises targeting the temporomandibular region, such as Rocabado exercises, may enhance sensorimotor control and balance.9
There are various conservative treatment approaches for CNP, including education, manual therapy, stabilization exercises, and electrotherapy.10 Available evidence supports the recommendation of a multidisciplinary treatment approach for optimizing outcomes and facilitating recovery among patients with musculoskeletal disorders, particularly those involving the TMJ and neck, which often exhibit multifactorial etiologies.11
Rocabado exercises (RE) constitute a tailored exercise regimen designed for TMJD, aimed at alleviating pain by facilitating the movement of synovial fluid across the joint surfaces. This process enhances circulation, fosters joint nourishment, and eliminates metabolites from the joint.12 As a consequence of employing this exercise regimen, a reduction in the severity of TMJ pain is attained.13
Several studies have evaluated the effectiveness of stabilization exercises performed alone versus those supplemented with mobilization techniques in cases of CNP.14 However, to our knowledge, there are no studies in the literature investigating the effectiveness of RE applied in addition to stabilization exercises. Given the close biomechanical, anatomical, and neurophysiological interaction between the jaw and neck, RE may be effective in the treatment of CNP. In this context, our aim was to examine the effectiveness of RE in individuals with CNP.
Materials and Methods
Study Design
This study is a randomized controlled trial. This study was conducted on patients diagnosed with CNP who were referred to Kırşehir Ahi Evran University School of Physical Therapy and Rehabilitation for treatment. The study was conducted between July and October 2023. Written and verbal informed consent was obtained from all participants before the study. The study was conducted in accordance with the principles of the Declaration of Helsinki. Permission for the study was approved by the Muş Alparslan University local ethics committee (Date: 18/05/2023, protocol number: 2023–5/34).
Participants
Participants were eligible for inclusion if they were between 18 and 65 years of age, had experienced non-specific CNP for at least three months, and reported moderate to severe pain intensity, defined as a Visual Analogue Scale (VAS) score of 3 cm or higher. Only individuals with chronic neck pain without TMJD and without clinical signs of neuropathic or radicular pain were included in the study, in order to ensure a homogeneous sample representing predominantly mechanical neck pain. Exclusion criteria included a diagnosis of TMJD, the presence of neuropathic or referred pain symptoms (such as radicular pain, paresthesia, numbness, or neurological deficits), a history of cervical spine surgery, osteoporosis, or any additional upper extremity pathology that could influence pain perception, neuromuscular control, or functional assessment outcomes. There was no participant drop-out during the study period, and this is thought to be related to the exercise programme administered under the supervision of a physiotherapist and regular follow-up.
Interventions
Cervical Stabilization Exercises
Level 1 (Week 1)
In Level 1, individuals were taught correct posture, maintenance of correct posture, and the craniocervical flexion (CCF) movement, which is the basis of CSE. The exercises were started after the patient understood the CCF movement and performed it correctly. A pressurized biofeedback device (Chattanooga Stabilizer Group Inc., Hixson, TN) was used to teach the patient the movement. Individuals were asked to remain in the CCF position for 10 seconds. They were asked to perform 10 repetitions after a rest period of 3–5 seconds. Then, the CCF movement was performed in prone, standing, and crawling positions in order to gain dynamic stabilization (Figure 1).14,15
 |
Figure 1 Level 1 cervical stabilization exercises. |
Level 2 (Week 2)
In Level 2, upper and lower extremity movements were incorporated into the CCF movement to enhance motor control. Limb movements were added bilaterally and then contralaterally on different surfaces and positions. The difficulty of the exercises was progressively heightened based on the individuals’ correct execution and tolerance. Then, cervical region-resistant isometric exercises were performed with the help of elastic bands. Isometric exercises were performed for 10–12 repetitions (Figure 2).14,15
 |
Figure 2 Level 2 cervical stabilization exercises. |
Level 3 (Week 3-6)
In this level of exercises, unlike the previous levels, individuals were asked to control the ball. Participants performed seated exercises on the exercise ball, involving limb movements, pressing the ball against the wall with their head, and coordinating both ball and limb movements using elastic bands, as outlined in the CCF protocol. For each exercise, participants performed a 10-second muscle contraction followed by 5 seconds of relaxation, completing 10 repetitions (Figure 3).14,15
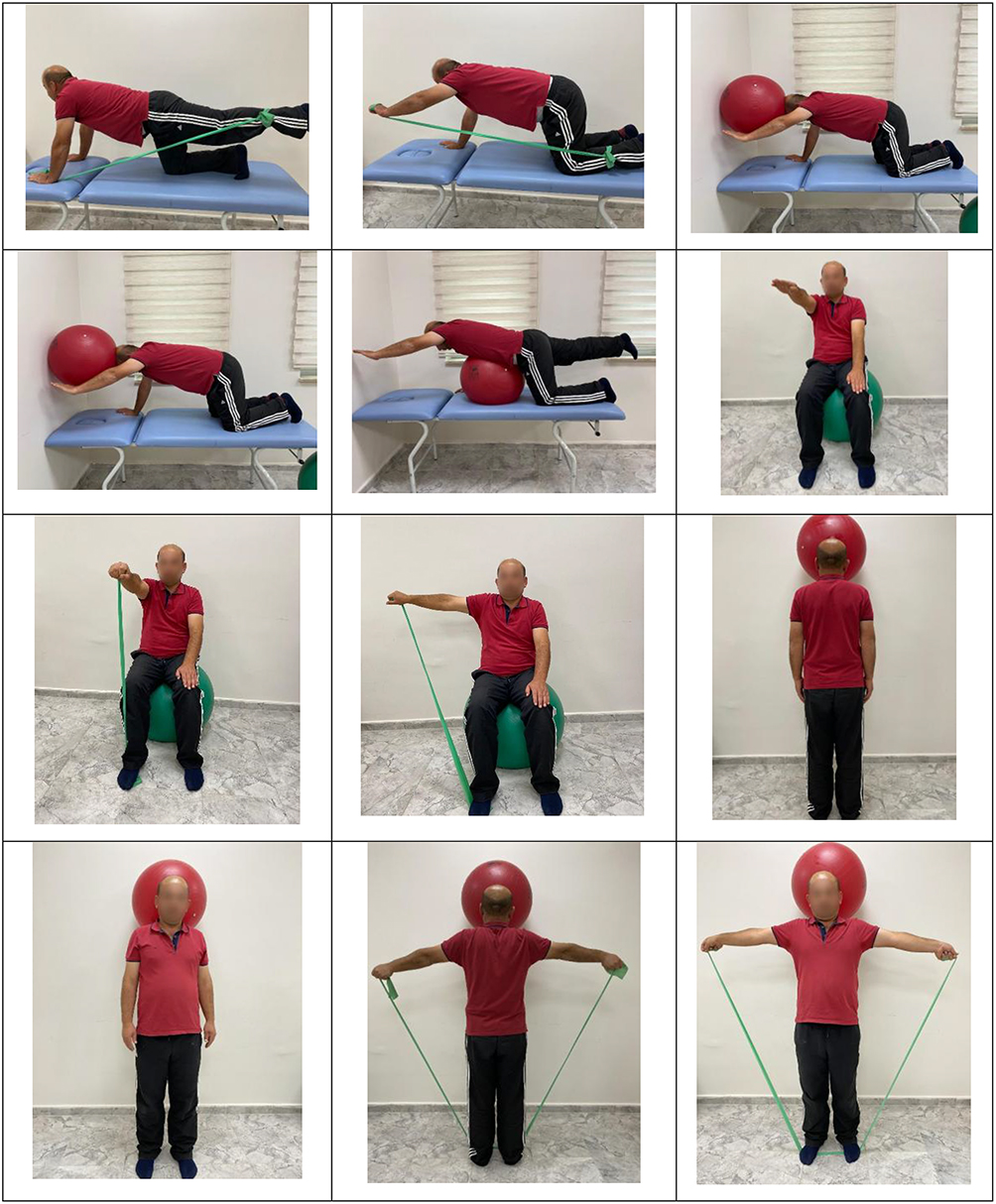 |
Figure 3 Level 3 cervical stabilization exercises. |
Rocabado Exercises
Individuals in RG performed RE in addition to CSE. RE were given as 6 repetitions and 6 sets after each CSE session. RE consist of six movements (Figure 4).12
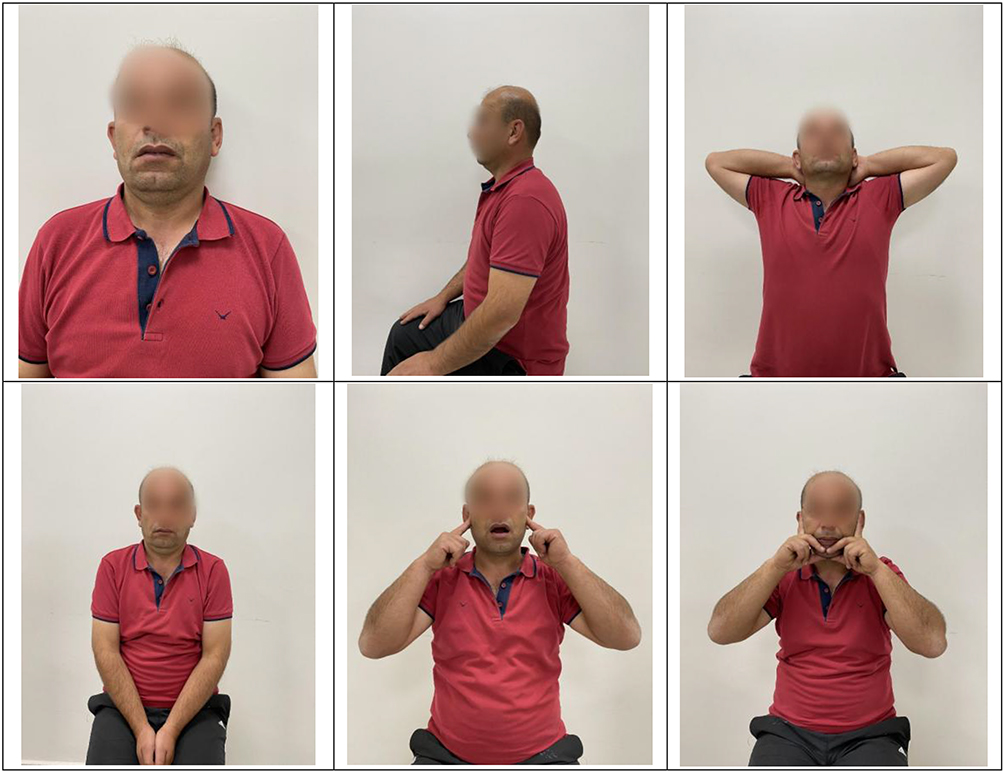 |
Figure 4 Rocabado exercises. |
Outcome Measurements
Demographic information including age, height, weight, and gender was documented. Clinic assessments were performed before and immediately after six weeks of treatment.
Primary Outcome
Disability
The assessment of neck disability resulting from NP utilized the Neck Disability Index (NDI), a validated and reliable tool in Turkish. Developed to gauge the influence of NP on daily activities, the NDI comprises 10 sections, with each section scored from 0 to 5 points. The total NDI score ranges from 0 to 50, with higher scores indicating greater neck-related disability.16
Secondary Outcomes
Pain Intensity
The VAS assesses the intensity of pain felt by patients in centimeters (cm) during different activities and time periods (rest, activity, and night). The patient is requested to indicate the intensity of their pain by marking a 10-cm line. Each 1 cm is scored from 0 to 10. “0” indicates no pain, and “10” indicates unbearable pain.17
Pressure Pain Threshold and Tolerance
Pressure pain threshold (PPT1) and pressure pain tolerance (PPT2) of the participants were measured using a digital algometer device (JTech Medical Industries, ZEVEX Company). All measurements were performed with participants in an upright sitting position, with the arms relaxed alongside the body. The midpoint of the upper portion of the trapezius muscle, located between the seventh cervical vertebra and the acromion, was used as the standardized measurement site. Measurements were obtained bilaterally (right and left sides) in all participants. Three consecutive assessments were performed for each side, and the mean value was recorded in kg/cm.18
Balance
The participants’ static and dynamic balance were evaluated utilizing the Biodex Balance System (Biodex, Inc., Shirley, New York). This equipment quantifies the anterior-posterior stability index (A-P), medial-lateral stability index (M-L), and overall stability index, covering variation in both planes. Individuals were asked to hold the black dot appearing on the screen of the device within the small circle in the center for 20 seconds and 3 repetitions. The mobility level of the device platform was set to 12 for dynamic balance assessment. Participants were asked to hold the black dot in the center of the small circle for 20 to 3 repetitions, this time on the moving platform. A-P, M-L, and overall stability values were recorded separately for both static and dynamic balance.19
Range of Motion
The cervical ROM of the participants was assessed in all directions (flexion, extension, right-left rotation, and right-left lateral flexion) using a clinical goniometer (Baseline Evaluation Tools, USA) in an upright sitting position on a stool fixed to the floor and recorded in degrees.20
Muscle Endurance
Participants’ cervical flexor endurance was assessed in the supine position, with arms along the sides of the torso and the legs maintained in a hook-lying posture. Participants were instructed to gently draw their chin towards their chest, and the duration they maintained this position was measured in seconds. Endurance of the extensor muscles in the cervical region was evaluated with the participant in a prone position. The participant’s head was permitted to hang off the edge of the bed, with a 2 kg weight bag affixed to it. The duration the participant sustained this position was recorded in seconds.21
Cervical Proprioception
The cervical region proprioception sense of the participants was evaluated with CJPET. CJPET evaluates the ability of the participant to find the neutral position again after maximal flexion, extension, and rotation movements of the head in sagittal and transverse planes. For the test, the participant was seated in a chair with eyes closed and head in neutral position. The laser lamp was positioned atop the participant’s head, and the midpoint of the target was identified as the neutral or starting position. The participants were then asked to perform the movement at maximum range of motion 10 times for each direction and to find the neutral position again. The five nested circles in the trigonometrically graded target were scored from the inside to the outside as 1 degree, 2 degrees, 3 degrees, 4.5 degrees, and 6 degrees, respectively. This score indicates the angle of deviation from the center. The first four of the 10 repetitions were averaged, and the last six were recorded in degrees.22
Sample Size
The required sample size was calculated using G*Power software (version 3.1.8.2, University of Düsseldorf, Düsseldorf, Germany). The primary outcome measure was the Neck Disability Index (NDI). Based on the between-group differences in NDI reported in a previous randomized controlled study investigating the effects of temporomandibular joint interventions in individuals with chronic neck pain an effect size of 0.22 was estimated.23 Assuming a two-group comparison, an alpha level of 0.05, and a statistical power of 80%, a minimum total sample size of 54 participants was required. To account for an anticipated dropout rate of 20%, the final target sample size was increased to 66 participants (33 per group).
Randomization and Blinding
Participants were randomly allocated to either the Rocabado group (RG) or the control group (CG) using a stratified randomization procedure based on age and gender to ensure balanced distribution of these variables between groups. Following stratification, participants were randomly assigned to one of the two groups (RG, n = 31; CG, n = 31). All baseline and post-intervention assessments were conducted by the same investigator (MC), who was blinded to group allocation. However, due to the nature of the interventions, participant blinding was not feasible.
Statistical Analysis
IBM SPSS version 23 (ver. 22.0; IBM Corp., NY, USA) package program was used for statistical analysis of the data. Descriptive analyses were performed using mean and standard deviation for normally distributed variables. The normality of continuous variables was assessed using the Shapiro–Wilk and Kolmogorov–Smirnov tests, supported by visual inspection of histograms and Q–Q plots. All variables showed normal distribution. For nominal variables, numerical values and percentages were employed. An independent sample t-test was utilized to compare the pre-treatment values between groups, while the chi-square test (χ2) was employed to compare categorical variables such as gender. Paired sample t-test was used to compare the pre- and post-treatment changes of two groups within groups. A two-way mixed design repeated measures analysis of variance (ANOVA) was used to evaluate the change of the groups over time and group-time interactions. Effect size (η2) was interpreted as 0.10: small effect, 0.25: medium effect, and 0.40: large effect.24
Results
The eligibility of 66 individuals diagnosed with CNP was evaluated. Four people who were not eligible for the study were excluded from the study. A total of 62 people were randomly divided into two groups and the study was completed. The flow chart of the study is shown in Figure 5.
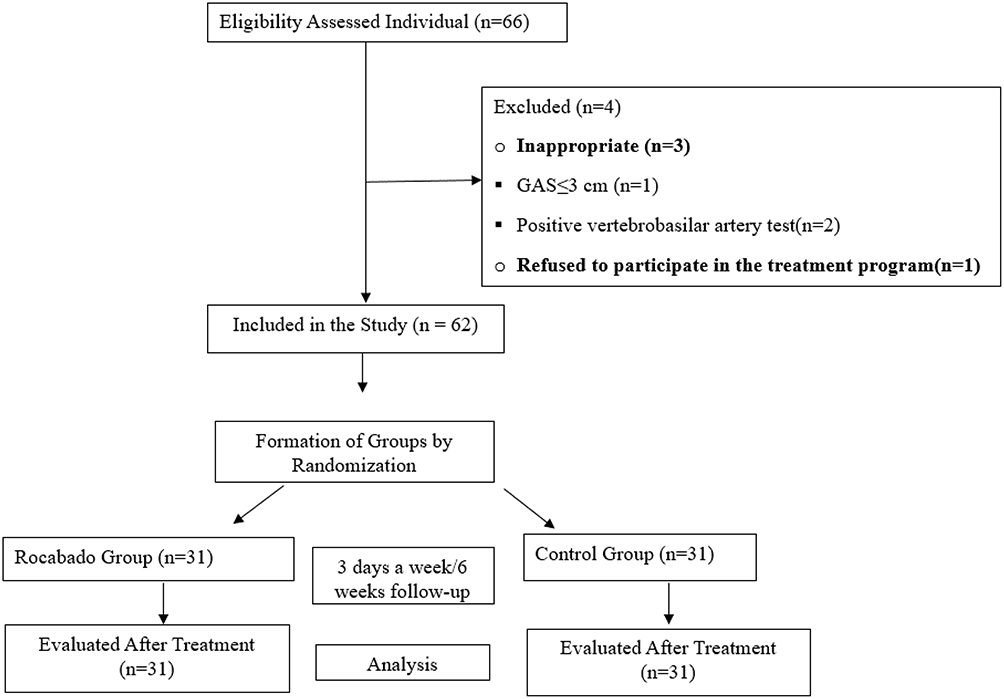 |
Figure 5 Flowchart diagram. |
Table 1 shows the baseline demographic and clinical characteristics between the study groups with no significant differences.
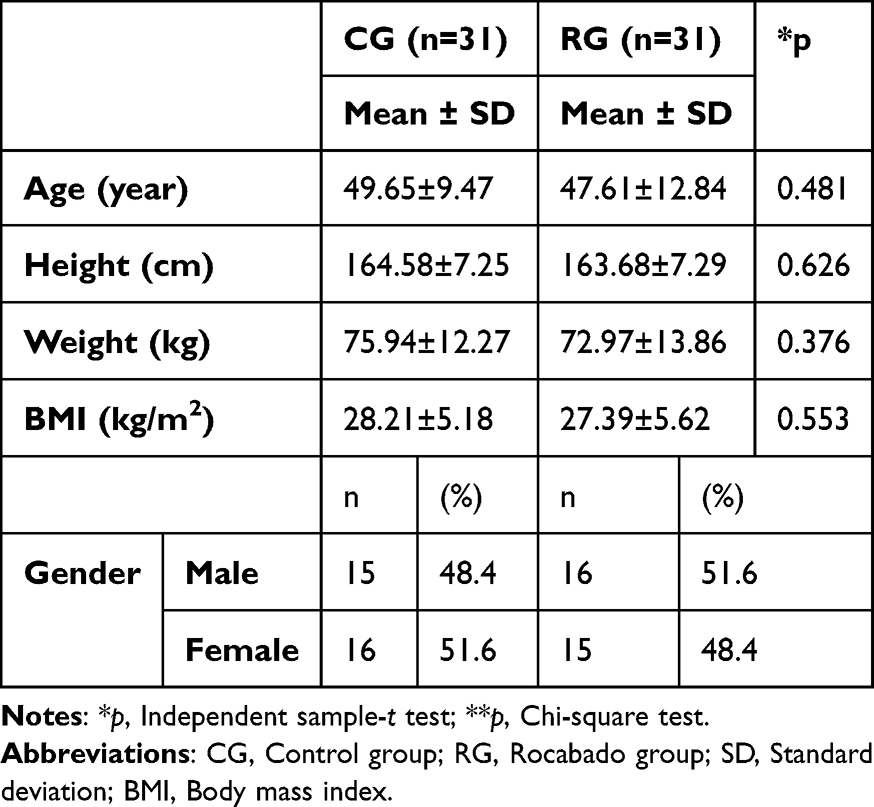 |
Table 1 Demographic Characteristics of the Groups |
The comparison of VAS, PPT1, PPT2, ROM, proprioception, and balance values between the RG and CG groups before and after treatment is presented in Table 2. Upon analyzing the changes over time within each group, significant improvements were observed in all scores of VAS, PPT1, PPT2, ROM, proprioception, and balance values in both groups (p<0.05). When comparing the changes over time (Group*Time) between the groups post-treatment, a significant difference favored the RG group in pressure PPT1, PPT2, ROM (flexion), proprioception, and balance values (p<0.05). However, no significant difference was found between the groups in ROM and VAS values (p>0.05).
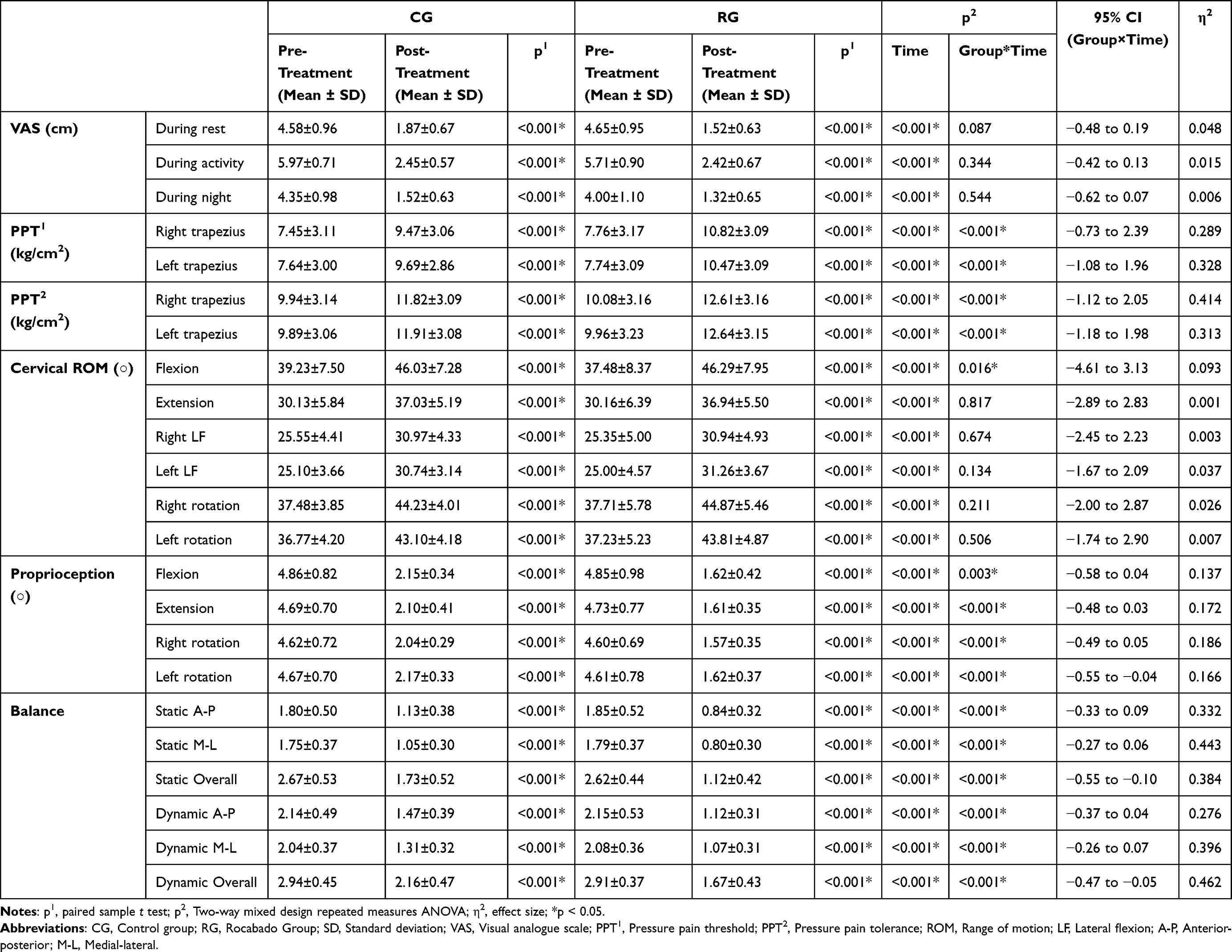 |
Table 2 Comparison of CG and RG Groups Pre-Treatment and Post-Treatment |
The comparison of muscle endurance and NDI values between the RG and CG before and after treatment is displayed in Table 3. Upon analyzing the changes over time within each group, significant improvements were observed in muscle endurance and NDI values in both groups (p<0.05). However, when comparing the changes over time (Group*Time) between the groups post-treatment, no significant difference was found (p>0.05).
 |
Table 3 Comparison of Muscle Strength, Muscle Endurance, NDI, and NYPA Values of the CG and RG Groups Pre-Treatment and Post-Treatment |
Discussion
When the results of the study were analyzed, it was observed that pain intensity, PPT1, PPT2, ROM, disability status, muscle endurance, proprioception, and balance levels of individuals with CNP improved significantly both in RG and CG. It was also concluded that RE applied in addition to CSE were more effective than CSE alone on flexion ROM, proprioception, balance, PPT1, and PPT2 in individuals with CNP.
Ghaderi et al25 reported that CSE was effective in reducing pain in individuals with nonspecific NP. Çelenay et al26 concluded that CSE were effective in reducing pain in individuals with mechanical NP. Ylinen et al27 reported that CSE was effective in reducing pain in individuals with non-specific CNP. In this study, we observed significant improvements in pain intensity, PPT1, and PPT2 in both RG and CG.
Ghodrati et al23 reported that the addition of TMJ intervention to the physiotherapy program was more effective in reducing pain in individuals with CNP. Walczyńska-Dragon et al28 reported that occlusal splinting may improve NP in individuals with TMJD. In this study PPT1 and PPT2 increased significantly in both groups. However, the improvement in PPT1 and PPT2 showed a significant difference in favor of RG. This result may be due to inhibition of the pathways that carry the pain sensation of the TMJ and neck. In addition to statistical significance, the magnitude of pain reduction observed in the RG appears to be clinically meaningful, as the between-group differences approached or exceeded commonly reported minimal clinically important differences for pain intensity measured by VAS in chronic neck pain. This finding supports the clinical relevance of adding jaw-focused exercises to cervical rehabilitation programs.
Previous research by Düşünceli et al29 indicated that combining CSE with physiotherapy contributed to increased ROM in individuals with CNP, while Yesil et al30 also confirmed the positive effect of CSE on ROM. In line with these findings, our study observed parallel improvements in cervical ROM in both RG and CG, which may be explained by the alleviation of pain.
Akıncı et al31 reported that jaw exercises increased cervical ROM in individuals with CNP. Ghodrati et al23 found that supplementing standard treatment with TMJ intervention led to increased cervical ROM in patients with non-specific chronic neck pain. When this study results were analyzed, cervical ROM increased significantly in both groups. However, except for the flexion ROM value, the groups were not superior to each other in other ROM values.
Lee and Shin32 reported that neuromuscular control exercises improved cervical proprioception in individuals with NP. Jull et al33 concluded that CCF training was effective for impaired proprioception. Hidalgo-Peréz et al34 reported that CSE improved proprioception in healthy individuals. According to this study findings, CSE is effective in improving cervical proprioception in both groups. The results suggest that the increased proprioception following CSE may be due to the improvement of the quality of cervical afferent input.
Changes in jaw posture are likely to affect proprioception in the cervical region.35 While a review of the literature did not reveal any studies investigating the impact of jaw exercises on cervical proprioception in individuals with NP, there are studies examining the effect of jaw clenching on proprioception and postural balance. In these studies, it is stated that jaw clenching improves postural balance and proprioception.36 When the results of this study were analyzed, significant improvement was observed in cervical proprioception in both groups. In addition, RE applied in addition to CSE were found to be superior in improving cervical proprioception. This result may be due to the fact that RE improve jaw posture and stimulate the postural control mechanism of the jaw sensory motor system.
Bernal-Utrera et al37 concluded that CSE improved body balance in individuals with non-specific CNP. Song et al38 stated that CSE improved balance in individuals with anterior head tilt. Yong et al39 stated that CSE reduces lateral oscillations and thus positively affects balance. When this study were analyzed, significant improvements were observed in both dynamic and static balance in both groups in which CSE was applied. We can attribute this result to the fact that CSE improves impaired activation in deep cervical muscles and increases functionality.
Amaral et al40 reported that TMJ mobilization improves postural control in patients with TMJD. Zafar et al41 stated that the jaw sensory-motor system directly or indirectly affects postural control. Hosoda et al42 suggested that occlusion contributes to maintaining postural balance and improving stability when an unexpected sway occurs in the standing position. We concluded that RE applied in conjunction with CSE were more efficacy in reducing both dynamic and static balance parameters. We attribute this outcome to the alteration of the jaw joint position by RE, which may influence the postural mechanisms of the joint, known for its abundance of proprioceptors.
Ghaderi et al25 reported that CSE increased flexor muscle endurance in individuals with non-specific NP. In another study, Cho et al43 reported that CSE was effective in increasing deep and superficial cervical muscle strength in individuals with CNP. In this study, we found a significant increase in muscle endurance in both groups in accordance with the literature. This result may be due to the effect of CCF movement, which is the basis of CSE, on increasing deep cervical muscle strength.
Häggman-Henrikson et al44 stated that applying neck exercises to patients with TMJD could increase the muscle strength and endurance of the jaw joint. Moon et al45 stated that co-contraction of masticatory muscles during CSE helps to increase the thickness of the longus colli muscle. In another study, Böthun et al46 stated that resistant jaw opening increased jaw-neck motor function. They stated that this was due to the fact that the resistance given to the mandible caused an increase in functional demand in the jaw-neck system. When this study results were analyzed, the groups were not superior to each other in terms of muscle endurance.
Javdaneh et al47 reported that CSE decreased the level of disability in individuals with CNP. Kaka et al48 reported that CSE resulted in improvement in disability level in individuals with non-specific NP. When the results of this study were examined, we found a significant improvement in the level of disability in both RG and CG. This may be due to a decrease in the level of pain during activity.
Nicolakis et al49 reported that exercise and manual therapy reduced the level of disability in patients with TMJD. Crăciun et al50 reported that medication and physiotherapy were effective in reducing the level of disability in patients with TMJD. In another study, Wänman et al51 found that jaw exercises were effective on the level of neck disability in patients with TMJD. When the results of this study were analyzed, significant improvement was observed in the neck disability level in both groups, but the groups were not superior to each other.
This study has several notable strengths. First, its randomized controlled design enhances the internal validity of the findings. Second, the inclusion of comprehensive and objective outcome measures, such as pressure pain threshold and tolerance, balance, and cervical proprioception, alongside patient-reported outcomes, provides a multidimensional evaluation of treatment effects. Additionally, the absence of participant attrition and the high adherence rate, achieved through supervised interventions, strengthen the reliability of the results. Finally, to our knowledge, this is one of the first randomized controlled trials to investigate the additive effects of jaw exercises to CSE in individuals with CNP, contributing novel evidence to the existing literature. The present study has several limitations. First, the follow-up period was relatively short, and long-term effects of the interventions were not evaluated. In addition, participants were not blinded to group allocation, which may have introduced potential placebo or performance bias. Furthermore, the lack of similar studies in the literature limits direct comparisons of our findings. Future studies with longer follow-up periods, blinded designs, and larger sample sizes are recommended to confirm and expand upon these results.
Conclusion
In the treatment of CNP, CSE can improve pain intensity, ROM, endurance, and disability level. Nevertheless, it can be asserted that the addition of RE to CSE proves more efficacious in enhancing pain intensity, PPT1, PPT2, proprioception, and balance when contrasted with CSE alone among individuals with CNP.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to privacy or ethical restrictions. But are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
This randomized controlled study was approved by the local ethics committee of Muş Alparslan University (approval date: 18 May 2023; protocol number: 2023-5/34). The study was conducted in accordance with the principles of the Declaration of Helsinki, and all participants voluntarily took part in the study without any form of coercion or undue influence. Written informed consent was obtained from all participants prior to participation. In addition, written informed consent was obtained from the participant for the use and publication of the figures presented in this manuscript.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Beltran-Alacreu H, López-de-uralde-villanueva I, Calvo-Lobo C, Fernández-Carnero J, La Touche R. Clinical features of patients with chronic non-specific neck pain per disability level: a novel observational study. Revista da Assoc Méd Brasileira. 2018;64:700–15. doi:10.1590/1806-9282.64.08.700
2. Viljanen M, Malmivaara A, Uitti J, Rinne M, Palmroos P, Laippala P. Effectiveness of dynamic muscle training, relaxation training, or ordinary activity for chronic neck pain: randomised controlled trial. BMJ. 2003;327(7413):475. doi:10.1136/bmj.327.7413.475
3. Wu A-M, Cross M, Elliott JM, et al. Global, regional, and national burden of neck pain, 1990–2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2024;6(3):e142–e155. doi:10.1016/S2665-9913(23)00321-1
4. Blanpied PR, Gross AR, Elliott JM, et al. Neck pain: revision 2017: clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the American Physical Therapy Association. J Orthopaedic Sports Phys Ther. 2017;47(7):A1–A83.
5. Bartsch T, Goadsby P. Increased responses in trigeminocervical nociceptive neurons to cervical input after stimulation of the dura mater. Brain. 2003;126(8):1801–1813.
6. de Wijer A, de Leeuw JRJ, Steenks MH, Bosman F. Temporomandibular and cervical spine disorders: self-reported signs and symptoms. Spine. 1996;21(14):1638–1646.
7. Alcantara J, Plaugher G, Klemp DD, Salem C. Chiropractic care of a patient with temporomandibular disorder and atlas subluxation. J Manipul Physiolog Therapeut. 2002;25(1):63–70.
8. Marfurt CF, Rajchert DM. Trigeminal primary afferent projections to “non‐trigeminal” areas of the rat central nervous system. J Comp Neurol. 1991;303(3):489–511.
9. Yin CS, Lee YJ, Lee YJ. Neurological influences of the temporomandibular joint. J Bodywork Movement Ther. 2007;11(4):285–294.
10. Miller J, Gross A, D’Sylva J, et al. Manual therapy and exercise for neck pain: a systematic review. Manual Ther. 2010;15(4):334–354. doi:10.1016/j.math.2010.02.007
11. Brendbekken R, Harris A, Ursin H, Eriksen HR, Tangen T. Multidisciplinary intervention in patients with musculoskeletal pain: a randomized clinical trial. Int J Behav Med. 2016;23:1–11. doi:10.1007/s12529-015-9486-y
12. Mulet M, Decker KL, Look JO, Lenton PA, Schiffman EL. A randomized clinical trial assessing the efficacy of adding 6 x 6 exercises to self-care for the treatment of masticatory myofascial pain. J Orofacial Pain. 2007;21(4):318–328.
13. Borg-Stein J, Iaccarino MA. Myofascial pain syndrome treatments. Phys Med Rehab Clin. 2014;25(2):357–374. doi:10.1016/j.pmr.2014.01.012
14. Kocaman H, Yıldız NT, Canlı M, Alkan H. Comparison of the effects of mulligan mobilization technique combined with cervical stabilization exercises with the effects of cervical stabilization exercises alone in chronic neck pain: randomized controlled study. Karya J Health Sci. 2023;4(3):227–234. doi:10.52831/kjhs.1374767
15. Celenay ST, Kaya DO, Akbayrak T. Cervical and scapulothoracic stabilization exercises with and without connective tissue massage for chronic mechanical neck pain: a prospective, randomised controlled trial. Manual Ther. 2016;21:144–150. doi:10.1016/j.math.2015.07.003
16. Kesiktas N, Ozcan E, Vernon H. Clinimetric properties of the Turkish translation of a modified neck disability index. BMC Musculoskel Disorders. 2012;13(1):1–6. doi:10.1186/1471-2474-13-25
17. Boonstra AM, Preuper HRS, Reneman MF, Posthumus JB, Stewart RE. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int J Rehab Res. 2008;31(2):165–169. doi:10.1097/MRR.0b013e3282fc0f93
18. Azevedo DC, de Lima Pires T, de Souza Andrade F, McDonnell MK. Influence of scapular position on the pressure pain threshold of the upper trapezius muscle region. Eur J Pain. 2008;12(2):226–232. doi:10.1016/j.ejpain.2007.05.004
19. Ramos GS, Silva-Batista C, Palma BP, Ugrinowitsch C, TFd C. Risk of falls using the biodex balance system in non-faller patients with parkinson disease. Somatosensory Motor Res. 2022;39(2–4):111–115. doi:10.1080/08990220.2021.2018295
20. Farooq MN, Bandpei MAM, Ali M, Khan GA. Reliability of the universal goniometer for assessing active cervical range of motion in asymptomatic healthy persons. Pakistan J Med Sci. 2016;32(2):457. doi:10.12669/pjms.322.8747
21. Andias R, Neto M, Silva AG. The effects of pain neuroscience education and exercise on pain, muscle endurance, catastrophizing and anxiety in adolescents with chronic idiopathic neck pain: a school-based pilot, randomized and controlled study. Physiother Theory Pract. 2018;34(9):682–691. doi:10.1080/09593985.2018.1423590
22. Özüdoğru A, Canlı M, Kuzu Ş, Aslan M, Ceylan I, Alkan H. Muscle strength, balance and upper extremity function are not predictors of cervical proprioception in healthy young subjects. Somatosensory Motor Res. 2023;40(2):78–82. doi:10.1080/08990220.2023.2183832
23. Ghodrati M, Mosallanezhad Z, Shati M, et al. Adding Temporomandibular joint treatments to routine physiotherapy for patients with non-specific chronic neck pain: a randomized clinical study. J Bodywork Movement Ther. 2020;24(2):202–212. doi:10.1016/j.jbmt.2019.11.004
24. Maher JM, Markey JC, Ebert-May D. The other half of the story: effect size analysis in quantitative research. CBE—Life Sci Edu. 2013;12(3):345–351. doi:10.1187/cbe.13-04-0082
25. Ghaderi F, Jafarabadi MA, Javanshir K. The clinical and EMG assessment of the effects of stabilization exercise on nonspecific chronic neck pain: a randomized controlled trial. J Back Musculoskel Rehab. 2017;30(2):211–219. doi:10.3233/BMR-160735
26. Celenay ST, Akbayrak T, Kaya DO. A comparison of the effects of stabilization exercises plus manual therapy to those of stabilization exercises alone in patients with nonspecific mechanical neck pain: a randomized clinical trial. J Orthopaedic Sports Phys Ther. 2016;46(2):44–55. doi:10.2519/jospt.2016.5979
27. Ylinen J, Takala E-P, Nykänen M, et al. Active neck muscle training in the treatment of chronic neck pain in women: a randomized controlled trial. JAMA. 2003;289(19):2509–2516. doi:10.1001/jama.289.19.2509
28. Walczyńska-Dragon K, Baron S, Nitecka-Buchta A, Tkacz E. Correlation between TMD and cervical spine pain and mobility: is the whole body balance TMJ related? BioMed Res Int. 2014;2014:1–7. doi:10.1155/2014/582414
29. Dusunceli Y, Ozturk C, Atamaz F, Hepguler S, Durmaz B. Efficacy of neck stabilization exercises for neck pain: a randomized controlled study. J Rehab Med. 2009;41(8):626. doi:10.2340/16501977-0392
30. Yesil H, Hepguler S, Dundar U, Taravati S, Isleten B. Does the use of electrotherapies increase the effectiveness of neck stabilization exercises for improving pain, disability, mood, and quality of life in chronic neck pain?: a randomized, controlled, single-blind study. LWW. 2018;2018:1.
31. Akıncı B, Zorlutuna B. Kronik Boyun Ağrısı Tedavisinde Çene Kasları Egzersizleri İle Boyun İzometrik Egzersizlerinin Etkinliklerinin Karşılaştırılması: randomize, Kontrollü Çalışma. Düzce Üniversitesi Sağlık Bilimleri Enstitüsü Dergisi. 2020;10(1):12–21.
32. Lee J-D, Shin W-S. Immediate effects of neuromuscular control exercise on neck pain, range of motion, and proprioception in persons with neck pain. Phys Ther Rehab Sci. 2020;9(1):1–9. doi:10.14474/ptrs.2020.9.1.1
33. Jull G, Kristjansson E, Dall’Alba P. Impairment in the cervical flexors: a comparison of whiplash and insidious onset neck pain patients. Manual Ther. 2004;9(2):89–94. doi:10.1016/S1356-689X(03)00086-9
34. Hidalgo‐Peréz A, Fernández‐García Á, López‐de‐Uralde‐Villanueva I, et al. Effectiveness of a motor control therapeutic exercise program combined with motor imagery on the sensorimotor function of the cervical spine: a randomized controlled trial. Int J Sports Phys Ther. 2015;10(6):877.
35. Alghadir AH, Zafar H, Iqbal ZA. Effect of three different jaw positions on postural stability during standing. Funct Neurol. 2015;30(1):53.
36. Cherry EA, Brown LE, Coburn JW, Noffal GJ. Effect of remote voluntary contractions on knee extensor torque and rate of velocity development. J Strength Conditioning Res. 2010;24(9):2564–2569. doi:10.1519/JSC.0b013e3181e7f961
37. Bernal-Utrera C, Anarte-Lazo E, Gonzalez-Gerez JJ, et al. Effect of combined manual therapy and therapeutic exercise protocols on the postural stability of patients with non-specific chronic neck pain. A secondary analysis of randomized controlled trial. J Clin Med. 2021;11(1):84. doi:10.3390/jcm11010084
38. Song G-B, Kim -J-J, Kim K-R, Kim G-Y. The effects of neck stabilization exercise and proprioceptive neuromuscular facilitation on neck alignment, NDI, and static balance in adults with forward-head posture in a sitting position. PNF Movement. 2020;18(1):11–22.
39. Yong M-S, Lee H-Y, Ryu Y-U, Lee M-Y. Effects of craniocervical flexion exercise on upper-limb postural stability during a goal-directed pointing task. J Phys Ther Sci. 2015;27(6):2005–2007. doi:10.1589/jpts.27.2005
40. Amaral AP, Politti F, Hage YE, Arruda EE, Amorin CF, Biasotto-Gonzalez DA. Immediate effect of nonspecific mandibular mobilization on postural control in subjects with temporomandibular disorder: a single-blind, randomized, controlled clinical trial. Braz J Phys Ther. 2013;17:121–127.
41. Zafar H, Alghadir AH, Iqbal ZA, Iqbal A, Anwer S, Alnahdi AH. Influence of different jaw positions on dynamic balance using Y‐balance test. Brain Behav. 2020;10(1):e01507.
42. Hosoda M, Masuda T, Isozaki K, et al. Effect of occlusion status on the time required for initiation of recovery in response to external disturbances in the standing position. Clin Biomechan. 2007;22(3):369–373.
43. Cho H-Y, Park Y-J, Moon -H-H, et al. The effect of Swiss ball stabilisation exercise on deep and superficial cervical muscle and pain in patients with chronic neck pain. Ind J Sci Technol. 2015;8:14.
44. Häggman‐Henrikson B, Nordh E, Eriksson PO. Increased sternocleidomastoid, but not trapezius, muscle activity in response to increased chewing load. Eur J Oral Sci. 2013;121(5):443–449.
45. Moon H-J, Goo B-O, Cho S-H. The effect of cocontraction of the masticatory muscles during neck stabilization exercises on thickness of the neck flexors. J Phys Ther Sci. 2015;27(3):659–661.
46. Böthun A, Häggman‐Henrikson B, Wiesinger B, Wänman A, Hellström F, Österlund C. Jaw–neck motor strategy during jaw‐opening with resistance load. J Oral Rehab. 2022;49(5):514–521.
47. Javdaneh N, Molayei F, Kamranifraz N. Effect of adding motor imagery training to neck stabilization exercises on pain, disability and kinesiophobia in patients with chronic neck pain. Complementary Ther Clin Pract. 2021;42:101263.
48. Kaka B, Ogwumike OO. Effect of neck stabilization and dynamic exercises on pain, disability and fear avoidance beliefs in patients with non-specific neck pain. Physiotherapy. 2015;101:e704.
49. Nicolakis P, Erdogmus CB, Kollmitzer J, et al. Long-term outcome after treatment of temporomandibular joint osteoarthritis with exercise and manual therapy. CRANIO®. 2002;20(1):23–27.
50. Crăciun MD, Geman O, Leuciuc FV, Holubiac IŞ, Gheorghiţă D, Filip F. Effectiveness of physiotherapy in the treatment of temporomandibular joint dysfunction and the relationship with cervical spine. Biomedicines. 2022;10(11):2962.
51. Wänman A, Marklund S. Treatment outcome of supervised exercise, home exercise and bite splint therapy, respectively, in patients with symptomatic disc displacement with reduction: a randomised clinical trial. J Oral Rehab. 2020;47(2):143–149.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Use of QR Codes for Promoting a Home-Based Therapeutic Exercise in Patients with Lumbar Disc Herniation and Lumbar Spinal Stenosis: A Prospective Randomized Study
Chang MC, Park D, Choo YJ
Journal of Pain Research 2022, 15:4065-4073
Published Date: 23 December 2022
Effect of Exercise Interventions for Rheumatoid Arthritis: A Systematic Review and Network Meta-Analysis of Randomised Controlled Trials
Zhang Y, He Z, Yin Z, Wang J, Gao W, Jie L
Journal of Pain Research 2025, 18:5109-5126
Published Date: 30 September 2025
Differential Effects of Cycling Exercise on Pain Types in Patients with Early Parkinson’s Disease: A Subgroup Analysis of a Randomized Pilot Trial
Jun JS, Choi S, Kang N, Park K, Jeon B, Byun K, Kim R
Journal of Pain Research 2025, 18:7225-7232
Published Date: 28 December 2025