Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Prognostic Value of Pace Variability, a Novel 6MWT-Derived Feature, in Patients with Chronic Obstructive Pulmonary Disease
Authors Huang CT, Ruan SY ![]() , Lai F, Chien JY
, Lai F, Chien JY ![]() , Yu CJ
, Yu CJ ![]()
Received 28 March 2023
Accepted for publication 3 July 2023
Published 21 July 2023 Volume 2023:18 Pages 1555—1564
DOI https://doi.org/10.2147/COPD.S407708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Chun-Ta Huang,1 Sheng-Yuan Ruan,1 Feipei Lai,2– 4 Jung-Yien Chien,1 Chong-Jen Yu1
1Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan; 2Graduate Institute of Biomedical Electronics and Bioinformatics, National Taiwan University, Taipei, Taiwan; 3Department of Computer Science & Information Engineering, National Taiwan University, Taipei, Taiwan; 4Department of Electrical Engineering, National Taiwan University, Taipei, Taiwan
Correspondence: Jung-Yien Chien, Department of Internal Medicine, National Taiwan University Hospital, No. 7, Zhongshan S. Road, Zhongzheng Dist, Taipei, 100, Taiwan, Tel +886-2-23562905, Fax +886-2-23222890, Email [email protected]
Purpose: The 6-minute walk test (6MWT) is often used to evaluate chronic obstructive pulmonary disease (COPD) patients’ functional capacity, with 6-minute walk distance (6MWD) and related measures being linked to mortality and hospitalizations. This study investigates the prognostic value of pace variability, a significant indicator in sports medicine, during the 6MWT for COPD patients.
Patients and Methods: We retrospectively screened consecutive COPD patients who had been prospectively enrolled in a pay-for-performance program from January 2019 to May 2020 to determine their eligibility. Patient characteristics, including demographics, exacerbation history, and 6MWT data, were analyzed to investigate their potential associations with prognosis. The primary outcome was a composite of adverse events, including overall mortality or hospitalizations due to exacerbations during a 1-year follow-up period. To analyze the 6MWT data, we divided it into three 2-minute epochs and calculated the average walk speed for each epoch. We defined pace variability as the difference between the maximum and minimum average speed in a single 2-minute epoch, divided by the average speed for the entire 6-minute walk test.
Results: A total of 163 patients with COPD were included in the study, and 19 of them (12%) experienced the composite adverse outcome. Multivariable logistic regression analyses revealed that two predictors were independently associated with the composite outcome: % predicted 6MWD < 72 (adjusted odds ratio [aOR] 7.080; 95% confidence interval [CI] 1.481– 33.847) and pace variability ≥ 0.39 (aOR 9.444; 95% CI 2.689– 33.170). Patients with either of these adverse prognostic features had significantly worse composite outcome-free survival, with both log-rank P values less than 0.005. Notably, COPD patients with both adverse features experienced an especially poor outcome after 1 year.
Conclusion: Patients with COPD who exhibited greater pace variability during the 6MWT had a significantly higher risk of overall mortality and COPD-related hospitalizations, indicating a worse prognosis.
Keywords: 6-minute walk test, chronic obstructive pulmonary disease, outcome, pace, variability
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic and debilitating condition that is often marked by periods of exacerbation. The diagnosis of COPD requires post-bronchodilator spirometry to demonstrate persistent airflow limitation.1 Despite being a mandatory component for COPD diagnosis, the spirometric parameters used to define and assess the severity of airflow limitation in COPD patients are not well correlated with patient symptoms and outcomes.2–4 Therefore, evaluating patients with COPD is now increasingly being done by determining their exercise capacity. This can be achieved through laboratory tests (eg, formal cardiopulmonary test) or field tests (eg, walking a predefined distance over a specific time). While the cardiopulmonary exercise test is the standard method for studying exercise limitation and identifying its cause in pulmonary disorder patients,5 the 6-minute walk test (6MWT) is more widely used to evaluate exercise performance in individuals with COPD because it is inexpensive, simple, easy to perform, and reliable.6,7
The 6-minute walk distance (6MWD) is the primary measurement of the 6MWT, which assesses the distance walked in 6 minutes. This measurement is a well-recognized independent predictor for mortality, hospitalizations, and exacerbations in COPD patients.8 In addition, the 6MWD measurement has been found to have associations with physical activity, health-related quality of life, and pulmonary function,7,9,10 and may also serve as an indicator of the effectiveness of interventions for patients with COPD.7,11 Besides the 6MWD, a number of variables derived from the 6MWT, such as exercise-induced oxygen desaturation (EID) and 6-minute walk work, are shown to be associated with mortality and hospitalizations of COPD subjects.12
Pace variability or variability of pacing has been widely studied in sports medicine.13 Evidence showed that a pacing strategy that an individual subconsciously selected will produce a homeostatically acceptable exercise intensity for completion of the task in the most efficient way.14 A research on cycling indicated that greater variability in cycling pace can exert negative consequences in athlete performance.15 In the marathon events, the winners can run an even pace over the 42.195-km distance.13,16 In this regard, we speculated that COPD patients would change their pace in order to minimize symptom burden during a submaximal exercise testing, 6MWT. Thus, the main objective of this study was to investigate the potential prognostic significance of pace variability in COPD patients by utilizing data from a registry database that had been collected prospectively. We hypothesized that COPD patients with greater pace variability would have a poorer 1-year prognosis compared with those with lesser pace variability.
Materials and Methods
Study Settings and Population
This observational study was conducted in the National Taiwan University Hospital, a university-affiliated medical center in Taiwan. Between January 2019 and May 2020, we screened all patients with spirometry-confirmed COPD, defined as post-bronchodilator FEV1/FVC <0.70, who were enrolled in the Taiwan nationwide COPD pay-for-performance program to determine their eligibility for the study.17 In brief, the pay-for-performance program was launched in April 2017 and patients enrolled in this program received comprehensive pharmacologic and non-pharmacologic therapeutics based on Taiwan’s COPD guidelines.18 Patients were strongly advised to schedule regular follow-up appointments every 3 months and several quality indicators, such as exacerbations and hospitalizations, were regularly monitored and assessed. In the present study, COPD subjects were included if they had their first-ever 6MWT within 90 days of the date of program enrollment. The exclusion criteria were as follows: loss to follow-up or non-respiratory mortality within 1 year of the 6MWT and early stoppers in the 6MWT. The study was conducted in compliance with the Declaration of Helsinki. The Research Ethics Committee of the National Taiwan University Hospital approved this study (201905058RINB), and since it was a retrospective and non-interventional investigation, the need for written informed consent was waived.
Data Collection and Outcome Measures
The prospective registry database of the COPD pay-for-performance program was used to collect patient demographics, smoking habits, body mass indices (BMI), dyspnea levels (using the modified Medical Research Council (mMRC) dyspnea scale), comorbidities, exacerbation histories, and lung function measurements (post-bronchodilator spirometry). The exercise data from the 6MWT (see below) were also retrieved for analyses. Current smokers included those currently smoking and those who quit smoking less than 12 months before the 6MWT. The BMI was calculated using the formula weight (in kilograms) divided by the square of height (in meters). Histories of exacerbations were collected during the 1-year period prior to the 6MWT and only moderate to severe exacerbations were recorded.1 The primary outcome of interest in this study was a combined negative outcome of overall mortality or hospitalizations due to COPD exacerbations within a year after the 6MWT.
6MWT
The 6MWT was conducted following the ATS guidelines.6 In short, patients were asked to walk in a straight flat corridor supervised by a well-trained respiratory therapist. Patients were given standardized instructions every minute during the 6MWT.7 They were allowed to take breaks and rest as needed but were encouraged to continue walking as soon as possible. Oxygen was supplemented for patients who required long-term oxygen therapy and those what had hypoxemia at rest. Post-exercise SpO2 was measured using a pulse oximeter with a finger sensor. EID was defined as a nadir SpO2 ≤88% throughout the 6MWT.19 The distance covered during the test, ie, 6MWD, was measured and reported in meters. Additionally, it was reported as a percentage of the predicted 6MWD, which was calculated based on age, gender, height, and weight using the reference equations.20 The perception of breathlessness at the end of the 6MWT was measured using the Modified Borg Scale.21
Pace Variability
There is no standard way to represent variability of pacing. Several definitions, such as coefficient of variation, calculated as the standard deviation (SD) divided by the mean, and standard deviation alone,15,22 have been used in the literature to describe pace variability. For this study, the 6MWT was split into three 2-minute segments, and the mean walking speeds for each 2-minute segment as well as the overall 6-minute period were calculated. Pace variability was then calculated using the following formula: [(maximum average speed in a single 2-minute segment) minus (minimum average speed in a single 2-minute segment)] divided by (average speed over the 6-minute period). The decision to use a 2-minute time span was based on the fact that the 2-minute walk test has been utilized to assess functional capacity and serves as an outcome measure for COPD patients.23
Validation Cohort
We assembled another COPD cohort consisting of patients enrolled in the pay-for-performance program from July 2017 to December 2018 to validate our study findings. The same inclusion and exclusion criteria were applied to the validation cohort. We aimed to evaluate the performance of cutoffs established in this study to discriminate COPD patients with different outcomes at 1 year.
Statistical Methods
The statistical analysis was conducted using SPSS for Windows (version 20, IBM, Illinois, Chicago, IL). All reported P values were two-sided and statistical significance was defined as a P value of <0.05.
The results were reported as mean ± standard deviation (SD) or percentage (%). To assess between-group differences, the independent sample t-test or χ2-square test was used, as appropriate. Receiver operating characteristic (ROC) curves were utilized to determine the sensitivity and specificity of 6MWT-derived variables in predicting the composite adverse outcome over the 1-year observation period. The best cutoffs were defined by the Youden index ((specificity + sensitivity) − 1).24 To examine the association of selected variables with the composite adverse outcome, a multivariable logistic regression model was constructed, and odds ratios (ORs) and their 95% confidence intervals (CIs) were reported. Variables that had a P value of <0.2 in the univariate analyses were included in the multivariable model. Kaplan–Meier curves were plotted to compare the incidence for the composite adverse outcome in patients with COPD according to dichotomous independent outcome predictors and the Log rank test was employed to assess the statistical significance of differences between curves.
Since physiological studies have shown that during exercise, the use of supplemental oxygen can decrease minute ventilation and postpone the occurrence of dynamic hyperinflation, leading to a delay in the onset of dyspnea, which may enable higher exercise intensity,25 a sensitivity analysis was conducted while excluding patients requiring oxygen supplement during the 6MWT.
Results
Study Subjects
During the study period, a total of 163 COPD patients were included, and Figure 1 shows the flow diagram of the study population. The study cohort had a mean age of 71 years and 90% of them were males (Table 1). Approximately two-fifths of the patients were underweight and more than a half had a normal weight. Forty-four percent of the patients had significant dyspnea (mMRC scale ≥2) and 28% were classified as GOLD grade III or IV. About one out of eight patients had experienced moderate to severe exacerbations in the past 1 year before the 6MWT. During the 6MWT, the patients walked 388 meters on average, representing 83% of the predicted 6MWD (Table 2). The mean nadir SpO2 was 91% and 31% of the cohort exhibited EID. Pace variability of the study subjects was 0.36 ± 0.22.
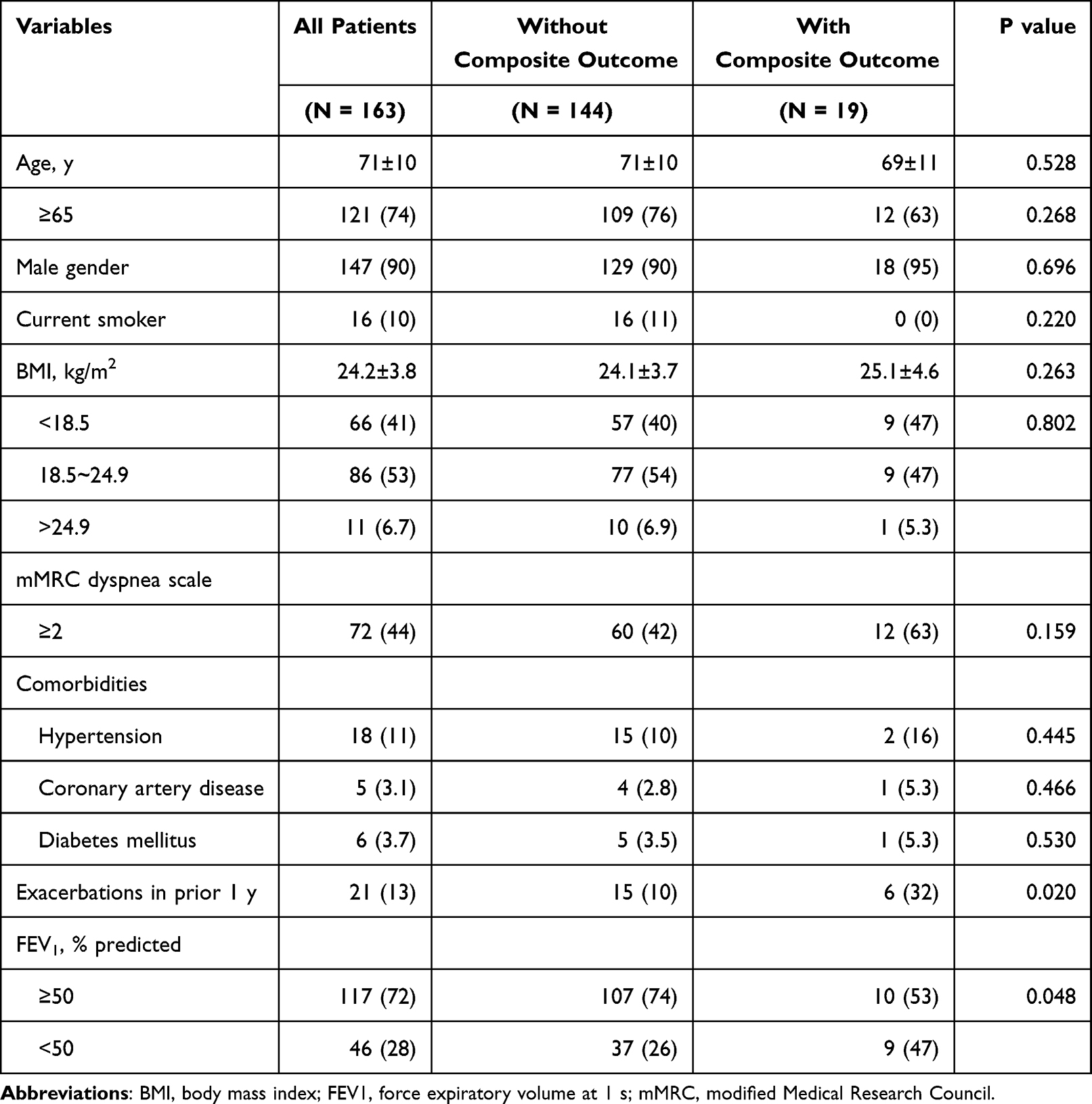 |
Table 1 Demographics and Characteristics of Patients with Chronic Obstructive Pulmonary Disease Categorized by the Composite Adverse Outcome |
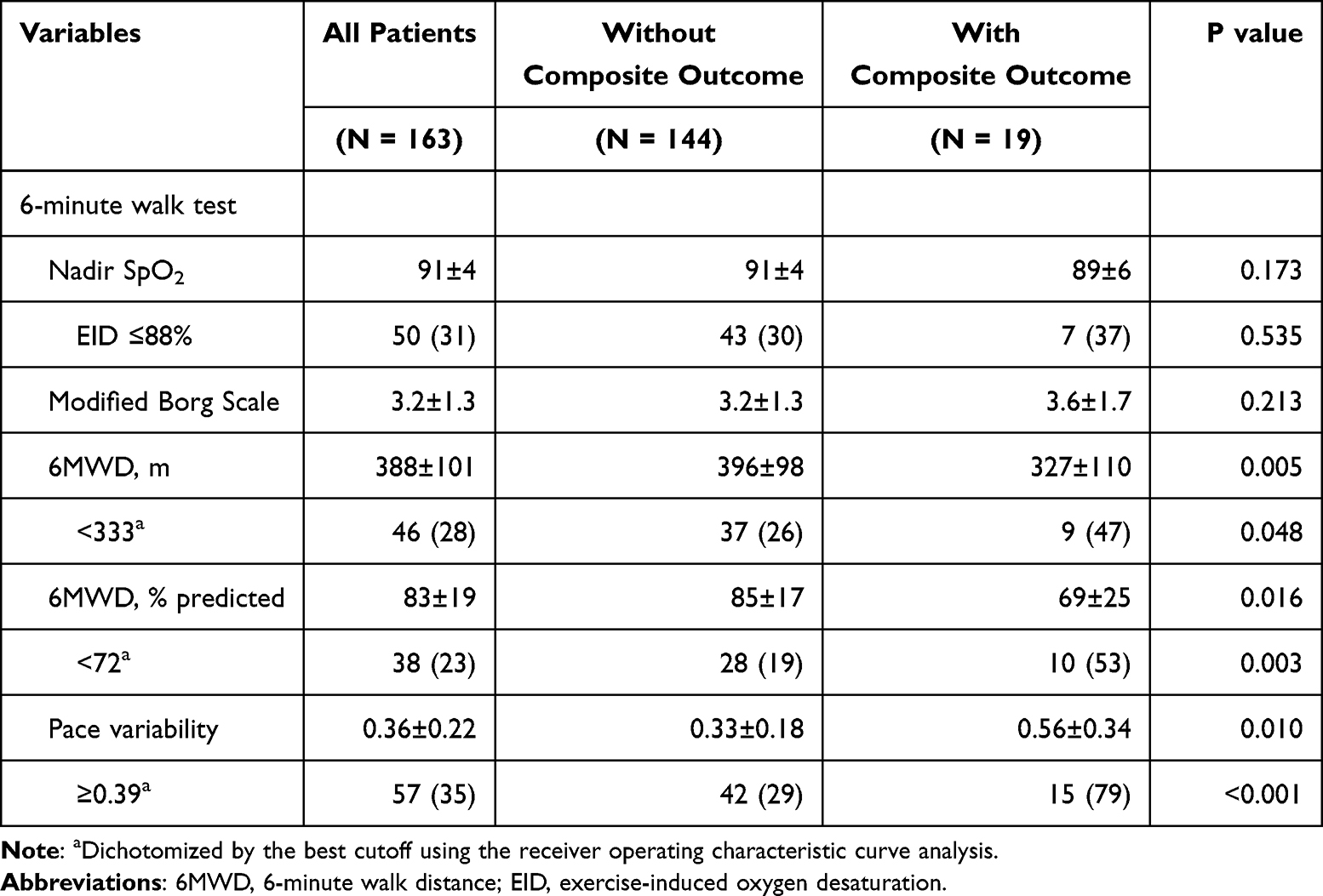 |
Table 2 Variables Derived from the 6-Minute Walk Test and Their Association with the Composite Adverse Outcome |
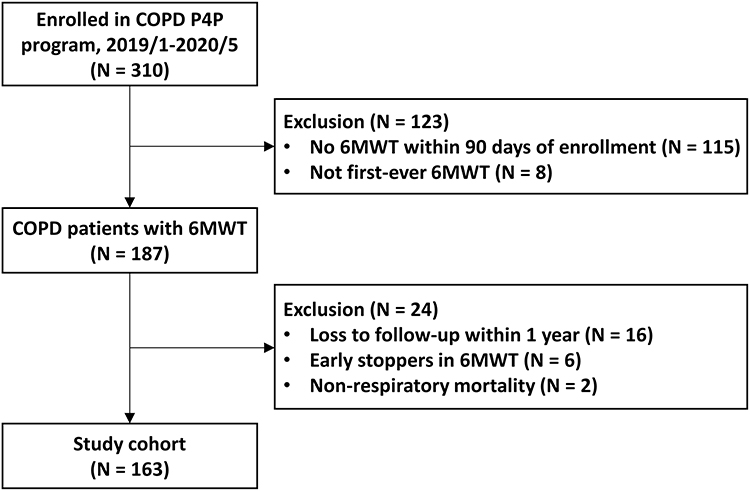 |
Figure 1 Study flow diagram. Abbreviations: 6MWT, 6-minute walk test; COPD, chronic obstructive pulmonary disease; P4P, pay-for-performance. |
Composite Adverse Outcome
At 1-year follow-up, the composite adverse outcome of overall mortality or COPD hospitalizations developed in 19 (12%) of the study population. Patients with the composite outcome were more likely to experience exacerbations in the prior 1 year (32% vs 10%) and have an FEV1 <50% predicted (47% vs 26%) compared with those without the composite outcome (Table 1). The 6MWD was shorter in COPD patients with the outcome (327 ± 110 meters) than in those without (396 ± 98 meters). The % predicted 6MWD was also lower for study subjects encountering the adverse events (Table 2). Patients with the composite adverse outcome had greater pace variability (0.56 ± 0.34) compared with those without the composite adverse outcome (0.33 ± 0.18). Figure 2 presents the ROC curves to predict the composite outcome for the 6MWD, % predicted 6MWD, and pace variability. The best cutoffs for the three aforementioned variables were <333 meters, <72%, and ≥0.39, respectively. Study subjects with the composite adverse outcome more likely walked for a distance <333 meters or <72% of predicted 6MWD and had pace variability ≥0.39 during the 6MWT (Table 2).
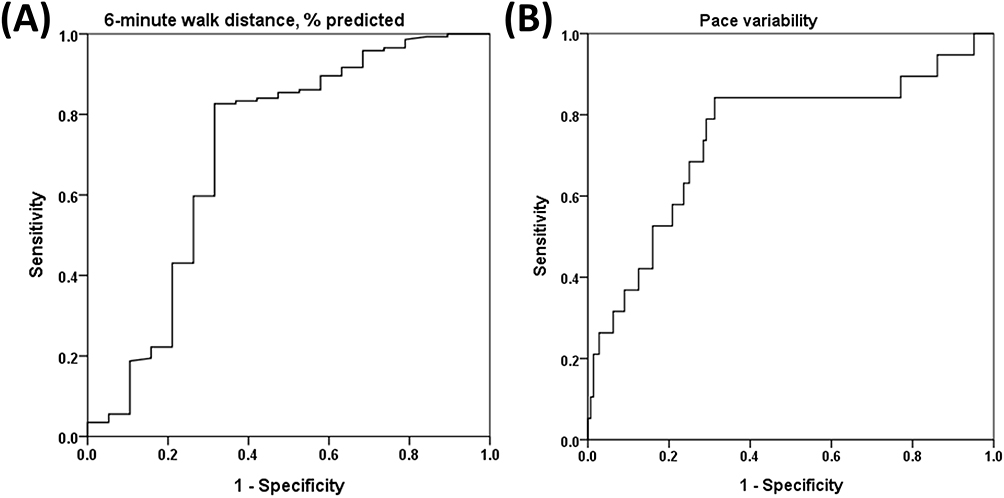 |
Figure 2 Receiver-operating characteristic curve analysis showing the accuracy of (A) 6-minute walk distance, % predicted and (B) pace variability to discriminate chronic obstructive pulmonary disease patients with and without the composite adverse outcome. The area under the curve (AUC), 95% confidence interval (CI), and P value were as follows: AUC = 0.71, 95% CI = 0.56–0.86, P = 0.003 for 6-minute walk distance, % predicted. AUC = 0.75, 95% CI = 0.61–0.88, P = 0.001 for pace variability. |
Multivariable Analysis
Multivariable logistic regression analyses (Table 3) showed the association between patient characteristics and 6MWT-derived variables and the composite adverse outcome. Two independent predictors for the adverse outcome were identified as % predicted 6MWD <72 (adjusted OR, 7.080; 95% CI, 1.481–33.847) and pace variability ≥0.39 (adjusted OR, 9.444; 95% CI, 2.689–33.170). Patients with % predicted 6MWD <72 showed significantly worse composite outcome-free survival compared with patients with predicted 6MWD ≥72 (Figure 3A). Figure 3B shows the same result for dichotomous pace variability (≥0.39 vs <0.39). Moreover, COPD subjects with both % predicted 6MWD <72 and pace variability ≥0.39 had a notably worse outcome at the end of the one-year follow-up period (Figure 3C). The sensitivity analysis by excluding 4 patients needing oxygen during the walk test did not change the prognostic significance of pace variability and % predicted 6MWD in the multivariable analysis (Results not shown).
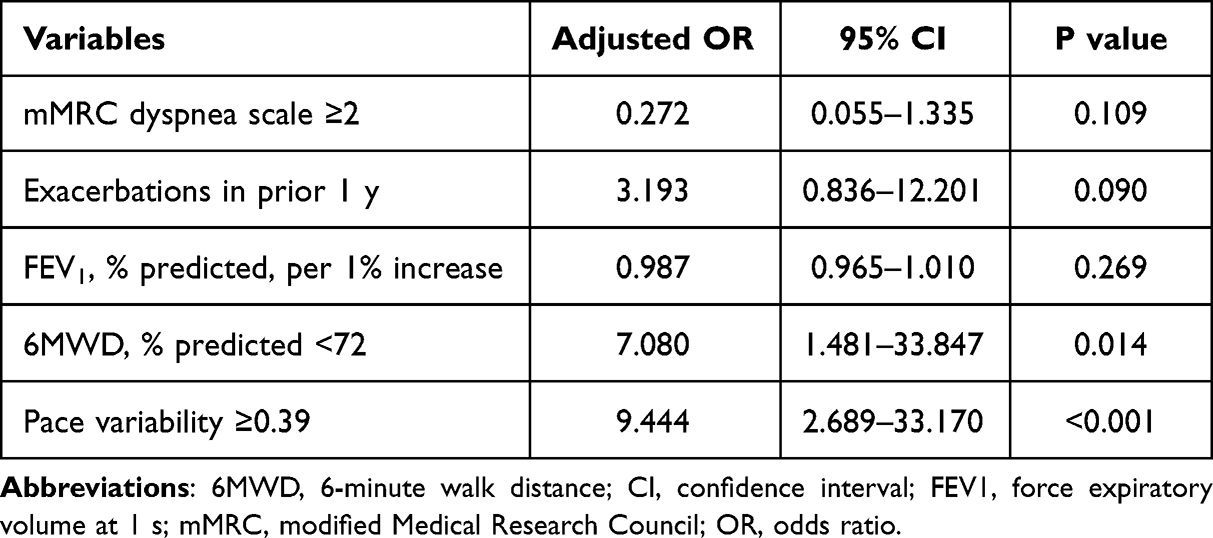 |
Table 3 Association of Patient Features with the Composite Adverse Outcome Using the Multivariable Logistic Regression Analysis |
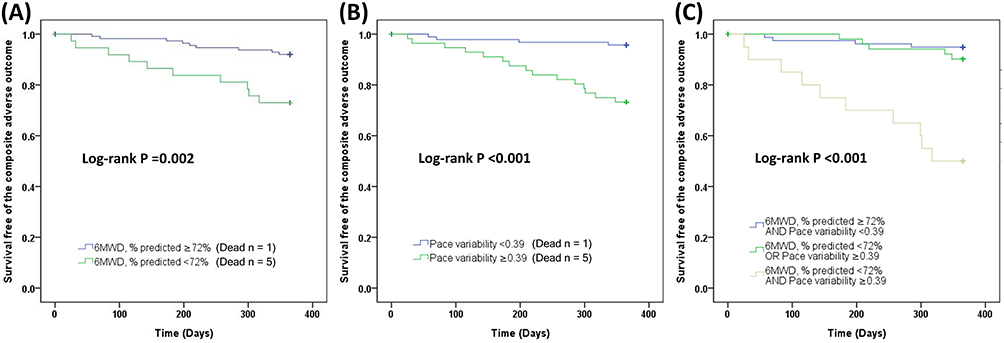 |
Figure 3 Kaplan–Meier curves for the composite adverse outcome of respiratory mortality or hospitalization for chronic obstructive pulmonary disease, stratified by the best cutoff of (A) 6-minute walk distance (6MWD), % predicted, (B) pace variability, and (C) both 6MWD, % predicted and pace variability. |
Validation
The validation cohort comprised 178 individuals with COPD, and their characteristics can be found in the supplementary material (Supplementary Table 1). Using the cutoffs of % predicted 6MWD and pace variability obtained in our study, we were similarly able to identify COPD patients with distinct 1-year outcomes (Supplementary Figure 1).
Discussion
In this study, we investigated the potential prognostic value of a new feature called pace variability, which is derived from the 6MWT, for predicting adverse outcomes in patients with COPD over a one-year follow-up period. The study revealed that a higher pace variability during the 6MWT can serve as a significant prognostic indicator for mortality and hospitalizations. Additionally, the combination of pace variability and the traditional measurement of % predicted 6MWD can refine the prognosis and better predict adverse outcomes. In brief, this study provides the first evidence supporting the prognostic value of pace variability during the 6MWT in COPD patients, highlighting its importance in identifying high-risk individuals.
Pacing strategies have been well discussed in the literature with regard to sports medicine, particularly for long-distance sport events. Of those, running events like marathons and half-marathons have gained the highest popularity in recent decades. Although pacing in a marathon can be evaluated using several methods, faster runners have been shown to adopt a pacing strategy with lesser pace variability regardless of applied methods.26–28 Studies have suggested several mechanisms and theories to explain the phenomenon, such as depletion of glycogen stores, rise in core temperature, and neurophysiological interferences.28–30 For the first time, the current study investigated pacing of patients with COPD in a distinctly different event, ie, 6MWT, and showed a prognostically significant association between greater pace variability and an adverse outcome. The pathophysiological explanations behind this observation remain obscure and should be certainly varied from those in competitive exercises. We speculate that COPD patients with greater pace variability were not able to maintain a constant distribution of pace for two reasons as follows. First, they experienced a higher intensity of breathlessness associated with lower cardiopulmonary reserve during the 6MWT and had to slow down their pace unintentionally. Second, they were less likely to preserve physiological homeostasis in response to intrinsic and extrinsic sensory signals because of limited physical performance and cognitive function.31 The aforementioned speculations may also partly explain why greater pace variability was linked to a poor 1-year prognosis in this study. On the other hand, our study suggests a promising but unproven strategy for exercise training in COPD, ie, even pacing brings more benefits than uneven pacing does.
The application of the 6MWT has been confirmed as valid for patients with COPD and can be utilized to categorize them into various risk groups based on their probability of mortality and hospitalizations for up to three years of follow-up.8,12,32 Our study reinforces the use of the 6MWT as a reliable test in COPD, as we found that the 6MWD (with cutoff points at 333 meters or 72% of predicted) was a significant indicator of composite adverse outcome survival in the univariable analysis. Furthermore, in the multivariable analysis, it provided independent prognostic information. The 6MWD cutoff in this study was consistent with a large meta-analysis showing a discriminatory value of 350 meters to differentiate risks of death and hospitalizations.8 The cutoff value of the % predicted 6MWD has not been well established in COPD; however, our cutoff point was close to those (72% and 70%, respectively) established by Mura et al33 and Mancuzo et al34 for idiopathic pulmonary fibrosis. Another noteworthy discovery of this study is that the % predicted 6MWD, calculated using the reference equations of Enright and Sherrill, was a more dependable predictor of survival and severe COPD exacerbations compared to the 6MWD in absolute values.20 This observation lends support to the need for the creation of reference equations on a larger healthy population that encompasses diverse racial and ethnic backgrounds.35
In this study, we proposed a new prognostic indicator, pace variability, to be evaluated during the 6MWT. However, our aim was not to supplant traditional valuable indices such as % predicted 6MWD. We found that both pace variability and % predicted 6MWD had comparable discriminative power in differentiating COPD patients with different outcomes regarding overall mortality and COPD-related hospitalizations. Notably, taking both indicators together provides more value in recognizing COPD subjects with particularly worse outcomes. A rational application of our study's findings is to supplement the existing 6MWT variable with our novel one to better inform prognostication for COPD patients.
This study has several limitations that should be taken into consideration. First, the cohort in this study consisted of COPD patients enrolled in a pay-for-performance program and a limited number of patients suffered from the composite adverse outcome; thus, the generalizability is still to be seen cautiously. However, as a novel index of the 6MWT, our findings doubtlessly encourage more researches in this field. Second, only patients with their first-ever 6MWT were included. Therefore, the well-known learning effect for the 6MWD should be borne in mind while applying our study findings to the context that the subjects have a practice walk or two sessions of 6MWT are performed based on the 2014 ERS/ATS standard.36 Third, a change in a patient’s management plan was not protocolized given the non-interventional nature of the current study; thus, the confounding effects of both pharmacological and non-pharmacological therapy on prognosis cannot be excluded. Fortunately, this was a single institutional study conducted in an academic medical center where patients in the pay-for-performance program were predominantly treated in accordance with Taiwan’s COPD guidelines.18 These unique features may minimize the variations in quality of patient care among physicians and their impact on our study results. Finally, despite the well-established reproducibility of the 6MWT in patients with COPD,37 there is still limited knowledge regarding the reproducibility of pace variability, particularly in an elderly population. While a learning effect has been observed in repeated 6MWTs,37 its specific impact on pace variability in COPD patients is not yet clear. Further research is necessary to address this issue and provide more insights.
Conclusion
In summary, pace variability, a novel but easily accessible 6MWT-derived feature, differed between COPD patients with and without the composite adverse outcome during the 1-year follow-up. Patients with COPD who displayed greater pace variability during the 6MWT were found to have a notably poorer prognosis in terms of respiratory mortality and COPD-related hospitalizations. Furthermore, patients showing both a lower % predicted 6MWD and greater pace variability during the 6MWT experienced a particularly poor 1-year outcome. Further studies are required to validate our findings in a larger patient population with COPD.
Data Sharing Statement
All data requests should be submitted to Dr Jung-Yien Chien ([email protected]) for consideration. Access to anonymized data might be granted following investigator review.
Acknowledgments
We would like to express our gratitude to the technical support provided by the staff of the Eighth Core Lab, Department of Medical Research, National Taiwan University Hospital during the study. Additionally, we would like to thank the staff of the Department of Medical Research, National Taiwan University Hospital for the Integrated Medical Database (NTUH-iMD).
Funding
This work was supported by grants to J.Y.C. from the Ministry of Science and Technology, Taiwan (MOST 111-2314-B-002-201-MY3) and National Taiwan University Hospital (112-S0108). The study sponsors had no role in study design, data collection, analysis, and interpretation; in the writing of the manuscript; nor in the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
2. Kohli P, Pinto-Plata V, Divo M, et al. Functional capacity, health status, and inflammatory biomarker profile in a cohort of patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil Prev. 2015;35(5):348–355.
3. Smith LE, Moore E, Ali I, Smeeth L, Stone P, Quint JK. Prognostic variables and scores identifying the end of life in COPD: a systematic review. Int J Chron Obstruct Pulmon Dis. 2017;12:2239–2256.
4. Kakavas S, Kotsiou OS, Perlikos F, et al. Pulmonary function testing in COPD: looking beyond the curtain of FEV1. NPJ Prim Care Respir Med. 2021;31(1):23.
5. Laveneziana P, Di Paolo M, Palange P. The clinical value of cardiopulmonary exercise testing in the modern era. Eur Respir Rev. 2021;30(159):955.
6. Enright PL. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117.
7. Singh SJ, Puhan MA, Andrianopoulos V, et al. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1447–1478.
8. Celli B, Tetzlaff K, Criner G, et al. The 6-Minute-Walk Distance Test as a Chronic Obstructive Pulmonary Disease Stratification Tool. Insights from the COPD Biomarker Qualification Consortium. Am J Respir Crit Care Med. 2016;194(12):1483–1493.
9. Agusti A, Calverley PM, Celli B, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11(1):122.
10. Rebelo P, Brooks D, Marques A. Measuring intensity during free-living physical activities in people with chronic obstructive pulmonary disease: a systematic literature review. Ann Phys Rehabil Med. 2022;65(2):101607.
11. Puente-Maestu L, Palange P, Casaburi R, et al. Use of exercise testing in the evaluation of interventional efficacy: an official ERS statement. Eur Respir J. 2016;47(2):429–460.
12. Andrianopoulos V, Wouters EF, Pinto-Plata VM, et al. Prognostic value of variables derived from the six-minute walk test in patients with COPD: results from the ECLIPSE study. Respir Med. 2015;109(9):1138–1146.
13. Haney TA Jr, Mercer JA. A description of variability of pacing in marathon distance running. Int J Exerc Sci. 2011;4(2):133–140.
14. St Clair Gibson A, Noakes TD. Evidence for complex system integration and dynamic neural regulation of skeletal muscle recruitment during exercise in humans. Br J Sports Med. 2004;38(6):797–806.
15. Palmer GS, Noakes TD, Hawley JA. Effects of steady-state versus stochastic exercise on subsequent cycling performance. Med Sci Sports Exerc. 1997;29(5):684–687.
16. Ely MR, Martin DE, Cheuvront SN, Montain SJ. Effect of ambient temperature on marathon pacing is dependent on runner ability. Med Sci Sports Exerc. 2008;40(9):1675–1680.
17. Cheng SL, Li YR, Huang N, et al. Effectiveness of Nationwide COPD Pay-for-Performance Program on COPD Exacerbations in Taiwan. Int J Chron Obstruct Pulmon Dis. 2021;16:2869–2881.
18. Cheng SL, Lin CH, Chu KA, et al. Update on guidelines for the treatment of COPD in Taiwan using evidence and GRADE system-based recommendations. J Formos Med Assoc. 2021;120(10):1821–1844.
19. Golpe R, Pérez-de-Llano LA, Méndez-Marote L, Veres-Racamonde A. Prognostic value of walk distance, work, oxygen saturation, and dyspnea during 6-minute walk test in COPD patients. Respir Care. 2013;58(8):1329–1334.
20. Enright PL, Sherrill DL. Reference equations for the six-minute walk in healthy adults. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1384–1387.
21. Johnson MJ, Close L, Gillon SC, Molassiotis A, Lee PH, Farquhar MC. Use of the modified Borg scale and numerical rating scale to measure chronic breathlessness: a pooled data analysis. Eur Respir J. 2016;47(6):1861–1864.
22. Billat VL, Slawinski J, Danel M, Koralsztein JP. Effect of free versus constant pace on performance and oxygen kinetics in running. Med Sci Sports Exerc. 2001;33(12):2082–2088.
23. Johnston KN, Potter AJ, Phillips AC. Minimal important difference and responsiveness of 2-minute walk test performance in people with COPD undergoing pulmonary rehabilitation. Int J Chron Obstruct Pulmon Dis. 2017;12:2849–2857.
24. Akobeng AK. Understanding diagnostic tests 3: receiver operating characteristic curves. Acta Paediatr. 2007;96(5):644–647.
25. Lukacsovits J, Szollosi G, Varga JT. Cardiovascular effects of exercise induced dynamic hyperinflation in COPD patients-Dynamically hyperinflated and non-hyperinflated subgroups. PLoS One. 2023;18(1):e0274585.
26. Deaner RO, Carter RE, Joyner MJ, Hunter SK. Men are more likely than women to slow in the marathon. Med Sci Sports Exerc. 2015;47(3):607–616.
27. Trubee NW, Vanderburgh PM, Diestelkamp WS, Jackson KJ. Effects of heat stress and sex on pacing in marathon runners. J Strength Cond Res. 2014;28(6):1673–1678.
28. March DS, Vanderburgh PM, Titlebaum PJ, Hoops ML. Age, sex, and finish time as determinants of pacing in the marathon. J Strength Cond Res. 2011;25(2):386–391.
29. de Koning JJ, Foster C, Bakkum A, et al. Regulation of pacing strategy during athletic competition. PLoS One. 2011;6(1):e15863.
30. Roelands B, de Koning J, Foster C, Hettinga F, Meeusen R. Neurophysiological determinants of theoretical concepts and mechanisms involved in pacing. Sports Med. 2013;43(5):301–311.
31. Noakes TD, Peltonen JE, Rusko HK. Evidence that a central governor regulates exercise performance during acute hypoxia and hyperoxia. J Exp Biol. 2001;204(Pt 18):3225–3234.
32. Dajczman E, Wardini R, Kasymjanova G, Préfontaine D, Baltzan MA, Wolkove N. Six minute walk distance is a predictor of survival in patients with chronic obstructive pulmonary disease undergoing pulmonary rehabilitation. Can Respir J. 2015;22(4):225–229.
33. Mura M, Porretta MA, Bargagli E, et al. Predicting survival in newly diagnosed idiopathic pulmonary fibrosis: a 3-year prospective study. Eur Respir J. 2012;40(1):101–109.
34. Mancuzo EV, Soares MR, Pereira CAC. Six-minute walk distance and survival time in patients with idiopathic pulmonary fibrosis in Brazil. J Bras Pneumol. 2018;44(4):267–272.
35. Casanova C, Celli BR, Barria P, et al. The 6-min walk distance in healthy subjects: reference standards from seven countries. Eur Respir J. 2011;37(1):150–156.
36. Holland AE, Spruit MA, Troosters T, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1428–1446.
37. Hernandes NA, Wouters EF, Meijer K, Annegarn J, Pitta F, Spruit MA. Reproducibility of 6-minute walking test in patients with COPD. Eur Respir J. 2011;38(2):261–267.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Hospital Pharmacist Interventions for COPD Patients: A Systematic Literature Review and Logic Model
Lin G, Zheng J, Tang PK, Zheng Y, Hu H, Ung COL
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2757-2788
Published Date: 25 October 2022