Back to Journals » Journal of Pain Research » Volume 18
Effectiveness of High-Voltage, Long-Duration Pulsed Radiofrequency in the Treatment of Postherpetic Neuralgia in the Elderly: Protocol for a Randomized Clinical Trial
Authors Li W ![]() , He L, Lin P, Chen R, Liu R
, He L, Lin P, Chen R, Liu R
Received 27 September 2025
Accepted for publication 18 December 2025
Published 24 December 2025 Volume 2025:18 Pages 7087—7095
DOI https://doi.org/10.2147/JPR.S570761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Wangyu Li,1,2,* Long He,1,2,* Peng Lin,1,2,* Ri Chen,3 Rongguo Liu1,2
1Department of Painology, the First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 2Department of Painology, National Regional Medical Center, Binhai Campus of the First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 3Department of Painology, Fuzhou University Affiliated Provincial Hospital, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ri Chen, Email [email protected] Rongguo Liu, Email [email protected]
Introduction: Pulsed Radiofrequency (PRF) is a minimally invasive, non-neurodestructive interventional therapy commonly used in pain management. However, the optimal PRF parameters have yet to be clearly defined, and the clinical efficacy of different PRF settings in elderly patients with postherpetic neuralgia (PHN) remains uncertain. Therefore, this study aims to determine whether high-voltage, long-duration PRF (HLPRF) can offer better pain relief, improve sleep quality, and reduce anxiety symptoms in elderly PHN patients, without increasing the risk of PRF-related adverse events.
Methods: This investigator-initiated, single-center, randomized, two-arm clinical trial enrolls patients over 65 years of age with PHN who are scheduled for PRF surgery. A total of 88 eligible patients will be randomly assigned to either the standard PRF group or the HLPRF group. In the standard PRF group, the output voltage is set at 45 V with a pulse duration of 360 seconds. In the HLPRF group, the output voltage is set at 85 V and the pulse duration at 900 seconds. All other parameters and treatment protocols are consistent across both groups. Data for this trial were systematically collected at multiple time points, including at admission and at 4, 12, 26, and 52 weeks postoperatively. The primary outcome measure was the postoperative Numerical Rating Scale (NRS) score. Secondary outcomes included several key indicators: postoperative Pregabalin dosage, Pittsburgh Sleep Quality Index (PSQI), 12-Item Short Form Health Survey (SF-12), and Hospital Anxiety and Depression Scale (HADS). Adverse events occurring during the intraoperative period and throughout the postoperative follow-up will be meticulously documented as critical safety indicators. Subgroup analyses will be conducted post hoc to examine potential differences based on whether patients exhibit frailty, thereby providing nuanced insights into the treatment outcomes among different patient populations.
Conclusion: The results of this study may provide evidence-based medical evidence for the use of HLPRF for the treatment of PHN and may help to assist clinicians in selecting different parameters PRF for the treatment of PHN for clinical practice.
Trial Registration Number: ChiCTR2400086627.
Keywords: pulsed radiofrequency, postherpetic neuralgia, elderly patients, study protocol
Introduction
Herpes zoster (HZ), commonly referred to shingles, is triggered by the reactivation of the latent varicella-zoster virus (VZV) residing within the sensory ganglia. This reactivation manifests clinically as clusters of blisters that are typically distributed unilaterally along the dermatomes, a pattern that reflects the innervation by the affected nerve roots.1,2 On a global scale, the incidence of HZ is estimated to range from 3 to 5 cases per 1000 person-years. Notably, this incidence significantly escalates in individuals over the age of 50, reaching approximately 8 to 12 cases per 1,000 person-years by age 80.3 This age-related increase underscores the vulnerability of older populations to HZ.
Most patients suffering from HZ experience a severe painful condition known as zoster-associated pain (ZAP). ZAP is the most common form of pain associated with HZ and is often the primary reason for patients to seek medical attention. This type of pain can significantly impact the quality of life and is a critical factor in the clinical management of HZ.4 ZAP encompasses both acute-phase pain and postherpetic neuralgia (PHN). Acute-phase pain is the pain experienced from the onset of HZ until the lesions have healed. In contrast, PHN is defined as pain that persists for 1 month or more after the healing of the lesions and can be both persistent and variable in its nature.5 PHN is the most common complication of HZ, significantly affecting patients’ quality of life and increasing economic costs.6 PHN develops in roughly 20% of HZ patients,7,8 with risk factors such as advanced age, immunosuppression, severe acute-phase ZAP, and diabetes mellitus.9,10 Notably, the incidence of PHN escalates with age, affecting 18% of HZ patients over 50 years and 33% of those over 80 years.11 Frailty represents an emerging age-related global health burden, characterized by reduced physiological capacity in multiple organ systems, thereby increasing susceptibility to stressors. Research indicates that frailty is associated with impaired immune responses, heightened susceptibility to infectious diseases, and increased adverse reactions among the elderly. Moreover, frailty may exacerbate the risk of PHN.12–15 Therefore, in geriatric populations, identifying frailty may have significant implications for the prevention and treatment of PHN.
Ion channel modulators, primarily represented by anticonvulsants such as gabapentin and pregabalin, serve as the mainstay treatment for postherpetic neuralgia (PHN). Depending on the patient’s clinical progression, tricyclic antidepressants or serotonin-norepinephrine reuptake inhibitors may be considered as adjunctive therapy. However, fewer than 50% of patients achieve <50% pain relief. For refractory cases, the timely introduction of minimally invasive interventions in addition to pharmacotherapy may yield greater benefits.16–18 Pulsed Radiofrequency (PRF) is a non-neurodestructive, minimally invasive interventional therapy with good efficacy and safety in ZAP treatment.19 However, the optimal parameter settings for Pulsed Radiofrequency (PRF) are still undetermined. Recent studies have found that high-voltage long-duration PRF (HLPRF) is more effective for both pain relief and quality of life improvement in the acute phase of ZAP compared with standard PRF (SPRF). Moreover, HLPRF does not increase the incidence of PRF-related adverse events.20,21 However, the clinical efficacy of HLPRF in elderly patients with PHN has not been supported by evidence.
Therefore, we propose a randomized controlled trial to investigate whether HLPRF for the treatment of elderly patients with PHN provides better pain relief, improves sleep and anxiety symptoms, and does not increase the incidence of PRF-related adverse events.
Methods
Study Design
This is a single-center, prospective, randomized, controlled clinical study to be conducted in the Pain Department of Fuzhou University Affiliated Provincial Hospital. A total of 88 eligible patients will be randomly assigned to either the standard PRF group or the HLPRF group. The reporting of this trial followed the Consolidated Standards of Reporting Trials (CONSORT) Guidelines 201022 (Figure 1).
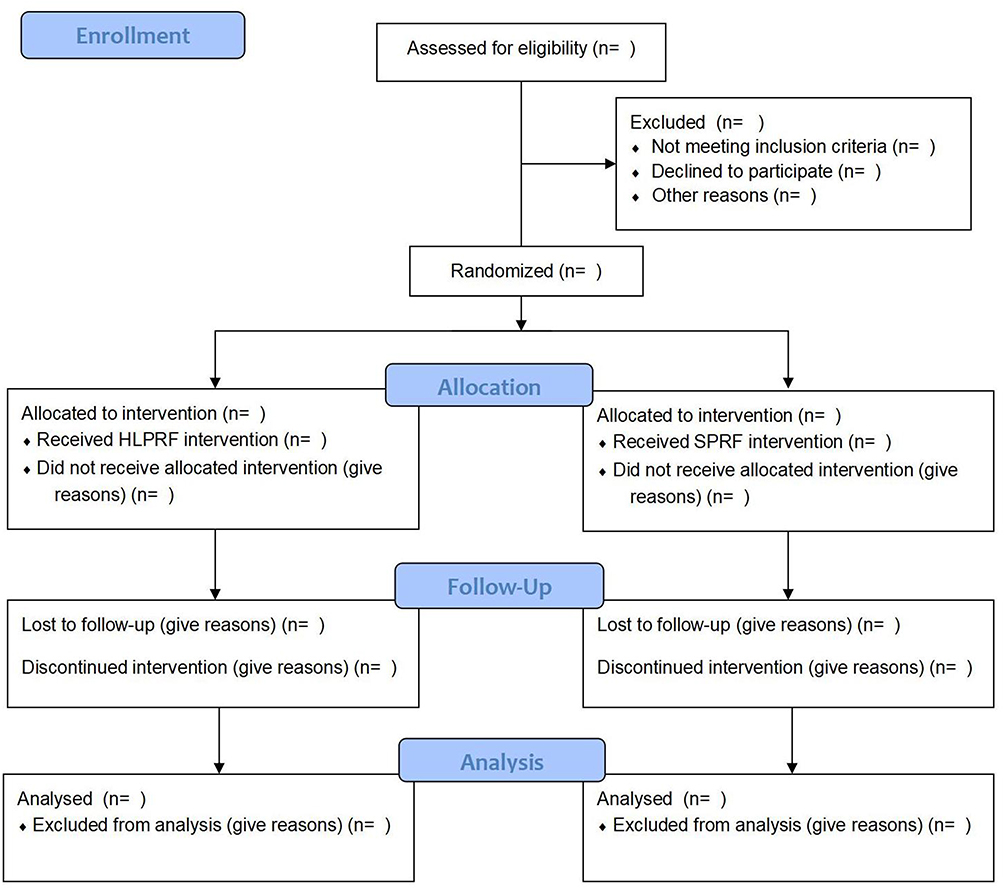 |
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram describing patient progress throughout the study. |
Ethics
The protocol was approved by the Medical Ethics Committee of Fujian Provincial Hospital prior to recruitment (approval number: K2024-06-064). The study protocol has completed clinical trial registration in the China Clinical Trial Registry (registration number: ChiCTR2400086627). All eligible patients were screened at admission. Eligible patients received information about the trial procedures, potential benefits, and complications, voluntarily signed a clinical trial informed consent form, and retained the right to withdraw at any time. This study was conducted in accordance with the Declaration of Helsinki (2013). The protocol design complies with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement (Supplementary 1) and IMMPACT recommended.23
Patient Recruitment
Inclusion criteria: (1) age >65 years; (2) meeting the diagnostic criteria for PHN; (3) persistent severe pain, ie, Numeric Rating Scale (NRS) pain score ≥6, accompanied by localized cutaneous nociceptive hypersensitivity, numbness, or sensory abnormality; and (4) poorly controlled pain with medication.
Exclusion criteria: (1) localized infection at the treatment site; (2) coagulation disorders; (3) history of severe cardiopulmonary, hepatic, or renal insufficiency; (4) severe thoracolumbar spinal stenosis, compression fracture, or scoliosis; (5) psychiatric disorders, inability or refusal to cooperate, or refusal to participate; and (6) substance abuse.
Withdrawal criteria: (1) unwillingness to continue participation or inability to follow the initial treatment plan; (2) inability to obtain any primary outcome data for any reason.
Randomization and Blinding
An independent researcher utilizing SAS 9.4 software will randomize eligible patients into two groups in a 1:1 ratio, assigning them either to the HLPRF group or the SPRF group. The allocation will be sealed by the investigator in sequentially numbered, sealed, and opaque envelopes. The sealed envelope containing the group assignment should be given to the surgeon prior to the procedure. It should be unsealed by the designated researcher to reveal the randomization group. The treatment plan is not to be disclosed to the patient during the operation. The surgeon, who is not responsible for recruiting patients, obtaining informed consent, and conducting the randomization, will be informed of the allocation results.
The study was unblinded only to the physicians who performed the PRF treatment. Although blinding was implemented, differences in the voltage and duration parameters between the two groups may have inadvertently revealed the group allocation to the patients. Outcome assessors and statisticians were blinded to the group assignments and operated independently of each other. This means that other individuals involved in the study, including outcome assessors, ward medical staff, and statisticians, remained blinded to the group assignments.
Interventions
The patient was observed in a prone position during a computed tomography (CT) scan. Continuous monitoring of the electrocardiogram (ECG), blood pressure, and heart rate was conducted, and intravenous access was established. The dorsal root ganglion (DRG) nerves targeted for treatment were identified based on areas of skin hyperpigmentation caused by HZ infection. This condition typically manifests with nociceptive hypersensitivity or abnormal pain. Thin-layer (2 mm) CT-guided guidance was employed to determine the location of the medial margin of the upper middle third of the intervertebral foramen corresponding to the target nerve. This information was used to design and define the puncture path. Following the induction of local anesthesia, PRF trocar needles (specifically, 20-gauge, 15-cm electrodes with a 10-mm active tip, model PMF-20-150-10, manufactured by Baylis Medical Inc., Montreal, QC, Canada) were carefully inserted until the tips reached the mid-upper intervertebral foramen. Subsequently, three-dimensional CT reconstruction was performed. The tip of the needle, connected to a PMG-230 pain therapy generator (Baylis Medical Inc., Montreal, QC, Canada), was moved slowly in sensory testing mode (50 Hz). When abnormal sensations (primarily soreness, numbness, heat, and occasional twitch-like or tingling sensations) were observed below 0.5 V and no myokinesis was observed above 1.0 V in the area of the skin where nociceptive sensitization was occurring, we confirmed that the tip of the needle was appropriately located on the target nerve of the DRG. Subsequent settings used on the pain treatment generator were as follows: in the S group, the output voltage was set to 45 V and the pulse duration to 360 seconds. In the HL group, the output voltage was set to 85 V, and the pulse duration was 900 seconds. Other parameters were consistent. At the end of the RF procedure, an analgesic compound (1% lidocaine 1 mL + saline 1.7 mL + 0.3 mL compound betamethasone) was injected into the DRG. The RF needle was removed at the end of the pulsed RF, and the wound was pressed for 2 minutes and then covered with a dressing.
Data Collection
The required data will be collected by trained researchers as per the participant schedule outlined in Table 1. The data will initially be recorded on paper Case Report Forms (CRFs) and subsequently stored in an Excel digital format. Follow-up visits will be conducted by researchers either in person or by telephone to enhance compliance with the intervention program. All CRFs will be retained for a minimum of 5 years post-study termination. Two independent researchers will enter all information into an Excel sheet on a password-protected computer. The final dataset will be accessible to the researchers and statisticians involved in the study.
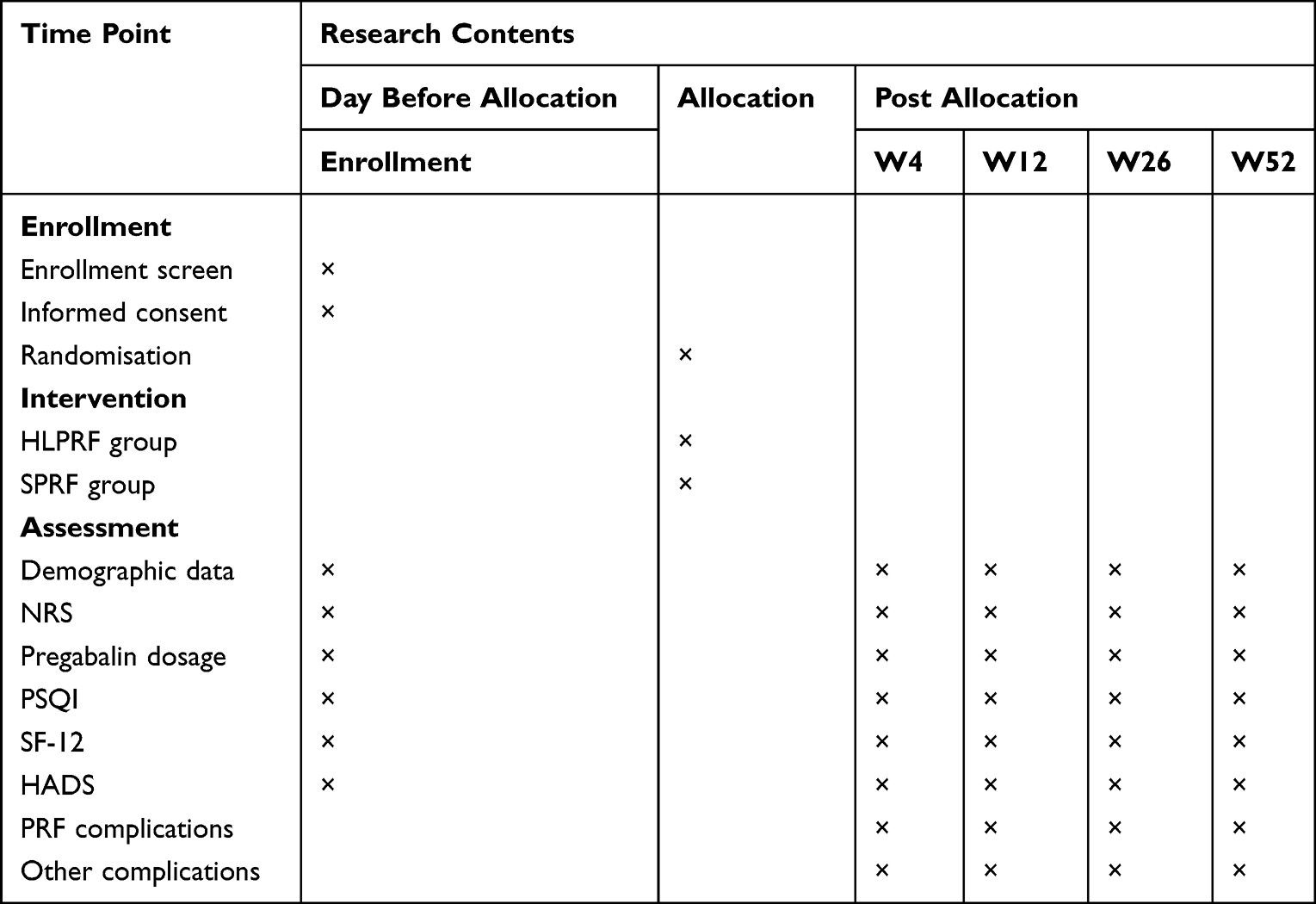 |
Table 1 Schedule of Enrollment, interventions, and Assessments |
Baseline Characteristics
After signing the informed consent form, the blinded investigator will record the patient’s demographics, disease characteristics, and other relevant data on the CRF at the time of admission. Demographic data will include age, gender, body mass index (BMI), HZ site, disease duration, and frailty score. The frailty score will be measured using the FRAIL scale, which consists of five items: (1) fatigue; (2) resistance: difficulty in walking up one flight of stairs; (3) decline in free mobility: inability to walk for one block; (4) coexistence of multiple illnesses: ≥5; and (5) weight loss: reduction of >5.0% of body weight over one year. This scale categorizes older adults into three stages: healthy, pre-frailty (presence of 1 or 2 items), and frailty (3 or more items satisfied).
Outcomes
Primary Outcome
The primary outcome of this trial will be measured using the NRS. The NRS allows patients to quantify the intensity of pain on an 11-point scale ranging from 0 to 10, where a score of 0 indicates no pain and a score of 10 represents the worst pain imaginable.24 The time points for measuring the primary outcome will be at admission, and at 4 weeks, 12 weeks, 26 weeks, and 52 weeks PRF treatment. The minimum clinically important difference (MCID) from baseline to follow-up will be 2 points.25 Pain recovery is defined as the complete or almost complete disappearance of symptoms, corresponding to an NRS score between 0 and 1.
Secondary Outcomes
Pregabalin Dosage: The dosage of pregabalin was recorded at specific time points, including admission and at 4, 12, 26, and 52 weeks following PRF treatment.
Pittsburgh Sleep Quality Index (PSQI): The PSQI is a widely used tool to assess the quality of sleep in subjects over the past month. It consists of 18 self-assessment items, which are integrated into 7 components: sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Each component is scored on a scale of 0 to 3, with higher scores indicating worse sleep quality. The total PSQI score is the sum of these component scores, ranging from 0 to 21.26 In this study, PSQI scores were recorded at multiple time points: at admission and at 4, 12, 26, and 52 weeks following peripheral radiofrequency (PRF) treatment. Data collection was conducted by a dedicated individual at each time point for both study groups.
12-item Short Form Health Survey (SF-12): The SF-12 is a comprehensive tool used to evaluate eight dimensions of health-related quality of life: physical functioning, role limitations due to physical health, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems, and mental health. From these eight dimension scores, separate total physical health scores and total mental health scores can be derived.27 In this study, SF-12 scores were recorded at specific time points: at admission and at 4, 12, 26, and 52 weeks PRF treatment in both study groups. Each score was documented by a dedicated individual at each designated time point.
Hospital Anxiety and Depression Scale (HADS): The HADS is a self-assessment tool that consists of two subscales: HADS-A (Anxiety) and HADS-D (Depression), totaling 14 items. Seven items are specifically designed to assess anxiety, and another seven items are aimed at evaluating depression. Each item is rated on a 4-point Likert scale based on the frequency of symptoms experienced over the past month. The scoring ranges from 0 to 3 for each item, with higher scores indicating more severe symptoms of anxiety or depression.28 In this study, HADS scores were systematically recorded at admission and at 4, 12, 26, and 52 weeks PRF treatment, in both study groups.
Security Indicators
Potential complications of surgery: (1) Intraoperative complications: These encompass intraoperative arrhythmias, nausea/vomiting, dizziness, excessive or decreased blood pressure, and puncture-related complications such as pneumothorax and intradural or paravertebral hematomas. (2) Postoperative complications: These include localized redness and swelling, puncture site infection, increased pain intensity, and numbness. We documented postoperative complications during the hospital stay and follow-up periods, treated them promptly, and recorded their recovery progress.
Sample Size Calculation
The sample size was determined based on the NRS scores after PRF treatment. Using an 80% test efficacy and a two-tailed alpha of 0.05, we aimed to detect a minimum difference of 1 point on the NRS, with a standard deviation of 1.5. The calculated sample size required for each group was 37 participants. Accounting for a 20% dropout rate, a total of 88 participants (44 per group) were ultimately recruited.
Statistical Analysis
Data were analyzed using SPSS 26.0 and R4.3.2. Continuous variables were presented as mean ± standard deviation ( ) or median [25th percentile, 75th percentile] (M[Q1,Q3]). Independent samples t-tests were employed for comparisons between groups with normally distributed data, while Mann–Whitney U-tests were used for non-normally distributed data. Categorical data were expressed as counts (percentages) and analyzed using chi-square tests or Fisher’s exact tests. Statistical significance was set at P < 0.05, with Bonferroni correction applied for pairwise comparisons across multiple time points. For primary and secondary outcomes, mixed effects models were employed for analysis. To quantify the overall treatment effect during the follow-up period, t-tests were used to compare between-group differences in the area under the curve (AUC) for each outcome measure. Subgroup analyses were conducted in post hoc fashion based on whether patients were debilitated. The primary analyses were performed upon completion of the study, adhering to the intention-to-treat principle.
) or median [25th percentile, 75th percentile] (M[Q1,Q3]). Independent samples t-tests were employed for comparisons between groups with normally distributed data, while Mann–Whitney U-tests were used for non-normally distributed data. Categorical data were expressed as counts (percentages) and analyzed using chi-square tests or Fisher’s exact tests. Statistical significance was set at P < 0.05, with Bonferroni correction applied for pairwise comparisons across multiple time points. For primary and secondary outcomes, mixed effects models were employed for analysis. To quantify the overall treatment effect during the follow-up period, t-tests were used to compare between-group differences in the area under the curve (AUC) for each outcome measure. Subgroup analyses were conducted in post hoc fashion based on whether patients were debilitated. The primary analyses were performed upon completion of the study, adhering to the intention-to-treat principle.
Data and Safety Monitoring Committee (DSMC)
Participants’health was monitored by the DSMC, which had the authority to suspend or terminate the trial to safeguard participants in the event of serious or unexpected adverse events. The DSMC meetings were chaired by Rongguo Liu, a pain physician.
Protocol Changes
Any significant protocol alterations will be promptly communicated to pertinent stakeholders, including the Medical Ethics Committee of Fujian Provincial Hospital, the Chinese Clinical Trials Registry, academic journals, and principal researchers.
Discussion
The primary objective of this study was to investigate the analgesic efficacy of HLPRF in elderly patients diagnosed with PHN, and to assess its impact on sleep quality and anxiety symptoms in this population.
Current research on High-Intensity Pulsed Radiofrequency (HLPRF) has primarily focused on retrospective studies. Notably, Wang et al20 conducted a prospective randomized controlled trial to compare the efficacy and safety of two different PRF modalities for the neuromodulation of the semilunar ganglion in elderly patients with acute trigeminal HZ. Their findings indicated that HLPRF significantly improved Visual Analog Scale scores and SF-36 quality of life scores, while also reducing the dosage of pregabalin, without increasing the incidence of adverse effects. Euasobhon et al29 reported that NRS demonstrated the highest sensitivity and stability for assessing chronic pain in patients. Consequently, we selected the NRS score as the primary outcome indicator in our study. Although the SF-36 has demonstrated utility for various assessment purposes, its length and complexity can pose challenges for patients, particularly in follow-up settings. To address this, the SF-12 was developed as a abbreviated version of the SF-36, reducing the questionnaire length by two-thirds while maintaining a high degree of measurement accuracy and consistency.27 Furthermore, the SF-12 has been validated in Chinese populations,30 making it a suitable choice for assessing both physical and mental health in this study.
In recent years, a strong correlation between sleep disorders and pain has been widely recognized. Studies have reported that 67–88% of patients with chronic pain disorders experience sleep problems.28,29,31,32 Additionally, up to 60% of chronic pain patients exhibit negative mood changes, such as anxiety and depression.33 Pain and mood disorders interact and reinforce each other, with pain being a major risk factor for the development of depression, and depression exacerbating pain.34,35 These interactions can lead to increased disability and economic burden.36 Recent studies have shown that PRF can effectively improve sleep quality and mood disorders in patients with acute-phase ZAP.37–39 However, the effect of HLPRF on sleep quality and mood disorders in patients with PHN remains unexplored. Therefore, we propose to investigate the role of HLPRF in improving sleep quality and mood disorders in patients with PHN.
The selection of parameters for PRF treatment is primarily based on previous studies.20,21,40 Typically, the duration for HLPRF is set to 900 seconds; however, the voltage output varies across studies, ranging from 60 to 100 volts. In the present study, we referenced findings from previous animal studies conducted in our group.41 These studies involved the application of PRF at different voltages to the DRG of neuropathic rats. We observed that 85 volts of PRF was most effective in alleviating pain, even surpassing higher voltages of 100 volts. This improved efficacy might be attributed to the restoration of DRG damage and the enhancement of DRG ultrastructure.42 Furthermore, considering the clinical experience accumulated in our center, we opted for an output voltage of 85 volts for the HLPRF treatment of the DRG in patients with PHN. This choice is supported by both experimental evidence and practical clinical applications, aiming to achieve optimal pain relief and functional improvement while minimizing potential adverse effects.
Frailty and pain constitute significant clinical and social challenges, and recent research has increasingly highlighted a robust association between these two conditions.41 Kilgore et al42 reported that among elderly patients undergoing microvascular decompression for trigeminal neuralgia, the presence of preoperative frailty may serve as a predictor of elevated postoperative pain levels. Similarly, in patients undergoing major noncardiac surgery, preoperative frailty was associated with an almost fivefold increased risk of developing chronic postoperative pain compared to non-frail patients. In light of these findings, the present study conducted a post hoc analysis to examine the influence of preoperative frailty on the outcomes of HLPRF treatment.
Limitations
It is the first randomized controlled clinical trial of HLPRF in elder PHN patients with the aim to prove the potential analgesic effect of HLPRF in this setting. The study is subject to several inherent limitations. Initially, the trial was conducted as a single-center, small-sample, prospective, randomized controlled trial, which may constrain the overall strength of the evidence. Future research could enhance the robustness of the findings by including large-sample, multicenter trials. Secondly, to assess the long-term effects of the intervention, a one-year follow-up period was established. However, the extended duration might inadvertently increase the rate of patient dropout, thereby potentially biasing the results. Finally, the current study solely examined the differential impacts of HLPRF and SPRF without delving into the independent roles of voltage and time course in the treatment efficacy of PRF. Future investigations should aim to elucidate these independent factors to provide a more comprehensive understanding of PRF’s therapeutic effects.
Conclusion
The results of this study may provide evidence-based medical evidence for the use of HLPRF for the treatment of PHN and may help to assist clinicians in selecting different parameters PRF for the treatment of PHN for clinical practice.
Trial Status
This is version 1.0 of the protocol, dated June 27, 2024. Recruitment began on July 8, 2024. Recruitment is anticipated to end on December 31, 2025. This study is still in progress.
Data Sharing Statement
The data of this study are available from the Rongguo Liu upon reasonable request.
Acknowledgments
We thank all study participants for their involvement in the study, and all the principal investigators and clinical staff participating in the trial for their efforts.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was sponsored by Joint Funds for Innovation of Science and Technology, Fujian Province (No. 2024Y9165), Joint Funds for Innovation of Science and Technology, Fujian Province (No. 2024Y9133) and Fujian Province Finance Project (No. BPB-2024LRG), Project supported by the Natural Science Foundation of Fujian Province, China (Grant No. 2024J011013).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gershon AA, Gershon MD, Breuer J, et al. Advances in the understanding of the pathogenesis and epidemiology of herpes zoster. J Clin Virol. 2010;48(Suppl 1):S2–S7. doi:10.1016/S1386-6532(10)70002-0
2. Asada H. Recent topics in the management of herpes zoster. J Dermatol. 2023;50:305–310. doi:10.1111/1346-8138.16666
3. Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open. 2014;4:e4833. doi:10.1136/bmjopen-2014-004833
4. Bricout H, Haugh M, Olatunde O, et al. Herpes zoster-associated mortality in Europe: a systematic review. BMC Public Health. 2015;15:466. doi:10.1186/s12889-015-1753-y
5. Zhang D, Lei T, Qin L, et al. Efficacy and safety of crisugabalin (HSK16149) in adults with postherpetic neuralgia: a Phase 3 randomized clinical trial. JAMA Dermatol. 2024;160:1182–1191. doi:10.1001/jamadermatol.2024.3410
6. Pica F, Gatti A, Divizia M, et al. One-year follow-up of patients with long-lasting post-herpetic neuralgia. BMC Infect Dis. 2014;14:556. doi:10.1186/s12879-014-0556-6
7. Johnson RW, Rice ASC. Clinical practice. Postherpetic neuralgia. N Engl J Med. 2014;371:1526–1533. doi:10.1056/NEJMcp1403062
8. Massengill JS, Kittredge JL. Practical considerations in the pharmacological treatment of postherpetic neuralgia for the primary care provider. J Pain Res. 2014;7:125–132. doi:10.2147/JPR.S57242
9. Forbes HJ, Bhaskaran K, Thomas SL, et al. Quantification of risk factors for postherpetic neuralgia in herpes zoster patients: a cohort study. Neurology. 2016;87:94–102. doi:10.1212/WNL.0000000000002808
10. Forbes HJ, Thomas SL, Smeeth L, et al. A systematic review and meta-analysis of risk factors for postherpetic neuralgia. Pain. 2016;157:30–54. doi:10.1097/j.pain.0000000000000307
11. Yawn BP, Gilden D. The global epidemiology of herpes zoster. Neurology. 2013;81:928–930. doi:10.1212/WNL.0b013e3182a3516e
12. Hoogendijk EO, Afilalo J, Ensrud KE, et al. Frailty: implications for clinical practice and public health. Lancet. 2019;394:1365–1375. doi:10.1016/S0140-6736(19)31786-6
13. Vetrano DL, Triolo F, Maggi S, et al. Fostering healthy aging: the interdependency of infections, immunity and frailty. Ageing Res Rev. 2021;69:101351. doi:10.1016/j.arr.2021.101351
14. Zorzoli E, Pica F, Masetti G, et al. Herpes zoster in frail elderly patients: prevalence, impact, management, and preventive strategies. Aging Clin Exp Res. 2018;30:693–702. doi:10.1007/s40520-018-0956-3
15. An S, Chae JS, Lee HJ, et al. Association of psoas: lumbar vertebral index (PLVI) with postherpetic neuralgia in patients aged 60 and older with herpes zoster. J Clin Med. 2024;13:3100. doi:10.3390/jcm13113100
16. Huerta MA, Garcia MM, Garcia-Parra B, et al. Investigational drugs for the treatment of postherpetic neuralgia: systematic review of randomized controlled trials. Int J Mol Sci. 2023;24.
17. Tang J, Zhang Y, Liu C, et al. Therapeutic strategies for postherpetic neuralgia: mechanisms, treatments, and perspectives. Curr Pain Headache Rep. 2023;27:307–319.
18. Yu Q, Wang X, Wu J, et al. Efficacy and safety of electroacupuncture for postherpetic neuralgia and biomarker evaluation: a study protocol for a multicenter, randomized trial. J Pain Res. 2025;18:5753–5768.
19. Rui M, Ni H, Xie K, et al. Progress in radiofrequency therapy for Zoster-associated pain about parameters, modes, targets, and combined therapy: a narrative review. Pain Ther. 2024;13:23–32. doi:10.1007/s40122-023-00561-7
20. Wan C, Song T. Comparison of two different pulsed radiofrequency modes for prevention of postherpetic neuralgia in elderly patients with acute/subacute trigeminal herpes zoster. Neuromodulation. 2022;25:1364–1371. doi:10.1111/ner.13457
21. Zhang E, Fei Y, Xu L, et al. Effect of repeated high-voltage long-duration pulsed radiofrequency on herpetic neuralgia. Pain Physician. 2022;25:E1047–E1055.
22. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. doi:10.1136/bmj.c332
23. Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain. 2003;106:337–345. doi:10.1016/j.pain.2003.08.001
24. Lee JJ, Lee MK, Kim JE, et al. Pain relief scale is more highly correlated with numerical rating scale than with visual analogue scale in chronic pain patients. Pain Physician. 2015;18:E195–E200.
25. Farrar JT, Young JPJ, Lamoreaux L, et al. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94:149–158. doi:10.1016/S0304-3959(01)00349-9
26. Buysse DJ, Reynolds CFR, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi:10.1016/0165-1781(89)90047-4
27. Ware JJ, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34:220–233. doi:10.1097/00005650-199603000-00003
28. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67:361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
29. Euasobhon P, Atisook R, Bumrungchatudom K, et al. Reliability and responsivity of pain intensity scales in individuals with chronic pain. Pain. 2022;163:e1184–e1191. doi:10.1097/j.pain.0000000000002692
30. Fong DYT, Chan BKY, Li S, et al. Average and individual differences between the 12-item MOS Short-form Health Survey version 2 (SF-12 V.2) and the veterans RAND 12-item Health Survey (VR-12) in the Chinese population. Health Qual Life Outcomes. 2022;20:102. doi:10.1186/s12955-022-02010-z
31. Todd J, Austin H, Clarke P, et al. Chronic pain, insomnia and their mutual maintenance: a call for cognitive bias research. J Pain. 2022;23:1530–1542. doi:10.1016/j.jpain.2022.03.241
32. Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013;14:1539–1552. doi:10.1016/j.jpain.2013.08.007
33. Rayner L, Hotopf M, Petkova H, et al. Depression in patients with chronic pain attending a specialised pain treatment centre: prevalence and impact on health care costs. Pain. 2016;157:1472–1479. doi:10.1097/j.pain.0000000000000542
34. Bravo L, Llorca-Torralba M, Suarez-Pereira I, et al. Pain in neuropsychiatry: insights from animal models. Neurosci Biobehav Rev. 2020;115:96–115. doi:10.1016/j.neubiorev.2020.04.029
35. Doan L, Manders T, Wang J. Neuroplasticity underlying the comorbidity of pain and depression. Neural Plast. 2015;2015:504691. doi:10.1155/2015/504691
36. Wang X, Peng M, Weng L, et al. Bibliometric study of the comorbidity of pain and depression research. Neural Plast. 2019;2019:1657498. doi:10.1155/2019/1657498
37. Wu C, Lin H, Chen S, et al. Efficacy of pulsed radiofrequency in herpetic neuralgia: a meta-analysis of randomized controlled trials. Clin J Pain. 2020;36:887–895. doi:10.1097/AJP.0000000000000867
38. Wang C, Dou Z, Yan M, et al. Efficacy and safety of pulsed radiofrequency in herpes zoster related trigeminal neuralgia: a systematic review and meta-analysis. J Pain Res. 2023;16:341–355. doi:10.2147/JPR.S396209
39. Ji M, Yao P, Han Z, et al. Pulsed radiofrequency combined with methylene blue paravertebral nerve block effectively treats thoracic postherpetic neuralgia. Front Neurol. 2022;13:811298. doi:10.3389/fneur.2022.811298
40. Sun C, Li X, Li C, et al. High-voltage, long-duration pulsed radiofrequency to the dorsal root ganglion provides improved pain relief for herpes zoster neuralgia in the subacute stage. Pain Physician. 2023;26:E155–E162. doi:10.36076/ppj.2023.26.E155
41. D’Agnelli S, Amodeo G, Franchi S, et al. Frailty and pain, human studies and animal models. Ageing Res Rev. 2022;73:101515. doi:10.1016/j.arr.2021.101515
42. Kilgore CB, Kalluri AL, Nair SK, et al. Frailty predicts worse pain outcomes for older TN patients treated with microvascular decompression. World Neurosurg. 2023;180:e700–e705. doi:10.1016/j.wneu.2023.10.009
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Preoperative Level of Glycemic Control with Pulsed Radiofrequency on the Incidence of Postherpetic Neuralgia in Patients with Herpes Zoster Combined with Type 2 Diabetes Mellitus: A Cohort Study
Hua B, An M, Chen L, Ni H, Ni C, Yao M
Diabetes, Metabolic Syndrome and Obesity 2024, 17:3975-3987
Published Date: 24 October 2024
Novel Ultrasound-Guided Cervical Sympathetic Chain Pulsed Radiofrequency for Subacute Herpes Zoster Neuralgia
Lin S, Lin M, Wang F, Zhuo Y, Lin K, Wang J
Journal of Pain Research 2024, 17:3627-3637
Published Date: 7 November 2024
Efficacy and Safety of Pulsed Radiofrequency Combined with Platelet-Rich Plasma in the Treatment of Postherpetic Neuralgia: A Systematic Review and Meta-Analysis
Lu Z, Zhao C, Ni H, Yao M
Journal of Pain Research 2025, 18:7213-7224
Published Date: 30 December 2025
A Study on the Efficacy and Safety of Intravenous Lidocaine Infusion Combined with Pulsed Radiofrequency in Preventing Postherpetic Neuralgia: A Randomized, Double-Blind, Controlled Trial
Xu P, Fan H, Yu M, Fei Y
Journal of Pain Research 2026, 19:562972
Published Date: 11 February 2026
Comparative Efficacy of Pulsed Radiofrequency-Based and Related Interventions for Postherpetic Neuralgia: A Network Meta-Analysis of Randomized Controlled Trials
Li L, Yang X, Chen S, Xuan C, Zhou M, Zhang Y, Wang X
Journal of Pain Research 2026, 19:607566
Published Date: 29 June 2026