Back to Journals » Patient Preference and Adherence » Volume 20
Effectiveness of an Internet-Based 4C Nursing Model on Pulmonary Rehabilitation Outcomes in Patients with Chronic Obstructive Pulmonary Disease: A Quasi-Experimental Study
Authors Shen F, Guo Z, Zhang Z, Zhou H
Received 13 March 2026
Accepted for publication 10 June 2026
Published 30 June 2026 Volume 2026:20 609086
DOI https://doi.org/10.2147/PPA.S609086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Fufen Shen1, Zhankun Guo2, Zhifen Zhang3, Hui Zhou4
1Second Department of Neurorehabilitation, Baoding Rehabilitation Hospital, Baoding, Hebei, People’s Republic of China; 2Party Committee Office, Baoding Rehabilitation Hospital, Baoding, Hebei, People’s Republic of China; 3Department of Respiratory Medicine, Baoding Rehabilitation Hospital, Baoding, Hebei, People’s Republic of China; 4Department of Physiotherapy, Beijing Fengtai Yinling Hospital of Traditional Chinese Medicine, Beijing, People’s Republic of China
Correspondence: Hui Zhou, Email [email protected]
Purpose: Pulmonary rehabilitation (PR) adherence in patients with chronic obstructive pulmonary disease (COPD) declines markedly after hospital discharge, underscoring the need for theory-driven, continuous care models. The 4C nursing model—integrating Comprehensiveness, Collaboration, Coordination, and Continuity—provides a structured, patient-centered framework that may simultaneously address multiple adherence barriers when delivered via internet-based platforms. This study evaluated the effectiveness of this integrated approach for COPD pulmonary rehabilitation.
Patients and Methods: A quasi-experimental study was conducted at Baoding Rehabilitation Hospital (January–December 2024). Ninety-four patients with COPD (GOLD stages II–III) were allocated sequentially to a control group (n = 47; conventional nursing care) or an intervention group (n = 47; internet-based 4C nursing model). Primary outcomes were COPD knowledge scores and PR adherence; secondary outcomes included the COPD Self-Efficacy Scale (CSES), FEV1% predicted, and the COPD Assessment Test (CAT). Outcomes were assessed at baseline, 3 months, and 6 months.
Results: Baseline characteristics were comparable between groups (all P > 0.05). At 6 months, the intervention group showed significantly greater improvements in COPD knowledge (mean difference 8.55; 95% CI 7.27– 9.83; Cohen’s d = 2.70), self-efficacy (mean difference 15.48; 95% CI 12.25– 18.71; d = 1.94), and PR adherence (mean difference 0.74; 95% CI 0.50– 0.97; d = 1.27), alongside significant improvements in FEV1% predicted (P = 0.005; d = 0.77) and CAT scores (P < 0.001; d = 1.39).
Conclusion: This single-center quasi-experimental study found that an internet-based 4C nursing model was associated with clinically meaningful improvements across multiple COPD outcomes over 6 months. These preliminary findings support the feasibility of theory-driven, telehealth-enhanced nursing care and warrant confirmation through multicenter randomized trials.
Keywords: chronic obstructive pulmonary disease, 4C nursing model, pulmonary rehabilitation, internet-based intervention, self-efficacy, telehealth
Introduction
Chronic obstructive pulmonary disease (COPD) remains one of the most formidable global health challenges, ranking as the third leading cause of death worldwide and imposing an escalating socioeconomic burden on healthcare systems.1,2 In China, the epidemiological landscape is particularly concerning: a nationally representative analysis demonstrated that the prevalence of spirometry-defined COPD among adults aged 40 years and older has risen to 13.7%, affecting an estimated 100 million individuals.3 The disease trajectory is characterized by progressive airflow limitation, recurrent exacerbations, and a relentless decline in functional capacity, ultimately culminating in diminished quality of life and premature mortality.4
Pulmonary rehabilitation (PR) has emerged as an indispensable component of comprehensive COPD management. International guidelines uniformly endorse PR as a Grade A evidence-based intervention that yields clinically meaningful improvements in exercise tolerance, dyspnea, and health-related quality of life.5,6 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations reaffirm that PR should be offered to all symptomatic patients with an FEV1 below 80% predicted, underscoring its therapeutic primacy alongside pharmacotherapy.7 Nevertheless, the translational gap between evidence and practice remains stark. Systematic reviews have revealed that fewer than 10% of eligible patients access structured PR programs, and among those who initiate rehabilitation, dropout rates range from 20% to 60%.8,9 Following hospital discharge, adherence deteriorates further, with the majority of patients abandoning prescribed exercise regimens within weeks.10 Barriers to sustained PR adherence include geographical inaccessibility, transportation limitations, insufficient disease knowledge, low self-efficacy, and inadequate post-discharge follow-up.10,11
The advent of digital health technologies has catalyzed a paradigm shift in chronic disease management. Internet-based and telehealth platforms have demonstrated considerable promise in overcoming traditional barriers to rehabilitation access by enabling remote monitoring, real-time communication, and sustained patient engagement beyond the confines of hospital settings.12,13 Recent systematic reviews and meta-analyses have affirmed that telehealth-delivered PR achieves outcomes comparable to or exceeding those of center-based programs in terms of exercise capacity, symptom burden, and quality of life.14,15 These digital interventions capitalize on the ubiquity of smartphones and social media platforms, which have achieved particularly high penetration among older adults in China through applications such as WeChat.16 However, realizing the full potential of internet-based PR requires addressing key contextual challenges, including variable digital literacy among older adults, unequal access to broadband infrastructure, and heterogeneity in patient technological competence—factors that can limit real-world uptake and necessitate tailored implementation strategies.
Despite the growing body of evidence supporting telehealth-based PR, a critical gap persists in the care model that underlies these interventions. Prior telehealth-based PR programs predominantly focus on exercise supervision or remote monitoring without embedding the intervention within a comprehensive, theory-driven nursing framework,17 failing to simultaneously address the multifaceted barriers to COPD rehabilitation adherence—insufficient disease knowledge, low self-efficacy, inadequate social support, and poor post-discharge care continuity. The 4C nursing model—originally conceptualized as a patient-centered care paradigm—integrates four synergistic dimensions that directly target these barriers: Comprehensiveness (holistic, individualized assessment to enhance knowledge and tailor rehabilitation plans), Collaboration (tripartite engagement among providers, patients, and families to build self-efficacy and social accountability), Coordination (multidisciplinary team integration to sustain adherence), and Continuity (seamless inpatient-to-outpatient transition to maintain long-term quality of life improvements).18,19 This model is uniquely suited to COPD pulmonary rehabilitation because each of its four dimensions directly maps to a primary outcome domain—Comprehensiveness to knowledge improvement, Collaboration to self-efficacy enhancement, Coordination to adherence maintenance, and Continuity to sustained quality-of-life benefits. Prior applications in stroke rehabilitation and chronic disease management have demonstrated its efficacy,20,21 yet its integration with internet-based delivery platforms for COPD pulmonary rehabilitation has not been systematically evaluated—a critical gap this study addresses.
We hypothesized that integrating the 4C nursing model with internet-based platforms would address multiple barriers to PR adherence simultaneously: the Comprehensiveness dimension ensures personalized rehabilitation planning; the Collaboration dimension leverages social support networks through digital communities; the Coordination dimension facilitates multidisciplinary input; and the Continuity dimension enables sustained post-discharge engagement. This study aimed to evaluate the effectiveness of an internet-based 4C nursing model on COPD-related knowledge, self-efficacy, PR adherence, pulmonary function, and quality of life in patients with moderate-to-severe COPD over a 6-month follow-up period.
Materials and Methods
Study Design and Setting
This quasi-experimental study with a nonequivalent control group design was conducted at the Department of Respiratory Medicine, Baoding Rehabilitation Hospital, Baoding, Hebei Province, China, between January 2024 and December 2024. The study protocol was approved by the institutional ethics committee of Baoding Rehabilitation Hospital (Approval number: 202302), and all participants provided written informed consent prior to enrollment. This study adheres to the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) statement.
Participants
Patients hospitalized for acute exacerbation of COPD were screened for eligibility. Inclusion criteria were: (1) a confirmed diagnosis of COPD based on the 2017 GOLD criteria (post-bronchodilator FEV1/FVC ratio < 0.70) 29; (2) hospitalization for acute exacerbation with a length of stay of 3 days or more; (3) GOLD spirometric severity stage II (50% ≤ FEV1% predicted < 80%) or stage III (30% ≤ FEV1% predicted < 50%) 27; (4) intact cognitive function and ability to provide informed consent; and (5) residence within Baoding municipality to facilitate follow-up. Exclusion criteria included: (1) coexisting pulmonary parenchymal diseases such as malignancy or active tuberculosis; (2) severe comorbidities including organ failure; (3) history of psychiatric illness or cognitive impairment precluding participation; and (4) loss to follow-up or occurrence of life-threatening events during the study period.
A total of 126 patients were screened during the enrollment period. Of these, 18 did not meet the inclusion criteria, 10 declined to participate, and 4 were excluded for other reasons. The remaining 94 eligible patients were allocated to the control group (n = 47) or the intervention group (n = 47) based on the timing of hospital admission (January–June 2024 for the control group, July–December 2024 for the intervention group) to minimize contamination between groups. Although this sequential allocation approach precludes randomization, we confirmed the absence of substantive changes in institutional COPD management protocols or pharmaceutical regimens during the study period, mitigating the risk of temporal confounding. No participants were lost to follow-up, yielding a 100% retention rate (Figure 1).
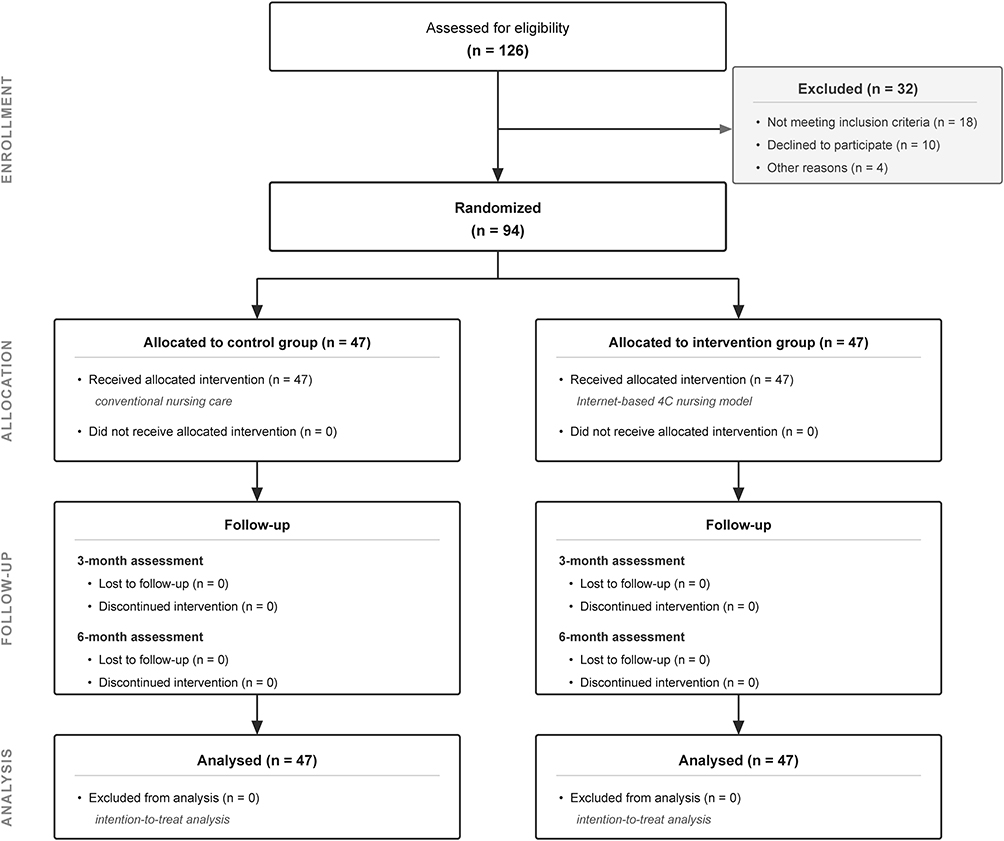 |
Figure 1 Study flow diagram. A total of 126 patients were screened for eligibility, of whom 94 met the inclusion criteria and were allocated to the control group (n = 47) or the intervention group (n = 47). No participants were lost to follow-up during the 6-month study period. |
Sample Size Calculation
The sample size was determined a priori using G*Power software (version 3.1.9.7) based on a two-tailed independent-samples t-test with an effect size of 0.60 (derived from preliminary literature on nursing interventions in COPD rehabilitation), a significance level (α) of 0.05, and a statistical power (1 − β) of 0.80. The minimum required sample size was 37 per group. Allowing for a 20% attrition rate, we targeted 47 participants per group, yielding a total sample of 94.
Interventions
Control Group: Patients in the control group received conventional nursing care as per institutional protocols. This encompassed standardized inpatient health education delivered through group lectures and bedside instruction, covering topics such as basic disease knowledge, effective coughing and sputum clearance techniques, medication adherence, and breathing exercises (pursed-lip breathing and diaphragmatic breathing). At discharge, patients received printed educational materials and were instructed to continue home-based exercises. Routine outpatient follow-up was scheduled at 3 and 6 months postdischarge.
Intervention Group: In addition to the conventional care components, patients in the intervention group received the internet-based 4C nursing model intervention, structured as follows:
- Comprehensiveness: Upon admission, each patient underwent a comprehensive multidimensional assessment encompassing pulmonary function, nutritional status, psychological well-being, exercise capacity, and social support. An individualized rehabilitation plan was developed, incorporating advanced airway clearance techniques, active cycle of breathing technique (ACBT), and forced expiratory technique (FET). A personalized health dossier was established for longitudinal tracking.
- Collaboration: A dedicated WeChat group titled “Pulmonary Rehabilitation Home” was established, comprising respiratory physicians, rehabilitation therapists, specialist nurses, patients, and designated family caregivers. This platform facilitated real-time question-and-answer sessions, peer support interactions, and family-mediated exercise supervision. Weekly themed discussions on disease management topics were moderated by the nursing team.
- Coordination: A multidisciplinary team consisting of respiratory physicians, rehabilitation therapists, clinical pharmacists, nutritionists, and psychological counselors collaborated to address the multifaceted needs of each patient. Case conferences were conducted biweekly to review patient progress and adjust rehabilitation plans accordingly.
- Continuity: Post-discharge follow-up was maintained through multiple internet-based channels. WeChat push notifications delivered tailored health education content twice weekly. Video consultations via Tencent Meeting were conducted biweekly during the first 3 months and monthly thereafter. These sessions included supervised exercise demonstrations, medication reconciliation, and psychosocial support. Monthly peer support meetings were organized through video conferencing to sustain motivation and social connection.
Outcome Measures
All outcome measures were assessed at three time points: baseline (day of admission), 3 months postdischarge, and 6 months postdischarge. Follow-up assessments at 3 and 6 months were conducted during scheduled outpatient visits.
Primary Outcomes
- COPD Knowledge: Assessed using a validated COPD Knowledge Questionnaire comprising 21 items, each scored 0 to 2, yielding a total score range of 0 to 42. Higher scores indicate greater disease knowledge. Scores of 28 or above denote high knowledge, 14 to 27 denote moderate knowledge, and below 14 denote low knowledge.22
- Self-Efficacy: Measured using the COPD Self-Efficacy Scale (CSES), a 30-item instrument scored on a 5-point Likert scale (1 = not at all confident to 5 = very confident), yielding total scores from 30 to 150. Higher scores reflect greater self-efficacy for managing COPD-related challenges.23
- Pulmonary Rehabilitation Adherence: Evaluated through a self-reported rehabilitation diary card, rated on a 3-point scale: 3 = full adherence (≥ 70% completion of prescribed exercises), 2 = partial adherence (40–70% completion), and 1 = nonadherence (< 40% completion).
Secondary Outcomes
- Pulmonary Function: FEV1 as a percentage of the predicted value (FEV1% predicted) was measured using a calibrated portable spirometer (MasterScreen PFT, Vyaire Medical) in accordance with American Thoracic Society/European Respiratory Society standards.24
- Quality of Life: Evaluated using the COPD Assessment Test (CAT), an 8-item patient-reported outcome measure scored 0 to 40. Lower scores indicate less disease impact: 0–10 (low impact), 11–20 (medium impact), 21–30 (high impact), and 31–40 (very high impact).25
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 (IBM Corp, Armonk, NY). Continuous variables were expressed as mean ± standard deviation (SD) and analyzed using independent-samples t-tests for between-group comparisons at each time point, with Levene’s test for equality of variances performed to verify homogeneity assumptions. Categorical variables were presented as frequencies and percentages and compared using the chi-square test or Fisher exact test as appropriate. Within-group changes over time were assessed using repeated-measures analysis of variance with Bonferroni correction applied for multiple pairwise comparisons. All statistical tests were two-tailed, and a P value less than 0.05 was considered statistically significant. Ninety-five percent confidence intervals (CIs) were calculated for all between-group mean differences. Effect sizes were calculated using Cohen’s d for between-group comparisons; values of 0.2, 0.5, and 0.8 were considered small, medium, and large, respectively. No participants were lost to follow-up and no missing data handling was required. Data are reported to two decimal places and P values to three decimal places.
Results
Baseline Characteristics
Table 1 presents the demographic and clinical characteristics of the 94 participants. The mean age was 64.77 ± 7.14 years in the control group and 66.66 ± 6.37 years in the intervention group (P = 0.176). The majority of participants were male (control: 80.85%; intervention: 61.70%). Disease duration averaged 9.30 ± 4.18 years in the control group and 10.64 ± 4.65 years in the intervention group (P = 0.143). The distribution of GOLD stages was comparable between groups (control: stage II 48.94%, stage III 51.06%; intervention: stage II 59.57%, stage III 40.43%; P = 0.296). No statistically significant differences were observed between groups for any baseline demographic or clinical variable (all P > 0.05), confirming the comparability of the two cohorts at study entry (Table 1).
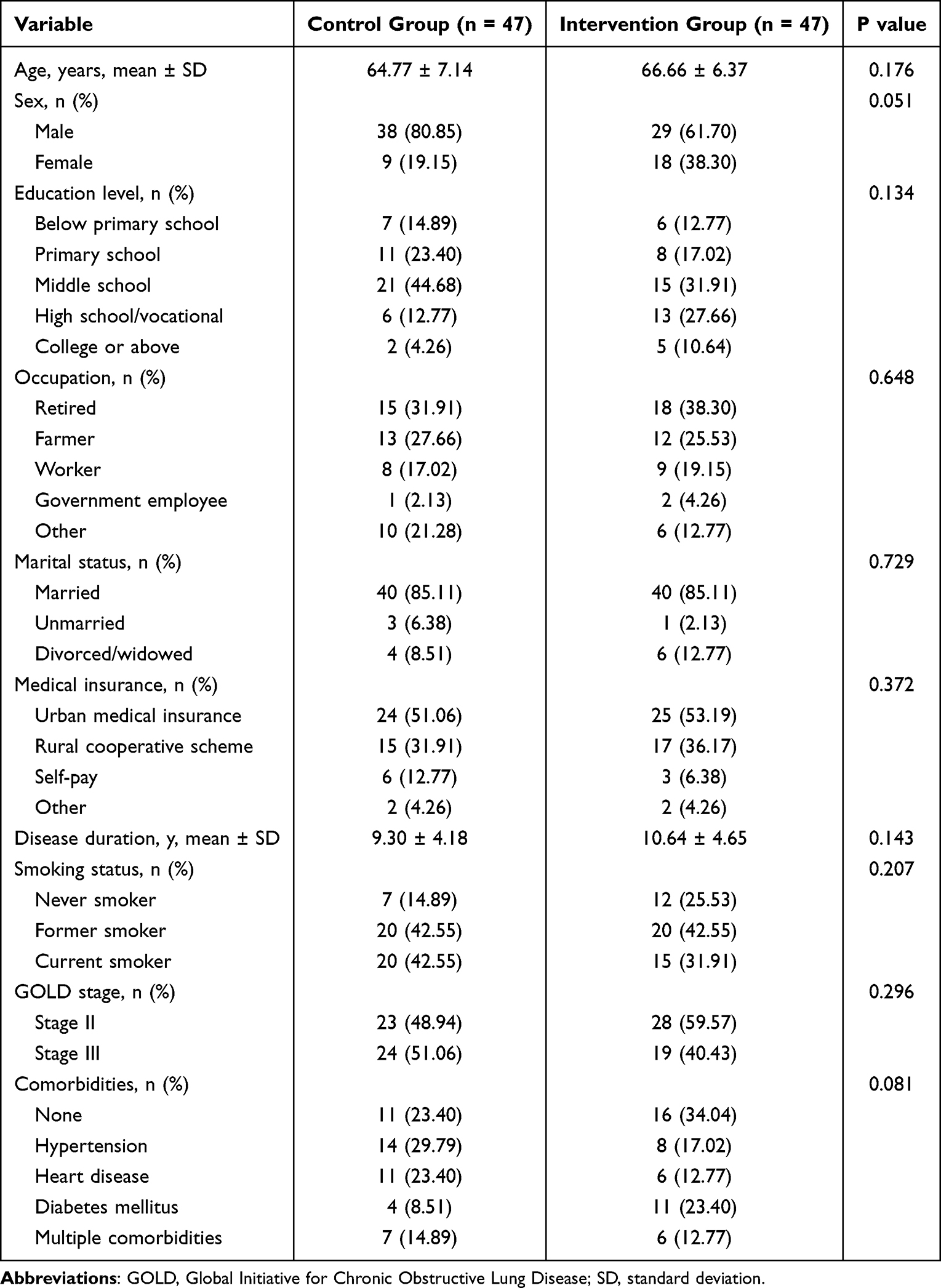 |
Table 1 Baseline Demographic and Clinical Characteristics of Study Participants |
Baseline outcome measures were similarly balanced: COPD knowledge scores (control 12.62 ± 2.53 vs intervention 13.06 ± 2.79; P = 0.313), self-efficacy scores (control 79.83 ± 7.48 vs intervention 78.87 ± 7.68; P = 0.434), PR adherence (control 1.94 ± 0.67 vs intervention 2.02 ± 0.71; P = 0.311), FEV1% predicted (control 51.88 ± 13.56 vs intervention 56.23 ± 13.62; P = 0.537), and CAT scores (control 21.70 ± 3.43 vs intervention 21.19 ± 3.52; P = 0.491).
COPD Knowledge
At 3 months, COPD knowledge scores in the intervention group increased to 21.30 ± 3.19, significantly exceeding the control group score of 15.87 ± 2.89 (mean difference 5.43; 95% CI 4.20–6.66; t = 3.12; P = 0.015; Cohen’s d = 1.79). This divergence widened at 6 months, with the intervention group achieving a mean score of 26.51 ± 3.37 compared with 17.96 ± 2.96 in the control group (mean difference 8.55; 95% CI 7.27–9.83; t = 2.84; P = 0.014; Cohen’s d = 2.70). The intervention group demonstrated a 102.99% improvement from baseline to 6 months, compared with 42.32% in the control group (Tables 2, 3, and Figure 2A).
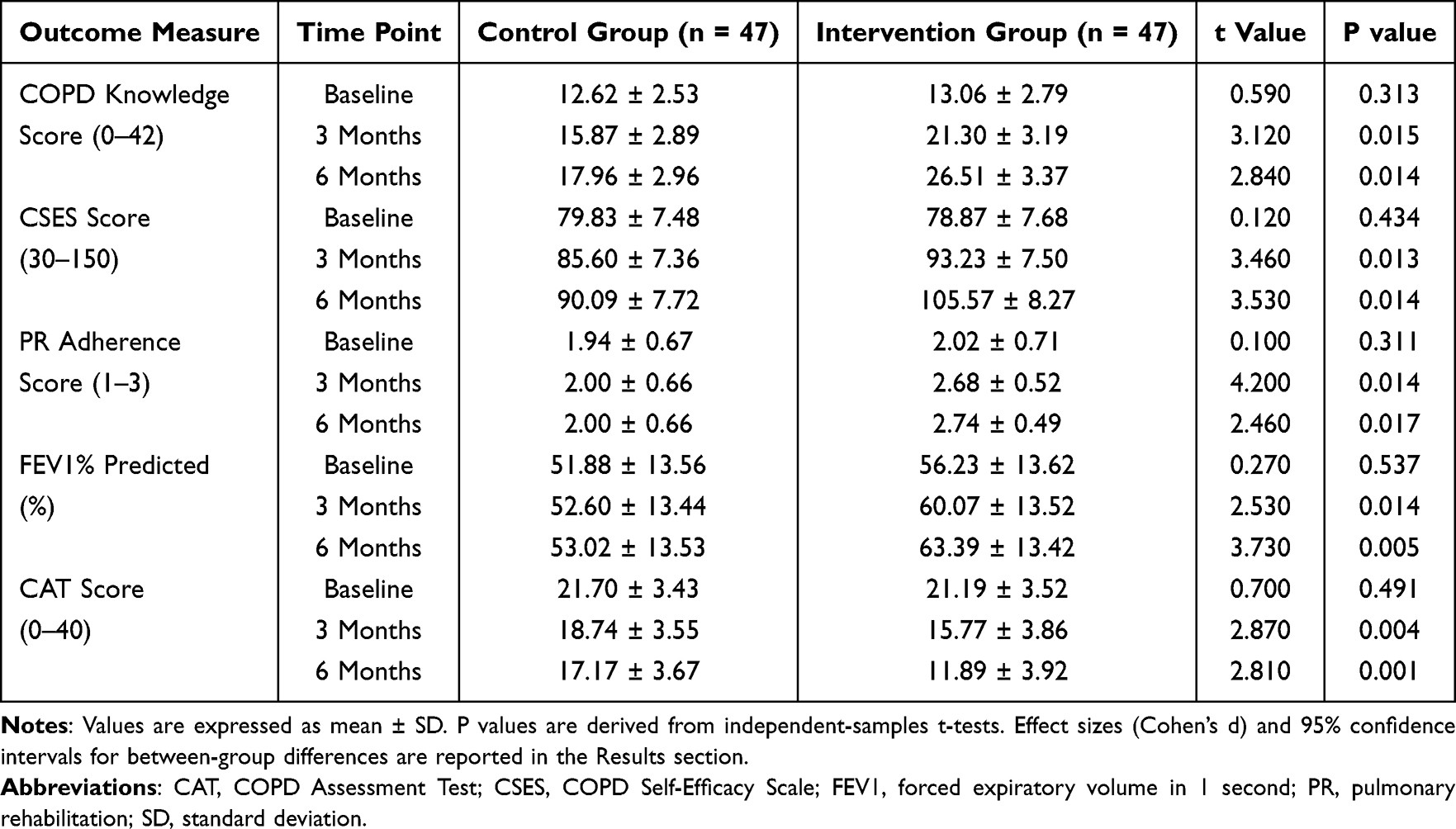 |
Table 2 Comparison of Outcome Measures Between Groups at Baseline, 3 Months, and 6 Months |
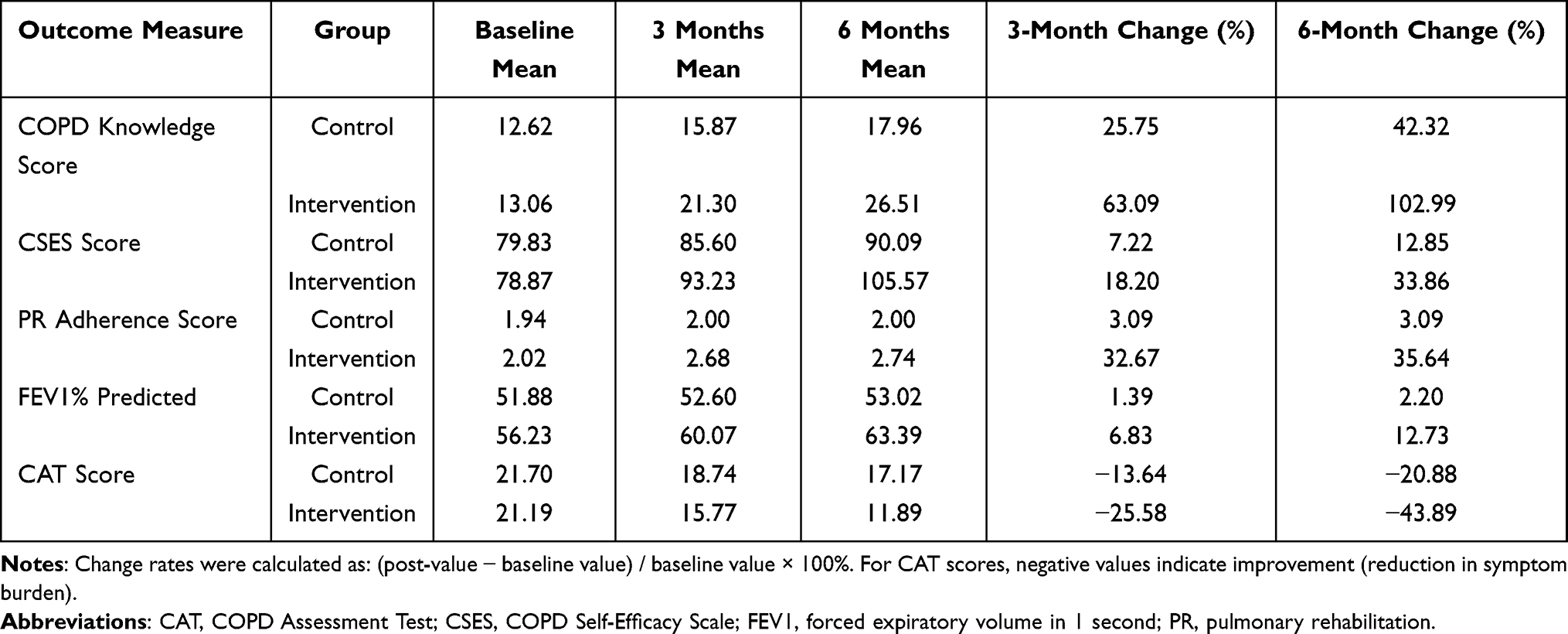 |
Table 3 Change Rates of Outcome Measures from Baseline to 3 Months and 6 Months |
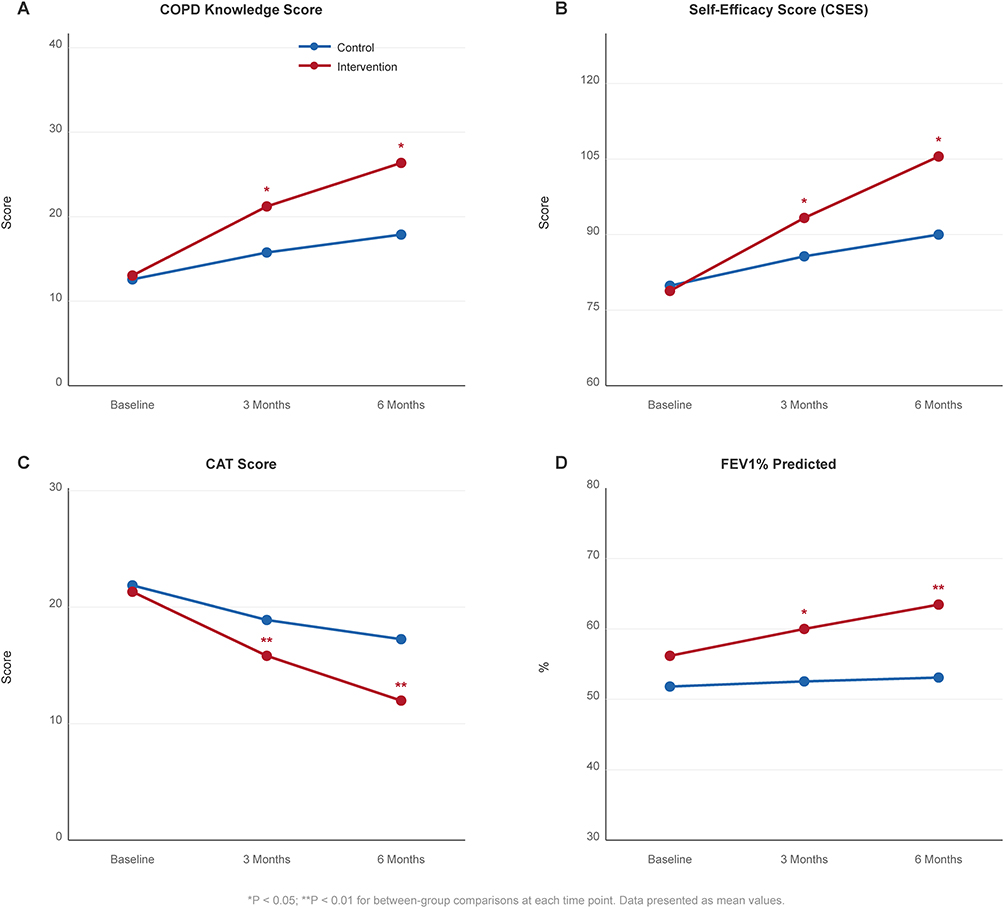 |
Figure 2 Trends in outcome measures over the 6-month study period. (A) COPD knowledge scores. (B) Self-efficacy scores measured by the COPD Self-Efficacy Scale. (C) COPD Assessment Test (CAT) scores. (D) FEV1% predicted values. Data are presented as mean ± standard deviation. Blue lines represent the control group; red lines represent the intervention group. *P < 0.05; **P < 0.01 for between-group comparisons. |
Self-Efficacy
Self-efficacy scores followed a parallel trajectory. No significant intergroup difference was detected at baseline (P = 0.434). By 3 months, the intervention group mean (93.23 ± 7.50) significantly surpassed that of the control group (85.60 ± 7.36; mean difference 7.63; 95% CI 4.63–10.63; t = 3.46; P = 0.013; Cohen’s d = 1.03). At 6 months, this gap expanded further (intervention 105.57 ± 8.27 vs control 90.09 ± 7.72; mean difference 15.48; 95% CI 12.25–18.71; t = 3.53; P = 0.014; Cohen’s d = 1.94), representing a 33.86% increase from baseline in the intervention group versus 12.85% in the control group (Tables 2, 3 and Figure 2B).
Quality of Life (CAT Scores)
CAT scores decreased in both groups over time, but the magnitude of improvement was substantially greater in the intervention group. At 3 months, the intervention group scored 15.77 ± 3.86 compared with 18.74 ± 3.55 in the control group (mean difference −2.97; 95% CI −4.47 to −1.47; t = 2.87; P = 0.004; Cohen’s d = 0.80). At 6 months, the intervention group achieved a mean CAT score of 11.89 ± 3.92 versus 17.17 ± 3.67 in the control group (mean difference −5.28; 95% CI −6.81 to −3.75; t = 2.81; P = 0.001; Cohen’s d = 1.39). Both groups transitioned from high-impact (baseline ≥21) to medium-impact status by 6 months; however, the intervention group’s 43.89% reduction in symptom burden substantially exceeded the control group’s 20.88% reduction, and the between-group difference exceeded the MCID of 2 CAT points at both follow-up timepoints, confirming clinical significance (Tables 2, 3 and Figure 2C).
Pulmonary Function
FEV1% predicted values were comparable at baseline (P = 0.537). At 3 months, the intervention group demonstrated a modest but statistically significant improvement (60.07 ± 13.52 vs 52.60 ± 13.44; mean difference 7.47; 95% CI 2.02–12.92; t = 2.53; P = 0.014; Cohen’s d = 0.55). By 6 months, the intergroup difference became more pronounced (intervention 63.39 ± 13.42 vs control 53.02 ± 13.53; mean difference 10.37; 95% CI 4.92–15.82; t = 3.73; P = 0.005; Cohen’s d = 0.77). The intervention group exhibited a 12.73% improvement in FEV1% predicted from baseline, contrasting with only 2.20% in the control group. As nonpharmacological interventions in established COPD typically produce modest spirometric changes, the observed improvement likely reflects optimization of airway clearance and respiratory muscle training rather than disease modification (Tables 2, 3 and Figure 2D).
Pulmonary Rehabilitation Adherence
Baseline adherence scores were comparable between groups (P = 0.311). At 3 months, the intervention group achieved a significantly higher mean adherence score (2.68 ± 0.52) than the control group (2.00 ± 0.66; mean difference 0.68; 95% CI 0.44–0.92; t = 4.20; P = 0.014; Cohen’s d = 1.14). This improvement was sustained at 6 months (intervention 2.74 ± 0.49 vs control 2.00 ± 0.66; mean difference 0.74; 95% CI 0.50–0.97; t = 2.46; P = 0.017; Cohen’s d = 1.27). The control group adherence score remained essentially unchanged from baseline (1.94 to 2.00), whereas the intervention group showed a 35.64% improvement (Tables 2, 3 and Figure 3).
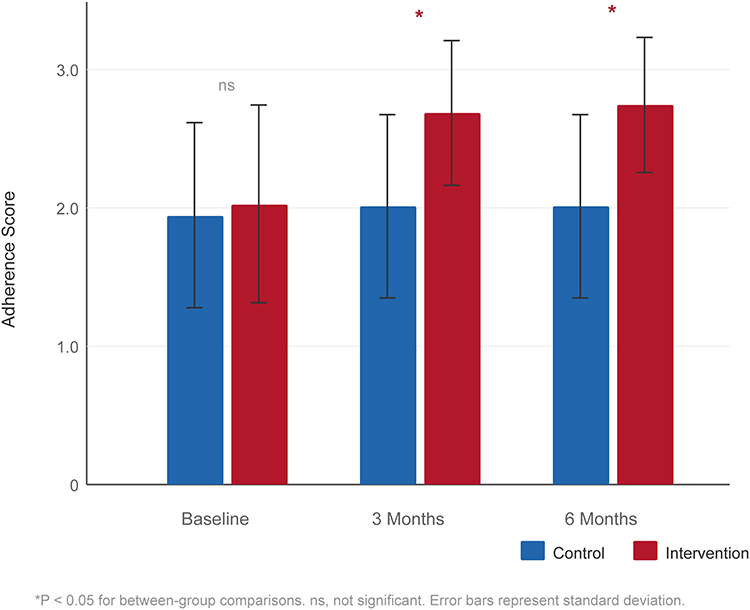 |
Figure 3 Pulmonary rehabilitation adherence scores at baseline, 3 months, and 6 months. Blue bars represent the control group; red bars represent the intervention group. Error bars indicate standard deviation. *P < 0.05 for between-group comparisons; ns, not significant. |
Discussion
This quasi-experimental study provides evidence suggesting that an internet-based 4C nursing model is associated with significant improvements across multiple dimensions of COPD pulmonary rehabilitation outcomes, including disease knowledge, self-efficacy, rehabilitation adherence, pulmonary function, and health-related quality of life over a 6-month follow-up period. To our knowledge, this is among the first studies to integrate the 4C nursing framework with internet-based delivery platforms specifically for COPD pulmonary rehabilitation, addressing a critical gap in the literature on theory-driven digital health interventions for chronic respiratory disease management.
The most striking finding was the marked improvement in COPD knowledge in the intervention group, with a 103% increase from baseline at 6 months compared with 42% in the control group. This magnitude of improvement aligns with contemporary evidence emphasizing that structured, multimodal health education—particularly when reinforced through digital platforms—can achieve substantially greater knowledge gains than traditional didactic approaches.22,26 The persistent WeChat-based health education push notifications, coupled with interactive video sessions, likely contributed to this outcome by providing repeated exposure to disease-specific information in accessible formats. These findings are consistent with a cross-sectional study by Jiang et al,16 which demonstrated that digital health literacy proficiency among older adults with COPD was associated with superior disease knowledge retention and self-management capacity.
The improvement in self-efficacy observed in the intervention group (33.86% increase at 6 months) merits particular attention. Self-efficacy, defined as an individual’s confidence in their ability to execute behaviors necessary to produce specific outcomes, is recognized as a pivotal mediator of health behavior change in chronic disease management.23,27 The 4C model’s Collaboration component—specifically the establishment of a patient-family-provider digital community—may have enhanced self-efficacy through multiple mechanisms: vicarious learning from peers, verbal encouragement from healthcare providers, and mastery experiences facilitated by supervised rehabilitation exercises. This interpretation is consistent with Bandura’s social cognitive theory and resonates with recent findings by Federman et al,21 who reported that comprehensive, patient-centered self-management support programs improved self-efficacy in patients with COPD.
Rehabilitation adherence in the intervention group improved by 35.64% at 6 months, while the control group showed negligible change. This finding addresses one of the most persistent challenges in COPD management. Prior literature consistently documents that PR adherence declines precipitously following hospital discharge, with adherence rates as low as 10% at 6 months in conventional care settings.8,10 The sustained adherence observed in our intervention group likely reflects the synergistic effects of the 4C model’s four dimensions: Comprehensiveness ensured that rehabilitation plans were tailored to individual capabilities; Collaboration maintained social accountability through the WeChat community; Coordination provided multidisciplinary expertise to address evolving rehabilitation needs; and Continuity sustained the patient-provider relationship through regular video follow-up. These results substantiate recent systematic reviews concluding that telehealth-delivered PR with structured follow-up achieves adherence rates comparable to supervised center-based programs.12,28
The 12.73% improvement in FEV1% predicted in the intervention group warrants careful interpretation. While the between-group difference at 6 months was statistically significant (P = 0.005), it is well established that pharmacological and nonpharmacological interventions for COPD rarely produce substantial spirometric improvement in patients with established airflow limitation.7 Nevertheless, the magnitude of improvement observed in our study is clinically meaningful and consistent with findings from the American Thoracic Society clinical practice guideline on pulmonary rehabilitation, which reported modest but significant FEV1% improvements following comprehensive PR programs.5 The incorporation of advanced respiratory techniques—including ACBT and FET—alongside conventional breathing exercises may have contributed to the enhanced spirometric outcomes by optimizing airway clearance and respiratory muscle function.
The reduction in CAT scores in the intervention group (from 21.19 at baseline to 11.89 at 6 months) represents a clinically significant transition from “high impact” to “low-to-medium impact” disease status, exceeding the minimal clinically important difference (MCID) of 2 points for the CAT.25 This improvement was nearly double that observed in the control group (43.89% vs 20.88% reduction). The comprehensive nature of the 4C intervention—addressing not only physical rehabilitation but also psychological support, nutritional guidance, and social connectivity—likely contributed to this multidimensional improvement in quality of life. A randomized controlled trial by Zanaboni et al15 similarly demonstrated that long-term telerehabilitation achieved greater improvements in health status than unsupervised home training in patients with COPD, underscoring the value of sustained professional engagement in remote rehabilitation delivery.
Several mechanisms may underlie the observed benefits of the internet-based 4C nursing model. First, the digital platform transcended the temporal and spatial constraints of conventional follow-up, enabling continuous engagement that is not feasible through periodic outpatient visits alone.12 Second, the WeChat-based community created a sustained ecosystem of social support, peer motivation, and information exchange—elements identified as critical facilitators of long-term behavior change in chronic disease populations.16 Third, the multidisciplinary coordination embedded within the model ensured that patients received integrated, expert-informed care that addressed the heterogeneous phenotypic manifestations of COPD.17 Fourth, the structured progression from intensive biweekly video follow-up to monthly sessions reflected a graduated autonomy transfer consistent with self-management theory, potentially building patients’ confidence to independently sustain rehabilitation behaviors.27 Finally, the application of behavioral change theories within the 4C framework provided a theoretical foundation for sustained engagement, as recently articulated in a comprehensive review by Chen et al.11
This study has several limitations that should be acknowledged. First, the quasi-experimental design precludes definitive causal inference; the sequential enrollment approach minimizes contamination between groups but introduces risks of temporal confounding and selection bias that cannot be fully eliminated without randomization. Second, the absence of outcome assessor blinding and the use of an investigator-developed intervention may introduce performance bias and investigator-related bias, potentially inflating observed effect sizes. Third, the single-center design and restriction to Baoding municipality residents limit generalizability to other healthcare settings, patient populations, or geographic regions.15 Fourth, the 6-month follow-up period is insufficient to assess the long-term durability of intervention effects, particularly for physiological outcomes such as FEV1% predicted.8 Fifth, certain outcome measures—including PR adherence and COPD knowledge—rely on patient self-report and are subject to recall and social desirability biases; no independent verification of diary card entries was performed. Sixth, while the sample size was determined by a priori power calculations, the study may have been underpowered to detect smaller but clinically meaningful differences in secondary outcomes. Seventh, the use of WeChat as the delivery platform raises considerations regarding digital literacy and equitable access; patients with limited technological proficiency or internet connectivity may have experienced reduced benefit from digital components, which may have contributed to the uniformly positive outcomes observed. Finally, while patient data were managed according to institutional protocols, formal independent cybersecurity auditing of the digital communication channels was not conducted, which represents an important gap in telehealth research reporting.
Future research should address these limitations through multicenter randomized controlled trials with larger sample sizes and extended follow-up periods.6 Investigations into the cost-effectiveness of internet-based 4C nursing models would provide essential health economic data to inform policy decisions. Additionally, studies should examine the moderating effects of digital literacy and technology access on intervention outcomes, to identify patient subgroups requiring additional support or modified delivery approaches. Mediation and moderation analyses would help identify the active mechanisms of each 4C component. The integration of wearable biosensors and artificial intelligence-driven monitoring systems with the 4C framework represents a promising avenue for further enhancing personalization and real-time responsiveness.28
Conclusions
This quasi-experimental, single-center study found that an internet-based 4C nursing model was associated with clinically meaningful improvements in COPD-related knowledge, self-efficacy, pulmonary rehabilitation adherence, pulmonary function, and quality of life in patients with moderate-to-severe COPD over a 6-month follow-up period. By integrating the principles of Comprehensiveness, Collaboration, Coordination, and Continuity within accessible digital platforms, this model simultaneously addresses multiple barriers to sustained pulmonary rehabilitation engagement. These findings are preliminary and hypothesis-generating, supporting the feasibility and potential value of theory-driven, telehealth-enhanced nursing care for post-discharge COPD management. Confirmation through multicenter randomized controlled trials with longer follow-up and cost-effectiveness analyses is needed before broad clinical implementation can be recommended.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Baoding Rehabilitation Hospital (Approval number: 202302). All methods were carried out in accordance with the Declaration of Helsinki. All participants provided written informed consent prior to enrollment, including explicit information regarding the nature of the internet-based intervention, the use of WeChat for communication and follow-up, and relevant data privacy considerations. Patient data transmitted through WeChat were managed under the platform’s privacy settings, and all identifiable information was stored securely on institutional servers with access restricted to the research team. Participants were informed of their right to withdraw from the digital communication components at any time without affecting their routine clinical care.
Acknowledgments
The authors thank the nursing staff of the Department of Respiratory Medicine at Baoding Rehabilitation Hospital for their assistance with data collection and patient follow-up.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Project of Hebei Provincial Health Commission (No. 2341ZF225).
Disclosure
The authors declare no competing interests in this work.
References
1. Boers E, Barrett M, Su JG. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
2. Al Wachami N, Guennouni M, Iderdar Y. Estimating the global prevalence of chronic obstructive pulmonary disease (COPD): a systematic review and meta-analysis. BMC Public Health. 2024;24(1):297. doi:10.1186/s12889-024-17686-9
3. Li M, Chen H, Zhou N. Burden of COPD in China and the global from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. BMJ Open Respiratory Res. 2023;10(1):e001698. doi:10.1136/bmjresp-2023-001698
4. Wang Y, Han R, Ding X. Chronic obstructive pulmonary disease across three decades: trends, inequalities, and projections from the Global Burden of Disease Study 2021. Front Med. 2025;12:1564878. doi:10.3389/fmed.2025.1564878
5. Rochester CL, Alison JA, Carlin B. Pulmonary rehabilitation for adults with chronic respiratory disease: an official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2023;208(4):e7–13. doi:10.1164/rccm.202306-1066ST
6. Jenkins AR, Burtin C, Camp PG. Do pulmonary rehabilitation programmes improve outcomes in patients with COPD posthospital discharge for exacerbation: a systematic review and meta-analysis. Thorax. 2024;79(5):438–447. doi:10.1136/thorax-2023-220333
7. Singh D, Stockley R, Anzueto A. GOLD Science Committee recommendations for the use of pre- and post-bronchodilator spirometry for the diagnosis of COPD. Eur Respir J. 2025;65(2):2401603. doi:10.1183/13993003.01603-2024
8. Watson JS, Jordan RE, Gardiner L. A systematic review of the effectiveness of interventions to promote referral, adherence, and uptake of pulmonary rehabilitation for patients with chronic obstructive pulmonary disease. Int J Chronic Obstr. 2023;18:1637–1654. doi:10.2147/COPD.S396317
9. Moy ML. Maintenance pulmonary rehabilitation: an update and future directions. Respiratory Care. 2024;69(6):724–739. doi:10.4187/respcare.11609
10. Qin H, Jia P, Yan Q. Barriers and facilitators to pulmonary rehabilitation in COPD: a mixed-methods systematic review. BMC Pulm Med. 2025;25(1):314. doi:10.1186/s12890-025-03769-9
11. Chen Y, Tan R, Long X. Applying behavioral change theories to optimize pulmonary rehabilitation in COPD patients: a review. Medicine. 2024;103(22):e38366. doi:10.1097/MD.0000000000038366
12. Zhuang M, Hassan II, Ahmad W. Effectiveness of digital health interventions for chronic obstructive pulmonary disease: systematic review and meta-analysis. J Med Internet Res. 2025;27(1):e76323. doi:10.2196/76323
13. Zanaboni P, Dinesen B, Hoaas H. Long-term telerehabilitation or unsupervised training at home for patients with chronic obstructive pulmonary disease: a randomized controlled trial. Am J Respir Crit Care Med. 2023;207(7):865–875. doi:10.1164/rccm.202204-0643OC
14. Song CY, Liu X, Wang YQ. Effects of home-based telehealth on the physical condition and psychological status of patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Int J Nurs Pract. 2023;29(3):e13062. doi:10.1111/ijn.13062
15. Cox NS, Rawlings S, Lannin NA. Supporting delivery of remote pulmonary rehabilitation across different healthcare contexts: a multi-national study. Chron Respir Dis. 2024;21:14799731241290518. doi:10.1177/14799731241290518
16. Jiang Y, Gao J, Sun P. Factors associated with the e-health literacy among older adults with chronic obstructive pulmonary disease: a cross-sectional study. Telemed E-Health. 2024;30(4):e1138–e1147. doi:10.1089/tmj.2023.0394
17. Aranburu-Imatz A, Lopez-Carrasco JC, Moreno-Luque A. Nurse-led interventions in chronic obstructive pulmonary disease patients: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022;19(15):9101. doi:10.3390/ijerph19159101
18. Zhang J, Gu LL, Xu Y. Integrated medical care and the continuous 4C nursing model to improve nursing quality and clinical treatment of patients with acute stroke: based on a retrospective case-control study. Cont Media Mol Imag. 2022;2022:4810280. doi:10.1155/2022/4810280
19. Jimenez G, Matchar D, Koh GCH. Revisiting the four core functions (4Cs) of primary care: operational definitions and complexities. Primary Health Care Res Develop. 2021;22:e68. doi:10.1017/S1463423621000669
20. Wufuer A, Ma J, Ainiwa P. Influence of continuous 4C nursing on quality of life and self-care ability of patients with diabetes retinopathy: an observational study. Medicine. 2024;103(20):e37920. doi:10.1097/MD.0000000000037920
21. Federman AD, O’Conor R, Nnemnbeng J. Feasibility trial of a comprehensive, highly patient-centered COPD self-management support program. Chron Obstructive Pulm Dis. 2024;11(1):13–25. doi:10.15326/jcopdf.2023.0419
22. Borge CR, Larsen MH, Osborne RH. Impacts of a health literacy-informed intervention in people with chronic obstructive pulmonary disease (COPD) on hospitalization, health literacy, self-management, quality of life, and health costs - a randomized controlled trial. Patient Educ Couns. 2024;123:108220. doi:10.1016/j.pec.2024.108220
23. Ceyhan Y, Aydin C. Impact of COPD stage on self management with COPD patients: the mediating role of symptoms management. J Clin Nurs. 2024;33(9):3615–3623. doi:10.1111/jocn.17119
24. Wilkinson JD, Wilhalme H, Cooper CB. Duration and frequency of spirometry needed to accurately reflect annualized change of FEV1 in chronic obstructive pulmonary disease. Ann Am Thoracic Soc. 2024;21(12):1706–1714. doi:10.1513/AnnalsATS.202401-099OC
25. Jones P, Soutome T, Matsuki T. Health status progression measured using weekly telemonitoring of COPD Assessment Test scores over 1 year and its association with COPD exacerbations. Chron Obstructive Pulm Dis. 2024;11(2):144–154. doi:10.15326/jcopdf.2023.0415
26. Clifton H, Welch L, Ewings S. Health literacy levels of patients with chronic obstructive pulmonary disease: a cross-sectional study. Br J Nurs. 2024;33(21):1016–1025. doi:10.12968/bjon.2023.0230
27. Pollard SL, Siddharthan T, Hossen S. Chronic obstructive pulmonary disease self-management in three low- and middle-income countries: a pilot randomized trial. Am J Respir Crit Care Med. 2023;208(10):1052–1062. doi:10.1164/rccm.202303-0505OC
28. Qi J, Cai Q, Zhang W. Effects of pulmonary telerehabilitation in patients with chronic obstructive pulmonary disease. Chinese Med J. 2025;138(12):1493–1495. doi:10.1097/CM9.0000000000003650
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:881-893
Published Date: 15 May 2023
Development of a Pulmonary Rehabilitation Patient Decision Aid for Patients with Chronic Obstructive Pulmonary Disease: Mixed Methods Study
Jiang Y, Guo J, Chen M, Zou X, Sun P, Gao J, Nuerdawulieti B, Wang S
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1377-1389
Published Date: 12 July 2023
Effects of Home-Based Training with Internet Telehealth Guidance in COPD Patients Entering Pulmonary Rehabilitation: A Systematic Review
Hartman M, Mináriková J, Batalik L, Pepera G, Su JJ, Formiga MF, Cahalin L, Dosbaba F
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2305-2319
Published Date: 19 October 2023
Addressing Barriers to Chronic Obstructive Pulmonary Disease (COPD) Care: Three Innovative Evidence-Based Approaches: A Review
Siu DCH, Gafni-Lachter L
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:331-341
Published Date: 1 February 2024
Exercise Prescription Training in Chronic Obstructive Pulmonary Disease: Benefits and Mechanisms
Liu S, Yang A, Yu Y, Xu B, Yu G, Wang H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1071-1082
Published Date: 15 April 2025