Back to Journals » International Journal of General Medicine » Volume 18
Effect of Recombinant Human Brain Natriuretic Peptide Therapy After PCI in Patients with Acute Myocardial Infarction and Its Impact on Cardiac Function: A Retrospective Controlled Study
Authors Yu H, Li N, Li J, Zhu J
Received 8 July 2025
Accepted for publication 26 October 2025
Published 4 November 2025 Volume 2025:18 Pages 6651—6659
DOI https://doi.org/10.2147/IJGM.S552471
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Hongbo Yu,1 Nannan Li,2 Jie Li,3 Jie Zhu4
1Department of Cardiovascular Medicine II, Qinhuangdao Hospital of Dongfang Hospital, Beijing University of Chinese Medicine (Qinhuangdao Hospital of Traditional Chinese Medicine), Qinhuangdao, Hebei, 066000, People’s Republic of China; 2Department of Cardiology, Dongying District People’s Hospital, Dongying, Shandong, People’s Republic of China; 3Department of Cardiology, The Fifth People’s Hospital of Dongying, Dongying, Shandong, People’s Republic of China; 4Department of Cardiovascular Diseases, Hengshui Hospital of Traditional Chinese Medicine, Hengshui, Hebei, 053000, People’s Republic of China
Correspondence: Jie Zhu, Email [email protected]
Objective: To investigate the efficacy of recombinant human brain natriuretic peptide (rhBNP) therapy after percutaneous coronary intervention (PCI) in patients with acute myocardial infarction (AMI) and its impact on cardiac function.
Methods: In this retrospective controlled study, 104 AMI patients who underwent PCI at our hospital between September 2021 and December 2024 were consecutively enrolled and assigned to groups based on the treatment period. The control group (n=52) (patients admitted from September 2021 to December 2022) received standard guideline-directed medical therapy (GDMT), while the observation group (n=52) (patients admitted from January 2023 to December 2024) received additional intravenous rhBNP treatment for 72 hours on top of GDMT. The therapeutic effects, cardiac ultrasound parameters (LVEF, LVEDD, LVESD, FS), key myocardial injury markers (CK-MB, cTnI), inflammatory markers (IL-6, TNF-α, Hcy), and major adverse cardiovascular events (MACE) incidence were compared. Multivariate regression analyses were performed to adjust for potential baseline confounders.
Results: The observation group demonstrated a significantly higher overall efficacy than the control group (94.23% vs 78.85%, P< 0.05). Post-treatment, both groups showed significant improvements in LVEF, FS, LVESD, and reductions in CK-MB, cTnI, IL-6, TNF-α, and Hcy, with the observation group exhibiting more pronounced benefits (P< 0.05). The between-group differences remained significant after adjusting for baseline characteristics. The incidence of MACE during the 6-month follow-up was significantly lower in the observation group (5.77% vs 19.23%, P< 0.05).
Conclusion: Adjunctive rhBNP therapy after PCI in AMI patients provides significant clinical benefits, including enhanced improvement of cardiac function, reduced myocardial injury and inflammatory stress, and a lower risk of MACE. However, these findings should be interpreted considering the study’s limitations, including its retrospective design and single-center nature. Future prospective randomized trials are warranted for confirmation.
Keywords: acute myocardial infarction, PCI, recombinant human brain natriuretic peptide, efficacy, cardiac function, MACE
Introduction
Acute myocardial infarction (AMI) refers to a clinical syndrome characterized by irreversible myocardial cell necrosis caused by acute and persistent ischemia and hypoxia of the coronary arteries. It is one of the most critical clinical types of coronary heart disease.1 With global population aging and changes in lifestyle, the incidence of AMI continues to rise, seriously threatening patients’ lives and quality of life.2,3 Percutaneous coronary intervention (PCI), the preferred treatment for AMI, can promptly reopen occluded coronary vessels, restore myocardial perfusion, and significantly reduce early mortality and complication rates, and has been widely used in clinical practice.4 However, despite PCI significantly improving short-term outcomes in AMI patients, challenges remain after the procedure, including myocardial reperfusion injury, worsening cardiac function, ventricular remodeling, and activation of inflammatory responses.5 Reperfusion injury can lead to calcium overload, oxidative stress, release of inflammatory factors, and other pathophysiological reactions, exacerbating myocardial cell apoptosis and necrosis, thus affecting left ventricular remodeling and long-term cardiac function recovery.6,7 Therefore, in addition to effective revascularization, how to further reduce myocardial damage, improve cardiac function, and optimize long-term outcomes has become a key and challenging issue in peri-PCI management of AMI.
Recombinant human brain natriuretic peptide (rhBNP) is a recombinant polypeptide drug with the same amino acid sequence as endogenous brain natriuretic peptide (BNP). BNP is mainly synthesized and secreted by ventricular cardiomyocytes and plays a vital role in maintaining cardiovascular homeostasis through its natriuretic, diuretic, vasodilatory, sympathetic-inhibiting, and anti-fibrotic effects.8,9 Since its introduction, rhBNP has been widely recognized in the treatment of acute and chronic heart failure, demonstrating good cardioprotective effects by relieving pre- and after-load, improving ventricular compliance, and reducing myocardial oxygen consumption.10,11 In addition, some studies12 suggest that rhBNP can inhibit ventricular remodeling, improve myocardial microcirculation, reduce biomarkers of myocardial cell injury, and exert certain anti-inflammatory effects. Therefore, it is considered potentially beneficial for cardiac function recovery after PCI in AMI patients. A limited number of clinical studies have explored the application of rhBNP in the AMI setting. For instance, some small-scale randomized trials have suggested potential benefits of rhBNP in improving hemodynamics and reducing infarct size in ST-segment elevation myocardial infarction (STEMI) patients.13,14 However, other investigations have reported neutral findings regarding its impact on hard clinical endpoints, and the evidence specifically focusing on its adjunctive use immediately after PCI remains inconclusive and relatively scarce.15 This lack of consensus highlights the need for further investigation.
However, clinical studies on the combined use of rhBNP in AMI patients after PCI remain relatively limited, and its specific therapeutic effects on cardiac function, myocardial injury, and inflammatory responses are still under debate. Consequently, there is a clear gap in evidence regarding the comprehensive evaluation of rhBNP’s effects on multi-dimensional outcomes including cardiac function parameters, biomarker profiles, and inflammatory stress in a real-world PCI cohort. Hence, further exploration of the clinical value of rhBNP as adjuvant therapy after PCI is of significant importance. Based on the above considerations, this study retrospectively analyzed clinical data from 104 AMI patients who underwent PCI in our hospital. It aimed to assess the practical efficacy of rhBNP as an adjuvant therapy postoperatively and to provide more reliable theoretical support and practical reference for the comprehensive management of AMI patients after intervention.
Materials and Methods
Study Subjects
This study was a single-center, retrospective controlled study. A total of 104 patients with AMI who underwent PCI at Qinhuangdao Hospital of Traditional Chinese Medicine from September 2021 to December 2024 were consecutively enrolled. The assignment to groups was based on the temporal sequence of admission and a shift in clinical practice. Specifically, patients admitted from September 2021 to December 2022 constituted the control group (n=52), reflecting the standard care prior to the increased use of rhBNP at our institution. Patients admitted from January 2023 to December 2024, during which period adjunctive rhBNP therapy was more routinely considered for eligible AMI patients post-PCI, constituted the observation group (n=52).
All patients met the diagnostic criteria for AMI outlined in the 2023 European Society of Cardiology (ESC) Guidelines for the Management of Acute Coronary Syndromes (ACS)16 and underwent coronary angiography and PCI during the index hospitalization. The inclusion criteria were: (1) Age 18–80 years; (2) Underwent emergency PCI within 12 hours of symptom onset; (3) Initiated the study medication regimen within 48 hours after PCI; (4) Complete clinical data, including cardiac ultrasound and laboratory test results. The exclusion criteria were: (1) Severe hepatic (Child-Pugh class C) or renal insufficiency (eGFR < 30 mL/min/1.73m2) or active malignancy; (2) Active systemic infection, rheumatic autoimmune disease, or other chronic inflammatory states; (3) Cardiogenic shock or mechanical complications (eg, ventricular septal rupture); (4) Severe valvular heart disease, congenital heart disease, or life-threatening arrhythmias; (5) Known hypersensitivity or contraindication to any study drug; (6) Pregnancy or lactation.
This study was approved by the Ethics Committee of Qinhuangdao Hospital of Traditional Chinese Medicine (Approval No. XNWKYLC2408). Written informed consent was obtained from all participants, and the study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Treatment Methods
All patients received standardized guideline-directed medical therapy (GDMT) after PCI, in accordance with contemporary guidelines.14 The standard regimen included:
Antiplatelet Therapy
Dual antiplatelet therapy with aspirin enteric-coated tablets (100 mg/d, Bayer Healthcare Co., Ltd., NMPA Approval No. J20130089) combined with either clopidogrel tablets (75 mg/d, Sanofi Pharmaceutical Co., Ltd., NMPA No. H20000673) or ticagrelor tablets (90 mg twice daily, AstraZeneca, NMPA No. H20130069), chosen based on ischemic/bleeding risk profile.
Statin Therapy
High-intensity statin therapy with atorvastatin calcium tablets (20–40 mg/d, Pfizer Inc., NMPA No. H20051408) initiated within 24 hours.
Beta-Blockers
Metoprolol sustained-release tablets were initiated or up-titrated as tolerated, starting at 47.5 mg/d, with a target dose of 95–190 mg/d (AstraZeneca, NMPA No. H20191031), contingent on heart rate (>50 bpm) and systolic blood pressure (>100 mmHg).
RAAS Inhibitors
An ACEI (eg, perindopril tablets, starting at 4 mg/d, Sanofi, NMPA No. H20040106) or ARB (eg, valsartan capsules, starting at 80 mg/d, Novartis, NMPA No. H20040210) was initiated within 24 hours and titrated to the maximum tolerated dose based on blood pressure and renal function.
Symptomatic Support
Intravenous furosemide (20–40 mg, Jiangsu Hengrui Pharmaceuticals Co., Ltd., NMPA No. H32021056) for volume overload or intravenous nitroglycerin injection (5 mg/ampoule, Tianjin Jinyao Group, NMPA No. H12020558) for persistent angina, as clinically required.
In addition to the above standard therapy, the observation group received intravenous recombinant human brain natriuretic peptide (rhBNP; trade name: Xinhuosu, Shenzhen Tai Kang Biological Products Co., Ltd., NMPA No. S20050036) initiated within 24 hours post-PCI. The administration followed a standardized protocol: an intravenous bolus of 1.5 μg/kg over 90 seconds, followed by a continuous infusion of 0.0075–0.01 μg·kg−1·min−1 for 72 hours. Vital signs, urine output, and adverse events were closely monitored.
Observation Indicators
Therapeutic Efficacy
After 4 weeks of treatment, efficacy was evaluated based on symptom relief, improvement in cardiac function, and ECG changes, and classified as follows: Markedly effective: significant chest pain relief, LVEF increased ≥10%, ECG nearly normal; Effective: symptom relief, LVEF increased 5–10%, partial ST-segment recovery; Ineffective: no improvement or worsening of symptoms, LVEF increased <5%, no significant ECG changes. Total effective rate = (markedly effective + effective) / total cases × 100%.
Cardiac Ultrasound Indices
Before and after treatment, cardiac color Doppler ultrasound (Philips IE33 model) was used to measure LVEF, LVEDD, LVESD, and FS levels.
Myocardial Injury Biomarkers
Before and after treatment, 5 mL of fasting cubital venous blood was collected in the morning. CK-MB, cTnT, cTnI, and H-FABP levels were measured using ELISA.
Inflammatory Stress Indicators
Before and after treatment, residual serum samples were used to measure IL-6, IL-8, and TNF-α levels using ELISA, and Hcy levels were measured using radioimmunoassay.
Follow-Up and MACE Monitoring
All patients were followed for 6 months postoperatively. Major adverse cardiovascular events (MACE) were assessed, including cardiac death, recurrent myocardial infarction, recurrent angina, recurrent heart failure, in-stent thrombosis, and target vessel revascularization.
Statistical Methods
Data were analyzed using SPSS 26.0. Continuous data with normal distribution are presented as mean ± standard deviation (mean ± sd)). Between-group comparisons used independent samples t-tests, and within-group pre-post comparisons used paired t-tests. Categorical data are presented as n (%) and were compared using the χ2 test or Fisher’s exact test. To account for potential baseline confounding, analysis of covariance (ANCOVA) was employed for continuous outcomes, adjusting for baseline values, age, and infarct location. For the MACE outcome, a multivariable Cox proportional hazards regression model was used, adjusting for key covariates including age, gender, history of diabetes, baseline LVEF, and multi-vessel disease. A two-sided P-value < 0.05 was considered statistically significant.
Results
Comparison of Baseline Data
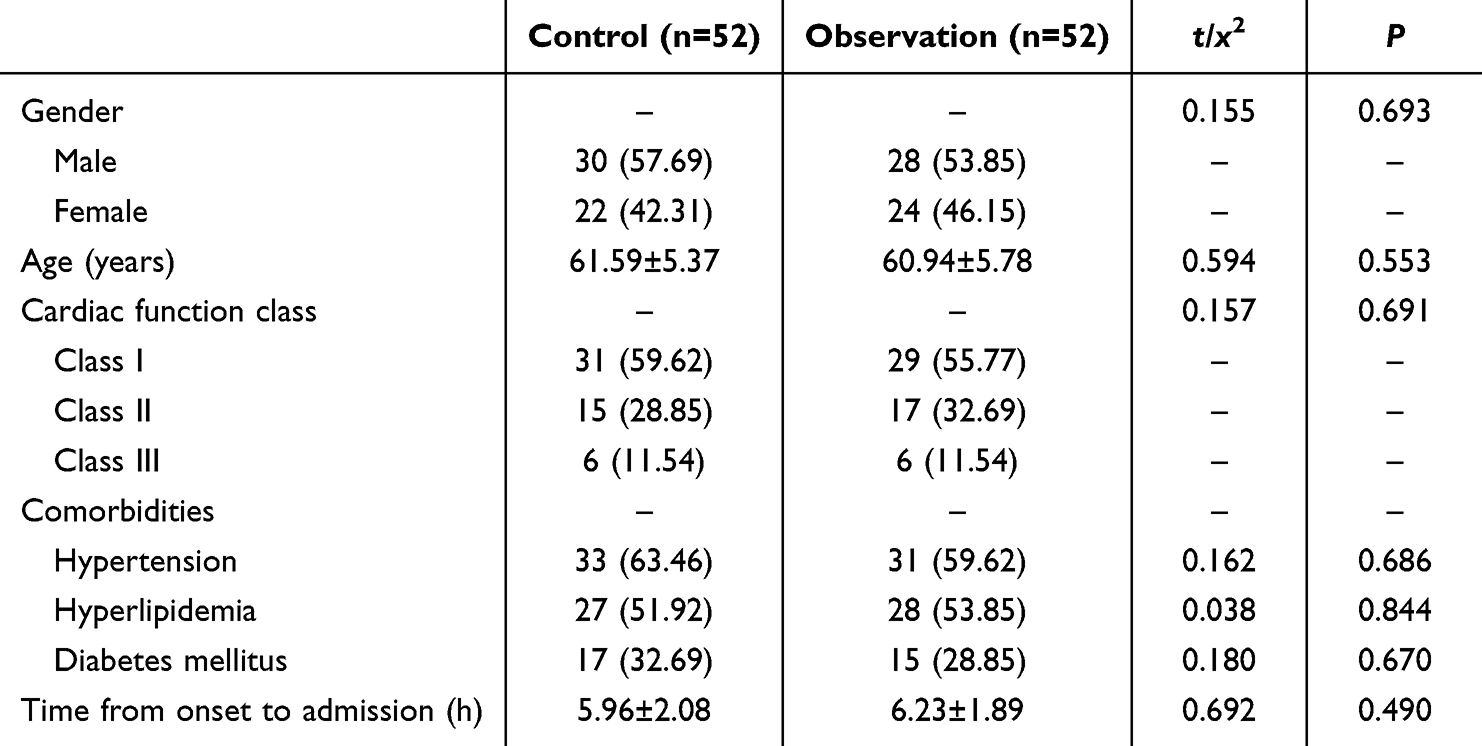
There were no statistically significant differences between the two groups in terms of gender, age, cardiac function classification, comorbidities, and time from onset to admission (P>0.05), indicating comparability. See Table 1.
 |

Comparison of Therapeutic Effects
After treatment, the observation group showed significantly better overall efficacy compared to the control group (total effective rate: 94.23% vs 78.85%, P<0.05), as shown in Table 2.
 |
Table 2 Comparison of Therapeutic Effects [n (%)] |
Comparison of Echocardiographic Parameters
After treatment, both groups showed significant increases in LVEF, LVEDD, and FS, and a significant decrease in LVESD. The improvement was more pronounced in the observation group (P<0.05), see Figure 1.
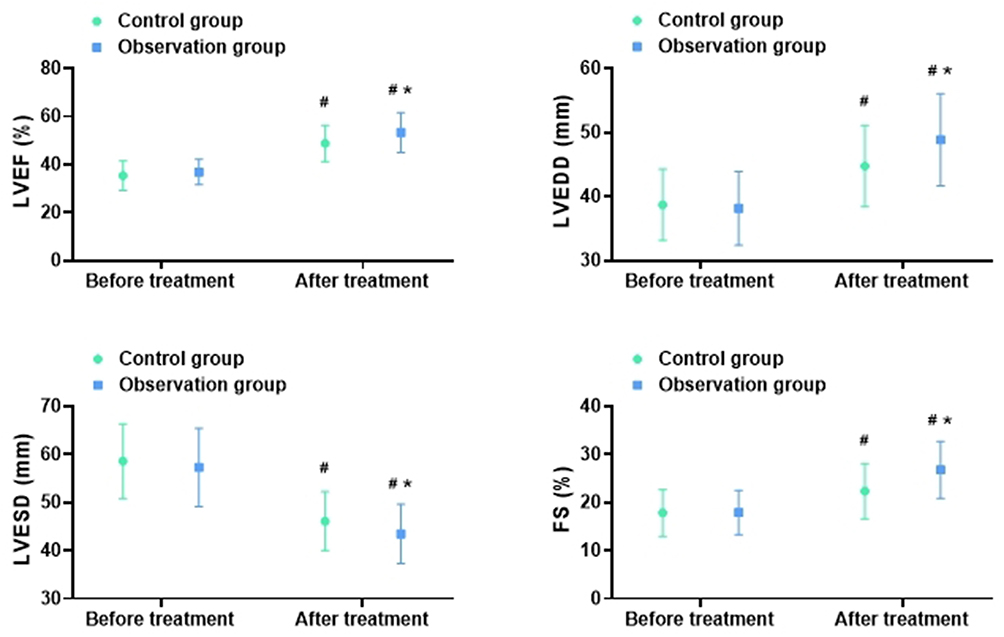 |
Figure 1 Comparison of Echocardiographic Parameters (Mean ± SD). Notes: #P < 0.05 vs pre-treatment within the same group. *P < 0.05 for between-group comparison after adjustment for baseline, age, and infarct location (ANCOVA). |
Comparison of Myocardial Injury Markers
After treatment, both groups exhibited significantly reduced levels of CK-MB, cTnT, cTnI, and H-FABP compared to before treatment, with greater reductions observed in the observation group (P<0.05), see Figure 2.
 |
Figure 2 Comparison of Myocardial Injury Markers (Mean ± SD). Notes: #P < 0.05 vs pre-treatment within the same group. *P < 0.05 for between-group comparison after adjustment for baseline, age, and infarct location (ANCOVA). |
Comparison of Inflammatory Stress Markers
After treatment, IL-6, IL-8, TNF-α, and Hcy levels significantly decreased in both groups compared to pre-treatment levels, with more substantial improvements observed in the observation group (P<0.05), see Figure 3.
 |
Figure 3 Comparison of Inflammatory Stress Markers (Mean ± SD). Notes: #P < 0.05 vs pre-treatment within the same group. *P < 0.05 for between-group comparison after adjustment for baseline, age, and infarct location (ANCOVA). |
Comparison of MACE Incidence
During the 6-month postoperative follow-up, the observation group had a significantly lower incidence of MACE compared to the control group (5.77% vs 19.23%, P<0.05). To further validate this finding, a multivariable Cox proportional hazards regression model was employed, adjusting for age, gender, history of diabetes, baseline LVEF, and multi-vessel disease. This adjusted analysis confirmed that patients in the observation group had a significantly lower risk of MACE compared to the control group (Hazard Ratio [HR] = 0.28, 95% Confidence Interval [CI]: 0.08–0.99, P = 0.048), see Table 3.
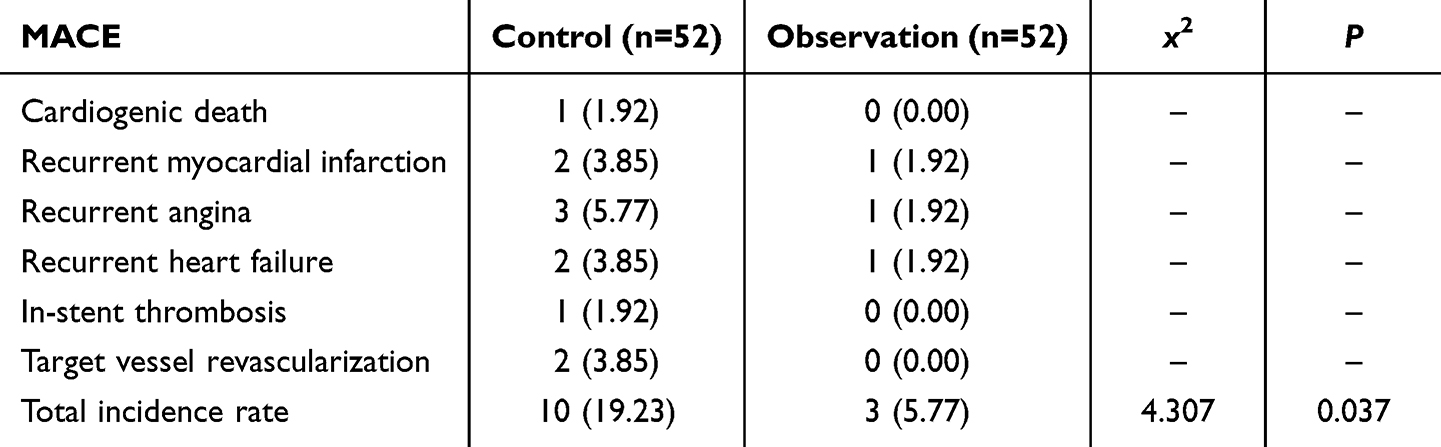 |
Table 3 Comparison of MACE Incidence [n (%)] |
Discussion
Acute myocardial infarction (AMI) remains a formidable challenge in clinical practice due to its sudden onset and potential for high morbidity and mortality.15 While PCI is the established standard for achieving timely coronary reperfusion and reducing acute-phase mortality, the long-term prognosis is often compromised by issues such as reperfusion injury, persistent inflammatory activation, and adverse left ventricular (LV) remodeling.17,18 Our study demonstrates that the early adjunctive use of rhBNP post-PCI yields superior clinical outcomes compared to standard therapy alone. The observation group exhibited a significantly higher total effective rate, alongside more pronounced improvements in LVEF, FS, and LVESD. These findings suggest that rhBNP not only enhances LV systolic function but may also mitigate pathological ventricular remodeling, likely attributable to its multi-faceted mechanisms of action.
The beneficial effects of rhBNP are rooted in its comprehensive physiological roles. As an endogenous neuroendocrine hormone, rhBNP promotes vasodilation and natriuresis while suppressing the renin-angiotensin-aldosterone system (RAAS) via the NPR-A/cGMP pathway.19,20 This results in reduced cardiac preload and afterload, improved myocardial compliance, and alleviation of volume overload,21 creating a hemodynamic environment conducive to cardiac recovery and resistance to remodeling.
Beyond hemodynamic improvement, our data indicate a significant reduction in myocardial injury biomarkers (CK-MB, cTnI, H-FABP) with rhBNP therapy. This cardioprotective effect is consistent with its potential to attenuate ischemia-reperfusion injury. Previous experimental and clinical studies have suggested that rhBNP can ameliorate calcium overload, suppress oxidative stress, and reduce cardiomyocyte apoptosis.22,23 Furthermore, its ability to enhance endothelial function and nitric oxide bioavailability may contribute to microvascular protection following PCI.14,24
The inflammatory cascade post-AMI is a key driver of ongoing myocardial damage and remodeling.25,26 In our study, the observation group showed markedly greater reductions in inflammatory cytokines (IL-6, TNF-α) and homocysteine (Hcy). The anti-inflammatory properties of rhBNP are supported by earlier work showing its capacity to inhibit neutrophil infiltration and pro-inflammatory cytokine release.27,28 The reduction in Hcy, an independent risk factor for endothelial dysfunction and cardiovascular events,29 further suggests a role for rhBNP in stabilizing vascular endothelium.
The most clinically significant finding was the reduction in 6-month MACE incidence with rhBNP therapy. This aligns with a growing body of evidence from other studies. For instance, a meta-analysis by Fang et al30 reported that rhBNP infusion in AMI patients was associated with improved LVEF and reduced risk of heart failure hospitalization. Similarly, a randomized trial by Yao et al31 found that peri-PCI rhBNP administration led to smaller infarct sizes and lower composite MACE rates at 30 days. Our results, which remain significant after multivariate adjustment, reinforce and extend these findings to a medium-term follow-up period, underscoring the potential of rhBNP to confer lasting cardiovascular benefits by simultaneously addressing myocardial injury, inflammation, and remodeling.
Limitations
This study has several limitations that should be acknowledged. First, its single-center, retrospective nature inherently carries risks of selection and unmeasured confounding bias, despite our statistical adjustments. Second, the relatively small sample size may limit the statistical power to detect differences in individual, less frequent MACE components. Third, the 6-month follow-up period is insufficient to evaluate the long-term impact of rhBNP on hard endpoints such as all-cause mortality or the progression of heart failure. Fourth, the absence of advanced imaging assessments (eg, cardiac magnetic resonance for myocardial salvage or fibrosis) prevents a more nuanced understanding of its effects on ventricular remodeling. Finally, as noted by a reviewer, the generalizability of our findings may be limited by the lack of racial and ethnic diversity in our patient sample, which was recruited from a single geographic region.
Conclusion
In conclusion, this study suggests that adjunctive therapy with recombinant human brain natriuretic peptide (rhBNP) following PCI in patients with AMI is associated with improved left ventricular function, reduced levels of myocardial injury and inflammatory stress biomarkers, and a lower incidence of major adverse cardiovascular events at 6 months compared to standard medical therapy alone. The multifaceted pharmacological profile of rhBNP, encompassing vasodilation, natriuresis, load reduction, and anti-inflammatory effects, underscores its potential clinical value in this setting. However, these findings and their implications must be interpreted in the context of the study’s limitations, including its retrospective design, potential for unmeasured confounding, and the absence of long-term follow-up beyond six months. Consequently, claims regarding long-term cardiac protection require validation. The promising results herein warrant verification in large-scale, multi-center, prospective randomized controlled trials to robustly establish the efficacy, safety, and optimal role of rhBNP within standardized AMI treatment pathways.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang J, Zhu XY, Tang C, et al. [Early differential diagnosis of acute myocardial infarction and acute myocarditis in young patients]. Zhonghua Yu Fang Yi Xue Za Zhi. 2025;59(3):365–374. Wolof. doi:10.3760/cma.j.cn112150-20240924-00770
2. Wang X, Zhou LY, Xu YL, et al. [Trend of incidence rate of acute myocardial infarction in Tengzhou City, Shandong Province, from 2013 to 2021]. Zhonghua Yu Fang Yi Xue Za Zhi. 2024;58(10):1556–1561. Wolof. doi:10.3760/cma.j.cn112150-20231027-00298
3. Jiang GH, Wang DZ, Zhang H, et al. [Epidemiological characteristics of pre-hospital mortality due to acute myocardial infarction from 1999 to 2016 in Tianjin city]. Zhonghua Yu Fang Yi Xue Za Zhi. 2020;54(1):99–103. Wolof. doi:10.3760/cma.j.issn.0253-9624.2020.01.018
4. Zheng XF, Wu LM, Chen LL. [Effects of percutaneous coronary intervention on cardiac function in ischemic cardiomyopathy patients with different left ventricular ejection fraction and SYNTAX score≤22]. Zhonghua Yi Xue Za Zhi. 2020;100(35):2768–2773. Danish. doi:10.3760/cma.j.cn112137-20200116-00106
5. Han YL, Li Y. [Emergency coronary intervention treatment for acute myocardial infarction: reach back on the past 40 years]. Zhonghua Xin Xue Guan Bing Za Zhi. 2023;51(12):1207–1211. Polish. doi:10.3760/cma.j.cn112148-20230814-00074
6. Zhong LH, Su YF, Zhang JQ, et al. [Predictive value of myocardial contrast echocardiography in evaluating myocardial perfusion and prognosis after percutaneous coronary intervention in patients with acute myocardial infarction]. Zhonghua Xin Xue Guan Bing Za Zhi. 2024;52(10):1186–1192. Polish. doi:10.3760/cma.j.cn112148-20231007-00219
7. Jin WY, Zhu TG, Chen H, et al. [Microvascular perfusion and cardiac function after revascularization assessed by myocardial contrast echocardiography in patients with acute ST-segment elevation myocardial infarction]. Zhonghua Xin Xue Guan Bing Za Zhi. 2023;51(2):151–157. Polish. doi:10.3760/cma.j.cn112148-20230104-00006
8. Liang L, Tang R, Xie Q, Han J, Li W. The clinical effect of recombinant human brain natriuretic peptide on asymptomatic peri-procedural myocardial injury after percutaneous transluminal coronary angioplasty. Sci Rep. 2020;10(1):15902.
9. Liu C, Xiong J, Yi X, et al. Decreased plasma ELABELA level as a novel screening indicator for heart failure: a cohort and observational study. Sci Rep. 2024;14(1):11333. doi:10.1038/s41598-024-61480-x
10. Yang J, Zhang L, Guo M, et al. Effects of recombinant human brain natriuretic peptide combined with tolvaptan on cardiac and renal function and serum inflammatory factors in patients with severe heart failure. Medicine. 2023;102(45):e35900. doi:10.1097/MD.0000000000035900
11. Pang Z, Pan C, Yao Z, et al. A study of the sequential treatment of acute heart failure with sacubitril/valsartan by recombinant human brain natriuretic peptide: a randomized controlled trial. Medicine. 2021;100(16):e25621. doi:10.1097/MD.0000000000025621
12. Liu JL, Zhang XF, Liu Z, et al. The role of recombinant human brain natriuretic peptide on the cardiac output of patients with acute decompensated heart failure using Guyton venous return curve: a STROBE-compliant retrospective study. Medicine. 2021;100(17):e25492. doi:10.1097/MD.0000000000025492
13. Miao ZL, Hou AJ, Zang HY, et al. Effects of recombinant human brain natriuretic peptide on the prognosis of patients with acute anterior myocardial infarction undergoing primary percutaneous coronary intervention: a prospective, multi-center, randomized clinical trial. J Thorac Dis. 2017;9(1):54–63. doi:10.21037/jtd.2017.01.15
14. Ning C, Zheng Y, Li J, Liu M, Fang Z. Effects of recombinant human brain natriuretic peptide in patients with acute myocardial infarction undergoing percutaneous coronary intervention: a systematic review and meta-analysis. Medicine. 2020;99(11):e19479. doi:10.1097/MD.0000000000019479
15. Zhang YJ, Yin L, Li J. Protective effect of recombinant human brain natriuretic peptide against contrast-induced nephropathy in elderly acute myocardial infarction patients: a randomized controlled trial. World J Clin Cases. 2022;10(33):12221–12229. doi:10.12998/wjcc.v10.i33.12221
16. Buske M, Feistritzer H-J, Jobs A, et al. [Management of acute coronary syndrome: ESC guidelines 2023]. Herz. 2024;49(1):5–14. German. doi:10.1007/s00059-023-05222-1
17. Wang X, Zhang Y, Shi LY, et al. [Clinical characteristics and in-hospital event rate of chronic obstructive pulmonary disease patients with concurrent acute myocardial infarction]. Zhonghua Yi Xue Za Zhi. 2024;104(45):4174–4178. Danish. doi:10.3760/cma.j.cn112137-20240625-01414
18. Yan GL, Yang MM, Zuo PF, et al. [Effects of remote ischemic preconditioning on contrast-induced acute kidney injury after percutaneous coronary intervention in patients with chronic total occlusion]. Zhonghua Yi Xue Za Zhi. 2021;101(11):776–781. Danish. doi:10.3760/cma.j.cn112137-20200627-01955
19. Li XW, Liu Y, Gao J, et al. [Analysis of short-term and long-term clinical outcomes in patients with acute myocardial infarction after one year of coronary stent implantation]. Zhonghua Yi Xue Za Zhi. 2020;100(15):1136–1141. Danish. doi:10.3760/cma.j.cn112137-20190805-01740
20. Gao Y, Zhang HB, Hou LL, et al. [Predictive value of plasma PCSK9 levels in acute myocardial infarction patients without reperfusion therapy for recurrence of cardiovascular events within 1 year]. Zhonghua Yi Xue Za Zhi. 2019;99(35):2750–2755. Danish. doi:10.3760/cma.j.issn.0376-2491.2019.35.007
21. Xu W, Wang W, Xiao Q, et al. Effect of recombinant human brain natriuretic peptide on acute carbon monoxide poisoning complicated with heart failure with reduced ejection fraction. Int Heart J. 2022;63(2):312–318. doi:10.1536/ihj.21-170
22. Ge Z, Li C, Liu Y, Sun X. The effect of recombinant human brain natriuretic peptide combined with Xinmailong on heart failure and its impact on cardiac function and inflammatory response. Int J Gen Med. 2025;18:1999–2008. doi:10.2147/IJGM.S509162
23. Ye M, Wang X, Sun Y, et al. [Clinical observation of Qiliqiangxin capsule combined with recombinant human brain natriuretic peptide in patients with acute heart failure]. Zhonghua Nei Ke Za Zhi. 2023;62(4):422–426. Polish. doi:10.3760/cma.j.cn112138-20220420-00291
24. Li N, Gao X, Wang W, et al. Protective effects of recombinant human brain natriuretic peptide on the myocardial injury induced by acute carbon monoxide poisoning. Cardiovasc Diagn Ther. 2020;10(6):1785–1794. doi:10.21037/cdt-20-591
25. Jiang Y, Luo B, Chen Y, et al. Predictive value of inflammatory prognostic index for contrast-induced nephropathy in patients undergoing coronary angiography and/or percutaneous coronary intervention. Sci Rep. 2024;14(1):15861. doi:10.1038/s41598-024-66880-7
26. Żurawska-Płaksej E, Płaczkowska S, Pawlik-Sobecka L, et al. Parameters of oxidative and inflammatory status in a three-month observation of patients with acute myocardial infarction undergoing coronary angioplasty-a preliminary study. Medicina. 2019;55(9):585. doi:10.3390/medicina55090585
27. Meng X, Fu M, Wang J, Xu H. Effects of recombinant human brain natriuretic peptide in patients with acute pulmonary embolism complicated with right ventricular dysfunction who underwent catheter-directed therapy. Int Heart J. 2022;63(1):8–14. doi:10.1536/ihj.21-086
28. Luo JC, Zhang YJ, Huang DL, et al. Recombinant human brain natriuretic peptide ameliorates venous return function in congestive heart failure. ESC Heart Fail. 2022;9(4):2635–2644. doi:10.1002/ehf2.13987
29. Yan J, Zhou J, Huang J, et al. The outcomes of acute myocardial infarction patients comorbidity with hypertension and hyperhomocysteinemia. Sci Rep. 2021;11(1):22936. doi:10.1038/s41598-021-02340-w
30. Fang J, Zeng W. A meta-analysis of the clinical efficacy of rhBNP in treating patients with acute myocardial infarction and heart failure. Am J Transl Res. 2021;13(4):2410–2421.
31. Yao L, Liu CJ, Zhang L, Lin Y, Hu YM. Influence of recombinant human B-type natriuretic peptide on improving ventricular function in patients with ST elevation myocardial infarction. Eur Rev Med Pharmacol Sci. 2023;27(8):3420–3429. doi:10.26355/eurrev_202304_32112
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cystatin C as a Predictor of Major Adverse Cardiovascular Event in Patients with Acute Myocardial Infarction Without Cardiogenic Shock and Renal Impairment After Coronary Intervention
Wasyanto T, Yasa A, Yudhistira Y
International Journal of General Medicine 2023, 16:2219-2227
Published Date: 3 June 2023
The Rehabilitation Efficacy of the Novel Metronomic Breathing Technique for Gerontic Patients After Percutaneous Coronary Intervention for Acute Myocardial Infarction—A Pilot Study
Wang Z, Zhu Z, Sun Y, Wang T, Lu Y, Che W, Liu W, Xu Y
Clinical Interventions in Aging 2024, 19:1029-1039
Published Date: 7 June 2024
Adherence to Cardiac Rehabilitation in Patients with Acute Myocardial Infarction After PCI: A Scoping Review
Li P, Zhang W, Wu B
Journal of Multidisciplinary Healthcare 2024, 17:4165-4176
Published Date: 28 August 2024
Associations Between Albumin/Neutrophil-to-Lymphocyte Ratio Score and New-Onset Atrial Fibrillation in Patients with Acute Myocardial Infarction Undergoing PCI
Yang SB, Zhao HW
Journal of Inflammation Research 2025, 18:61-71
Published Date: 3 January 2025
Serum sST2, IL-33, and Hcy Expression in Older Adults Patients with Myocardial Infarction and Their Predictive Value for MACE
Zheng LC, Liu F, Zheng PM, Xiao Z, Cui FC
Clinical Interventions in Aging 2025, 20:495-504
Published Date: 25 April 2025