Back to Journals » International Journal of General Medicine » Volume 17
Effect of Pre-Antibiotic Use Before First Stroke Incidence on Recurrence and Mortality: A Longitudinal Study Using the Korean National Health Insurance Service Database
Authors Park D ![]() , Kim HS
, Kim HS ![]() , Kim JH
, Kim JH
Received 27 December 2023
Accepted for publication 23 April 2024
Published 29 April 2024 Volume 2024:17 Pages 1625—1633
DOI https://doi.org/10.2147/IJGM.S456925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Dougho Park,1,2 Hyoung Seop Kim,3 Jong Hun Kim4
1Medical Research Institute, Pohang Stroke and Spine Hospital, Pohang, Republic of Korea; 2Department of Medical Science and Engineering, School of Convergence Science and Technology, Pohang University of Science and Technology, Pohang, Republic of Korea; 3Department of Physical Medicine and Rehabilitation, National Health Insurance Service Ilsan Hospital, Goyang, Republic of Korea; 4Department of Neurology, National Health Insurance Service Ilsan Hospital, Goyang, Republic of Korea
Correspondence: Jong Hun Kim, Department of Neurology, National Health Insurance Service Ilsan Hospital, 100 Ilsan-ro, Goyang, 10444, Republic of Korea, Tel +82-31-900-0213, Fax +82-31-900-0343, Email [email protected]
Purpose: Clinical studies on dysbiosis and stroke outcomes has been insufficient to establish clear evidence. This study aimed to investigate the effects of pre-antibiotic use before a stroke event on secondary outcomes using a longitudinal population-level database.
Patients and Methods: This retrospective cohort study included adults aged 55 years or older diagnosed with acute ischemic stroke (AIS) and acute hemorrhagic stroke (AHS) between 2004 and 2007. Patients were followed-up until the end of 2019, and the target outcomes were secondary AIS, AHS, and all-cause mortality. Multivariable Cox regression analyses were applied, and we adjusted covariates such as age, sex, socioeconomic status, hypertension, diabetes, and dyslipidemia. Pre-antibiotic use was identified from 7 days to 1 year before the acute stroke event.
Results: We included 159,181 patients with AIS (AIS group) and 49,077 patients with AHS (AHS group). Pre-antibiotic use significantly increased the risk of secondary AIS in the AIS group (adjusted hazard ratio [aHR], 1.03; 95% confidence interval [CI], 1.01– 1.05; p = 0.009) and secondary AHS in the AHS group (aHR, 1.08; 95% CI, 1.03– 1.12; p < 0.001). Furthermore, pre-antibiotic use in the AIS group was associated with a lower risk of mortality (aHR, 0.95; 95% CI, 0.94– 0.96; p < 0.001).
Conclusion: Our population-based longitudinal study revealed that pre-antibiotic use was associated with a higher risk of secondary stroke and a lower risk of mortality in the AIS and AHS groups. Further studies are needed to understand the relationship between dysbiosis and stroke outcomes.
Keywords: brain-gut axis, dysbiosis, mortality, stroke
Introduction
The gut houses trillions of microorganisms, collectively known as the gut microbiome.1 Dysbiosis, also known as antibiotic scars, occurs when antibiotic overuse leads to the destruction of beneficial bacteria in the gut.2 Beneficial bacteria help to regulate the immune system, digest food, and produce essential vitamins and nutrients. When antibiotics are administered, they can disrupt the balance of the gut microbiome, leading to the overgrowth of harmful bacteria and the reduction of beneficial bacteria.3 Dysbiosis represents wide-ranging and varied symptoms depending on the severity of the damage to the gut microbiome, and it can lead to health problems such as inflammatory autoimmune diseases, allergies, cancer, cardiovascular diseases, and stroke.4,5
The gut-brain axis is a bidirectional communication system that allows the gut and brain to influence each other’s functions.6 Several different pathways, including the nervous, immune, and endocrine systems, mediate the gut-brain axis.7 Studies have revealed that the occurrence and severity of acute ischemic stroke (AIS) and acute hemorrhagic stroke (AHS) could affect dysbiosis in patients and rodents.8 Inflammation is a key factor in the development of AIS,9,10 and the gut microbiome regulates inflammation in the body.11 Previous studies have shown that individuals with a diverse and balanced gut microbiome have lower levels of inflammation than those with an imbalance in gut bacteria.12 High blood pressure is another major risk factor for AIS and AHS. The gut microbiome plays a role in regulating blood pressure,13 and studies have shown that certain types of gut bacteria can produce compounds that can help lower blood pressure.14 Cholesterol levels are also linked to the gut microbiome; studies have reported that individuals with higher levels of certain types of gut bacteria had lower cholesterol levels, which could help reduce the risk of AIS.15,16 Overall, the gut microbiome plays a vital role in the development and prognosis of primary and secondary acute stroke.
However, more research is needed to fully understand the relationship between the gut microbiome and stroke and to develop strategies for using the gut microbiome to prevent and treat stroke in various directions. Most studies on the gut microbiome and stroke are experimental; therefore, more clinical studies are needed to establish causality and the best way to manipulate the gut microbiome for stroke prevention and better outcomes. Furthermore, studies demonstrating the relationship between antibiotic use and stroke secondary outcomes using longitudinal data are rare.
We hypothesized that the use of systemic antibiotics before stroke would affect the gut microbiota and, consequently, secondary events or mortality after stroke. This study aimed to investigate the effects of pre-antibiotic use before stroke occurrence on secondary outcomes and mortality using a longitudinal population-level database. Furthermore, using the Korean National Health Insurance Service (NHIS) database, we elucidated the effect of dysbiosis before the stroke event on long-term outcomes.
Materials and Methods
Study Design and Data Source
This retrospective cohort study used data from the Korean NHIS database and shared the same assigned cohort number with a previous relevant publication by authors (REQ202204012-005).17 The study included adults aged 55 years or older who were diagnosed with AIS and AHS from 2004 to 2007. Overall, 303,596 participants were included in this study. We excluded patients with underlying hemorrhagic or thrombotic conditions (Supplementary Table 1) and those who did not meet the diagnostic definition of acute stroke, as described in the next section. Among the 214,048 patients in the initial cohort, we further excluded individuals with previous cerebrovascular diseases during the washout period (2002–2003) and cases with missed sociodemographic data. The final sample size of participants included in the study was 208,258 (Figure 1). The study was reviewed and approved by the Institutional Review Board of the NHIS Ilsan Hospital (approval number: 2020–09-014) and conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived by the Institutional Review Board of the NHIS Ilsan Hospital because of the study’s retrospective design. This study was also conducted following the principles of the Declaration of Helsinki.
 |
Figure 1 Flowchart of patient inclusion in this study. Abbreviations: AIS, acute ischemic stroke; AHS, acute hemorrhagic stroke. |
Stroke Definition and Outcomes
Acute stroke was defined using the International Classification of Disease-10 codes.18 We defined AIS as hospitalization with an I63 code as the primary diagnosis (AIS group). Similarly, we defined AHS as hospitalization with I60–I62 codes as the primary diagnosis (AHS group). Simultaneously, we confirmed claim codes for brain computed tomography or magnetic resonance imaging within 7 days of hospitalization for both AIS and AHS. Secondary stroke events and all-cause mortality were defined as outcomes. The patients were followed up until December 31, 2019, and the first event after an acute stroke was the target outcome.
Covariates
The study identified age, sex, and socioeconomic status of the participants as demographic variables. We attempted to adjust for variables consistently available in our database among the confounding factors related to stroke prognosis identified in previous studies.19–22 Socioeconomic status was defined as the level of household income divided into three groups based on the health insurance premium quartiles (Level 1: 1st–7th quartiles; Level 2: 8th–14th quartiles; and Level 3: 15th–20th quartiles). Comorbidities, such as hypertension, diabetes, and dyslipidemia, were identified using medication claims and health screening data. Detailed definitions of hypertension, diabetes, and dyslipidemia in this study are provided in Supplementary Table 2.
Antibiotics
We identified the use of antibiotics before the acute stroke event using the claims data. We classified antibiotics into seven classes based on their target mechanisms: (1) cell wall (such as penicillin, cephalosporin, vancomycin, carbapenems, monobactam, polymyxin, and bacitracin); (2) ribosome 30S (such as aminoglycoside and tetracycline); (3) ribosome 50S (such as macrolide, chloramphenicol, lincosamide, linezolid, and streptogramin); (4) deoxyribonucleic acid synthesis (such as fluoroquinolones and metronidazole); (5) ribonucleic acid synthesis (such as rifampin); (6) mycolic acid synthesis (such as isoniazid); and (7) folic acid synthesis (such as sulfonamides and pyrimethamine). Pre-antibiotic use was identified 7 days to 1 year before acute stroke occurrence using claims data from the Health Insurance Review and Assessment Service. We did not consider the duration of antibiotic use because it may reflect a patient’s overall health rather than changes in the gut flora. Instead, antibiotics were analyzed according to whether they were used during the designated period. Only oral and intravenous forms of antibiotics were included, and topical antibiotics such as ointments or eye drops were excluded.
Statistical Analyses
Continuous variables are expressed as means and standard deviations and compared using a one-way analysis of covariance. Categorical variables are expressed as frequencies (proportions) and analyzed using the chi-square test. The cumulative probability of recurrent events and mortality were analyzed using Kaplan–Meier estimation. Multivariable Cox regression analysis was used to examine the risk of secondary stroke and mortality according to pre-antibiotic use, with adjustments for predetermined covariates, such as age, sex, socioeconomic status, hypertension, diabetes, and dyslipidemia. Our Cox proportional hazards models accounted for competing risks between the major cardio-cerebrovascular events (AIS, AHS, and acute myocardial infarction) and death using the Fine and Gray models.23 The partial effect model assessed the variable importance for each antibiotics class, using the proportion of the χ2 values. The level of statistical significance was set at p <0.05. All statistical analyses were performed using the SAS Enterprise Guide 7.15 (SAS Institute, Cary, NC, USA). R software version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria) was used to create Kaplan–Meier curves.
Results
Basic Characteristics and Outcome Events
The basic patient characteristics are summarized in Table 1. Finally, we included 159,181 patients with AIS and 49,077 patients with AHS. The participants’ mean age in the AIS group was 68.5 ± 11.5 years, which was significantly older than that in the AHS group (67.6 ± 11.2 years old) (p <0.001). The AIS group had a significantly lower proportion of women (49.1% vs 53.0%; p <0.001). Hypertension, diabetes, and dyslipidemia were significantly higher in the AIS group than in the AHS group (p <0.001 for all comparisons). The rate of pre-antibiotic use was significantly higher in the AIS group than in the AHS group (47.5% vs 43.0%; p <0.001). Moreover, the rate of pre-antibiotic use in the AIS group was significantly higher in all antibiotic classes except class 6, and no patient in this study’s cohort took class 5 antibiotics.
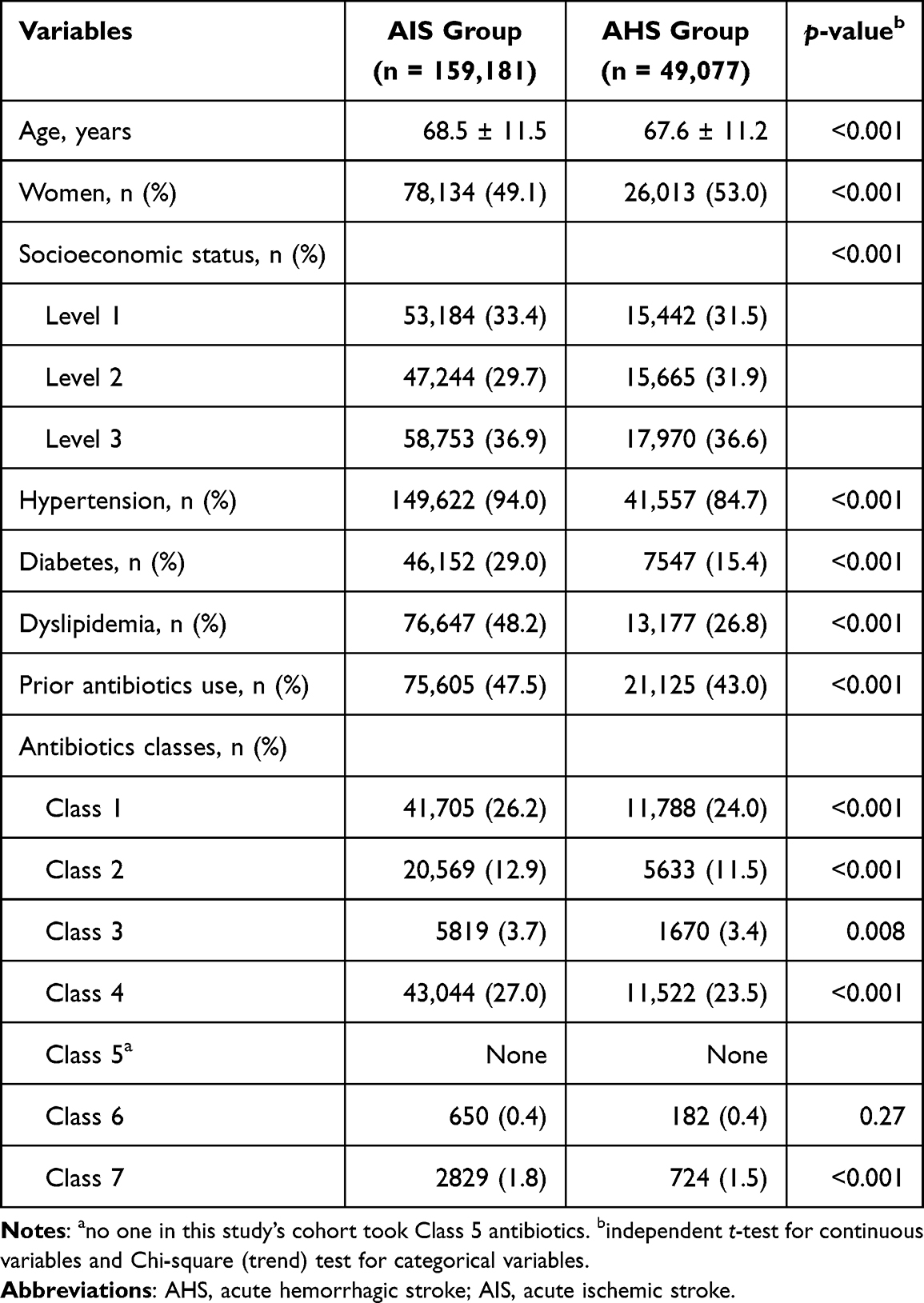 |
Table 1 Baseline Characteristics of Patients with Primary AIS and AHS |
Furthermore, 33,491 cases of secondary AIS (21.0%) and 73,300 deaths (46.1%) were observed during the time at risk. In the AHS group, 8574 secondary AHS cases (17.4%) and 24,990 deaths (50.9%) were observed. The death rate was higher in the AHS group, and the survival rate without major cardio-cerebrovascular events during the time at risk was higher in the AIS group (p <0.001) (Table 2).
 |
Table 2 Secondary Outcomes in Each Group |
Effect of Prior Antibiotics Uses on Recurrence and Mortality After Acute Stroke
Table 3 presents the Cox proportional hazards models for secondary stroke and mortality according to prior use of antibiotics in each group. In the AIS group, pre-antibiotic use was associated with a significantly higher risk of secondary AIS (adjusted hazard ratio [aHR], 1.03; 95% confidence interval [CI], 1.01–1.05; p = 0.009). However, no difference in the risk of secondary AIS was observed among those with prior antibiotic use in the AHS group (p = 0.49). In contrast, pre-antibiotic use in the AHS group was associated with a significantly higher risk of secondary AHS (aHR, 1.08; 95% CI, 1.03–1.12; p <0.001). No association was found between pre-antibiotic use and secondary AHS in the AIS group (p = 0.09). Regarding mortality, pre-antibiotic use in the AIS group was associated with a significantly lower risk of death (aHR, 0.95; 95% CI, 0.94–0.96; p <0.001). No significant association was found between pre-antibiotic use and mortality risk in the AHS group (p = 0.18).
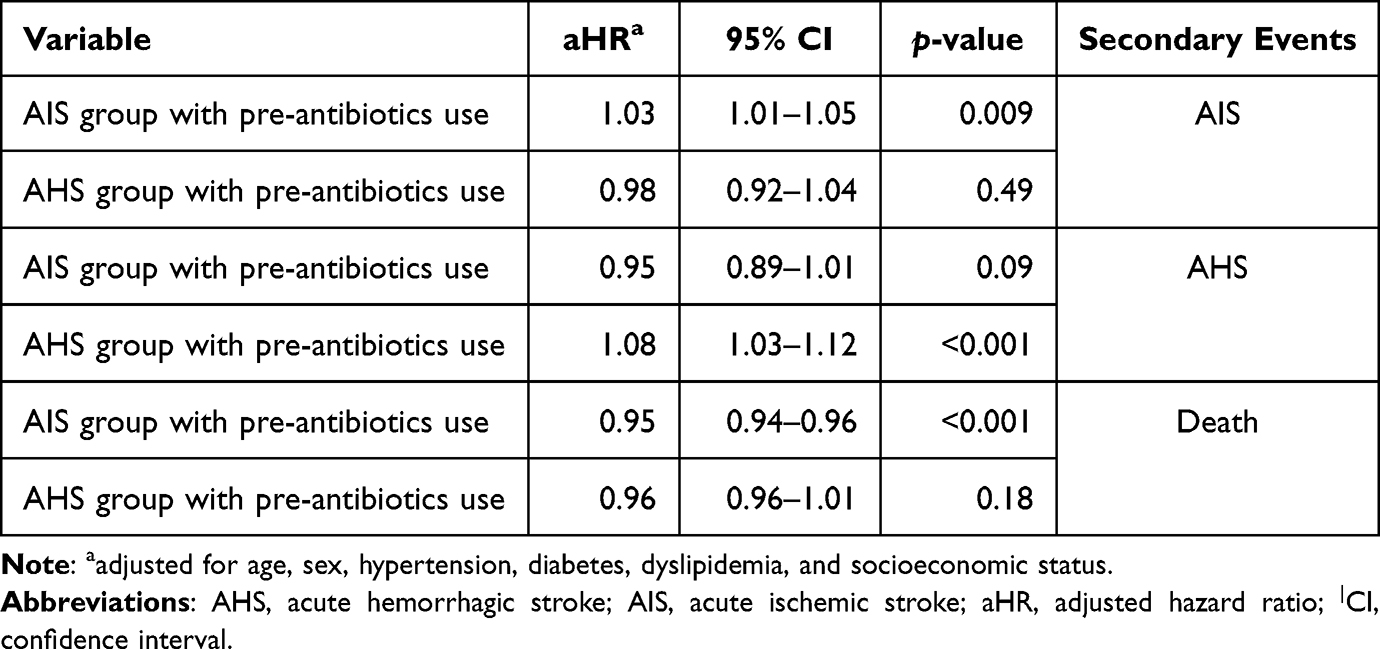 |
Table 3 Cox-Proportional Hazards Models for Secondary AIS, AHS, and Death According to Pre-Antibiotics Use |
Kaplan–Meier curves of the cumulative probability according to pre-antibiotic use for the significant cases of our Cox regression analyses are provided in Figure 2. Pre-antibiotic use significantly increased the cumulative probability of secondary AIS and AHS in the AIS and AHS groups, respectively. In contrast, pre-antibiotic use in the AIS group significantly decreased the cumulative probability of death.
 |
Figure 2 Kaplan–Meier curves for the cumulative probability according to pre-antibiotic use. P-values derived from the Log rank test are reported. (A) Pre-antibiotic use significantly increases the cumulative probability of secondary AIS in the AIS group and (B) secondary AHS in the AHS group. In contrast, (C) pre-antibiotic use in the AIS group significantly decreases the cumulative probability of death. Abbreviations: AIS, acute ischemic stroke; AHS, acute hemorrhagic stroke. |
The Impact of Each Antibiotic Class on Recurrence and Mortality After Acute Stroke
The results of further Cox proportional hazards models used to elucidate the importance of each antibiotic class are summarized in Table 4 and Figure 3. In the AIS group, pre-antibiotic use of class 2 (aHR, 1.07; 95% CI, 1.03–1.10; p <0.001) and class 4 (aHR 1.05; 95% CI, 1.03–1.08; p <0.001) significantly increased the risk of secondary AIS. In the AHS group, pre-antibiotic use of class 1 (aHR 1.06; 95% CI, 1.01–1.11; p = 0.01), class 4 (aHR, 1.06; 95% CI, 1.01–1.11; p = 0.02), and class 7 (aHR, 1.19; 95% CI, 1.02–1.39; p = 0.03) significantly increased the risk of secondary AHS. In the AIS group, pre-antibiotic use of class 3 (aHR 1.05; 95% CI, 1.01–1.09; p = 0.02) and class 6 (aHR, 1.27; 95% CI, 1.15–1.40; p <0.001) was significantly associated with a higher risk of mortality. In contrast, the pre-antibiotic use of class 1 (aHR 0.96; 95% CI, 0.95–0.98; p <0.001) and class 4 (aHR 0.98; 95% CI, 0.96–0.99; p = 0.004) significantly decreased the risk of mortality in the AIS group.
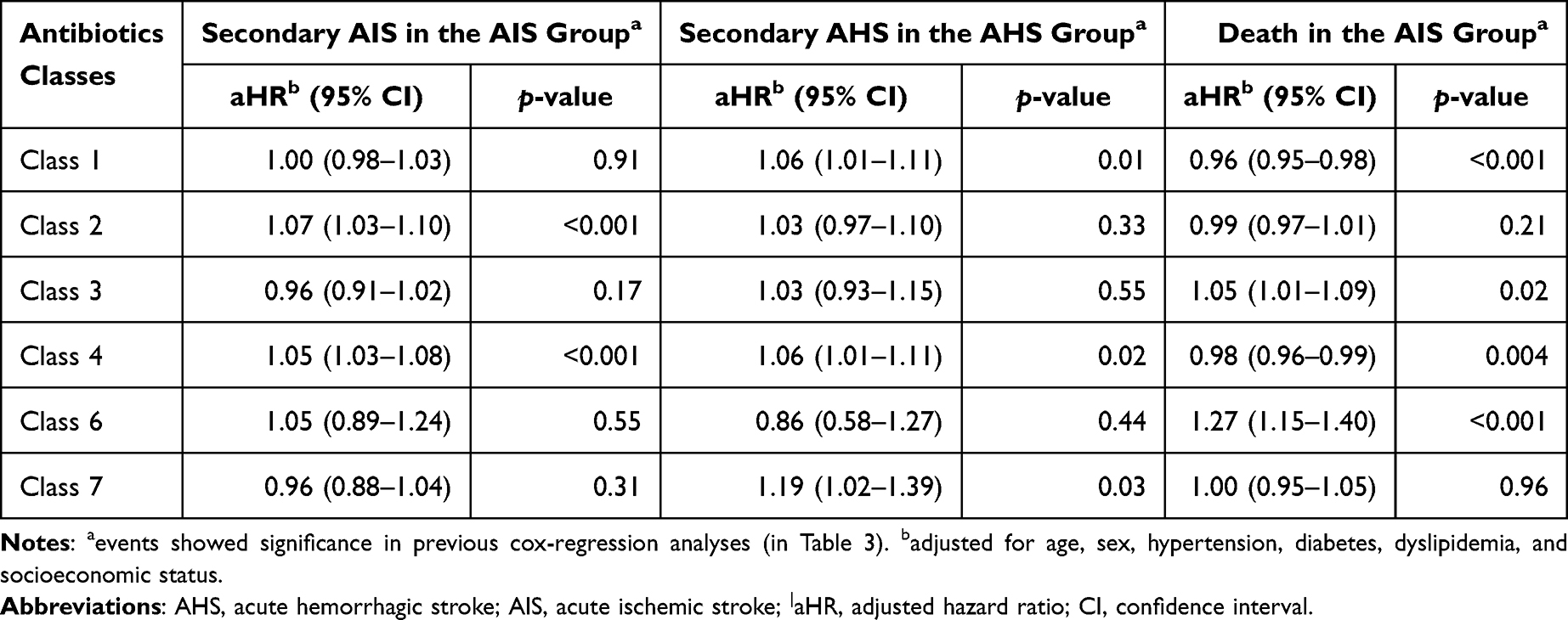 |
Table 4 Cox-Proportional Hazards Models According to Pre-Antibiotics Class |
 |
Figure 3 The feature importance of each antibiotic class is derived from the multivariable Cox regression analyses. Each antibiotics class’s importance is calculated using the proportion of the χ2 values. (A) Pre-antibiotic use of class 2 and class 4 was relatively important among all classes for the secondary AIS in the AIS group. (B) In the AHS group, pre-antibiotic use of class 1, class 4, and class 7 were relatively important for the risk of secondary AHS. Finally, (C) pre-antibiotic use of class 1, class 6, and class 4 were relatively important for decreased mortality in the AIS group. Abbreviations: AIS, acute ischemic stroke; AHS, acute hemorrhagic stroke. |
Discussion
We investigated the effect of pre-antibiotic use during a specific period before first stroke incidence on the long-term outcomes of secondary stroke and mortality. Our results showed that pre-antibiotic use significantly increased the risk of secondary AIS in the AIS group and secondary AHS in the AHS group. Regarding mortality, pre-antibiotic use in the AIS group was associated with a lower risk of mortality; however, no significant association was found between pre-antibiotic use and mortality risk in the AHS group. This study is the first to analyze the effects of dysbiosis caused by pre-antibiotic use before an acute stroke event on recurrence and mortality using a population-level database. Since previous large clinical studies on the relationship between dysbiosis and stroke have not been sufficient, our study using the NHIS database has a distinctive advantage. Moreover, our study provided outcome data for relatively longer periods than those in previous studies.
Previous studies have mainly focused on stroke-related dysbiosis; a vicious cycle in which the stroke itself induces dysbiosis associated with worse outcomes.24,25 This vicious cycle can be attributed to some factors such as changes in the gut microbiota composition, which could exacerbate systemic inflammation.12,26 In addition, dysbiosis after stroke has been linked to the regulation of body temperature, blood glucose, blood pressure, and hydration, ultimately affecting prognosis.6,27 In a clinical study with two cohorts of 152 patients with AIS by Xu et al,28 it was observed that gut dysbiosis developed and recovered after a stroke event, suggesting that acute-stage dysbiosis was an independent risk factor for poor early recovery after stroke. Xia et al29 presented a scale that represented the overall dysbiosis pattern, called the stroke dysbiosis index, and revealed that it was related to patient outcomes. The immunomodulatory functions of the gut microbiota modulates risk factors involved in secondary cardiovascular events in patients with primary stroke, and metabolites associated with the gut microbiota are involved in promoting atherosclerosis and thrombosis.30,31 In addition, increased antibiotic use was reported to be associated with higher mortality in patients with hemorrhagic stroke.32
As mentioned above, our study differs from previous studies in that we analyzed whether pre-stroke dysbiosis affects secondary stroke occurrence or post-stroke mortality. The infection itself is not only the risk factor for stroke but the widespread use of antibiotics can also induce dysbiosis. Previous studies have shown that dysbiosis could affect stroke occurrence and long-term outcomes after stroke;26,33 however, more clinical-based evidence is still needed. We attempted to establish evidence using a population-level database and confirmed that antibiotic use prior to stroke was an independent risk factor for secondary stroke.
Moreover, studies on major vascular outcomes based on antibiotic type revealed that azithromycin and levofloxacin were associated with cardiovascular events and death.34,35 On the other hand, a study reported that macrolide showed a favorable immune-modulatory effect in stroke.36 In summary, the outcomes based on the types of antibiotics used were discordant among the studies. In our study, class 4 was significantly associated with secondary stroke. However, it was difficult to observe the consistency in mortality, as it was associated with a rather low risk of death after AIS. Class 1 also increased the risk of secondary AHS in the AHS group; however, this class also lowered the mortality risk in the AIS group. Moreover, classes 3 and 6, which increased mortality risk in the AIS group, had no significant association with the occurrence of secondary stroke in both the AIS and AHS groups. Furthermore, we confirmed that discordance according to the type of antibiotic still existed in our population-level analysis.
This study had some limitations. As this was a retrospective study using claims data from the NHIS, we could not consider various clinical confounders related to secondary stroke and mortality. In addition, we did not consider the use of antibiotics after stroke occurrence; therefore, the direct effect of stroke-related dysbiosis could not be analyzed, and antibiotic use after a primary stroke can be an indicator of stroke severity, such as aspiration pneumonia and urinary tract infection; only pre-antibiotic use was analyzed. Although we utilized a large population database to robust our findings, the limitation of this study design was the absence of sufficient control groups. Therefore, we could not represent causality between pre-antibiotic usage and the secondary outcomes. In this context, several considerations for future study are needed–a larger sample size from multi-center and multi-ethnic for inferring causalities with control group and generalizability. Moreover, our longitudinal, observational study did not reveal a biological causality between antibiotic use and stroke secondary outcomes; therefore, novel methods such as Mendelian randomization analysis should be employed in future studies. Finally, stroke-related deaths could not be distinguished because we tracked all-cause mortality.
Conclusion
This study elucidated the effect of pre-antibiotic use during a specific period before the first incidence of stroke on long-term secondary outcomes. As a longitudinal, observational study using a population-level database, our study confirmed that pre-antibiotic use was significantly associated with the risk of secondary stroke. We also confirmed that pre-antibiotic use in the AIS group was associated with lower mortality risk. However, it is necessary to further establish evidence between dysbiosis and stroke outcomes by utilizing a sufficiently large and well-organized database in the future.
Data Sharing Statement
The data are not publicly available due to privacy and ethical restrictions of the Korean National Health Insurance data sharing system. The dataset used in this study can only be accessed by an authorized researcher through its own internal-networking system (J.H.K.).
Ethics Approval and Informed Consent
The study was reviewed and approved by the Institutional Review Board of the NHIS Ilsan Hospital (approval number: 2020-09-014) and conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived by the Institutional Review Board of the NHIS Ilsan Hospital because of the study’s retrospective design. This study was also conducted following the principles of the Declaration of Helsinki.
Acknowledgments
This study used data from the database compiled by the National Health Insurance Service (research management number: REQ202204012-005). The authors previously presented this cohort in a previous relevant publication (DOI: 10.3390/jcm12020568).
Funding
No external funding source for this study.
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Kamada N, Seo SU, Chen GY, Nunez G. Role of the gut microbiota in immunity and inflammatory disease. Nat Rev Immunol. 2013;13(5):321–335. doi:10.1038/nri3430
2. Weiss GA, Hennet T. Mechanisms and consequences of intestinal dysbiosis. Cell Mol Life Sci. 2017;74(16):2959–2977. doi:10.1007/s00018-017-2509-x
3. Rashid MU, Zaura E, Buijs MJ, et al. Determining the long-term effect of antibiotic administration on the human normal intestinal microbiota using culture and pyrosequencing methods. Clin Infect Dis. 2015;60(Suppl 2):S77–84. doi:10.1093/cid/civ137
4. DeGruttola AK, Low D, Mizoguchi A, Mizoguchi E. Current understanding of dysbiosis in disease in human and animal models. Inflamm Bowel Dis. 2016;22(5):1137–1150. doi:10.1097/MIB.0000000000000750
5. Carding S, Verbeke K, Vipond DT, Corfe BM, Owen LJ. Dysbiosis of the gut microbiota in disease. Microb Ecol Health Dis. 2015;26:26191. doi:10.3402/mehd.v26.26191
6. Rutsch A, Kantsjo JB, Ronchi F. The gut-brain axis: how microbiota and host inflammasome influence brain physiology and pathology. Front Immunol. 2020;11:604179. doi:10.3389/fimmu.2020.604179
7. Hu W, Kong X, Wang H, Li Y, Luo Y. Ischemic stroke and intestinal flora: an insight into brain-gut axis. Eur J Med Res. 2022;27(1):73. doi:10.1186/s40001-022-00691-2
8. Zhao J, Liu S, Yan J, Zhu X. The impact of gut microbiota on post-stroke management. Front Cell Infect Microbiol. 2021;11:724376. doi:10.3389/fcimb.2021.724376
9. Zhang P, Zhang X, Huang Y, et al. Atorvastatin alleviates microglia-mediated neuroinflammation via modulating the microbial composition and the intestinal barrier function in ischemic stroke mice. Free Radic Biol Med. 2021;162:104–117. doi:10.1016/j.freeradbiomed.2020.11.032
10. Elkind MSV, Boehme AK, Smith CJ, Meisel A, Buckwalter MS. Infection as a stroke risk factor and determinant of outcome after stroke. Stroke. 2020;51(10):3156–3168. doi:10.1161/STROKEAHA.120.030429
11. Agirman G, Yu KB, Hsiao EY. Signaling inflammation across the gut-brain axis. Science. 2021;374(6571):1087–1092. doi:10.1126/science.abi6087
12. Al Bander Z, Nitert MD, Mousa A, Naderpoor N. The gut microbiota and inflammation: an overview. Int J Environ Res Public Health. 2020;17(20):7618. doi:10.3390/ijerph17207618
13. Wilck N, Matus MG, Kearney SM, et al. Salt-responsive gut commensal modulates T(H)17 axis and disease. Nature. 2017;551(7682):585–589. doi:10.1038/nature24628
14. Verhaar BJH, Prodan A, Nieuwdorp M, Muller M. Gut microbiota in hypertension and atherosclerosis: a review. Nutrients. 2020;12(10):2982. doi:10.3390/nu12102982
15. Vourakis M, Mayer G, Rousseau G. The role of gut microbiota on cholesterol metabolism in atherosclerosis. Int J Mol Sci. 2021;22(15):8074. doi:10.3390/ijms22158074
16. Ramirez-Perez O, Cruz-Ramon V, Chinchilla-Lopez P, Mendez-Sanchez N. The role of the gut microbiota in bile acid metabolism. Ann Hepatol. 2017;16(Suppl. 1: s3–105.):s15–s20. doi:10.5604/01.3001.0010.5672
17. Park D, Kim MC, Hong D, Jeong YS, Kim HS, Kim JH. Recurrence and mortality risks in patients with first incident acute stroke or myocardial infarction: a longitudinal study using the Korean national health insurance service database. J Clin Med. 2023;12(2):568.
18. Kokotailo RA, Hill MD. Coding of stroke and stroke risk factors using international classification of diseases, revisions 9 and 10. Stroke. 2005;36(8):1776–1781. doi:10.1161/01.STR.0000174293.17959.a1
19. Park D, Lee SY, Jeong E, et al. The effects of socioeconomic and geographic factors on chronic phase long-term survival after stroke in South Korea. Sci Rep. 2022;12(1):4327. doi:10.1038/s41598-022-08025-2
20. Sennfalt S, Pihlsgard M, Petersson J, Norrving B, Ullberg T. Long-term outcome after ischemic stroke in relation to comorbidity - an observational study from the Swedish stroke register (Riksstroke). Eur Stroke J. 2020;5(1):36–46. doi:10.1177/2396987319883154
21. Wong YS, Tsai CF, Ong CT. Risk factors for stroke recurrence in patients with hemorrhagic stroke. Sci Rep. 2022;12(1):17151. doi:10.1038/s41598-022-22090-7
22. Khanevski AN, Bjerkreim AT, Novotny V, et al. Recurrent ischemic stroke: incidence, predictors, and impact on mortality. Acta Neurol Scand. 2019;140(1):3–8. doi:10.1111/ane.13093
23. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 2012;94(446):496–509. doi:10.1080/01621459.1999.10474144
24. Benakis C, Poon C, Lane D, et al. Distinct commensal bacterial signature in the gut is associated with acute and long-term protection from ischemic stroke. Stroke. 2020;51(6):1844–1854. doi:10.1161/STROKEAHA.120.029262
25. Pluta R, Januszewski S, Czuczwar SJ. The role of gut microbiota in an ischemic stroke. Int J Mol Sci. 2021;22(2):915. doi:10.3390/ijms22020915
26. Singh V, Roth S, Llovera G, et al. Microbiota dysbiosis controls the neuroinflammatory response after stroke. J Neurosci. 2016;36(28):7428–7440. doi:10.1523/JNEUROSCI.1114-16.2016
27. Winek K, Engel O, Koduah P, et al. Depletion of cultivatable gut microbiota by broad-spectrum antibiotic pretreatment worsens outcome after murine stroke. Stroke. 2016;47(5):1354–1363. doi:10.1161/STROKEAHA.115.011800
28. Xu K, Gao X, Xia G, et al. Rapid gut dysbiosis induced by stroke exacerbates brain infarction in turn. Gut. 2021;70(8):1486–1494. doi:10.1136/gutjnl-2020-323263
29. Xia GH, You C, Gao XX, et al. Stroke dysbiosis index (SDI) in gut microbiome are associated with brain injury and prognosis of stroke. Front Neurol. 2019;10:397. doi:10.3389/fneur.2019.00397
30. Haghikia A, Li XS, Liman TG, et al. Gut microbiota-dependent trimethylamine N-oxide predicts risk of cardiovascular events in patients with stroke and is related to proinflammatory monocytes. Arterioscler Thromb Vasc Biol. 2018;38(9):2225–2235.
31. Peh A, Ja O, Broughton BRS, Marques FZ. Gut microbiota and their metabolites in stroke: a double-edged sword. Stroke. 2022;53(5):1788–1801. doi:10.1161/STROKEAHA.121.036800
32. Wang F, Wang Y, Shi J, et al. Excessive antibiotics use increased in-hospital mortality in intracerebral hemorrhage patients with stroke-associated infection. Sci Rep. 2020;10(1):1950. doi:10.1038/s41598-020-58772-3
33. Chidambaram SB, Rathipriya AG, Mahalakshmi AM, et al. The influence of gut dysbiosis in the pathogenesis and management of ischemic stroke. Cells. 2022;11(7):1239. doi:10.3390/cells11071239
34. Ray WA, Murray KT, Hall K, Arbogast PG, Stein CM. Azithromycin and the risk of cardiovascular death. N Engl J Med. 2012;366(20):1881–1890. doi:10.1056/NEJMoa1003833
35. Lu ZK, Yuan J, Li M, et al. Cardiac risks associated with antibiotics: azithromycin and levofloxacin. Expert Opin Drug Saf. 2015;14(2):295–303. doi:10.1517/14740338.2015.989210
36. Smith CJ, Heal C, Vail A, et al. Antibiotic class and outcome in post-stroke infections: an individual participant data pooled analysis of vista-acute. Front Neurol. 2019;10:504. doi:10.3389/fneur.2019.00504
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Complications and Mortality After Surgery in Patients with Chronic Kidney Disease: A Retrospective Cohort Study Based on a Multicenter Clinical Database
Liao CC, Liu CC, Lee YW, Chang CC, Yeh CC, Chang TH, Chen TL, Lin CS
Journal of Multidisciplinary Healthcare 2024, 17:3535-3544
Published Date: 23 July 2024