Back to Journals » Drug Design, Development and Therapy » Volume 19
Effect of Neoadjuvant Immunochemotherapy on Postoperative Pulmonary Complications for Locally Advanced Esophageal Cancer: A Propensity Score Matching Cohort Study
Authors Du W ![]() , Qiao X, Yao J, Wang Z, Shi Y, Jia H
, Qiao X, Yao J, Wang Z, Shi Y, Jia H ![]()
Received 30 April 2025
Accepted for publication 28 August 2025
Published 3 September 2025 Volume 2025:19 Pages 7637—7651
DOI https://doi.org/10.2147/DDDT.S537794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Wei Du,1 Xi Qiao,1 Jifang Yao,2 Zhijiao Wang,1 Yuanyuan Shi,1 Huiqun Jia1
1Department of Anesthesiology, The Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, People’s Republic of China; 2Department of Thoracic Surgery, The Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, People’s Republic of China
Correspondence: Huiqun Jia, Department of Anesthesiology, The Fourth Hospital of Hebei Medical University, No. 12, Jiankang Road, Shijiazhuang, Hebei Province, People’s Republic of China, Email [email protected]
Purpose: Neoadjuvant immunochemotherapy (NICT) has shown promise in improving the oncological outcomes of locally advanced esophageal cancer (LAEC). However, concerns remain regarding its potential to induce pulmonary side effects that may increase the risk of perioperative adverse events. This study aimed to compare the incidence of postoperative pulmonary complications (PPCs) in patients receiving NICT and those undergoing non-neoadjuvant therapy.
Patients and Methods: This retrospective cohort study included 274 patients with LAEC who received either NICT or non-neoadjuvant therapy followed by radical esophagectomy. Propensity score matching was used to balance patient characteristics between the two groups. The primary outcome was the incidence of PPCs within the first seven days postoperatively. Conditional logistic regression models were used to assess the association between NICT and PPCs. Sensitivity analysis using inverse probability of treatment weighting was conducted to validate the robustness of the findings.
Results: A total of 182 patients were included in the final analysis, with 91 patients in each group. The incidence of PPCs was significantly higher in the NICT group than in the control group (46.2% vs 26.4%, P = 0.009). Respiratory infections (37.4% vs 22.0%, P = 0.035) and pleural effusions (22.0% vs 9.9%, P = 0.043) were more frequent in the NICT group. New-onset arrhythmia was the most common cardiovascular complication, with tachycardia occurring in 24.2% of patients in the NICT group compared to 9.9% in the control group (P = 0.018). Conditional logistic regression analysis revealed a significant association between NICT and PPCs (OR = 5.648, 95% CI: 1.579– 20.204, P = 0.008). Sensitivity analysis using IPTW further confirmed these results (OR = 2.893, 95% CI = 1.537– 5.446, P = 0.001).
Conclusion: Patients with locally advanced esophageal cancer who received at least two cycles of NICT had a significantly increased risk of developing postoperative pulmonary complications.
Keywords: neoadjuvant chemotherapy, immunotherapy, postoperative pulmonary complications, esophageal cancer
Introduction
Esophageal cancer (EC) is a highly aggressive malignancy with poor prognosis, ranking as the seventh leading cause of cancer-related deaths worldwide.1 This grim prognosis is particularly evident in locally advanced esophageal cancer (LAEC), where extensive locoregional involvement and early lymphatic dissemination create formidable therapeutic challenges.2
For more than a decade, the CROSS regimen—carboplatin plus paclitaxel with concurrent 41.4 Gy radiotherapy followed by surgery—has constituted the evidence-based backbone of multimodal therapy for LAEC.3 Yet, contemporary real-world analyses indicate that 29% of patients still fail to achieve an R0 resection after CROSS, and the hazard for distant recurrence within three years approaches 40%.4 These unmet clinical needs have catalyzed the integration of immune checkpoint inhibitors (ICIs) into perioperative treatment sequencing.5–7 The advent of neoadjuvant immunochemotherapy (NICT) marks a revolutionary shift in EC therapeutics, building on landmark trials KEYNOTE-1816 and KEYNOTE −590,7 which established the transition of immunotherapy to first-line therapy. By synergistically combining cytotoxic chemotherapy with immune modulation, NICT achieves unprecedented pathological complete response (pCR) rates.5,7 This dual mechanism not only enhances tumor immunogenicity, but may also induce durable systemic antitumor immunity, a potential game-changer in preventing micrometastatic recurrence.8 NICT has been included as a neoadjuvant treatment option for locally advanced esophageal cancer in the National Comprehensive Cancer Network (NCCN),9 European Society for Medical Oncology (ESMO), and Chinese Society of Clinical Oncology (CSCO) guidelines.10
Recent systematic reviews and meta-analyses have highlighted the potential benefits of NICT in terms of pCR rates and overall survival but have also noted an increased incidence of adverse events.11 Studies have shown that while NICT can significantly improve pCR rates and tumor regression grades, it may also lead to a higher incidence of certain adverse events.11 In the context of immune pneumonitis, a known complication of ICI therapy, surgical risk considerations become particularly relevant. Despite these oncologic gains, the perioperative safety profile of NICT remains incompletely defined. Esophagectomy is intrinsically associated with a high incidence of postoperative pulmonary complications (PPCs), including pneumonia, acute respiratory distress syndrome (ARDS), and prolonged mechanical ventilation, with a baseline incidence ranging from 22% to 46%.12,13 These complications disproportionately affect patient outcomes, leading to prolonged hospital stays and increased early postoperative mortality.14,15 Established risk factors, such as advanced age,16 pulmonary dysfunction,17 and smoking history18 are well validated. However, immune-related pneumonitis, documented in as many as 19% of patients in a recent series,19 confers a disproportionate mortality risk. More critically, preoperative exposure to NICT may prime a systemic cytokine storm,7 amplify T-cell–mediated parenchymal injury, and impede subsequent tissue repair, thereby potentiating the inflammatory cascade unleashed by transthoracic esophagectomy. The resulting pulmonary toxicity signature is qualitatively and quantitatively distinct from that observed with conventional cytotoxic regimens; however, its perioperative ramifications remain essentially unmapped. This knowledge gap is critical, given the rapid clinical adoption of NICT. Current evidence suggests that while NICT improves tumor responses, it may simultaneously alter postoperative pulmonary complication profiles through immune-mediated tissue remodeling and cytokine release. Therefore, we tested the hypothesis that the incidence of PPCs is higher among patients receiving NICT for LAEC during the first 7 postoperative days.
Materials and Methods
Study Design and Database
This study was approved by the Ethics Committee of the Fourth Hospital of Hebei Medical University (2023KS180). The requirement for informed consent was waived. This retrospective, single-center cohort analysis included patients with LAEC (cT2–4a N0–3 M0, AJCC/UICC 8th edition20) who underwent esophagectomy at the Fourth Hospital of Hebei Medical University between June 1, 2021, and December 31, 2023. No operative approach restriction was imposed; both transthoracic (Ivor Lewis and McKeown) and hybrid minimally invasive techniques were eligible. Case identification was performed using the institutional Surgery Registry, a prospectively maintained, internally audited database. Data abstraction was performed independently by two clinicians who cross-validated variables across the electronic health record, anesthesia information management system, and radiology and pathology reports.
Study Population
The inclusion criteria were as follows: patients with LAEC who (a) received neoadjuvant immunochemotherapy (NICT) for at least two cycles or non-neoadjuvant therapy as preoperative treatment, (b) underwent radical esophagectomy, (c) were aged 50–80 years, and (d) had adequate hematologic blood counts (white blood cell count > 3 × 109/L, platelet count > 50 × 109/L, hemoglobin concentration > 85 g/L).
The exclusion criteria were as follows: (a) prior neoadjuvant radiotherapy, (b) neoadjuvant chemotherapy alone, (c) incomplete key medical data, (d) history of respiratory infection within 30 days before surgery, (e) history of prior thoracic surgery, and (f) thoracotomy.
Exposure - Neoadjuvant Immunochemotherapy Procedure
The diagnosis of LAEC was confirmed via histopathological examination and computed tomography (CT). Neoadjuvant immunochemotherapy was administered based on the patient’s condition. The neoadjuvant chemotherapy regimen consisted of paclitaxel plus platinum-based drugs, whereas the immunotherapy regimen included programmed death receptor 1 (PD-1) inhibitors, such as pembrolizumab, tislelizumab, camrelizumab, or sintilimab. Patients received at least two cycles of neoadjuvant regimens prior to surgery.
The participants typically underwent 2–4 cycles of NICT. The total number of NICT cycles was determined by a multidisciplinary team. Efficacy evaluations were performed after each treatment cycle, and additional cycles were administered based on the tumor response, the patient’s physical condition, and ongoing clinical benefit from NICT.
Anesthesia and Perioperative Care
Intraoperative monitoring comprised continuous electrocardiographic assessment, pulse oximetry, invasive arterial blood pressure (BP) measurement, bispectral index (BIS) monitoring, capnography, inhalational anesthetic concentration, and urine output recording.
General anesthesia was induced with a combination of sufentanil, propofol or etomidate, and cis-atracurium or rocuronium. Anesthesia was maintained by sevoflurane inhalation and remifentanil infusion. Nondepolarizing neuromuscular blocking agents were administered to achieve muscle relaxation. The depth of anesthesia was titrated to maintain BIS values within 40–60. Fluid resuscitation and blood transfusion were administered according to standard clinical practice. Mechanical ventilation was delivered in a volume-controlled mode, with tidal volumes set at 7–8 mL/kg during two-lung ventilation and 5–6 mL/kg during one-lung ventilation. Intraoperative pulmonary recruitment maneuvers were performed intermittently. Blood gas analysis was performed periodically to ensure hemodynamic stability. Nonsteroidal anti-inflammatory drugs (NSAIDs) were administered unless contraindicated by the physician. Patients were extubated and transferred to the post-anesthesia care unit (PACU) if hemodynamically stable; otherwise, they were admitted to the intensive care unit (ICU).
In the PACU, patients underwent continuous monitoring of noninvasive BP, heart rate (HR), and pulse oximetry for a minimum of 30 min until they achieved a steward score of four.21 Patients who were subsequently transferred to the general wards continued to be monitored for BP and pulse oximetry until the second postoperative day, followed by once or twice daily monitoring until hospital discharge.
Surgical Process
Radical esophagectomy for esophageal cancer represents a technically complex surgical intervention that systematically progresses through three critical phases: tumor resection, regional lymphadenectomy, and digestive tract reconstruction. The procedure initiated with en bloc tumor resection aiming to achieve histologically negative margins (R0 resection), where the resection extent was planned based on comprehensive evaluation of tumor characteristics, including its anatomical location and depth of invasion, thereby ensuring optimal oncological clearance while preserving adjacent vital structures. Given the high metastatic potential of esophageal cancer to locoregional lymph nodes, a systematic lymph node dissection was performed. This includes the removal of the periesophageal, mediastinal, and, when indicated, abdominal lymph nodes. Adequate lymphadenectomy was crucial for accurate staging and reduction of locoregional recurrence. The final reconstructive phase employs a gastric conduit approach, wherein the stomach was carefully mobilized, fashioned into a tubular structure, and subsequently transposed either into the thoracic cavity or cervical region to reestablish gastrointestinal continuity. This reconstruction preserved the functional integrity of the upper digestive system and maintained the alimentary function and nutritional status postoperatively.
Outcomes
The primary outcome was the incidence of a composite of postoperative pulmonary complications (PPCs) within the first seven postoperative days. PPCs were defined according to established criteria and included respiratory infection, respiratory failure, pleural effusion, atelectasis, pneumothorax, bronchospasm, and aspiration pneumonitis22 (Supplement 1). These complications were classified as grade II or higher according to the Clavien–Dindo classification23 (Supplement 2). Any component of grade II or higher was considered a PPC. Diagnoses were based on physical examinations, laboratory findings, and imaging results.
Secondary outcomes included major adverse cardiac events, including new-onset arrhythmias requiring treatment, acute coronary syndrome (ACS), and myocardial injury. Surgical complications were defined as any adverse events directly related to the surgical procedure, such as anastomotic leakage and chylothorax. Sepsis was defined according to the third international consensus definition.24
Data Collection
Baseline, intraoperative, and postoperative data were retrospectively collected from medical records. Baseline data included demographic and morphometric characteristics, surgical diagnosis, preoperative comorbidities and their management, smoking history, and results of relevant laboratory tests and physical examinations. Intraoperative data included anesthesia duration, types and doses of anesthetics and medications, fluid balance and blood transfusion details, and specifics regarding the surgical type and duration. The postoperative data focused on the incidence of postoperative pulmonary complications, major adverse cardiac events, sepsis, and surgical complications.
Sample Size Estimation
Sample size estimation revealed a significant increase in PPCs from 26% in surgery-only patients to 49% following NICT. Traditional power calculation for this effect size (α=0.05, β=0.2) yielded 66 patients per arm. Accounting for PSM parameters, including an 80% propensity score overlap, the adjusted minimum required sample size increased to 83 patients per group to maintain adequate statistical power.
Statistical Analysis
We employed propensity score matching (PSM) with a 1:1 ratio using the nearest-neighbor method on a logit scale with a caliper limit of 0.1. This approach was used to minimize the impact of confounding factors that may influence treatment decisions and to balance patient characteristics, including age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, tumor location, minimally invasive esophagectomy (MIE), surgical incision, and clinical TN stage. Confounding variables were considered comparable when the standardized mean difference (SMD) was < 0.10 and the P-value was > 0.05.
After propensity score matching, a test of the balance of the covariates before and after matching was performed by plotting a love plot. The plot measures the difference in means between the treatment and control groups for each covariate using the SMD.
Continuous variables were expressed as mean ± standard deviation and analyzed using independent or paired Student’s t-tests for normally distributed data, or Wilcoxon signed-rank tests for non-parametric data. Categorical variables were presented as frequencies and percentages, with between-group comparisons performed using Chi-square tests or McNemar’s tests, as appropriate.
Conditional logistic regression was used to assess the association between NICT and PPCs. Three models were evaluated in this study: Model 1: Unadjusted for covariates. Model 2: Adjusted for cis-atracurium, total fluid input, RBC, total fluid output, blood loss, anesthesia duration, and surgery duration. Considering the potential synergistic effect of prolonged anesthesia and surgery duration,25,26 we included an interaction term (anesthesia duration × surgery duration) in Model 3. Model 3: Further adjusted for additional covariates, including the interaction term (anesthesia duration × surgery duration), in addition to the variables included in Model 2. Results were expressed as odds ratios (OR) with 95% confidence intervals (CI). Then, we employed a multi-criteria model selection approach using Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC).
To evaluate the robustness of our findings, we performed sensitivity analysis incorporating inverse probability of treatment weighting (IPTW) to account for potential residual confounding and re-assess the primary outcome measures.
We repeated the primary analysis in predefined subgroups stratified by age (≥65 years), gender, number of NICT cycles, surgical incision (one-incision, Ivor Lewis or McKeown) and surgical approach (open transthoracic vs minimally invasive esophagectomy).
All statistical tests were two-sided, with statistical significance set at P < 0.05. Analyses were performed using R statistical software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
Patients Characteristics
In total, 274 patients with LAEC who underwent combination therapy were enrolled in this study cohort. In the Control group, 150 patients did not receive neoadjuvant therapy preoperatively, whereas 124 patients in the NICT group received at least two cycles of chemotherapy combined with immunotherapy preoperatively (Figure 1).
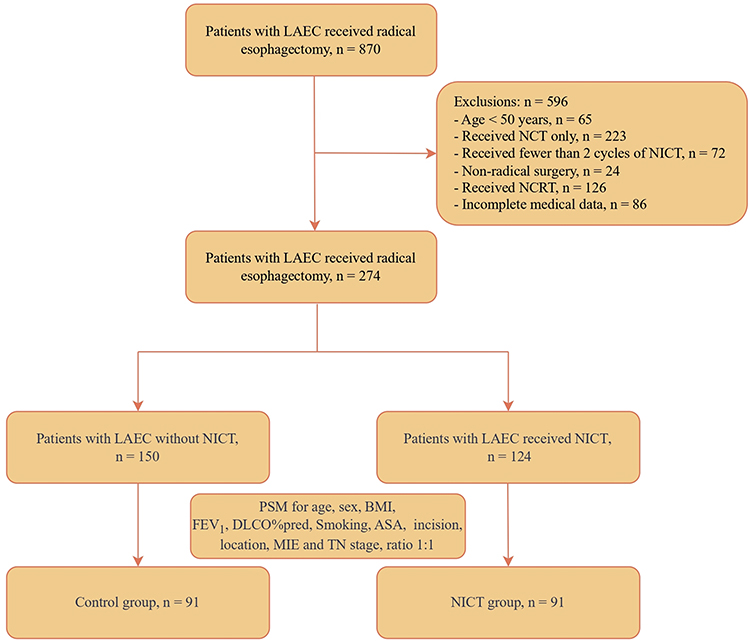 |
Figure 1 Flowchart of patient selection. Abbreviations: LAEC, locally advanced esophageal cancer; NCT, neoadjuvant chemotherapy; NCRT, neoadjuvant chemoradiotherapy; NICT, neoadjuvant immunochemotherapy; PSM, propensity score matching; BMI, body mass Index; FEV₁, forced expiratory volume in 1 second; DLCO%pred, diffusing capacity of the carbon monoxide (DLCO) predicted; ASA, American Society of Anesthesiologists; MIE, minimally invasive esophagectomy. |
Preoperative Immune-Related Adverse Events (irAEs)
Before initiating treatment, patients underwent comprehensive assessments to evaluate their overall health status, including thyroid hormone levels, liver and kidney function, pituitary function (ACTH), NT-pro BNP, and cTnI. During neoadjuvant therapy, patients are closely monitored, with tumor response evaluated after the first two and subsequent cycles. Surgery is scheduled 4–6 weeks after the last cycle, during which time patients undergo another comprehensive assessment, including a CT scan.
In the current cohort, 11 patients (8.9%) developed grade 1–2 thyroid dysfunction, and five patients (4.0%) developed hepatitis. These abnormalities were corrected with treatment before surgery, and the patients were scheduled for surgery 4–6 weeks later. Four patients (3.2%) developed immune-mediated pneumonitis, presenting with fever, cough, and dyspnea. After successful treatment and radiological improvement, the patients underwent surgery eight weeks later.
Propensity Score Matching and Balance Assessment
Prior to propensity score matching (PSM), the control group exhibited a higher mean age (P = 0.004), and the NICT group had a greater proportion of patients with American Society of Anesthesiologists (ASA) status III (P = 0.027). After matching in a 1:1 ratio, 182 patients were included, with 91 in each group. The baseline characteristics of the patients in both groups were well balanced after PSM, including demographics (sex and age), BMI, smoking status, forced expiratory volume in the first second (FEV1), diffusing capacity of the carbon monoxide % predicted (DLCO%pred), tumor characteristics (location of esophageal cancer, clinical TNM stage), and surgical status (type of surgical incision, whether minimally invasive esophagectomy [MIE] was performed). All P values exceeded 0.05, and the standardized mean differences (SMD) were less than 0.10 (Table 1).
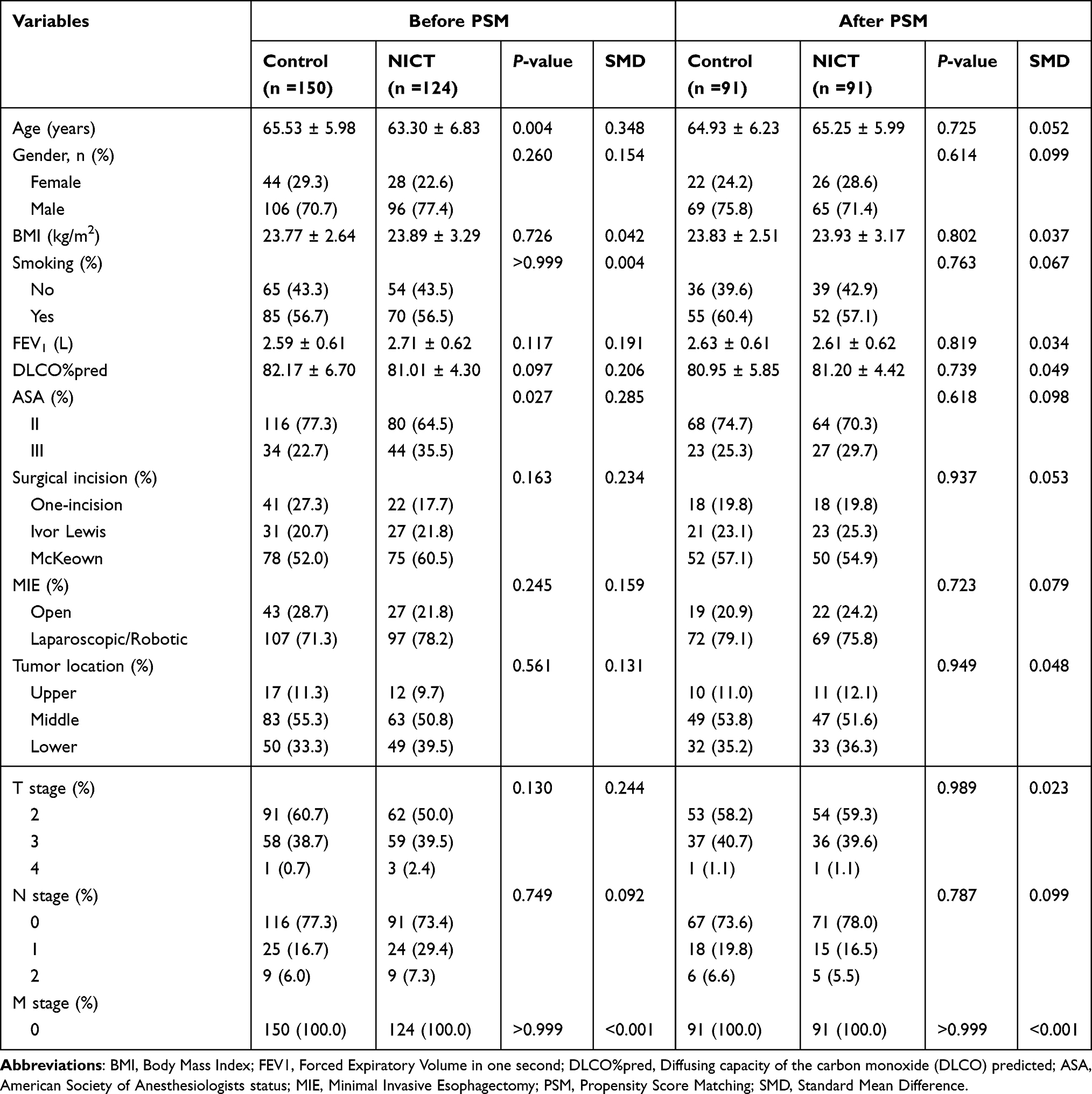 |
Table 1 Baseline Characteristics of Enrolled Patients |
The Love plot, a critical tool for assessing the effectiveness of PSM, visually demonstrated the balance achieved between the treatment and control groups. The plot revealed that SMD values for all covariates were less than 0.1 after matching, indicating a successful balance between the groups (Figure 2). Specifically, for age, gender, FEV1, ASA classification, surgical incision, MIE, tumor location, and clinical T stage, SMD values were greater than 0.10 before matching but less than 0.10 after matching. This finding confirms that PSM effectively mitigated the differences between the two groups for these covariates. The improved balance of each covariate after matching enhanced the credibility of our findings and underscored the robustness of our matching method in controlling for confounders.
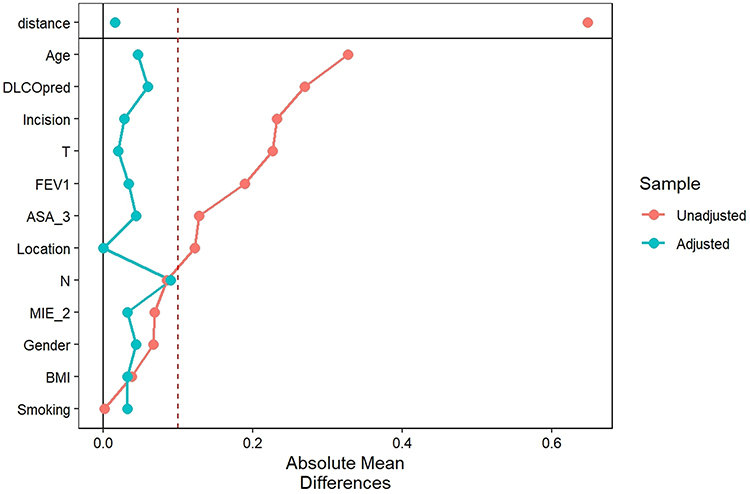 |
Figure 2 Covariate balance before and after propensity score matching. Orange circles: Unadjusted differences (pre-matching). Blue circles: Adjusted differences (post-propensity score matching). Abbreviations: FEV₁, forced expiratory volume in 1 second; ASA, American Society of Anesthesiologists; MIE, minimally invasive esophagectomy. |
Intraoperative Outcomes
Among the 182 propensity score–matched patients, all underwent radical esophagectomy, and no intraoperative deaths were reported. Compared with the control group, the NICT group had a higher total intraoperative fluid output (median 700 mL [IQR, 600–970 mL] vs 620 mL [IQR, 500–850 mL]; P = 0.007; Table 2). The NICT group also had a greater median blood loss (260 mL [IQR, 200–300 mL] vs 200 mL [IQR, 150–200 mL]; P < 0.001; Table 2) and a higher incidence of patients requiring red blood cell (RBC) transfusion (11.0% vs 1.1%; P = 0.013; Table 2). Additionally, the duration of surgery and anesthesia was significantly longer in the NICT group (surgery, P = 0.011; anesthesia, P = 0.017).
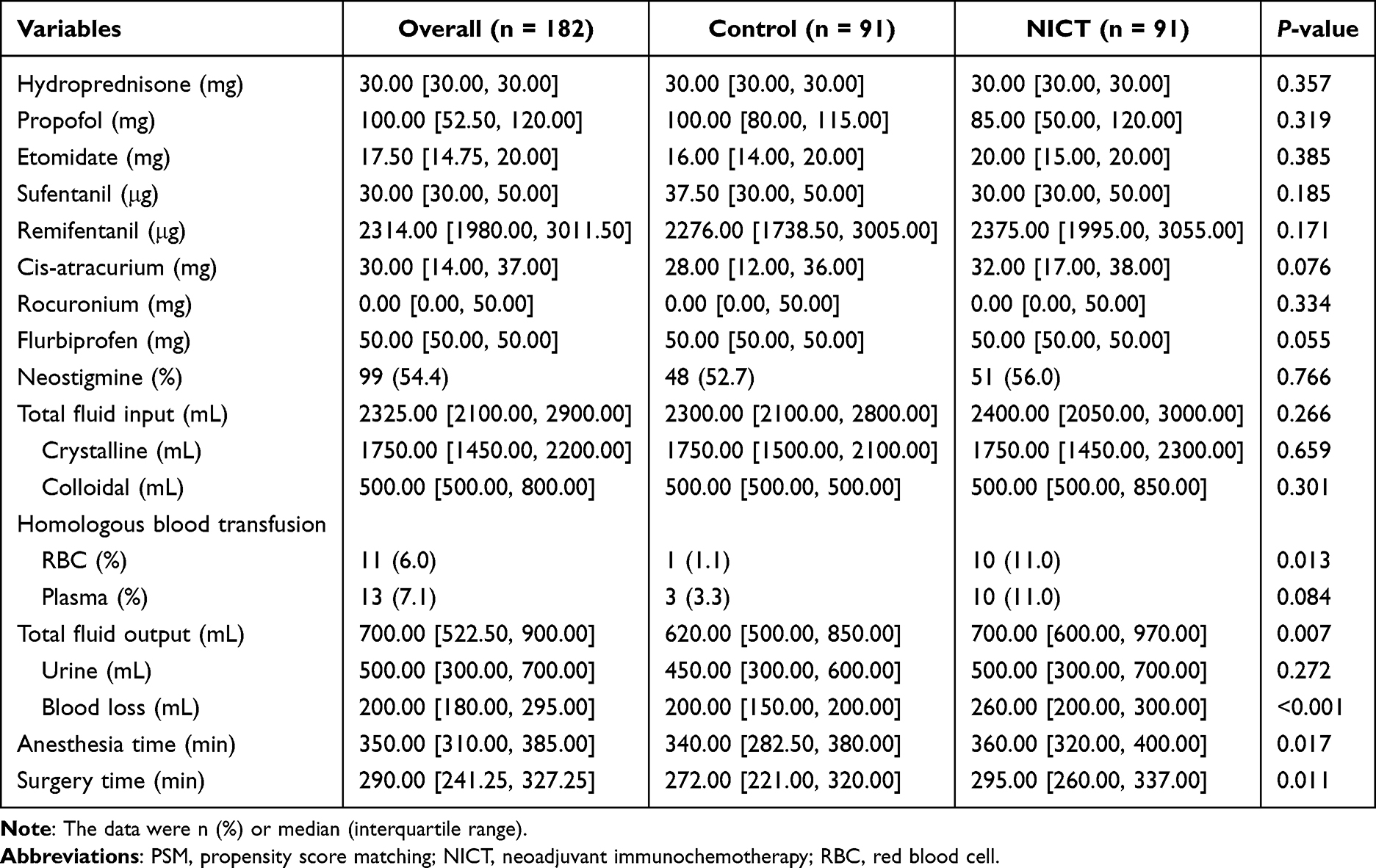 |
Table 2 Intraoperative Data of PSM Patients |
Primary Outcome
Among the postoperative complications, pulmonary complications were the most prevalent, with an overall incidence of 36.3%. The proportion of patients who experienced composite PPCs within seven days after radical esophagectomy was significantly higher in the NICT group than in the control group (46.2% vs 26.4%, P = 0.009; Table 3). Among the individual pulmonary complications, the incidence of respiratory infections (37.4% vs 22.0%, P = 0.035) and pleural effusions (22.0% vs 9.9%, P = 0.043) were significantly higher in the NICT group than in the control group. Other pulmonary complications, including respiratory failure (7.7% vs 7.7%, P > 0.999), atelectasis (13.2% vs 9.9%, P = 0.643), and pneumothorax (2.2% vs 2.2%, P > 0.999), were not significantly different. Thoracoabdominal two-incision Ivor-Lewis and three-incision McKeown surgeries accounted for 80% of the included procedures. PPCs were a composite indicator, with many individual patients experiencing multiple pulmonary complications. These findings demonstrate the high incidence of PPCs following radical esophagectomy.
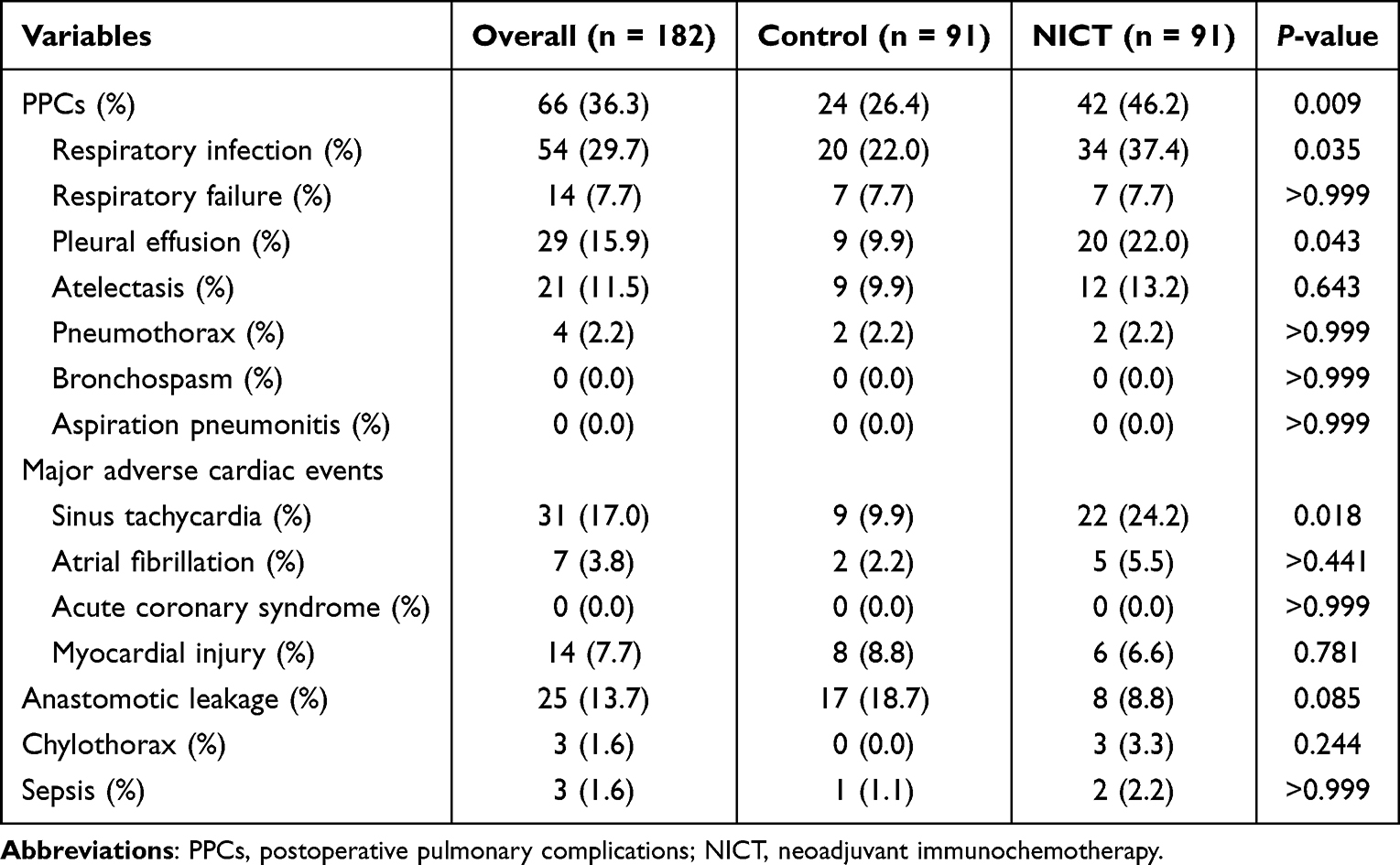 |
Table 3 Postoperative Outcomes |
Second Outcomes
New-onset arrhythmia was the most common cardiovascular complication, with tachycardia occurring in 24.2% of patients in the NICT group compared to 9.9% in the control group (P = 0.018). The incidence of atrial fibrillation was similar between the groups (5.5% vs 2.2%, P > 0.441). Myocardial injury occurred in eight patients (8.8%) in the control group and six patients (6.6%) in the NICT group. The incidence of anastomotic leakage and chylothorax was similar between the two groups. Sepsis was observed in two patients in the NICT group and one patient in the control group (Table 3).
Association of NICT with PPCs
We conducted conditional logistic regression analyses to examine the association between NICT and PPCs using multivariable models designed to adjust for potential confounding factors. Model 1 was unadjusted for covariates. Model 2 included adjustments for intraoperative variables (cis-atracurium, total fluid input, red blood cell transfusion, total fluid output, blood loss, anesthesia duration, and surgery duration). Model 3 incorporated a more comprehensive set of covariates, including an interaction term (anesthesia duration × surgery duration), to account for confounding factors.
In the unadjusted analysis (Model 1), NICT exposure was significantly associated with a substantial increase in the odds of developing PPCs (OR = 2.636, 95% CI: 1.317–5.277, P = 0.006). In the multivariate analysis, after adjusting for intraoperative variables (Model 2), the NICT group had significantly higher odds of developing PPCs than the control group (adjusted OR = 4.829, 95% CI: 1.430–16.311, P = 0.011). This association persisted in Model 3 after additional adjustment for the interaction term (anesthesia duration × surgery duration), with an adjusted OR of 5.648 (95% CI: 1.579–20.204, P = 0.008), indicating robust evidence of increased PPCs risk associated with NICT (Table 4).
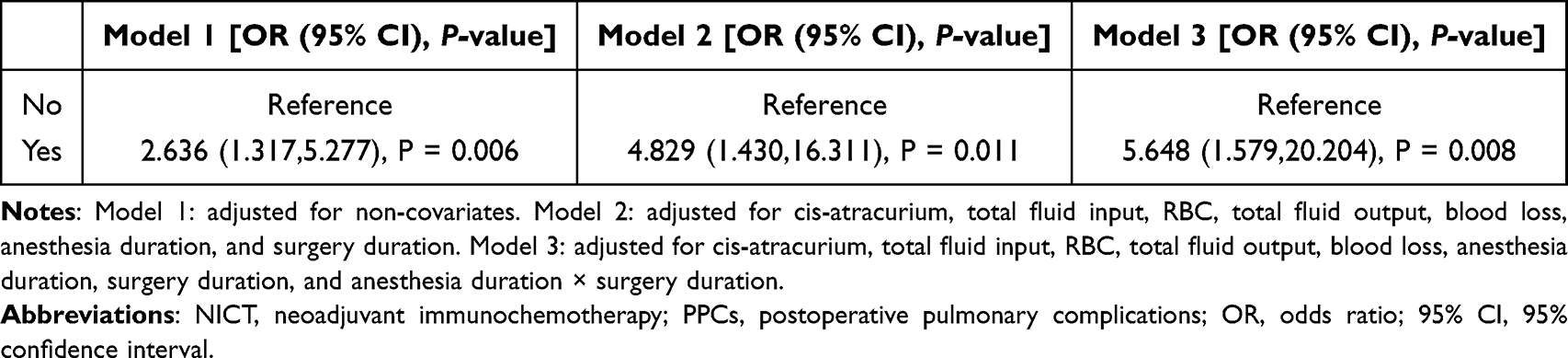 |
Table 4 Association Between NICT and PPCs |
Statistical model selection using both the AIC and BIC criteria consistently identified the final model. The analysis revealed NICT as a statistically significant independent predictor (β = 1.162, SE = 0.294; P < 0.0001), demonstrating an odds ratio of 3.20 (95% confidence interval: 1.80–5.68). This indicates that patients in the intervention group exhibited 3.2-fold greater odds of developing PPCs than those the in control group. Furthermore, total fluid output showed a modest yet statistically significant positive association (β = 0.0011; P = 0.038), suggesting a small but measurable increase in PPCs risk per unit increase in output. The robustness of this model was confirmed by its consistent selection across varying penalty parameters, including stringent BICq adjustments (q > 0.83). This finding suggests that the inclusion of both treatment status and total fluid output variables achieves an optimal balance between model explanatory power and parsimony, even under conditions favoring more conservative model specifications.
Sensitive Analysis
To further assess the robustness of our findings, we employed Inverse Probability of Treatment Weighting (IPTW) to form two new groups of samples. The original data were weighted by the inverse probability of treatment, and weighted averages were used to equalize baseline imbalances between the groups (Figure 3). Weighted multivariable-adjusted logistic regression analysis, incorporating the same covariates as in Model 3, revealed that the association between NICT and PPCs remained robust (OR 2.893, 95% CI: 1.537–5.446, P = 0.001).
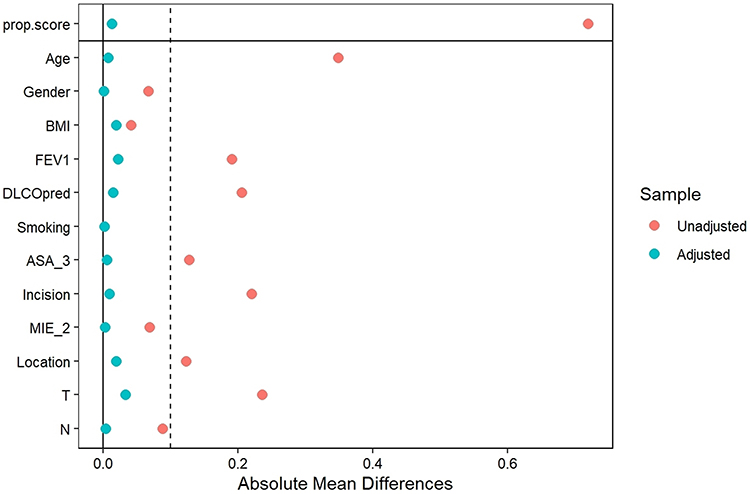 |
Figure 3 Assessment of Covariate Balance Before and After Adjustment. Balance was achieved through propensity score matching incorporating all listed covariates. Abbreviations: FEV₁, forced expiratory volume in 1 second; ASA, American Society of Anesthesiologists; MIE, minimally invasive esophagectomy. |
Subgroup Analyses
Subgroup analyses were conducted to investigate the association between various factors and PPCs incidence. The results indicated that patients aged ≥65 years (OR 2.690, 95% CI 1.204–6.009), males (OR = 2.120, 95% CI 1.032–4.355), and those undergoing McKeown surgery (OR 2.398, 95% CI 1.082–5.318) had a higher incidence of PPCs (Figure 4).
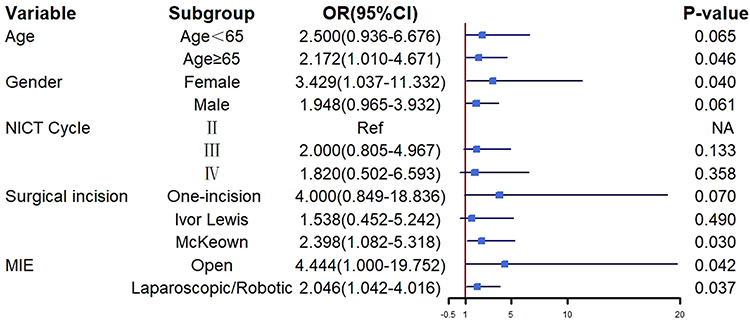 |
Figure 4 Forest plot of subgroup analyses. Abbreviations: NICT, neoadjuvant immunochemotherapy; MIE, minimally invasive esophagectomy. |
Discussion
Our findings showed that administering at least two cycles of neoadjuvant immunochemotherapy significantly increased the risk of postoperative pulmonary complications in patients with locally advanced esophageal cancer undergoing radical esophagectomy. After adjusting for multiple confounders, the risk of developing PPCs remained higher in the NICT group than in the non-NICT group. Sensitivity analysis confirmed the robustness of these results.
Neoadjuvant chemoradiotherapy, as established by the CROSS trial, has been the standard treatment for LAEC, with chemotherapy being more prevalent.27 Despite significant survival benefits, most patients still experience postoperative recurrence, primarily due to distant metastases.3,4 The advent of immunotherapy has significantly impacted this paradigm, ushering in a new era of neoadjuvant immunotherapy. Studies have demonstrated the potential of combining immunotherapy and chemotherapy in the neoadjuvant setting. The KEYNOTE-590 study showed that pembrolizumab combined with chemotherapy significantly improved overall and progression-free survival in previously untreated LAEC.7 Similarly, the ESCORT-NEO study found that neoadjuvant camrelizumab combined with chemotherapy significantly increased the pathological complete response rate.5 In our study, the chemotherapy regimen in the NICT group was consistent with previous studies that utilized paclitaxel (PTX) or albumin-bound paclitaxel (nab-PTX), and platinum-based drugs. Immunotherapy was administered PD-1 immune checkpoint inhibitors (ICIs), including pembrolizumab, tislelizumab, camrelizumab, or sintilimab. This combination leverages the synergistic effects of chemotherapy and immunotherapy to enhance antitumor efficacy. In the current cohort, the majority of patients who did not receive neoadjuvant therapy were staged as clinical T2N0 (cT2N0). For cT2N0 esophageal cancer, there is no consensus regarding the optimal treatment strategy. A systematic review and meta-analysis by Mota et al concluded that neoadjuvant therapy does not confer a survival benefit over upfront surgery in this stage.11 Similarly, a contemporary study using the National Cancer Database found no differences in cancer-specific or overall survival between induction chemoradiotherapy and immediate resection for T2N0 disease.28 These findings suggest that while neoadjuvant therapy may improve tumor response rates, it does not significantly impact long-term survival in this specific subgroup of patients. Some patients with advanced disease, particularly those experiencing severe dysphagia, significantly impaired quality of life, or concerns about the adverse risks of neoadjuvant treatment, opted for direct surgical intervention.
In clinical practice, esophageal cancer treatment has transitioned from singular surgical approach to multidisciplinary comprehensive model. NICT has emerged as a crucial component in the management of LAEC. However, our findings suggested that NICT was significantly increases postoperative pulmonary complications compared to surgery alone, particularly respiratory infections (leukocytosis/fever) and intervention-requiring pleural effusions—consistent with known esophagectomy risks (40–80% pulmonary complications).29,30 We propose that multiple cycles of preoperative chemotherapeutic and immunological agents may exert varying degrees of impact on immune and lung function, effects that are not readily detectable through preoperative pulmonary function tests. For instance, cisplatin can induce lung cell damage and ciliary disruption by increasing oxidative stress.31 Paclitaxel and its derivatives, such as nanoparticulate nab-paclitaxel, can induce lung injury through multiple mechanisms,32 with the incidence of paclitaxel-induced pneumonitis ranging from 0.73% to 12.00%.33 Additionally, synchronized immunotherapy may have a more pronounced impact on the lungs, with immune-related pneumonia being the most common adverse event. Patients receiving PD-1 inhibitors are more likely to develop immune-related pneumonia, which can be life-threatening.34 The clinical manifestations of immune-related pneumonia include fever, cough, chest pain, dyspnea, and respiratory failure in severe cases. Imaging findings may indicate nonspecific interstitial pneumonia or cryptogenic organizing pneumonia.35 These effects can lead to increased capillary permeability and fluid accumulation in the pleural space, contributing to pleural effusion. The risk of acute respiratory failure was notably higher after invasive surgeries than after general surgical procedures, reaching 7.7% in the present study. These findings underscore the need for meticulous patient selection and tailored perioperative strategies to mitigate NICT-associated pulmonary morbidity while preserving therapeutic efficacy.
The association between NICT and increased PPCs underscores the importance of careful intraoperative management. Studies have revealed that muscle relaxants and increased fluid volumes lead to a higher incidence of PPCs.36 We further adjusted for the potential confounding effects of these intraoperative parameters using logistic regression. Our results indicate that while these factors contribute to PPCs risk, they do not fully account for the observed association between NICT and PPCs. Similarly, Zhang et al37 found that in patients with non-adenocarcinoma non-small cell lung cancer undergoing surgery after neoadjuvant therapy, the incidence of PPCs was 33.3%, and the operation time was longer in the immune checkpoint inhibitor group. Our findings highlight the importance of careful intraoperative management and perioperative care in LAEC patients receiving NICT.
Among postoperative cardiovascular complications, new-onset arrhythmias were the most common, particularly sinus and supraventricular tachycardias as well as atrial fibrillation. The incidence of new-onset supraventricular tachycardia was higher in patients who received NICT than in those who did not. This likely reflects the cardiotoxicity of antineoplastic agents. The 2022 European Society of Cardiology Guidelines on Oncology Cardiology characterize oncology-related cardiac insufficiency.38 Paclitaxel can induce arrhythmias, including bradycardia, heart block, and atrial fibrillation.39 Concurrent TP chemotherapy was an independent predictor of cardiac complication.13 Similarly, ICIs can cause myocarditis and arrhythmias, with clinical manifestations ranging from asymptomatic to severe symptoms, such as dyspnea, palpitations, and chest pain. Elevated troponin and natriuretic peptide levels are important diagnostic criteria for ICI-related myocarditis.40 Our study found that troponin or NT-proBNP levels were significantly elevated in patients with new-onset arrhythmias and heart failure.41 Although some biomarker elevations reflected postoperative inflammation/volume overload, these findings underscore the need for cardiovascular monitoring in NICT-treated patients.
Our findings revealed that patients treated with NICT exhibited a higher incidence of intraoperative bleeding than those who were not. The adverse effects of antineoplastic agents on the microvasculature and normal tissues are well documented and cannot be ignored. These agents can disrupt the delicate balance of the tumor microenvironment, leading to an increased risk of bleeding, impaired wound healing, and alterations in coagulation and platelet aggregation.42 Such effects may be exacerbated in the postoperative period, potentially leading to life-threatening complications. We encountered a case of pericardial tamponade in a patient with esophagogastric-junction carcinoma who underwent neoadjuvant immuno-chemotherapy followed by radical esophagectomy, underscoring the potential for rare yet life-threatening sequelae.43 Given these risks, enhanced perioperative management is essential for patients receiving NICT who require a higher level of care. Clinically feasible measures to prevent these complications should be explored in future studies.
NICT has emerged as a promising treatment for esophageal cancer, offering improved R0 resection rates and survival benefits. PD-1 enhances antitumor immunity by activating tumor-specific lymphocytes.44,45 However, this progress is accompanied by increased immune-related adverse events due to immune over-activation.46,47 These toxicities, including pneumonitis and cardiotoxicity, can significantly affect patient outcomes. Moreover, late-onset pulmonary sequelae are an emerging frontier in the safety profiling of NICT. Population-based pharmacovigilance and prospective registries now indicate that checkpoint-inhibitor pneumonitis may appear ≥90 days after the last ICI dose, with incidence rates as high as 19% and case-fatality exceeding 12% in real-world cohorts.48 Mechanistically, persistent alveolar T-cell activation and IL-1β/IL-17–driven epithelial–mesenchymal transition underpin this fibrotic cascade, suggesting a biological continuum between early post-operative inflammation and late structural lung damage. Our institutional follow-up program will be further studied in the future using high-resolution CT to capture these late events.
Perioperative risk mitigation after NICT requires a deliberate, evidence-based bundle of interventions. Based on the ESMO Clinical Practice Guidelines49 and the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group,50 the recommend protocol: Preoperative window-Low-dose chest CT within 4 weeks to exclude sub-clinical checkpoint-inhibitor pneumonitis (CIP); any ground-glass infiltrate mandates pulmonology review and ≥4 weeks of steroid taper if ≥grade 2. Intraoperative bundle-Lung-protective ventilation and restrictive fluid strategy balanced crystalloid and Continuous neuromuscular monitoring to ensure complete reversal to attenuate aspiration risk in patients with prior ICI-related myositis. Postoperative surveillance- Daily chest X-ray and C-reactive protein for 5 days; any rise in oxygen requirement triggers immediate high-resolution CT and multidisciplinary review. Early mobilization and the I COUGH protocol (Incentive spirometry, Coughing, Oral care, Understanding, Getting out of bed, Head-of-bed elevation), which reduced PPCs with a multidisciplinary patient care program.51
A comprehensive approach is essential to address these challenges, including thorough patient education, close monitoring of disease progression, and intensified postoperative care to identify and manage complications. Optimal management requires multidisciplinary collaboration for early complication detection and tailored interventions, underscoring the need for research into personalized strategies that maximize efficacy and minimize adverse effects.
Our study had some limitations. First, this was a retrospective study conducted at a single center. Although PSM was performed to balance the demographic characteristics, the retrospective design at a single institution may have introduced selection bias. Therefore, external validation in other study settings is required to improve the generalizability of the results. Second, owing to the retrospective nature of the study, important outcome indicators such as pain, delirium, and quality-of-life scores were unavailable. Prospective studies are needed to investigate these aspects in patients receiving neoadjuvant immunochemotherapy. Third, further follow-up is needed to evaluate the long-term survival outcomes of patients for a comprehensive evaluation and analysis. Efforts should be made to extend follow-up in the future to evaluate long-term efficacy and survival benefits.
Conclusion
Patients with locally advanced esophageal cancer who receive at least two cycles of neoadjuvant immunochemotherapy appear to have an increased incidence of early postoperative pulmonary complications. Although NICT holds promise for improving oncologic outcomes, the potential for increased PPCs underscores the need for careful patient selection and enhanced perioperative management. These findings, derived from a retrospective analysis, are exploratory and require prospective validation to establish definitive clinical guidelines. Future prospective studies should focus on confirming these results and exploring strategies to mitigate the risk of PPCs while maximizing the oncologic benefits of NICT.
Abbreviations
LAEC, locally advanced esophageal cancer; NCT, neoadjuvant chemotherapy; NCRT, neoadjuvant chemoradiotherapy; NICT, neoadjuvant immunochemotherapy; PSM, propensity score matching; BMI, body mass Index; FEV₁, forced expiratory volume in 1 second; DLCO%pred, diffusing capacity of the carbon monoxide (DLCO) predicted. ASA, American Society of Anesthesiologists; MIE, minimally invasive esophagectomy. PPCs, postoperative pulmonary complications. OR, odds ratio. 95% CI: 95% confidence. RBC, red blood cell.
Ethics Approval and Declaration of Helsinki
The study was approved by the Ethics Committee of the Fourth Hospital of Hebei Medical University (2023KS180) and conducted according to the Declaration of Helsinki.
Acknowledgments
We would like to thank everyone who has helped with our research.
Author Contributions
Wei Du: Writing – original draft, Writing – review & editing, Visualization, Software, Methodology, Formal analysis, Conceptualization, Funding acquisition. Xi Qiao: Resources, Methodology, Validation, Investigation, Writing – review & editing. Jifang Yao: Methodology, Supervision, Writing – review & editing. Zhijiao Wang: Resources, Validation, Writing – review & editing. Yuanyuan Shi: Resources, Data curation, Writing – review & editing. Huiqun Jia: Supervision, Writing – review & editing, Project administration. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Medical Science Research Project of Hebei (No. 20230795).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Merkow RP, Bilimoria KY, Keswani RN, et al. Treatment trends, risk of lymph node metastasis, and outcomes for localized esophageal cancer. J Natl Cancer Inst. 2014;106(7):dju133–dju133. doi:10.1093/jnci/dju133
3. Eyck BM, van Lanschot JJB, Hulshof M, et al. Ten-year outcome of neoadjuvant chemoradiotherapy plus surgery for esophageal cancer: the randomized controlled CROSS trial. J Clin Oncol. 2021;39(18):1995–2004. doi:10.1200/jco.20.03614
4. Yang H, Liu H, Chen Y, et al. Neoadjuvant chemoradiotherapy followed by surgery versus surgery alone for locally advanced squamous cell carcinoma of the esophagus (NEOCRTEC5010): a Phase III multicenter, randomized, open-label clinical trial. J Clin Oncol. 2018;36(27):2796–2803. doi:10.1200/jco.2018.79.1483
5. Qin J, Xue L, Hao A, et al. Neoadjuvant chemotherapy with or without camrelizumab in resectable esophageal squamous cell carcinoma: the randomized Phase 3 ESCORT-NEO/NCCES01 trial. Nat Med. 2024;30(9):2549–2557. doi:10.1038/s41591-024-03064-w
6. Kojima T, Shah MA, Muro K, et al. Randomized phase III KEYNOTE-181 study of pembrolizumab versus chemotherapy in advanced esophageal cancer. J Clin Oncol. 2020;38(35):4138–4148. doi:10.1200/jco.20.01888
7. Sun JM, Shen L, Shah MA, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet. 2021;398(10302):759–771. doi:10.1016/s0140-6736(21)01234-4
8. van der Wilk BJ, Eyck BM, Wijnhoven BPL, et al. Neoadjuvant chemoradiotherapy followed by active surveillance versus standard surgery for oesophageal cancer (SANO trial): a multicentre, stepped-wedge, cluster-randomised, non-inferiority, phase 3 trial. Lancet Oncol. 2025;26(4):425–436. doi:10.1016/s1470-2045(25)00027-0
9. Verschoor YL, van de Haar J, van den Berg JG, et al. Neoadjuvant atezolizumab plus chemotherapy in gastric and gastroesophageal junction adenocarcinoma: the Phase 2 PANDA trial. Nat Med. 2024;30(2):519–530. doi:10.1038/s41591-023-02758-x
10. Muro K, Lordick F, Tsushima T, et al. Pan-Asian adapted ESMO clinical practice guidelines for the management of patients with metastatic oesophageal cancer: a JSMO-ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann Oncol. 2019;30(1):34–43. doi:10.1093/annonc/mdy498
11. Wang Z, Shao C, Wang Y, et al. Efficacy and safety of neoadjuvant immunotherapy in surgically resectable esophageal cancer: a systematic review and meta-analysis. Int J Surg. 2022;104:106767. doi:10.1016/j.ijsu.2022.106767
12. Kalata S, Singh B, Graham N, et al. Epidemiology of postoperative complications after esophagectomy: implications for management. Ann Thorac Surg. 2023;116(6):1168–1175. doi:10.1016/j.athoracsur.2023.09.004
13. Liang Z, Luo K, Wang Y, et al. Clinical and dosimetric predictors for postoperative cardiopulmonary complications in esophageal squamous cell carcinoma patients receiving neoadjuvant chemoradiotherapy and surgery. Ann Surg Oncol. 2023;30(1):529–538. doi:10.1245/s10434-022-12526-9
14. Nijbroek SG, Schultz MJ, Hemmes SNT. Prediction of postoperative pulmonary complications. Curr Opin Anaesthesiol. 2019;32(3):443–451. doi:10.1097/aco.0000000000000730
15. Fernandez-Bustamante A, Frendl G, Sprung J, et al. Postoperative pulmonary complications, early mortality, and hospital stay following noncardiothoracic surgery: a multicenter study by the perioperative research network investigators. JAMA Surg. 2017;152(2):157–166. doi:10.1001/jamasurg.2016.4065
16. Lin HS, Watts JN, Peel NM, Hubbard RE. Frailty and post-operative outcomes in older surgical patients: a systematic review. BMC Geriatr. 2016;16(1):157. doi:10.1186/s12877-016-0329-8
17. Mallaev M, Tsvetkov N, Simmen U, et al. A risk score to predict postoperative complications in patients with resectable non-small cell lung cancer. J Thorac Dis. 2025;17(3):1520–1530. doi:10.21037/jtd-24-1668
18. Sposato B, Scalese M, Milanese M, Scichilone N, Scala R, Perrella A. Smoking and obesity increase airway hyperesponsiveness risk in the elderly. Curr Aging Sci. 2016;9(4):284–294. doi:10.2174/1874609809666160413113604
19. Suresh K, Voong KR, Shankar B, et al. Pneumonitis in non-small cell lung cancer patients receiving immune checkpoint immunotherapy: incidence and risk factors. J Thorac Oncol. 2018;13(12):1930–1939. doi:10.1016/j.jtho.2018.08.2035
20. Rice TW, Patil DT, Blackstone EH. 8th edition AJCC/UICC staging of cancers of the esophagus and esophagogastric junction: application to clinical practice. Ann Cardiothorac Surg. 2017;6(2):119–130. doi:10.21037/acs.2017.03.14
21. Steward DJ. A simplified scoring system for the post-operative recovery room. Can Anaesth Soc J. 1975;22(1):111–113. doi:10.1007/bf03004827
22. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/eja.0000000000000118
23. Yan T, Liang XQ, Wang GJ, et al. Prophylactic penehyclidine inhalation for prevention of postoperative pulmonary complications in high-risk patients: a double-blind randomized trial. Anesthesiology. 2022;136(4):551–566. doi:10.1097/aln.0000000000004159
24. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
25. van Zuylen ML, Meewisse AJG, Ten Hoope W, et al. Effects of surgery and general anaesthesia on sleep-wake timing: CLOCKS observational study. Anaesthesia. 2022;77(1):73–81. doi:10.1111/anae.15564
26. Cheng H, Clymer JW, Po-Han Chen B, et al. Prolonged operative duration is associated with complications: a systematic review and meta-analysis. J Surg Res. 2018;229:134–144. doi:10.1016/j.jss.2018.03.022
27. Kitagawa Y, Ishihara R, Ishikawa H, et al. Esophageal cancer practice guidelines 2022 edited by the Japan esophageal society: part 1. Esophagus. 2023;20(3):343–372. doi:10.1007/s10388-023-00993-2
28. Speicher PJ, Ganapathi AM, Englum BR, et al. Induction therapy does not improve survival for clinical stage T2N0 esophageal cancer. J Thorac Oncol. 2014;9(8):1195–1201. doi:10.1097/jto.0000000000000228
29. Shirinzadeh A, Talebi Y. Pulmonary complications due to esophagectomy. J Cardiovasc Thorac Res. 2011;3(3):93–96. doi:10.5681/jcvtr.2011.020
30. Deana C, Vecchiato M, Azzolina D, et al. Effect on post-operative pulmonary complications frequency of high flow nasal oxygen versus standard oxygen therapy in patients undergoing esophagectomy for cancer: study protocol for a randomized controlled trial-OSSIGENA study. J Thorac Dis. 2024;16(8):5388–5398. doi:10.21037/jtd-24-575
31. Han YK, Kim JS, Jang G, Park KM. Cisplatin induces lung cell cilia disruption and lung damage via oxidative stress. Free Radic Biol Med. 2021;177:270–277. doi:10.1016/j.freeradbiomed.2021.10.032
32. Bielopolski D, Evron E, Moreh-Rahav O, Landes M, Stemmer SM, Salamon F. Paclitaxel-induced pneumonitis in patients with breast cancer: case series and review of the literature. J Chemother. 2017;29(2):113–117. doi:10.1179/1973947815y.0000000029
33. Vahid B, Marik PE. Pulmonary complications of novel antineoplastic agents for solid tumors. Chest. 2008;133(2):528–538. doi:10.1378/chest.07-0851
34. Chuzi S, Tavora F, Cruz M, et al. Clinical features, diagnostic challenges, and management strategies in checkpoint inhibitor-related pneumonitis. Cancer Manag Res. 2017;9:207–213. doi:10.2147/cmar.S136818
35. Naidoo J, Wang X, Woo KM, et al. Pneumonitis in patients treated with anti-programmed death-1/programmed death ligand 1 therapy. J Clin Oncol. 2017;35(7):709–717. doi:10.1200/jco.2016.68.2005
36. Kirmeier E, Eriksson LI, Lewald H, et al. Post-anaesthesia pulmonary complications after use of muscle relaxants (POPULAR): a multicentre, prospective observational study. Lancet Respir Med. 2019;7(2):129–140. doi:10.1016/s2213-2600(18)30294-7
37. Zhang H, Mao X, Xu J, et al. Risk factors for postoperative pulmonary complications in non-adenocarcinoma non-small cell lung cancer patients undergoing surgery after neoadjuvant therapy. Transl Lung Cancer Res. 2025;14(2):552–562. doi:10.21037/tlcr-2025-25
38. Lyon AR, López-Fernández T, Couch LS, et al. ESC guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43(41):4229–4361. doi:10.1093/eurheartj/ehac244
39. Han X, Zhou Y, Liu W. Precision cardio-oncology: understanding the cardiotoxicity of cancer therapy. NPJ Precis Oncol. 2017;1(1):31. doi:10.1038/s41698-017-0034-x
40. Puzanov I, Subramanian P, Yatsynovich YV, et al. Clinical characteristics, time course, treatment and outcomes of patients with immune checkpoint inhibitor-associated myocarditis. J Immunother Cancer. 2021;9(6):e002553. doi:10.1136/jitc-2021-002553
41. Mahmood SS, Fradley MG, Cohen JV, et al. Myocarditis in patients treated with immune checkpoint inhibitors. J Am Coll Cardiol. 2018;71(16):1755–1764. doi:10.1016/j.jacc.2018.02.037
42. Villanueva-Bueno C, Escudero-Vilaplana V, Collado-Borrell R, et al. Medication guide for the perioperative management of oral antineoplastic agents in cancer patients. Expert Opin Drug Saf. 2022;21(1):107–119. doi:10.1080/14740338.2021.1965990
43. Du W, Wang H, Shen J, Qiao X, Yao J, Li C. Cardiac tamponade, a rare complication of gastric cardia cancer resection after neoadjuvant chemotherapy combined with immunotherapy: a case report and literature review. Front Oncol. 2023;13:1189500. doi:10.3389/fonc.2023.1189500
44. Ai L, Xu A, Xu J. Roles of PD-1/PD-L1 pathway: signaling, cancer, and beyond. Adv Exp Med Biol. 2020;1248:33–59. doi:10.1007/978-981-15-3266-5_3
45. Munari E, Mariotti FR, Quatrini L, et al. PD-1/PD-L1 in cancer: pathophysiological, diagnostic and therapeutic aspects. Int J Mol Sci. 2021;22(10):5123. doi:10.3390/ijms22105123
46. Li C, Faiz SA, Boysen-Osborn M, Sheshadri A, Wattana MK. Immune checkpoint inhibitor-associated pneumonitis: a narrative review. West J Emerg Med. 2025;26(2):210–218. doi:10.5811/westjem.20305
47. Simbaqueba Clavijo C, Odaro O, Gandhi A, et al. Immunotherapy-related adverse events and clinical outcomes in adult solid-tumor patients admitted to an onco-hospitalist medicine service. Cancers. 2025;17(3):403. doi:10.3390/cancers17030403
48. Durbin SM, Zubiri L, Perlman K, et al. Late-onset immune-related adverse events after immune checkpoint inhibitor therapy. JAMA Network Open. 2025;8(3):e252668. doi:10.1001/jamanetworkopen.2025.2668
49. Haanen J, Obeid M, Spain L, et al. Management of toxicities from immunotherapy: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(12):1217–1238. doi:10.1016/j.annonc.2022.10.001
50. Puzanov I, Diab A, Abdallah K, et al. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J Immunother Cancer. 2017;5(1):95. doi:10.1186/s40425-017-0300-z
51. Cassidy MR, Rosenkranz P, McCabe K, Rosen JE, McAneny D. I COUGH: reducing postoperative pulmonary complications with a multidisciplinary patient care program. JAMA Surg. 2013;148(8):740–745. doi:10.1001/jamasurg.2013.358
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perioperative Risk Factors for Postoperative Pulmonary Complications After Minimally Invasive Esophagectomy
Li X, Yu L, Fu M, Yang J, Tan H
International Journal of General Medicine 2024, 17:567-577
Published Date: 15 February 2024
Promising Response to Neoadjuvant Chemotherapy Plus Immunotherapy in Metaplastic Breast Carcinoma
Tan Q, Li N, Wang Y, Du T, Liang G, Zhao Z, Tang J, Wu H
Breast Cancer: Targets and Therapy 2025, 17:447-454
Published Date: 23 May 2025