Back to Journals » Journal of Pain Research » Volume 19
Effect of Electroacupuncture on Postoperative Urinary Retention After Radical Hysterectomy for Cervical Cancer: Study Protocol for A Randomized Controlled Trial
Authors Lu C ![]() , Chen N, Sun H
, Chen N, Sun H ![]() , Wang C, Zhao L, Bao W, Deng D, Wang P
, Wang C, Zhao L, Bao W, Deng D, Wang P ![]() , Li X
, Li X
Received 26 January 2026
Accepted for publication 12 March 2026
Published 18 March 2026 Volume 2026:19 598960
DOI https://doi.org/10.2147/JPR.S598960
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Chao Lu,1 Nisang Chen,2 Haiju Sun,3 Chunlan Wang,4 Lingqin Zhao,4 Wenlong Bao,1 Dehou Deng,1 Peipei Wang,1 Xiaoyu Li2
1Department of Traditional Chinese Medicine, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2The Third Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 3Department of Acupuncture and Tuina, The First Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, People’s Republic of China; 4Department of Gynecological Oncology, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Chao Lu, Department of Traditional Chinese Medicine, Zhejiang Cancer Hospital, No. 1, East Banshan Road, Gongshu District, Hangzhou, Zhejiang, 310022, People’s Republic of China, Email [email protected] Xiaoyu Li, The Third Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310053, People’s Republic of China, Email [email protected]
Introduction: Postoperative urinary retention (POUR) is a prevalent complication following radical surgery for cervical cancer, significantly impairing patients’ quality of life. Electroacupuncture (EA) has shown potential benefits in alleviating POUR symptoms. However, its efficacy in some specific clinical contexts remains to be systematically evaluated.
Methods and Analysis: This is a prospective, single-blinded, single-center, randomized controlled trial designed to compare the efficacy of EA versus sham EA for POUR after radical cervical cancer surgery. A total of 208 patients with POUR after radical hysterectomy for cervical cancer will be randomly allocated to the EA group or the sham EA group at a 1:1 ratio. Participants in the EA group will receive EA treatment at a frequency of 5 sessions per week for 2 weeks, while those in the sham EA group will undergo sham EA interventions on the same schedule. The primary outcome will be the response rate of participants with successful urinary catheter removal. Secondary outcomes will include the changes in post-void residual (PVR) volume, assessment of urinary tract infection (UTI), and quality of life assessment according to the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-C30 (EORTC QLQ-C30) scale. All analyses will be conducted in accordance with the intention-to-treat principle.
Ethics/Dissemination: This study protocol was approved by the Medical Ethics Committee of Zhejiang Cancer Hospital on 20 October 2025 (approval number: IRB-2025-1315). The trial will evaluate the clinical efficacy and safety of EA on POUR after radical hysterectomy for cervical cancer. Results will be disseminated to the medical community through peer-reviewed publications and conference presentations to inform clinical practice.
Trial Registration: Registered on ClinicalTrials.gov with the identification number of NCT07253194 (https://register.clinicaltrials.gov/, 28 November 2025).
Keywords: electroacupuncture, EA, postoperative urinary retention, pour, cervical cancer, post-void residual, PVR, study protocol
Introduction
Cervical cancer is a prevalent malignant neoplasm, ranking fourth globally in terms of incidence among female malignancies. According to newly released data for 2022, there were approximately 660,000 new cervical cancer cases and 350,000 associated deaths worldwide that year.1 In China, with an estimated 150,000 new cases and 56,000 deaths attributed to cervical cancer in 2022.2 In the clinic, radical hysterectomy combined with pelvic lymphadenectomy is the preferred treatment for most cervical cancer patients.3 While surgical intervention significantly improves overall survival rates, the procedure inherently induces varying degrees of injury to pelvic nerves that innervate bladder and urethral function. This nerve damage frequently leads to secondary bladder dysfunction, manifesting in a spectrum of complications, among which postoperative urinary retention (POUR) is the most common.4,5 Reported incidence rates of POUR following cervical cancer surgery range widely, from 8% to 80%.6 The primary clinical manifestations include dysuria, inability to initiate micturition or complete bladder emptying, and significant post-void residual (PVR) volume. Notably, POUR in this patient population differs from other etiologies. Most cervical cancer patients exhibit postoperative debilitation, and many require adjuvant anticancer therapies (eg., radiotherapy and chemotherapy) after surgery. These adjuvant treatments further impair systemic function, hinder the recovery of bladder function, and ultimately contribute to prolonged POUR, significantly compromising patients’ quality of life.
At present, urinary retention is primarily managed with an indwelling urethral catheterization. However, long-term indwelling catheterization is associated with urethral trauma and an elevated risk of urinary tract infection (UTI).7,8 In clinical practice, healthcare providers commonly implement pelvic floor muscle exercise guidance and require patients to regularly clamp the urinary catheter to facilitate bladder function recovery in affected patients. These interventions, however, exhibit limited clinical efficacy and are often hindered by poor patient compliance. In recent years, intermittent clean self-catheterization (ICSC) has been increasingly adopted in the clinical care of POUR. It provides patients with more opportunities to exercise urination independently, while enabling dynamic monitoring of PVR volume, which can promote bladder function recovery to a certain extent.9 Notwithstanding these advantages, ICSC imposes high demands on patient cooperation and compliance, which can pose challenges for some elderly patients, especially those with low educational attainment or those with physical limitations that impair self-operation. Moreover, improper catheterization operation or prolonged ICSC use will inevitably increase the risk of UTI.10 Consequently, there is an urgent need for a safer, simpler, and more effective therapeutic regimen to facilitate recovery in patients with POUR.
In recent years, the traditional Chinese medicine (TCM) therapies have been extensively investigated for the management of POUR and have yielded promising preliminary results.11,12 As an invasive TCM intervention with low adverse effects and high safety profiles, acupuncture is also widely applied in the treatment of POUR associated with various surgical procedures.13,14 Electroacupuncture (EA), an intervention that integrates traditional acupuncture with modern electrical stimulation technology, exhibits notable advantages in the treatment of postoperative neurogenic bladder.15,16 Despite many reports indicating that acupuncture and EA can effectively alleviate POUR after cervical cancer surgery,17,18 these interventions have not been incorporated as recommended treatments in international guidelines for bladder dysfunction.19,20 Domestically, the expert consensus on POUR after radical hysterectomy notes that while acupuncture may be used for POUR following gynecologic oncology surgery, the supporting clinical evidence remains of low quality.21 Synthesizing prior literature and clinical experience, we acknowledge that acupuncture or EA may exhibit therapeutic potential for POUR after cervical cancer surgery. However, high-quality evidence from evidence-based medicine studies is still lacking. Therefore, we propose to conduct a prospective, blinded, randomized controlled trial to comprehensively validate the clinical efficacy of EA for POUR after radical hysterectomy for cervical cancer and generate preliminary evidence to address the current evidence gap.
Methods
Objective
To evaluate the effect of EA on POUR after radical hysterectomy for cervical cancer.
Trial Design
This study is a 2-arm parallel, participant-blinded, single-center, randomized controlled trial that will be conducted at the Zhejiang Cancer Hospital from January 1, 2026, to December 31, 2028. A total of 208 POUR participants will be recruited and randomly divided into two groups in a 1:1 ratio, namely the EA group and the sham EA group. The interventions will be delivered over 2 weeks, and the follow-up will be conducted 2 weeks after the last treatment. Figure 1 is a flowchart detailing the research process. In addition, Table 1 shows the trial schedule for enrollment, treatment, and outcome evaluation. The study will adhere to the CONSORT guidelines22 and the SPIRIT statement.23
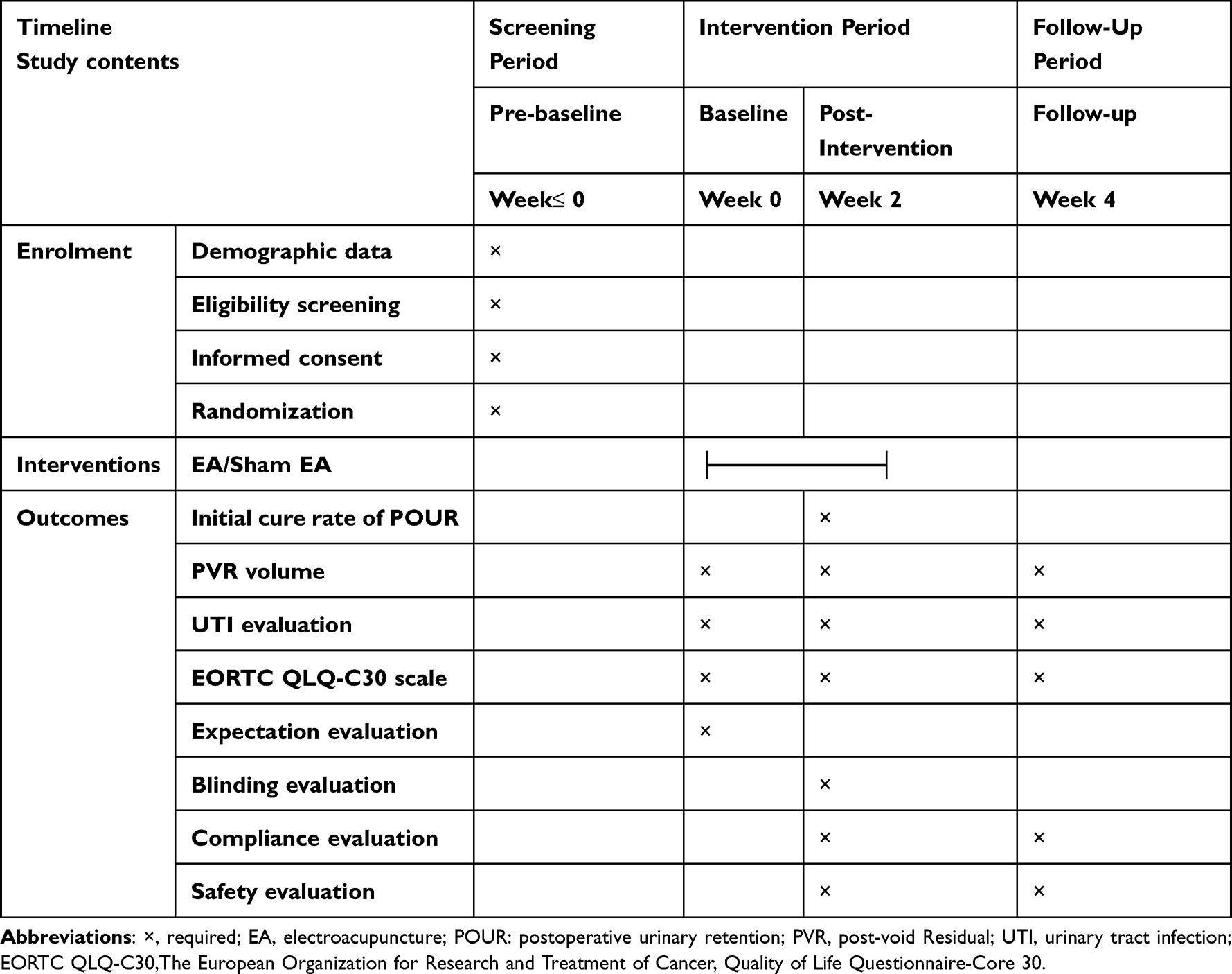 |
Table 1 Study Schedule of Enrolment, Interventions, and Outcomes |
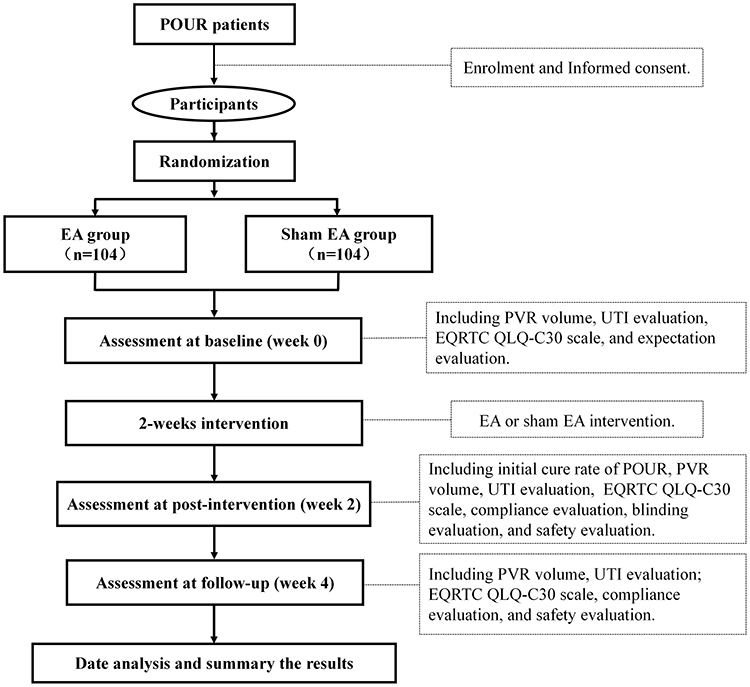 |
Figure 1 Flowchart of the trial. Abbreviations: POUR, Postoperative urinary retention; EA, Electroacupuncture; PVR, Post-void residual; UTI, Urinary tract infection; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30. |
Ethical Standards and Registration
The trial will be conducted in accordance with the principle of the Declaration of Helsinki. This protocol (version 1.0, 20250912) has been approved by the Medical Ethics Committee of Zhejiang Cancer Hospital on 20 October 2025 (approval number: IRB-2022-1315) and registered on ClinicalTrials.gov with the identification number of NCT07253194 (https://register.clinicaltrials.gov/, 28 November 2025).
Informed Consent
All POUR patients participating in the trial will have the right to obtain all relevant information about the trial, including benefits or potential risks, and they can participate according to their wishes. All participants will be allowed to drop out at any point in the trial. The information of participants will be kept confidential. All participants need to provide written informed consent if they are included in the trial.
Study Procedure
The duration of the trial will include three study phases, including screening in the baseline phase (week 0), a 2-week treatment phase (weeks 1–2), and a follow-up phase (week 4). The qualification of prospective participants will be determined by researchers who will not be involved in the intervention or assessment. At the screening meeting, patients will be given more detailed information about the study procedures. Before the first treatment (baseline, week 0), after the last treatment (post-treatment, week 2), and at the second week of follow-up after treatment (week 4), all participants will be required to complete several checks and questionnaires as the outcomes of the study to evaluate the efficacy and safety, including PVR volume test, urinalysis, EORTC QLQ-C30 questionnaires, and evaluation for expected value, blinding, compliance, and safety. The participants cannot take drugs that may influence the outcomes of the study during the trial, including diuretic drugs or unspecified POUR-related therapeutic drugs. If the patient has to take drugs that will influence the outcomes of the study due to disease progression, the patient will be considered to drop out. In order to promote enrollment, all treatment costs and outcome measurements will be free for participants.
Inclusion Criteria and Exclusion Criteria
The diagnosis of cervical cancer adopts the diagnostic criteria of the International Federation of Obstetrics and Gynecology (FIGO) for cervical cancer.24 POUR refers to the inability to urinate by oneself for more than 14 days after a radical hysterectomy or the PVR volume >100mL despite the ability to urinate by oneself.25
Cervical cancer patients who had been diagnosed with POUR will be eligible if they ① 18 to 70 years old; ② Anticipated survival of at least 6 months; ③ Met the diagnostic criteria for POUR of cervical cancer, and the duration of POUR is less than 6 months; ④ No serious urinary system disease in the past, and no urinary retention before operation; ⑤ Karnofsky functional status score (KPS) ≥70 points; ⑥ Stable vital signs, no serious mental illness, capable of daily living, able to cooperate in completing all treatments and examinations; ⑦ Voluntarily participate and sign a written informed consent form.
Exclusion criteria included the following: ① Obstructive urinary retention, such as urethral stricture or stones induced urinary system diseases; ② Merge other serious systemic diseases, and advanced cachexia patients; ③ Patients who are intolerant to electrical stimulation therapy, such as those with pacemakers installed; ④ With psychiatric disorder or severe cognitive impairment; ⑤ Severe skin damage, infection, and ulceration at the treatment site; ⑥ Those who are participating in other acupuncture or drug clinical trials.
Randomization and Allocation Concealment
Randomization will be conducted by a researcher who is not involved in outcome evaluation and statistical analysis. The dynamic randomization method will be conducted by the central random system to generate a random allocation sequence of 208 numbers and divide them into two groups in a 1:1 ratio: the EA group and the sham EA group. The acupuncturist will obtain a random number and the corresponding intervention method corresponding to the sequence number according to the participant’s visit order.
Blinding
This study will cause blindness to the participants. Participants will be informed that they have a 50% probability of being allocated to one of two intervention groups: the EA group or the sham EA group. For the sham EA intervention, acupuncture needles will be inserted shallowly at the same acupoints as those used in the EA group. This shallow needling will induce mild acupunctural pain in participants, while the current output intensity of the EA device will be 0. During the intervention sessions, all participants will lie in a prone position on a treatment bed in an individual treatment room. This positioning will prevent participants from visualizing the EA procedure performed on the lumbosacral region. Due to the special nature of acupuncture and EA operations, the acupuncture therapist cannot be blind to the intervention. However, they will not be involved in the outcome assessments or data analyses. The researcher who collects outcome data will be unaware of the group allocation of the participants.
Intervention
All the participants will receive the EA or sham EA intervention based on the conventional treatment. Conventional treatment: All participants will have indwelling catheters. During indwelling urinary catheterization, the catheter will be maintained unobstructed to avoid kinking, obstruction, and compression.
The EA Group
Participants will undergo EA treatment. Acupoint selection: Shenshu (BL23), Pangguanghu (BL28), Ciliao (BL32), Zhongliao (BL33), Huiyang (BL35), and Zhibian (BL54). Acupuncture procedure: Participants will be positioned prone. Disposable acupuncture needles (0.30 × 50 mm) will be vertically inserted into BL32, BL23, BL28, and BL35 at a depth of 40 ± 8 mm. The disposable acupuncture needle (0.45 × 75 mm) will be inserted into BL54 at a depth of 55 ± 10 mm, with the direction of insertion toward Shuidao (ST28). During the acupuncture procedure, participants will perceive a distinct sensation at the acupoints, characterized by sensations such as localized muscle soreness, numbness, or twitching. Acupoint localization will adhere to the national standard (GB/T 123456–2021), as detailed in Table 2 and shown in Figure 2. EA application: EA will be applied to the BL32 and BL54 points on both sides of the spine at a frequency of 2 Hz and a stimulation intensity of 2 ± 1.5 mA (current delivery cannot pass through the midline of the spine). The intensity of stimulation is such that the patient can feel muscle vibrations but no obvious pain. Each treatment will last for 30 minutes, 5 days per week, for 2 consecutive weeks. Follow-up will be performed 2 weeks after the final treatment.
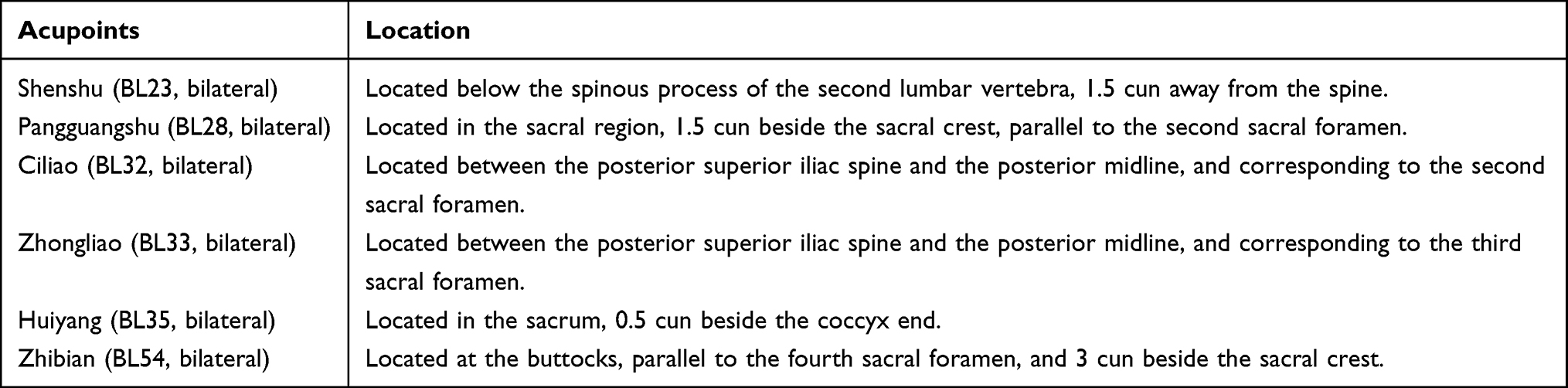 |
Table 2 Location of Acupoints |
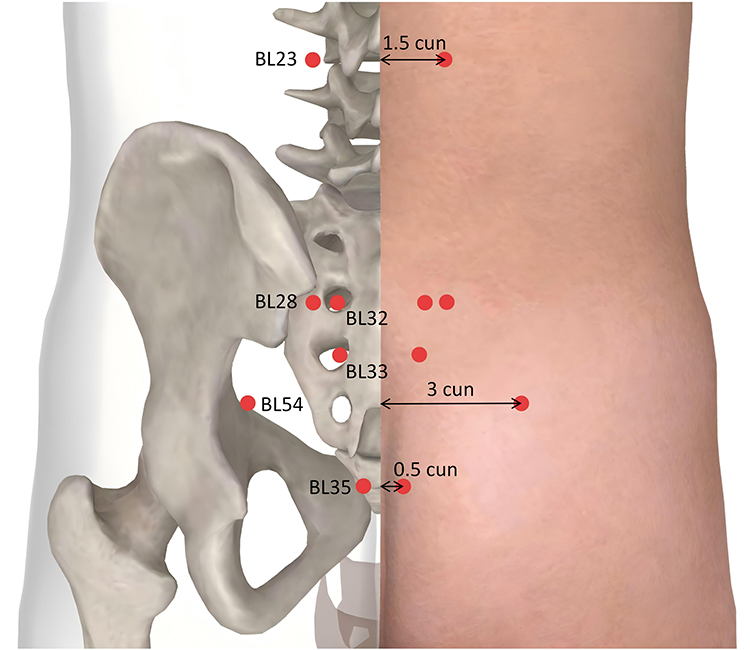 |
Figure 2 The location of acupoints. Notes: BL23, Shenshu point, bilateral; BL28, Pangguangshu point, bilateral; BL32, Ciliao point, bilateral; BL33, Zhongliao point, bilateral; BL35:Huiyang point, bilateral; BL54, Zhibian point, bilateral. The detailed positioning description can be seen in Table 2. The electroacupuncture group and the sham electroacupuncture group will use the same acupoints but will apply acupuncture to the skin at different depths. BL32 and BL54 will be connected via electroacupuncture or sham electroacupuncture. |
The Sham EA Group
Participants will receive sham EA treatment. Acupoint selection: consistent with the EA group. Sham acupuncture procedure: The disposable acupuncture needle (0.25 × 40 mm) will be used, and all acupoints will be shallowly penetrated into the skin using a vertical method, with a needle depth of 5 ± 2 mm (the needle body can remain vertical). With mild needle pain, no characteristic response sensation will be induced. Sham EA application: EA electrodes will be attached identically to the EA group at a frequency of 2 Hz and a nominal intensity of 2 mA. However, no electrical current will be delivered via the EA device, as the connecting wires will undergo specialized modification to preclude the formation of a closed electrical circuit. Each treatment session will also last 30 minutes, 5 days per week, for 2 consecutive weeks. The Follow-up will also be performed 2 weeks after the final treatment.
Equipment: Disposable acupuncture needles (Hwato brand, produced by Suzhou Medical Instrument Factory) with the specifications of 0.25 × 40 mm, 0.30 × 50 mm, and 0.45 × 75 mm will be used. The EA device employed will be the Hans-200E model, produced by Nanjing Jisheng Medical Technology Co., Ltd. All interventions will be performed by 3 licensed acupuncturists with at least 10 years of clinical experience, and every participant will receive EA or sham EA by the same acupuncturist throughout the trial.
Outcome Measures
After enrollment, all participants will complete a baseline evaluation at week 0. This assessment will include the collection of basic demographic data and medical history, such as age, height, weight, surgical approach, duration of POUR illness (ie., indwelling catheter duration), the recent PVR volume, the presence of UTI, participant expectations evaluation regarding EA treatment, and any special considerations. The primary outcome will be the response rate among participants who removed their urinary catheters after the intervention. Secondary outcomes include the changes in PVR volume, assessment of UTI, and evaluation of patient quality of life according to the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC QLQ-C30) scale.26 And the scale will be linearly converted into standardized scores ranging from 0 to 100 for comparative analysis.27
Primary Outcome
The response rate of participants who will successfully remove the urinary catheter, which will be defined as the participants in each group who will remove their urinary catheters after intervention (week 2), in proportion to the total number of patients in each group, multiplied by 100%. It can also be understood as the initial cure rate of POUR. The standard for patients to remove the urinary catheter is that the PVR volume is less than 100mL, with no obvious discomfort during urination.28
Secondary Outcomes
Other Outcomes
At baseline (week 0), all participants will complete an assessment of their expectations regarding the EA intervention on POUR. Following the completion of the intervention (week 2), the blinding evaluation will be performed for all participants. At 2 weeks post-intervention (week 4), all participants will undergo follow-up to assess for recurrence of POUR based on clinical manifestations. Participants reporting urinary symptoms, including dysuria, frequent urination, urinary urgency, or incomplete bladder emptying, will undergo repeat measurements of PVR volume and UTI. Recurrence of POUR will be defined as PVR volume >100 mL, requiring further clinical intervention. For participants diagnosed with UTI, antibacterial therapy or other targeted treatments will be administered per clinical judgment. During follow-up, assessments of quality of life (using the EORTC QLQ-C30) will also be performed. The compliance assessment of participants will be conducted throughout the entire study period.
Safety Evaluation
All adverse events (AEs) occurring during the study will be documented, including acupuncture- and EA-related AEs (eg., severe needling pain, subcutaneous hematoma, dizziness, nausea, and fainting). For each AE, the time of onset, management provided, outcome, follow-up details, and decision regarding whether the participant’s continued trial participation will be recorded. Additionally, quality of life assessments will also be incorporated as safety evaluation indicators.
Quality Control
All acupuncturists and evaluators will complete specialized training before trial initiation to ensure standardized practices. Training content will encompass the diagnosis of POUR, inclusion and exclusion criteria, intervention protocols (including acupoint localization, EA, and sham EA procedural details), and case report form (CRF) evaluation criteria. All study data will be documented in CRFs and entered into an electronic data capture system by independent researchers and will be verified by another independent researcher. Participant dropouts will be tracked throughout the trial. The trial will be monitored by the Clinical Research Department of Zhejiang Cancer Hospital every half year. The monitoring team will be responsible for data oversight and verification of consistency between source data and recorded data, ensuring the accuracy and quality of study data throughout the trial period.
Statistical Methods
Sample Size
This is a prospective randomized controlled trial with a 1:1 allocation ratio, and the sample size was determined via two-sided hypothesis testing. Based on preliminary clinical trial data, the cure rate was 78.4% in the EA group and 47.0% in the conventional treatment group. Assuming a 10% improvement in the cure rate with sham EA (placebo acupuncture) based on conventional treatment, the expected cure rate in the sham EA group will be 57.0%. Sample size calculation was performed using PASS 15 software with Tests for Two Proportions by using Fisher’s Exact Test, a significance level (α) of 0.05, and a statistical power of 0.80. For the comparison of two independent proportions, the calculated sample size was 83 participants per group. Accounting for a 20% dropout rate, the final sample size was adjusted to 104 participants per group, resulting in a total of 208 patients to be enrolled.
Statistical Analysis
De-identified outcome data will be analyzed by a statistician blinded to group assignments using IBM SPSS Statistics (Version 26.0, IBM, USA). All analyses will be based on the intention-to-treat (ITT) population. Continuous data will be represented by the mean (standard deviation, SD) or the median (interquartile range, IQR), and categorical data as frequencies and percentages. Independent samples t-tests will be used to compare normally distributed continuous variables between the two groups. Paired samples t-tests will assess changes from baseline to post-intervention and during follow-up within each group. Nonparametric tests (Mann–Whitney U-test for between-group comparisons, Wilcoxon signed-rank test for within-group comparisons) will be employed for non-normally distributed continuous variables. Missing data will be addressed via the last observation carried forward (LOCF) method or multiple imputation, with the specific approach determined based on the pattern and mechanism of missingness. Blind evaluation will use the BANG Bling index, performed by R, version 4.2.3 (R Foundation for Statistical Computing). All statistical tests will be two-sided, with a pre-specified significance level of 0.05.
Discussion
POUR following cervical cancer surgery is primarily attributed to injury to the bladder detrusor muscle, urethral sphincter, and pelvic autonomic nerves during radical hysterectomy and pelvic lymphadenectomy.33 Surgical manipulation disrupts pelvic floor support structures, leading to loss of the bladder’s anatomical stability, bend excessively backward, and the formation of an acute angle between the bladder’s posterior wall and urethra, resulting in the accumulation of urine in the bladder, which is difficult to discharge. Additionally, overextension of the bladder due to postoperative pelvic hematoma, inflammation, and adhesions can also lead to short-term bladder paralysis. Furthermore, patients’ emotional distress and pain after surgery can also impact bladder function and increase the incidence of POUR.34 Indwelling urinary catheterization is commonly used to manage urinary retention, but it carries a risk of UTI and may hinder the recovery of autonomous micturition. Beyond infectious risks, long-term indwelling catheterization severely disrupts patients’ daily living and social activities; over time, this functional limitation often leads patients to significant anxiety, further diminishing overall quality of life. Thus, early catheter removal is critical to not only promoting bladder function recovery but also mitigating their psychosocial and functional burdens.
Current therapeutic strategies for POUR include pharmacological interventions and physical therapy. Pharmacological approaches primarily involve parasympathomimetic agents (eg, neostigmine and cisapride) aimed at enhancing bladder detrusor contraction and improving bladder tone.6,35 However, these medications have limited efficacy and are associated with adverse effects.36 On the other hand, physical therapy modalities such as bladder training and the CISC method are more widely utilized in clinical practice.37 Recommended as the “gold standard” by the International Continence Society for managing neurogenic bladder, CISC alleviates chronic urinary retention of diverse etiologies.38 Nevertheless, CISC requires high levels of patient cooperation and compliance. Improper operation or prolonged CISC use can also increase the risk of urinary system infections. In contrast, acupuncture and EA, which are the external therapies of TCM characterized by low risk and good safety, have been widely applied in the management of POUR arising from various etiologies.13 Neurogenic bladder dysfunction was listed as a condition with remarkable curative effects when treated with acupuncture in the World Health of Acupuncture Special Issue, which was published by the World Health Organization (WHO) in 1980.39 The domestic expert consensus on POUR after radical hysterectomy has also acknowledged acupuncture as a treatment option, supported by numerous clinical trials.21 However, robust evidence from high-quality clinical trials remains lacking to fully validate its efficacy and safety in some specific populations. Although acupuncture or EA may exhibit therapeutic potential for POUR after cervical cancer surgery, high-quality evidence from evidence-based medicine studies is still lacking. Therefore, we will conduct this trial to comprehensively validate the clinical effect of EA for POUR.
In this clinical trial, we focused on optimizing the intervention acupoints. Previous literatures have summarized the acupoint selection rules for POUR treatment, indicating that Zhongji (RN3), Guanyuan (RN4), Sanyinjiao (SP6), Ciliao (BL32), Pangguangshu (BL28), Shenshu (BL23), Yinlingquan (SP9), Shuidao (ST28), Zhibian (BL54), and Qihai (RN6) are the most frequently used acupoints.18,40 However, these acupoints are distributed across the lumbar, abdominal, and lower limb regions, precluding simultaneous needle insertion. This requires patients to reposition during treatment, which significantly prolongs each treatment session duration and may induce patient fatigue. Additionally, excessive acupoint selection can increase the pain associated with acupuncture. Nevertheless, several clinical studies have demonstrated that simplified acupuncture using only lumbosacral acupoints can effectively treat POUR.41,42 Our clinical practice found that acupuncture targeting lumbosacral acupoints (BL23, BL28, BL32, BL33, BL35, and BL54) achieved favorable therapeutic effects, with no significant difference in efficacy compared to the traditional comprehensive acupoint selection scheme (encompassing lumbar, sacral, abdominal, and lower limb regions). This evidence justifies the focus on optimized lumbosacral acupoint selection in the current trial, with the goal of balancing efficacy, patient comfort, and treatment feasibility.
The selection of specific lumbosacral acupoints in this trial is further supported by clinical evidence, anatomical mechanisms, and TCM theory. Specifically, multiple studies have indicated that EA at the “Baliao” points (including BL31, BL32, BL33, and BL34) could effectively treat POUR;42,43 even single acupuncture at BL32 could achieve satisfactory outcomes.41,44 Anatomically, the “Baliao” points correspond to the four pairs of sacral posterior foramina, adjacent to detrusor muscle neurons, striated muscle neurons, where the sacral pulp urination center is. The parasympathetic fibers of the anterior branch of the sacral nerve, distributed below these acupoints, participate in the formation of the pelvic visceral nerve, which innervates the detrusor muscle of the bladder, inhibits the urethral sphincter, and plays a crucial role in regulating urination function. Additionally, the pudendal nerve, originating from the anterior horn motor neurons of the S2-S4 spinal cord segments, controls urination by modulating the contraction and relaxation of the external bladder sphincter. BL54 was also selected as a key acupoint for EA stimulation in this trial. Previous reports have confirmed the efficacy of acupuncture at BL54 in treating neurogenic bladder disorders (eg., urinary retention and urinary incontinence),45,46 and improving bladder function in controlling urine.47 Notably, the “Zhibian point through Shuidao point” needling technique, which means acupuncture BL54 towards ST28, is specifically indicated for treating urinary retention.48 From a TCM perspective, POUR is primarily attributed to dysfunction of bladder gasification dysfunction. The kidney and bladder are considered “exterior-interior related” in TCM theory; thus, acupuncture at BL23 (Shenshu, the back-shu point of the kidney) and BL28 (Pangguangshu, the back-shu point of the bladder) is believed to optimize the functional interplay between these two organs, thereby regulating bladder gasification function and improving urination symptoms. BL35 was included given as the crossing point of the Bladder Meridian and Du Meridian, with anatomical proximity to the levator ani tendon and pudendal nerve trunk. Acupuncture at BL35 can promote pelvic floor muscle recovery and modulate bladder function, making it one of the key acupoints for neurogenic bladder disorders.49
In this trial, the rate of urinary catheter removal was designated as the primary outcome, as successful catheter removal is a key clinical concern for POUR patients. In clinical practice, PVR volume < 100 mL with no absence of significant voiding discomfort is generally accepted as the minimum criterion for catheter removal in patients with POUR following radical hysterectomy for cervical cancer.28,30 Changes in bladder PVR volume after radical hysterectomy are directly associated with bladder function recovery. However, indwelling catheters postoperatively confer a risk of UTI; notably, receipt of radiotherapy during the catheterization period after radical hysterectomy markedly elevates this risk. Severe UTI often leads to disease progression, which further hinders catheter removal. Therefore, in this study, changes in bladder PVR and UTI assessment will be defined as secondary outcomes, and patient quality of life will be comprehensively evaluated using the EORTC QLQ-C30 scale. Previous studies have suggested that urodynamic testing can be performed in patients with urinary retention to assess recovery of bladder function.50,51 However, this test shares inherent commonality with PVR measurement; a reduction in PVR is inevitably accompanied by improvements in urodynamic parameters, whereas a large PVR is consistently indicative of detrusor dysfunction. Additionally, this invasive test is often associated with patient discomfort, including pain, embarrassment, and anxiety52, and most patients are unwilling to undergo it in clinical practice. Considering ethical principles, urodynamic testing is not deemed indispensable in this trial. In this trial, a blinding strategy will be implemented for all participants, with separation of intervention providers and outcome assessors to ensure allocation concealment. Additionally, we will evaluate the effect, blinding, participant compliance, and safety of the EA intervention, which serves to enhance the reliability of the study findings.
On the other hand, this study has several limitations. First, it is a single-center trial, and potential heterogeneity in population characteristics cannot be ruled out, which may introduce selection bias into the study results. Second, double-blinding of treatment cannot be achieved due to the inherent nature of acupuncture and EA interventions, precluding blinding of intervention providers, which is a well-recognized challenge in current acupuncture and EA clinical trials. Third, the absence of urodynamic testing precludes direct measurement of urine flow rate and bladder detrusor pressure, leading to incomplete assessment of outcome indicators. Fourth, the follow-up period is relatively short; although all participants were followed up at 2 weeks post-intervention, clinical practice indicates that a small subset of patients may experience disease recurrence months later. Despite these limitations, the findings of this study are expected to provide valuable insights for the clinical application of EA in the management of POUR after radical hysterectomy for cervical cancer.
The findings of this study will preliminarily determine the effect of EA on POUR after radical hysterectomy for cervical cancer, thereby providing evidence-based reference for clinical practice. It is anticipated that the result will contribute to improving POUR in patients after radical cervical cancer surgery and enhancing their quality of life.
Abbreviations
POUR, Postoperative urinary retention; EA, Electroacupuncture; PVR, Post-void residual; UTI, Urinary tract infection; ICSC, Intermittent clean self-catheterization; TCM, traditional Chinese medicine; ITT, Intention-to-treat; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30.
Data Sharing Statement
The study protocol and clinical study report data will be available upon reasonable request from the corresponding author Chao Lu ([email protected].) after publication.
Ethics Approval
Ethical approval was granted on 20 October 2025 by the Medical Ethical Committee of Zhejiang Cancer Hospital (license number: IRB-2025-1315) and registered on ClinicalTrials.gov with the identification number of NCT07253194 (https://register.clinicaltrials.gov/, 28 November 2025). Written informed consent will be obtained from all participants.
Acknowledgments
The authors appreciate the support from all participants who will be included in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work is supported by the Zhejiang Province Traditional Chinese Medicine Science and Technology Project (No.2026ZL0220).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2024;74(3):229–13. doi:10.3322/caac.21834
2. Zheng RS, Chen R, Han BF, et al. Cancer incidence and mortality in China, 2022. Zhonghua zhong liu za zhi Chin j oncol. 2024;46(3):221–231. doi:10.3760/cma.j.cn112152-20240119-00035
3. Kanao H, Fujiwara K, Ebisawa K, Hada T, Ota Y, Andou M. Various types of total laparoscopic nerve-sparing radical hysterectomies and their effects on bladder function. J Gynecol Oncol. 2014;25(3):198–205. doi:10.3802/jgo.2014.25.3.198
4. Cao TT, Wen HW, Gao YN, et al. Urodynamic assessment of bladder storage function after radical hysterectomy for cervical cancer. Chinese Med J. 2020;133(19):2274–2280. doi:10.1097/cm9.0000000000001014
5. Novackova M, Pastor Z, Chmel R Jr, Brtnicky T, Chmel R. Urinary tract morbidity after nerve-sparing radical hysterectomy in women with cervical cancer. Int Urogynecol J. 2020;31(5):981–987. doi:10.1007/s00192-019-04083-9
6. Plotti F, Angioli R, Zullo MA, et al. Update on urodynamic bladder dysfunctions after radical hysterectomy for cervical cancer. Crit rev oncol/hematol. 2011;80(2):323–329. doi:10.1016/j.critrevonc.2010.12.004
7. Lin YW, Lin YP, Chen YS. Comment on the safety and feasibility of no-placement of urinary catheter after single-port laparoscopic surgery in patients with benign ovarian tumor: a retrospective cohort study. Taiwanese J Obstetrics Gynecol. 2024;63(1):127. doi:10.1016/j.tjog.2023.03.018
8. Mengatto MF, Castro BGR, Nobrega L, et al. Early removal of indwelling urinary catheter after radical surgery for early-stage cervical cancer-A cohort study. J Surg Oncol. 2020;122(7):1498–1505. doi:10.1002/jso.26167
9. Fletke KJ, Jeong DH, Herrera AV. Urinary Catheter Management. Am Family Phys. 2024;110(3):251–258.
10. Fisher H, Oluboyede Y, Chadwick T, et al. Continuous low-dose antibiotic prophylaxis for adults with repeated urinary tract infections (AnTIC): a randomised, open-label trial. Lancet Infect Dis. 2018;18(9):957–968. doi:10.1016/s1473-3099(18)30279-2
11. Lin S-K, Lin P-H, Hsu R-J, Chuang H-C, Liu J-M. Traditional Chinese medicine therapy reduces the catheter indwelling risk in dementia patients with difficult voiding symptoms. J Ethnopharmacol. 2017;203:120–126. doi:10.1016/j.jep.2017.03.040
12. Huang KY, Liang S, Du HG, et al. Transcutaneous electrical acupoint stimulation for prevention of postoperative urinary retention: a systematic review. Heliyon. 2024;10(1):e23537. doi:10.1016/j.heliyon.2023.e23537
13. Zhao Q, Yan C, Dan M, Jia H. Efficacy and safety of acupuncture for urinary retention after hysterectomy: a systematic review and meta-analysis. Medicine. 2021;100(22):e26064. doi:10.1097/md.0000000000026064
14. Olia M, Jafarian A, Mohseni M. Efficacy of low-frequency electroacupuncture on urinary retention after spinal anesthesia. J PeriAnesthesia Nurs. 2023;38(5):745–747. doi:10.1016/j.jopan.2023.01.003
15. Tran PD, Nguyen QD, Ngo TD. Effectiveness of electroacupuncture for managing urinary retention post lumbar spine surgery: a retrospective single-cohort study. J. Pharmacopunct. 2024;27(2):123–130. doi:10.3831/kpi.2024.27.2.123
16. Zhang W, Song S, Zhang T, Ju X, Shu S, Zhou S. Electroacupuncture for urinary retention after stroke: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. 2024;57:101877. doi:10.1016/j.ctcp.2024.101877
17. Tan J, Gong R, Zhang Q, Zheng Y, Ma L, Shi S. Meta-analysis of clinical efficacy of electroacupuncture versus conventional treatment for postoperative urinary retention in cervical cancer. Medicine. 2023;102(43):e35580. doi:10.1097/md.0000000000035580
18. Guo Y, Pan H, Chen S, Tian M, Huang Y, Zhou Y. Effectiveness of acupuncture on urinary retention after radical hysterectomy for cervical cancer in China: a systematic review and meta-analysis. Front Med. 2024;11:1375963. doi:10.3389/fmed.2024.1375963
19. Sartori AM, Kessler TM, Castro-Díaz DM, et al. Summary of the 2024 update of the european association of urology guidelines on neurourology. Europ urol. 2024;85(6):543–555. doi:10.1016/j.eururo.2024.03.026
20. Ginsberg DA, Boone TB, Cameron AP, et al. The AUA/SUFU guideline on adult neurogenic lower urinary tract dysfunction: treatment and follow-up. J Urol. 2021;206(5):1106–1113. doi:10.1097/ju.0000000000002239
21. PX ZY, Weimin K, Yang X, Shiqian Z. Chinese expert consensus on comprehensive treatment for urinary retention after radical hysterectomy (2022 edition). Chin. J. Pract. Gynecol. Obstet. 2022;38(11):1111–1115. doi:10.19538/j.fk2022110112
22. Hopewell S, Chan AW, Collins GS, et al. CONSORT 2025 statement: updated guideline for reporting randomised trials. PLoS Med. 2025;22(4):e1004587. doi:10.1371/journal.pmed.1004587
23. Chan AW, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Internal Med. 2013;158(3):200–207. doi:10.7326/0003-4819-158-3-201302050-00583
24. FIGO staging for carcinoma of the vulva, cervix, and corpus uteri. Int J Obstet Gynaecol. 2014;125(2):97–98. doi:10.1016/j.ijgo.2014.02.003
25. McDermott CD, Tunitsky-Bitton E, Dueñas-Garcia OF, et al. Postoperative urinary retention. Urogynecology. 2023;29(4):381–396. doi:10.1097/spv.0000000000001344
26. Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J National Cancer Inst. 1993;85(5):365–376. doi:10.1093/jnci/85.5.365
27. Fayers PM, Aaronson NK, Bjordal K, Curran D, Grønvold M. The EORTC QLQ-C30 Scoring Manual. 3rd Edition. Eur Organisation for Res Treatment Cancer. 2001.
28. Chen GD, Lin LY, Wang PH, Lee HS. Urinary tract dysfunction after radical hysterectomy for cervical cancer. Gynecologic Oncol. 2002;85(2):292–297. doi:10.1006/gyno.2002.6614
29. Mainprize TC, Drutz HP. Accuracy of total bladder volume and residual urine measurements: comparison between real-time ultrasonography and catheterization. Am J Clin Exp Obstet Gynecol. 1989;160(4):1013–1016. doi:10.1016/0002-9378(89)90327-x
30. Chuang FC, Kuo HC. Management of lower urinary tract dysfunction after radical hysterectomy with or without radiotherapy for uterine cervical cancer. J Formos Med Assoc = Taiwan yi zhi. 2009;108(8):619–626. doi:10.1016/s0929-6646(09)60382-x
31. Shen Q, Deng D, Li G, et al. Electroacupuncture frequency for chemotherapy-induced neuropathy in breast cancer: a randomized controlled trial. Oncologist. 2025;30(9). doi:10.1093/oncolo/oyaf262
32. Lu C, Shen Q, Deng D, et al. Effects of electroacupuncture and mecobalamin for utidelon-induced peripheral neuropathy in breast cancer patients: a randomized controlled clinical trial. J Pain Res. 2025;18:3593–3608. doi:10.2147/jpr.S526405
33. Zullo MA, Manci N, Angioli R, Muzii L, Panici PB. Vesical dysfunctions after radical hysterectomy for cervical cancer: a critical review. Crit rev oncol/hematol. 2003;48(3):287–293. doi:10.1016/s1040-8428(03)00125-2
34. Wang J, Feng M, Liao T, et al. Effects of clean intermittent catheterization and transurethral indwelling catheterization on the management of urinary retention after gynecological surgery: a systematic review and meta-analysis. Transl Androlo Urol. 2023;12(5):744–760. doi:10.21037/tau-23-220
35. Madeiro AP, Rufino AC, Sartori MG, Baracat EC, Lima GR, Girão MJ. The effects of bethanechol and cisapride on urodynamic parameters in patients undergoing radical hysterectomy for cervical cancer. A randomized, double-blind, placebo-controlled study. Int Urogynecol Jo and Pelvic Floor Dysfunction. 2006;17(3):248–252. doi:10.1007/s00192-005-1318-1
36. Manchana T, Prasartsakulchai C. Bethanechol chloride for the prevention of bladder dysfunction after radical hysterectomy in gynecologic cancer patients: a randomized controlled trial study. Int J Gynecological Cancer. 2011;21(4):730–736. doi:10.1111/IGC.0b013e3181f7d6de
37. Aue-Aungkul A, Kietpeerakool C, Rattanakanokchai S, et al. Postoperative interventions for preventing bladder dysfunction after radical hysterectomy in women with early-stage cervical cancer. Cochrane Database Syst Rev. 2021;1(1):Cd012863. doi:10.1002/14651858.CD012863.pub2
38. Di Benedetto P. Clean intermittent self-catheterization in neuro-urology. Eur J Phys Rehabil Med. 2011;47(4):651–659.
39. Jinsheng H, Wang ZY, Jia L. What are the 43 diseases the World Health Organization (WHO) announced the promotion of acupuncture treatment? J Traditional Chin Med. 1989;9(08):57. doi:10.13288/j.11-2166/r.1989.08.034
40. Xu jianwen ZY, Hongling J. Analysis of acupoint selection rules for postoperative urinary retention after acupuncture treatment based on data mining technology. Liaoning J Tradit Chin Med. 2023;50(09):1–4. doi:10.13192/j.issn.1000-1719.2023.09.001
41. Gu SF, Li MQ, Li Y, Chen M, Han LL. Acupuncture at Ciliao (BL 32) for prevention of postpartum urinary retention in elderly parturient women: a randomized controlled trial. Zhongguo zhen jiu = Chin acupuncture & moxibustion. 40(6):611–614. doi:10.13703/j.0255-2930.20190528-k0005
42. Wu GF, Wang WM. Indication rules of Baliao points based on the clinical literature research. Zhongguo zhen jiu = Chinese acupuncture & moxibustion. 2019;39(1):96–102. doi:10.13703/j.0255-2930.2019.01.024
43. Wang XQ, Guan LS. Effect of percutaneous electrical stimulation at the Baliao point on preventing postpartum urinary retention after labor analgesia. World J. Clin. Cases. 2024;12(16):2758–2764. doi:10.12998/wjcc.v12.i16.2758
44. Long ZL, Liu ZS. Brief analysis on main indications and compatibility rules of Ciliao (BL 32) based on data mining. Zhongguo Zhen Jiu = Chinese Acupuncture & Moxibustion. 2022;42(4):459–463. doi:10.13703/j.0255-2930.20211106-k0001
45. Wang HJ, Cao YX, Ji JQ, et al. Acupuncture of “Zhibian (BL 54) through Shuidao (ST 28)” for female stress urinary incontinence: a randomized controlled trial. Zhongguo zhen jiu = Chin acupuncture & moxibustion. 2020;40(10):1061–1064. doi:10.13703/j.0255-2930.20200410-k0005
46. Zhang C, Quan RF, Chai L, Hu HH. Effects on urinary retention after spinal cord injury treated with acupuncture at Zhibian (BL 54) and Shuidao (ST 28) with elongated needle. Zhongguo zhen jiu = Chin acupuncture & moxibustion. 2019;39(4):359–363. doi:10.13703/j.0255-2930.2019.04.004
47. Dai J, Zhang X, Lian F, et al. Clinical study on improving the function of female bladder in controlling urine by acupuncture Zhibian (BL54) under ultrasound guidance. World J Urol. 2024;42(1):300. doi:10.1007/s00345-024-05004-2
48. Zhang Y, Wang H, Cao Y, et al. Origin, development and advantageous disease spectrum of the “Zhibian (BL 54) through Shuidao (ST 28) needling technique”. Zhongguo zhen jiu = Chin acupuncture & moxibustion. 44(2):200–203. doi:10.13703/j.0255-2930.20230619-k0003
49. Liu Y, Liu L, Wang X. Electroacupuncture at points Baliao and Huiyang (BL35) for post-stroke detrusor overactivity. Neural Regen. Res. 2013;8(18):1663–1672. doi:10.3969/j.issn.1673-5374.2013.18.004
50. Rosier P, Schaefer W, Lose G, et al. International continence society good urodynamic practices and terms 2016: urodynamics, uroflowmetry, cystometry, and pressure-flow study. Neurourol Urodynamics. 2017;36(5):1243–1260. doi:10.1002/nau.23124
51. Panicker JN. Neurogenic bladder: epidemiology, diagnosis, and management. Seminars in Neurology. 2020;40(5):569–579. doi:10.1055/s-0040-1713876
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Transcutaneous Electrical Acupoint Stimulation on Postoperative Urinary Retention After Radical Hysterectomy for Cervical Cancer: Study Protocol for A Pilot Randomized Controlled Trial
Li G, Chen N, Li X, Deng D, Bao W, Wang C, Zhao L, Wang P, Liang Y, Lu C
International Journal of Women's Health 2026, 18:595680
Published Date: 23 March 2026