Back to Journals » International Journal of Women's Health » Volume 18
Effect of Transcutaneous Electrical Acupoint Stimulation on Postoperative Urinary Retention After Radical Hysterectomy for Cervical Cancer: Study Protocol for A Pilot Randomized Controlled Trial
Authors Li G ![]() , Chen N, Li X, Deng D, Bao W, Wang C, Zhao L, Wang P
, Chen N, Li X, Deng D, Bao W, Wang C, Zhao L, Wang P ![]() , Liang Y
, Liang Y ![]() , Lu C
, Lu C ![]()
Received 12 January 2026
Accepted for publication 16 March 2026
Published 23 March 2026 Volume 2026:18 595680
DOI https://doi.org/10.2147/IJWH.S595680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Guangliang Li,1,* Nisang Chen,2,* Xiaoyu Li,2,* Dehou Deng,3 Wenlong Bao,3 Chunlan Wang,4 Lingqin Zhao,4 Peipei Wang,3 Yi Liang,5 Chao Lu3
1Department of Breast Medical Oncology, Zhejiang Cancer Hospital, Hangzhou, People’s Republic of China; 2The Third Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 3Department of Traditional Chinese Medicine, Zhejiang Cancer Hospital, Hangzhou, People’s Republic of China; 4Department of Gynecological Oncology, Zhejiang Cancer Hospital, Hangzhou, People’s Republic of China; 5Department of Acupuncture, the Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Lu, Department of Traditional Chinese Medicine, Zhejiang Cancer Hospital, No. 1, East Banshan Road, Gongshu District, Hangzhou, 310022, People’s Republic of China, Email [email protected] Yi Liang, Department of Acupuncture, the Third Affiliated Hospital of Zhejiang Chinese Medical University, 219 Moganshan Road, Hangzhou, 310053, People’s Republic of China, Email [email protected]
Introduction: Postoperative urinary retention (POUR) is a common complication in women after radical hysterectomy for cervical cancer and may substantially impair quality of life. Transcutaneous Electrical Acupoint Stimulation (TEAS) has shown potential in alleviating POUR, but its efficacy remains to be further evaluated. This pilot study aims to preliminarily evaluate the effect of TEAS in women who develop POUR after radical hysterectomy for cervical cancer.
Methods and Analysis: This protocol describes a prospective, single-blinded, single-center pilot randomized controlled trial that will compare TEAS with sham TEAS for the management of POUR after radical hysterectomy for cervical cancer. A total of 76 eligible patients will be randomly assigned in a 1:1 ratio to the TEAS group or the sham TEAS group. Participants in the TEAS group will receive TEAS once daily for 2 weeks, while those in the sham TEAS group will receive sham stimulation on the same schedule. The primary outcome is the change in post-void residual (PVR) volume. Secondary outcomes include the rate of successful urinary catheter removal, incidence of urinary tract infection (UTI), and quality of life assessed using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-C30 (EORTC QLQ-C30). Safety will also be evaluated. All statistical analyses will be conducted according to the intention-to-treat (ITT) principle.
Ethics/Dissemination: The trial has received ethics approval from the Medical Ethics Committee of Zhejiang Cancer Hospital (14 October 2025; IRB-2025-1262). Findings will be disseminated in peer-reviewed journals to inform clinical decision-making in POUR management.
Trial Registration Number: ITMCTR2025002091.
Keywords: transcutaneous electrical acupoint stimulation, TEAS, postoperative urinary retention, POUR, post-void residual, PVR, cervical cancer, study protocol
Introduction
Cervical cancer constitutes one of the most prevalent malignant tumors worldwide, with radical hysterectomy remaining a cornerstone of clinical treatment for eligible patients.1 However, this surgical intervention is frequently associated with a spectrum of postoperative complications, among which postoperative urinary retention (POUR) stands out as a common issue.2,3 Previous publication indicates that the incidence of POUR following radical hysterectomy for cervical cancer varies substantially, ranging from 8% to 80%.4 The clinical manifestations of POUR include postoperative dysuria, inability to initiate micturition or complete bladder emptying, and significant post-void residual (PVR) volume. Notably, patients with cervical cancer often present with postoperative debility, and a considerable proportion require adjuvant anti-neoplastic therapies (eg., radiotherapy, chemotherapy). These sequential treatments may further compromise patients’ physiological function, impede the recovery of bladder neurogenic and contractile function, prolong the duration of POUR, and ultimately exert a profound adverse impact on patients’ quality of life.
At present, indwelling urethral catheterization remains the primary therapeutic intervention for POUR. Nevertheless, prolonged indwelling catheterization is associated with inherent risks, including urethral mucosal trauma and a substantially elevated incidence of urinary tract infection (UTI).5,6 In recent years, intermittent clean self-catheterization (ICSC) has emerged as an increasingly utilized approach in the clinical management of POUR. Defined as the discontinuation of long-term indwelling catheters, this strategy involves catheter insertion on an as-needed basis, with prompt removal following complete bladder emptying, and is recognized as an effective method to facilitate rapid bladder evacuation.7 ICSC affords patients increased opportunities for independent voiding practice, enables real-time dynamic monitoring of post-void residual (PVR) volume, and may modestly promote bladder function recovery through targeted voiding training, which is clinically meaningful because reducing PVR can decrease the risk of urinary retention–related complications such as urinary tract infection and the need for recatheterization, thereby improving patient comfort and recovery outcomes.8 Despite these benefits, ICSC imposes considerable demands on patient adherence and self-management capacity, presenting particular challenges among elderly individuals or those with limited functional independence. Furthermore, improper catheterization technique or prolonged ICSC implementation inevitably heightens the risk of UTI.9 Our clinical practice indicated that sole reliance on patient-directed pelvic floor muscle training or ICSC is associated with suboptimal patient acceptance and compliance, resulting in limited therapeutic efficacy. Consequently, there is an urgent need for a safer, simpler, and more effective therapeutic regimen to facilitate recovery in patients with POUR.
In recent years, traditional Chinese medicine (TCM)-based therapeutic strategies have been extensively explored for the management of POUR, with preliminary studies yielding promising efficacy signals.10,11 As a minimally invasive TCM intervention characterized by a favorable safety profile, acupuncture has been widely applied in the treatment of POUR secondary to various surgical procedures.12,13 Electroacupuncture (EA), an innovative modification that integrates traditional acupuncture with modern electrical stimulation technology, has demonstrated distinct therapeutic advantages in the management of postoperative neurogenic bladder dysfunction.14,15 However, acupuncture and EA are associated with inherent limitations that may compromise patient acceptance, including the procedural discomfort (eg., acupuncture-related pain) associated with these interventions and the requirement for frequent hospital visits, which impose substantial time and logistical burdens on patients. Transcutaneous electrical acupoint stimulation (TEAS) is a non-invasive derivative of EA technology, which delivers electrical stimulation via electrode patches affixed to the surface of targeted acupoints.16 TEAS devices feature relatively straightforward operations, and patients can be readily trained in proper usage protocols, enabling self-administered treatment in a home-based setting.17 Compared with traditional acupuncture or EA, TEAS offers enhanced patient acceptability, primarily attributed to its non-invasive nature and elimination of acupuncture-related discomfort.11 From a mechanistic perspective, electrical stimulation at the Baliao acupoints may modulate pelvic autonomic and pudendal nerve pathways involved in bladder control, thereby promoting recovery of detrusor and voiding function.
While some preliminary studies have suggested that TEAS may alleviate symptoms associated with POUR, the therapeutic efficacy of this intervention remains insufficiently validated.18,19 Most existing preliminary studies have been conducted in various surgical settings rather than specifically focusing on POUR after radical hysterectomy for cervical cancer, and no randomized controlled trial has yet evaluated home-based TEAS in this population. Therefore, we propose to conduct a pilot, single-blinded randomized controlled trial to preliminarily assess the clinical efficacy and feasibility of TEAS in the management of POUR among patients who have undergone radical hysterectomy for cervical cancer.
Methods
Objective
To evaluate the effect of TEAS on POUR after radical hysterectomy for cervical cancer.
Trial Design
This study is designed as a pilot, participant-blinded, single-center randomized controlled trial to be conducted at Zhejiang Cancer Hospital, with a planned study period from November 01, 2025, to November 30, 2028. A total of 76 eligible patients with POUR following radical cervical cancer surgery will be recruited and randomly assigned to either the TEAS group or the sham TEAS group at a 1:1 allocation ratio. The intervention phase will last for 2 consecutive weeks, and a follow-up assessment will be performed 2 weeks after the completion of the final intervention session. The detailed study workflow is illustrated in Figure 1, while Table 1 outlines the trial timeline encompassing participant enrollment, intervention delivery, and outcome measure assessments. This study will be conducted in full compliance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines20 and the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement.21
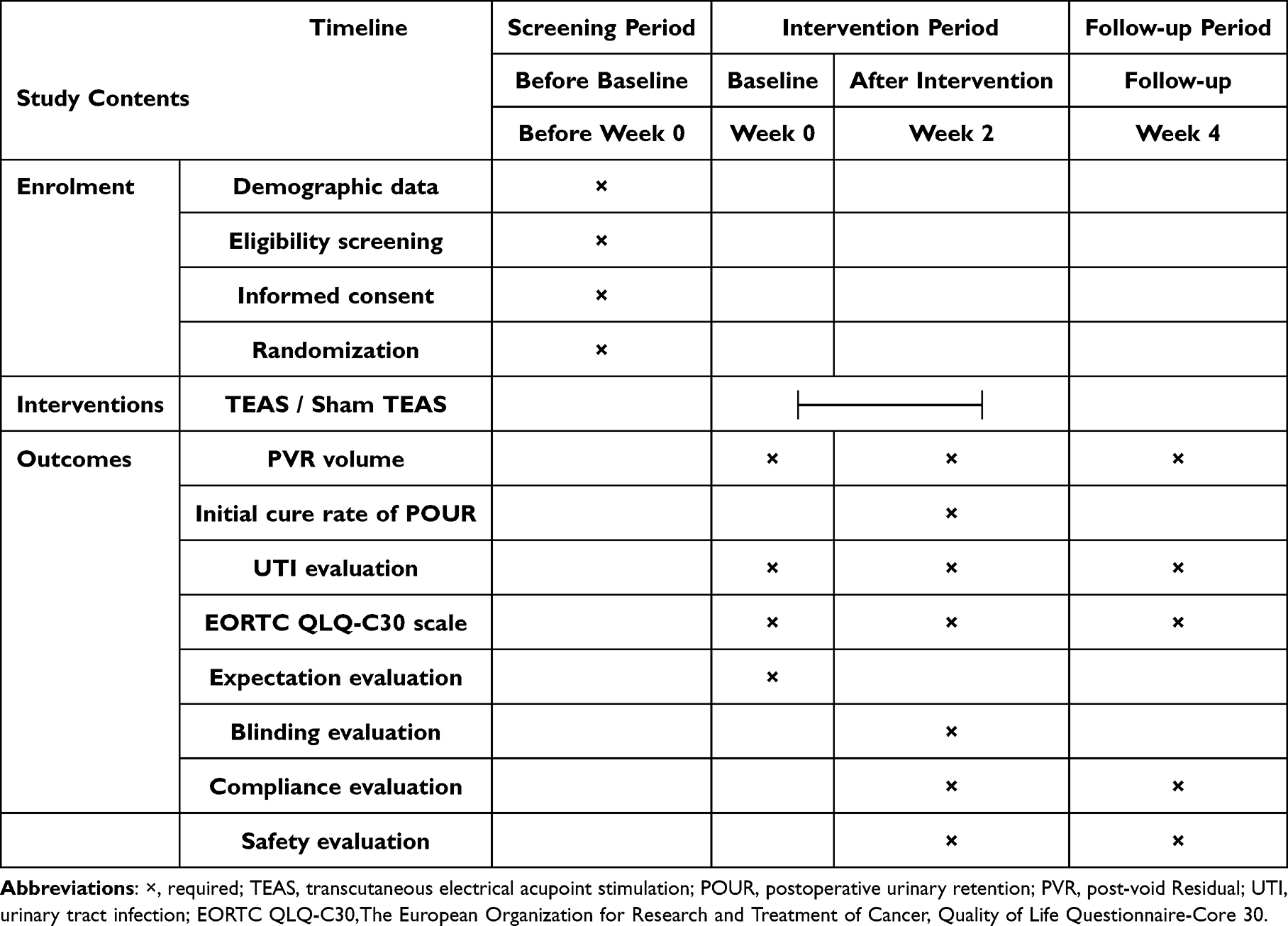 |
Table 1 Study Schedule of Enrolment, Interventions, and Outcomes |
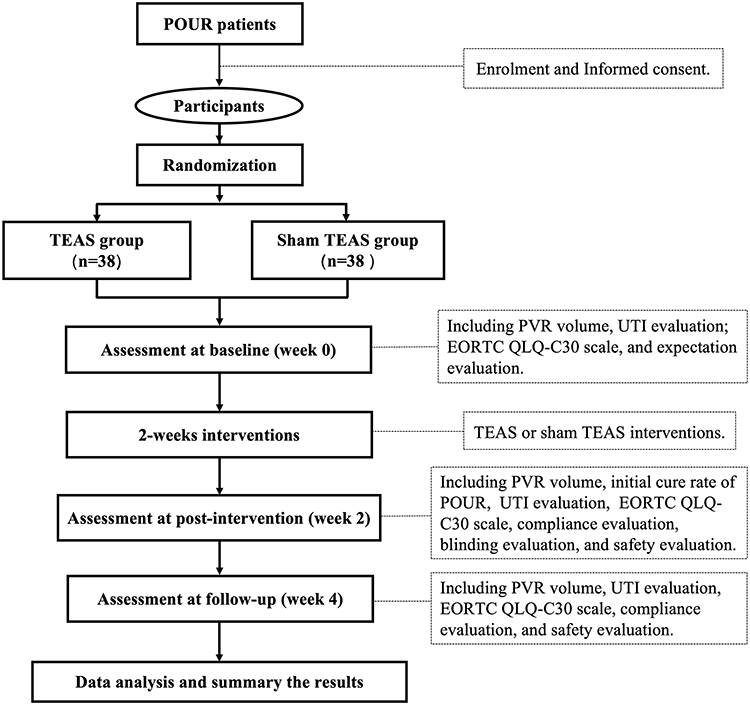 |
Figure 1 Flowchart of the trial. POUR: Postoperative urinary retention; TEAS, Transcutaneous Electrical Acupoint Stimulation; PVR: Post-void residual; UTI: Urinary tract infection; EORTC QLQ-C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30. |
Ethical Standards and Registration
This trial will be conducted in strict adherence to the ethical principles outlined in the Declaration of Helsinki. The study protocol has undergone formal review and obtained approval from the Medical Ethics Committee of Zhejiang Cancer Hospital on October 14, 2025 (approval number: IRB-2022-1262). Additionally, this trial has been prospectively registered in the International Traditional Medicine Clinical Trial Registry (website: itmctr.ccebtcm.org.cn) under the registration number ITMCTR2025002091.
Informed Consent
All eligible patients with POUR invited to participate in this trial will be afforded the right to receive comprehensive information regarding the study, including potential benefits, foreseeable risks, and alternative treatment options. Participation will be entirely voluntary, based on each individual’s free and informed decision. Participants will retain the right to withdraw from the trial at any time without providing a specific reason and without incurring any adverse consequences to their ongoing clinical care. All personal and clinical data of participants will be handled in strict compliance with data protection regulations and maintained with strict confidentiality, with access restricted to authorized study personnel only. Prior to enrollment, all participants must provide written informed consent after a thorough explanation of the study details by a trained member of the research team.
Study Procedure
This trial will consist of three sequential study phases, including screening in the baseline phase (week 0), a 2-week intervention phase (weeks 1–2), and a follow-up phase (week 4). Eligibility assessment of potential participants will be conducted by independent researchers who are not involved in intervention or outcome assessment, to minimize bias. During the screening visit, patients will receive comprehensive verbal and written information regarding study procedures, risks, and expectations. Outcome assessments to evaluate therapeutic efficacy and safety will be performed at three time points: baseline (week 0), post-intervention (week 2), and follow-up (week 4). These assessments will include post-void residual (PVR) volume measurement, urinalysis, completion of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-C30 (EORTC QLQ-C30), and evaluations of treatment expectations, blinding, intervention compliance, and adverse events. Throughout the trial period, participants will be prohibited from using medications that may interfere with study outcomes, including diuretics and any unapproved therapies targeting POUR. If a participant requires initiation of such medications due to disease progression or other medical necessities, they will be considered to withdrawn from the trial and classified as a dropout. To support recruitment efforts, all study-related interventions, outcome measurements will be provided to participants free of charge.
Inclusion Criteria and Exclusion Criteria
The diagnosis of cervical cancer will be established in accordance with the diagnostic criteria for cervical cancer issued by the International Federation of Gynecology and Obstetrics (FIGO).22 POUR is defined as either the inability to achieve spontaneous voiding for more than 14 days following radical hysterectomy, or a PVR volume exceeding 100 mL despite the ability to void spontaneously.23 The detailed inclusion and exclusion criteria for study participation are shown in Table 2.
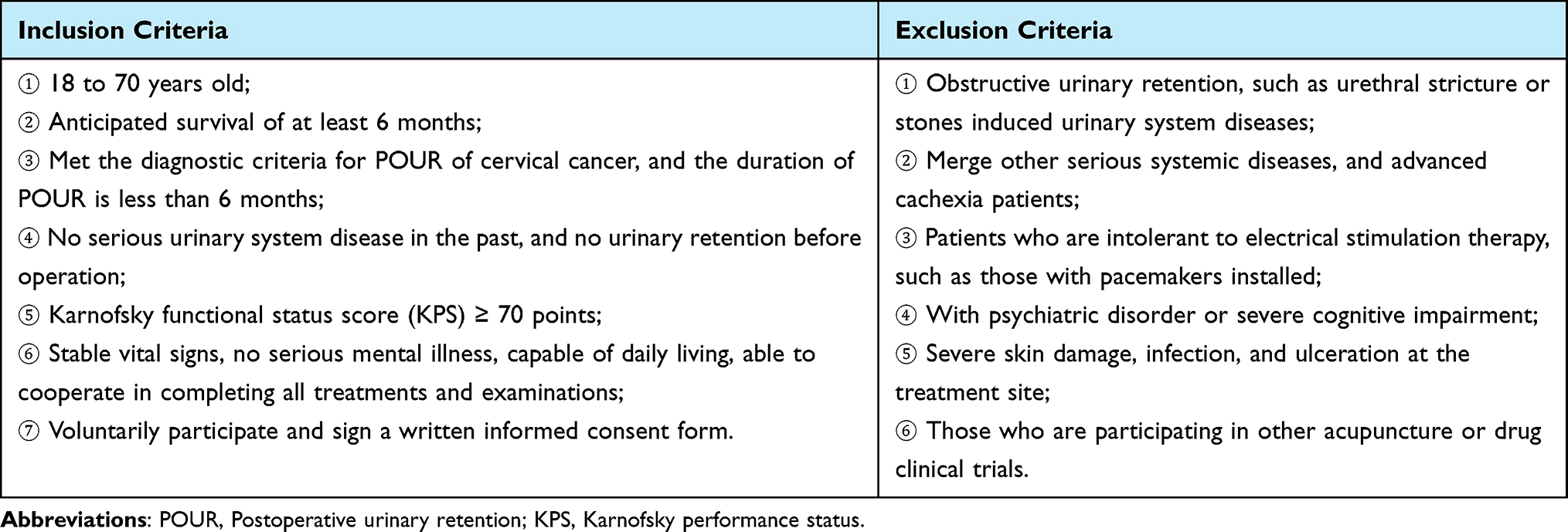 |
Table 2 Inclusion Criteria and Exclusion Criteria |
Randomization and Allocation Concealment
Randomization will be performed by an independent researcher who is not involved in outcome assessment or statistical analysis, to minimize selection bias. The randomization procedure will utilize the dynamic randomization method of the central random system to generate a random allocation sequence consisting of 76 unique numbers, which will be allocated into two equal groups (1:1 allocation ratio): the TEAS group and the sham TEAS group. Following enrollment, the treating acupuncturist will retrieve the random number and corresponding intervention assignment associated with each participant’s sequential visit order, ensuring concealment of allocation until the initiation of treatment.
Blinding
Participant blinding will be implemented in this study. Before enrollment, participants will be informed that they have a 50% probability of being assigned to either the TEAS group or the sham TEAS group. The TEAS devices and electrode patches used in both groups are identical in external appearance to maintain blinding integrity. The only distinction is that the current wires of the sham TEAS devices have undergone specialized modification to prevent any electrical current output. Participants will be informed that the perception of electrical stimulation may vary among individuals and across treatment sessions. All participants will receive home-based TEAS treatment. Trained researchers will provide standardized hands-on training to participants, instructing them on proper TEAS device operation and self-administration techniques. This home-based intervention model can minimize potential communication between participants, thereby enhancing the success of blinding. Due to the requirement for acupuncturists to conduct pre-intervention verification of TEAS devices (a necessary step for TEAS administration), the acupuncturists cannot be blinded to the intervention assignment. However, these acupuncturists will be excluded from all outcome assessment and data analysis. Additionally, the researchers responsible for outcome data collection and statistical analysis will be blind to participants’ group allocations (assessor and analyst blinding), which further minimizes detection bias.
Intervention
All participants will receive either TEAS or sham TEAS intervention based on the conventional treatment. Conventional treatment will consist of an indwelling urethral catheterization for all participants.
The TEAS Group
TEAS will be administered at the lumbosacral acupoints of participants. Acupoints selection: Ciliao (BL32) and Xialiao (BL34). Acupoint localization will adhere to the national standard for acupoint naming and positioning (GB/T 12345–2021), with detailed anatomical landmarks illustrated in Figure 2. TEAS Intervention: Participants will be positioned in a prone posture. Disposable electrode patches connected to the TEAS device will be affixed to bilateral BL32 and BL34 acupoints, with electrode placement carefully aligned to avoid current conduction across the spinal midline. The TEAS device will be set to an alternating frequency of 2/10 Hz, and the current intensity will be titrated to 35 ± 5 mA, defined as the threshold at which participants perceive visible muscle vibration without experiencing significant discomfort or pain (individualized based on patient tolerance). Each TEAS session will last 30 minutes, administered once daily for 2 consecutive weeks. A follow-up assessment will be conducted 2 weeks after the final intervention session.
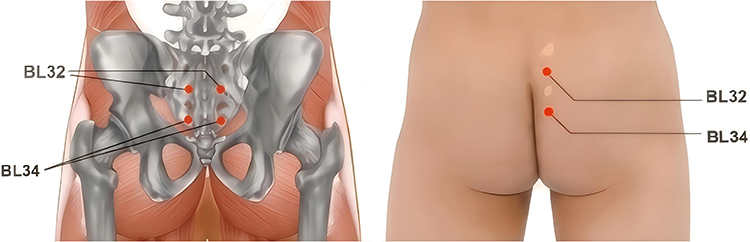 |
Figure 2 The location of acupoints. The TEAS group and the sham TEAS group will use the same acupoints. BL32 (Ciliao) and BL34 (Xialiao) on each side will be connected via TEAS or the sham TEAS. Location: BL32, located in the sacrum, and corresponding to the second sacral foramen. BL34, located in the sacrum, and corresponding to the fourth sacral foramen. |
All participants will conduct a home-based TEAS intervention. Standardized training on device operation, acupoint localization, and intervention procedures will be provided to participants and their caregivers via in-person demonstrations and supplementary instructional videos. Except for the first intervention session (conducted in the hospital treatment room to verify proficiency), all subsequent interventions will be self-administered by participants or their caregivers at home. To ensure study quality and intervention adherence, participants can access the attending physician via the hospital’s online platform, with real-time support (eg., video consultations) available to address technical or clinical questions. Participants will be required to complete a daily intervention log to document session timing, and any adverse events potentially related to TEAS (eg., skin irritation at electrode sites, discomfort) will be recorded in detail. The completed intervention log will be returned to the attending physician at the 2-week intervention completion visit for review and compliance verification.
The Sham EA Group
Participants assigned to the sham TEAS group will receive a sham TEAS intervention. Acupoint Selection: Identical to the TEAS group (bilateral BL32 and BL34). Sham TEAS process: Use the same TEAS device, with disposable electrode patches affixed to the same target acupoints. The device will be set to display the same parameters as the TEAS group: an alternating frequency of 2/10Hz and a nominal current intensity of 35 mA. Critically, the external wiring of sham devices will be specially modified to disrupt circuit closure, resulting in no actual electrical current delivery to the participant. The intervention duration and frequency will be the same as the TEAS group. A follow-up assessment will also be conducted 2 weeks after the final intervention.
Sham TEAS will also be self-administered by participants at home, with standardized training provided to participants and their caregivers via in-person demonstrations and instructional videos (identical to the TEAS group’s training protocol). To preserve blinding integrity, no prior disclosure of reduced or absent stimulation sensation will be provided to participants; instead, training will emphasize that perceived stimulation may vary by individual (a neutral statement consistent with active treatment expectations). Participants will also be required to complete a daily intervention log (identical to the active group) to document session timing and any potential adverse events. The completed log will be returned to the attending physician at the 2-week intervention completion visit for compliance verification.
All TEAS and sham TEAS interventions will be performed under two guidance of certified acupuncturists with a minimum of 10 years of clinical experience in acupuncture. The TEAS devices utilized in this study are the Hwato SDZ-IIB model, manufactured by Suzhou Medical Equipment Co., Ltd. (Suzhou, China). These devices will be provided to participants free of charge for the duration of the intervention, along with a sufficient supply of disposable electrode patches to complete the 2-week treatment course. Participants will be required to return the TEAS/sham TEAS device to the research team upon completion of the 2-week intervention period. In the event of accidental device damage or loss during the study period, participants will not be held liable for compensation.
Outcome Measures
Following enrollment, all participants will undergo a comprehensive baseline assessment at week 0. This evaluation will include collection of demographic characteristics (age, height, weight, body mass index [BMI]) and clinical data, including surgical approach (eg., laparoscopic, open radical hysterectomy), duration of POUR, most recent PVR volume, presence of concurrent UTI (confirmed by urinalysis and/or urine culture), participant expectations regarding TEAS treatment, and any relevant comorbidities or special clinical considerations.
The primary outcome will be the change in PVR volume from baseline to post-intervention. All participants will measure PVR volume at baseline (week 0), and post-intervention (week 2). It will be measured by professional nurses, using a direct measurement method (inserting a catheter to drain and measure residual urine volume). PVR volume is a direct indicator for evaluating the recovery of bladder urination function. Specifically, participants will be asked to void spontaneously, after which PVR volume will be measured immediately by trained nurses using a standardized sterile catheterization procedure. All measurements will be performed by trained professional nurses using the direct catheterization method: after spontaneous voiding, a sterile urethral catheter will be inserted to drain and quantify the residual urine volume, with results recorded in milliliters. To ensure measurement consistency, nurses will complete standardized training on catheterization technique, sterile procedures, and volume quantification before study initiation.24 Repeated catheterization is required for PVR measurement; therefore, the same measurement schedule and catheterization procedure will be applied to both groups to minimize potential bias in UTI incidence. PVR volume is a well-validated, objective indicator of bladder emptying function recovery in patients with POUR.24 It is generally accepted that indwelling urinary catheters can be discontinued when the PVR volume <100 mL combined with the participant’s self-report of no significant voiding-related symptoms.25,26
Secondary outcomes include the response rate among participants who removed their urinary catheters after intervention, assessment of UTI, and evaluation of patient quality of life according to the EORTC QLQ-C30 scale. ① The response rate of participants who will successfully remove the urinary catheter. Defined as the proportion of participants in each group who achieve successful urinary catheter removal at post-intervention (week 2), calculated as (number of participants with successful catheter removal/total number of participants in the group) × 100%. This outcome reflects the initial clinical response rate (or “initial cure rate”) for POUR. ② Assessment of UTI. Urinalysis and/or urine culture will be performed at baseline (week 0) and post-intervention (week 2) to systematically assess the presence of urinary tract infection (UTI). All decisions regarding the initiation, type, and duration of UTI-directed medications (eg., antibiotics) will be documented in the study case report form (CRF). Analysis will be performed to compare differences in the proportion of UTI participants between the two groups. ③ Patient quality of life according to the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC QLQ-C30) scale. The EORTC QLQ-C30 scale is a well-validated, internationally standardized instrument widely used to assess health-related quality of life in oncology clinical trials.27 This self-administered questionnaire comprises 5 functional subscales, 3 symptom subscales, 6 single-item symptom measures, and 1 global health status subscale. Higher scores on the functional subscales indicate better quality of life, whereas higher scores on the symptom subscales reflect more severe symptoms. All raw scores will be linearly transformed to standardized scores ranging from 0 to 100 to facilitate comparative analyses.28,29 The EORTC QLQ-C30 will be administered at baseline (week 0), post-intervention (week 2), and follow-up (week 4).
Other outcomes: All participants will complete a validated questionnaire to assess their expectations regarding the therapeutic efficacy of TEAS for POUR at baseline (week 0), Following the completion of the 2-week intervention (week 2), a blinded evaluation will be conducted to assess the success of participant blinding. Participants will be asked to guess their assigned group (TEAS vs. sham TEAS) and rate their confidence in this guess (eg., 1 = not confident to 5 = extremely confident). This assessment will quantify blinding effectiveness and minimize detection bias. During follow-up (week 4), all participants will undergo clinical evaluation to assess for POUR recurrence. Recurrence will be defined as the PVR volume >100 mL in participants who previously achieved successful catheter removal, accompanied by the need for further clinical intervention. Participants reporting urinary symptoms (eg., dysuria, frequency, urgency, or incomplete bladder emptying) will undergo repeat urinalysis/urine culture to evaluate UTI. During follow-up, assessments of quality of life (EORTC QLQ-C30 scale) will also be performed. All treatment decisions and outcomes will be documented in the study case report form (CRF).
Safety Evaluation
All adverse events (AEs) occurring during the study will be documented and assessed, including TEAS-related AEs (eg., skin irritation at electrode sites, local discomfort, or dizziness). For each reported AE, the following details will be recorded in the CRF: (1) date and time of onset; (2) severity (graded per Common Terminology Criteria for Adverse Events [CTCAE], Version 5.0: Grade 1 = mild, Grade 2 = moderate, Grade 3 = severe, Grade 4 = life-threatening); (3) suspected relationship to the TEAS intervention (definite, probable, possible, unlikely, or unrelated); (4) medical management provided; (5) clinical outcome (resolved, resolving, persistent, or fatal); (6) follow-up duration and findings; and (7) any decision regarding modification of the intervention or participant withdrawal from the trial.
Quality Control
All acupuncturists and evaluators will complete specialized training before trial initiation to ensure standardized practices. Training content will encompass the standardized diagnosis and assessment of POUR, strict adherence to study inclusion/exclusion criteria, detailed intervention protocols (including acupoint localization, TEAS device operation, sham TEAS implementation, and safety precautions), CRF completion guidelines (including accurate documentation of outcomes, AEs, and compliance data). All study data will be documented in CRFs and entered into an electronic data capture system by independent researchers. Participant dropouts will be tracked throughout the trial. The trial will be monitored by the Clinical Research Department of Zhejiang Cancer Hospital. The monitoring team will be responsible for data oversight and verification of consistency between source data and recorded data, ensuring the accuracy and quality of study data throughout the trial period.
Statistical methods
Sample Size
This study is designed as a prospective, single-center, pilot, randomized controlled trial with a 1:1 allocation ratio. Given the paucity of prior clinical data on TEAS for POUR to inform a formal power calculation, the sample size was determined based on methodological standards for pilot studies.30 A target sample size of 30 participants per group was initially selected to provide preliminary estimates of intervention efficacy and variability, which will inform the design of larger-scale confirmatory trials. To account for potential participant dropout (estimated at 20%), the sample size was inflated to 38 participants per group. Thus, a total of 76 participants will be enrolled in the trial to ensure adequate statistical precision for the primary outcome in the final analytical sample.
Statistical Analysis
De-identified outcome data will be analyzed by an independent statistician masked to participant group assignments using IBM SPSS Statistics (Version 26.0; IBM Corp., Armonk, NY, USA). All statistical analyses will be based on the intention-to-treat (ITT) population. Continuous variables will be presented as mean (standard deviation, SD) if normally distributed, or median (interquartile range, IQR) if non-normally distributed. Categorical variables will be presented as frequencies (n) and percentages (%). Normally distributed continuous variables will be compared using independent samples t-tests, while non-normally distributed continuous variables will be analyzed using the Mann–Whitney U-test. Categorical variables will be compared using the chi-square test or Fisher’s exact test. Within-group changes from baseline (week 0) to post-intervention (week 2) and follow-up (week 4) will be assessed using paired samples t-tests for normally distributed variables and the Wilcoxon signed-rank test for non-normally distributed variables. For the primary outcome, analysis of covariance (ANCOVA) will be used, where appropriate, to compare post-intervention PVR volume between groups with adjustment for baseline PVR values. Baseline covariates will be inspected for imbalance and may be included in exploratory adjusted analyses if clinically relevant. Missing outcome data will be handled primarily using multiple imputation, and the last observation carried forward (LOCF) method will be applied in sensitivity analyses where appropriate. Baseline characteristics, including receipt of adjuvant therapy where applicable, will be summarized descriptively. The success of participant blinding will be evaluated using the Bang Blinding Index, calculated via R software (version 4.2.3; R Foundation for Statistical Computing). All statistical tests will be two-sided with a pre-specified significance level of α = 0.05. Given the pilot nature of the study, p-values will be interpreted cautiously and primarily used for exploratory purposes rather than definitive hypothesis testing. For the primary outcome, treatment effect estimates with 95% confidence intervals will be reported.
Discussion
POUR is a common clinical complication following cervical cancer surgery, primarily attributed to iatrogenic injury to the bladder detrusor muscle, urethral sphincter, and pelvic autonomic nerves during radical hysterectomy and pelvic lymphadenectomy.31 Indwelling urinary catheterization is the conventional first-line management for POUR; however, this approach carries inherent risks, including UTI, catheter-related discomfort, delayed recovery of spontaneous voiding, and reduced quality of life. Current therapeutic strategies for POUR encompass pharmacological interventions and physical therapy. Pharmacological approaches primarily rely on parasympathomimetic agents (eg., neostigmine) aimed at enhancing bladder detrusor contraction and improving bladder tone.4,32 However, these medications are limited by modest efficacy and a spectrum of adverse effects (eg., gastrointestinal upset, bradycardia).33 Physical therapy modalities, such as CISC and acupuncture-related therapies, are more widely adopted in clinical practice.34–36 Recommended as the “gold standard” by the International Continence Society for neurogenic bladder management, CISC effectively alleviates chronic urinary retention of diverse etiologies.37 Nevertheless, CISC requires high levels of patient adherence and technical proficiency; improper technique or prolonged use may increase the risk of urinary system infections and patient burden.
In recent years, acupuncture and EA have gained increasing clinical traction for the management of POUR of diverse etiologies, supported by accumulating evidence of potential benefit.12,36 Domestic expert consensus on POUR following radical hysterectomy has endorsed acupuncture and EA as a feasible therapeutic option, with a growing body of clinical data suggesting potential benefit.35,38 However, these interventions are associated with inherent limitations that hinder widespread accessibility and patient adherence. These mainly include invasiveness and the need for repeated hospital visits, which may reduce accessibility and adherence. In contrast, TEAS, a non-invasive modality characterized by a favorable safety profile, has been increasingly adopted in the clinical management of a spectrum of cancer-related conditions and post-surgical complications.39,40 Distinguished from invasive acupuncture and EA, TEAS delivers therapeutic stimulation via surface electrode patches without skin penetration, eliminating needle-related pain and improving patient acceptability. Furthermore, TEAS devices are designed for user-friendly operation, enabling patients or their caregivers to master self-administration techniques with minimal training and facilitating home-based treatment delivery.41,42 Our research team has previously demonstrated the high feasibility of home-based self-administered TEAS for cancer-related conditions, with patients achieving consistent treatment compliance and operational proficiency in clinical practice.17 Given these advantages, TEAS addresses the key limitations of EA while retaining the therapeutic mechanism of acupoint stimulation. To preliminarily validate the efficacy and feasibility of home-based self-administered TEAS for POUR, we designed this prospective, randomized, blinded controlled trial. This study aims to fill the evidence gap regarding non-invasive, home-delivered interventions for POUR, with the potential to optimize treatment accessibility, reduce healthcare burden, and improve patient-centered outcomes.
Previous studies have shown that the high-frequency acupoints used for acupuncture treatment of POUR involve the “Baliao” (BL31–34), Shenshu (BL23), Pangguangshu (BL28), and Zhibian (BL54) acupoints in the lumbar and sacral regions, as well as the Zhongji (RN3), Guanyuan (RN4), and Shuidao (ST28) acupoints in the abdomen, and the Yinlingquan (SP9) and Sanyinjiao (SP6) acupoints in the lower limbs.43,44 While these acupoints have demonstrated therapeutic potential, their wide anatomical distribution presents a practical barrier for patient home use. Patients often struggle to accurately locate and self-administer stimulation to multiple discrete sites, which risks compromising treatment adherence and consistency. Our team’s decade-long clinical experience in POUR management has consistently identified the “Baliao” acupoint cluster (BL31–34) as a high-priority therapeutic target for modulating pelvic autonomic nerve function and bladder detrusor activity. A targeted literature review of acupoints mechanisms for POUR, which confirmed the “Baliao” acupoint cluster (especially BL32, BL33, and BL34) anatomical association with the sacral plexus, which is a key neural pathway regulating urinary function.45,46 The parasympathetic fibers of the anterior branch of the sacral nerve, distributed below these acupoints, participate in the formation of the pelvic visceral nerve, which innervates the detrusor muscle of the bladder, inhibits the urethral sphincter, and plays a crucial role in regulating urination function. An animal experiment demonstrated that acupuncture at the Ciliao (BL32) significantly improves bladder internal pressure, reduces residual urine volume, adjusts the micturition threshold, and increases the discharge frequency of the pelvic nerve, ultimately enhancing pelvic nerve excitability and bladder detrusor function.47 Xialiao (BL 34), holds particular clinical relevance due to its distinct anatomical location. It lies in proximity to the levator ani tendon and the main trunk of the pudendal nerve (which innervates the bladder detrusor, urethral sphincter, and pelvic floor musculature). Stimulating at BL34 can promote pelvic floor muscle recovery and modulate bladder function.
In clinical practice, changes in bladder PVR volume after radical hysterectomy are directly associated with bladder function recovery. PVR volume <100 mL with no absence of significant voiding discomfort is generally accepted as the minimum criterion for catheter removal in POUR patients.25,26 Thus, changes in bladder PVR volume at post-intervention will be defined as the primary outcome. The rate of urinary catheter removal, UTI assessment, and the EORTC QLQ-C30 scale will be defined as secondary outcomes. In this trial, a blinding strategy will be implemented for all participants. However, because TEAS involves perceptible electrical stimulation, participants may speculate about their group allocation, which may introduce a potential risk of unblinding. Intervention providers and outcome assessors will be strictly separated to ensure adequate allocation concealment. Furthermore, we will systematically evaluate the participant expectation, blinding integrity, participant compliance, and safety profile of the TEAS intervention, which serves to enhance the reliability of the study results. If the findings are positive, this pilot trial may provide preliminary evidence to support larger-scale studies and the integration of TEAS into postoperative supportive care for patients with POUR after radical hysterectomy for cervical cancer. More broadly, this study may also contribute to the growing interest in non-pharmacologic and integrative approaches to postoperative rehabilitation in oncology care.
Limitations
This study has several limitations that should be acknowledged. First, the single-center design cannot rule out potential differences in population characteristics, which may introduce selection bias and limit the generalizability of the findings. Second, the absence of urodynamic testing precluded the measurement of urine flow rate and bladder detrusor pressure, resulting in an incomplete assessment of supplement outcome indicators related to bladder function. Third, the follow-up period was relatively short: while all participants were assessed at 4 weeks post-intervention, clinical practice indicates that a subset of patients may experience disease recurrence several months later, which could not be captured in the current study. Despite these limitations, the findings of this study still provide valuable insights for the clinical application of TEAS in the management of postoperative urinary retention (POUR) in patients with cervical cancer.
Conclusions
The findings of this study will preliminarily evaluate the feasibility and potential role of TEAS in the management of POUR after radical hysterectomy for cervical cancer. As a pilot study, the results are intended to be hypothesis-generating and may inform the design of future studies. It is anticipated that the findings may contribute to the optimization of POUR management and ultimately improve patients’ overall quality of life.
Abbreviations
POUR, Postoperative urinary retention; EA, Electroacupuncture; TEAS, Transcutaneous electrical acupoint stimulation; PV, Post-void residual; UTI, Assessment of urinary tract infection; ICSC, Intermittent clean self-catheterization; ITT, Intention-to-treat; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30.
Data Sharing Statement
The study protocol and clinical study report data will be available upon reasonable request from the corresponding author Chao Lu ([email protected].) after publication.
Ethics Approval
Ethical approval was granted on 14 October 2025 by the Medical Ethical Committee of Zhejiang Cancer Hospital (license number: IRB-2025-1262) and has been registered in the International Traditional Medicine Clinical Trial Registry (itmctr.ccebtcm.org.cn) with the identification number of ITMCTR2025002091. Written informed consent will be obtained from all participants.
Acknowledgments
The authors appreciate the support from all participants who will be included in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work is supported by the Zhejiang Province Traditional Chinese Medicine Science and Technology Project (No.2026ZL0220); Zhejiang Province Health Industry Science and Technology Program Project (No.2025HY0239). The Key Project of Health Science and Technology Program of National Health Commission and Zhejiang Province (Grant No. WKJ-ZJ-2436).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2024;74(3):229–13. doi:10.3322/caac.21834
2. Cao -T-T, Wen H-W, Gao Y-N, et al. Urodynamic assessment of bladder storage function after radical hysterectomy for cervical cancer. Chinese Med J. 2020;133(19):2274–2280. doi:10.1097/cm9.0000000000001014
3. Novackova M, Pastor Z, Chmel R Jr, Brtnicky T, Chmel R. Urinary tract morbidity after nerve-sparing radical hysterectomy in women with cervical cancer. Int Urogynecol J. 2020;31(5):981–987. doi:10.1007/s00192-019-04083-9
4. Plotti F, Angioli R, Zullo MA, et al. Update on urodynamic bladder dysfunctions after radical hysterectomy for cervical cancer. Crit Rev Oncol Hematol. 2011;80(2):323–329. doi:10.1016/j.critrevonc.2010.12.004
5. Lin Y-W, Lin Y-P, Chen Y-S. Comment on the safety and feasibility of no-placement of urinary catheter after single-port laparoscopic surgery in patients with benign ovarian tumor: a retrospective cohort study. Taiwanese J Obstetrics Gynecol. 2024;63(1):127. doi:10.1016/j.tjog.2023.03.018
6. Mengatto MF, Castro BGR, Nobrega L, et al. Early removal of indwelling urinary catheter after radical surgery for early-stage cervical cancer—A cohort study. J Surg Oncol. 2020;122(7):1498–1505. doi:10.1002/jso.26167
7. Engberg S, Clapper J, McNichol L, Thompson D, Welch VW, Gray M. Current evidence related to intermittent catheterization: a scoping review. J Wound Ostomy Continence Nurs. 2020;47(2):140–165. doi:10.1097/won.0000000000000625
8. Fletke KJ, Jeong DH, Herrera AV. Urinary catheter management. Am Family Phys. 2024;110(3):251–258.
9. Fisher H, Oluboyede Y, Chadwick T, et al. Continuous low-dose antibiotic prophylaxis for adults with repeated urinary tract infections (AnTIC): a randomised, open-label trial. Lancet Infect Dis. 2018;18(9):957–968. doi:10.1016/s1473-3099(18)30279-2
10. Lin S-K, Lin P-H, Hsu R-J, Chuang H-C, Liu J-M. Traditional Chinese medicine therapy reduces the catheter indwelling risk in dementia patients with difficult voiding symptoms. J Ethnopharmacol. 2017;203:120–126. doi:10.1016/j.jep.2017.03.040
11. Huang K-Y, Liang S, Du H-G, et al. Transcutaneous electrical acupoint stimulation for prevention of postoperative urinary retention: a systematic review. Heliyon. 2024;10(1):e23537. doi:10.1016/j.heliyon.2023.e23537
12. Zhao Q, Yan C, Dan M, Jia H. Efficacy and safety of acupuncture for urinary retention after hysterectomy: a systematic review and meta-analysis. Medicine. 2021;100(22):e26064. doi:10.1097/md.0000000000026064
13. Olia M, Jafarian A, Mohseni M. Efficacy of low-frequency electroacupuncture on urinary retention after spinal anesthesia. J Perianesthes Nurs. 2023;38(5):745–747. doi:10.1016/j.jopan.2023.01.003
14. Tran PD, Nguyen QD, Ngo TD. Effectiveness of electroacupuncture for managing urinary retention post lumbar spine surgery: a retrospective single-cohort study. J Pharmacopuncture. 2024;27(2):123–130. doi:10.3831/kpi.2024.27.2.123
15. Zhang W, Song S, Zhang T, Ju X, Shu S, Zhou S. Electroacupuncture for urinary retention after stroke: a systematic review and meta-analysis of randomized controlled trials. Complement Therapies Clin Prac. 2024;57:101877. doi:10.1016/j.ctcp.2024.101877
16. Zhang Y-C, Zhao D-X, Fan H-Y, et al. Effects of transcutaneous electrical acupoint stimulation on recovery after internal spinal fixation: a randomised controlled trial. BMC Anesthesiology. 2025;25(1):530. doi:10.1186/s12871-025-03400-8
17. Lyu Z, Shen Q, Tian S, et al. Effects of patient-controlled transcutaneous electrical acupoint stimulation on cancer induced bone pain relief in patients with non-small cell lung cancer: study protocol for a randomized controlled trial. J Pain Res. 2024;17:1285–1298. doi:10.2147/jpr.S437296
18. Zhang Y-F, Li X-Y, Liu X-Y, et al. Transcutaneous electrical acupoints stimulation improves spontaneous voiding recovery after laparoscopic cholecystectomy: a randomized clinical trial. World J Surg. 2023;47(5):1153–1162. doi:10.1007/s00268-023-06924-7
19. Zhang Y, Gong L, Zhang Y, et al. Effect of transcutaneous acupoint electrical stimulation on urinary retention and urinary ATP in elderly patients after laparoscopic cholecystectomy: a prospective, randomized, controlled clinical trial. Clin Intervent Aging. 2022;17:1751–1760. doi:10.2147/cia.S382912
20. Hopewell S, Chan A-W, Collins GS, et al. CONSORT 2025 statement: updated guideline for reporting randomised trials. PLoS Med. 2025;22(4):e1004587. doi:10.1371/journal.pmed.1004587
21. Chan A-W, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Internal Med. 2013;158(3):200–207. doi:10.7326/0003-4819-158-3-201302050-00583
22. FIGO Committee on Gynecologic Oncology. FIGO staging for carcinoma of the vulva, cervix, and corpus uteri. Int J Gynecol Obstet. 2014;125(2):97–98. doi:10.1016/j.ijgo.2014.02.003
23. McDermott CD, Tunitsky-Bitton E, Dueñas-Garcia OF, et al. Postoperative urinary retention. Urogynecology. 2023;29(4):381–396. doi:10.1097/spv.0000000000001344
24. Mainprize TC, Drutz HP. Accuracy of total bladder volume and residual urine measurements: comparison between real-time ultrasonography and catheterization. Am J Clin Exp Obstet Gynecol. 1989;160(4):1013–1016. doi:10.1016/0002-9378(89)90327-x
25. Chuang F-C, Kuo H-C. Management of lower urinary tract dysfunction after radical hysterectomy with or without radiotherapy for uterine cervical cancer. J Formosan Med Assoc. 2009;108(8):619–626. doi:10.1016/s0929-6646(09)60382-x
26. Chen G-D, Lin L-Y, Wang P-H, Lee H-S. Urinary tract dysfunction after radical hysterectomy for cervical cancer. Gynecologic Oncol. 2002;85(2):292–297. doi:10.1006/gyno.2002.6614
27. Aaronson NK, Ahmedzai S, Bergman B, et al. The European organization for research and treatment of cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J National Cancer Inst. 1993;85(5):365–376. doi:10.1093/jnci/85.5.365
28. Shen Q, Deng D, Li G, et al. Electroacupuncture frequency for chemotherapy-induced neuropathy in breast cancer: a randomized controlled trial. Oncologist. 2025;30(9). doi:10.1093/oncolo/oyaf262
29. Lu C, Shen Q, Deng D, et al. Effects of electroacupuncture and mecobalamin for utidelon-induced peripheral neuropathy in breast cancer patients: a randomized controlled clinical trial. J Pain Res. 2025;18:3593–3608. doi:10.2147/jpr.S526405
30. Ying X, Freedland KE, Powell LH, Stuart EA, Ehrhardt S, Mayo-Wilson E. Determining sample size for pilot trials: a tutorial. BMJ. 2025;390:e083405. doi:10.1136/bmj-2024-083405
31. Zullo MA, Manci N, Angioli R, Muzii L, Panici PB. Vesical dysfunctions after radical hysterectomy for cervical cancer: a critical review. Crit Rev Oncol Hematol. 2003;48(3):287–293. doi:10.1016/s1040-8428(03)00125-2
32. Madeiro AP, Rufino AC, Sartori MGF, Baracat EC, Lima GRD, Girão MJBC. The effects of bethanechol and cisapride on urodynamic parameters in patients undergoing radical hysterectomy for cervical cancer. A randomized, double-blind, placebo-controlled study. Int Urogynecol J Pelvic Floor Dysfunc. 2006;17(3):248–252. doi:10.1007/s00192-005-1318-1
33. Manchana T, Prasartsakulchai C. Bethanechol chloride for the prevention of bladder dysfunction after radical hysterectomy in gynecologic cancer patients: a randomized controlled trial study. Int J Gynecolog Cancer. 2011;21(4):730–736. doi:10.1111/IGC.0b013e3181f7d6de
34. Aue-Aungkul A, Kietpeerakool C, Rattanakanokchai S, et al. Postoperative interventions for preventing bladder dysfunction after radical hysterectomy in women with early-stage cervical cancer. Cochrane Database Syst Rev. 2021;1(1):Cd012863. doi:10.1002/14651858.CD012863.pub2
35. Xu H, He Y, Miao F, et al. Acupuncture treatment of postoperative urinary retention in cervical cancer: systematic evaluation and meta-analysis. Medicine. 2025;104(8):e41520. doi:10.1097/md.0000000000041520
36. Tan J, Gong R, Zhang Q, Zheng Y, Ma L, Shi S. Meta-analysis of clinical efficacy of electroacupuncture versus conventional treatment for postoperative urinary retention in cervical cancer. Medicine. 2023;102(43):e35580. doi:10.1097/md.0000000000035580
37. Di Benedetto P. Clean intermittent self-catheterization in neuro-urology. Eur J Phys Rehabil Med. 2011;47(4):651–659.
38. Zhang Yi PX, Weimin K, Yang X, Shiqian Z. Chinese expert consensus on comprehensive treatment for urinary retention after radical hysterectomy (2022 edition). Chinese J Prac Gynecol Obstet. 2022;38(11):1111–1115. doi:10.19538/j.fk2022110112
39. Wu S, Lou J, Zou H, et al. Transcutaneous electrical acupoint stimulation (TEAS) facilitates postoperative recovery in day lung cancer surgery: a randomized controlled trial. J Pain Res. 2025;18:3017–3026. doi:10.2147/jpr.S529193
40. Li Y, Xu X, Chen Y, et al. Transcutaneous electrical acupoint stimulation for the recovery of postoperative gastrointestinal function in patients with colorectal cancer: a systematic review and meta-analysis. Medicine. 2025;104(33):e43699. doi:10.1097/md.0000000000043699
41. Huang C, Czuber-Dochan W, Norton C. Home-based transcutaneous electrical acupuncture-point stimulation for depressive symptoms in inflammatory bowel disease: a randomized feasibility study. Eur J Gastroenterol Hepatol. 2025;37(12):1326–1336. doi:10.1097/meg.0000000000003034
42. Wang Y, Yang J-W, Liu J-H, et al. Home-based transcutaneous electrical acupoint stimulation for high-normal blood pressure: a randomized controlled trial. J Clin Hypertens. 2022;24(8):984–992. doi:10.1111/jch.14496
43. Guo Y, Pan H, Chen S, Tian M, Huang Y, Zhou Y. Effectiveness of acupuncture on urinary retention after radical hysterectomy for cervical cancer in China: a systematic review and meta-analysis. Front Med. 2024;11:1375963. doi:10.3389/fmed.2024.1375963
44. Xu jianwen ZY, Hongling J. Analysis of acupoint selection rules for postoperative urinary retention after acupuncture treatment based on data mining technology. Liaoning J Trad Chin Med. 2023;50(09):1–4. doi:10.13192/j.issn.1000-1719.2023.09.001
45. Wu G-F, Wang W-M. Indication rules of Baliao points based on the clinical literature research. Zhongguo zhen jiu. 2019;39(1):96–102. doi:10.13703/j.0255-2930.2019.01.024
46. Wang X-Q, Guan L-S. Effect of percutaneous electrical stimulation at the Baliao point on preventing postpartum urinary retention after labor analgesia. World J Clin Cases. 2024;12(16):2758–2764. doi:10.12998/wjcc.v12.i16.2758
47. Sun Shuxia GY. Influence of acu-moxibustion on nerve injury induced urine retention in the rabbit. Acupuncture Res. 2003;(04):263–266.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Electroacupuncture on Postoperative Urinary Retention After Radical Hysterectomy for Cervical Cancer: Study Protocol for A Randomized Controlled Trial
Lu C, Chen N, Sun H, Wang C, Zhao L, Bao W, Deng D, Wang P, Li X
Journal of Pain Research 2026, 19:598960
Published Date: 18 March 2026