")
Back to Journals » Infection and Drug Resistance » Volume 16
Effect of Antimicrobial Exposure in Pregnancy on Adverse Pregnancy Outcomes and Admission Rate to the Neonatal Intensive Care Unit: A Multi-Center Cohort Study
Authors Li Y, Zhang C, Huang X, Tang J
Received 18 October 2022
Accepted for publication 27 January 2023
Published 25 April 2023 Volume 2023:16 Pages 2441—2451
DOI https://doi.org/10.2147/IDR.S392504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yueyan Li,1 Chen Zhang,2 Xuan Huang,1 Jing Tang1
1Department of Pharmacy, Obstetrics and Gynecology Hospital of Fudan University, Shanghai, People’s Republic of China; 2Institute of Reproduction and Development, Obstetrics and Gynecology Hospital of Fudan University, Shanghai, People’s Republic of China
Correspondence: Jing Tang, Department of Pharmacy, Obstetrics and Gynecology Hospital of Fudan University, Shanghai, People’s Republic of China, Tel +86 21 33180593, Fax +86 21 33180593, Email [email protected]
Purpose: Antimicrobial agents are frequently prescribed during pregnancy. This study aims to explore the association between antimicrobial exposure and pregnancy outcomes.
Patients and Methods: A multi-center retrospective cohort study of pregnant patients (n=370) was conducted in 22 tertiary hospitals in China. Adverse pregnancy outcomes and admission of neonate to neonatal intensive care unit (NICU) were considered as outcomes. The effect of antimicrobial exposure on pregnancy outcomes was assessed using a multivariate logistic regression model.
Results: Use of first-generation cephalosporins during pregnancy was associated with a significantly higher risk of adverse pregnancy outcomes (odds ratio [OR]: 3.64 [95% confidence interval, CI: 1.43– 9.24], P = 0.007) and admission of neonate to the NICU (OR: 3.41, 95% CI: 1.37– 8.53, P=0.009) compared with use of third-generation cephalosporins, after adjusting for gestational age of exposure to antimicrobial agents, cesarean section, and antimicrobial dose. Similarly, a higher risk of adverse pregnancy outcomes (OR: 14.76, 95% CI: 4.43– 49.11) and neonatal NICU admission (OR: 11.74, 95% CI: 3.59– 38.35) were observed among women with first-generation cephalosporins use compared with mothers with no antimicrobial use.
Conclusion: Both first- and third-generation cephalosporins use was associated with an increased risk of adverse pregnancy and neonatal outcomes. In addition, first-generation cephalosporins were associated with an increased risk of those pregnant and neonatal outcomes, when compared with third-generation cephalosporins. We should require to determine the indications and contraindications for use of cephalosporins during pregnancy.
Keywords: maternal infections, antimicrobial agents, adverse pregnancy outcomes, NICU, cephalosporin
Introduction
Infectious diseases commonly occur during pregnancy, due to changes in the maternal internal environment and weakened immune functions. Infection induces the production of numerous inflammatory cytokines.1 Most maternal pathogens may transmit to the progeny through the placenta, birth canal, or even during postpartum breastfeeding, and the immune response triggered by these cytokines can adversely affect fetal development. Therefore, infection is one of the main causes of first-trimester abortion,2 premature delivery,3 premature rupture of membranes,4 and neonatal complications5 in the second and third trimesters.
Appropriate selection of the antimicrobial regime for treatment of infection during pregnancy is a key imperative to reduce adverse pregnancy outcomes. However, due to ethical constraints, it is difficult to prospectively assess the risks and benefits of different antimicrobials in infectious diseases during pregnancy. In previous study, antimicrobial therapy can prolong pregnancy and reduce neonatal morbidity in women with preterm premature rupture of membranes (PPROM) at a gestation of 34 weeks or less.6 However, due to the altered pharmacokinetics affecting the absorption and excretion of drugs, the use of antimicrobials during pregnancy is still controversial.7 There is inconsistent evidence regarding the association between gestational antimicrobial use and the risk of pregnancy outcomes. According to a meta-analysis of data from 61 studies, use of macrolides and clindamycin in women with a higher risk of preterm birth may lower the incidence of preterm birth, while metronidazole may increase the preterm birth rate when used alone in the second trimester.8 Accordingly, a large number of studies focused on exposure to a single antimicrobial or a combination of antimicrobials;9–12 there is a paucity of studies that have compared the outcomes between different antimicrobial agents. In addition, in most studies, only a few confounders were considered, such as the timing of use, the use of broad or narrow-spectrum antibiotics, and the dose.13–15 Moreover, this subject has rarely been investigated in the Chinese population. Therefore, we performed a multicenter retrospective cohort study to compare the effect of exposure to different antimicrobial agents on the pregnancy outcomes in Chinese pregnant women with infectious diseases, after adjusting for confounders related to the obstetric history and antimicrobial use.
Materials and Methods
Data Source
A multi-center study was conducted in 22 tertiary hospitals in China (6 general hospitals and 16 maternity hospitals) (Supplementary Table 1). Data pertaining to the following variables were collected from the medical record system: demographic information, obstetric history, gestational age (GA) of exposure to antimicrobial agents, GA at delivery, information about infectious disease, pathogenic bacteria, onset time, treatment time, course and dose of antimicrobial used, treatment outcomes, and the condition of neonate, birth weight, and Apgar score. This research was approved by the Ethics Committee of Department of Obstetrics and Gynecology affiliated to Fudan University (2020–131). All data are available at the ResMan Manager of Chinese Clinical Trial Registry (Registration number: ChiCTR2100044398). Informed consents were obtained.
Study Population
This was a retrospective cohort study based on the above database. Antimicrobial use was considered as exposure, and pregnant patients were followed-up until delivery. The endpoint event was maternal and neonatal health condition and development of adverse pregnancy outcomes or neonatal intensive care unit (NICU) admission. The study included patients treated between January 1, 2009, and December 31, 2020. Inclusion criteria: (1) maternal age >20 years; (2) GA at the time of hospital admission with infectious disease: <37 weeks; (3) admitted to hospital due to an infectious disease diagnosed according to the Chinese version of International Classification of Diseases-Tenth Revision.16 The exclusion criterion was exposure to antitumor drugs, incomplete records, and puerperal infections. Finally, a total of 370 pregnant women were included in this study. The flow chart of the study population is shown in Figure 1.
 |
Figure 1 Flow chart of the study population. |
Measurements
Exposure variables: Antimicrobial agents were classified according to Anatomic Therapeutic Chemical (ATC) classification system.17 The control group consisted of all those who did not redeem any prescriptions. Those who received at least one prescription were defined as exposure group. See Supplementary Table 2 for the specific types and names of antimicrobial agents.
Outcome variables: There were two outcome variables of interest. First, the pregnancy outcome was coded as healthy or adverse [including premature birth (ICD-10:060); abortion (ICD-10:004); and undefined fetal death (ICD-10: P95)]. Second, admission of infant to the NICU, which is typically due to any of the following conditions: birth trauma, hypoxia/asphyxia, shock/resuscitation, infection/sepsis, respiratory complications, premature birth, low birth weight.18
Covariates: Based on previous literature on antimicrobial use in pregnancy,19 the covariates examined in this study covered the following three domains: demographic characteristics, obstetric history, and factors related to antimicrobial use. Demographic characteristics included maternal age (20-, 35-, 45-), GA of maternal exposure to antimicrobial agents (first trimester: 1–13 weeks, second trimester: 13–27 weeks, third trimester: >27 weeks), and complications. Obstetric history included history of pregnancies, birth, and abortions, delivery type (normal childbirth, cesarean section, or obstetric forceps). Antimicrobial use-related factors included drug administration route, drug dose (defined daily dose, DDD, higher value represents higher tendency of clinical use), whether single antimicrobial or combination used, and the spectrum of activity of the antibiotic. Based on previous research, second- and third-generation cephalosporins, macrolides, penicillins, and streptomycin were considered as broad-spectrum antibiotics, and the first-generation cephalosporins and other antibiotics such as β-lactamase sensitive penicillins were considered as narrow-spectrum antibiotics.
Statistical Analysis
First, chi-square test or Fisher's exact test was used to compare the baseline characteristics between pregnant women with healthy and adverse pregnancy and neonatal outcomes. Second, univariate logistic regression was applied to explore the association between covariates and the two outcome variables. Variables that showed a significant (P < 0.05) association on univariate analysis were included in multivariate logistic regression analysis. Third, the effect of antimicrobial use on the two outcomes of interest was estimated using multivariate logistic regression. Moreover, third-generation cephalosporins were used as a reference to test the above relationship again.
SPSS 25.0 software was used to establish the database and to perform data analysis. For all statistical tests, two-sided P values <0.05 were considered indicative of statistical significance.
Results
Baseline Characteristics
This multi-center retrospective cohort study included 370 pregnant women treated at 22 hospitals, which represents the widest coverage by any study on this subject in China. The study population showed a wide geographical distribution across the country (Figure 2). The highest number of cases belonged to the eastern region (99 and 30 cases treated at specialized hospitals and general hospitals, respectively), while the western region accounted for the lowest number of cases (16 treated at specialized hospitals).
 |
Figure 2 Distribution of included cases. (A) The distribution of hospitals. (B) The distribution of included pregnant women. |
As shown in Table 1 and Table 2, 37 patients with upper respiratory tract bacterial infection or gastritis did not receive antimicrobial treatment due to mild symptoms; 54.05% of these patients experienced adverse pregnancy outcomes and 51.35% neonates required NICU admission. Among the 333 pregnant women who used antimicrobial agents, 60.06% experienced adverse outcomes and 60.36% of neonates required NICU admission. Maternal age, GA of exposure to antimicrobial agents, number of pregnancies and abortions, delivery type, complications, single/combined drug use, drug dose, the spectrum of antibiotic, and its type were all significantly different between patients with healthy and adverse pregnancy outcomes. Similar results were observed concerning neonatal outcomes. A total of 333 patients (90%) have used at least one antimicrobial; among these, 269 (72.7%) have used only one kind of antimicrobial. The most commonly used antimicrobial agents were third-generation cephalosporins (26.76%) followed by first-generation cephalosporins (15.68%).
 |
Table 1 Baseline Characteristics Stratified by Pregnancy and Neonatal Outcomes |
 |
Table 2 Characteristics Related to Drug Use Stratified by Pregnancy and Neonatal Outcomes |
Antimicrobial Use in Infectious Disease
Pathogenic microorganisms were identified in only approximately one-third of cases; the gram-negative bacteria included Escherichia coli and Pseudomonas aeruginosa; and gram-positive bacteria included group B streptococcus and Staphylococcus aureus. Mycoplasma with urealyticum and Candida albicans were the main fungi. The majority of cases received empirical antimicrobial therapy prior to the detection of the causative organism.
A total of 19 infectious diseases were found in 370 patients. Specific diseases, diagnoses, and the number of cases are listed in Supplementary Table 3. The top three disease diagnoses were urethritis (N71), vaginitis or vulvitis (N76), and acute upper respiratory infection (J06). More than half of all cases with cystitis, acute nephritic syndrome, acute appendicitis, gastritis and duodenitis, or acute bronchitis received third-generation cephalosporins; other commonly used drugs were second-generation cephalosporins followed by penicillins. For infection of the reproductive system, such as vaginitis or vulvitis, cervicitis, and urethritis, a lower proportion of cases were treated with third-generation cephalosporins, while a greater proportion was treated with second-generation cephalosporins and antifungal agents. The use of antimicrobial for different diseases is illustrated in Figure 3.
 |
Figure 3 Trends of antibacterial agents for different diagnosis categories. |
Univariate Regression
The results of univariate logistic regression are shown in Table 3. The same set of variables showed a significant association for both pregnancy and neonatal outcomes. Maternal age, GA of exposure to antimicrobial agents, number of abortions, delivery type, single or combined use, dose, first-generation cephalosporins, and combined use were all significantly associated with pregnancy and neonatal outcomes (P < 0.05). Since whether or not combined use was included in the antimicrobial classification, this variable was not included in the subsequent multivariate regression.
 |
Table 3 Results of Univariate Logistic Regression Showing Factors Associated with Pregnancy Outcome and NICU Admission |
Multivariate Regression
Furthermore, a multivariate regression model was used to explore the differences in outcomes after adjusting for maternal age, GA of exposure to antimicrobial agents, number of abortions, delivery type, and drug dose. When compared with no antimicrobial use (Table 4), use of antimicrobial combination was a risk factor for adverse pregnancy outcome [odds ratio (OR): 18.94, 95% CI: 5.24–68.38], followed by use of first-generation cephalosporins (OR: 14.76, 95% CI: 4.43–49.12), as well as third-generation cephalosporins (OR: 4.033, 95% CI: 1.424–11.424), Moreover, GA of exposure to antimicrobial agents near delivery was associated with an increased risk of adverse pregnancy outcomes. Compared with normal vaginal delivery, cesarean section was associated with an increased risk of adverse pregnancy outcomes. Concerning neonatal outcome, in addition to GA of exposure to antimicrobial agents, delivery type, antimicrobial dose, and the number of previous abortions were significant risk factors for NICU admission.
 |
Table 4 Results of Multivariate Logistic Regression Showing the Effect of Antimicrobial Use on the Pregnancy and Neonatal Outcome (Non-Exposure as Reference) |
On the other hand, somewhat different results were obtained when using those exposed to third-generation cephalosporins (most commonly used) as a reference in multivariate regression (Table 5). Use of first-generation cephalosporins during pregnancy was associated with a significantly higher risk of adverse pregnancy outcomes (odds ratio [OR]: 3.63 [95% confidence interval, CI: 1.43–9.24], P = 0.007) and admission of neonate to the NICU (OR: 3.41, 95% CI: 1.37–8.53) compared with use of third-generation cephalosporins. While use of antifungal agents (OR: 0.230, 95% CI: 0.061–0.874) was associated with a lower risk of pregnancy outcomes. As for neonatal outcomes, use of first-generation cephalosporins (OR: 3.414, 95% CI: 1.366–8.529) and use of combination antimicrobial therapy (OR: 4.116, 95% CI: 1.702–9.956) were risk factors compared with third-generation cephalosporins.
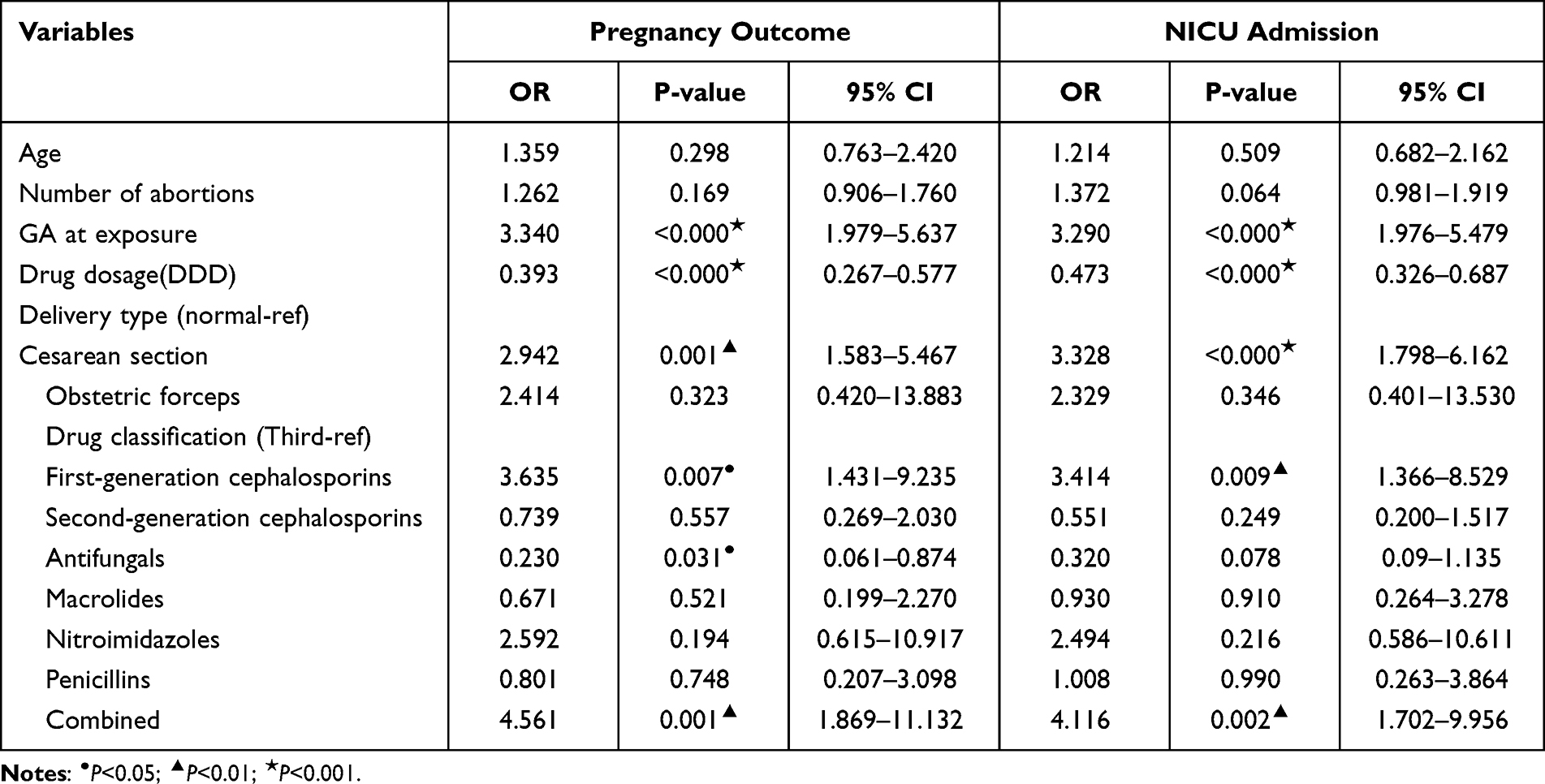 |
Table 5 Results of Multivariate Logistic Regression Analysis Showing the Effect of Antimicrobial Use on Pregnancy and Neonatal Outcomes (Third-Generation Cephalosporins as Reference) |
Discussion
The morbidity and mortality burden attributable to infection during pregnancy is an ongoing concern.20 Severe infection during pregnancy is a major health problem across the world. Use of antimicrobial agents during pregnancy can affect the gut flora of the newborn, which has a critical impact on the development of innate immunity. Perinatal use of antimicrobial agents can adversely affect immune tolerance and increase the risk of allergic and autoimmune diseases in early childhood.21
In this retrospective cohort study, we examined the effect of antimicrobial exposure on pregnant patients and neonates. In our cohort, cephalosporins, especially third-generation cephalosporins, were the most commonly used antimicrobial drugs to treat infection in pregnancy. Compared with third-generation cephalosporins, use of first-generation cephalosporins and combination of antimicrobial agents were significant risk factors for adverse pregnancy outcomes, while use of antifungal drugs was associated with reduced risk of adverse pregnancy outcomes, even after adjusting for age, GA of exposure to antimicrobial agents, number of abortions, delivery type, and drug dose.
In our study, parenteral ceftriaxone sodium was the most commonly used third-generation cephalosporin, while parenteral cefazolin sodium was the most commonly used first-generation cephalosporin. Cefazolin is characterized as a narrow spectrum antimicrobial, which is most effective against streptococcal and staphylococcal infections, and it has a destructive effect on the bacterial cell wall. Cefazolin is used for the treatment of urological diseases, for the prevention of postoperative infections. While ceftriaxone exhibits a broad spectrum of activity against Enterobacteriaceae and some Gram-positive bacteria, including Streptococcus spp. and MSSA.22 And is used to treat infectious diseases of the upper respiratory tract, lungs, kidneys, and many others. A randomized, double-blind trial showed comparable efficacy of a single daily dose of intravenous ceftriaxone with that of multiple doses of cefazolin for the treatment of acute pyelonephritis in pregnancy.23 This indicated the safety and benefits of use of ceftriaxone during pregnancy.
Clotrimazole tablets were the most commonly used antifungal agents in our cohort. The mechanisms of action of antifungal drugs include targeting the synthesis of the fungal cell membrane, cell wall components, membrane permeability, synthesis of nucleic acids, and the mitotic spindle function of the fungi during cell division. However, vaginal route of administration may have less impact on matrix than parenteral route, besides, compared with other infectious diseases, the symptoms of vaginitis were lighter, which may have biased our results.
Some limitations of our study should be acknowledged. The antimicrobial exposure rate and the OR may have been overestimated due to the limited sample size. Moreover, our study population comprised only hospitalized pregnant women who are more likely to be prescribed antimicrobial agents for treatment of infection. Moreover, the measurement of drug dose (DDD) does not necessarily reflect the doses dispensed. DDD may not be a reliable measure of antimicrobial consumption. Nonetheless, our study compared the use of different antimicrobial agents during pregnancy and examined some crucial confounding variables, which have seldom been adjusted for in previous studies. Future studies should include prescribed daily doses in the analysis for a more robust evaluation of antimicrobial consumption.
Conclusion
Although previous studies have demonstrated the safety of the use of cephalosporins during pregnancy, our results indicated an association between adverse pregnancy outcomes and cephalosporins exposure, especially first-generation cephalosporins. The use of combination antimicrobial therapy also significantly increased the risk of adverse pregnancy outcomes. Our results underline the need for detailed guidelines for use of cephalosporins in pregnant women to minimize avoidable risks.
Highlights
- The retrospective cohort study showed effects of antimicrobial on pregnant women.
- Cephalosporins were the most commonly used antimicrobial drugs during pregnancy.
- Use of first-generation cephalosporins was risky for adverse pregnancy outcomes.
Ethical Approval Statement
This research was approved by the Ethics Committee of Department of Obstetrics and Gynecology affiliated to Fudan University (2020-131). All data are available at the ResMan Manager of Chinese Clinical Trial Registry (Registration number: ChiCTR2100044398). Informed consents were obtained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was supported by the project of health industry research of the Shanghai Municipal Health Commission (201940153).
Disclosure
There are no conflicts of interest to disclose.
References
1. Hamilton-Miller JM. Immunopharmacology of antibiotics: direct and indirect immunomodulation of defence mechanisms. J Chemother. 2001;13(2):107–111. doi:10.1179/joc.2001.13.2.107
2. Logan S, Price L. Infectious disease in pregnancy. Obstet Gynaecol Reproduc Med. 2011;21(12):331–338. doi:10.1016/j.ogrm.2011.09.012
3. Jacobsson B, Pettersson K, Modzelewska D, Abrahamsson T, Bergman L, Hakansson S. [Preterm delivery: an overview on epidemiology, pathophysiology and consequences for the individual and the society] Fortidsbord storsta perinatala problemet - 5,7 procent av graviditeter i Sverige slutar for tidigt, inte klarlagt varfor - kostar miljardbelopp varje ar. Lakartidningen. 2019;116:15. Swedish.
4. Tchirikov M, Schlabritz-Loutsevitch N, Maher J, et al. Mid-trimester preterm premature rupture of membranes (PPROM): etiology, diagnosis, classification, international recommendations of treatment options and outcome. J Perinat Med. 2018;46(5):465–488. doi:10.1515/jpm-2017-0027
5. Pesch MH, Saunders NA, Abdelnabi S. Cytomegalovirus infection in pregnancy: prevention, presentation, management and neonatal outcomes. J Midwifery Womens Health. 2021;66(3):397–402. doi:10.1111/jmwh.13228
6. Hutzal CE, Boyle EM, Kenyon SL, et al. Use of antibiotics for the treatment of preterm parturition and prevention of neonatal morbidity: a metaanalysis. Am J Obstet Gynecol. 2008;199(6):620.e1–620.e8. doi:10.1016/j.ajog.2008.07.008
7. Muanda FT, Sheehy O, Bérard A. Use of antibiotics during pregnancy and risk of spontaneous abortion. CMAJ. 2017;189(17):E625–E633. doi:10.1503/cmaj.161020
8. Morency AM, Bujold E. The effect of second-trimester antibiotic therapy on the rate of preterm birth. J Obstet Gynaecol Can. 2007;29(1):35–44. doi:10.1016/S1701-2163(16)32350-7
9. Daniel S, Doron M, Fishman B, Koren G, Lunenfeld E, Levy A. The safety of amoxicillin and clavulanic acid use during the first trimester of pregnancy. Br J Clin Pharmacol. 2019;85(12):2856–2863. doi:10.1111/bcp.14118
10. Wasz-Hockert O, Nummi S, Vuopala S, Jarvinen PA. Transplacental passage of azidocillin, ampicillin and penicillin G during early and late pregnancy. Scand J Infect Dis. 1970;2(2):125–130. doi:10.3109/inf.1970.2.issue-2.09
11. Yefet E, Schwartz N, Chazan B, Salim R, Romano S, Nachum Z. The safety of quinolones and fluoroquinolones in pregnancy: a meta-analysis. BJOG. 2018;125(9):1069–1076. doi:10.1111/1471-0528.15119
12. Batagol R. Dangers of tetracyclines in pregnancy. Med J Aust. 1980;2(10):578. doi:10.5694/j.1326-5377.1980.tb100784.x
13. Milliken S, Allen RM, Lamont RF. The role of antimicrobial treatment during pregnancy on the neonatal gut microbiome and the development of atopy, asthma, allergy and obesity in childhood. Expert Opin Drug Saf. 2019;18(3):173–185. doi:10.1080/14740338.2019.1579795
14. Subtil D, Brabant G, Tilloy E, et al. Early clindamycin for bacterial vaginosis in pregnancy (PREMEVA): a multicentre, double-blind, randomised controlled trial. Lancet. 2018;392(10160):2171–2179. doi:10.1016/S0140-6736(18)31617-9
15. Ford N, Shubber Z, Jao J, Abrams EJ, Frigati L, Mofenson L. Safety of cotrimoxazole in pregnancy: a systematic review and meta-analysis. J Acquir Immune Defic Syndr. 2014;66(5):512–521. doi:10.1097/QAI.0000000000000211
16. NHaFPCotP SAotP. Classification and Code of Diseases. Beijing: Standards Press of China; 2016.
17. Zhao H, Wei L, Li H, et al. Appropriateness of antibiotic prescriptions in ambulatory care in China: a nationwide descriptive database study. Lancet Infect Dis. 2021;21:S1473-3099(20)30596–X. PMID: 33515511. doi:10.1016/S1473-3099(20)30596-X
18. Haidari ES, Lee HC, Illuzzi JL, Phibbs CS, Lin H, Xu X. Hospital variation in admissions to neonatal intensive care units by diagnosis severity and category. J Perinat. 2021;41(3):468–477. doi:10.1038/s41372-020-00775-z
19. Amann U, Egen-Lappe V, Strunz-Lehner C, Hasford J. Antibiotics in pregnancy: analysis of potential risks and determinants in a large German statutory sickness fund population. Pharmacoepidemiol Drug Saf. 2006;15(5):327–337. doi:10.1002/pds.1225
20. Kourtis AP, Read JS, Jamieson DJ. Pregnancy and infection. N Engl J Med. 2014;370(23):2211–2218. doi:10.1056/NEJMra1213566
21. Russell ARB, Steer PJ. Antibiotics in preterm labour--The ORACLE speaks. Lancet. 2008;372(9646):1276–1278. doi:10.1016/S0140-6736(08)61248-9
22. Zelenitsky SA, Beahm NP, Iacovides H, Ariano RE, Zhanel G. Limitations of ceftriaxone compared with cefazolin against MSSA: an integrated pharmacodynamic analysis. J Antimicrob Chemother. 2018;73(7):1888–1894. doi:10.1093/jac/dky120
23. Sanchez-Ramos L, McAlpine KJ, Adair CD, Kaunitz AM, Delke I, Briones DK. Pyelonephritis in pregnancy: once-a-day ceftriaxone versus multiple doses of cefazolin. A randomized, double-blind trial. Am J Obstet Gynecol. 1995;172(1 Pt 1):129–133. doi:10.1016/0002-9378(95)90100-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.