Back to Journals » Journal of Asthma and Allergy » Volume 16
Effect of Acute PM2.5 Exposure on Lung Function in Children: A Systematic Review and Meta-Analysis
Authors Zhang Y, Guo Z, Zhang W, Li Q, Zhao Y, Wang Z, Luo Z
Received 26 January 2023
Accepted for publication 19 April 2023
Published 10 May 2023 Volume 2023:16 Pages 529—540
DOI https://doi.org/10.2147/JAA.S405929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor David Price
Yueming Zhang,1– 3 Ziyao Guo,1,2 Wen Zhang,3 Qinyuan Li,1,2 Yan Zhao,1,2 Zhili Wang,1,2 Zhengxiu Luo1,2
1Department of Respiratory Medicine, Children’s Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2National Clinical Research Center for Child Health and Disorders, Ministry of Education Key Laboratory of Child Development and Disorders, Chongqing Key Laboratory of Pediatrics, Chongqing, People’s Republic of China; 3Department of Respiratory, Xi’an Children’s Hospital, Xi’an, Shaanxi, People’s Republic of China
Correspondence: Zhengxiu Luo, Department of Respiratory Medicine, Children’s Hospital of Chongqing Medical University, Chongqing, People’s Republic of China, Email [email protected]
Objective: The objective of this study was to conduct a systematic review and meta-analysis to identify the adverse effects of acute PM2.5 exposure on lung function in children.
Design: Systematic review and meta-analysis. Setting, participants and measures: Eligible studies analyzing PM2.5 level and lung function in children were screened out. Effect estimates of PM2.5 measurements were quantified using random effect models. Heterogeneity was investigated with Q-test and I2 statistics. We also conducted meta-regression and sensitivity analysis to explore the sources of heterogeneity, such as different countries and asthmatic status. Subgroup analyses were conducted to determine the effects of acute PM2.5 exposure on children of different asthmatic status and in different countries.
Results: A total of 11 studies with 4314 participants from Brazil, China and Japan were included finally. A 10 μg/m3 increase of PM2.5 was associated with a 1.74L/min (95% CI: − 2.68, − 0.90) decrease in peak expiratory flow (PEF). Since the asthmatic status and country could partly explain the heterogeneity, we conducted the subgroup analysis. Children with severe asthma were more susceptible to PM2.5 exposure (− 3.11 L/min per 10 μg/m3 increase, 95% CI − 4.54, − 1.67) than healthy children (− 1.61 L/min per 10 μg/m3 increase, 95% CI − 2.34, − 0.91). In the children of China, PEF decreased by 1.54 L/min (95% CI − 2.33, − 0.75) with a 10 μg/m3 increase in PM2.5 exposure. In the children of Japan, PEF decreased by 2.65 L/min (95% CI − 3.82, − 1.48) with a 10 μg/m3 increase of PM2.5 exposure. In contrast, no statistic association was found between every 10 μg/m3 increase of PM2.5 and lung function in children of Brazil (− 0.38 L/min, 95% CI − 0.91, 0.15).
Conclusion: Our results demonstrated that the acute PM2.5 exposure exerted adverse impacts on children’s lung function, and children with severe asthma were more susceptible to the increase of PM2.5 exposure. The impacts of acute PM2.5 exposure varied across different countries.
Keywords: particulate matter 2.5, PM2.5, children, peak expiratory flow, PEF, acute exposure, meta-analysis
Introduction
Air pollution, a culprit of human respiratory problems, is challenging human health worldwide.1 The fine particulate matters of different aerodynamic diameters, such as particulate matter 2.5 (PM2.5), PM1.0, PM10, are the major contributors to air pollution. PM2.5 is defined as the most harmful type of air fine particulate matter with an aerodynamic equivalent diameter of less than 2.5µm.2 As a major pollutant, PM2.5 is characterized by small size, complex composition, allergen absorptivity and sensitization-enhancing property.3 The sources of PM2.5 include automobile emissions, urban constructions, smokestacks, power plants, industrial and biomass burning.3 PM2.5 not only penetrates into the deep tissue of the human respiratory system due to its small size but also carries toxic and harmful substances, such as transition metals and polycyclic aromatic hydrocarbons (PAHs), into human bodies.4 PM2.5 brings with a myriad of different adverse effects, such as asthma,5 chronic obstructive pulmonary disease (COPD),3 cardiovascular disease,6 and cancer.7 Exposure to PM2.5 confers an increased risk of wheeze-associated disorders,8 asthma-related emergency and hospitalization in children.9
Lung function is an early indicator to evaluate and quantify the effect of air pollution on the respiratory system and a sub-clinical marker with clinical implications for lung health across the lifespan.10 Children are more susceptible to air pollution because of their faster breath rate and immature immunity.11 The developmental trajectory of lungs is divided into three phases: the growth phase, the plateau phase, and the decrement phase.12 The growth phase is critical for lung function.12 Toxic exposure in the growth phase is associated with future adverse clinical outcomes, such as propensity to develop respiratory diseases and early multimorbidity.13 Hence, it is urgent to investigate the effects of PM2.5 exposure on childhood lung function.
Previous meta-analyses indicated that both acute and long-term exposure to outdoor PM2.5 was significantly associated with decreased lung function in healthy and asthmatic adults.14,15 One meta-analysis based on European birth cohort study revealed that long-term exposure to PM2.5 resulted in decreased lung function in schoolchildren.16 However, this study only focused on the relation between PM2.5 exposure and FEV1 alteration during a long-term exposure. Acute and long-term PM2.5 exposure may have different impacts. Multiple meta-analyses revealed that the acute exposure of PM2.5 had an adverse impact on pediatric asthma hospital visits and exacerbation.17,18 Children undergo a growth phase of lungs, but there were few meta-analyses clarifying the association between acute exposure of PM2.5 and childhood lung function. The objective of this study was to quantify the effect of acute outdoor PM2.5 exposure on the lung function of children by performing a comprehensive systematic review and meta-analysis.
Methods
Patients and Ethics
No patients involved.
Design
This study followed the Preferred Reporting in Systematic Reviews and Meta-Analyses (PRISMA) guidelines.19
Literature Search and Selection
A comprehensive literature search was conducted to identify articles published on the acute effect of PM2.5 on children’s lung function. We systematically searched Embase, PubMed, the Cochrane library, Web of Science, China biomedical literature database (CNKI), and Chinese Biomedical Literature (CBM) databases for literature published before February 2022 and identified the studies describing the relationship between acute PM2.5 exposure and lung function in children aged 18 years or younger with no geographical or linguistic restrictions. The PubMed search string used was as follows:
(PM2.5 OR Ultrafine Fibers OR Ultrafine Fiber OR Fiber, Ultrafine OR Airborne Particulate Matter OR Particulate Matter, Airborne OR Air Pollutants, Particulate OR Particulate Air Pollutants OR Ambient Particulate Matter OR Particulate Matter, Ambient OR Particulate Matter*) AND (children OR Child*) AND (Function Test, Respiratory OR Function Tests, Respiratory OR Test, Respiratory Function OR Tests, Respiratory Function OR Pulmonary Function Tests OR Function Test, Pulmonary OR Function Tests, Pulmonary OR Test, Pulmonary Function OR Tests, Pulmonary Function OR Lung Function Tests OR Function Test, Lung OR Function Tests, Lung OR Lung Function Test OR Test, Lung Function OR Tests, Lung Function OR Pulmonary Function Test OR Respiratory Function Tests*).
Detailed search strategies are presented in Additional Table 1. In order to avoid bias, two reviewers independently assessed the eligible studies by examining the full text of articles based on the pre-defined eligibility criteria.
Inclusion and Exclusion Criteria
Studies examining the relationship between acute (daily) exposure to outdoor air PM2.5 and lung function in children were eligible for this review. The review process is shown in Figure 1. Studies were included when meeting all the following criteria: (i) quantitatively analyzing the changes in lung function indexes with every 10 μg/m3 PM2.5 increase; (ii) involving children aged 18 years or younger as study subjects; (iii) published in full-text; (iv) analyzing acute exposure to PM2.5. Studies were excluded if meeting any of the following criteria: (i) published in reviews, conference abstracts, editorial letters, or comments; (ii) not related to ambient PM2.5 (eg, only related to indoor, passive smoking or other pollutions); (iii) without measurement of lung function in children; (iv) without quantitative results for the effects; (v) only analyzing long-term exposure to PM2.5; (vi) with insufficient data.
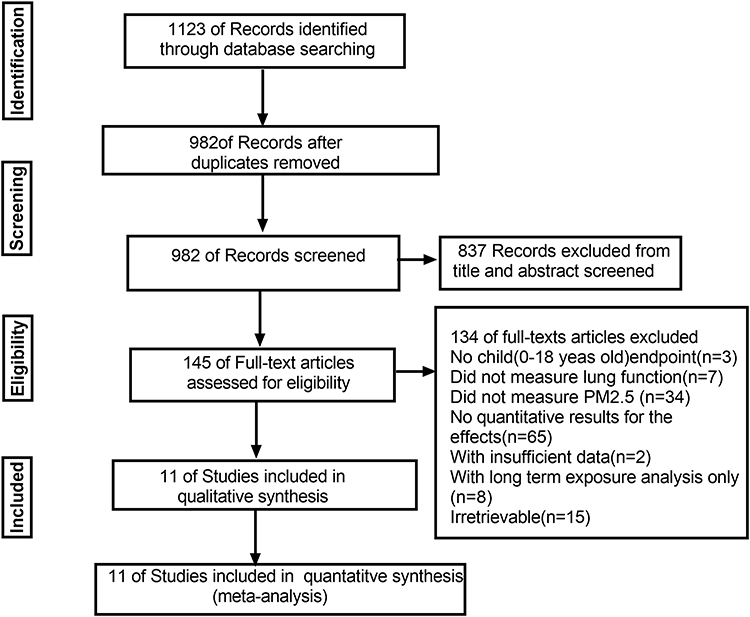 |
Figure 1 Flow diagram of the selection procedure of studies. Notes: A PRISMA flow diagram that details the inclusion and exclusion of studies considered for this systematic review. PRISMA figure adapted from Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009, 339:b2535. Creative Commons.19 |
Data Extraction
Two reviewers extracted the data from the eligible literature, including study time, study types, country, simple size, average age of population, daily mean concentration of PM2.5, controlled variables, lag days of exposure, and statistical analysis model. All effect measurements were transformed to per 10µg/m3 increase in PM2.5, assuming a linear relationship between the concentration of particulate matter and lung function. Some studies assessed the effect of acute exposure to air pollution by different time periods (lag of 0, 1, or 2 days, etc.). We defined the acute exposure effect as 1 day (lag 1) to 7 days (lag 7) after exposure to PM2.5. In order to reduce the heterogeneity among the original studies, we recorded the effect noted at 1 day after exposure whenever possible. The reviewers then used a standardized data extraction format in Microsoft Office Excel 2019 to extract all the data needed. A third person resolved the disagreement between the two reviewers. Extraction of these data is presented in Table 1, according to the Preferred Reporting Items for Systematic and Meta-analyses (PRISMA) guidelines.19
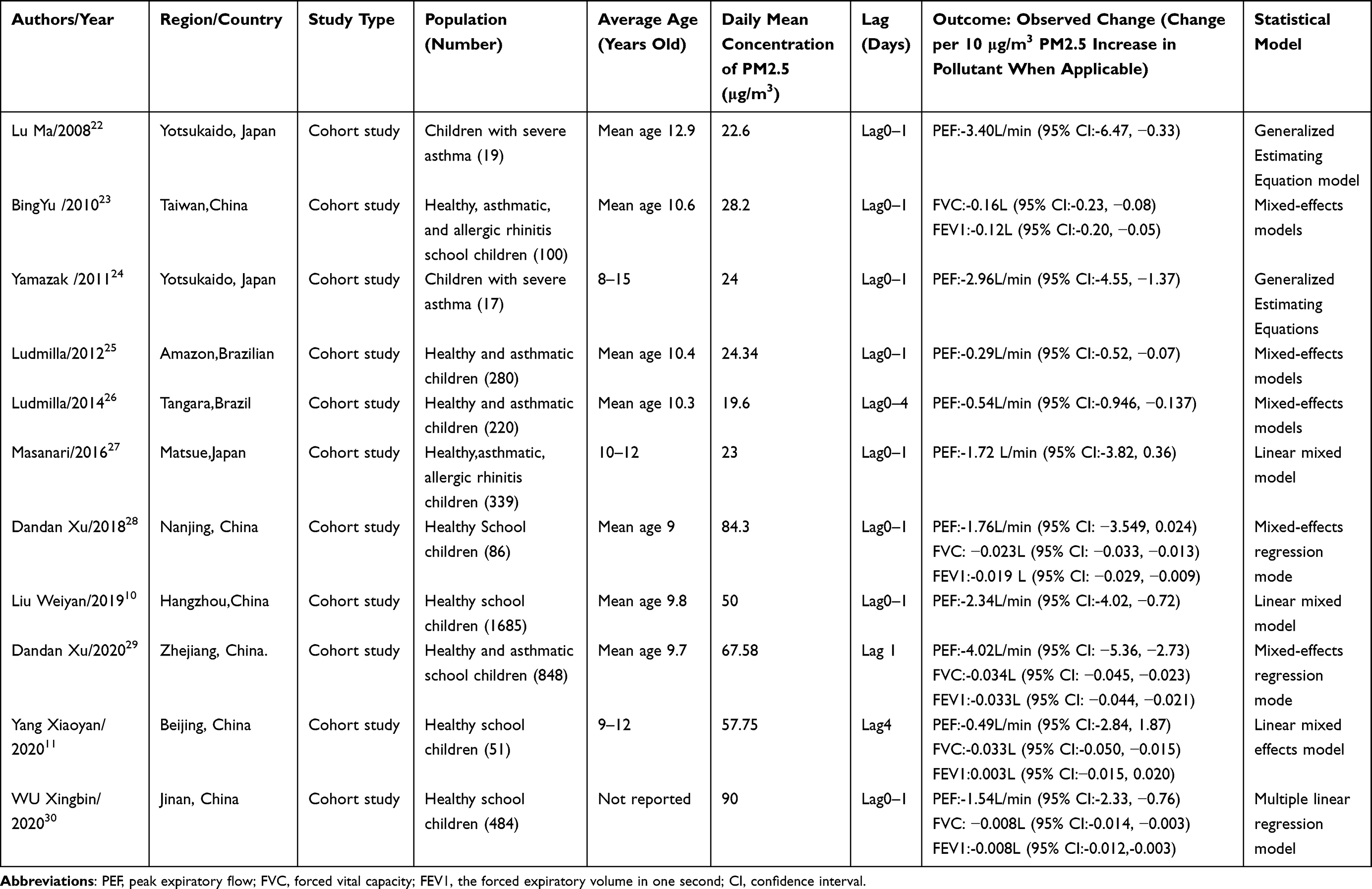 |
Table 1 Study Characteristics |
Study Quality Assessment
Two investigators independently performed quality assessment of the cohort studies using the Newcastle-Ottawa Scale (NOS).20 NOS contains 8 items with 9 as the highest score, and a maximum of 2 scores could be obtained for comparability. The scales and grading are presented in Additional Figure 1. Adjustment for confounding was based on three factors: (a) asthma status, asthmatic medicinal usage, passive smoking; (b) environmental parameters, such as temperature and humidity; (c) individual factors, such as age, gender, BMI, height, weight and other co-morbidities (eg, allergic rhinitis, allergic conjunctivitis, atopic dermatitis, food allergy and medication use). The quality was considered good if all 3 factors, fair if 2 factors and poor if 1 or less factors were adjusted.
Statistical Analysis
To determine the effect of acute PM2.5 exposure on lung function in children, we conducted the meta-analysis separately for different indices such as PEF, FEV1and FVC. Effect estimates per 10 μg/m3 were combined to calculate summary effect estimates using generic inverse variance method assuming a random effects model or a fixed effects model. A forest plot was used to assess visually the change of indicators of children’s lung function and corresponding 95% confidence. If a confidence interval was presented, the corresponding standard error was calculated as (upper CI − lower CI)/(xn − x0 × 3.92), where CI referred to confidence interval, xn denoted exposure at the level of group n, and x0 denoted exposure at the reference group. The standard error was calculated following the method recommended by published articles.21 Heterogeneity among studies was statistically investigated with the Q-test and the I2 statistics. When I2>50%, the random effects model was used; when I 2<50%, the fixed effects model was used. Publication bias was assessed using funnel plot and Egger’s linear regression method. We also performed meta-regression analysis of the source of heterogeneity. Considering that the heterogeneity between groups of FEV1 and FVC was 0%, meta-regression and subgroup analysis were conducted to clarify the impact of asthmatic status on PEF of children. Meta-regression included the following potential covariates: country, severe asthma status, sample size, statistic methods, and publication year. We also performed a subgroup analysis by dividing the children into three country groups and severe asthma status. We performed sensitivity analysis by omitting one study in each turn to assess the stability of the results of change of PEF. All analyses were performed using the R computing framework (www.r-project.org).
Results
Literature Search
We systematically searched PubMed, Embase, Web of Science, the Cochrane library, China biomedical literature database (CBM) and Chinese National Knowledge Infrastructure (CNKI) and identified 1123 studies in the initial search (Figure 1). Among the 145 studies published in full-text reviews, 134 were excluded, and ultimately 11 studies were included in this meta-analysis.10,11,22–30 The primary reason for exclusion was the lack of quantitative results about the effects. Other reasons included the lack of outdoor PM2.5 measurement or lung function.
Characteristics of Included Studies
The characteristics of the 11 studies examining the association between acute exposure to outdoor PM2.5 and lung function in children are described in Table 1. Of these studies, ten studies examined the association between PEF and acute exposure to PM2.5.10,11,22,24–30 Data from 4129 individuals from three different countries were examined in these reports. Among these studies, six were conducted in China, three in Japan, and two in Brazil. Two studies included children with severe asthma, three studies included both healthy and asthmatic children, two studies included healthy, asthmatic, allergic rhinitis school-age children, and four studies only included healthy children. All the studies focused on the acute exposure of PM2.5 and lung function in children.
Risk of Bias Among Included Studies
The quality of included studies was assessed by the two authors. By applying the NOS, study quality was appraised as follows: eight studies were rated as good,10,22–27,29 and three as fair.11,28,30 Five studies that included both asthmatic and healthy children failed to provide the exact information about the quantitative lung function change of two groups of children,23,25–27,29 so they were not considered as healthy or asthmatic group in subgroup analysis. The results for each item from each study are shown in Additional Table 2.
Meta-Analyses
The association between acute exposure to ambient PM2.5 and lung function indicators in children is graphically displayed in Figure 2. A significant association was found between PM2.5 exposure and PEF (L/min) in children (P < 0.01). A 10 μg/m3 increase of PM2.5 was associated with a change in PEF of −1.74L/min (95% CI: −2.68, −0.90). In contrast, no statistically significant associations of a 10 μg/m3 increase of PM2.5 with FVC and FEV1 were observed (−0.03L [95% CI: −0.08, −0.01] and – 0.02L [95% CI: −0.05, 0.00], respectively). There was substantial heterogeneity among studies included in the PEF analysis (I2 = 70.89%), but low heterogeneity among studies included in the FVC (I2 = 0.0%) and FEV1 (I2 = 0.0%) analyses, respectively. There was no statistical evidence of publication bias for any of the analyses (Egger’s regression test: p = 0.15 for PEF, p = 0.40 for FVC, and p = 0.52 for FEV1). Forest plots of change in PEF, FVC, FEV1 with per 10 ug/m3 increase in PM2.5 level are shown in Figure 2. Funnel plots for the publication bias are provided in Additional Figures 2–4.
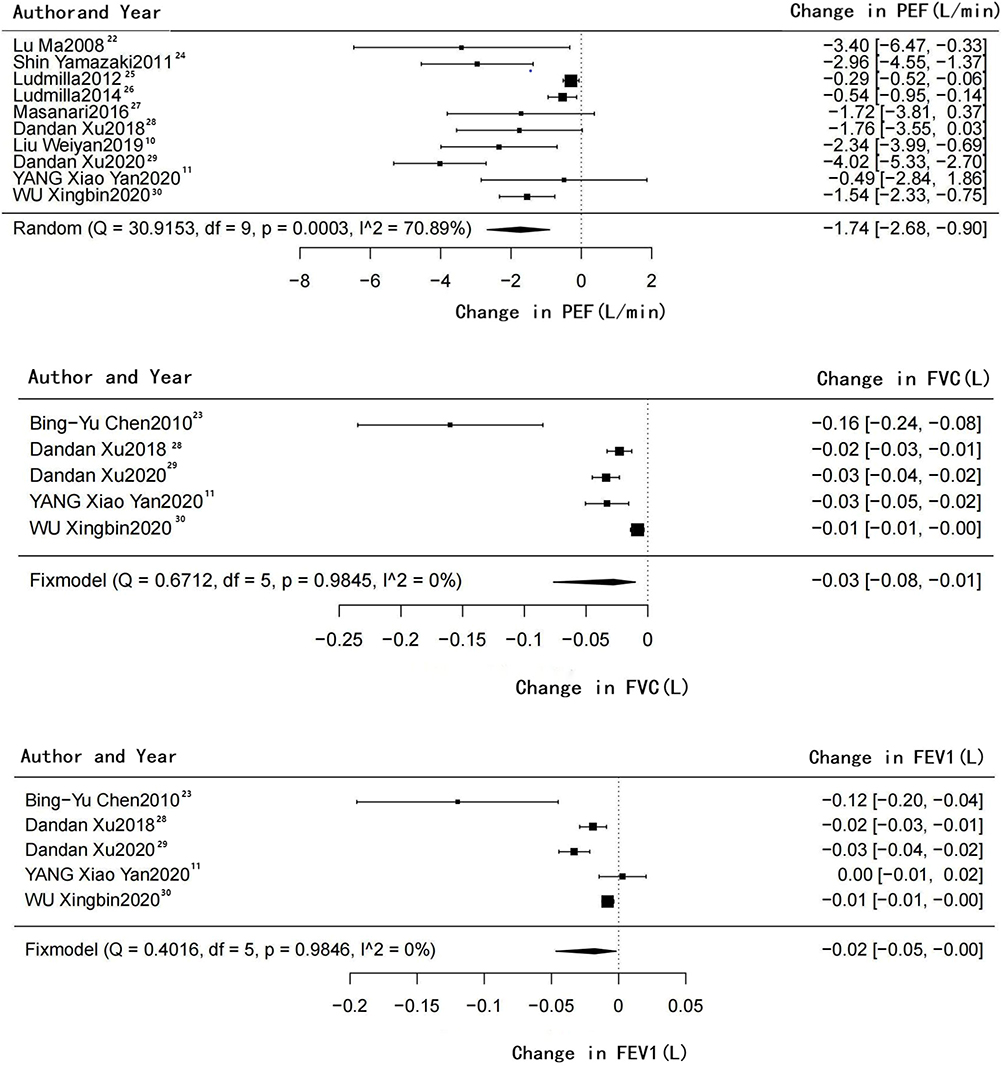 |
Figure 2 Forest plots of changes in PEF, FVC, FEV1 per 10 ug/m3 increase in PM2.5 level. Notes: The summary estimate for PEF was calculated using a random-effects meta-analysis. The summary estimates for FVC, FEV1 were calculated using a fixed-effects meta-analysis. |
Meta-Regression and Subgroup Analysis
We conducted the univariate meta-regression analysis and subgroup analysis for the studies included in the PEF analysis. Meta-regression results demonstrated that the studies in Brazil showed significant heterogeneity compared with those in other countries (P = 0.0261, R2 = 30.99%). The following factors could partly explain the heterogeneity but did not contribute to statistical significance: severe asthma status (P = 0.0906, R2 = 16.71%), study country (P = 0.0713, 36.79%), sample size (P = 0.0684, 21.71%). Since severe asthma status could partly explain the heterogeneity, we conducted subgroup analyses of the studies that included children with severe asthma and healthy children. There were two studies including the children with severe asthma and four studies including healthy children, so we performed subgroup analysis on these six studies. Four studies including both asthmatic and healthy children were not included in subgroup analysis due to insufficient data of the original research. When the concentration of ambient PM2.5 showed a 10 μg/m3 increase, there was a significant decrease in PEF (−1.61 L/min, −2.34, −0.91) in healthy subgroup, but a more significant decrease was found in severe asthmatic group (−3.11 L/min, −4.54, −1.67). We also conducted subgroup analyses of the studies in different countries. There were 10 studies involving three countries. Studies in Brazil showed a PEF changed by −0.38 L/min (−0.91, 0.15), which was not statistically significant. The results in China and Japan showed PEF changed by −1.54 L/min (−2.33, −0.75) and −2.65 L/min (−3.82, 0.36), respectively. The results of subgroup analysis and meta-regression are described in Table 2 and Additional Table 3, respectively.
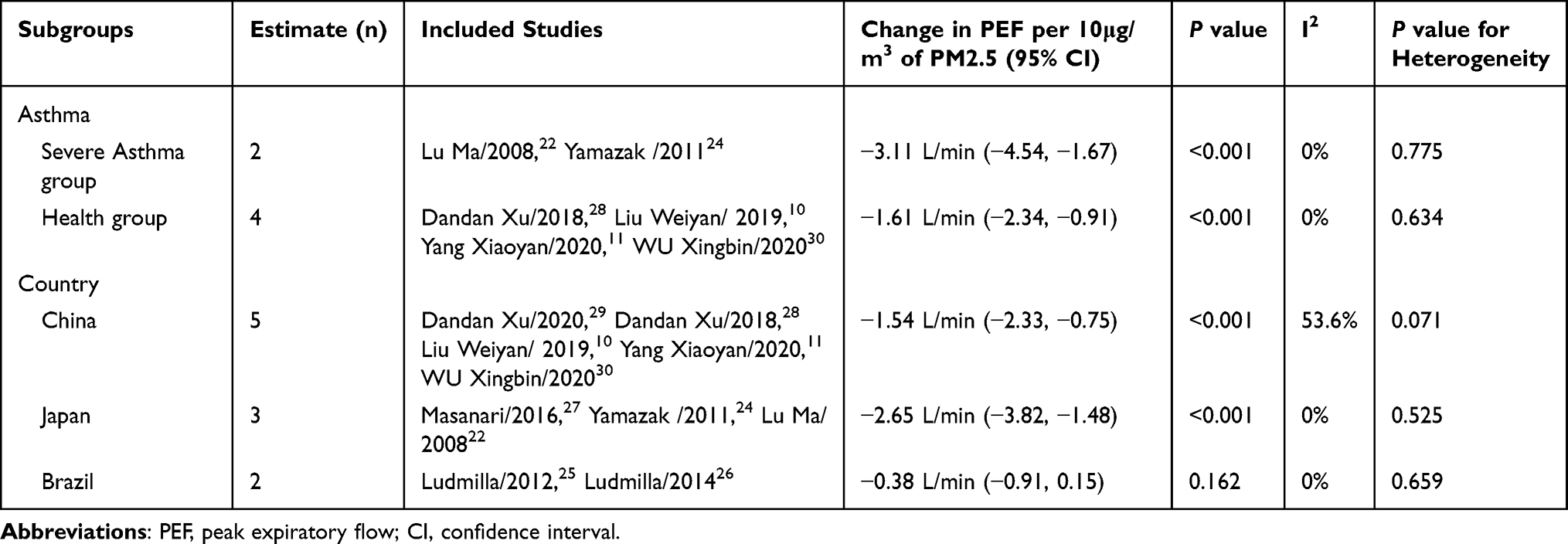 |
Table 2 Subgroup Analysis by Asthma and Country Examining the Relationship Between PM2.5 and PEF in Children |
Sensitivity Analysis
Sensitivity analysis was performed by excluding one study at a time to assess the stability of the results of PEF. The decreases in PEF remained significant after excluding the articles one by one. When we removed the article of Ludmilla25 or Dandan Xu,25 the heterogeneity was reduced to 60.22% and 55.60%, respectively, indicating that the two studies were the source of heterogeneity. Ludmilla’s research was conducted in Brazil and Dandan Xu’s research had a large sample size (848), which might contribute to the heterogeneity.
Discussion
This study is, to our knowledge, the first meta-analysis assessing the effects of acute exposure to outdoor PM2.5 on lung function in children. We found that an increase in PM2.5 level was significantly associated with a decrease in PEF (−1.74L/min per 10μg/m3 increase in PM2.5). Elevated PM2.5 exposure was also associated slight alteration of FVC and FEV1 but without significant difference.
The effect of acute PM2.5 exposure on PEF was more significant in children with severe asthma, suggesting that asthmatic children are more vulnerable to PM2.5 exposure than healthy ones. Zhang et al31 showed that PM2.5 exposure induced higher variation in Nitric Oxide Synthase 2 (NOS2) in children with asthma, which contributed to a greater alteration of lung function. In addition, patients with severe asthma produced more cytokines than healthy ones when exposed to PM2.5.32 In contrast, Ludmilla’s research25 indicated that PM2.5 exposure had little effect on asthmatic children. However, it is also revealed that there was a significant reduction in PEF with a 10 ug/m3 increase of PM2.5 in non-asthmatic children. This discovery may result from the fact that the asthmatic subjects tend to take medication when they perceive the deteriorating air quality. Previous studies showed that anti-inflammatory medication in asthmatic children could significantly alleviate the effect of PM2.5 exposure on PEF.33 The impact of acute PM2.5 exposure was more obvious in studies involving children with severe asthma, suggesting that asthma status may amplify the effect of acute PM2.5 exposure on lung function.
PM2.5 exposure appeared to exert a profounder effect on children’s lung function than that of adults, indicating that children are more vulnerable to PM2.5 exposure than adults. One meta-analysis found a 10 μg/m3 increase of PM2.5 was associated with a 1.02L/min decrease of PEF in non-smoking asthmatic adults, while no decrease of PEF was found in smokers.4 Ge Mu showed a 10 μg/m3 increase of PM2.5 was associated with a 0.972 L/min decrease of PEF among 4697 urban adults.34 The change of PEF in our finding was more obvious than these previous studies. In addition, Jingchun Fan’s meta-analysis showed that the risk of asthma emergency department visits due to per 10 μg/m3 increase in PM2.5 was much higher in children than in adults.35 Sandra also revealed that younger children were more susceptible to air pollution.26 Compared with adults, children have undeveloped lungs, higher baseline respiratory rates, more time spending outdoors, more frequent mouth-breathing, and larger lung surface area per unit of body weight, all making them more vulnerable to PM2.5 exposure.36
The reduction of lung function can be attributed to the inflammatory response, oxidative stress, and bronchial epithelium cell apoptosis caused by PM2.5. Pro-inflammatory response induced by airborne PM can weaken pulmonary function in schoolchildren.27 An in vivo study suggested that a variety type of cells might cause inflammation response through different pathways when exposed to PM2.5: Macrophages released proinflammatory mediators via the LPS/MyD88 pathway, while type II alveolar cells mainly caused oxidative stress-dependent inflammation.37 Decreased lung function was related to not only proinflammatory mediators but also microRNAs. After PM2.5-inhalation, Balb/c mice showed decreased MiR-146a and miR-146b, and dramatically increased IL-6, INF-γ and TNF-α; miR-146a level was found negatively related to PEF.38 Persistent endoplasmic reticulum stress caused by oxidative stress contributes to the lung damage induced by PM2.5 exposure.39 An in vitro study demonstrated that PM2.5 could not only cause inflammatory responses and oxidative injury but also trigger the autophagy‑mediated apoptosis of mice bronchial epithelium cells via PI3K/AKT/mTOR pathway.40
In the analysis stratified by geographical location, PM2.5 showed varied effects on PEF of children in different countries. The results indicated that PM2.5 exposure in different countries might have different physiologic consequences. Firstly, this phenomenon may result from different concentrations, compositions, and inflammatory chemotaxis of PM2.5 in these countries.9,41,42 The effect of air pollution may be less obvious in areas with low PM2.5 concentrations, so larger sample sizes are needed to illustrate the associations between PM2.5 exposure and lung function in different areas.9,41 The effects of PM2.5 exposure on lung function in children may depend more on the pro-inflammatory response to the PM composition than on the PM mass concentration.9,41 The different contents of allergens, polycyclic aromatic hydrocarbons, especially heavy metals in PM2.5 exposure can lead to various inflammatory responses.9,41,43 Secondly, population susceptibility, gene polymorphisms and dietary habits may also contribute to different effects of PM2.5 exposure among countries. A cohort study in China found that gene–environment interaction of Sirtuin 1 (SIRT1) was associated with mortality caused by PM2.5 exposure among the elder people.44 DNA repair gene XPC might play a role in the pathogenesis of respiratory diseases, and children with the CC alleles of XPC polymorphisms were found to be more susceptible to the adverse effects of ambient air pollution.45 People often eating antioxidant food such as fruits and vegetables may be less vulnerable to the adverse effects of PM.46 Lastly, the distinct climate, temperatures and humidity may also contribute to the varied effects of PM2.5 exposure in different countries.47
In the subgroup analysis, we found the alteration of PEF in children’s pulmonary function was not statistically significant in Brazil. However, the change of PEF of Chinese children was significant. This may be explained by the lower PM2.5 concentration in Brazil than in China. In our study, the PM2.5 concentration in China fluctuated between 50 and 90μg/m3, but between 19.6 and 24.34 μg/m3 in Brazil. The relatively higher PM2.5 concentration in China is responsible for the bigger change of PEF in children. In addition, in the non-severe asthmatic children of Brazil, inhaling drugs such as corticosteroids during air pollution deterioration made the effect on PEF slighter, according to the study. The results of meta-regression showed significant heterogeneity among the studies of Brazil. The non-statistically significant change of PEF in Brazilian children may contribute to the heterogeneity. This could also be partially explained by the small number of studies in Brazil. In contrast, the average PM2.5 concentration in Japan was lower than that in China, but the change of PEF in Japanese children was larger. This may be caused by the fact that two studies only focused on severe asthmatic children in Japan.
The results of sensitivity analysis revealed that Dandan Xu’s study,25 which had a large sample size (848), was one source of heterogeneity, but it did not change the statistical significance of the pooled result. The result of sensitivity analysis and meta-regression indicated that the different sample size of the studies spanning over 25 years could partly explain the heterogeneity. Another possible explanation for the heterogeneity was that the proportions of asthmatic children were different across studies excluding individuals with severe asthma and the children who could not be divided into asthmatic or healthy group due to incomplete information.
The alteration of FVC and FEV1 at PM2.5 exposure were slight in our study, showing no statistical significance. In contrast, Ge Mu found that each 10 μg/m3 increase in the previous-day personal PM2.5 exposure was associated with significant decreases in FVC and FEV1.34 Ralph J. Delfino48 also revealed that FEV1 decrements were significantly associated with the increasing personal PM2.5 exposure, but not the ambient PM2.5. We speculate that the personal PM2.5 exposure might exert more significant impacts than ambient PM2.5 exposure on FVC and FEV1. Our result may also be influenced by the smaller sample size in studies including FVC and FEV1 in children exposed to ambient PM2.5. Furthermore, the study of ESCAPE Project suggested16 that long-term exposure to PM2.5 might result in reduced FEV1 in schoolchildren, indicating that the different effects of long-term and short-term PM2.5 exposure on FEV1.
Our meta-analysis has some limitations. First, the number of studies in this meta-analysis was small. The results should therefore be interpreted with caution. Second, these studies were mainly on school-age children because the children of this age are more frequently exposed to PM2.5. It was impractical to perform subgroup analysis stratified by age due to the similar age of children in different studies. Therefore, studies on children of other age groups are needed in the future. In addition, sex, passive smoking, purifier, and sex may also influence the results of the different studies. Third, we assumed that there was a linear relationship between PM2.5 exposure and lung function. We did not know whether this linear relationship did exist between PM2.5 and lung function because of the lack of data. But this method was also used in other meta-analyses about relationship between air pollution and lung function.5,14 Fourth, although we tried to choose the effect of one pollution model of lag 0–1 or lag 1 in order to reduce the heterogeneity of the original studies, we could not exclude the effect of other air pollutants and different lag days in the original studies. Lastly, we discussed the effect of ambient PM2.5 exposure on children’s lung function, while the results may be different from those studies on personal PM2.5 exposure. The influence of co-morbidities, medications, and sex on the lung function of children cannot be ruled out, even though they were considered as concomitant variables in the original studies included in this meta-analysis. We could not conduct the subgroup analysis based on the above concomitant variables, because some of the studies did not analyze these variables. The results should be considered with caution. Hence, more researches are needed in future work.
Despite the limitations, our meta-analysis also has some strengths. First, as far as we know, it is the first meta-analysis about the association between acute PM2.5 exposure and lung function in children. Second, we attempted to reduce heterogeneity among studies by using a consistent lag time (one day) when possible and analyzing different subgroups by asthmatic status and countries. Third, we also demonstrated the different effects of PM2.5 exposure on lung function in children of three countries. Last, we strived to address the issue of confounding and performed subgroup analysis on studies with severe asthmatic and healthy children, which demonstrated more obvious effects of acute PM2.5 exposure on children with severe asthma.
Conclusion
In summary, our results demonstrated that acute PM2.5 exposure was associated with reduced PEF in children. Acute PM2.5 exposure may induce more obvious effects on children with severe asthma. The impacts of PM2.5 vary across different countries. Measures such as wearing masks should be taken to protect children from ambient PM2.5 exposure, especially for asthmatic ones. The government should propose effective plans to reduce the environmental pollution. Further researches are required to better quantify and compare the adverse effects caused by different concentration of PM2.5.
Abbreviations
CI, 95% confidence interval; PM2.5, particulate matter 2.5; PEF, peak expiratory flow; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s; PAHs, polycyclic aromatic hydrocarbons; COPD, chronic obstructive pulmonary disease; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta Analyses; NOS, Newcastle-Ottawa Scale; NOS2, Nitric Oxide Synthase 2; SIRT1, Sirtuin 1.
Data Sharing Statement
All data used in this meta-analysis are freely and publicly available from the cited papers used in the analysis; the full citations are in the reference list.
Ethics Approval and Consent to Participate
Not applicable here, as this is a systematic review and meta-analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare that there are no competing interests.
References
1. Yang M, Guo YM, Bloom MS, et al. Is PM1 similar to PM2.5? A new insight into the association of PM1 and PM2.5 with children’s lung function. Environ Int. 2020;145:106092. doi:10.1016/j.envint.2020.106092
2. Song Y, Huang B, He Q, et al. Dynamic assessment of PM(2.5) exposure and health risk using remote sensing and geo-spatial big data. Environ Pollut. 2019;253:288–296. doi:10.1016/j.envpol.2019.06.057
3. Feng S, Gao D, Liao F, et al. The health effects of ambient PM2.5 and potential mechanisms. Ecotoxicol Environ Saf. 2016;128:67–74. doi:10.1016/j.ecoenv.2016.01.030
4. Lin Y, Zou J, Yang W, et al. A review of recent advances in research on PM2.5 in China. Int J Environ Res Public Health. 2018;15(3):438. doi:10.3390/ijerph15030438
5. Edginton S, O’ Sullivan DE, King WD, et al. The effect of acute outdoor air pollution on peak expiratory flow in individuals with asthma: a systematic review and meta-analysis. Environ Res. 2021;192:110296. doi:10.1016/j.envres.2020.110296
6. Zhang S, Routledge MN. The contribution of PM2.5 to cardiovascular disease in China. Environ Sci Pollut Res Int. 2020;27(30):37502–37513. doi:10.1007/s11356-020-09996-3
7. Hamra GB, Guha N, Cohen A, et al. Outdoor particulate matter exposure and lung cancer: a systematic review and meta-analysis. Environ Health Perspect. 2014;122(9):906–911. doi:10.1289/ehp/1408092
8. Yan W, Wang X, Dong T, et al. The impact of prenatal exposure to PM2.5 on childhood asthma and wheezing: a meta-analysis of observational studies. Environ Sci Pollut Res Int. 2020;27(23):29280–29290. doi:10.1007/s11356-020-09014-6
9. Zheng X, Ding H, Jiang L, et al. Association between Air pollutants and asthma emergency room visits and hospital admissions in time series studies: a systematic review and meta-analysis. PLoS One. 2015;10(9):e138146. doi:10.1371/journal.pone.0138146
10. Weiyan L, Chun Y, Hui Y, et al. Short-term effects of air pollution on lung function of school-age children in Hangzhou. Chin J Prev Vet. 2019;53(6):614–618. doi:10.3760/cma.j.issn.0253-9624.2019.06.014
11. Yang XY, Wen B, Han F, et al. Acute effects of individual exposure to fine particulate matter on pulmonary function in schoolchildren. Biomed Environ Sci. 2020;33(9):647–659. doi:10.3967/bes2020.086
12. Turner S. Lung function tracking - does it wobble during adolescence? Am J Respir Crit Care Med. 2018;198:1470–1471. doi:10.1164/rccm.201807-1244ED
13. Belgrave D, Granell R, Turner SW, et al. Lung function trajectories from pre-school age to adulthood and their associations with early life factors: a retrospective analysis of three population-based birth cohort studies. Lancet Respir Med. 2018;6(7):526–534. doi:10.1016/S2213-2600(18)30099-7
14. Edginton S, O’Sullivan DE, King W, et al. Effect of outdoor particulate air pollution on FEV 1 in healthy adults: a systematic review and meta-analysis. Occup Environ Med. 2019;76(8):583–591. doi:10.1136/oemed-2018-105420
15. Qibin L, Yacan L, Minli J, et al. The impact of PM2.5 on lung function in adults with asthma. Int J Tuberc Lung Dis. 2020;24(6):570–576. doi:10.5588/ijtld.19.0394
16. Gehring U, Gruzieva O, Agius RM, et al. Air pollution exposure and lung function in children: the ESCAPE project. Environ Health Perspect. 2013;121(11–12):1357–1364. doi:10.1289/ehp.1306770
17. Ma Y, Yu Z, Jiao H, et al. Short-term effect of PM2.5 on pediatric asthma incidence in Shanghai, China. Environ Sci Pollut Res Int. 2019;26(27):27832–27841. doi:10.1007/s11356-019-05971-9
18. Huang W, Schinasi LH, Kenyon CC, et al. Effects of ambient air pollution on childhood asthma exacerbation in the Philadelphia metropolitan Region, 2011–2014. Environ Res. 2021;197:110955. doi:10.1016/j.envres.2021.110955
19. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339(jul21 1):b2535. doi:10.1136/bmj.b2535
20. Wells G. The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses: symposium on systematic reviews: beyond the basics; 2014.
21. Greenland S, Longnecker MP. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am J Epidemiol. 1992;135(11):1301–1309. doi:10.1093/oxfordjournals.aje.a116237
22. Ma L, Shima M, Yoda Y, et al. Effects of airborne particulate matter on respiratory morbidity in asthmatic children. J Epidemiol. 2008;18(3):97–110. doi:10.2188/jea.JE2007432
23. Chen BY, Chao HJ, Chan CC, et al. Effects of ambient particulate matter and fungal spores on lung function in schoolchildren. Pediatrics. 2011;127(3):e690–e698. doi:10.1542/peds.2010-1038
24. Yamazaki S, Shima M, Ando M, et al. Effect of hourly concentration of particulate matter on peak expiratory flow in hospitalized children: a panel study. Environ Health. 2011;10(1):15. doi:10.1186/1476-069X-10-15
25. Jacobson LS, Hacon SS, Castro HA, et al. Association between fine particulate matter and the peak expiratory flow of schoolchildren in the Brazilian subequatorial Amazon: a panel study. Environ Res. 2012;117:27–35. doi:10.1016/j.envres.2012.05.006
26. Jacobson LS, Hacon SS, de Castro HA, et al. Acute effects of particulate matter and black carbon from seasonal fires on peak expiratory flow of schoolchildren in the Brazilian Amazon. PLoS One. 2014;9(8):e104177. doi:10.1371/journal.pone.0104177
27. Watanabe M, Noma H, Kurai J, et al. A panel study of airborne particulate matter composition versus concentration: potential for inflammatory response and impaired pulmonary function in children. Allergol Int. 2017;66(1):52–58. doi:10.1016/j.alit.2016.04.014
28. Xu D, Zhang Y, Zhou L, et al. Acute effects of PM2.5 on lung function parameters in schoolchildren in Nanjing, China: a panel study. Environ Sci Pollut Res Int. 2018;25(15):14989–14995. doi:10.1007/s11356-018-1693-z
29. Xu D, Chen Y, Wu L, et al. Acute effects of ambient PM2.5 on lung function among schoolchildren. Sci Rep. 2020;10(1):4061. doi:10.1038/s41598-020-61003-4
30. Wu X. Acute effects of air pollution on lung function of schoolchildren during heating season in Jinan, China. Hygiene. 2020;10(04):382–387.
31. Zhang Y, Salam MT, Berhane K, et al. Genetic and epigenetic susceptibility of airway inflammation to PM2.5 in school children: new insights from quantile regression. Environ Health. 2017;16(1):88. doi:10.1186/s12940-017-0285-6
32. Jose C, Liana C, Ubiratan S. External environmental pollution as a risk factor for asthma. Clin Rev Allergy Immunol. 2021;12:1–8.
33. Trenga CA, Sullivan JH, Schildcrout JS, et al. Effect of particulate air pollution on lung function in adult and pediatric subjects in a Seattle panel study. Chest. 2006;129(6):1614–1622. doi:10.1378/chest.129.6.1614
34. Mu G, Zhou M, Wang B, et al. Personal PM2.5 exposure and lung function: potential mediating role of systematic inflammation and oxidative damage in urban adults from the general population. Sci Total Environ. 2021;755(Pt 1):142522. doi:10.1016/j.scitotenv.2020.142522
35. Fan J, Li S, Fan C, et al. The impact of PM2.5 on asthma emergency department visits: a systematic review and meta-analysis. Environ Sci Pollut Res Int. 2016;23(1):843–850. doi:10.1007/s11356-015-5321-x
36. Bateson TF, Schwartz J. Children’s response to air pollutants. J Toxicol Environ Health A. 2007;71(3):238–243. doi:10.1080/15287390701598234
37. He M, Ichinose T, Yoshida S, et al. PM2.5-induced lung inflammation in mice: differences of inflammatory response in macrophages and type II alveolar cells. J Appl Toxicol. 2017;37(10):1203–1218. doi:10.1002/jat.3482
38. Hou T, Chen Q, Ma Y. Elevated expression of miR-146 involved in regulating mice pulmonary dysfunction after exposure to PM2.5. J Toxicol Sci. 2021;46(10):437–443. doi:10.2131/jts.46.437
39. Ding H, Jiang M, Li D, et al. Effects of real-ambient PM2.5 exposure on lung damage modulated by Nrf2(-/). Front Pharmacol. 2021;12:662664. doi:10.3389/fphar.2021.662664
40. Han X, Zhuang Y. PM2.5 induces autophagy-mediated cell apoptosis via PI3K/AKT/mTOR signaling pathway in mice bronchial epithelium cells. Exp Ther Med. 2021;21(1):1. doi:10.3892/etm.2020.9433
41. Garcia E, Rice MB, Gold DR. Air pollution and lung function in children. J Allergy Clin Immunol. 2021;148(1):1–14. doi:10.1016/j.jaci.2021.05.006
42. Ding L, Zhu D, Peng D, et al. Air pollution and asthma attacks in children: a case-crossover analysis in the city of Chongqing, China. Environ Pollut. 2017;220(Pt A):348–353. doi:10.1016/j.envpol.2016.09.070
43. Zhang J, Feng L, Hou C, et al. How the constituents of fine particulate matter and ozone affect the lung function of children in Tianjin, China. Environ Geochem Health. 2020;42(10):3303–3316. doi:10.1007/s10653-020-00574-7
44. Yao Y, Liu L, Guo G, et al. Interaction of Sirtuin 1 (SIRT1) candidate longevity gene and particulate matter (PM2.5) on all-cause mortality: a longitudinal cohort study in China. Environ Health. 2021;20(1):25. doi:10.1186/s12940-021-00718-x
45. Ghosh R, Rossner P, Honkova K, et al. Air pollution and childhood bronchitis: interaction with xenobiotic, immune regulatory and DNA repair genes. Environ Int. 2016;87:94–100. doi:10.1016/j.envint.2015.10.002
46. Orellano P, Quaranta N, Reynoso J, et al. Effect of outdoor air pollution on asthma exacerbations in children and adults: systematic review and multilevel meta-analysis. PLoS One. 2017;12(3):e174050. doi:10.1371/journal.pone.0174050
47. Barnett AG, Williams GM, Schwartz J, et al. Air pollution and child respiratory health: a case-crossover study in Australia and New Zealand. Am J Respir Crit Care Med. 2005;171(11):1272–1278. doi:10.1164/rccm.200411-1586OC
48. Delfino RJ, Staimer N, Tjoa T, et al. Personal and ambient air pollution exposures and lung function decrements in children with asthma. Environ Health Perspect. 2008;116(4):550–558. doi:10.1289/ehp.10911
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Vitamin C Supplementation on Chronic Obstructive Pulmonary Disease (COPD): A Systematic Review and Meta-Analysis
Lei T, Lu T, Yu H, Su X, Zhang C, Zhu L, Yang K, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2201-2216
Published Date: 10 September 2022
The Effects of a Healthy Diet on Asthma and Wheezing in Children and Adolescents: A Systematic Review and Meta-Analysis
Zhang J, He M, Yu Q, Xiao F, Zhang Y, Liang C
Journal of Asthma and Allergy 2023, 16:1007-1024
Published Date: 25 September 2023
Impact of Lung Function on Asthma Exacerbation Rates in Children Treated with Dupilumab: The VOYAGE Study
Guilbert TW, Murphy KR, Hamelmann E, Ross KR, Gupta A, Fiocchi A, Xia C, Gall R, Ledanois O, Radwan A, Jacob-Nara JA, Rowe PJ, Deniz Y
Journal of Asthma and Allergy 2024, 17:81-87
Published Date: 8 February 2024
Association Between Lung Function of Children and Their Socioeconomic Conditions: A Systematic Review
Alzayed A
International Journal of General Medicine 2024, 17:2265-2278
Published Date: 18 May 2024
Real-World Effectiveness of Triple Extrafine Fixed-Dose Combination with Beclomethasone/Formoterol/Glycopyrronium on Symptoms and Lung Function in COPD: A Systematic Review and Meta-Analysis
Rogliani P, Manzetti GM, Cazzola M, Calzetta L
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1723-1736
Published Date: 27 May 2025