Back to Journals » Journal of Pain Research » Volume 18
Effect of Acupuncture on Functional Connectivity of the Limbic Network in Patients with Knee Osteoarthritis: A Resting State Functional Magnetic Resonance Imaging Study
Authors Wu N ![]() , Lou XS, Chang YN, Li JY, Zhang ZH, Hu JH, Fan Y
, Lou XS, Chang YN, Li JY, Zhang ZH, Hu JH, Fan Y ![]() , Feng XD
, Feng XD ![]() , Yin S
, Yin S ![]()
Received 15 February 2025
Accepted for publication 17 July 2025
Published 31 July 2025 Volume 2025:18 Pages 3765—3780
DOI https://doi.org/10.2147/JPR.S519308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Houman Danesh
Nan Wu,1,* Xia-Shuang Lou,1,* Yi-Niu Chang,2,* Jing-Yi Li,1 Zhen-Hua Zhang,3 Jia-Hui Hu,3 Yue Fan,3 Xiao-Dong Feng,1,3 Shuai Yin3
1School of Rehabilitation Medicine, Henan University of Chinese Medicine, Zhengzhou, Henan, 450046, People’s Republic of China; 2Zhengzhou Railway Vocational & Technical College, Zhengzhou, Henan, 451460, People’s Republic of China; 3Rehabilitation Center, The First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, Henan, 450000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao-Dong Feng, The First Affiliated Hospital of Henan University of Chinese Medicine, No. 19, Renmin Road, Zhengzhou, 450000, People’s Republic of China, Tel +8615303828605, Email [email protected] Shuai Yin, The First Affiliated Hospital of Henan University of Chinese Medicine, No. 19, Renmin Road, Zhengzhou, 450000, People’s Republic of China, Tel +8613458588608, Email [email protected]
Background: Knee osteoarthritis (KOA) is a prevalent degenerative joint disorder. Acupuncture therapy demonstrates significant efficacy in alleviating KOA symptoms. However, the central neuroimaging mechanisms underlying acupuncture’s therapeutic effects remain incompletely elucidated. This study investigated brain network differences between KOA patients and healthy controls and further examined the effects of acupuncture on aberrant functional connectivity (FC) within brain networks in KOA patients.
Patients and Methods: Blood Oxygenation Level Dependent functional Magnetic Resonance Imaging (BOLD-fMRI) combined with Independent Component Analysis (ICA) was employed to investigate resting-state functional connectivity differences between 45 KOA patients and 15 healthy subjects. KOA patients were then randomized to: acupuncture group, placebo acupuncture group, or waiting for treatment group. After the intervention, the BOLD-fMRI scan was performed again, the influence of different intervention methods on the brain functional connectivity of KOA patients was investigated by ICA, and the central mechanism of acupuncture treatment of KOA was studied.
Results: Baseline KOA patients showed significantly reduced FC in the limbic network versus healthy subjects, specifically in the right temporal pole, right parahippocampal gyrus, right hippocampus, bilateral anterior cingulate gyrus, right amygdala, right orbital part of the inferior frontal gyrus, bilateral medial and paracingulate gyrus. Clinically, the acupuncture group showed significantly greater improvement in pain and mobility than both the placebo acupuncture group and waiting for treatment group (p < 0.05). Neuroimaging revealed that only the acupuncture group demonstrated significantly increased FC post-intervention in key limbic regions, including the anterior cingulate gyrus, lenticular putamen, amygdala, temporal pole, hippocampus, pallidum, parahippocampal gyrus and caudate nucleus.
Conclusion: Reduced limbic network functional connectivity is a central pathological feature in knee osteoarthritis. Acupuncture’s therapeutic efficacy is mediated primarily by focal neuromodulation restoring these aberrant limbic connectivity patterns. In contrast, placebo acupuncture exerts its placebo effects primarily through engagement of the reward circuitry.
Keywords: acupuncture, functional magnetic resonance imaging, independent component analysis, limbic system, osteoarthritis, knee
Graphical Abstract:

Introduction
Knee osteoarthritis (KOA) is a common degenerative disease of the knee that has become the fourth leading cause of disability worldwide, affecting more than 250 million people.1,2 The pathogenesis involves distinct etiological pathways: primary KOA typically arises from age-related cartilage degeneration and genetic susceptibility, whereas secondary KOA commonly initiates from traumatic knee injuries that induce acute inflammatory responses and subsequently accelerate joint degeneration.3,4 In recent years, the incidence of KOA has increased significantly, KOA accounts for more than 80% of global osteoarthritis, and the incidence of symptomatic KOA is 8.1%.5,6 Chronic pain is the main clinical manifestation of KOA, and acupuncture is considered to be a safer, more effective and cost-effective treatment. Acupuncture treatment for KOA has a long history of use. Compared to traditional oral Non-steroidal anti-inflammatory drugs (NSAIDs), acupuncture treatment for osteoarthritis offers the advantages of lower risk and lower cost.7 While surgical treatment demonstrates superior efficacy for end-stage KOA,8 the associated risks such as incision infection and deep vein thrombosis make it less suitable for the early stages of KOA.9 Modern clinical medical research confirms that acupuncture for KOA chronic pain significantly improves pain symptoms, knee joint motor function, and quality of life.10,11 The pathogenesis of KOA remains largely unclear. However, recent years have seen researchers increasingly recognize that abnormal functioning of the central nervous system plays a significant role in the complex clinical symptoms associated with KOA,12,13 and that the regulation of the central nervous system is also an important central pathway for the analgesic effects of acupuncture.14,15 We therefore posit that acupuncture alleviates KOA chronic pain through targeted modulation of brain functional activity. Examining central nervous system (CNS) dynamics in KOA patients will help elucidate the pathogenesis of this disease and reveal central mechanisms underlying acupuncture efficacy. Blood oxygen-dependent functional magnetic resonance imaging (BOLD-fMRI)16 is a non-invasive brain functional imaging technology that can provide functional activity information of the whole brain. Its advantages include high sensitivity, good repeatability, and no radiation harm, and it has been widely used in the study of chronic pain mechanism.17,18 Independent component analysis (ICA)19 is a data-driven blind source analysis method, which can effectively avoid the influence of prior assumptions on experimental results. By identifying resting brain networks and noise components, the observed data were decomposed into independent functional networks, and the connectivity state of brain networks related to diseases was directly reflected. At present, it has been widely used in studies on functional connectivity of resting brain networks.20,21 This study takes patients with KOA as the primary research subjects, conducts acupuncture intervention on them, and compares with placebo acupuncture group and waiting group, using BOLD-fMRI and independent component analysis (ICA), aiming to explore the central neural modulatory mechanisms of acupuncture treatment for KOA.
Materials and Methods
Participants
The study was conducted from September 2020 to January 2022 at the Rehabilitation Center of the First Affiliated Hospital of Henan University of Chinese Medicine in China. The diagnostic criteria for KOA in this study are formulated with reference to the guidelines for bone and joint Diagnosis and Treatment of the Chinese Medical Association22 and the diagnostic criteria for KOA of the American College of Rheumatology (ACR).23 KOA cases were defined by ICD-10 codes M17.0, M17.1, M17.4, M17.5, and M17.9.
Inclusion criteria of KOA patients: 1) Age 45–75 years old; 2) Meet the diagnostic criteria of knee osteoarthritis, right-handed; 3) Kellgren-Lawrence knee osteoarthritis radiological diagnostic grading standard grade I–III; 4) Good compliance. To receive treatment voluntarily and obtain the informed consent of the patient himself or his family. (Patients can be included if they meet all of the above 4 criteria).
Exclusion criteria: 1) Combined with other knee joint diseases, such as tuberculosis, tumor, rheumatism; 2) Combined with knee joint contusion or other trauma; 3) Serious cardiovascular disease, liver and kidney function damage, immune deficiency; 4) Have severe drug and alcohol dependence, mania or schizophrenia; 5) With obvious headache, dysmenorrhea and other chronic pain diseases, head trauma history; 6) History of hyaluronic acid or corticosteroid injection within 3 months; 7) Received acupuncture, massage and other treatments within 8 weeks; 8) MRI contraindications, such as claustrophobia. (Any of the above is excluded).
KOA diagnoses were confirmed by attending physicians (holding qualifications at or above the level of attending physician in China’s medical certification system) who received study-specific training from our research team.
Inclusion criteria of healthy subjects: 1) right-handed; 2) Age 45–75 years old; 3) Good physical condition, after the relevant hospital examination proved that the indicators are normal, no symptoms of KOA; 4) Signed informed consent without participating in other clinical projects.(Healthy subjects can be included if they meet all of the above 4 criteria).
Exclusion criteria: 1) Pregnant or lactating women; 2) People with symptoms of depression or anxiety, chronic pain disorders, or a history of head trauma; 3) Individuals with a chronic history of insomnia and indigestion; 4) Addiction problems, such as smoking, alcoholism; 5) MRI contraindications, such as claustrophobia. (Any of the above is excluded).
Experimental Design and Sample Size
The sample size calculations for neuroimaging studies differed from those of general randomized controlled trials (RCT). A review article reported that by searching the PubMed database for English-language articles published between 1995 and 2014 that used neuroimaging techniques to conduct scans on humans, 168 articles were included. The mean sample size of these studies was 15 cases.24 Additionally, prior fMRI studies demonstrate that 12 to 15 patients per group provide sufficient statistical power.25,26 Consequently, the study was designed with 15 participants allocated to each group. Patients with KOA will be divided into three intervention groups, resulting in a total of 45 KOA subjects and 15 healthy subjects.
The included KOA patients were randomly divided into acupuncture group, placebo acupuncture group and waiting treatment group according to the ratio of 1:1:1. The acupuncture group underwent 4 courses of acupuncture intervention, totaling 20 sessions, while the placebo acupuncture group also received 4 courses of acupuncture intervention, amounting to 20 sessions. The waiting treatment group did not receive any intervention within 4 weeks. Each KOA patient underwent a BOLD-fMRI scan at baseline before treatment and after 4 weeks of treatment. All subjects were evaluated before and after the treatment. To explore the effects of different intervention methods on the brain functional connectivity of KOA patients by ICA and to explore the central mechanism of acupuncture treatment of KOA by analyzing the correlation between the changes in brain regions with functional connectivity differences and the improvement of clinical observation indicators.
Masking and Intervention
Using a computer-generated table of random numbers and a light-tight, closed-letter method to hide the randomization sequence, the researchers divided the KOA subjects into acupuncture, placebo acupuncture, and waiting treatment groups in a 1:1:1 ratio. Participants in the random assignment did not participate in recruitment, and the grouping was managed by the leader of the research group. Doctors, evaluators, and subjects were blinded to the grouping status. A single treatment room was used for blind evaluation, and efficacy was evaluated by a third party. In the data analysis stage, the principle of separation between the researcher, clinical operator, and statistician was implemented. All statistical analyses were performed by statisticians who remained blinded to group allocation and treatment assignments. Acupoint selection scheme of acupuncture group (as shown in Figure 1): Dubi (ST35), Neixiyan (EX-LE4), Yanglingquan (GB34), Yinlingquan (SP9) and two ashi acupoints (the point where the patient feels most pain) of knee joint. Specific positioning refers to the positioning standard of the People’s Republic of China national GB/T123446-2006 “Name and Location of acupointscin 2006. Acupuncture methods: 1) The patient was asked to lie flat and maintain a comfortable position, and then the skin was disinfected with complexed iodine, and the acupoint was vertically pierced with 21~26mm; 2) After acupuncture and moxibustion acupuncture into the acupoint to flat-supplement and flat-purgation techniques to “deqi”; 3) Keep the needle for 30 minutes, and repeat the needle every 10 minutes.In the placebo acupuncture group, the stimulation points were located at dubi (ST35), Neixiyan (EX-LE4), Yanglingquan (GB34), Yinlingquan (SP9) and two ashi points 1 cm away from the lateral median line of lower limbs. To minimize the effect of comfort acupuncture, acupuncturists are required to use a sterile needle (Global brand, Suzhou, China, 0.30 mm in diameter, 20 mm length) to leave the needle for 30 min without further injection or manual operation after skin puncture. The waiting treatment group received no intervention and only received 20 free acupuncture treatments after the trial to thank the patients for their cooperation.
 |
Figure 1 Acupoints location. |
Clinical Assessment
All participants received standardized guideline-recommended conventional care, including: patient education on knee osteoarthritis management, lifestyle modification recommendations. This protocol does not recommend that the subjects receive other physical or medical interventions during the study. If the subject develops sudden severe knee pain, ibuprofen sustained-release capsules can be taken temporarily, and one capsule (300 mg) can be taken up to two times a day. (Fenbide, approval number: Sinopremedy H10900089, manufacturer: Sino American Tianjin Schix Pharmaceutical Co, LTD).
All patients were evaluated for clinical efficacy before and after treatment. Visual Analog Scale27 (VAS), The Western Ontario and McMaster Universities Osteoarthritis Index28 (WOMAC)and Knee Injury and Osteoarthritis Outcome Score29 (KOOS) evaluated the clinical symptoms of patients. Arthritis quality of life measurement scale simplified scale Arthritis quality of life measurement scale simplified scale30 (AIMS2-SF) was used to evaluate the quality of life of patients. Pain symptoms often affect patients’ mood changes, leading to anxiety and depression. To explore the relationship between emotional changes and functional status of limbic network connectivity in patients with knee osteoarthritis, the Beck Anxiety Inventory (BAI)31 and Beck Depression Inventory (BDI)32 assessed the emotional and psychological status of patients with KOA.
fMRI Data Acquisition
The nuclear magnetic data collection of all enrolled KOA patients and healthy subjects was carried out in the nuclear magnetic resonance room of the First Affiliated Hospital of Henan University of Chinese Medicine. High-resolution structural and functional images were scanned using Ingenia 3.0 Tesla Magnetic resonance scanner (Philips Medical System, Best, The Netherlands) and head orthogonal coils. Each KOA patient received a BOLD-fMRI scan at baseline before treatment and after 4 weeks of treatment.
The patient was placed in the supine position, and a 1270 anti-noise earplug was inserted to reduce the impact of noise. The head of each participant was fixed using a sponge cushion. The patient was instructed to relax the whole body during the scan, breathe evenly, keep quiet, do not shake, stay awake and try not to do any thinking. The scanning sequence included 3DT1 structure image and resting state BOLD-fMRI sequence. 3DT1 structure: Repetition Time (TR): 7.7ms, Echo Time (ET): 3.8ms, Field of View (FOV): 256 mm×256 mm, imaging Matrix: 256×256, Slice Thickness: 1 mm; The whole brain EPI sequence scan was used in the resting BOLD-fMRI. Scanning parameters: TR/TE2000/30ms, FOV, 240 mm×240 mm; scanning matrix, 64×64; Flip Angle (FA), 90°; layer thickness, 5 mm; and layer number, 50 layers.
Data Processing and Analyzing
Statistical Analysis
SPSS26.0 statistical software was used to analyze the data. The counting data were described by the number of cases (n), and the measurement data were expressed as the mean ± standard deviation (±s). All statistical tests were conducted using a bilateral test; the test level was α=0.05, and the difference was considered statistically significant when p<0.05. The main analysis contents were as follows: 1) Characteristics; 2) Clinical efficacy analysis. The total score and sub-dimension scores of clinical evaluation indicators before and after intervention in each group were compared to verify and evaluate the clinical efficacy of acupuncture in the treatment of KOA. 3) Inter-group efficacy analysis: The non-parametric Kruskal–Wallis rank sum test was used to compare the total score of clinical evaluation indicators and the difference in sub-dimension scores between the three groups before and after intervention, that is, the difference in scale scores between the three groups before and after intervention.
BOLD-fMRI Data Analysis
The processing and analysis of magnetic resonance imaging data were carried out using Matlab2018 (MathWorks, Inc. USA) platform. Using the Matlab2018 platform and the auxiliary tool software Resting-State fMRI Data Analysis Toolkit plus (RESTplus) based on the SPM12 software system, the magnetic resonance imaging data were pre-processed. The specific steps are as follows: 1) Format conversion: convert fMRI data files in original DICOM format into NIFTI format that can be recognized by software; 2) Eliminate the data of the first 10 time points; 3) Slice Timing; 4) Head motion correction: the data of subjects whose head motion range exceeds 3 mm and rotation angle exceeds 3° are excluded in this test; 5) spatial normalization, the corrected image is registered to the standard spatial template of the Montreal Neurological Institute (MNI) with the standard segmentation of 3mm×3mm×3mm; 6) Smooth, using 6 mm full width and half height Gaussian kernel function to smooth the data to enhance the normality of the data and facilitate statistical analysis.
Independent Component Analysis (ICA)
This study used GIFT software based on Matlab2018 platform (http://mialab.mrn.org/software/gift), independent component analysis (ICA), the horizontal space is independent component analysis (Group - ICA) to identify brain resting state networks. First, 36 independent components are estimated according to the minimum description length criterion, and the number of components is set. Then, through principal component analysis (PCA) dimensionality reduction, the ICASSO operation method was used to repeat the calculation 50 times to obtain the reconstructed independent components and their time series. After component identification using the YeoRSN template, ingredients with a high coincidence were selected by the naked eye. Finally, the 4D NIfTI files of each subject were converted into 3D NIfTI files using the SPM 12 software, and the same components were extracted for statistical analysis.
Correlation Analysis
The different brain regions between KOA patients and healthy subjects were selected as regions of interest (ROI), and the Extract ROI Signals function in RESTplus software was used to extract the corresponding ROI signal values of each subject before and after treatment. Calculate the difference between the signal values before and after processing. Pearson’s correlation analysis was conducted between the signal difference corresponding to the ROI and the difference between clinical evaluation indicators using SPSS 26.0. p<0.05 was considered to be correlated, and r value represented the degree of correlation. A scatter plot was constructed using GraphPad 8.0.
Results
Baseline Characteristics
A total of 72 KOA patients were enrolled in the trial, and 45 eligible KOA patients were eventually admitted. By December 2022, 15 healthy subjects had completed one BOLD-fMRI scan and 45 KOA patients (15 in the acupuncture group, 15 in the placebo acupuncture group, and 15 in the waiting group) had completed two BOLD-fMRI scans (at baseline and four weeks after the intervention), compliance was 100%, and no adverse events occurred, as illustrated in Figure 2. There were no statistical differences between KOA patients and healthy subjects in terms of age, sex, height, weight, body mass index, and other demographic characteristics (p >0.05), and the clinical data of the two groups were comparable, as shown in Table 1. There were no significant differences in the VAS scale, WOMAC total score and its subscales, KOOS total score and its subscales, AIMS2-SF scale, Beck Anxiety Inventory score, Beck Depression Inventory score, and demographic characteristics such as age, sex, height, weight, and body mass index among the three groups of KOA patients at baseline (p >0.05), which are comparable, as shown in Tables 2 and 3.
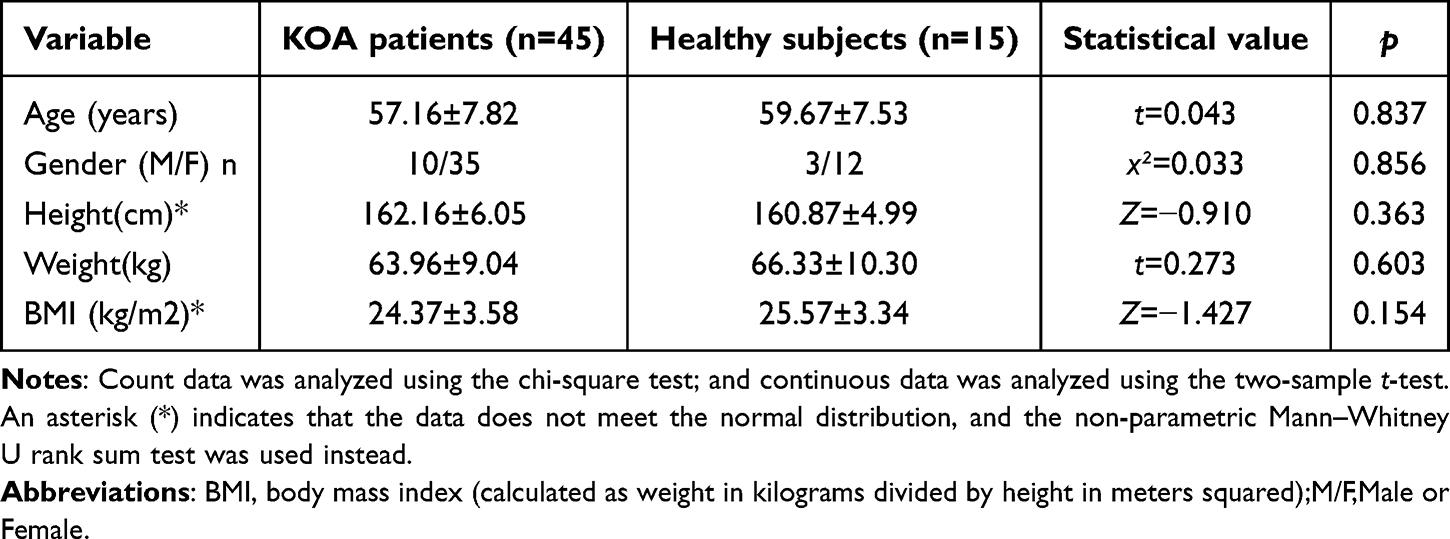 |
Table 1 Comparison of General Demographic Characteristics Between KOA Patients and Healthy Subjects ( |

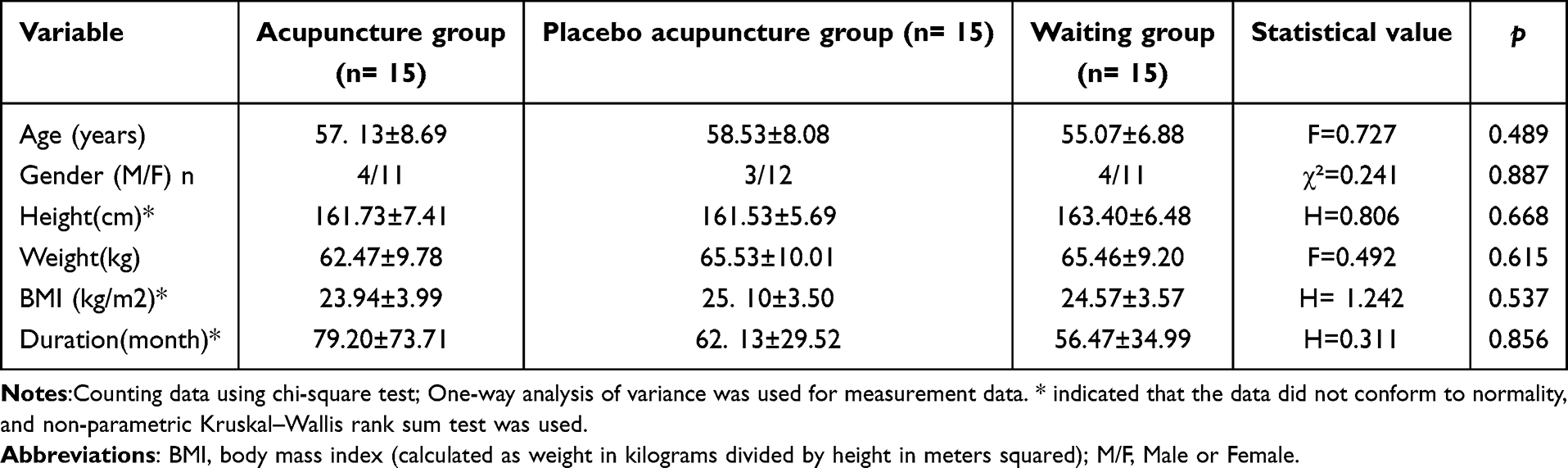 |
Table 2 Comparison of General Demographic Data of the Three Groups of Subjects ( |

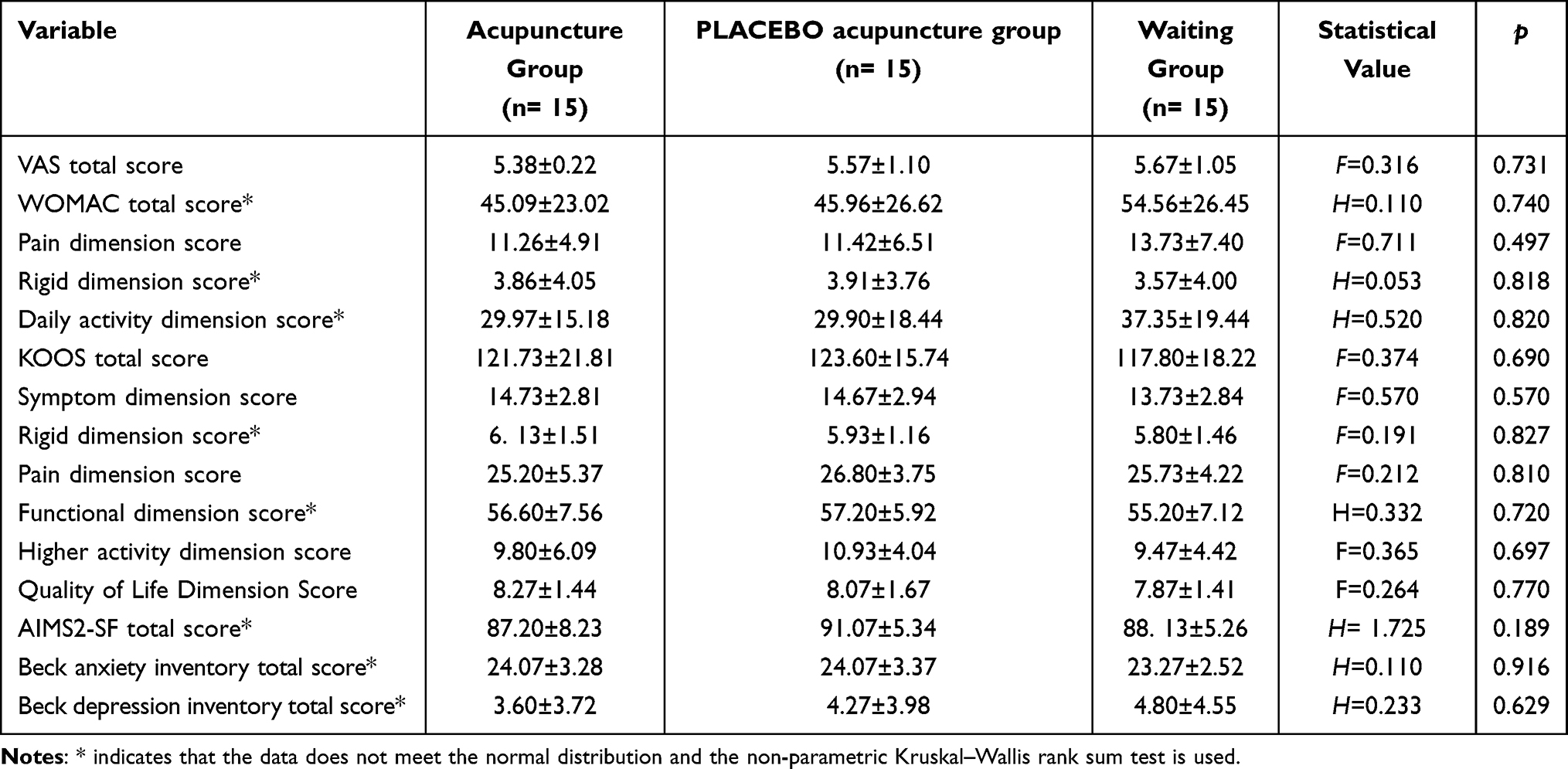 |
Table 3 Comparison of Clinical Evaluation Indicators in Three Groups of KOA Patients at Baseline ( |

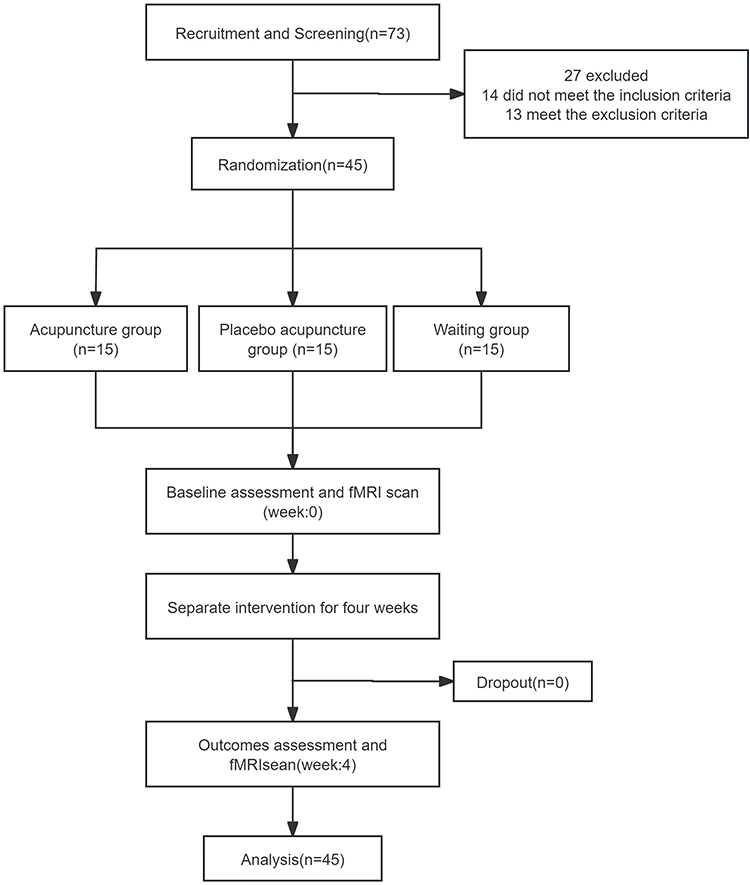 |
Figure 2 Flowchart of screening, enrollment, randomization, and treatment. |
Clinical Outcomes
The change in the clinical efficacy index score in the acupuncture group was much greater than that in the placebo acupuncture group and waiting treatment group, with statistical significance (p<0.05), while the improvement in Beck depression score in the acupuncture group, placebo acupuncture group, and waiting treatment group were not statistically different (p>0.05). See Table 4 for details.
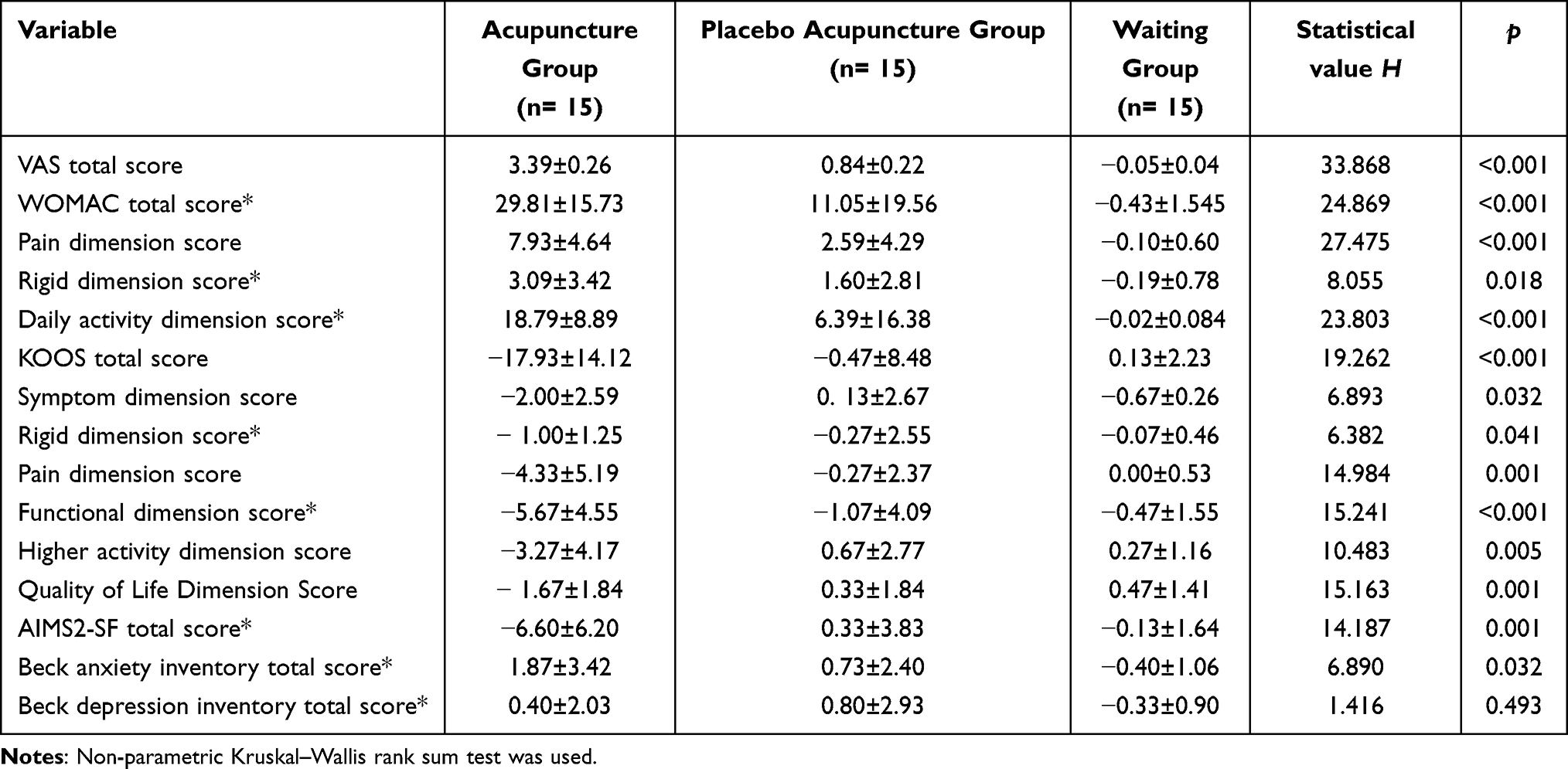 |
Table 4 Comparison of the Difference in Clinical Evaluation Indicators Between the Three Groups of KOA Patients Before and After Intervention ( |

ICA Analysis
Compared with healthy subjects, KOA patients showed decreased functional connectivity in the limbic network, including the right temporal pole, right parahippocampal gyrus, right hippocampus, bilateral anterior cingulate gyrus, right amygdala, right orbital part of the inferior frontal gyrus, and bilateral medial and paracingulate gyrus. See Table 5, Figure 3 for details.
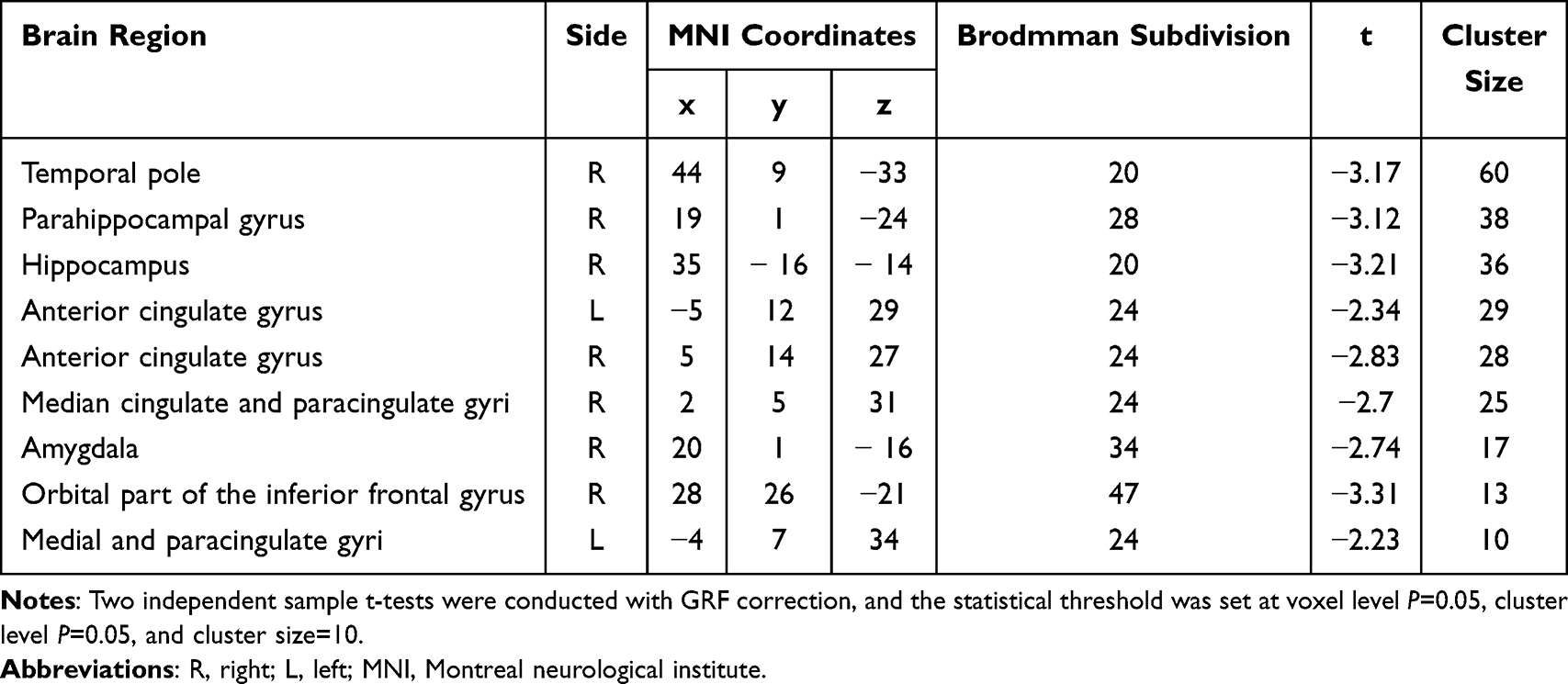 |
Table 5 Brain Regions Where the Network Functional Connectivity in KOA Patients Is Lower Than in Healthy Subjects |
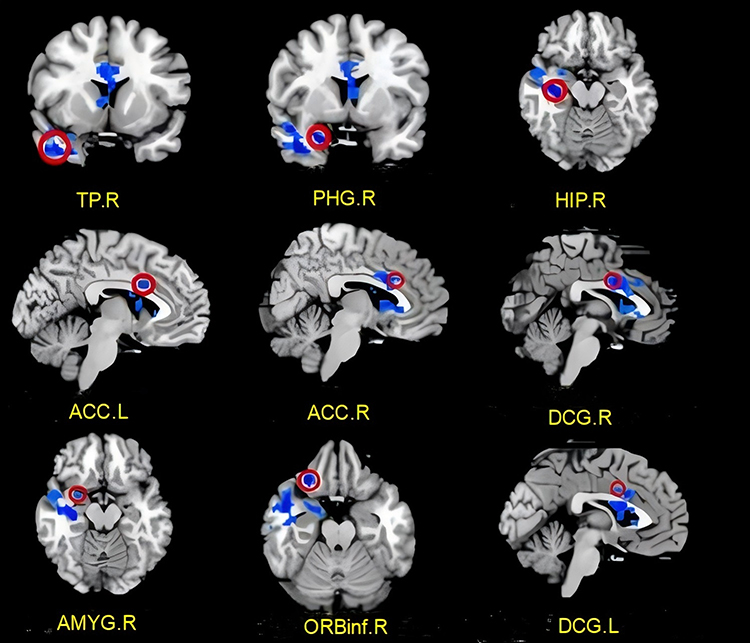 |
Figure 3 KOA patients had lower functional connectivity in the limbic network than healthy subjects. Abbreviations: TP, Temporal pole; PHG, Parahippocampal gyrus; HIP, Hippocampus; ACC, Anterior cingulate gyrus; DCG, Median cingulate and paracingulate gyri; AMYG, Amygdala; ORBinf, Inferior frontal gyrus, orbital part; R, right; L, left. |
Acupuncture group: After treatment, the functional connections of the limbic network in KOA patients increased in the following areas: bilateral anterior cingulate gyrus, right lenticular putamen, right amygdala, right temporal pole, right hippocampus, right pallidus, right parahippocampal gyrus, and right caudate nucleus. See Table 6, Figure 4 for details.
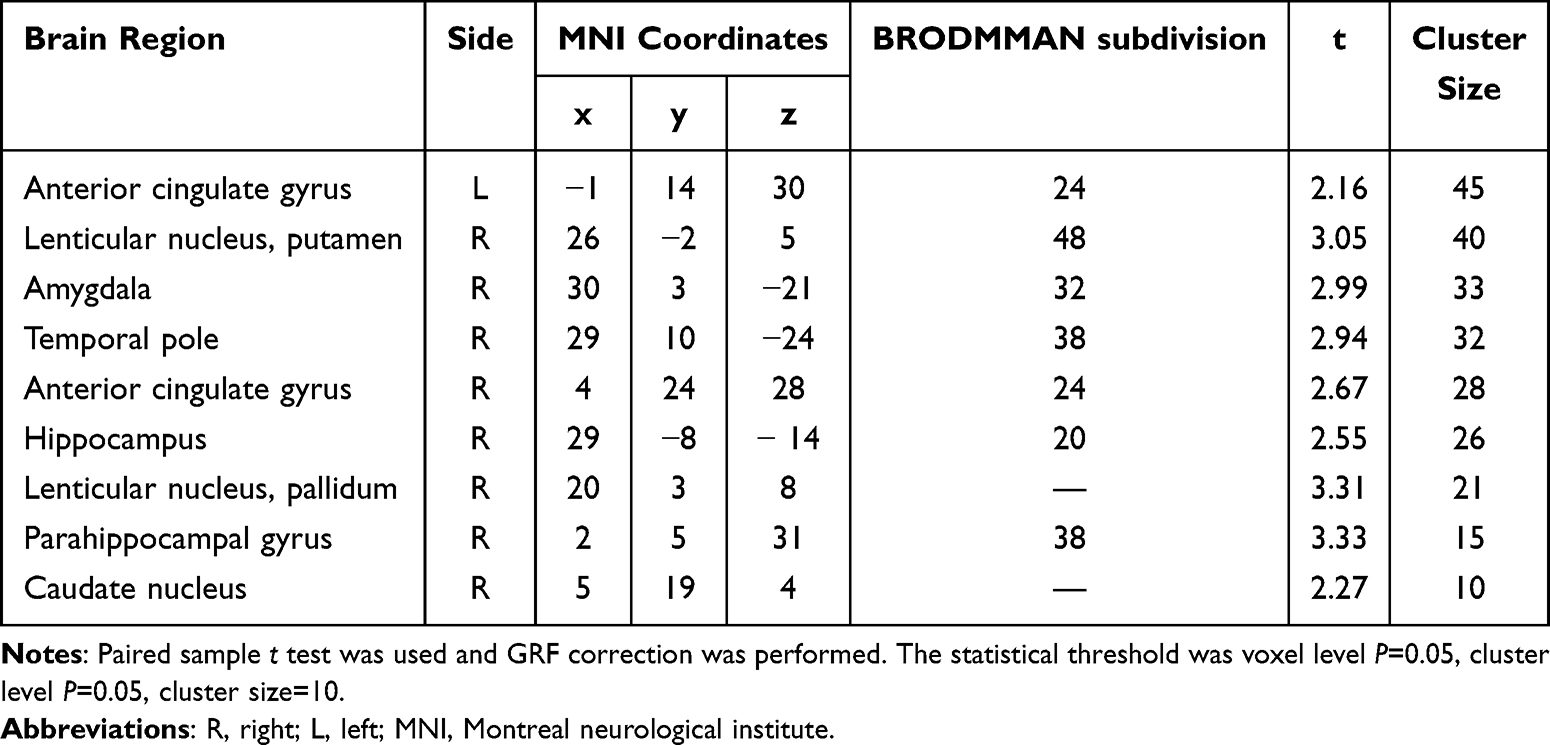 |
Table 6 Brain Regions with Elevated Limbic Network Functional Connections in Patients with KOA in the Acupuncture Group |
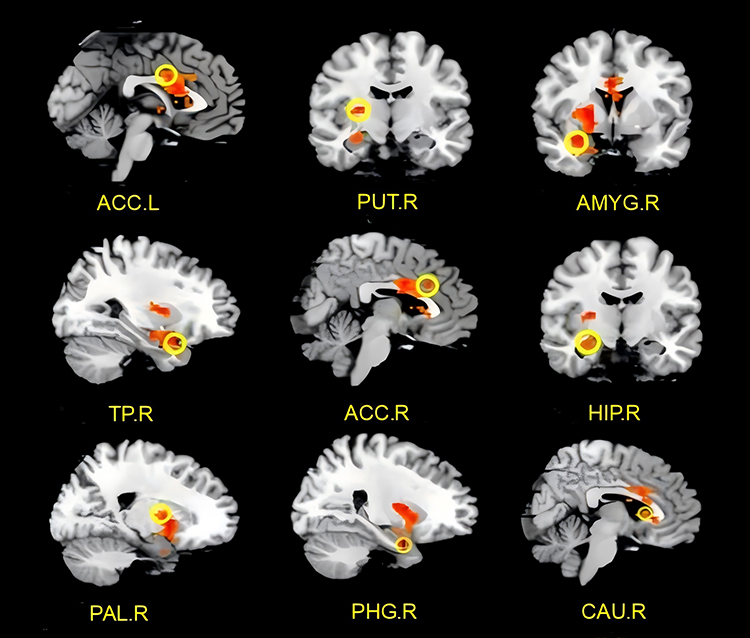 |
Figure 4 After acupuncture intervention, the functional connections of the limbic network in KOA patients increased. Abbreviations: ACC, Anterior cingulate gyrus; PUT, Lenticular nucleus, putamen; AMYG, Amygdala; TP, Temporal pole; HIP, Hippocampus; PAL, Lenticular nucleus, pallidum; PHG, arahippocampal gyrus; CAU, Caudate nucleus; R, right; L, left. |
Placebo acupuncture group: After intervention, the functional connections of the limbic network in KOA patients increased, and the functional connections increased in the regions of the right lenticular putamen and the right pallidus, and no regions with reduced functional connections were found. See Table 7, Figure 5 for details.
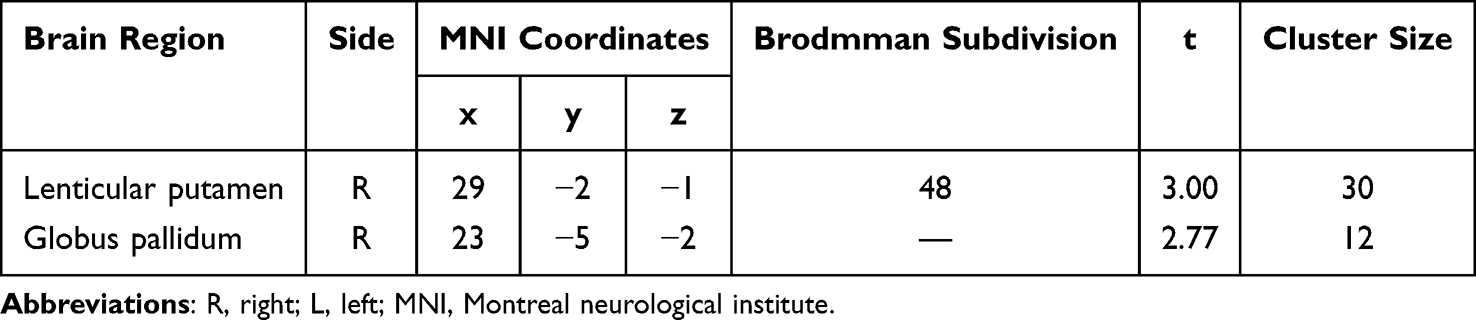 |
Table 7 Brain Regions with Elevated Functional Connectivity of the Resting Limbic Network in KOA Patients in the Placebo Acupuncture Group |
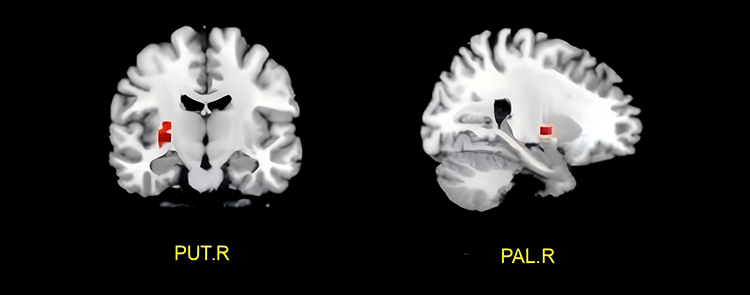 |
Figure 5 Functional connectivity of limbic network increased in KOA patients after placebo acupuncture intervention. Abbreviations: PUT, Lenticular nucleus, putamen; PAL, Lenticular nucleus, pallidum; R, right; L, left. |
Correlation Analysis
The correlation between the signal difference of the altered brain area before and after acupuncture intervention and the improvement in the clinical evaluation index and its sub-dimension score was analyzed. The results showed that there was a significant negative correlation between the left anterior cingulate gyrus and WOMAC stiffness dimension score, the right lenticular putamen and WOMAC pain dimension score, the right amygdala and KOOS and KOOS pain dimension scores, and the right temporal pole and KOOS symptom dimension score. The right anterior cingulate gyrus was negatively correlated with the WOMAC score, right hippocampus was negatively correlated with the KOOS pain dimension score, and right hippocampus was negatively correlated with the KOOS functional dimension score (p<0.05). See Table 8 and Figure 6 for details.
 |
Table 8 Correlation Between Functional Connection Changes of Edge Network and Clinical Evaluation Scale in KOA Patients Before and After Acupuncture |
 |
Figure 6 Correlation between functional connection changes and clinical evaluation indicators in patients with KOA after acupuncture. Abbreviations: TP, Temporal pole; PHG, Parahippocampal gyrus; HIP, Hippocampus; ACC, Anterior cingulate gyrus; AMYG, Amygdala; PUT, Lenticular nucleus, putamen; R, right; L, left. |
In the placebo acupuncture group, the signal difference in the brain areas with functional connection changes before and after intervention, including the right lenticulum putamina and the right pallidus, was correlated with the improvement in clinical evaluation indexes such as VAS, WOMAC, and KOOS. The results showed that there was a significant negative correlation between the right lenticular putamen and the total KOOS score and between the right pallidus and WOMAC pain score (p<0.05). Further details are provided in Table 9 and Figure 7.
 |
Table 9 Correlation Between Functional Connectivity Changes of Reward System and Clinical Evaluation Scale in KOA Patients After Placebo Acupuncture |
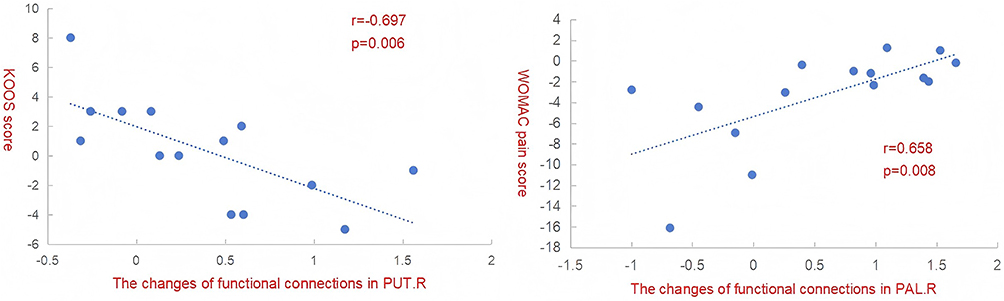 |
Figure 7 Correlation between functional connection changes and clinical evaluation indicators in KOA patients after placebo acupuncture. Abbreviations: PUT, Lenticular nucleus, putamen; PAL, Lenticular nucleus, pallidum; R, right; L, left. |
Discussion
In recent years, the incidence of KOA has increased significantly, and the related medical costs have also increased significantly, bringing a huge social and economic burden. At present, the treatment of KOA mainly includes drug therapy (Non-steroidal anti-inflammatory drugs,NSAIDs) and surgical treatment, but the use of NSAIDs is often accompanied by cardiovascular thrombotic events of different degrees and gastrointestinal and digestive complications and other side effects.7 While surgical treatment demonstrates excellent long-term outcomes for end-stage KOA,8 risks such as surgical site infection and deep vein thrombosis9 render it less ideal for early-stage KOA patients.These inevitable side effects and complications make the clinical treatment of KOA a great challenge. In recent years, many scholars have conducted a large number of randomized controlled trials, most of which show that acupuncture is safe and effective in treating KOA.33–37 Compared with traditional oral NSAIDs, acupuncture therapy for KOA also has the advantages of low risk and low cost.38 At present, it is believed that a variety of factors such as immune inflammatory response,5,39 joint injury40 and endocrine system disorder41 may cause KOA. However, the complex pathogenesis of KOA is not completely clear, and the simple peripheral mechanism of action cannot fully explain the scientific connotation of acupuncture treatment of KOA. Therefore, the purpose of this study was to investigate the central mechanism of acupuncture treatment of KOA. Limbic network is an important resting state functional network associated with chronic pain. Its important components include hippocampus, parahippocampal gyrus, entorhinal area, cingulate gyrus, orbitofrontal cortex, temporal pole, striatum, nucleus accumbens and amygdala.
Studies have shown that patients with chronic pain have functional abnormalities in several brain regions related to limbic network, including the prefrontal cortex, hippocampus, amygdala and nucleus accumbens, which are responsible for pain, reward, emotion, memory and other functions.42 In addition, the volume of gray matter in nucleus accumbens of trigeminal neuralgia patients was significantly lower than that of healthy controls.43 The degree of pain in patients with chronic low back pain is positively correlated with the functional connectivity between the amygdala and the executive control network.44 These studies suggest that chronic pain can disrupt the structure and function of the limbic network through constant nociceptive stimulation. In addition, chronic pain may also involve the reinforcement learning of negative emotions and the dysfunction of the reward system, and the limbic network responsible for emotional motivation, learning memory and reward function also plays a crucial role in this process.45 In this study, we investigated the differences in functional connectivity between 45 KOA patients and 15 healthy subjects at rest, and found that functional connectivity in the limbic network brain regions: right temporal pole, right parahippocampal gyrus, right hippocampus, bilateral anterior cingulate gyrus, right amygdala, right orbital part of the inferior frontal gyrus, bilateral medial and paracingulate gyrus was significantly reduced in KOA patients. In the limbic network of KOA chronic pain patients, the temporal pole46,47 and the parahippocampal gyrus48 can regulate pain, cognition, attention and emotion.The hippocampus is an important component of the limbic network involved in the encoding of pain and long-term memory of pain and pain-related emotions.42,49 The anterior cingulate gyrus50 is a key brain region for pain perception, emotion, and pain cognitive integration. The amygdala can regulate the perception and cognition of emotional disorders such as fear, anxiety and depression as well as pain.51 The orbitofrontal gyrus is involved in pain transmission and also regulates pain.52 Therefore, we believe that the abnormal functional connectivity of the limbic network is the central pathological change of KOA chronic pain.
Many studies have shown21,53,54 that functional networks are involved in the pathogenesis of chronic pain, and the regulation of functional networks is also an important way for acupuncture to exert analgesic effects. Therefore, we divided the KOA patients into three groups for the intervention. After acupuncture intervention, functional connections of the bilateral anterior cingulate gyrus, right lenticular putamen, right amygdala, right temporal pole, right hippocampus, right pallidus, right parahippocampal gyrus, and right caudate fringe network in KOA patients were significantly enhanced.
The lentiform putamen and pallidum constitute the lentiform nucleus, and together with the caudate nucleus constitute the striatum, which plays an important role in the brain’s reward, pleasure, addiction, fear, and placebo effect.55 Combined with the role of these brain regions in chronic pain, we speculated that acupuncture may be the key to the therapeutic effect of acupuncture on functional brain regions related to pain processing and emotional cognition in KOA patients with chronic pain, including the anterior cingulate gyrus, amygdala, temporal pole, hippocampus, and parahippocampal gyrus. Acupuncture may have a placebo effect in regulating brain regions related to reward mechanisms, such as the lenticular putamen and pallidum. Moreover, there was a high correlation between the functional connectivity of the limbic network and the improvement of clinical indicators, such as clinical symptoms, joint function, quality of life, and emotional cognition, in the acupuncture group. However, after the placebo acupuncture intervention in KOA patients, changes in limbic network functional connectivity occurred only in brain regions associated with reward, and these changes were only correlated with the subjective perception of pain and stiffness. Once again, acupuncture can regulate the functional connectivity of the limbic network of KOA patients through concentrated targeting and may improve patients’ clinical symptoms, joint function, quality of life, and emotional cognition. Placebo acupuncture can only change KOA patients’ subjective feelings of pain and stiffness through reward effects but cannot improve their joint function, quality of life, and emotional cognition.
Based on the results of this study, we hypothesized that acupuncture may regulate pain processing and emotional cognition in patients with chronic KOA pain through the anterior cingulate gyrus, amygdala, temporal pole, hippocampus, and parahippocampal gyrus; exert a therapeutic effect on KOA treatment; and exert a placebo effect on KOA treatment through the reward effect on the regulation of the lenticular putamen and pallidus.
This study focused on the resting state function network to explore the central etiology and pathogenesis of chronic pain in patients with KOA and to explore the central mechanisms of acupuncture treatment of KOA. In contrast to previous local analysis methods such as whole-brain low-frequency amplitude, local consistency, and whole brain voxel analysis, the independent component analysis adopted in this study focuses more on the observation of brain functional networks. Compared with functional connection analysis based on seed points, independent component analysis does not require prior assumptions and can make the research results more objective and scientific. The study design was different from the comfort acupuncture design used in the previous acupuncture treatment of KOA. In previous studies, researchers only selected non-meridian and non-acuesthesia as the control group, without considering the acupuncture dose and “deqi” effects, ignoring the placebo effect of acupuncture on the treatment of KOA. In the design of comfort acupuncture, in addition to considering the selection of stimulation points in the comfort acupuncture group, the operation of comfort acupuncture was optimized, which greatly reduced the therapeutic effect of acupuncture in the comfort acupuncture group.
However, the restricted number of eligible participants in this study imposes inherent limitations on the findings. Furthermore, the absence of multiple comparison correction may introduce bias into the results. As these findings represent a preliminary stage of discovery, further studies are required for validation.
Conclusion
Reduced functional connectivity across multiple regions of the limbic network represents a key central pathological feature in knee osteoarthritis (KOA). Focal neuromodulation targeting these aberrant limbic connectivity patterns likely constitutes a primary central mechanism of acupuncture efficacy. In contrast, placebo acupuncture exerts its placebo effects primarily through engagement of the reward circuitry. Owing to the modest cohort and exploratory status of this research, future validation through adequately powered studies with rigorous statistical designs is imperative.
Data Sharing Statement
The dataset generated in this study is not publicly available due to the subject’s right to informed consent. If there is a reasonable request, please contact the corresponding author.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of the First Affiliated Hospital of Henan University of Chinese Medicine (Ethics batch number: 2019HL-133-01), and registered at the Clinical Trial Registry (registration number: ChiCTR2000038554). The test strictly followed the guidelines of the Declaration of Helsinki. All participants recruited for this study received written informed consent.
Acknowledgments
The authors would like to express their heartfelt thanks to all those who participated in this study.
Author Contributions
All authors played an important role in the conception of the article, research design, data collection, analysis, interpretation, writing, revision, and critical review, thus ensuring the accuracy and reliability of the research results. Each author reviewed the final published manuscript and agreed to submit it to the Journal of Pain Research. Authors accept reviews and are responsible for all aspects of the research.
Funding
This study is supported by China Postdoctoral Science Foundation (2021M701122), Scientific Research Project of Henan Higher Education Institutions (22A360002, 23A360010), and the Science and Technology Department of Henan Province (222102310469, 232102311209 and 242301420110). Further details can be found in Supplementary Material 1–6.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hsu H, Siwiec RM. Knee Osteoarthritis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
2. A CUI, Li H, Wang D, et al. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 2020;29-30:100587. doi:10.1016/j.eclinm.2020.100587
3. Belluzzi E, Olivotto E, Toso G, et al. Conditioned media from human osteoarthritic synovium induces inflammation in a synoviocyte cell line. Connect Tissue Res. 2019;60(2):136–145. doi:10.1080/03008207.2018.1470167
4. Biz C, Maso G, Gambato M, et al. Challenging surgical treatment of displaced articular tibial plateau fractures: do early knee radiographic features have a predictive value of the mid-term clinical functional outcomes? Orthop Surg. 2019;11(6):1149–1162. doi:10.1111/os.12577
5. Xiao Y, Ding L, Yin S, et al. Relationship between the pyroptosis of fibroblast-like synoviocytes and HMGB1 secretion in knee osteoarthritis. Mol Med Rep. 2021;23(2):97. doi:10.3892/mmr.2020.11736
6. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
7. Zeng C, Doherty M, Persson MSM, et al. Comparative efficacy and safety of Acetaminophen, topical and oral non-steroidal anti-inflammatory drugs for knee osteoarthritis: evidence from a network meta-analysis of randomized controlled trials and real-world data. Osteoarthritis Cartilage. 2021;29(9):1242–1251. doi:10.1016/j.joca.2021.06.004
8. Siviero P, Marseglia A, Biz C, et al. Quality of life outcomes in patients undergoing knee replacement surgery: longitudinal findings from the QPro-Gin study. BMC Musculoskelet Disord. 2020;21(1):436. doi:10.1186/s12891-020-03456-2
9. Wang YZ. Dislocation in elderly patients after knee osteoarthritis replacement and its influencing factors. Chin J Gerontol. 2021;41(12):2543–2546.
10. Liu W, Fan Y, Wu Y, et al. Efficacy of acupuncture-related therapy in the treatment of knee osteoarthritis: a network meta-analysis of randomized controlled trials. J Pain Res. 2021;14:2209–2228. doi:10.2147/JPR.S315956
11. Li J, YX L, Luo LJ, et al. The effectiveness and safety of acupuncture for knee osteoarthritis: an overview of systematic reviews. Medicine. 2019;98(28):e16301. doi:10.1097/MD.0000000000016301
12. Cottam WJ, Iwabuchi SJ, Drabek MM, Reckziegel D, Auer DP. Altered connectivity of the right anterior insula drives the pain connectome changes in chronic knee osteoarthritis. Pain. 2018;159(5):929–938. doi:10.1097/j.pain.0000000000001209
13. Ushio K, Nakanishi K, Mikami Y, et al. Altered resting-state connectivity with pain-related expectation regions in female patients with severe knee osteoarthritis. J Pain Res. 2020;13:3227–3234. doi:10.2147/JPR.S268529
14. Liu L, Tian T, Li X, et al. Revealing the neural mechanism underlying the effects of acupuncture on migraine: a systematic review. Front Neurosci. 2021;15:674852. doi:10.3389/fnins.2021.674852
15. Chang CM, Yang CP, Yang CC, Shih PH, Wang SJ. Evidence of potential mechanisms of acupuncture from functional MRI data for migraine prophylaxis. Curr Pain Headache Rep. 2021;25(7:49. doi:10.1007/s11916-021-00961-4.
16. Yue Q, Wang L, Fang KW, et al. Neuroimaging advances in chronic pain: a focus on magnetic resonance. Imaging Chin J Pain Med. 2018;24(12):943–946. doi:10.3969/j.issn.1006-9852.2018.12.012
17. Yang YC, Zeng K, Wang W, et al. The changes of brain function after spinal manipulation therapy in patients with chronic low back pain: a rest bold fMRI study. Neuropsychiatr Dis Treat. 2022;18:187–199. doi:10.2147/NDT.S339762
18. Li Z, Zeng F, Yin T, et al. Acupuncture modulates the abnormal brainstem activity in migraine without aura patients. Neuroimage Clin. 2017;15:367–375. doi:10.1016/j.nicl.2017.05.013
19. Sariya YK, Anand RS. Comparison of separation performance of independent component analysis algorithms for fMRI data. J Integr Neurosci. 2017;16(2):157–175. doi:10.3233/JIN-170006
20. Zou Y, Tang W, Li X, Xu M, Li J. Acupuncture reversible effects on altered default mode network of chronic migraine accompanied with clinical symptom relief. Neural Plast. 2019;2019:5047463. doi:10.1155/2019/5047463
21. Chen X, Spaeth RB, Freeman SG, et al. The modulation effect of longitudinal acupuncture on resting state functional connectivity in knee osteoarthritis patients. Mol Pain. 2015;11:67. doi:10.1186/s12990-015-0071-9
22. Zhang Z, Huang C, Jiang Q, et al. Guidelines for the diagnosis and treatment of osteoarthritis in China (2019 edition). Ann Transl Med. 2020;8(19):1213. doi:10.21037/atm-20-4665
23. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American college of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2020;72(2):149–162. doi:10.1002/acr.24131
24. Qiu K, Jing M, Sun R, et al. The status of the quality control in acupuncture-neuroimaging studies. Evid Based Complement Alternat Med. 2016;2016(1):3685785. doi:10.1155/2016/3685785
25. Hayasaka S, Peiffer AM, Hugenschmidt CE, Laurienti PJ. Power and sample size calculation for neuroimaging studies by non-central random field theory. Neuroimage. 2007;37(3):721–730. doi:10.1016/j.neuroimage.2007.06.009
26. Desmond JE, Glover GH. Estimating sample size in functional MRI (fMRI) neuroimaging studies: statistical power analyses. J Neurosci Methods. 2002;118(2):115–128. doi:10.1016/s0165-0270(02)00121-8
27. Delgado DA, Lambert BS, Boutris N, et al. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. J Am Acad Orthop Surg Glob Res Rev. 2018;2(3):e088. doi:10.5435/JAAOSGlobal-D-17-00088
28. Symonds T, Hughes B, Liao S, Ang Q, Bellamy N. Validation of the Chinese Western Ontario and McMaster universities osteoarthritis index in patients from mainland china with osteoarthritis of the knee. Arthritis Care Res. 2015;67(11):1553–1560. doi:10.1002/acr.22631
29. Cheung RT, Ngai SP, Ho KK. Chinese adaptation and validation of the knee injury and osteoarthritis outcome score (KOOS) in patients with knee osteoarthritis. Rheumatol Int. 2016;36(10):1449–1454. doi:10.1007/s00296-016-3539-7
30. Zhu JL, Zhang YP, Pang LZ, Fu H. Tests of reliability and validity of short-form arthritis lmpact measurement scales 2 (AIMS2-SF). Chin J Prev Control Chronic Non-Communicable Diseases. 2006;(02):75–77.
31. Liang Y, Wang L, Zhu J. Factor structure and psychometric properties of Chinese version of beck anxiety inventory in Chinese doctors. J. Health Psychol. 2018;23(5):657–666. doi:10.1177/1359105316658971
32. Wang JY, Cao WJ, Guan ZY, Wu T, Wang RJ, Liu XD. Reliability validity, and application of the beck depression inventory (BDI) in. Med Students Chin J Health Statist. 2018;35(02):253–255.
33. Tu JF, Yang JW, Shi GX, et al. Efficacy of intensive acupuncture versus sham acupuncture in knee osteoarthritis: a randomized controlled trial. Arthritis Rheumatol. 2021;73(3):448–458. doi:10.1002/art.41584
34. Lin LL, Li YT, Tu JF, et al. Effectiveness and feasibility of acupuncture for knee osteoarthritis: a pilot randomized controlled trial. Clin Rehabil. 2018;32(12):1666–1675. doi:10.1177/0269215518790632
35. Tu JF, Wang LQ, Shi GX, et A. Effect of acupuncture on knee injury and osteoarthritis outcome score in patients with knee osteoarthritis. Chin Acupunc Moxibust. 2021;41(01):27–30. doi:10.13703/j.0255-2930.20191212-0001
36. Li WD. Randomized controlled observation of acupuncture treatment for knee osteoarthritis. Shanghai J Acupun Moxibust. 2014;33(10):937–940. doi:10.13460/j.issn.1005-0957.2014.10.0937
37. Zhu B. Randomized controlled trial of clinical effect of acupuncture combined with thunder fire moxibustion in the treatment of knee osteoarthritis [dissertation]. Beijing: Beijing University of Chinese Medicine; 2016.
38. Woods B, Manca A, Weatherly H, et al. Cost-effectiveness of adjunct non-pharmacological interventions for osteoarthritis of the knee. PLoS One. 2017;12(3):e0172749. doi:10.1371/journal.pone.0172749
39. Zhao D, Zhong W, Han D, Li Y, Jiang Y, Gu G. Elevated Frequencies of Total and MAIT Cell Subsets in Patients with Knee Osteoarthritis. PeerJ. 2019;7:e7443. doi:10.7717/peerj.7443
40. Poulsen E, Goncalves GH, Bricca A, Roos EM, Thorlund JB, Juhl CB. Knee osteoarthritis risk is increased 4-6 fold after knee injury - a systematic review and meta-analysis. Br. J Sports Med. 2019;53(23):1454–1463. doi:10.1136/bjsports-2018-100022
41. Xu RM, Chen MX, Lin YW, et A. Clinical efficacy of postmenopausal knee osteoarthritis with liver and kidney deficiencies based on theory of syndrome differentiation and treatment of kidney. Chin J Exp Traditional Med Formulae. 2020;26(13):150–155. doi:10.13422/j.cnki.syfjx.20200334
42. Lin YX, Wang RY, Cui Y, et al. The role of limbic system in chronic pain in osteoarthritis. Chinese J Rheumatol. 2021;25(08):555–558. doi:10.3760/cma.j.cn141217-20201112-00397
43. Tsai YH, Yuan R, Patel D, et al. Altered structure and functional connection in patients with classical trigeminal neuralgia. Hum Brain Mapp. 2018;39(2):609–621. doi:10.1002/hbm.23696
44. Jiang Y, Oathes D, Hush J, et al. Perturbed connectivity of the amygdala and its subregions with the central executive and default mode networks in chronic pain. Pain. 2016;157(9):1970–1978. doi:10.1097/j.pain.0000000000000606
45. Borsook D, Linnman C, Faria V, Strassman AM, Becerra L, Elman I. Reward deficiency and anti-reward in pain chronification. Neurosci Biobehav Rev. 2016;68:282–297. doi:10.1016/j.neubiorev.2016.05.033
46. Yao X, Yuan S, Yang W, et al. Emotional intelligence moderates the relationship between regional gray matter volume in the bilateral temporal pole and critical thinking disposition. Brain Imaging Behav. 2018;12(2):488–498. doi:10.1007/s11682-017-9701-3
47. Lee YC, Jahng GH, Ryu CW, Byun JY. Change in gray matter volume and cerebral blood flow in patients with burning mouth syndrome. J Oral Pathol Med. 2019;48(4):335–342. doi:10.1111/jop.12838
48. Zhang YN, Huo JW, Huang YR, Hao Y, Chen ZY. Altered amplitude of low-frequency fluctuation and regional cerebral blood flow in females with primary dysmenorrhea: a resting-state fMRI and arterial spin labeling study. J Pain Res. 2019;12:1243–1250. doi:10.2147/JPR.S177502
49. Tajerian M, Hung V, Nguyen H, et al. The hippocampal extracellular matrix regulates pain and memory after injury. Mol Psychiatry. 2018;23(12):2302–2313. doi:10.1038/s41380-018-0209-z
50. Bliss TV, Collingridge GL, Kaang BK, Zhuo M. Synaptic plasticity in the anterior cingulate cortex in acute and chronic pain. Nat Rev Neurosci. 2016;17(8):485–496. doi:10.1038/nrn.2016.68
51. Janak PH, Tye KM. From circuits to behaviour in the amygdala. Nature. 2015;517(7534):284–292. doi:10.1038/nature14188
52. Yoshino A, Okamoto Y, Okada G, et al. Changes in resting-state brain networks after cognitive-behavioral therapy for chronic pain. Psychol Med. 2018;48(7):1148–1156. doi:10.1017/S0033291717002598
53. Li K, Zhang Y, Ning Y, et al. The effects of acupuncture treatment on the right frontoparietal network in migraine without aura patients. J Headache Pain. 2015;16(1):518. doi:10.1186/s10194-015-0518-4
54. Zhang Y. The specified effects of acupuncture treatment on the Default Mode Network in migraine patients without aura: a resting-state functional magnetic resonance imaging study [dissertation]. Beijing: Beijing University of Chinese Medicine; 2014.
55. Li N, Jasanoff A. Local and global consequences of reward-evoked striatal dopamine release. Nature. 2020;580(7802):239–244. doi:10.1038/s41586-020-2158-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.