Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Dynamic Evolution Characteristics and Nursing Intervention Windows of Perioperative Deep Vein Thrombosis in Patients with Lower Extremity Traumatic Fractures: A Prospective Cohort Study
Authors Hu X, Wang Y, Li Y, Cao H, He M, Li Y ![]()
Received 23 January 2026
Accepted for publication 9 April 2026
Published 17 April 2026 Volume 2026:22 598379
DOI https://doi.org/10.2147/TCRM.S598379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Xuehua Hu,1,* Yunying Wang,2,* Yu Li,2 Hong Cao,1 Min He,1 Ying Li2
1Department of Perioperative Nursing, Xiangyang Central Hospital, Affiliated Hospital of Hubei University of Arts and Science, Xiangyang, 441106, People’s Republic of China; 2Department of Orthopedics Nursing, Xiangyang Central Hospital, Affiliated Hospital of Hubei University of Arts and Science, Xiangyang, 441106, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Li, Department of Orthopedics Nursing, Xiangyang Central Hospital, Affiliated Hospital of Hubei University of Arts and Science, No. 136 Jingzhou Street, Xiangyang, Hubei Province, 441106, People’s Republic of China, Email [email protected] Min He, Department of Perioperative Nursing, Xiangyang Central Hospital, Affiliated Hospital of Hubei University of Arts and Science, No. 136 Jingzhou Street, Xiangyang, Hubei Province, 441106, People’s Republic of China, Email [email protected]
Background and Purpose: Deep vein thrombosis (DVT) is a major complication after lower extremity traumatic fractures. Current nursing assessment is largely postoperative-centered and may overlook risk evolution during the preoperative waiting period.
Methods: In this prospective observational cohort study, 948 patients with lower extremity traumatic fractures were enrolled between January 2019 and January 2026. Serial color Doppler ultrasound examinations were performed at five timepoints: admission, preoperative, postoperative day 1, postoperative day 3, and discharge. Univariate and multivariate logistic regression analyses were used to identify predictors of preoperative DVT. A dynamic nomogram was developed and evaluated using receiver operating characteristic analysis, calibration, decision curve analysis, and SHAP-based interpretation.
Results: The overall incidence of perioperative DVT was 32.9% (312/948). DVT showed a distinct “twin-peak” temporal pattern, with the highest incidence during the preoperative waiting period and a second peak on postoperative day 3. Thrombi also shifted from predominantly distal veins at admission to greater proximal involvement after surgery. Independent predictors of preoperative DVT were age > 65 years, preoperative waiting time > 3 days, D-dimer > 1.85 mg/L, albumin < 35 g/L, and time from injury to admission > 12 h. The nomogram showed good discrimination (AUC 0.905, 95% CI 0.882– 0.928), outperforming individual predictors such as D-dimer (AUC 0.796). Decision curve analysis demonstrated clinical net benefit, and SHAP analysis identified D-dimer and albumin as the most influential variables.
Conclusion: Perioperative DVT after lower extremity fractures follows a dynamic pattern with a critical preoperative risk window. The proposed nomogram may support stage-specific nursing assessment and targeted interventions, particularly by reducing preoperative delay and optimizing nutritional status.
Keywords: deep vein thrombosis, lower extremity fracture, dynamic evolution, nomogram, nursing assessment, preoperative period
Introduction
Lower extremity traumatic fractures are a leading cause of hospitalization and disability worldwide, placing a substantial burden on healthcare systems. Among the potential complications, DVT remains one of the most insidious, with reported incidence rates ranging from 10% to 60% depending on the prophylaxis strategy and fracture type.1,2 Despite the widespread implementation of guidelines from the American College of Chest Physicians (ACCP), perioperative DVT continues to pose significant risks, including fatal PE and debilitating post-thrombotic syndrome (PTS).3,4 Unlike elective orthopedic surgeries, trauma patients present with a distinct “perfect storm” of Virchow’s triad: severe endothelial injury from the fracture, hemodynamic stasis due to immobilization, and a systemic hypercoagulable state triggered by the acute inflammatory response.5 While the association between trauma and thrombosis is well-established, managing this risk in the chaotic acute care setting remains a persistent challenge for nursing professionals.6,7 Current research and clinical attention have focused primarily on postoperative DVT, whereas the preoperative waiting period and preoperative DVT risk in lower extremity fracture patients remain relatively understudied.8,9 In many tertiary centers, trauma patients frequently experience a “preoperative waiting period” ranging from several days to over a week to manage soft tissue swelling or stabilize comorbid conditions.10–12
Recent studies suggest that this interval acts as a “second hit” to the coagulation system; however, the dynamic evolution of thrombosis during this specific window remains poorly mapped.13,14 Most existing literature relies on cross-sectional screenings at discharge, potentially missing early-onset thrombi. Consequently, the temporal distribution of DVT—specifically whether it follows a linear progression or a bimodal “twin-peak” pattern—and the topographical propagation of thrombi from distal to proximal veins remain unclear.15 Understanding these dynamics is essential for shifting nursing care from passive observation to stage-specific surveillance.16,17
Furthermore, current nursing assessments rely heavily on static risk assessment models (RAMs) such as the Caprini score. While effective in general surgery, these tools often fail to capture the rapid physiological fluctuations characteristic of trauma patients.18 For instance, dynamic biomarkers like D-dimer and serum Albumin—a marker of nutritional status and negative acute-phase reactant—have shown predictive value in retrospective studies but are rarely integrated into bedside nursing assessments.19 Low albumin levels, indicative of malnutrition and inflammation, have been independently associated with VTE risk, yet this modifiable factor is frequently overlooked. There is an urgent need for an objective, dynamic prediction tool that integrates demographic, logistical, and biological variables to stratify risk accurately.20
To address these gaps, this prospective cohort study was designed to delineate the dynamic characteristics of perioperative DVT. Unlike previous studies, we employed serial ultrasound screenings from admission to discharge to capture the full trajectory of thrombogenesis. The primary objectives were to: (1) map the temporal and topographical evolution of DVT; (2) identify stage-specific risk factors, focusing on the impact of preoperative waiting time; and (3) construct and validate a dynamic nomogram to guide nursing interventions. By evaluating the clinical net benefit of this model using DCA, this study aims to provide empirical evidence for establishing “Risk-Driven Nursing Intervention Windows,” ultimately improving patient safety through precision nursing.
Methods
Study Design and Setting
This prospective observational cohort study was conducted at the Department of Orthopedics, Xiangyang Central Hospital (a tertiary teaching hospital in Central China) between January 2019 and January 2026. The study protocol was designed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Xiangyang Central Hospital (Approval No. 2019–47-07). Written informed consent was obtained from all participants or their legal guardians upon admission. The reporting of this study follows the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Participants
We continuously recruited patients admitted for lower extremity traumatic fractures.
Inclusion criteria: (1) Age ≥ 18 years; (2) Diagnosis of closed fractures of the hip (femoral neck, intertrochanteric), femoral shaft, tibia/fibula, patella, or ankle confirmed by X-ray or CT imaging; (3) Scheduled for surgical intervention (internal fixation or arthroplasty).
Exclusion criteria: (1) Pathological fractures (e.g., due to tumor or metastasis); (2) History of previous DVT or PE; (3) Current use of anticoagulants or antiplatelet agents prior to injury; (4) Multiple trauma with Injury Severity Score (ISS) > 16 or requiring ICU admission; (5) Refusal to participate or inability to cooperate with the scheduled ultrasound follow-up (eg., severe cognitive impairment).
Data Collection
Data were collected by two trained research nurses using a standardized case report form (CRF).
- Demographic and Clinical Characteristics: Age, gender, Body Mass Index (BMI), smoking status, comorbidities (hypertension, diabetes, cardiovascular disease), and fracture location.
Logistical Factors: Time from injury to admission (hours) and Preoperative waiting time (days).
- Laboratory Biomarkers: Venous blood samples were drawn on admission (T1) under fasting conditions. Key indicators included D-dimer, Serum Albumin, Hemoglobin, and neutrophil-to-lymphocyte ratio (NLR).
- Risk Assessment: The Caprini Risk Assessment Model (RAM) score was calculated for each patient upon admission.
Perioperative Prophylaxis and Injury Severity Assessment
Additional perioperative management information, including duration of immobilization/bed rest and use of mechanical prophylaxis, was reviewed from the medical charts when available. Trauma severity was partially controlled at enrollment by excluding patients with multiple trauma, ISS >16, or ICU admission.
Dynamic DVT Screening Protocol
Unlike routine practice where screening is symptom-driven, this study employed a serial dynamic screening protocol. Bedside color Doppler ultrasound (CUS) was performed by a designated team of three senior sonographers (with >5 years of vascular experience) who were blinded to the patients’ biomarkers. Screenings were performed at five specific timepoints to capture the temporal evolution:
- T1 (Admission): Within 24 hours of hospitalization (Baseline).
- T2 (Preoperative): 1 day before the scheduled surgery.
- T3 (Postoperative Early): Postoperative day 1.
- T4 (Postoperative Peak): Postoperative day 3.
- T5 (Discharge): Prior to discharge or on postoperative day 7.
DVT Diagnosis Criteria: DVT was diagnosed based on the loss of compressibility of the vein, intraluminal filling defects, or absence of spontaneous flow using standard CUS criteria. Thrombosis was topographically classified as Proximal DVT (popliteal, femoral, or iliac veins) or Distal DVT (anterior/posterior tibial, peroneal, or muscular calf veins). The primary outcome of this study was serial ultrasound-defined perioperative DVT. Pulmonary embolism (PE) was not a prespecified endpoint and was not systematically assessed because routine confirmatory chest imaging was not performed in all patients.
Sample Size Consideration
The final cohort included 948 patients, among whom 312 developed perioperative DVT. Considering that the final multivariable preoperative model included five independent predictors, the available number of outcome events exceeded the conventional minimum requirement of 10 events per variable for regression-based model development. Therefore, the sample size was considered adequate for multivariable logistic regression and nomogram construction.
Statistical Analysis
Data analysis was performed using SPSS version 26.0 (IBM Corp, Armonk, NY) and R software version 4.1.2 (The R Foundation). Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data were expressed as mean ± standard deviation (SD) and compared using the Student’s t-test. Non-normally distributed data were expressed as median (interquartile range, IQR) and compared using the Mann–Whitney U-test. Categorical variables were presented as frequencies (percentages) and analyzed using the Chi-square test or Fisher’s exact test. Univariate logistic regression was first applied to screen for potential risk factors. Variables with p < 0.10 were entered into the multivariate logistic regression model (Forward Stepwise method) to identify independent predictors for preoperative and postoperative DVT. Results were reported as Odds Ratios (OR) with 95% Confidence Intervals (CI).
Based on the multivariate analysis results of the preoperative model, a prognostic nomogram was constructed using the rms package in R. Evaluated using the ROC curve and the Area Under the Curve (AUC). The AUCs of the combined model and individual predictors were compared using the DeLong test. Assessed using calibration plots with 1,000 bootstrap resamples to compare predicted vs. observed probabilities. The Brier score was calculated to quantify predictive accuracy. DCA was performed using the rmda package to quantify the net benefit of the nomogram at different threshold probabilities. Furthermore, to enhance model interpretability, SHAP (SHapley Additive exPlanations) values were calculated to quantify the global and local contribution of each feature to the prediction model. A two-tailed P-value < 0.05 was considered statistically significant.
Results
Baseline Demographic and Clinical Characteristics
During the study period, a total of 1,350 patients with lower extremity traumatic fractures were screened for eligibility. As illustrated in the study flowchart (Figure 1), 402 patients were excluded based on strictly defined criteria, including age <18 years, pathological fractures, prior history of thromboembolism, or refusal to participate. Ultimately, 948 patients were enrolled in the final analysis. The overall incidence of perioperative DVT was 32.9% (312/948). The baseline demographic and clinical characteristics of the DVT and Non-DVT groups are summarized in Table 1. Patients in the DVT group were significantly older (65.2 ± 10.8 vs. 54.1 ± 11.6 years, p<0.001) and exhibited a higher Body Mass Index (BMI) compared to the Non-DVT group (p<0.001).
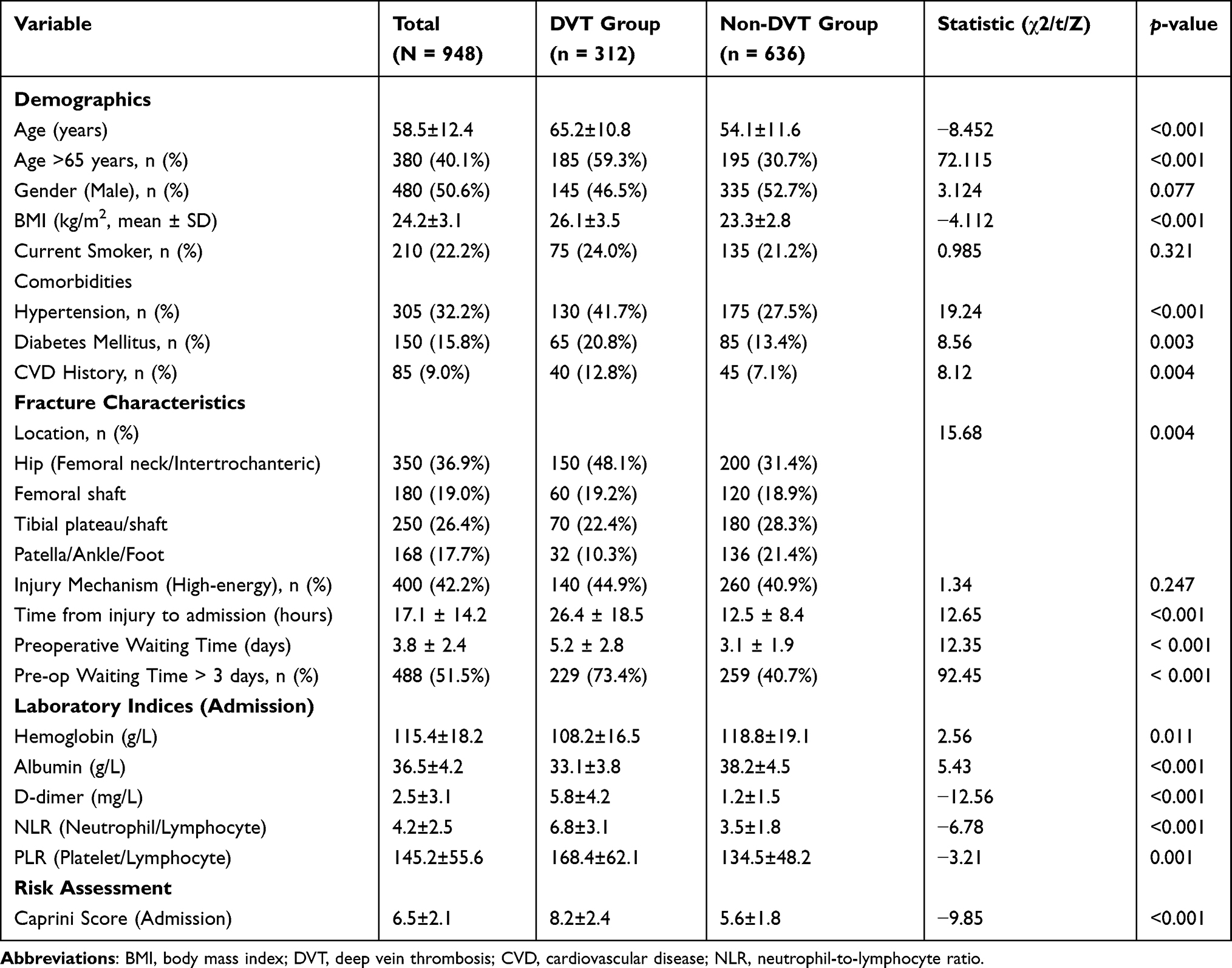 |
Table 1 Comparison of Baseline Demographic and Clinical Characteristics Between Patients with and Without Perioperative DVT |
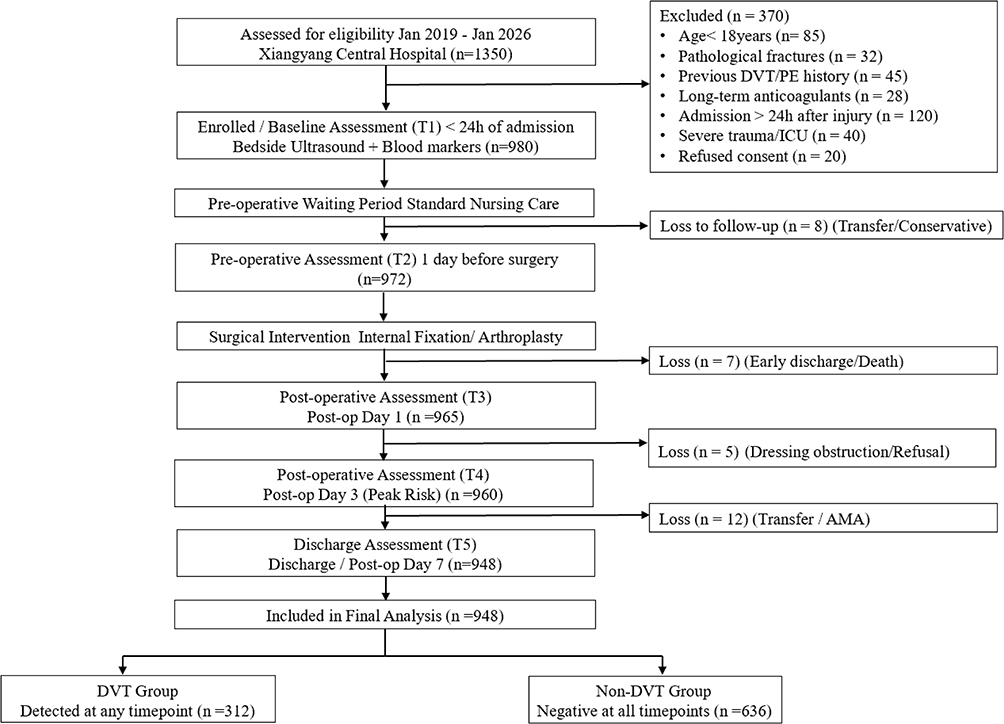 |
Figure 1 Flowchart of study participants. |
Logistical and physiological admission parameters differed significantly between the two groups. The DVT group experienced a significantly longer delay from injury to admission (26.4 ± 18.5 vs. 12.5 ± 8.4 hours, p < 0.001). Furthermore, the preoperative waiting time was significantly prolonged in the DVT group compared to the Non-DVT group (5.2 ± 2.8 vs. 3.1 ± 1.9 days, p < 0.001). Laboratory findings on admission revealed a distinct hypercoagulable and inflammatory state in the DVT group, characterized by significantly elevated D-dimer levels (5.8 ± 4.2 vs. 1.2 ± 1.5 mg/L, P<0.001) and a higher Neutrophil-to-Lymphocyte Ratio (NLR) (p<0.001). Conversely, serum albumin levels were markedly lower in the DVT group (33.1 ± 3.8 vs. 38.2 ± 4.5 g/L, p<0.001) (Table 1).
Dynamic Temporal and Topographical Evolution of Perioperative DVT
Serial ultrasound screening showed a dynamic temporal pattern of perioperative DVT. The incidence of DVT did not follow a linear progression but exhibited a distinct “twin-peak” distribution. The first and highest peak occurred during the preoperative waiting period (T2). After a transient decline at T3, a second peak was observed on postoperative day 3 (T4). In terms of topographical evolution, the anatomical distribution of thrombi changed during the perioperative course. At admission (T1), most thrombi were located in the distal deep veins, particularly the muscular calf veins. As hospitalization progressed, a progressive proximal shift was observed. By T4, the proportion of proximal DVT involving the popliteal and femoral veins had increased (Figure 2).
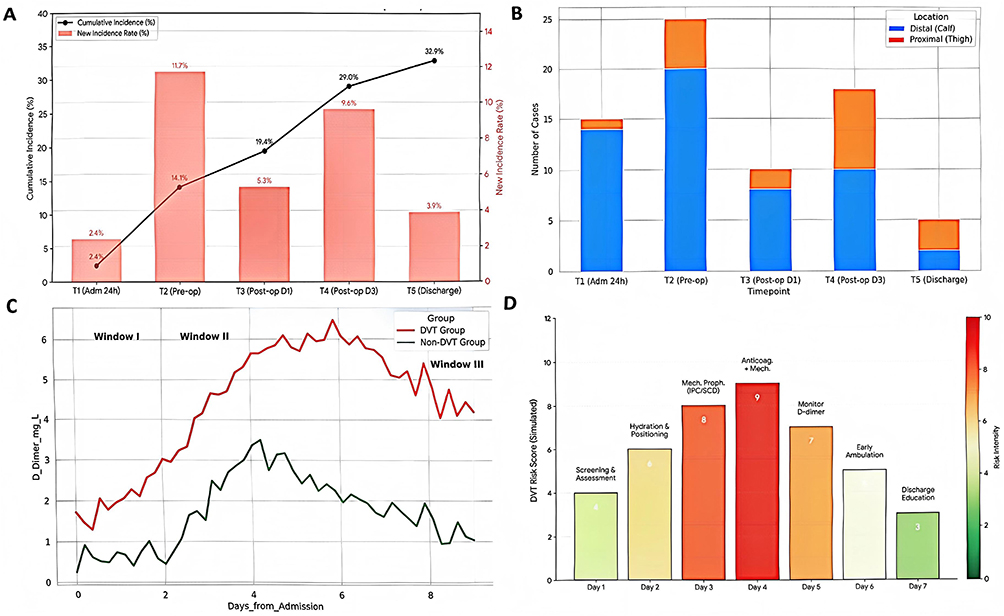 |
Figure 2 (A) Dynamic temporal distribution of perioperative Deep Vein Thrombosis (DVT) incidence. The combination chart illustrates the incidence of new DVT cases (bars) and the cumulative incidence rate (line) across five key timepoints: T1 (within 24h of admission), T2 (preoperative day), T3 (postoperative day 1), T4 (postoperative day 3), and T5 (discharge). (B) Topographical evolution of thrombus distribution throughout the perioperative period. Stacked bar chart displaying the changing proportions of thrombus locations over time. Blue bars represent distal thrombosis (isolated in calf muscle veins), while Orange barsrepresent proximal thrombosis (involving popliteal or femoral veins). (C) Longitudinal trajectories of plasma D-dimer levels stratified by DVT status across three defined nursing intervention windows. Window I (Admission Screening, grey), Window II (Preoperative Optimization, orange), and Window III (Postoperative Surveillance, blue). (D) Heatmap visualization of the Risk-Driven Nursing Intervention Matrix. This diagram correlates the patient’s daily dynamic risk score with the corresponding intensity of nursing interventions. The X-axis represents the length of hospital stay (days), and the color intensity reflects the risk magnitude (Red = High Risk; Green = Low Risk). |
Identification of Stage-Specific Risk Factors
To facilitate targeted nursing interventions, independent risk factors were identified separately for the preoperative and postoperative phases using multivariate logistic regression. For preoperative DVT, five independent risk factors were identified: Age > 65 years (OR=1.95, p=0.002), Preoperative Waiting Time > 3 days (OR=3.10, p<0.001), Admission D-dimer > 1.85 mg/L (OR=3.55, p<0.001), Low Albumin < 35 g/L (OR=2.25, p=0.004), and Time from injury to admission > 12h (OR=1.72, p=0.015). Notably, while the Neutrophil-to-Lymphocyte Ratio (NLR) was included in the initial analysis, it failed to reach statistical significance in the multivariate model (OR=0.81, p=0.052) and was therefore excluded from the final prediction model. The strong association between prolonged waiting time and DVT risk further validates the “twin-peak” observation, identifying the waiting period as a modifiable risk factor (Table 2).
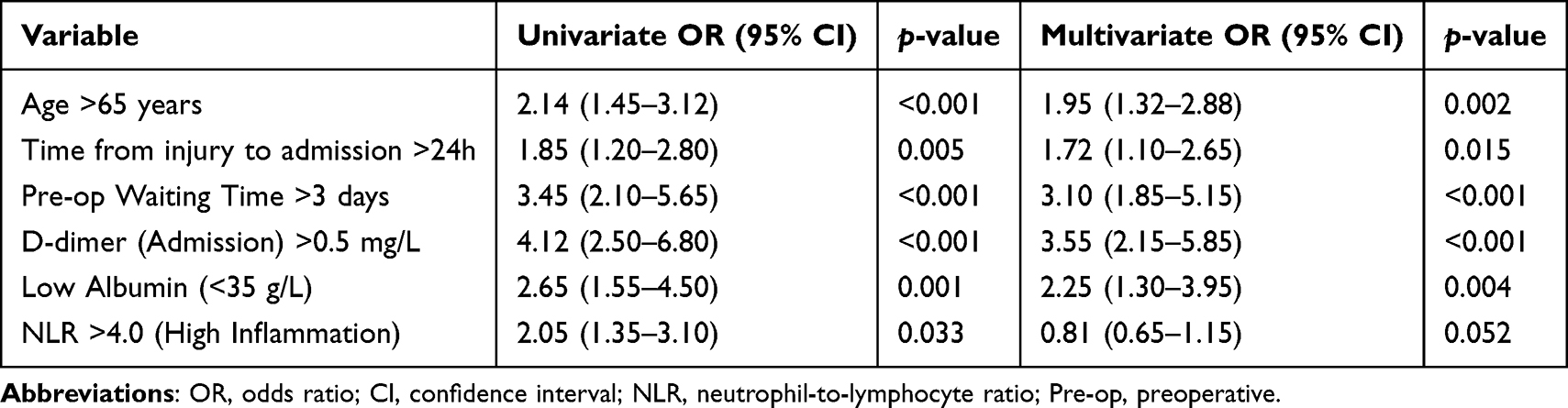 |
Table 2 Univariate and Multivariate Logistic Regression Analysis of Risk Factors Associated with Preoperative DVT |
For new-onset postoperative DVT, the risk profile shifted towards surgical and care-related factors. Independent predictors included Surgery Duration >120 min (OR=1.85, p=0.007), Intraoperative Blood Loss >400 mL (OR=1.55, p=0.038), Postoperative Bed Rest >3 days (OR=2.55, p<0.001), and Lack of Mechanical Prophylaxis (OR=1.95, p=0.004) (Table 3).
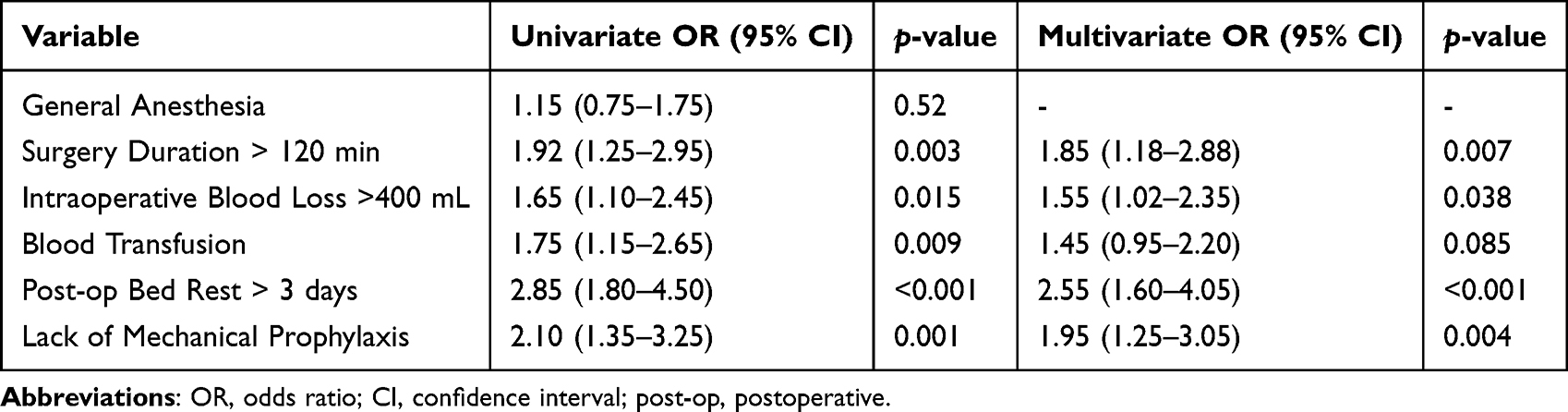 |
Table 3 Univariate and Multivariate Logistic Regression Analysis of Independent Predictors for New-Onset Postoperative DVT |
Construction and Validation of the Dynamic Nursing Assessment Model
ROC curve analysis revealed that the combined nomogram achieved an AUC of 0.905 (95% CI: 0.882–0.928), which was higher than that of D-dimer (AUC=0.796), Age (AUC=0.745), Preoperative Waiting Time (AUC=0.701), Albumin (AUC=0.659), and Time from Injury to Admission (AUC=0.601) (all p < 0.001) (Figure 3A and Table 4). Based on the identified predictors, including Age, Preoperative Waiting Time, D-dimer, Albumin, and Time from Injury to Admission, a dynamic nomogram was then constructed (Figure 3B). At the optimal cut-off value (>125 points), the nomogram showed a sensitivity of 87.5% and a specificity of 82.4%. The calibration curve showed agreement between the predicted probabilities and the observed frequencies of DVT (Figure 3C). Decision curve analysis showed that the nomogram provided a higher net benefit than the treat-all and treat-none strategies across threshold probabilities of approximately 0%–80% (Figure 3D).
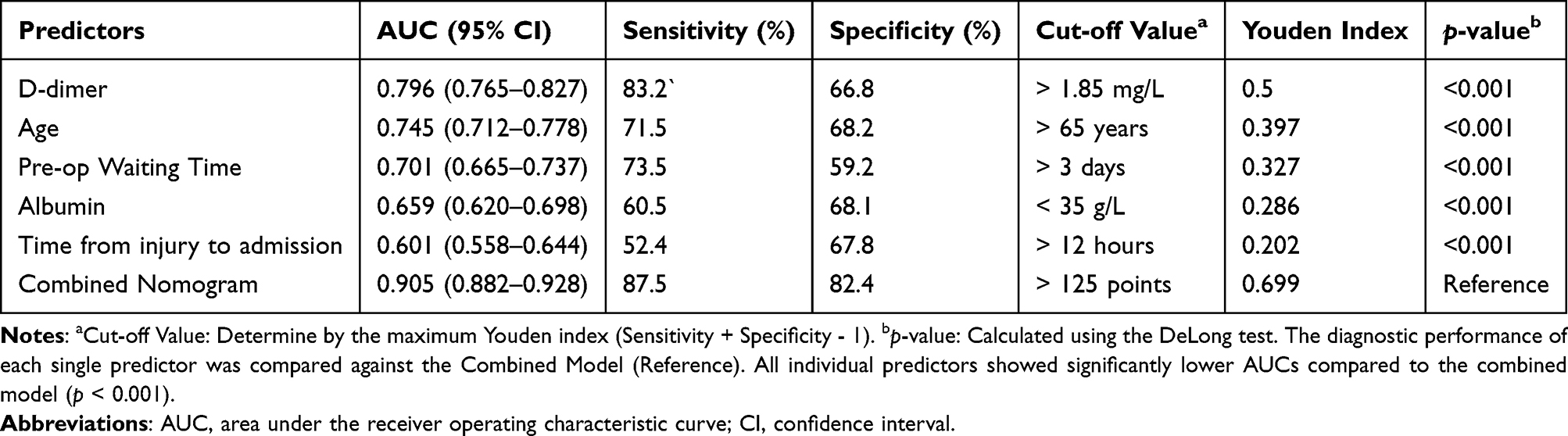 |
Table 4 Comparison of Diagnostic Performance Between the Combined Model and Individual Predictors for Perioperative DVT |
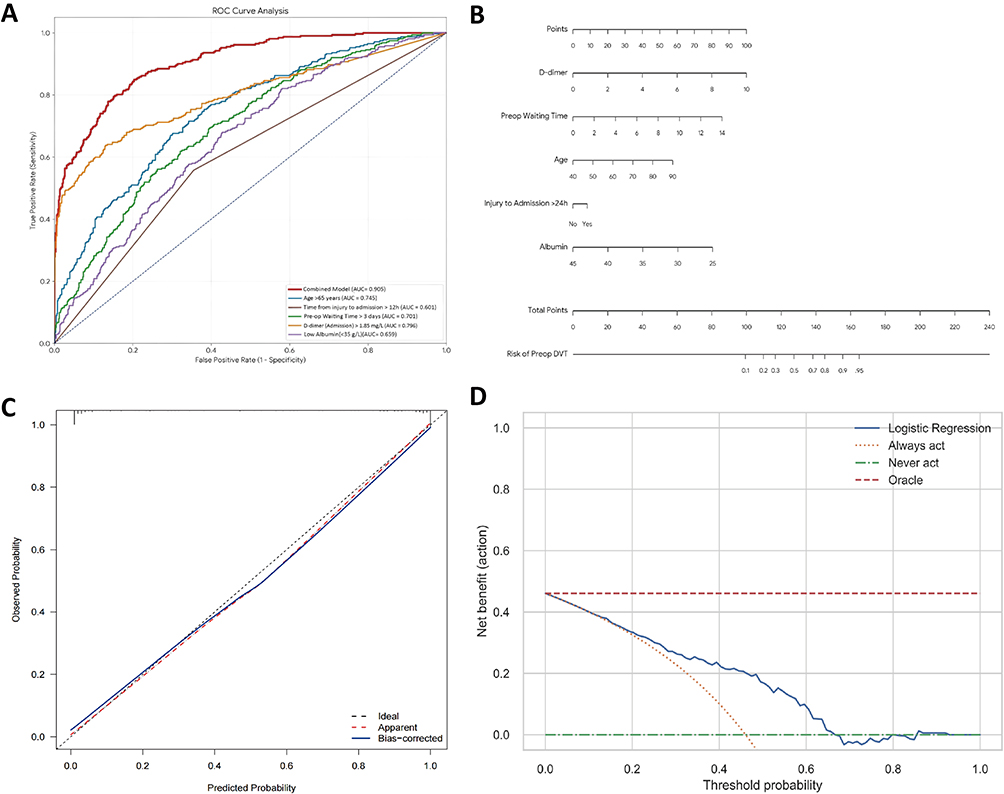 |
Figure 3 Development and validation of the dynamic nomogram for preoperative DVT prediction. (A) Receiver operating characteristic (ROC) curve analysis. The Combined Model (Red line) demonstrates superior discrimination with an AUC of 0.905, significantly outperforming individual predictors: D-dimer (Orange, AUC = 0.796), Age > 65 years (Blue, AUC = 0.745), Pre-op Waiting Time > 3 days (Green, AUC = 0.701), Low Albumin (Purple, AUC = 0.659), and Time from injury to admission > 24h (Brown, AUC = 0.601). (B) Dynamic prognostic nomogram. The nomogram integrates five independent risk factors: D-dimer, Albumin, Preop Waiting Time, Age, and Time from injury to admission > 24h. To estimate risk, locate the patient’s value on each variable axis, draw a vertical line to the “Points” scale, sum the points to find the “Total Points,” and project downwards to determine the “Risk of Preop DVT.” (C) Calibration plot. The x-axis represents the nomogram-predicted probability, and the y-axis represents the actual observed probability. The diagonal dashed line indicates ideal prediction (perfect agreement), while the solid blue line represents the bias-corrected performance (bootstrapped 1000 times), indicating excellent calibration between the predicted and observed outcomes. (D) Decision Curve Analysis (DCA). The graph illustrates the clinical net benefit of the prediction model. The Logistic Regression model (Blue solid line) is compared against the theoretical perfect predictor “Oracle” (Red dashed line), the “Always act” strategy (Orange dotted line), and the “Never act” strategy (Green dash-dot line), demonstrating a positive net benefit across a wide range of threshold probabilities. |
Model Interpretability and Feature Importance Analysis
SHAP analysis was performed to visualize the contribution of each predictor to the model output. The SHAP summary plot showed the directional impact of each feature on DVT prediction. Higher values of D-dimer and Preoperative Waiting Time were associated with positive SHAP values, whereas higher Albumin levels were associated with negative SHAP values (Figure 4A). The global feature importance ranking demonstrated that D-dimer had the highest mean |SHAP| value (1.85), followed by Albumin (1.17), Preoperative Waiting Time (0.92), Age (0.80), and Time from Injury to Admission >12 h (0.54) (Figure 4B).
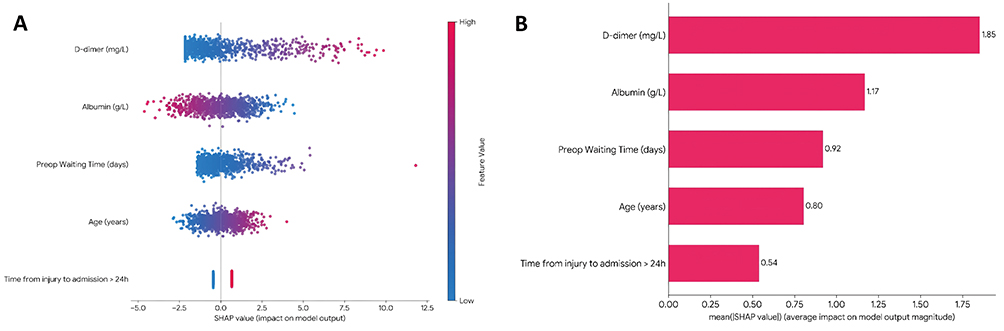 |
Figure 4 Model interpretability and feature importance analysis using SHAP values. (A) SHAP summary plot. The graph visualizes the distribution of SHAP values for each risk factor, illustrating their impact on the model’s output. The x-axis represents the SHAP value, where a positive value indicates an increased risk of DVT. Each dot corresponds to an individual patient. The color gradient reflects the feature value, with red indicating high values and blue indicating low values (e.g., higher D-dimer levels and lower Albumin levels are associated with positive SHAP values). (B) Global feature importance ranking. The bar chart displays the mean absolute SHAP value (mean |SHAP value|) for each predictor, quantifying their overall contribution to the predictive model. D-dimer (1.85) was identified as the most significant predictor, followed by Albumin (1.17) and Preoperative Waiting Time (0.92). |
Discussion
This prospective cohort study demonstrated that perioperative DVT after lower extremity traumatic fractures follows a dynamic pattern, with the preoperative waiting period representing a clinically important risk window. These findings support a shift from static postoperative-centered prophylaxis toward a dynamic, stage-specific nursing strategy guided by evolving perioperative risk.
The “Twin-Peak” Phenomenon: Rethinking the Preoperative Window
A key finding of this study was the identification of a “twin-peak” pattern of DVT incidence, with a notable preoperative peak at T2. DVT is traditionally considered a postoperative complication triggered by surgical trauma.21 In contrast, our data indicate that thrombotic risk may begin to increase before surgery, likely under the combined effects of fracture-related injury and preoperative immobilization. These findings suggest that the clinically relevant prevention window starts at admission, highlighting the need for earlier perioperative prophylactic assessment and intervention.
This finding suggests a need to reconsider the traditional “postoperative-centric” perspective presented in earlier guidelines. While foundational studies, such as those by Geerts et al, primarily emphasized postoperative risks, our results appear to be more consistent with emerging trauma-specific evidence.22 Zhu et al recently reported a high prevalence of preoperative DVT in tibial fractures, attributing it to injury severity.23 Our study advances this knowledge by identifying “Preoperative Waiting Time >3 days” as a modifiable independent risk factor (OR=3.10). Unlike non-modifiable factors like age, waiting time is logistical. This provides a compelling evidence base for nursing managers to advocate for “Fast-Track” protocols, viewing the reduction of Door-to-OR time not just as an efficiency metric, but as a critical patient safety intervention.
Furthermore, the bimodal distribution supports stage-specific nursing interventions. During the preoperative peak, priority should be given to minimizing immobilization and strengthening mechanical prophylaxis, whereas during the postoperative peak, emphasis should shift to early mobilization and closer surveillance for complications. Recognizing these distinct high-risk windows may help optimize nursing resource allocation and improve the timing of perioperative prevention.
Albumin and Inflammation: The Hidden Link Between Nutrition and Thrombosis
Our study identified serum albumin as an independent predictor of DVT. In routine nursing assessment, albumin is often regarded primarily as a nutritional marker related to wound healing.24 However, our findings suggest that it may also be linked to thrombogenesis. Hypoalbuminemia may promote edema, hemoconcentration, and increased blood viscosity by reducing plasma oncotic pressure, thereby disturbing vascular homeostasis. In addition, as a negative acute-phase reactant, low albumin may reflect systemic inflammation and endothelial dysfunction rather than nutritional deficiency alone.25–27 This combined hemodynamic and inflammatory relevance may explain its prognostic value in trauma patients.
This study helps refine thrombotic risk assessment by addressing an important limitation of existing predictive tools. Although the widely used Caprini Risk Assessment Model is comprehensive, it does not include markers of nutritional or inflammatory status such as serum albumin. Consequently, some patients with marked hypoalbuminemia may have their thrombotic risk underestimated. Our findings are consistent with those of Chi et al, who reported an independent association between hypoalbuminemia and VTE risk in medical inpatients.28 In addition, studies by Ma et al and Zhang et al showed that incorporating albumin into the Caprini framework improved discrimination for postoperative DVT.29,30 Together, these findings support the inclusion of albumin in dynamic risk screening for acute fracture patients.
The present findings support the interplay between nutrition, inflammation, and thrombosis. In addition to conventional prophylactic measures such as compression and anticoagulation, optimizing nutritional status may represent a complementary strategy for DVT prevention. Previous studies have shown that early enteral nutrition and albumin supplementation in malnourished or hypoproteinemic patients may help restore oncotic pressure, reduce systemic inflammation, and improve vascular homeostasis.31,32 From this perspective, nursing care may extend beyond coagulation monitoring to include nutritional and metabolic management as part of a multidisciplinary prevention strategy.33
Distal-to-Proximal Propagation: The Necessity of Dynamic Surveillance
Regarding the topographical evolution of thrombosis, serial ultrasound demonstrated a distal-to-proximal shift during the perioperative period. Most thrombi identified at admission were located in the distal calf muscular veins, whereas the proportion of proximal thrombi increased postoperatively. This finding suggests possible propagation of distal thrombi during the perioperative course, potentially facilitated by perioperative immobilization and surgical factors.
This observation adds to the ongoing discussion regarding the management of isolated distal deep vein thrombosis (IDDVT). Current ACCP guidelines recommend serial ultrasonographic surveillance rather than routine anticoagulation for low-risk patients.34 However, accumulating evidence suggests that trauma-related IDDVT may carry a higher risk of propagation because of the pronounced hypercoagulable state. In a cohort of critically ill trauma patients, early anticoagulation reduced thrombus progression by nearly 70%, and trauma was identified as an independent risk factor for propagation.35 These findings differ from those of outpatient studies involving predominantly medical patients and suggest that distal thrombi in trauma patients may serve as a source of proximal extension and PE.36,37
Accordingly, a single screening approach may be insufficient to detect the dynamic evolution of perioperative thrombosis. Our findings support serial ultrasound surveillance, or at least targeted re-scanning for patients with distal thrombi. Nursing assessment is important in this context, as subtle changes in calf tenderness or swelling may prompt earlier ultrasound reassessment.
Clinical Utility of the Nomogram: From “One-Size-Fits-All” to Precision Nursing
To enhance clinical applicability, we developed a nomogram with good diagnostic performance and calibration. Decision curve analysis further showed a higher net benefit than the treat-all and treat-none strategies across threshold probabilities of 0%–80%. These findings support its potential value in perioperative risk stratification.
Compared with conventional static tools such as the Caprini and Wells scores, our dynamic nomogram may offer advantages in orthopedic trauma populations. Although the Caprini model remains widely recommended for VTE prevention, it often shows a “ceiling effect” in fracture patients, with most individuals classified as high risk and limited discrimination of those at particularly high or imminent risk.38
Recent studies have refined the Caprini framework by incorporating biochemical and temporal variables to improve prediction. For example, Guo et al39 added D-dimer and injury-to-admission time in elderly hip fracture patients and reported improved discrimination, while Wu et al40 combined the Caprini score with thrombotic molecular markers and achieved higher diagnostic accuracy in trauma patients. These findings highlight the value of incorporating dynamic physiological information beyond fixed baseline variables.
Building upon this evidence, our model introduces two key dynamic predictors—preoperative waiting time and D-dimer levels—to represent the evolving hypercoagulable state that characterizes the perioperative course of fracture patients. While Prabhakaran et al previously attempted to modify trauma-specific risk stratification, few prior studies have quantified the mechanistic contribution of preoperative delay to thrombogenesis.41 By addressing this gap, our model offers a real-time and individualized approach that better reflects the temporal evolution of risk, thereby improving early identification and preventive nursing strategies for high-risk trauma patients.
Strengths and Limitations
The main strength of this study lies in its prospective design and five-timepoint ultrasound surveillance, which enabled dynamic characterization of perioperative DVT evolution. In addition, SHAP analysis improved the interpretability of the prediction model by illustrating the contribution of each risk factor. However, several limitations should be acknowledged. First, this was a single-center study, and the findings require external validation in multicenter cohorts. Second, PE was not systematically assessed because routine CTPA screening was not performed in all patients; future studies should therefore include concurrent PE surveillance. Third, long-term follow-up for PTS was not included. Future research should extend the observation period and explore additional markers, including genomic indicators, to further refine the prediction model.
Conclusions
In conclusion, this study establishes that perioperative DVT in patients with lower extremity traumatic fractures follows a dynamic “twin-peak” evolution, identifying the preoperative waiting period as a critical, high-risk window that is frequently overlooked in current practice. By integrating dynamic variables—specifically preoperative waiting time, Time from injury to admission, and serum albumin—into a validated nomogram (AUC 0.905) we provide a robust, evidence-based tool that significantly outperforms traditional static risk models in predicting thrombotic events. These findings advocate for a fundamental paradigm shift in nursing management from standardized, postoperative-centric prophylaxis to a dynamic, stage-specific strategy that prioritizes the minimization of logistical delays and early nutritional optimization to effectively reduce patient risk.
Data Sharing Statement
The data supporting the conclusions of this manuscript will be made available by the corresponding authors upon reasonable request.
Ethics Approval
The study protocol was designed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Xiangyang Central Hospital (Approval No. 2019-47-07). Written informed consent was obtained from all participants or their legal guardians upon admission.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Xuehua Hu and Yunying Wang are co-first authors in this study. The authors declare that they have no competing interests.
References
1. Zeng X, Zhu D, Xiao Z, Lin H. Risk factors and clinical value of deep venous thrombosis after traumatic lower limb fractures. J Clin Lab Anal. 2025;39:e70019. doi:10.1002/jcla.70019
2. Zhao W-G, Zhang W-L, Zhang Y-Z. Characteristics of deep venous thrombosis in isolated lower extremity fractures and unsolved problems in guidelines: a review of recent literature. Orthop Surg. 2022;14(8):1558–13. doi:10.1111/os.13306
3. Ahmed M, Mohammed A, Widaa MA, et al. Assessment of venous thromboembolism (VTE) risk evaluation and compliance with guidelines in surgical patients: a clinical audit at the prince osman digna referral hospital. Cureus. 2025:17e90550. doi:10.7759/cureus.90550
4. Mukhopadhyay S, Johnson TA, Duru N, et al. Fibrinolysis and inflammation in venous thrombus resolution. Front Immunol. 2019;10:1348. doi:10.3389/fimmu.2019.01348
5. Sasson I, Sorin V, Ziv-Baran T, et al. Unexpected early pulmonary thrombi in war injured patients. Eur Radiol. 2025;36(2):1196–1204. doi:10.1007/s00330-025-11925-2
6. Rappold JF, Sheppard FR, Carmichael IS, et al. Venous thromboembolism prophylaxis in the trauma intensive care unit: an American association for the surgery of trauma critical care committee clinical consensus document. Trauma Surg Acute Care Open. 2021;6e643. doi:10.1136/tsaco-2020-000643
7. Ratnasekera A, Seng SS, Ciarmella M, et al. Thromboprophylaxis in hospitalized trauma patients: a systematic review and meta-analysis of implementation strategies. Trauma Surgery Acute Care Open. 2024;9(1):e1420. doi:10.1136/tsaco-2024-001420
8. Taoka T, Ohmori T, Kanazawa T, Toda K, Ishihara T, Ito Y. Delayed surgery after hip fracture affects the incidence of venous thromboembolism. J Orthop Surg Res. 2023;18(1):630. doi:10.1186/s13018-023-04122-8
9. Yang W, Wei Q, Wang H, et al. Preoperative incidence and risk factors of deep venous thrombosis in patients with isolated femoral shaft fracture. BMC Surg. 2022;22(1):83. doi:10.1186/s12893-022-01534-x
10. Ma J, Tian M, Zhu Y, Hu J, Zhang Y, Li X. Development and validation of a predictive model for preoperative deep vein thrombosis following traumatic thoracolumbar fractures. Sci Rep. 2024;14(1):19547. doi:10.1038/s41598-024-70464-w
11. Qiu CX, Chan PH, Royse KE, et al. The preoperative waiting time on long-term survival following elderly hip fracture surgery. Geriatrics. 2025;10:153. doi:10.3390/geriatrics10060153
12. Ley EJ, Brown C, Moore EE, et al. Updated guidelines to reduce venous thromboembolism in trauma patients: a Western Trauma Association critical decisions algorithm. J Trauma Acute Care Surg. 2020;89(5):971–981. doi:10.1097/TA.0000000000002830
13. Touw CE, Nemeth B, Rondon A, et al. Lower-leg injury and knee arthroscopy have distinct effects on coagulation. Blood Adv. 2022;6(17):5232–5243. doi:10.1182/bloodadvances.2022007828
14. Hartono F, Yusuf I, Suhadi B, Fachruddin A, Augustinus Y. Trauma magnitude of the meta-epyphyseal cancellous affects the incidence of deep vein thrombosis. A prospective cohort study on the dynamic of Collagen I, Collagen IV, Tissue factor, P-Selectin and nitric oxide in the thrombus formation following hip and knee surgeries. Ann Med Surg. 2021;63:102190. doi:10.1016/j.amsu.2021.102190
15. Lv B, Wang H, Zhang Z, Li W. Distribution characteristics of perioperative deep vein thrombosis (DVT) and risk factors of postoperative DVT exacerbation in patients with thoracolumbar fractures caused by high-energy injuries. Eur J Trauma Emerg Surg. 2024;50(4):1481–1487. doi:10.1007/s00068-024-02468-0
16. Palareti G, Schellong S. Isolated distal deep vein thrombosis: what we know and what we are doing. J Thromb Haemost. 2012;10(1):11–19. doi:10.1111/j.1538-7836.2011.04564.x
17. Wang X, Sun C, Liu Y, et al. Association between thrombus signal intensity and pulmonary embolism in patients with proximal deep vein thrombosis: a magnetic resonance imaging study. Arterioscler Thromb Vasc Biol. 2025;45(10):1957–1968. doi:10.1161/ATVBAHA.125.322857
18. Zhang X, Hao A, Lu Y, Huang W. Deep vein thrombosis and validation of the Caprini risk assessment model in Chinese orthopaedic trauma patients: a multi-center retrospective cohort study enrolling 34,893 patients. Eur J Trauma Emerg Surg. 2023;49(4):1863–1871. doi:10.1007/s00068-023-02265-1
19. Yao W, Zhang K, Lv Q, Deng Z, Ding W. D-dimer-albumin ratio (DAR) as a new biomarker for predicting preoperative deep vein thrombosis after geriatric Hip fracture patients. J Orthop Surg Res. 2023;18(1):645. doi:10.1186/s13018-023-04139-z
20. Wang T, Guo J, Long Y, Yin Y, Hou Z. Risk factors for preoperative deep venous thrombosis in hip fracture patients: a meta-analysis. J Orthop Traumatol. 2022;23(1):19. doi:10.1186/s10195-022-00639-6
21. Xiong X, Cheng B. Preoperative risk factors for deep vein thrombosis in knee osteoarthritis patients undergoing total knee arthroplasty. J Orthop Sci. 2023;28(1):180–187. doi:10.1016/j.jos.2021.09.016
22. Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126(3 Suppl):338S–400S. doi:10.1378/chest.126.3_suppl.338S
23. Zhu Y, Chen W, Li J, et al. Incidence and locations of preoperative deep venous thrombosis (DVT) of lower extremity following tibial plateau fractures: a prospective cohort study. J Orthop Surg Res. 2021;16(1):113. doi:10.1186/s13018-021-02259-y
24. Rowan MP, Cancio LC, Elster EA, et al. Burn wound healing and treatment: review and advancements. Crit Care. 2015;19(1):243. doi:10.1186/s13054-015-0961-2
25. Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: pathogenesis and clinical significance. JPEN J Parenter Enteral Nutr. 2019;43(2):181–193. doi:10.1002/jpen.1451
26. Ahmed MS, Jadhav AB, Hassan A, Meng QH. Acute phase reactants as novel predictors of cardiovascular disease. ISRN Inflammation. 2012;2012:953461. doi:10.5402/2012/953461
27. Pathophysiology ED. Evaluation, and management of edema in childhood nephrotic syndrome. Front Pediatr. 2015;3:111. doi:10.3389/fped.2015.00111
28. Chi G, Gibson CM, Liu Y, et al. Inverse relationship of serum albumin to the risk of venous thromboembolism among acutely ill hospitalized patients: analysis from the APEX trial. Am J Hematol. 2019;94(1):21–28. doi:10.1002/ajh.25296
29. Ma L, Mao L, Jia P, et al. Utility of a Caprini-combined prediction model in patients with gynecological venous thromboembolism in China. Front Med Lausanne. 2025;12:1618023. doi:10.3389/fmed.2025.1618023
30. Zhang S, Pang Q, Liu W, et al. Preoperative albumin can predict the risk of postoperative deep venous thrombosis in non-cardiac surgery. Front Med Lausanne. 2025;12:1635218. doi:10.3389/fmed.2025.1635218
31. He Y, Xiao J, Shi Z, He J, Li T. Supplementation of enteral nutritional powder decreases surgical site infection, prosthetic joint infection, and readmission after Hip arthroplasty in geriatric femoral neck fracture with hypoalbuminemia. J Orthop Surg Res. 2019;14(1):292. doi:10.1186/s13018-019-1343-2
32. Abunnaja S, Cuviello A, Sanchez JA. Enteral and parenteral nutrition in the perioperative period: state of the art. Nutrients. 2013;5(2):608–623. doi:10.3390/nu5020608
33. Kalantar-Zadeh K, Anker SD, Horwich TB, Fonarow GC. Nutritional and anti-inflammatory interventions in chronic heart failure. Am J Cardiol. 2008;101(11):89E–103E. doi:10.1016/j.amjcard.2008.03.007
34. Robert-Ebadi H, Righini M. Should we diagnose and treat distal deep vein thrombosis? Hematol Am Soc Hematol Educ Program. 2017;2017(1):231–236. doi:10.1182/asheducation-2017.1.231
35. Fan S, Fu B, Liu J, Liu Y, Wang X, Chen H. Anticoagulation in critically ill patients with isolated distal deep vein thrombosis: a retrospective cohort study. BMC Cardiovasc Disord. 2025;25(1):646. doi:10.1186/s12872-025-05087-8
36. Schellong SM, Goldhaber SZ, Weitz JI, et al. Isolated distal deep vein thrombosis: perspectives from the GARFIELD-VTE registry. Thromb Haemost. 2019;119(10):1675–1685. doi:10.1055/s-0039-1693461
37. Franco L, Giustozzi M, Agnelli G, Becattini C. Anticoagulation in patients with isolated distal deep vein thrombosis: a meta-analysis. J Thromb Haemost. 2017;15(6):1142–1154. doi:10.1111/jth.13677
38. Han S, Bai Y, Jiao K, et al. Development and validation of a newly developed nomogram for predicting the risk of deep vein thrombosis after surgery for lower limb fractures in elderly patients. Front Surg. 2023;10:1095505. doi:10.3389/fsurg.2023.1095505
39. Guo Y-F, Zhang D, Guo A, et al. Optimizing preoperative venous thromboembolism risk assessment in elderly hip fracture patients: a refined caprini model integrating D-dimer and injury-to-admission time. Clin Appl Thromb Hemost. 2025;31:1279389659. doi:10.1177/10760296251396133
40. Wu Z, Du Y, Cai X, Xu Q. Caprini score combined with thrombotic molecular markers for predicting DVT in patients with traumatic fractures. Sci Rep. 2025;15(1):1847. doi:10.1038/s41598-025-85941-z
41. Prabhakaran K, Gogna S, Lombardo G, Latifi R. Venous thromboembolism in geriatric trauma patients—risk factors and associated outcomes. J Surg Res. 2020;254:327–333. doi:10.1016/j.jss.2020.05.008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Nomogram for Predicting Postoperative Deep Vein Thrombosis Risk in Patients After Laparoscopic Partial Nephrectomy
Wu C, Li Y, Wang X, Pan H, Jiang D
Cancer Management and Research 2026, 18:533674
Published Date: 12 January 2026
Development and Validation of a Nursing-Integrated Nomogram to Predict 1-Year Ulcer Recurrence in Patients with Diabetic Foot Ulcers After Endovascular Therapy
Fu L, Zeng W, Ding H, Chen Z, Chen X
Diabetes, Metabolic Syndrome and Obesity 2026, 19:591186
Published Date: 23 April 2026