Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Dynamic AFP-Defined Disease State Transitions in Hospitalized Patients with Hepatocellular Carcinoma Using the Multi-State Markov Model: A Retrospective Cohort Study
Authors Song Q ![]() , Zhang H, Jia M, Yu Y
, Zhang H, Jia M, Yu Y ![]() , Jiang Y, Yuan J, Su S
, Jiang Y, Yuan J, Su S ![]()
Received 12 February 2026
Accepted for publication 14 May 2026
Published 26 May 2026 Volume 2026:13 603210
DOI https://doi.org/10.2147/JHC.S603210
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Jörg Trojan
Qingxian Song,1,* Huiyi Zhang,1,2,* Meng Jia,1 Yingni Yu,1 Ying Jiang,3 Jun Yuan,1,2 Shu Su1,4
1Key Laboratory of Molecular Biology for Infectious Diseases, Department of Infectious Diseases, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2School of Public Health, Chongqing Medical University, Chongqing, People’s Republic of China; 3Department of Travel Health, Chongqing International Travel Healthcare Centre (Port Outpatient of Chongqing Customs), Chongqing, People’s Republic of China; 4Department of Epidemiology and Biostatistics, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shu Su, Key Laboratory of Molecular Biology for Infectious Diseases, Department of Infectious Diseases, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China, Email [email protected] Jun Yuan, School of Public Health, Chongqing Medical University, Chongqing, People’s Republic of China, Email [email protected]
Background: Hepatocellular carcinoma (HCC) exhibits highly variable disease trajectories, posing challenges for longitudinal monitoring and prognostic assessment. Alpha-fetoprotein (AFP) is widely used in HCC management, but transitions between discrete AFP states over time have not been explicitly modeled.
Methods: We conducted a retrospective cohort study of 2,750 hospitalized HCC patients between 2016 and 2024, encompassing 17,076 hospitalizations. AFP measurements were categorized into four clinical relevant states (S1–S4, from low to high). A multi-state Markov (MSM) model was constructed to estimate transition probabilities, transition rates, and sojourn times, and to assess the effects of hepatitis B virus (HBV) infection, antiviral therapy, and major clinical covariates. Longitudinal AFP transitions were visualized using Sankey diagrams.
Results: Among 2,750 hospitalized HCC patients, AFP-defined disease states S1 and S4 were relatively stable, whereas intermediate states S2 and S3 exhibited frequent bidirectional transitions. Tenofovir disoproxil fumarate (TDF) therapy was associated with S2→S1 AFP decrease (HR 1.350, 95% CI 1.065– 1.710). Elevated alanine aminotransferase (ALT) showed bidirectional effects (S1→S2: HR 1.310, 95% CI 1.011– 1.696; S3→S4: HR 1.517, 95% CI 1.130– 2.035; S2→S1: HR 1.493, 95% CI 1.191– 1.872; S3→S2: HR 1.685, 95% CI 1.295– 2.193; S4→S3: HR 1.527, 95% CI 1.153– 2.021), while elevated aspartate aminotransferase (AST), and total bilirubin (TBIL) were associated with lower likelihood of AFP decrease (AST S4→S3: HR 0.664, 95% CI 0.486– 0.908; TBIL S3→S2: HR 0.687, 95% CI 0.492– 0.958; S4→S3: HR 0.674, 95% CI 0.472– 0.965). Shorter sojourn times and higher hospitalization frequencies indicated clinical instability in intermediate disease states, suggesting a potentially modifiable window for clinical intervention.
Conclusion: This study characterizes dynamic AFP-defined disease state transitions in hospitalized patients with HCC. Intermediate disease states represent unstable but potentially modifiable phases strongly influenced by antiviral therapy and liver function status. These findings support the value of longitudinal AFP monitoring beyond single time-point assessment and individualized clinical management.
Keywords: hepatocellular carcinoma, alpha-fetoprotein, multi-state Markov model, disease state transitions
Introduction
Hepatocellular carcinoma (HCC) poses a major public health burden due to its high incidence and mortality rates.1 Its pathogenesis is multifactorial, involving chronic viral hepatitis, liver cirrhosis, metabolic disorders, and a complex tumor microenvironment.2 Despite significant progress in imaging techniques and systemic therapies, the overall prognosis of HCC remains suboptimal.3,4 Moreover, HCC is characterized by marked biological heterogeneity and dynamic disease progression, with patients often exhibiting variable clinical trajectories over time, including changes in tumor burden, liver functional reserve, and treatment response.5–7 These dynamic processes reflect the interplay between tumor progression and underlying liver disease and pose persistent challenges for accurate disease monitoring and prognostic assessment in clinical practice. While longitudinal data have been increasingly used for prognostic modeling,8,9 few studies have formally characterizing transitions between distinct clinical disease states over time. This highlights the need for approaches that capture the temporal dynamics of HCC.
Alpha-fetoprotein (AFP) is the most widely used serological biomarker for HCC surveillance and prognostic assessment.10 Previous studies have shown that elevated AFP levels are associated with tumor burden, vascular invasion, metastatic potential, and overall survival.11–14 Experimental and translational studies further suggest that AFP may be involved in disease progression by inhibiting apoptosis through the Fas–FADD signaling pathway15 and modulating the tumor immune microenvironment through suppression of natural killer cell activity.16 Longitudinal changes in AFP levels may reflect not only tumor burden but also underlying biological activity and microenvironmental dynamics. In clinical practice, AFP trajectories are heterogeneous, encompassing sustained elevation, gradual decline, or marked fluctuations, highlighting the complex and dynamic nature of HCC progression. However, its transitions across clinically relevant states over time have not been well quantified. Thus, clarifying the longitudinal trajectories of AFP and transition between clinically relevant AFP-defined states may improve the interpretation of AFP monitoring results and provide evidence to guide clinical monitoring, risk assessment, and individualized management of HCC patients.
However, most previous studies have focused on baseline AFP measurements or group-based trajectory modeling, without systematically capturing the temporal dynamics and recurrent transitions among clinically relevant AFP-defined states.11–14 The multi-state Markov (MSM) model is capable of providing a statistical framework to analyze transitions among distinct disease states over time.17 By estimating transition rates, transition probabilities, and mean sojourn times, MSM models capture the recurrent and intermediate transitions that conventional trajectory analyses cannot fully resolve.
Building on these considerations, this study utilizes real-world longitudinal data from hospitalized HCC patients between 2016 and 2024. AFP measurements were categorized into clinically relevant disease states, and MSM models were applied to characterize AFP-defined disease state transition patterns. This study aims to characterize AFP transition patterns in real-world HCC patients, quantify transition risks between clinically defined states, and explore the influence of demographic, comorbidity, and biochemical covariates on disease progression. These findings provide quantitative estimates of dynamic risk that may inform future clinical decision models and support individualized monitoring strategies.
Materials and Methods
Study Design and Study Population
This retrospective cohort study included all adult hospitalized patients diagnosed with HCC at the Second Affiliated Hospital of Chongqing Medical University between January 1, 2016, and December 31, 2024. The Second Affiliated Hospital of Chongqing Medical University is a top tertiary hospital for infectious and liver diseases in China. The hospital houses the Chongqing Medical University Viral Hepatitis Research Institute, a national key discipline and clinical center for infectious diseases. The hospital has long-standing expertise in the diagnosis and management of chronic viral hepatitis and related liver diseases. As a high-volume referral hospital, it provides comprehensive care for patients with chronic viral hepatitis and HCC across a broad spectrum of disease etiologies and clinical stages.
Hospitalized patients were included because laboratory examinations were routinely and systematically performed during admission, allowing construction of longitudinal AFP trajectories. All data were extracted from the hospital electronic medical record system (HIS/LIS) and anonymized prior to analysis. Patients aged ≥18 were included if they had HCC and if AFP was measured during hospitalization. HCC was diagnosed according to the Guidelines for the Diagnosis and Treatment of Primary Liver Cancer issued by the National Health Commission of China,18 with diagnosis confirmed by imaging, histopathology, or comprehensive clinical assessment by experienced physicians. Patients who had undergone liver transplantation were excluded because transplantation significantly alters AFP dynamics and disease progression. Patients with fewer than two hospitalizations during the study period were also excluded, as insufficient follow-up would limit the evaluation of AFP level transitions over time. For each hospitalization, the value of AFP and all other laboratory tests was defined as the first measurement recorded within 72 hours of admission.
The study was approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University (Approval No. 2025135; approved on June 6, 2025), and the requirement for informed consent was waived due to the retrospective and anonymized nature of the study. The study was conducted in accordance with the Declaration of Helsinki. This study was reported in accordance with the STROCSS 2025 criteria.19
Definition of AFP-Defined Disease States
Serum AFP was measured using chemiluminescent immunoassay (CLIA) in our hospital’s central laboratory. The upper limit of normal (ULN) was defined as 20 ng/mL, consistent with the Guidelines for the Diagnosis and Treatment of Primary Liver Cancer.18 Disease activity was classified into four clinically relevant states based on AFP levels (S1–S4, from low to high), guided by national guidelines and prior literature:13,14,18
- State 1 (S1): AFP < 20 ng/mL
- State 2 (S2): 20 ≤ AFP < 200 ng/mL
- State 3 (S3): 200 ≤ AFP < 1000 ng/mL
- State 4 (S4): AFP ≥ 1000 ng/mL
Given the continuous nature of AFP and the clinically defined thresholds of these states, direct transitions between nonadjacent AFP levels within a single hospitalization were considered uncommon in routine clinical practice. Therefore, transitions were constrained to adjacent states by specifying a restricted transition intensity matrix, which improved model interpretability and numerical stability (Figure S1). The multi-state Markov model was fitted under a continuous-time framework. Given that disease status was only observed at discrete hospitalization visits, state transitions were assumed to occur within the intervals between consecutive admissions, and the time scale used for transition intensity estimation was the elapsed time (in years) between admissions. This approach allows for irregular observation intervals and enables robust estimation of transition intensities in real-world longitudinal data.
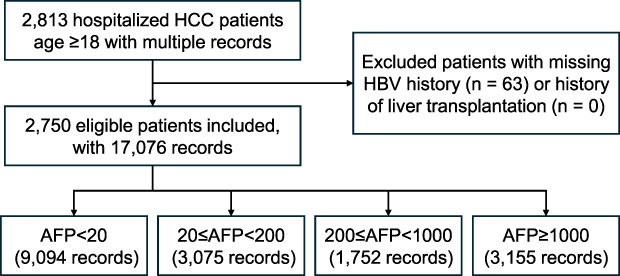 |
Figure 1 Flow diagram of patient selection and inclusion. Abbreviations: AFP, alpha-fetoprotein; HBV, hepatitis B virus. |
Covariate Selection and Definitions
Covariates were selected a priori based on biological plausibility and previous evidence linking liver function, systemic inflammation, viral activity, and tumor burden to AFP dynamics and HCC progression. Variables were grouped into the following categories: 1) HBV infection and antiviral therapy status (HBV&Trearment): patients were categorized into four groups based on HBV infection and antiviral therapy status: HBV-positive receiving tenofovir (TDF), HBV-positive receiving other antiviral therapies (Other-AVT), HBV-positive without treatment (Untreated), and HBV-negative (Uninfected); 2) Demographics: age and sex; 3) Comorbidities: Non-alcoholic fatty liver disease (NAFLD), alcoholic liver disease (ALD), and HIV infection (HIV); 4) Hematology and inflammatory markers: red blood cell count (RBC), white blood cell count (WBC), hemoglobin (HGB), platelet count (PLT), lymphocyte count (LYM), monocyte count (MONO), neutrophil count (NEUT), eosinophil count (EOS), basophil count (BASO), albumin/globulin ratio (AG); 5) Liver and renal function indices: alanine aminotransferase (ALT), aspartate aminotransferase (AST), γ-glutamyl transferase (GGT), alpha-L-fucosidase (AFU), 5′-nucleotidase (5′-NT), alkaline phosphatase (ALP), cholinesterase (ChE), total bilirubin (TBIL), direct bilirubin (DBIL), indirect bilirubin (IBIL), total bile acid (TBA), lactate (LAC), estimated glomerular filtration rate (eGFR), serum creatinine (SCr), prealbumin (PAB), total protein (TP), albumin (ALB), globulin (GLB), uric acid (UA), blood urea nitrogen (BUN), C-reactive protein (CRP); 6) Electrolytes: sodium (Na), potassium (K), chloride (Cl), calcium (Ca), magnesium (Mg), phosphorus (P). A complete list of variables and their definitions is provided in Table S1.
HBV infection was defined as HBsAg > 0.05 IU/mL, HBV DNA > 20 IU/mL, or a documented history of HBV antiviral therapy. Patients were classified into two age groups: <65 years (non-elderly) and ≥65 years (elderly).20,21 All laboratory variables were classified as normal or abnormal (high/low) according to the Chinese Health Industry Standards WS/T 404 series (National Health Commission of China).22
Statistical Analysis
Categorical variables were summarized as n (%). The missing data rate for all variables was below 10% and assumed to be missing at random. Missing values were imputed using a random forest algorithm, which is suitable for handling nonlinear relationships and mixed data types. We calculated the observed proportions of patients across the four AFP-defined disease states (S1–S4) for each hospitalization. Sankey diagrams were generated to visualize the dynamic changes of AFP levels across multiple hospitalizations. State transitions were identified using the state.msm function from the msm package in R, consistent with the structure of the multi-state Markov model.
Multi-State Markov Model
The MSM model was developed using the R package msm to characterize AFP-defined disease states transitions. The transition intensity matrix was estimated via maximum likelihood and then used to calculate state transition probabilities, mean sojourn times, and the effects of covariates on transition rates. Model convergence was assessed using the Hessian matrix. A positive definite Hessian indicates that the log-likelihood has reached a local maximum, with stable parameter estimates and computable standard errors, whereas a non-positive definite Hessian suggests model non-convergence. Model fit was evaluated using the log-likelihood (LL), Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC). Covariates were transformed into dummy variables, and variance inflation factors (VIFs) were all below 10, indicating no significant multicollinearity. Furthermore, considering the high correlations among TBIL, DBIL and IBIL, sensitivity analyses were conducted by replacing TBIL with both DBIL and IBIL.
Three models were constructed to evaluate the effects of covariates on AFP-defined disease states transitions. The basic model estimated the overall transition intensities and probabilities without adjusting for covariates. Univariate models were then fitted, in which each covariate was analyzed separately to assess its independent association with transition rates. Finally, a multivariate model was developed, incorporating all covariates that were statistically significant in the univariate analyses, to estimate adjusted hazard ratios (HRs) and 95% confidence intervals (CI). To further explore the effects of HBV infection and antiviral therapy status and other key variables, model-based estimates were obtained by varying one covariate at a time while keeping all other factors at their baseline (normal) levels. These model-based estimates were used to quantify adjusted transition rates, mean sojourn times, and transition probabilities across different covariate levels.
Sensitivity Analysis
To evaluate model robustness and explore the potential differential effects of bilirubin fractions, sensitivity analyses were performed by replacing TBIL with its individual components, DBIL and IBIL, in separate models. Because TBIL is the sum of DBIL and IBIL, including them simultaneously in the same model could introduce multicollinearity. This allowed assessment of the consistency of the results and revealed whether DBIL and IBIL contribute differently to AFP-defined disease states transitions.
All analyses were performed using R (version 4.3.2). Two-sided tests were used, with p < 0.05 considered statistically significant.
Results
Study Population
In initial screening, a total of 2,813 hospitalized patients with HCC were identified. After excluding patients with missing HBV infection history or prior liver transplantation (n = 63), 2,750 eligible patients were finally included, comprising 17,076 medical records for longitudinal analysis (Figure 1). The median age at first admission was 54 years (IQR: 48–62), 80.3% (2,209) were aged < 65 years, and 87.0% (2,393) of patients were male. Most patients were admitted to hepatobiliary surgery (42.7%, 1,173) or infectious disease departments (39.0%, 1,073). The median duration of hospitalization per patient was 4 days (IQR: 2–7) (Table 1).
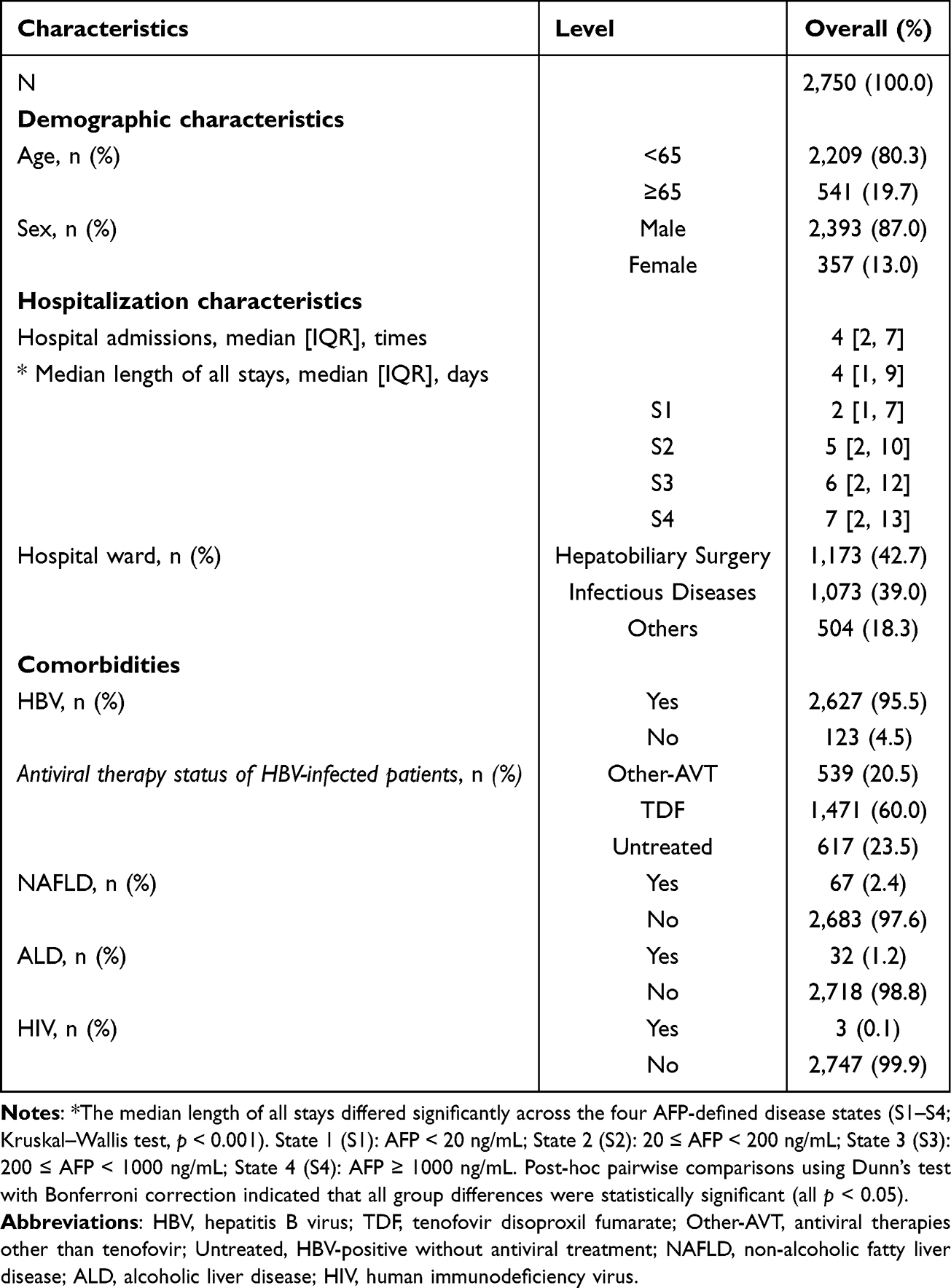 |
Table 1 Demographic and Clinical Characteristics of the Study Population |
Association of AFP-Defined Disease States with Hospitalization Duration
To evaluate the association between the four AFP-defined disease states and disease severity, we examined hospitalization duration across states. The median length of hospital stays increased progressively across states: S1 (2 [IQR: 1–7] days), S2 (5 [2–10]), S3 (6 [2–12]), and S4 (7 [2–13]) (p < 0.001; all pairwise comparisons significant by Dunn’s post-hoc test) (Table 1).
Patient Disease State Distribution and Transition Patterns
The distribution of patients across the four disease states (S1–S4) during the first five admissions was visualized using a Sankey diagram. At baseline (Admission 1), 38.84% of patients were classified as S1, 21.64% as S2, 12.29% as S3, and 27.24% as S4. Across all hospitalizations, S1 and S4 were relatively stable states, whereas intermediate states S2 and S3 exhibited frequent bidirectional transitions (Figure 2). A total of 14,326 state transitions were observed during the study period (Table S2). Among these, the majority of within-state transitions reflected disease stability: 93.07% of S1, 62.42% of S2, 53.12% of S3, and 84.06% of S4 remained in the same state at the subsequent admission.
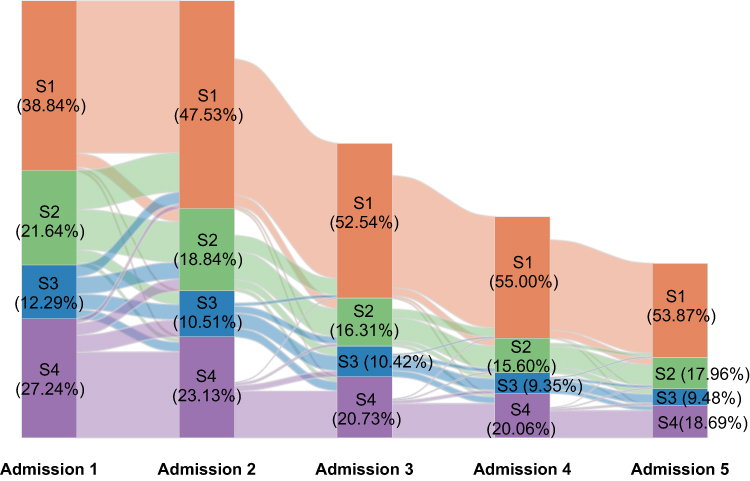 |
Figure 2 Sankey diagram of patient status transitions across the first five hospital admissions. Notes: Disease activity was classified into four clinically relevant states based on serum alpha-fetoprotein (AFP) levels: State 1 (S1): AFP < 20 ng/mL; State 2 (S2): 20 ≤ AFP < 200 ng/mL; State 3 (S3): 200 ≤ AFP < 1000 ng/mL; State 4 (S4): AFP ≥ 1000 ng/mL. |
One-year transition probabilities estimated from the multistate Markov model are presented in Table 2. Overall, patients in S1 (0.77, 95% CI: 0.76–0.79) and S4 (0.45, 95% CI: 0.42–0.48) showed a high probability of remaining in the same state, whereas patients in S2 (0.18, 95% CI: 0.17–0.19) and S3 (0.14, 95% CI: 0.13–0.16) were less likely to remain stable.
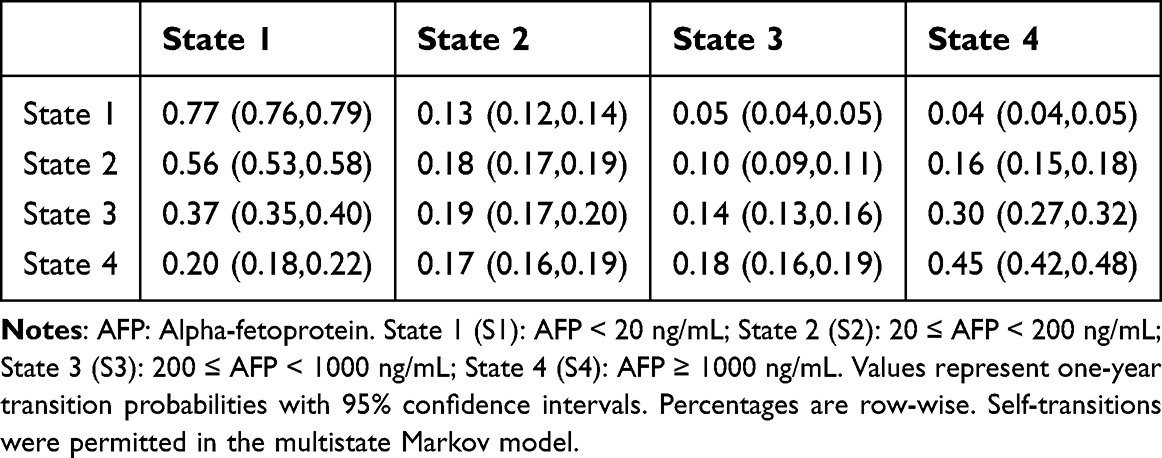 |
Table 2 One-Year Transition Probabilities Between AFP-Defined Disease States Estimated from the Base Multistate Markov Model |
Covariate Effects on Transition Probabilities
Variables significantly associated with state transitions in the univariate analysis (Table S3) were subsequently included in the multivariable Markov model (Table 3). In patients with HBV infection, receipt of TDF was associated with an increased likelihood of AFP decrease (S2→S1: HR 1.350, 95% CI 1.065–1.710) compared with other-AVT. Untreated patients had a lower likelihood of AFP decrease (S3→S2: HR 0.666, 95% CI 0.520–0.853). Uninfected patients exhibited a lower likelihood of both AFP increase (S1→S2: HR 0.357, 95% CI 0.172–0.742) and decrease (S2→S1: HR 0.148, 95% CI 0.056–0.390). NAFLD was associated with a reduced likelihood of AFP decrease from S2 to S1 (HR 0.630, 95% CI 0.397–0.999). In addition, HIV infection was significantly associated with an increased risk of AFP increase (S1→S2: HR 8.758, 95% CI 2.372–32.340). However, this estimate is derived from only six HIV-infected individuals (three baseline and three incident infections) in the cohort and therefore should be interpreted with caution due to limited statistical stability.
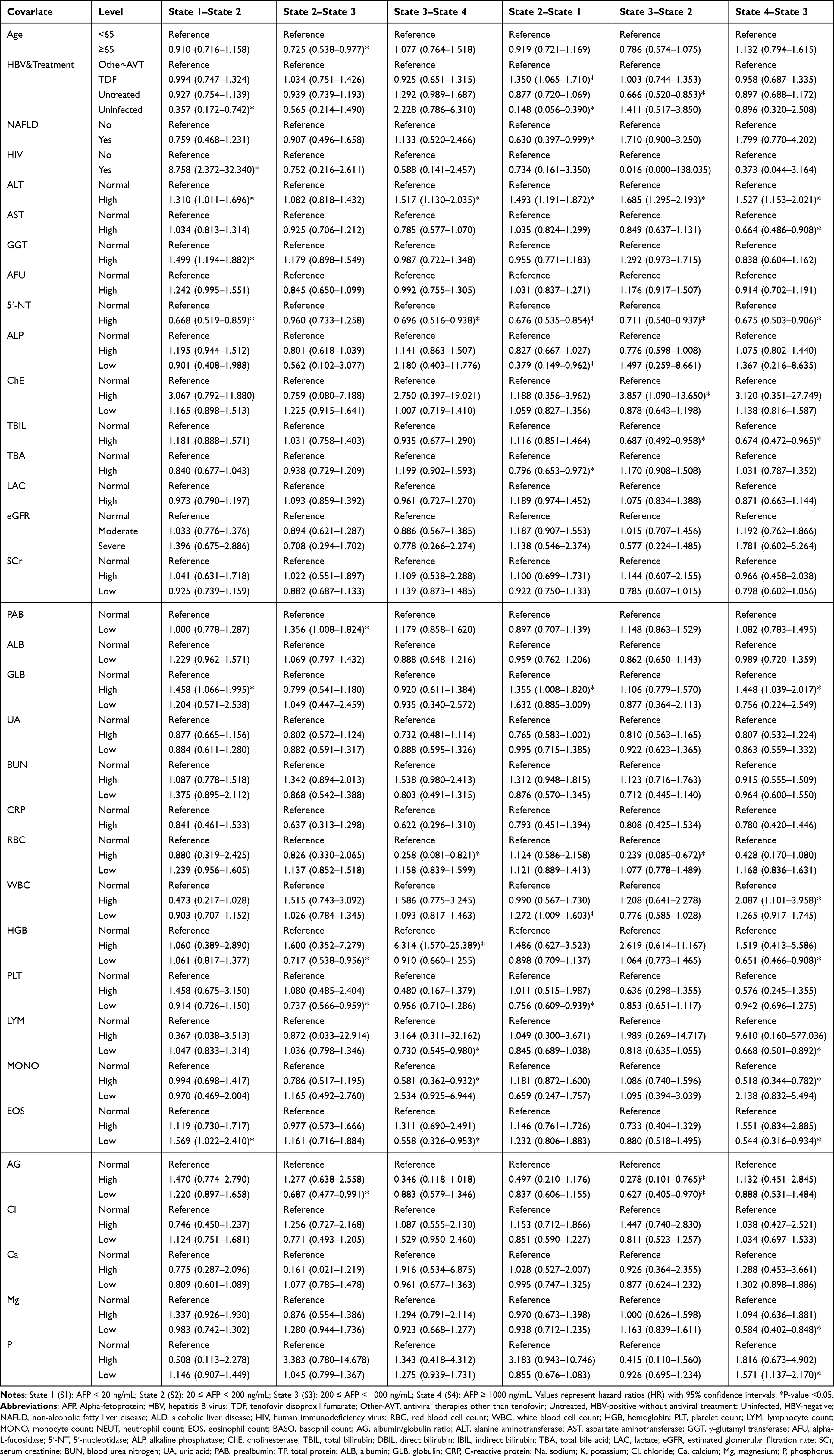 |
Table 3 Multivariable Associations of Clinical Covariates with Transition Hazards Between AFP-Defined Disease States (S1–S4) |
Among liver function indicators, elevated ALT was linked to both increased risk of AFP increase (S1→S2: HR 1.310, 95% CI 1.011–1.696; S3→S4: HR 1.517, 95% CI 1.130–2.035) and higher likelihood of AFP decrease (S2→S1: HR 1.493, 95% CI 1.191–1.872; S3→S2: HR 1.685, 95% CI 1.295–2.193; S4→S3: HR 1.527, 95% CI 1.153–2.021). Elevated AST and high TBIL were both associated with a lower likelihood of AFP decrease (AST S4→S3: HR 0.664, 95% CI 0.486–0.908; TBIL S3→S2: HR 0.687, 95% CI 0.492–0.958; S4→S3: HR 0.674, 95% CI 0.472–0.965). Elevated GGT and low PAB were associated with an increased risk of AFP increase (GGT S1→S2: HR 1.499, 95% CI 1.194–1.882; PAB S2→S3: HR 1.356, 95% CI 1.008–1.824). In contrast, renal function indicators were not significantly associated with state transitions. Other laboratory markers showing significant associations with state transitions are detailed in Table 3.
Model-Based Transition Probabilities and Subgroup Analysis
Model-based transition probabilities were estimated and visualized by subgroup to further illustrate the effects of key covariates. Overall, the transition probability curves largely corroborated the multivariable findings. For example, patients receiving TDF showed a higher probability of transitioning from S2 to S1 over time compared with patients receiving non-TDF therapy (Figure 3), consistent with the increased S2→S1 hazard observed in the multivariable model (HR 1.350, 95% CI 1.065–1.710). In contrast, uninfected participants exhibited lower probabilities of disease progression and AFP decrease, indicating a different transition pattern. Detailed subgroup transition curves are presented in Figures S2–S12.
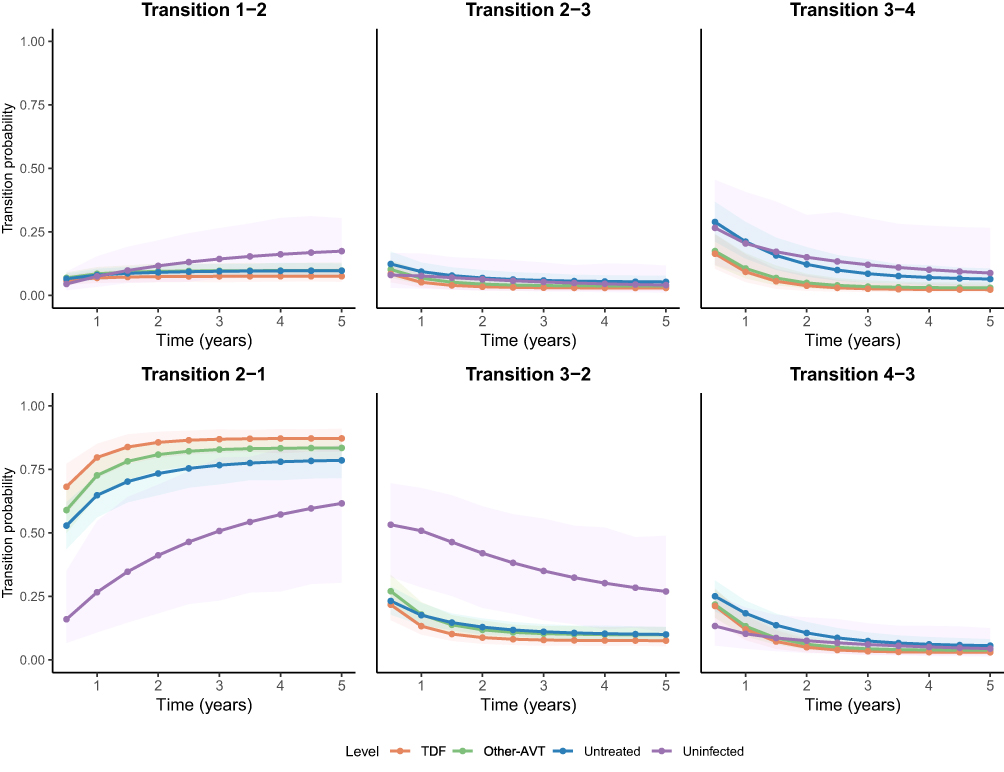 |
Figure 3 Estimated transition probabilities between AFP-defined disease states by HBV infection and antiviral therapy status. Abbreviations: AFP, alpha-fetoprotein; AVT, antiviral therapy; TDF, Tenofovir disoproxil fumarate. |
Sojourn Times, Total Length of Stay, and Number of Admissions
Patients spent the longest time in the stable state S1 (mean sojourn 2.00 years, 95% CI 1.82–2.18; total length of stay (TotLOS) 3.57 years, 95% CI 3.47–3.66; mean number of admissions 1.43, 95% CI 1.30–1.57), followed by S4 (sojourn 0.64 years, 95% CI 0.57–0.72; TotLOS 0.44 years, 95% CI 0.40–0.49; admissions 0.83, 95% CI 0.73–0.94), whereas the intermediate states S2 (0.25 years, 95% CI 0.23–0.26; TotLOS 0.68 years, 95% CI 0.63–0.73; admissions 2.90, 95% CI 2.70–3.13) and S3 (0.16 years, 95% CI 0.15–0.18; TotLOS 0.31 years, 95% CI 0.28–0.35; admissions 2.01, 95% CI 1.83–2.23) were shorter (Figure 4).
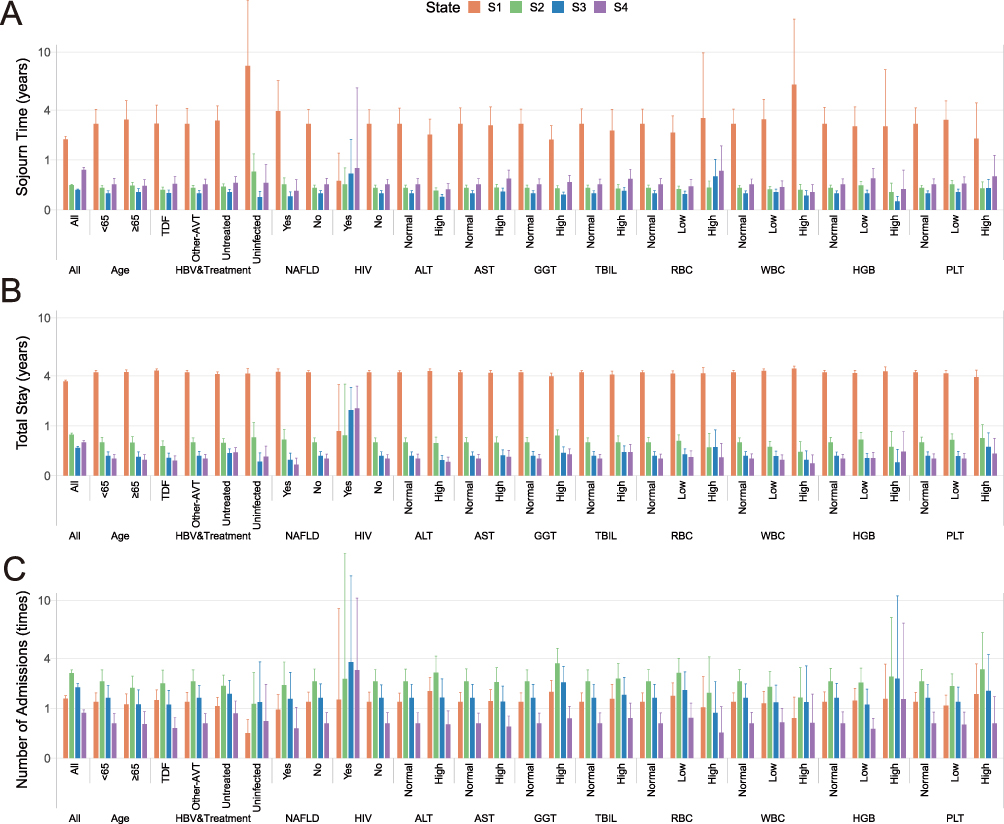 |
Figure 4 Model-based estimates of subgroup-specific outcomes for AFP-defined disease states S1–S4 (y-axis square root scaled). (A) Mean sojourn time; (B) Total length of stay; (C) Mean number of admissions. Abbreviations: HBV, hepatitis B virus; TDF, tenofovir disoproxil fumarate; AVT, antiviral therapy; NAFLD, non-alcoholic fatty liver disease; HIV, human immunodeficiency virus; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; TBIL, total bilirubin; RBC, red blood cell count; WBC, white blood cell count; HGB, hemoglobin; PLT, platelet count. Notes: Disease activity was classified into four clinically relevant states based on serum alpha-fetoprotein (AFP) levels: State 1 (S1): AFP < 20 ng/mL; State 2 (S2): 20 ≤ AFP < 200 ng/mL; State 3 (S3): 200 ≤ AFP < 1000 ng/mL; State 4 (S4): AFP ≥ 1000 ng/mL. |
Patterns of TotLOS and number of admissions were generally consistent with sojourn time estimates. Patients in S1 accumulated longer total lengths of stay but experienced fewer hospital admissions over time, whereas patients in intermediate states had shorter cumulative stays but more frequent admissions. Patients in S4 showed intermediate patterns, reflecting prolonged hospitalization periods with fewer transitions. Across subgroup analyses, similar trends were observed for most biochemical and hematologic indicators, with modest differences between categories. Overall, these utilization patterns were consistent with the estimated transition hazards and transition probabilities, supporting the robustness of the multi-state model results (Figure 4).
Sensitivity Analyses
Sensitivity analyses replacing TBIL with DBIL and IBIL yielded consistent results. For DBIL, high levels were generally consistent with the TBIL results, with a significantly lower likelihood of AFP decrease observed in the S2→S1 transition (HR 0.578, 95% CI 0.406–0.823). For IBIL, high levels were not significantly associated with any transitions. These findings indicate that the main results for TBIL are robust, and that the observed associations are largely driven by DBIL (Table S4).
Discussion
Using a multi-state Markov model, this study provides a longitudinal and state-based characterization of AFP-defined disease states among hospitalized patients with HCC. Our findings highlight pronounced heterogeneity in disease dynamics, with substantial volatility concentrated in intermediate states. While S1 represents a biologically quiescent state, S4 likely corresponds to an advanced disease phase characterized by persistently elevated AFP and limited short-term reversibility. Moreover, TDF therapy, HBV infection status, and liver indicators significantly influenced both progression and reversal.
A key observation of this study is that AFP-defined intermediate states (S2 and S3) exhibited frequent bidirectional transitions, shorter sojourn times, and higher admission frequencies compared with S1 and S4. Such instability is not captured by static prognostic models and underscores the value of multi-state approaches for identifying phases of heightened clinical fluctuation.23,24 Compared with S1 and S4, S2 and S3 are more likely to represent transitional stages in disease progression, during which fluctuations in tumor burden or liver function, increased risk of infection or complications, and changes in nutritional and inflammatory status can make clinical states prone to both AFP decrease and AFP increase in the short term. In addition, shorter sojourn times and higher admission frequencies among patients in S2 and S3 also indicate clinical instability in intermediate states, emphasizing their relevance for close monitoring and timely clinical decision-making.
Our findings further demonstrated that HBV infection status and antiviral therapy significantly influence disease state transitions. Specifically, patients receiving TDF exhibited more favorable transition patterns compared with those treated with other AVT. The higher probability of AFP decrease from S2 to S1 among TDF users suggested that potent viral suppression and improved inflammation control can yield short-term clinical benefits. Prior research has shown that TDF possesses stronger antiviral potency and a higher genetic barrier to resistance.25–27 Sustained viral suppression may reduce hepatic inflammatory activity and promote functional recovery, enabling some patients to transition toward more favorable states.28 Conversely, patients not receiving antiviral therapy exhibited a lower likelihood of AFP decrease from S3 to S2, indicating that inadequate viral control not only accelerates disease progression but also limits the potential for reversal. Notably, HBV-negative patients followed a distinct transition pattern characterized by lower AFP increase rates but also reduced AFP decrease rates, highlighting etiological differences in disease dynamics. Prior evidence suggested that liver injury from NAFLD or alcohol-related liver disease often exhibits a more chronic and cumulative pattern, which may be associated with smaller short-term fluctuations.29–31 Consistent with this observation, NAFLD was associated with a reduced likelihood of AFP decrease, suggesting that underlying metabolic liver injury may impede recovery of AFP-defined disease states. Evidence indicated that NAFLD-related HCC often presents with more advanced disease, lower response to curative therapy, and poorer prognosis compared with other etiologies. Specifically, NAFLD can drive chronic hepatic inflammation, steatohepatitis, fibrosis, and eventual malignant transformation.32,33 These pathophysiological processes may underlie the reduced transition toward milder disease states observed in patients with NAFLD in our cohort. These findings underscore that dynamic disease states in HCC are modifiable and that early and effective antiviral therapy, particularly TDF, can increase the likelihood of AFP decrease while reducing the risk of further AFP increase, highlighting the value of timely identification and intervention in high-risk HCC patients with HBV infection. The results also highlight the need for individualized management. HCC patients with HBV infection benefit most from potent antiviral therapy, whereas those with metabolic or alcohol-related liver disease may require long-term strategies aimed at mitigating chronic liver injury.
Several routine biochemical and hematological indicators demonstrated significant associations with state transitions. Elevated AST, GGT, TBIL, and low PAB were generally associated with adverse outcomes, either increasing the risk of AFP increase or reducing the likelihood of AFP decrease, consistent with their established roles as markers of cholestasis, tumor activity, or impaired hepatic reserve.34–36 ALT elevation was associated with both higher and lower AFP levels, reflecting its dual role as a marker of hepatocellular injury and a sensitive indicator of reversible inflammatory activity. Although ALT has traditionally been regarded as a marker of hepatocellular injury, recent studies indicate that its accuracy as a sole indicator for assessing liver disease progression is limited,37 and its levels are influenced by multiple factors.38,39 Persistent elevation reflects hepatocellular damage and increases the risk of AFP increase, whereas short-term inflammatory activation is reversible, so AFP decrease may still occur following interventions or viral suppression. Collectively, these routinely available laboratory indicators, within the multi-state modeling framework, reflect real-time liver function and inflammatory status and can be used to estimate short-term risk of disease state transitions. This framework enables identification of individuals at elevated risk of clinical deterioration or improvement based on current laboratory profiles, thereby supporting more timely and individualized decisions regarding monitoring intensity and therapeutic management.
Several limitations should be noted in this study. First, the study was based on a hospitalized HCC cohort, which is inherently enriched for patients with more advanced disease, complications, or treatment needs. This may introduce selection bias and limit generalizability to the broader HCC population, particularly patients managed in outpatient setting. Accordingly, the observed disease dynamics should be interpreted as reflecting the progression patterns within a hospital-based population rather than the full natural history of HCC in the general population. Second, disease states were defined using AFP level categories derived from routinely collected inpatient laboratory data. While this approach reflects real-world monitoring practices, it lacks the biological resolution to distinguish between AFP elevations driven by tumor progression versus those caused by HBV viral flares or other inflammatory events. Future studies incorporating imaging findings, tumor burden measures, and molecular biomarkers may further refine state definitions and improve biological interpretability. Third, our analysis only captured hospitalizations occurring within this study hospital. Admissions at other institutions were not tracked, which may lead to underestimation of total transitions and slightly bias transition probabilities. Fourth, laboratory variables were categorized rather than modeled continuously due to model complexity and the large number of covariates, which may result in loss of information and reduced statistical power. Despite these limitations, this study was designed to characterize clinically observable, hospital-based disease dynamics rather than reconstruct the complete natural history of HCC. The large sample size, longitudinal inpatient data, and multi-state modeling framework enable a structured and interpretable characterization of bidirectional disease transitions and heterogeneous covariate effects across multiple pathways. The analytical framework is computationally tractable, clinically interpretable, and biologically plausible, providing a practical basis for translation into clinical research and decision support.
Conclusions
In conclusion, this study systematically characterized dynamic inpatient disease activity trajectories in hospitalized patients with HCC. Intermediate disease states stratified by AFP levels were identified as dynamically unstable yet potentially modifiable phases. The observed associations with antiviral therapy and liver function further indicate that these intermediate states may represent clinically relevant stages within disease evolution. Incorporating dynamic AFP-defined states into clinical assessment may therefore support more timely risk stratification and assist clinical risk stratification and may support consideration of surveillance strategies based on real-time disease dynamics. However, given the observational nature of the study and the use of AFP as a surrogate biomarker, these findings should be interpreted as hypothesis-generating. Further prospective and multi-center studies integrating imaging and molecular biomarkers are needed to validate these dynamic states and to clarify their clinical utility in guiding patient management.
Abbreviations
AFP, Alpha-fetoprotein; HCC, Hepatocellular carcinoma; MSM, Multi-state Markov model; TDF, Tenofovir disoproxil fumarate; ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; GGT, γ-Glutamyl transferase; AFU, Alpha-L-fucosidase; 5′-NT, 5′-Nucleotidase; ALP, Alkaline phosphatase; ChE, Cholinesterase; TBIL, Total bilirubin; DBIL, Direct bilirubin; IBIL, Indirect bilirubin; TBA, Total bile acid; LAC, Lactate; eGFR, Estimated glomerular filtration rate; SCr, Serum creatinine; PAB, Prealbumin; TP, Total protein; ALB, Albumin; GLB, Globulin; UA, Uric acid; BUN, Blood urea nitrogen; CRP, C-reactive protein; HBV, Hepatitis B virus; AVT, Antiviral therapy; NAFLD, Non-alcoholic fatty liver disease; ALD, Alcoholic liver disease; HIV, Human immunodeficiency virus; RBC, Red blood cell count; WBC, White blood cell count; HGB, Hemoglobin; PLT, Platelet count; LYM, Lymphocyte count; MONO, Monocyte count; NEUT, Neutrophil count; EOS, Eosinophil count; BASO, Basophil count; IQR, Interquartile range; HR, Hazard ratio; CI, Confidence interval; TotLOS, Total length of stay.
Data Sharing Statement
The data that support the findings of this study are available on request from Dr. Shu Su, one of the corresponding authors. The data are not publicly available due to ethical restrictions.
Ethical Approval
The study was approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University (Approval No. 2025135; approved on June 6, 2025). No data were accessed or extracted for research purposes prior to ethical approval. The requirement for informed consent was waived by the Ethics Committee due to the retrospective use of de-identified data. The study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
SS is supported by the National Natural Science Foundation of China (82304246), Kuanren Talent programmes of the second affiliated hospital of Chongqing Medical University (202417-16) and Public Health Talent Program of Chongqing (GWZQN202536).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Yang JD, Hainaut P, Gores GJ, et al. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16:589–16. doi:10.1038/s41575-019-0186-y
2. Amin N, Anwar J, Sulaiman A, et al. Hepatocellular carcinoma: a comprehensive review. Diseases. 2025;13:207. doi:10.3390/diseases13070207
3. Wang MD, Diao YK, Yao LQ, et al. Emerging role of molecular diagnosis and personalized therapy for hepatocellular carcinoma. Iliver. 2024;3:100083. doi:10.1016/j.iliver.2024.100083
4. Reveron-Thornton RF, Teng MLP, Lee EY, et al. Global and regional long-term survival following resection for HCC in the recent decade: a meta-analysis of 110 studies. Hepatol Commun. 2022;6:1813–1826. doi:10.1002/hep4.1923
5. Giannini EG, Bucci L, Garuti F, et al. Patients with advanced hepatocellular carcinoma need a personalized management: a lesson from clinical practice. Hepatology. 2018;67:1784–1796. doi:10.1002/hep.29668
6. Sun J, Xia D, Bai W, et al. Tumor burden affects the progression pattern on the prognosis in patients treated with sorafenib. Front Oncol. 2024;14:1405178. doi:10.3389/fonc.2024.1405178
7. Zhao J, Gao J, Liu W, et al. Dynamic conditional survival nomogram for primary hepatocellular carcinoma: a population-based analysis. Discov Oncol. 2025;16:854. doi:10.1007/s12672-025-02642-9
8. Shen L, Zeng Q, Guo P, et al. Dynamically prognosticating patients with hepatocellular carcinoma through survival paths mapping based on time-series data. Nat Commun. 2018;9:2230. doi:10.1038/s41467-018-04633-7
9. Ma X, Huang L, Yu M, et al. Dynamic prediction of the risk of hepatocellular carcinoma after DAA treatment for hepatitis C patients. Cancer Control. 2025;32:10732748251316609. doi:10.1177/10732748251316609
10. Galle PR, Foerster F, Kudo M, et al. Biology and significance of alpha-fetoprotein in hepatocellular carcinoma. Liver Int. 2019;39:2214–2229. doi:10.1111/liv.14223
11. Xiao Y, Chen W, Deng W, et al. Prognostic value of alpha-fetoprotein in unresectable hepatocellular carcinoma treated with hepatic artery infusion chemotherapy combined with lenvatinib and camrelizumab. J Hepatocell Carcinoma. 2024;11:1251–1263. doi:10.2147/jhc.S460922
12. Chi X, Jiang L, Yuan Y, et al. A comparison of clinical pathologic characteristics between alpha-fetoprotein negative and positive hepatocellular carcinoma patients from Eastern and Southern China. BMC Gastroenterol. 2022;22:202. doi:10.1186/s12876-022-02279-w
13. Mazza S, Frigerio C, Alfieri D, et al. Prognostic role of basal serum alpha-fetoprotein in patients with hepatocellular carcinoma suitable for curative treatment. Medicina. 2024;60:692. doi:10.3390/medicina60050692
14. Hsu CY, Liu PH, Lee YH, et al. Using serum α-fetoprotein for prognostic prediction in patients with hepatocellular carcinoma: what is the most optimal cutoff? PLoS One. 2015;10:e0118825. doi:10.1371/journal.pone.0118825
15. Chen T, Dai X, Dai J, et al. AFP promotes HCC progression by suppressing the HuR-mediated Fas/FADD apoptotic pathway. Cell Death Dis. 2020;11:822. doi:10.1038/s41419-020-03030-7
16. Lu Y, Lin B, Li M. The role of alpha-fetoprotein in the tumor microenvironment of hepatocellular carcinoma. Front Oncol. 2024;14:1363695. doi:10.3389/fonc.2024.1363695
17. Jackson C. Multi-State models for panel data: the msm package for R. J Statistical Software. 2011;38:1–28. doi:10.18637/jss.v038.i08
18. National Health Commission of China. Guidelines for the Diagnosis and Treatment of Primary Liver Cancer. Beijing; 2024.
19. A RA, Ginimol M, Rasha R, et al. Revised Strengthening the Reporting of Cohort, Cross-Sectional and Case-Control Studies in Surgery (STROCSS) guideline: an update for the age of artificial intelligence. Premier J Sci. 2025;2. doi:10.70389/PJS.100081
20. Wang CM, Chen ZX, Ma PC, et al. Oncological prognosis and morbidity of hepatectomy in elderly patients with hepatocellular carcinoma: a propensity score matching and multicentre study. BMC Surg. 2023;23:323. doi:10.1186/s12893-023-02230-0
21. Sabharwal S, Wilson H, Reilly P, et al. Heterogeneity of the definition of elderly age in current orthopaedic research. Springerplus. 2015;4:516. doi:10.1186/s40064-015-1307-x
22. National Health Commission of China. Reference Intervals for Common Clinical Biochemistry Tests (WS/T 404 Series). Beijing; 2015-2022.
23. Chen RX, Gan YH, Ge NL, et al. A new prediction model for prognosis of patients with intermediate-stage HCC after conventional transarterial chemoembolization: an internally validated study. J Cancer. 2019;10:6535–6542. doi:10.7150/jca.34064
24. Kim J, Kim JH, Ko E, et al. Model predicting survival in intermediate-stage HCC patients reclassified for TACE based on the 2022 BCLC criteria. Cancers. 2025;17:894. doi:10.3390/cancers17050894
25. Kim HJ, Cho JY, Kim YJ, et al. Long-term efficacy of tenofovir disoproxil fumarate therapy after multiple nucleos(t)ide analogue failure in chronic hepatitis B patients. Korean J Intern Med. 2015;30:32–41. doi:10.3904/kjim.2015.30.1.32
26. Yang J, Chen Y, Sun H, et al. Tenofovir versus entecavir on decreasing risk of HBV-related hepatocellular carcinoma recurrence after liver transplantation. Infect Agent Cancer. 2023;18:2. doi:10.1186/s13027-022-00478-4
27. Peng JX, Wang LZ, Wang QT, et al. Tenofovir versus entecavir on the prognosis of hepatitis B virus-related hepatocellular carcinoma: a reconstructed individual patient data meta-analysis. Front Pharmacol. 2024;15:1393861. doi:10.3389/fphar.2024.1393861
28. Buti M, Fung S, Gane E, et al. Long-term clinical outcomes in cirrhotic chronic hepatitis B patients treated with tenofovir disoproxil fumarate for up to 5 years. Hepatol Int. 2015;9:243–250. doi:10.1007/s12072-015-9614-4
29. Puhakka E, Ahmed H, Haikonen R, et al. Serum Metabolite profile in progressive versus nonprogressive alcohol-related liver disease: a Cross-Sectional Metabolomics Study. Liver Int. 2025;45:e70128. doi:10.1111/liv.70128
30. Hagström H, Shang Y, Hegmar H, et al. Natural history and progression of metabolic dysfunction-associated steatotic liver disease. Lancet Gastroenterol Hepatol. 2024;9:944–956. doi:10.1016/s2468-1253(24)00193-6
31. Zhang Q, Hu J, Qiu S, et al. Clinical differences between HBV and alcohol related ACLF in a WGO classification multicenter study. Sci Rep. 2025;15:25292. doi:10.1038/s41598-025-09620-9
32. Alqahtani SA, Chan WK, Yu ML. Hepatic outcomes of nonalcoholic fatty liver disease including cirrhosis and hepatocellular carcinoma. Clin Liver Dis. 2023;27:211–223. doi:10.1016/j.cld.2023.01.019
33. Fang J, Celton-Morizur S, Desdouets C. NAFLD-Related HCC: focus on the latest relevant preclinical models. Cancers. 2023;15:3723. doi:10.3390/cancers15143723
34. Xing M, Gao M, Li J, et al. Characteristics of peripheral blood Gamma-glutamyl transferase in different liver diseases. Medicine. 2022;101:e28443. doi:10.1097/md.0000000000028443
35. Wang W, Zhang G, Liu H, et al. Clinical outcomes and early- prognostic biomarkers of primary biliary cholangitis with ductopenia. Front Immunol. 2025;16:1680942.
36. Xu XS, Wan Y, Song SD, et al. Model based on γ-glutamyltransferase and alkaline phosphatase for hepatocellular carcinoma prognosis. World J Gastroenterol. 2014;20:10944–10952. doi:10.3748/wjg.v20.i31.10944
37. Zeng Z, Hao H, Bi X, et al. Study on liver histopathology of chronic HBV infected patients with different normal ALT values. Front Immunol. 2022;13:1069752. doi:10.3389/fimmu.2022.1069752
38. Burra P, Cammà C, Invernizzi P, et al. Does the hepatologist still need to rely on aminotransferases in clinical practice? A reappraisal of the role of a classic biomarker in the diagnosis and clinical management of chronic liver diseases. Ann Hepatol. 2025;30:101900. doi:10.1016/j.aohep.2025.101900
39. Wang D, Zhou BY, Xiang L, et al. Alanine aminotransferase as a risk marker for new-onset metabolic dysfunction-associated fatty liver disease. World J Gastroenterol. 2024;30:3132–3139. doi:10.3748/wjg.v30.i25.3132
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Prognostic Nomogram for Patients with AFP and DCP Double-Negative Hepatocellular Carcinoma After Local Ablation
Qiao W, Li J, Wang Q, Jin R, Zhang H
Journal of Hepatocellular Carcinoma 2024, 11:271-284
Published Date: 3 February 2024
Efficacy and Safety of Transcatheter Arterial Chemoembolization Combined with Lenvatinib Plus Anti-PD-1 Inhibitors for Hepatocellular Carcinoma Patients with Extrahepatic Metastases: A Multicenter Retrospective Study
Liu DY, Li YN, Wu JY, Zeng ZX, Fu YK, Li H, Ou XY, Zhang ZB, Wang SJ, Wu JY, Yan ML
Journal of Hepatocellular Carcinoma 2024, 11:2339-2349
Published Date: 25 November 2024
Long-Term Outcome of No-Touch Radiofrequency Ablation for Treating AFP-Positive Small Hepatocellular Carcinoma
Wu G, Huang X, Ou X, Zou M, Xia F, Zhang L, Feng K, Ma K, Wang Q
Journal of Hepatocellular Carcinoma 2026, 13:603375
Published Date: 14 April 2026