Back to Journals » Journal of Pain Research » Volume 16
Dural Puncture Epidural with 25-G Spinal Needles versus Conventional Epidural Technique in Conjunction with PIEB for Labor Analgesia: A Randomized Trial
Authors Lin W ![]() , Yang Y, Lin J, Chen J, Lin Q
, Yang Y, Lin J, Chen J, Lin Q
Received 29 August 2023
Accepted for publication 31 October 2023
Published 8 November 2023 Volume 2023:16 Pages 3797—3805
DOI https://doi.org/10.2147/JPR.S424082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Dawood Sayed
Wenqian Lin,1– 3 Yongyong Yang,1– 3 Jun Lin,1– 3 Jianxing Chen,1– 3 Qun Lin1– 3
1Department of Anesthesiology, The First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, People’s Republic of China; 2Department of Anesthesiology, National Regional Medical Center, Binhai Campus of the First Affiliated Hospital, Fujian Medical University, Fuzhou, 350212, People’s Republic of China; 3Anesthesiology Research Institute, The First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, People’s Republic of China
Correspondence: Qun Lin, Department of Anesthesiology, The First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, People’s Republic of China, Email [email protected]
Purpose: To compare the effect of Dural puncture epidural (DPE) and conventional epidural (EP), in conjunction with programmed intermittent epidural bolus (PIEB) and low-concentration ropivacaine strategy.
Methods: After written informed consent was obtained, healthy nulliparous women with singleton pregnancies, vertex presentation at 38– 42 weeks’ gestation, cervical dilation of 3– 5 cm, and a desire for pain relief were randomly assigned to DPE or EP group. Dural matter was puncture with 25G Whitacre needle in DPE group. Analgesia was initiated with 15 mL of 0.1% ropivacaine over 5 minutes and was maintained by PIEB (8 mL of 0.08% ropivacaine with 2 μg/mL fentanyl every 40 min). Primary outcome was the percentage of adequate analgesia, defined as NRPS ≤ 1, at 30 minutes after the initiation of the epidural bolus.
Results: Out of 130 enrolled parturients, 127 were included in final analysis (64 in DPE group, 63 in EP group). No significant difference was found in percentage of adequate analgesia at 30 minutes (risk ratio: 1.09; 95% confidence interval: 0.90– 1.31; P = 0.366). At 8, 12, 14, and 16 minutes, percentage of adequate analgesia was higher in DPE group (P = 0.023, 0.027, 0.016 and 0.033, respectively). NPRS scores in DPE group decreased more dramatically within the first 30 min. The incidence of S2 sensory blocks at 20 and 30 min in DPE group was higher (P = 0.010 and 0.006, respectively). There were no differences in patient satisfaction, delivery mode, adverse effects, fetal bradycardia, and Apgar scores at 1 and 5 minutes.
Conclusion: The combination of the use of DPE technique with 25G spinal needle and PIEB technique for labor analgesia appears to enhance the quality of labor analgesia by accelerating onset and providing improved sacral blockade, without increasing adverse effects.
Keywords: dural puncture epidural, labor analgesia, programmed intermittent bolus, ropivacaine
Introduction
Labor pain is widely regarded as one of the most intense types of pain experienced by women during their lifetime. Effective pain relief is crucial for most women in labor. Neuraxial analgesia offers potent pain relief with minimal adverse effects. It also serves as a viable option for surgical anesthesia in case of cesarean delivery.1,2 The prevailing methods for providing neuraxial analgesia are conventional epidural (EP) and combined spinal-epidural (CSE) techniques.3 However, the EP technique is associated with slow onset and motor blockade, while the CSE technique often leads to more adverse effects such as pruritus and fetal bradycardia.1,4,5
Thus, dural puncture epidural (DPE) technique has been introduced with the aim of improving analgesic efficacy and reducing adverse effects.2,6 DPE involves dural puncture using a spinal needle, without directly delivering local anesthetic into the subarachnoid space.2 The created dural conduit is believed to facilitate translocation of epidural medication to the subarachnoid space, thereby expediting analgesic onset and enhancing its quality.7 However, existing data do not consistently support the clinical benefits associated with the DPE technique.2,6,8 Programmed intermittent epidural bolus (PIEB) is a novel method for maintenance of labor analgesia that intermittently injects a preset volume of local anesthetic into the epidural space at regular intervals. PIEB is associated with superior analgesic effects, lesser local anesthetic consumption, and lower risk of motor block compared to conventional continuous epidural infusion (CEI).9–12 Lower concentrations of ropivacaine can lead to sensory-motor dissociation block, which is associated with a decreased risk of motor block.12,13
In theory, DPE technique combined with PIEB infusion of low-concentration local ropivacaine for initial and maintenance analgesia may provide additional benefits for women in labor. However, limited data exist on this specific pain management strategy. To investigate the superiority of the DPE technique over the EP technique for labor analgesia in terms of analgesia onset and maintenance, side effects, and maternal satisfaction, we conducted this study to compare the two techniques in conjunction with PIEB administration of low-concentration ropivacaine.
Methods
Study Design and Participants Recruitment
This study was conducted in accordance with the principles of the Declaration of Helsinki. It was approved by the Ethics Committee of First Affiliated Hospital of Fujian Medical University (No: MRCTA, ECFAH of FMU 2019237, July 20, 2019) and registered at www.chictr.org.cn (No: ChiCTR1900024717; July 23, 2019). Written informed consent was obtained from all participants after being fully informed of the potential risks and benefits of the study.
Eligible participants were healthy nulliparous women with singleton pregnancies, classified as American Society of Anesthesiologists (ASA) class I or II, vertex presentation at 38–42 weeks’ gestation in active labor with a cervical dilation 3–5 cm, and a request for labor relief. Exclusion criteria included <20 or >40 years old, morbid obesity, diseases of pregnancy (gestational diabetes, gestational hypertension, and preeclampsia), contraindications to neuraxial blocks, conditions with high risk of a cesarean delivery (eg, placenta previa, history of uterine anomaly, or surgery), and known fetal abnormalities. Patients would be excluded from the study if the cerebrospinal fluid (CSF) return could not be observed from the spinal needle while performing the dural puncture or a delivery occurred within 1 hour after the administration of initial epidural dose.
Randomization
Patients were randomly assigned to either the DPE or EP group in a 1:1 ratio using a computer-generated random number table. Allocations were concealed in sequentially numbered opaque sealed envelopes. On request for labor pain relief, one anesthesiologist opened the envelope before initiating the procedure of neuraxial block. The patients, obstetricians, nurses, and anesthesia providers involved in labor analgesia management and data collection were blinded to the group allocation.
Analgesia Initial and Maintenance
Neuraxial procedures were performed in a right lateral decubitus flexed position at L3-L4 or L4-L5 interspace with a 17-G Tuohy needle. The epidural space was identified using the loss of resistance to saline technique. Dural puncture was performed with a 25-G Whitacre needle in DPE group, and the needle was retracted following the observation of cerebrospinal fluid flow. A 19-G single open end epidural catheter (Arrow International, Reading, PA) was inserted 5 cm into the epidural space. After a negative aspiration for blood and CSF, 3 mL of 2% lidocaine was administered as the test dose. Five minutes after, labor analgesia was initiated with divided doses of 15 mL 0.1% ropivacaine over 3 minutes given via the epidural catheter. Labor analgesia was maintained using the PIEB technique starting 30 minutes after the initial dose, with the following parameters: administration of 8 mL of 0.08% ropivacaine with 2 µg/mL fentanyl every 40 minutes, a demand dose of 8 mL for patient-controlled epidural analgesia (PCEA), a lockout interval of 15 minutes, and a maximum dose of 35 mL/h.
When patients requested additional pain relief beyond self-administered PCEA boluses, it was considered as inadequate analgesia. It was treated by administration of top-up dose (10 mL 0.08% ropivacaine with 2 µg/mL fentanyl). If inadequate pain persisted after 15 minutes, the catheter pulled back 1 cm and administrated a top-up dose. If inadequate pain persisted after 15 minutes, another top-up dose would be administrated. If the labor analgesia is not improved after the above intervention, epidural catheter replacement would be considered.
Data Collection
The labor pain was assessed using the verbal numeric pain rating scale (NPRS) score from 0 to 10 (0 = no pain, 10 = worst imaginable pain) after the initial dose completed (T0) and at 2 min intervals for the 30 min, then at 60 min and one hourly interval thereafter. The primary outcome of this study was the percentage of adequate analgesia at 30 minutes after the initiation of the epidural bolus. Adequate analgesia was defined as a NRPS score of ≤1.
Sensory and motor blocks were evaluated simultaneously with pain assessment. Sensory block was assessed using a pinprick stimulus. Thoracic dermatomal sensory levels were assessed along the midclavicular line. Lower extremity dermatomal levels were assessed at the inguinal crease (L1), anterior thigh (L2), medial knee (L3), medial malleolus (L4), between the great and second toes (L5), lateral heel (S1), and midpoint of popliteal fossa (S2), and the lowest level was recorded. Asymmetric block was defined as a difference in the sensory block level >2 dermatomes between the left and right sides. Motor block level was assessed using a modified Bromage score from 0 to 3 (0 = full flexion of knees and ankles, 1 = partial flexion of knees, full flexion of ankles, 2 = inability to flex knees and partial flexion of ankles, and 3 = inability to flex knees and ankles). Presence of motor blockade was defined as modified Bromage score ≥1.
The following variables were also documented: demographic data (including age, height, weight, gestational age, blood pressure, fetal heart rate, pain score, and cervical dilation before analgesia), mode of delivery, need for epidural top-up, catheter adjustment or replacement, adverse effects (hypotension defined as systolic blood pressure <90 mmHg or a decrease of systolic blood pressure by more than 20% from baseline, nausea, pruritus, fetal bradycardia defined as a heart rate less than 110 bpm for 10 minutes, postdural puncture headache), duration of labor, Apgar scores at 1 and 5 minutes, and satisfaction with analgesia (0 = very dissatisfied, 10 = very satisfied).
Sample Size Calculation
The primary endpoint of the study was the proportion of patients with NPRS ≤1 at 30 minute after the initial dose. The sample size was calculated using PASS version 15 software to achieve 80% power (two-tailed) with a medium effect size of 0.5 at an α level of 0.05 for the proportions of two groups. Thus, a sample size of 63 patients per group was required. We planned to enroll up to 130 patients (65 patients per group) in this study.
Statistical Analysis
Statistical processing was performed using the software packages IBM SPSS version 27. All data were expressed as mean ± standard deviation (SD) or median [interquartile ranges], number (percentage) or number, as appropriate. NPRS≤1, S2 blockade, asymmetric blocks, mode of delivery, fetal bradycardia and catheter adjustment were compared using Chi-square test. Adverse effects and catheter replacement were compared using Fisher’s exact test. Normal distribution of data was assessed by Kolmogorov–Smirnov test. Continuous parametric data were compared using the t test. Continuous non-parametric data were compared using the Mann–Whitney U-test. NPRS score was analyzed using general linear models (GLMs) for repeated measures to examine group differences in repeated measure effects. Time to adequate analgesia (NPRS ≤ 1) was analyzed using Kaplan–Meier curves and Cox regression. A P value <0.05 was considered significant.
Results
A total of 171 parturients were screened for eligibility. Of them, 130 parturients were enrolled in the study. Three women were excluded from data collection after randomization. Finally, 127 women completed the study, with 64 women in DPE group and 63 women in EP group (Figure 1). CSF return was successfully confirmed in all patients in DPE group. The demographic and baseline characteristics are shown in Table 1. No significant differences were found in demographic and baseline characteristics between two groups.
 |
Table 1 Demographic and Baseline Characteristics |
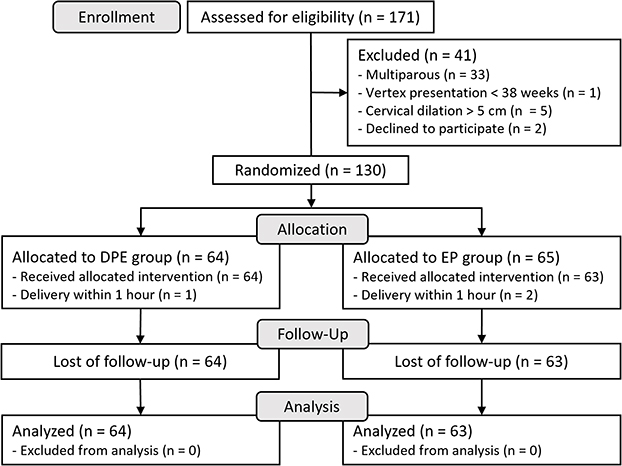 |
Figure 1 CONSORT trials flow diagram.DPE, dural puncture epidural; EP, conventional epidural. Notes: Adapted from Schulz KF, Altman DG, Moher D, CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3): e1000251. Copyright: © 2010 Schulz et al. Creative Commons Attribution License.14 |
The percentage of NPRS ≤ 1 at 30 minute after the initial epidural dose was 81.3% in DPE group and 74.6% in EP group. Significant difference was not found between DPE and EP group in percentage of adequate analgesia at 30 minutes (risk ratio [RR] 1.09; 95% confidence interval [CI] 0.90–1.31; P = 0.366). However, the percentage of patients with NPRS ≤ 1 in the DPE group was significantly higher compared to the EP group at 8, 12, 14, and 16 minutes (P = 0.023, 0.027, 0.016 and 0.033, respectively; Supplemental Table 1).
Kaplan–Meier curves of the time to achieve adequate analgesia are shown in Figure 2. A Log rank test analyzing the time to NPRS ≤1 showed a significant difference between the groups (P = 0.046). In the DPE group, women achieved an NPRS ≤1 significantly faster compared to those in the EP group (P = 0.024). The median time (interquartile range) to NPRS ≤1 achieved was 11 (6–17.5) minutes in DPE group and 16 (10–60) minutes in EP group (Table 2).
 |
Table 2 Outcomes Associated with DPE vs EP |
 |
Figure 2 Kaplan–Meier curves for time to adequate analgesia (NRPS ≤ 1) after epidural loading dose. Abbreviations: DPE, dural puncture epidural; EP, conventional epidural; NPRS, numeric pain rating scale. |
Figure 3 shows the NPRS scores for all patients at each data collection point within 30 minutes. The NPRS scores decreased over time in both groups (P < 0.001), but the decrease was more rapid in the DPE group than in the EP group (P = 0.023 for the interaction between neuraxial technique and time) within the first 30 minutes. Figure 4 displays the hourly NPRS scores. There was no significant difference between two groups in the hourly NPRS scores.
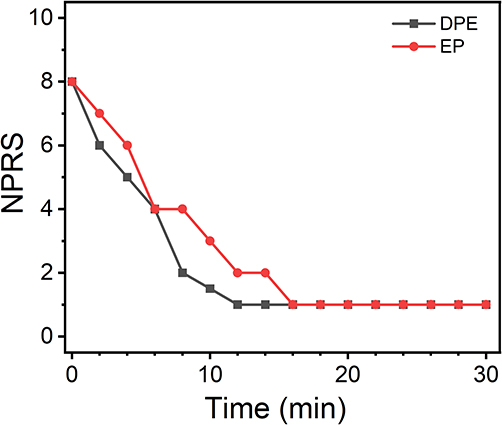 |
Figure 3 Median NPRS scores at 30 minutes after epidural loading dose. NPRS deceased over time (P < 0.001). NPRS in DPE group decreased more rapidly than in EP group (P = 0.023, interaction between neuraxial technique and time). Abbreviations: DPE, dural puncture epidural; EP, conventional epidural; NPRS, numeric pain rating scale. |
 |
Figure 4 Box plots of the NRPS scores hourly. Median and mean values are shown as a solid line (-) and (×) mark within box of 25th and 75th percentile values, respectively. Whiskers represent 5th and 95th percentile values. No significant differences were found between groups. Abbreviations: DPE, dural puncture epidural; EP, conventional epidural, NPRS, numeric pain rating scale. |
Compared with EP group, the S2 sensory blocks at 20 and 30 min were more frequently observed in DPE group (P = 0.010 and 0.006, respectively), whereas no difference was found at 10 min (P = 0.057). No significant differences were found in the incidence of asymmetric blocks at 30 min (RR = 0.530; CI: 0.226–1.241; P = 0.134) and in the requirement for epidural top-up bolus during the whole labor analgesia period (RR = 0.626; CI: 0.353–1.111; P = 0.103) (Table 2).
The mode of delivery, modified Bromage scores, newborn Apgar scores, adverse effects, and patient satisfaction scores did not significantly differ between the two groups (Table 2).
Discussion
In this study, we compared the DPE and EP techniques for the neuraxial labor analgesia in nulliparous women with singleton. Both groups received low concentrations of ropivacaine as epidural medication, administered using programmed intermittent epidural bolus technique for maintenance of labor analgesia. In the DPE group, dural puncture was performed using 25G Whitacre spinal needles. Our findings suggest a faster onset of analgesia and better sacral block in the DPE group.
The main distinction between the DPE and EP techniques lies in whether the dura mater is intentionally punctured with spinal needle or kept intact. This small difference is main determinant of the effect of DPE technique. On one hand, the direct observation of cerebrospinal fluid backflow through the spinal needle could help confirm the correct position of the epidural needle tip within the epidural space.2,6 This is highly advantageous for patients with technically challenging epidural procedures, such as obese individuals.2 On the other hand, epidural medication could transfer through the conduit created by dural puncture into subarachnoid space which was confirmed radiologically by Leach et al.15 And there is a significant association between the size of dural conduit and the medication translocation.6,16 One possible explanation for epidural-to-CSF transfer via the conduit, rather than the reverse, is that the administration of epidural medication can result in elevated epidural pressure, though it is physiologically lower than intrathecal pressure. And pencil-point spinal needles are used for dural puncture instead of Quincke needles, which has been shown to reduce CSF leakage via the dural hole and thus the risk of postdural puncture headache (PDPH).17
This translocation of medication is postulated to enhance the analgesic effect during labor analgesia. Some studies have demonstrated that the DPE technique is associated with faster analgesic onset, a lower incidence of sacral block sparing and asymmetric block, and a reduced need for additional physician bolus interventions.5,11,12,18 But conflicting results also have been reported in others, with no significant differences observed in sacral block, asymmetric block, and the requirement for epidural top-up bolus between the DPE and EP techniques.2,19,20 Two systematic reviews published in 2019 concluded that the evidence regarding the superiority of the DPE technique over the EP technique during labor analgesia remains inconclusive, due to the substantial heterogeneities.6,21 The variations in analgesic techniques used, such as the size of the spinal needle, concentration and type of local anesthetics, and other factors, may have contributed to the inconsistent findings. The differences in population enrollment could also have influenced the outcomes.
Dural conduit with a larger diameter would make epidural medication transfer more easily. Comparing 27G and 25G needles, Contreras et al found that 25G spinal needles had a statistically shorter onset time for labor analgesia.18 A recent meta-analysis demonstrated that the DPE technique with 25G spinal needle offers advantages over the EP technique.7 These advantages include hastened onset of analgesia, decreased necessity for epidural top-ups, and a reduced occurrence of asymmetric block.7 Larger size spinal needles (25G) were used in our study. We observed higher percentages of adequate analgesia at 8, 12, 14, and 16 minutes after the initial epidural dose in the DPE group, along with a significant shorter median time to adequate analgesia. And NPRS scores in DPE group decreased more dramatically than that in EP group within the first 30 min. Besides, we also found that the incidence of S2 sensory blocks at 20 and 30 min in DPE group was significantly higher. These findings also support the notion that the DPE technique leads to a faster onset of analgesia and better sacral blockade.
Besides, variations in local anesthetics, the total drug mass and the technique of medication infusion can create distinct diffusion gradient pressures that drive the transfer of drugs across the dural conduit or meninges.2,6 When the movement of drug through the dural conduit is significantly faster than the rate of drug diffusion through the meninges, the effect of drug translocation through the dural conduit is clinically relevant.22 And if a drug with a slow transmeningeal transfer rate will greatly benefit from dural puncture.6 Rabbit models suggest that the bupivacaine’s native diffusion through intact meninges is much slower than that of lidocaine.23 Ropivacaine appears to share similar characteristics with bupivacaine on this aspect.6 Thereby, the presence of dural conduit would favor ropivacaine translocation into subarachnoid space. Besides, a lower concentration of ropivacaine exhibits a more pronounced motor-sensory separation block than other local anesthetics.13 So, it seems greatly useful in labor analgesia, given the undesirability of motor blockade. Additionally, dural conduit played a proportionally more important role in transmeningeal medication transfer, when local anesthetics with a low concentration were used.6 This is another possible explanation for the superior analgesic effect observed in the DPE group during the initial 30 minutes in our study.
In our study, the initial dose was given at a higher injection rate (15 mL of 0.1% ropivacaine in 3 minutes) in our study, whereas Tan et al used a slower injection rate (15 mL of 0.1% ropivacaine in 6 minutes). A increased injection rate could result in higher injection pressure and epidural pressure.24 This elevated epidural pressure might lead to a greater enhancement of medication translocation through the dural conduit. Similarly, programmed intermittent epidural bolus (PIEB) involves scheduled intervals of rapid and high-pressure medication injection, it may also increase drug transfer through the dural puncture.2,8 Song et al suggest that employing the DPE plus PIEB technique could achieve superior analgesia quality than the EP/DPE plus continuous infusion technique.11 However, the rapid and higher-pressure injection could also result in wider epidural drug spread in epidural space, possibly masking any analgesic benefits resulting from increased drug transfer through the dural conduit. This could potentially explain the absence of significant difference in the incidence of asymmetric block and the need for additional top-up boluses between two groups in our study.
Consistent with previous studies,2,11,19 no difference was found in the patient satisfaction in our study. And most of women in both groups expressed high satisfaction with the labor analgesia. It is worth noting that, besides the quality of overall labor analgesia, satisfaction may be influenced by many other factors during childbirth, such as maternal decision-making sharing, consciousness of emotional control and maternal expectations.25
Furthermore, no significant differences were observed in the mode of delivery, the incidence of adverse effects (including postpartum headache, pruritus, nausea, hypotension), the occurrence of fetal bradycardia, and Apgar scores at both 1 and 5 minutes. These results align with prior research.2,11,12 And it indicates that while the dural conduit facilitate the medication translocation into the subarachnoid space, this translocation rate seems slow enough, and still insufficient to cause an increase in the complications that were much common in CSE technique.2,19 In other words, both techniques in our study were safety for the mother and the fetus.
Limitations
There are several potential limitations in this study. Firstly, due to the cyclical nature of uterine contractions and the varying frequency of contractions among different parturients, determining the precise onset of adequate labor analgesia is difficult. It is plausible that this onset could transpire prior to our observed timeframe. Additionally, whether a faster epidural injection speed leads to higher epidural pressure and, subsequently, promotes epidural translocation requires further investigation. Thirdly, the factors governing the epidural medication through the meninges are intricate, and the settings of the PIEB pump, such as the programmed dosing interval, also exerts an influence on observed effects. Hence, our findings are specific to utilization of 25G needles for DPE, low concentration of ropivacaine, and administration via PIEB technique with specific pump settings. Further investigation is needed to determine the optimal pump settings in combination with the DPE technique in future studies.
Conclusion
In conclusion, employing the DPE technique with 25G spinal needles appears to enhance the quality of labor analgesia by accelerating onset and providing improved sacral blockade. Comparable results were observed between DPE and EP techniques in terms of side effects, mode of delivery, and maternal satisfaction, when combined with the PIEB technique and low-concentration ropivacaine for initiating and maintaining analgesia in parturients. These findings collectively indicate that the use of the DPE technique for labor analgesia is beneficial.
Data Sharing Statement
Data and other materials are available from the corresponding author on reasonable request within 6 months.
Acknowledgments
We thank all the patients and researchers who participated in this study.
Funding
This project was supported by Startup Fund for Scientific Research of Fujian Medical University (No.2019QH1084).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Rao WY, Xu F, Dai SB, et al. Comparison of dural puncture epidural, epidural and combined spinal-epidural anesthesia for cesarean delivery: a randomized controlled trial. Drug Des Devel Ther. 2023;17:2077–2085. doi:10.2147/DDDT.S415684
2. Tan HS, Reed SE, Mehdiratta JE, et al. Quality of labor analgesia with dural puncture epidural versus standard epidural technique in obese parturients: a double-blind randomized controlled study. Anesthesiology. 2022;136(5):678–687. doi:10.1097/ALN.0000000000004137
3. Sharawi N, Williams M, Athar W, et al. Effect of dural-puncture epidural vs standard epidural for epidural extension on onset time of surgical anesthesia in elective cesarean delivery: a randomized clinical trial. JAMA Network Open. 2023;6(8):e2326710–e2326710. doi:10.1001/jamanetworkopen.2023.26710
4. Punj J, Thangavel K. Dural puncture epidural for labour analgesia in Indian parturients may need dose alteration for maximal benefits! J Anaesthesiol Clin Pharmacol. 2022;38(4):667–669. doi:10.4103/joacp.JOACP_613_20
5. Chau A, Bibbo C, Huang CC, et al. Dural puncture epidural technique improves labor analgesia quality with fewer side effects compared with epidural and combined spinal epidural techniques: a randomized clinical trial. Anesth Analg. 2017;124(2):560–569. doi:10.1213/ANE.0000000000001798
6. Layera S, Bravo D, Aliste J, De QT. A systematic review of DURAL puncture epidural analgesia for labor. J Clin Anesth. 2019;53:5–10. doi:10.1016/j.jclinane.2018.09.030
7. Lin W, Lin J, Yang Y, Lin L, Lin Q. Dural puncture epidural with 25-G spinal needles versus conventional epidural technique for labor analgesia: a systematic review of randomized controlled trials. Technol Health Care. 2023;1–16. doi:10.3233/THC-230059
8. Yin H, Tong X, Huang H. Dural puncture epidural versus conventional epidural analgesia for labor: a systematic review and meta-analysis of randomized controlled studies. J Anesth. 2022;36(3):413–427. doi:10.1007/s00540-022-03061-8
9. Holgado CM, Girones A, Tapia N, Molina-Fernandez MI D, Anez C. Labor outcomes with epidural analgesia: an observational before-and-after cohort study comparing continuous infusion versus programmed intermittent bolus plus patient-controlled analgesia. Minerva Anestesiol. 2020;86(12):1277–1286. doi:10.23736/S0375-9393.20.14516-4
10. Yao HQ, Huang JY, Deng JL, et al. Randomized assessment of the optimal time interval between programmed intermittent epidural boluses when combined with the dural puncture epidural technique for labor analgesia. Anesth Analg. 2023;136(3):532–539. doi:10.1213/ANE.0000000000006201
11. Song Y, Du W, Zhou S, et al. Effect of dural puncture epidural technique combined with programmed intermittent epidural bolus on labor analgesia onset and maintenance: a randomized controlled trial. Anesth Analg. 2021;132(4):971–978. doi:10.1213/ANE.0000000000004768
12. Wang J, Zhang L, Zheng L, et al. A randomized trial of the dural puncture epidural technique combined with programmed intermittent epidural boluses for labor analgesia. Ann Palliat Med. 2021;10(1):404–414. doi:10.21037/apm-20-2281
13. Zheng T, Zheng CY, Yan LP, et al. Comparing the minimum local anesthetic dose of ropivacaine in real-time ultrasound-guided spinal anesthesia and traditional landmark-guided spinal anesthesia: a randomized controlled trial of knee surgery patients. Ann Transl Med. 2021;9(19):1492. doi:10.21037/atm-21-3888
14. Schulz KF, Altman DG, Moher DC Statement: updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010;7(3):e1000251.
15. Leach A, Smith GB. Subarachnoid spread of epidural local anaesthetic following dural puncture. Anaesthesia. 1988;43(8):671–674. doi:10.1111/j.1365-2044.1988.tb04155.x
16. Bernards Christopher M, Kopacz Dan J, Michel Maher Z. Effect of needle puncture on morphine and lidocaine flux through the spinal meninges of the monkey in vitro: implications for combined spinal-epidural anesthesia. Anesthesiology. 1994;80(4):853–858. doi:10.1097/00000542-199404000-00019
17. Nath S, Koziarz A, Badhiwala JH, et al. Atraumatic versus conventional lumbar puncture needles: a systematic review and meta-analysis. Lancet. 2018;391(10126):1197–1204. doi:10.1016/S0140-6736(17)32451-0
18. Contreras F, Morales J, Bravo D, et al. Dural puncture epidural analgesia for labor: a randomized comparison between 25-gauge and 27-gauge pencil point spinal needles. Reg Anesth Pain Med. 2019;44(7):750–753. doi:10.1136/rapm-2019-100608
19. Bakhet WZ. A randomized comparison of epidural, dural puncture epidural, and combined spinal-epidural without intrathecal opioids for labor analgesia. J Anaesthesiol Clin Pharmacol. 2021;37(2):231–236. doi:10.4103/joacp.JOACP_347_19
20. Gupta D, Srirajakalidindi A, Soskin V. Dural puncture epidural analgesia is not superior to continuous labor epidural analgesia. Middle East J Anaesthesiol. 2013;22(3):309–316.
21. Heesen M, Rijs K, Rossaint R, Klimek M. Dural puncture epidural versus conventional epidural block for labor analgesia: a systematic review of randomized controlled trials. Int J Obstet Anesth. 2019;40:24–31. doi:10.1016/j.ijoa.2019.05.007
22. Thomas JA, Pan PH, Harris LC, Owen MD, D’Angelo R. Dural puncture with a 27-gauge Whitacre needle as part of a combined Spinal–Epidural technique does not improve labor epidural catheter function. Anesthesiology. 2005;103(5):1046–1051. doi:10.1097/00000542-200511000-00019
23. Clement R, Malinovsky JM, Le Corre P, Dollo G, Chevanne F, Le Verge R. Cerebrospinal fluid bioavailability and pharmacokinetics of bupivacaine and lidocaine after intrathecal and epidural administrations in rabbits using microdialysis. J Pharmacol Exp Ther. 1999;289(2):1015–1021.
24. W-g S, Jang M, Yoon J, Lee LY, Lee I. The effect of epidural injection speed on epidural pressure and distribution of solution in anesthetized dogs. Vet Anaesth Analg. 2014;41(5):526–533. doi:10.1111/vaa.12147
25. Tzeng I-S, Kao M-C, Pan P-T, et al. A meta-analysis of comparing intermittent epidural boluses and continuous epidural infusion for labor analgesia. Int J Environ Res Public Health. 2020;17(19):7082. doi:10.3390/ijerph17197082
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optimal Programmed Intermittent Epidural Bolus Interval Timing When Using 10 mL of 0.1% Ropivacaine and 0.5 mcg/mL Sufentanil for Labor Analgesia in Patients Without Breakthrough Pain: A Prospective, Randomized Study
Xu DC, Ying J, Zhao J, Chen XD, Deng GP, Zhao YP, Xiao F
Drug Design, Development and Therapy 2024, 18:5563-5571
Published Date: 3 December 2024
EC50 and EC95 of Epidural Ropivacaine for Intraoperative Analgesia During High-Intensity Focused Ultrasound for Adenomyosis: A Prospective Double-Blind Up-and-Down Concentration-Finding Study
Yang S, Zhang Y, Yang F, Luo L
Drug Design, Development and Therapy 2026, 20:594039
Published Date: 12 May 2026