Back to Journals » Journal of Pain Research » Volume 19
Dual-Site Pain in the Low Back and Knee as a Risk Factor for Dementia: A Population-Based Cohort Study
Authors Endo Y ![]() , Kobayashi H
, Kobayashi H ![]() , Watanabe K
, Watanabe K ![]() , Otani K
, Otani K ![]() , Sekiguchi M, Ono R, Konno SI, Matsumoto Y
, Sekiguchi M, Ono R, Konno SI, Matsumoto Y
Received 21 October 2025
Accepted for publication 29 January 2026
Published 3 February 2026 Volume 2026:19 570261
DOI https://doi.org/10.2147/JPR.S570261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Yuji Endo,1,* Hiroshi Kobayashi,1 Kazuyuki Watanabe,1 Koji Otani,1,* Miho Sekiguchi,1 Rei Ono,2 Shin-ichi Konno,1 Yoshihiro Matsumoto1
1Department of Orthopedic Surgery, Fukushima Medical University, Fukushima, Japan; 2Department of Physical Activity Research, National Institute of Biomedical Innovation, Health, and Nutrition (National Institute of Health and Nutrition), Osaka, Japan
*These authors contributed equally to this work
Correspondence: Koji Otani, Department of Orthopedic Surgery, Fukushima Medical University School of Medicine, Fukushima, 960-1295, Japan, Tel +81-24-547-1276, Fax +81-24-548-5505, Email [email protected] Yuji Endo, Department of Orthopedic Surgery, Fukushima Medical University School of Medicine, Fukushima, 960-1295, Japan, Tel +81-24-547-1276, Fax +81-24-548-5505, Email [email protected]
Purpose: Chronic pain is a major public health concern and has been linked to cognitive decline. However, the effect of pain occurring simultaneously in two musculoskeletal sites on dementia risk remains unclear. In this study, we aimed to examine whether dual-site pain (DSP; in this study defined as cooccurring chronic low back and knee pain) is associated with an increased risk of dementia in community-dwelling older adults.
Patients and Methods: We analyzed data from 2060 participants aged ≥ 65 years in the Locomotive Syndrome and Health Outcomes in the Aizu Cohort Study. DSP was defined as the presence of both chronic low back and knee pain lasting > 3 months. Participants without DSP served as the reference group. Incident dementia was identified from long-term care insurance certification records, and Cox proportional hazards models were used to estimate hazard ratios (HRs) adjusting for demographic and vascular risk factors, depressive symptoms, and physical activity.
Results: Over 6 years, 197 participants (9.6%) developed dementia. The incidence was higher in the DSP group (16.5%, 26/158) than in the control group (9.0%, 171/1902). After adjustment, DSP remained significantly associated with dementia (HR = 1.57, 95% CI: 1.02– 2.42).
Conclusion: Dual-site pain involving the low back and knee is a significant risk factor for dementia among older adults. Early identification and management of DSP may help preserve cognitive health, highlighting the need for integrated strategies addressing both musculoskeletal and cognitive well-being.
Keywords: dual-site pain, dementia, epidemiology, cohort study
Introduction
The global population is aging rapidly, with no indications of this trend slowing down.1 With the aging population, the incidence of dementia increases. In 2019, the global economic burden of dementia was estimated at USD 1.3 trillion globally, a figure projected to increase in the coming years.2 Therefore, preventing dementia and extending healthy life expectancy are critical. Although various preventive measures against dementia have been proposed, identifying new insights that can contribute to its prevention remains a primary focus.
Chronic pain is defined as pain that persists for > 3 months and has been reported to accelerate memory loss and increase the risk of dementia.3 Notably, chronic pain affects >30% of the global population, imposing substantial economic and healthcare burdens.4 With an aging society, the prevalence of multisite chronic pain (MCP) is expected to increase further. Consequently, in orthopedic clinics, patients who have cooccurring chronic low back and knee pain are commonly encountered globally.5,6 Recent evidence has suggested an association between musculoskeletal disorders and cognitive function,7–9 suggesting that appropriate treatment may help prevent cognitive decline. However, the mechanisms underlying this association remain unclear. Notably, a Japanese prospective cohort study reported that the coexistence of chronic low back and knee pain was associated with an increased risk of dementia, highlighting the potential importance of pain affecting these two sites.10 However, in that study, pain was not restricted to chronic conditions, and it remains unclear whether persistent dual-site pain confers a higher risk of dementia than single-site pain.
We therefore hypothesized that dual-site pain (DSP; in this study, defined as cooccurring chronic low back and knee pain) may serve as a risk factor for dementia development.11 Accordingly, the present study aimed to evaluate whether DSP increases the risk of dementia in community-dwelling older adults. Understanding the links between musculoskeletal health and neurological disorders could not only inform strategies to alleviate chronic pain but also improve cognitive function, enabling early interventions that enhance the quality of life of older adults.
Materials and Methods
Study Design
This study used data from the Locomotive Syndrome and Health Outcomes in the Aizu Cohort Study (LOHAS), a population-based prospective cohort study investigating the risk factors for cardiovascular disease, quality of life, medical costs, and mortality attributable to locomotor dysfunction. LOHAS also provides epidemiological information required for policymaking regarding locomotor dysfunction detection. Participants in the LOHAS were residents of Minamiaizu and Tadami in Fukushima Prefecture, Japan, who underwent regular health examinations conducted by the municipalities in 2009 and opted for locomotor health examinations. All examinations were performed simultaneously. Details of the study design have been previously described.12 Inclusion criteria were age ≥65 years and completion of a questionnaire on chronic low back and knee pain.
For indicating low back pain, a diagram of the lower back was provided, and participants were asked to indicate if they experienced pain in the illustrated area. The duration of pain was categorized as <1, 1–3, >3 months. No diagram was provided for knee pain; however, the same duration options were used. In both cases, pain lasting >3 months was classified as chronic pain. We excluded participants with missing data, those with dementia at baseline, and those who had passed away or relocated. Additionally, we used data from long-term care insurance certification (LTCI) in Japan to identify participants requiring care. Specifically, this care refers to the support and services provided to individuals certified as needing long-term care, including assistance with daily activities, physical rehabilitation, and other forms of support tailored to their level of care needs.
Previous studies from our group have examined the associations between lumbar spinal stenosis or radiographic knee osteoarthritis and dementia risk within the same regional framework. However, the present analysis is distinct in that it focuses on self-reported dual-site chronic pain in the low back and knee, based on questionnaire data from a different recruitment phase of the LOHAS cohort.7,8
All participants provided written informed consent for the use of their data before participating in the study, which included consent for the future use of administrative data, including LTCI certification data obtained from municipal governments for research purposes. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Research Ethics Committee of the Fukushima Medical University, Japan (approval No. 673). All participants provided written informed consent at enrollment in the Locomotive Syndrome and Health Outcomes in the Aizu Cohort Study (LOHAS), which included permission for the use of their questionnaire data and linkage with relevant administrative health data, such as Long-Term Care Insurance (LTCI) records. Therefore, additional consent to review medical or administrative records was not required by the Research Ethics Committee of Fukushima Medical University. All data were anonymized prior to analysis to ensure participant confidentiality.
Definition of DSP
The DSP group was operationally defined as those who answered “yes” to both “low back pain lasting more than 3 months” and “knee pain lasting more than 3 months” in the questionnaire. Those who did not meet these criteria were categorized into the control group.
Outcome Measures and Definition of Dementia
The primary outcome was the incidence of newly diagnosed dementia identified through the Japanese LTCI system, classified as class II or higher according to the criteria for dementia. Class II dementia is defined as follows:
They can be independent if someone pays attention to them, even if they show some symptoms/behaviors or communication difficulties that interfere with their daily lives.13
This definition has been widely used in previous Japanese epidemiological studies based on LTCI records to identify dementia.14,15 The diagnosis of dementia was based on opinion statements submitted by the attending physicians to the municipality and standardized in-home assessments conducted by trained personnel as part of the LTCI certification process. The date of LTCI certification was used as the date of dementia onset in the survival analyses. Using the official LTCI data, we comprehensively investigated the incidence of dementia in community-dwelling older adults.
Measurement of Confounding Factors
Based on current evidence, we included age, sex, and vascular risk factors, such as diabetes, hypertension, dyslipidemia,16,17 depressive symptoms,18,19 and daily activity.20,21 Diabetes mellitus was defined as a random glucose concentration ≥200 mg/dL, a fasting glucose concentration ≥126 mg/dL, a glycosylated hemoglobin level ≥6.5%, or the use of hypoglycemic medication. Hypertension was defined as systolic blood pressure >130 mmHg, diastolic blood pressure >85 mmHg, or antihypertensive medication use. Dyslipidemia was defined as a fasting blood count of low-density lipoprotein cholesterol level ≥140 mg/dL, high-density lipoprotein cholesterol level <40 mg/dL, triglyceride level ≥150 mg/dL, or use of dyslipidemia medication.
Depressive symptoms were identified using the Center for Epidemiologic Studies Depression Scale (CES-D), which comprises 20 items. The CES-D is a self-reported questionnaire where participants evaluate their mood and behavior over the past week. A score of ≥10 was defined as having depressive symptoms.22
Daily activity was defined as “moderate-intensity walking or exercise at least once a week” based on the rating chart devised by the International Physical Activity Questionnaire (IPAQ).23 Moderate-intensity exercise was defined as exercise accompanied by light sweating (3.0–5.9 metabolic equivalents; METs).24 In the present study, exercise below this level (<3.0 METs) was assessed as a low activity level.
Statistical Analysis
All investigated factors were compared across groups using t-tests and chi-squared tests. Demographic characteristics, main exposure (DSP), and outcomes (dementia development) were described as appropriate indices. The effect measures included p-values from the Log rank test and hazard ratios (HRs) derived from the Cox proportional hazards model adjusted for similar confounders. The proportional hazards assumption of the Cox model was tested using Schoenfeld residuals, and no violations were detected in the global test (p = 0.149).
Statistical analyses were performed using JMP Pro version 16.0.0 (SAS Institute Inc., Cary, NY, USA). A p-value of <0.05 was considered significant.
Sensitivity Analysis
To assess the robustness of the primary findings, we conducted a sensitivity analysis using an alternative exposure definition. Participants were categorized into four groups based on their baseline pain status: pain-free, knee pain only, low back pain only, and DSP. Cox proportional hazards models, adjusted for the same confounders as in the primary analysis, were used to estimate hazard ratios for incident dementia, with the pain-free group serving as the reference category.
Results
Study Participants and Outcome Data
Of the 3790 participants from the LOHAS in 2009, 2514 remained after excluding those with missing data or aged <65 years. Among these, 19 had dementia at baseline, 97 died during the follow-up, and 338 relocated. After these exclusions, a total of 2060 participants were included in the final analysis (Figure 1).
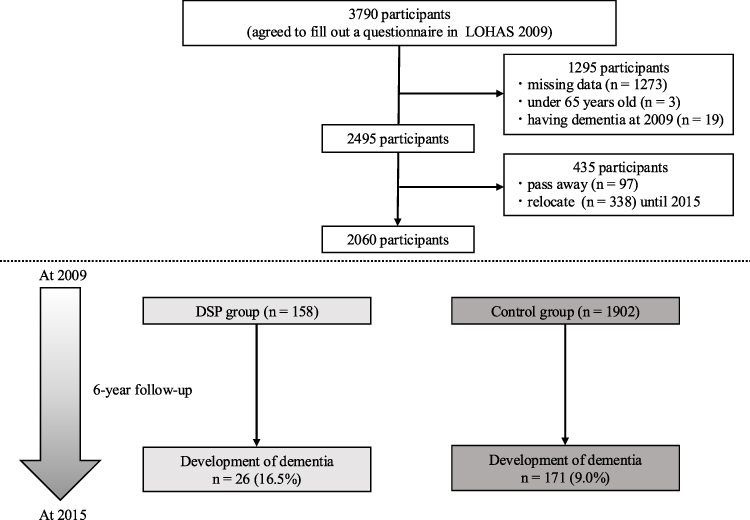 |
Figure 1 Flowchart of participant selection and follow-up. This flowchart illustrates the selection process of the study cohort and follow-up outcomes from 2009 to 2015. It presents the initial number of participants, exclusion criteria (age, pre-existing conditions, death, or relocation), and outcomes. Of the 3790 eligible participants, 2060 were followed up for >6 years, and data on dementia incidence were collected. Abbreviation: LOHAS, Locomotive Syndrome and Health Outcomes in the Aizu Cohort Study. |
Baseline Characteristics of Participants
Table 1 summarizes the baseline characteristics of the participants. The mean age was 72.5 years, and 59.5% were women. The DSP group included 158 participants, whereas the control group included 1902 participants. The DSP group had a significantly higher proportion of women (72.8% vs 58.1%), more individuals with depressive symptoms (18.4% vs 7.8%), and lower levels of daily activity (62.0% vs 50.9%) than those in the control group (p < 0.001).
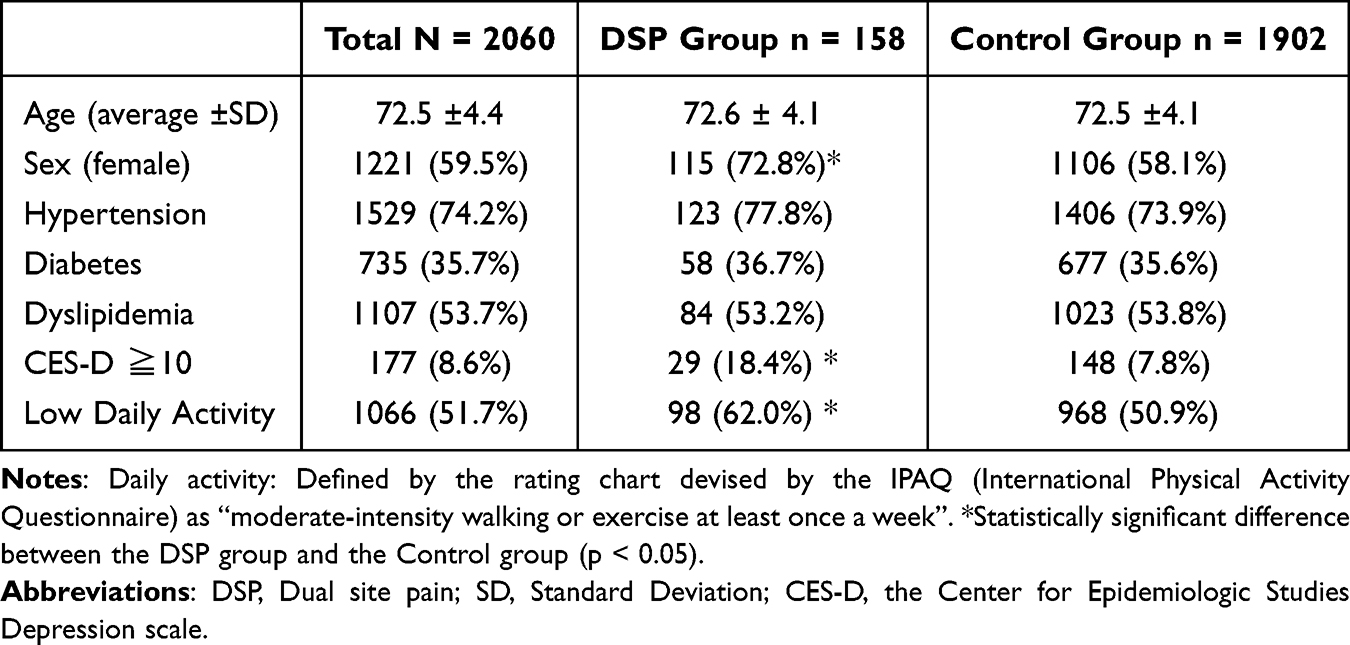 |
Table 1 The Demographic Data of Participants in the DSP Group and Control Group |
Study Outcome: Dementia
All participants were included in the final analysis. Among the 2060 participants, 197 (9.6%) developed dementia in 2015, including 26 (16.5%) and 171 (9.0%) participants in the DSP and control groups, respectively. The DSP group exhibited a significantly higher incidence of newly diagnosed dementia compared with the control group (p < 0.001).
Over the 6-year follow-up period, Kaplan–Meier curves were used to depict the cumulative incidence of dementia development between the two groups. The curve demonstrated significant divergence, as supported by the Log rank test (p < 0.001; Figure 2).
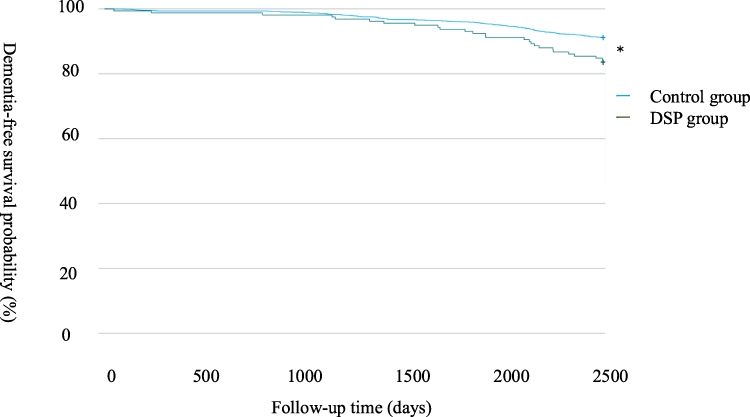 |
Figure 2 Cumulative Incidence of Dementia: Kaplan–Meier Analysis. Kaplan–Meier curves illustrate the cumulative incidence of dementia development between the two groups, exhibiting significant divergence, as evidenced by the Log rank test (p < 0.001). *p < 0.001. Abbreviation: DSP, Dual-site pain. |
Risk Factors for the Development of Dementia
Cox regression analysis indicated a higher rate of dementia development in the DSP group than in the control group after adjusting for confounding factors (HR = 1.57, 95% confidence interval; 1.02–2.42) (Table 2).
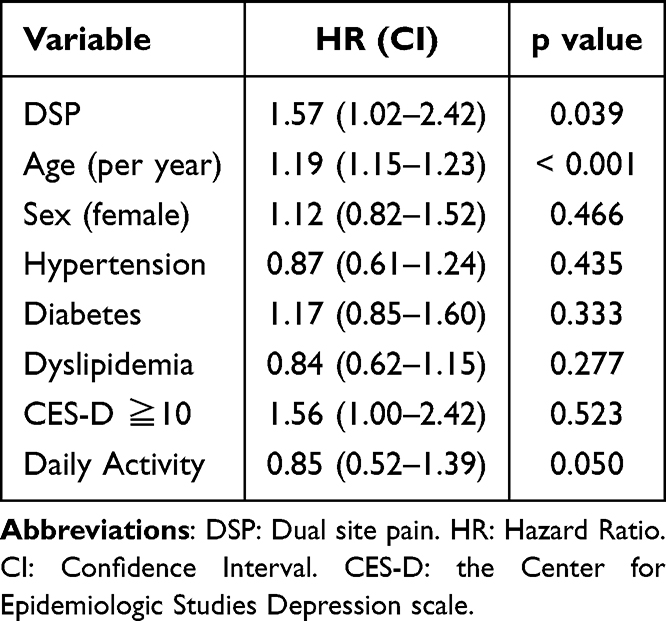 |
Table 2 Association Between DSP and the Development of Dementia Using Cox Proportional Hazards Model |
Pain Status and the Risk of Dementia
In a sensitivity analysis using an alternative four-category pain classification, only participants with DSP showed a significantly higher risk of development of dementia compared with pain-free group, whereas knee pain only and low back pain only were not significantly associated with development of dementia (Table 3).
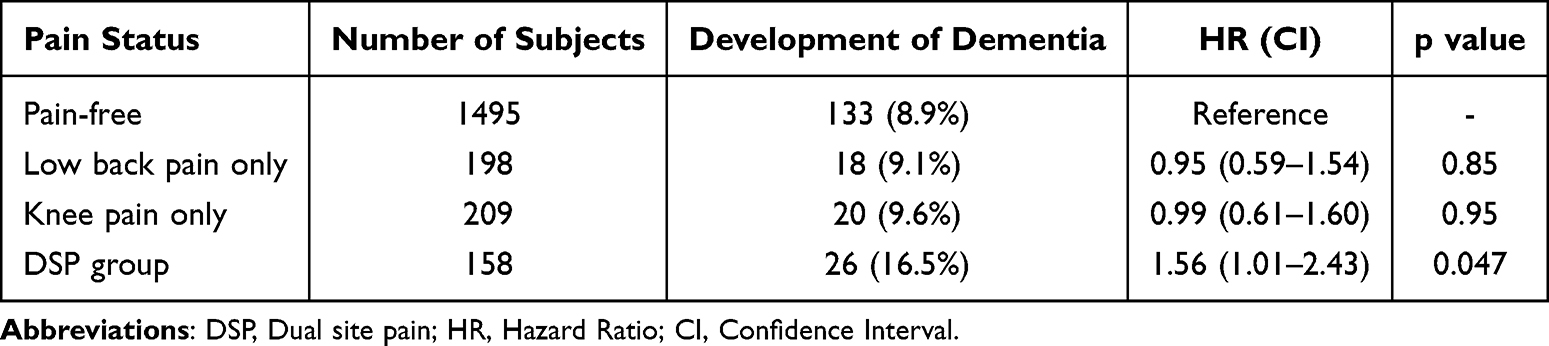 |
Table 3 Sensitivity Analysis of the Association Between Pain Status and the Development of Dementia |
Discussion
This study demonstrated that participants with cooccurring chronic low back and knee pain (DSP) had a significantly higher risk of developing dementia over a 6-year follow-up period, even after adjusting for age, sex, diabetes, hypertension, dyslipidemia, depressive symptoms, and daily activity. These findings highlight DSP as an independent risk factor for dementia in community-dwelling older adults.
Our findings are consistent with previous studies reporting an association between chronic pain at multiple sites and the risk of dementia, demonstrating that dementia risk increases with the number of chronic pain sites, suggesting a cumulative effect of multisite pain on cognitive decline.25 In a Japanese prospective cohort11 also reported that the coexistence of knee pain and low back pain was associated with a higher risk of dementia. Extending these findings, our study showed that DSP involving the low back and knee, but not single-site pain, was independently associated with the development of dementia after comprehensive adjustment for confounding factors.
Several biological pathways may explain the association between DSP and dementia. Central sensitization may promote the transition from localized to more widespread pain, lowering the pain threshold and producing hypersensitivity.26 Chronic pain can also spread to additional body regions through altered gait and biomechanical changes,27–29 which might increase the overall burden of pain and its effect on cognitive function. Chronic pain has additionally been linked to hippocampal atrophy17 and microglial activation, which may induce neuronal apoptosis and contribute to brain atrophy and cognitive decline.3,30 Furthermore, DSP may indirectly increase dementia risk through reduced physical activity and comorbid depression, both of which are well-established risk factors for cognitive impairment.18,21,31
A major strength of this study was the use of a population-based prospective cohort with a 6-year follow-up, allowing for the temporal assessment of pain and dementia onset. However, several limitations should be acknowledged. First, dementia diagnosis was based on opinion forms for long-term care certification rather than internationally standardized diagnostic tools (eg, ICD or DSM), and participants without certification were presumed to be dementia-free. In addition, the date of LTCI certification was used as the date of dementia onset, which may not exactly reflect the true clinical onset and could result in temporal misclassification. Second, the study was limited to rural older adults, and dementia outcomes were identified only among individuals who applied for LTCI certification, which may affect generalizability. Third, we lacked information on pain severity, duration, or treatment during follow-up, and we were unable to capture pain at sites other than the low back and knee. Fourth, although we observed significant differences, the relatively small size of the DSP group may have limited the statistical power. Finally, the “pain-free” category may have included individuals with pain at other sites; therefore, we cannot definitively conclude that single-site pain is unrelated to dementia.
These findings highlight the importance of comprehensive pain management strategies, including physical therapy, psychological support, and routine monitoring of chronic pain, as potential interventions to delay dementia onset. From a research perspective, future studies should incorporate standardized dementia diagnostic tools, detailed pain assessments (including severity and treatment), and resilience factors that may protect against cognitive decline even in individuals with DSP. Larger, more diverse cohorts are warranted to confirm these findings and to further clarify the mechanisms linking musculoskeletal pain and dementia.
Conclusion
This population-based prospective study demonstrated that cooccurring chronic low back and knee pain are significant risk factors for the development of dementia in older adults. These findings suggested that identifying and managing DSP may contribute to delaying dementia onset and improving quality of life in aging populations. Comprehensive pain management strategies, including physical therapy, psychological support, and routine monitoring, should be considered as part of integrated approaches to preserve cognitive health. Future studies using standardized dementia diagnostics, detailed assessment of pain characteristics, and inclusion of other pain sites are warranted to confirm and extend these findings.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available at this time. However, the data can be made available on reasonable request from the corresponding authors.
Acknowledgments
This work was supported by JSPS KAKENHI (Grant Number 19K09578). We also acknowledge the iHOPE Institute for providing laboratory facilities and data access. The authors thank all participants for their cooperation in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Ageing and health. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
2. World Health Organization. Dementia. 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/dementia.
3. Cao S, Fisher DW, Yu T, Dong H. The link between chronic pain and Alzheimer’s disease. J Neuroinflamm. 2019;16:204. doi:10.1186/s12974-019-1608-z
4. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397:2082–8. doi:10.1016/S0140-6736(21)00393-7
5. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;10:1789–1858.
6. Oka Y, Jiroumaru T, Wachi M, Kida N. Prevalence and treatment of chronic musculoskeletal pain focused on service gaps: a comparative analysis by age group and body part. PeerJ. 2024;12:e18389.
7. Endo Y, Kobayashi H, Watanabe K, et al. Radiographic knee osteoarthritis is a risk factor for the development of dementia: locomotive syndrome and health outcomes in the Aizu cohort study. J Clin Med. 2024;13:4956. doi:10.3390/jcm13164956
8. Kobayashi H, Tominaga R, Otani K, et al. Lumbar spinal stenosis is a risk factor for the development of dementia: locomotive syndrome and health outcomes in the Aizu cohort study. Eur Spine J. 2023;32:488–494. doi:10.1007/s00586-022-07318-4
9. Weber A, Mak SH, Berenbaum F, et al. Association between osteoarthritis and increased risk of dementia: a systemic review and meta-analysis. Medicine. 2019;98:e14355.
10. Yamada K, Kubota Y, Tabuchi T, et al. A prospective study of knee pain, low back pain, and risk of dementia: the JAGES project. Sci Rep. 2019;9(1):10690. doi:10.1038/s41598-019-47005-x
11. Berr C, Wancata J, Ritchie K. Prevalence of dementia in the elderly in Europe. Eur Neuropsychopharmacol. 2005;15:463–471. doi:10.1016/j.euroneuro.2005.04.003
12. Otani K, Takegami M, Fukumori N, et al; LOHAS Research Group. Locomotor dysfunction and risk of cardiovascular disease, quality of life, and medical costs: design of the locomotive syndrome and health outcome in Aizu cohort study (LOHAS) and baseline characteristics of the study population. J Orthop Sci. 17;2012:261–271. doi:10.1007/s00776-012-0200-5
13. Campbell JC, Ikegami N. Long-term care insurance comes to Japan. Health Aff. 2000;19:26–39. doi:10.1377/hlthaff.19.3.26
14. Ikeda A, Yamagishi K, Tanigawa T, et al. Cigarette smoking and risk of disabling dementia in a Japanese rural community: a nested case-control study. Cerebrovasc Dis. 2008;25(4):324–331. PMID: 18303251. doi:10.1159/000118377
15. Ihira H, Sawada N, Inoue M, et al. Association between physical activity and risk of disabling dementia in Japan. JAMA Netw Open. 2022;5(3):e224590. PMID: 35348711; PMCID: PMC8965633. doi:10.1001/jamanetworkopen.2022.4590
16. Layne-Stuart CM, Carpenter AL. Chronic pain considerations in patients with cardiovascular disease. Anesthesiol Clin. 2022;40:791–802. doi:10.1016/j.anclin.2022.08.018
17. Zhao W, Zhao L, Chang X, Lu X, Tu Y. Elevated dementia risk, cognitive decline, and hippocampal atrophy in multisite chronic pain. Proc Natl Acad Sci U S A. 2023;120:e2215192120.
18. Bennett S, Thomas AJ. Depression and dementia: cause, consequence or coincidence? Maturitas. 2014;79:184–190. doi:10.1016/j.maturitas.2014.05.009
19. IsHak WW, Wen RY, Naghdechi L, et al. Pain and depression: a systematic review. Harv Rev Psychiatry. 2018;26:352–363. doi:10.1097/HRP.0000000000000198
20. Borisovskaya A, Chmelik E, Karnik A. Exercise and chronic pain. Adv Exp Med Biol. 2020;1228:233–253.
21. Rovio S, Kåreholt I, Helkala EL, et al. Leisure-time physical activity at midlife and the risk of dementia and Alzheimer’s disease. Lancet Neurol. 2005;4:705–711. doi:10.1016/S1474-4422(05)70198-8
22. Lewinsohn PM, Seeley JR, Roberts RE, Allen NB. Center for epidemiologic studies depression scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychol Aging. 1997;12:277–287. doi:10.1037/0882-7974.12.2.277
23. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
24. O’Donovan G, Lee IM, Hamer M, Stamatakis E. Association of “weekend warrior” and other leisure time physical activity patterns with risks for all-cause, cardiovascular disease, and cancer mortality. JAMA Intern Med. 2017;177:335–342. doi:10.1001/jamainternmed.2016.8014
25. Tian J, Jones G, Lin X, et al. Association between chronic pain and risk of incident dementia: findings from a prospective cohort. BMC Med. 2023;21(1):169. doi:10.1186/s12916-023-02875-x
26. Imamura M, Alfieri FM, Filippo TR, Battistella LR. Pressure pain thresholds in patients with chronic nonspecific low back pain. J Back Musculoskelet Rehabil. 2016;29:327–336. doi:10.3233/BMR-150636
27. Coulthard P, Pleuvry BJ, Brewster M, Wilson KL, Macfarlane TV. Gait analysis as an objective measure in a chronic pain model. J Neurosci Methods. 2002;116:197–213. doi:10.1016/S0165-0270(02)00042-0
28. Dananberg HJ. Gait style as an etiology to chronic postural pain. Part I. Functional hallux limitus. J Am Podiatr Med Assoc. 1993;83:433–441. doi:10.7547/87507315-83-8-433
29. Ogawa EF, Shi L, Bean JF, et al. Chronic pain characteristics and gait in older adults: the MOBILIZE boston study II. Arch Phys Med Rehabil. 2020;101:418–425. doi:10.1016/j.apmr.2019.09.010
30. Whitlock EL, Diaz-Ramirez LG, Glymour MM, et al. Association between persistent pain and memory decline and dementia in a longitudinal cohort of elders. JAMA Intern Med. 2017;177(8):1146–1153. doi:10.1001/jamainternmed.2017.1622
31. Bryant LL, Grigsby J, Swenson C, Scarbro S, Baxter J. Chronic pain increases the risk of decreasing physical performance in older adults: the San Luis Valley health and aging study. J Gerontol a Biol Sci Med Sci. 2007;62:989–996. doi:10.1093/gerona/62.9.989
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Non-Traumatic Subdural Hematoma and Cancer: A Cohort Study
Okholm SH, Nagy D, Körmendiné Farkas D, Fuglsang CH, Troelsen FS, Henderson VW, Sørensen HT
Clinical Epidemiology 2023, 15:629-633
Published Date: 8 May 2023
Ibuprofen for Acute Pericarditis and Associated Cardiovascular Risks: A Danish Nationwide, Population-Based Cohort Study
Eika JK, Bonnesen K, Pedersen L, Ehrenstein V, Sørensen HT, Schmidt M
Clinical Epidemiology 2024, 16:793-802
Published Date: 14 November 2024
Chronic Back Pain Increases Alzheimer’s Disease Risk Independent of Gross Brain Structural Alterations: Genetic Evidence from Two Populations
Huang FF, Sun Y, Hu Y, Chang JR, Zhou Z, Zheng DKY, Hsu CL, Samartzis D, Karppinen J, Al Zoubi FM, Fu SN, Wong AYL
Journal of Pain Research 2026, 19:591448
Published Date: 5 June 2026