Back to Journals » Clinical Ophthalmology » Volume 17
Dry Eye Disease as a Cause of Refractive Errors After Cataract Surgery – A Systematic Review
Authors Biela K ![]() , Winiarczyk M, Borowicz D, Mackiewicz J
, Winiarczyk M, Borowicz D, Mackiewicz J
Received 31 January 2023
Accepted for publication 1 May 2023
Published 6 June 2023 Volume 2023:17 Pages 1629—1638
DOI https://doi.org/10.2147/OPTH.S406530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Katarzyna Biela,1,2,* Mateusz Winiarczyk,1,* Dorota Borowicz,2,* Jerzy Mackiewicz1,*
1Department of Vitreoretinal Surgery, Medical University of Lublin, Lublin, 20079, Poland; 2Department of Ophthalmology, Provincial Hospital in Zamosc, al. John Paul II 10, Zamosc, 22400, Poland
*These authors contributed equally to this work
Correspondence: Katarzyna Biela, Provincial Hospital in Zamosc, al. John Paul II 10, Zamosc, 22400, Poland, Email [email protected]
Abstract: Dry eye disease (DED) is a multifactorial ocular surface disorder characterized by loss of tear film homeostasis with associated ocular symptoms, like dryness, foreign body sensation, and inflammation. Numerous reports confirm an increase in dry eye symptoms after cataract surgery. DED also significantly disturbs preoperative biometric measurements, mainly by changes in keratometry measurements. The purpose of this study is to evaluate the effect of DED on biometric measurements before cataract surgery and postoperative refractive errors. PubMed database was searched for keywords: cataract surgery, dry eye disease, refractive error, refractive outcomes, keratometry, and biometry. Four clinical studies evaluating the effect of DED on refractive errors were included. In all studies, biometry was performed before and after dry eye treatment, and the mean absolute error was compared. Various substances have been used to treat dry eye, such as cyclosporin A, liftitegrast, and loteprednol. The refractive error was significantly lower after treatment in all studies. The results unanimously indicate that refractive errors can be reduced by proper treatment of DED before cataract surgery.
Keywords: dry eye disease, cataract surgery, refractive error, refractive outcome, biometry
Introduction
Cataract removal surgery is one of the most commonly performed eye surgeries.1,2 It is estimated that 7 million such procedures are performed per year in Europe and 20 million worldwide.3 Competition between centers and increasingly higher patient expectations cause the need to optimize this procedure and systematically reduce the refractive error rate. A significant postoperative refractive error is defined as the difference between the expected and actual spherical equivalent of postoperative refraction above 1.0 D.4
A non-contact optical biometry remains the gold standard for measuring intraocular lens power before cataract surgery.5 One of the most important parameters in calculating lens power is keratometry. Errors in keratometric measurements are responsible for about 10% of refractive errors after cataract surgery.6 One of the most prominent causes of incorrect outcome is ocular surface disorders (OSD), including dry eye disease (DED).
Dry eye disease, as defined by Tear Film and Ocular Surface Society Dry Eye Workshop II (TFOS DEWS II), is
a multifactorial ocular surface disease characterized by loss of tear film homeostasis with associated ocular symptoms, in the etiology of which factors such as tear film instability and hyperosmolarity, inflammation and damage to ocular surface structures, and neurosensory abnormalities play an important role.7
The prevalence of the condition is 5–42%, according to various studies, with up to 50% of the population likely to have subjective symptoms.8–10 The condition belongs to the spectrum of OSD. Age is one of the main risk factors for DED. In the Beaver Dam Offspring Study (BOSS), dry eye symptoms were reported in 5–30% of the elderly, and the prevalence of dry eye was 8.4% in patients younger than 60, 15% in people aged 70 to 79, and 20% in patients older than 80.11 In the elderly, the main cause of DED is loss of Meibom’s glands and inflammation of the ocular surface. These features may be related to common triggers of DED in the elderly, such as systemic inflammatory diseases, glaucoma, and topical or systemic drug use.12 Age is also one of the most important risk factors for developing cataracts. Cataracts are the leading cause of blindness in people aged 50 and older in 2020 (15.2 million cases worldwide).13
It is known that intraocular surgery can aggravate the symptoms of DED.14,15 There are fewer data on the effect of ocular surface disorders on the accuracy of preoperative biometric measurements and the refractive effect of surgery. The purpose of this study is to evaluate the relationship between DED and refractive errors after cataract surgery.
Methodology
A PubMed database was searched using the keywords: cataract surgery, dry eye disease, and interchangeably: refractive error, refractive outcome, keratometry, and biometry. Eighty-seven records were obtained. Duplicate articles −17 - were rejected. Sixty titles of papers were analyzed, 21 of which dealt with issues unrelated to the topic of this work (for example, evaluation of diagnostic equipment and assessment of the epidemiology of certain OSD). Of the remaining 39 publications, another 27 were rejected – they concerned refractive surgery or the effect of cataract surgery on the development of dry eye. The remaining 12 full-text articles were analyzed. They described the impact of dry eye on cataract surgery. The review included original papers that evaluated the impact of dry eye disease and its treatment on the final refractive outcome after cataract surgery. The points evaluated were keratometry and biometry before and after treatment, and refractive outcome after cataract surgery. Publications that evaluated only the effect of dry eye and treatment on keratometry and biometry scores, without a final refractive effect evaluation, were rejected. Four publications meeting the criteria were included in the review.
Results
The four analyzed publications are based on a similar methodology.16–19 Patients undergoing cataract surgery were diagnosed with DED and appropriate treatment was ordered afterwards. Biometric measurements were taken twice – before and after treatment.16,17,19 In one case, biometry was performed only after treatment, and the results were compared with the control group, which applied only to usual artificial tear.18 Treatment included eyelid margin hygiene, artificial tears, and adjunctive substances, which varied in each study – dexamethasone 0.1% 3 times a day for 2 weeks, and in the absence of improvement cyclosporin A twice a day for 6 months,16 cyclosporin A 0.09% twice a day for 28 days,17 loteprednol 0.5% 4 times a day in combination with cyclosporin A 0.05% twice a day for 14 days18 or lifitegrast 5% for 28 days.19 The refractive outcome 1 month after treatment was determined. The measurement before and after treatment was compared 1 month after surgery for the predicted and actual refractive error.
The preoperative diagnosis of DED was based on various criteria, including the tear breakup time (TBUT) ≤10 second and staining of the ocular surface in all of these studies. In addition, the Ocular Surface Disease Index (OSDI),16 The Standardize Patient Evaluation of Eye Disease (SPEED),17,19 Schirmer test,16,18 and conjunctival hyperemia17,19 were used.
A total of 304 subjects participated in the studies, of which 35 dropped out. The effect of dry eye therapy on refractive outcome was studied in a group of 217 subjects, while 52 subjects were the control group in one of the studies. All patients studied met the eligibility criteria for their respective studies. In the study assessing the effect of dexamethasone, 24 patients were included, 7 of whom required additional cyclosporine therapy. Seventeen patients were included in the results, with a mean age of 54.7 ± 3.6 years. Seventy-five patients were enrolled in the study with cyclosporine 0.09%, outcomes in 64 were evaluated, and the mean age was 70.5 ± 7.4. The effect of loteprednol in combination with cyclosporin A was evaluated in 53 patients, with a mean age of 67.9 ± 11.8. The effect of liftitegrast was evaluated in 83 patients, with a mean age of 71.3 ± 11.6. Demographics in the study groups are shown in Table 1.
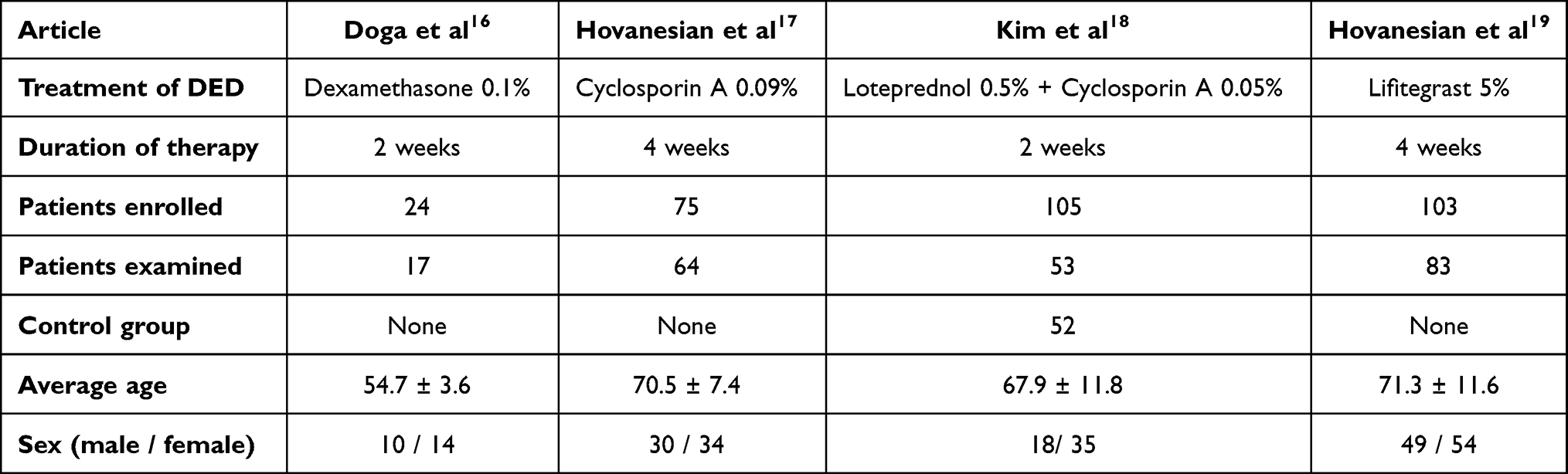 |
Table 1 Baseline Characteristics for Enrolled Patients in Trials Evaluating Dry Eye Treatment on Refractive Errors |
All analyzed studies showed a reduction in refractive errors in the eyes after treatment of DED compared to the biometric examination performed before treatment. A postoperative refractive examination was performed 1 month after treatment. Regardless of the substance used, all studies achieved satisfactory refractive error rates of ± 0.75 or ± 1.0 in treated patients. Mean absolute error was also significantly lower after treatment, but the lack of analysis of this value in one of the publications is noteworthy. Nevertheless, it can be concluded that treatment of dry eye before surgery improves refractive outcomes after cataract surgery. A summary of the results is shown in Table 2.
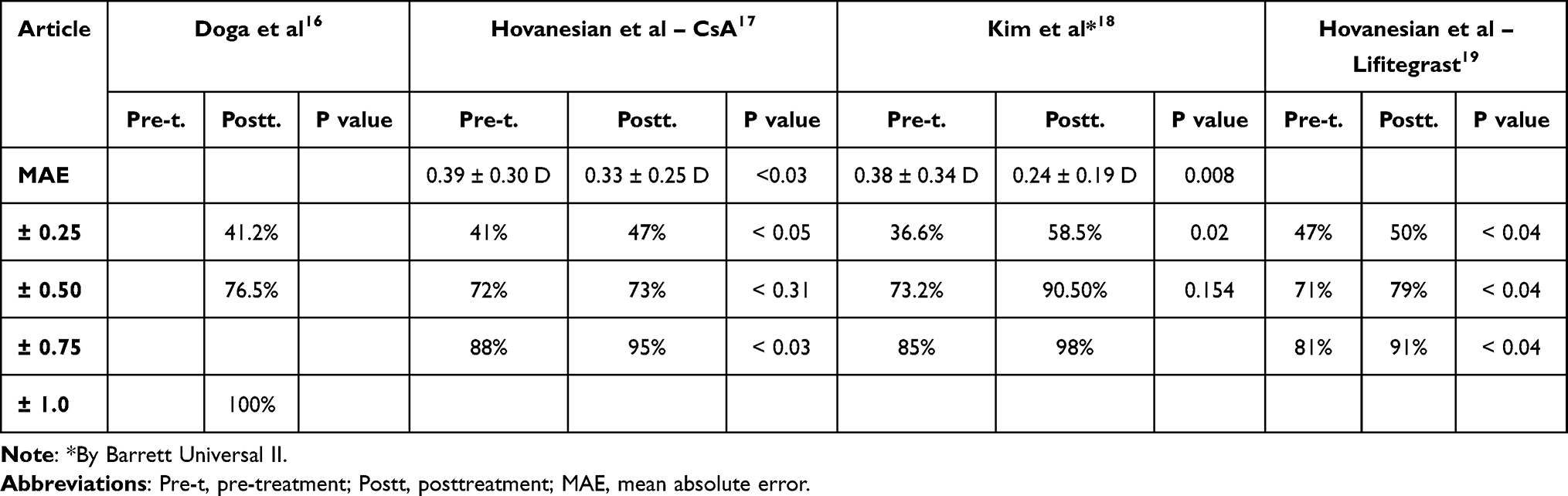 |
Table 2 Effect of Dry Eye Treatment on Refractive Errors After Cataract Surgery |
Discussion
Dry Eye Disease - Definition
A definition of dry eye disease was proposed by TFOS DEWS II in 2017. According to its guidelines,
Dry eye is a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.7
Due to the pathophysiology of the changes leading to dry eye, we can divide this disease into three types: aqueous deficient dry eye (ADDE), evaporative dry eye (EDE), and mixed form.7 However, recent studies suggest that in most cases these subtypes coexist or occur as a continuum.7,20
This multifactoriality of the condition and the multitude of possible symptoms contribute to a complex diagnostic scheme based on numerous tests.
Diagnosis of Dry Eye Disease
There are many available tests to determine both signs and symptoms of DED. Clinical evaluation is often not objective. A significant role in the diagnostic process is attributed to patient-reported signs, often with poor correlation to symptoms.21 In clinical practice, the preferred diagnostic tools are patient history, TBUT, and fluorescein and lissamine green staining, with none of the above-mentioned tests being clearly preferred by ophthalmologists as the only choice in the diagnosis of dry eye.22 However, TFOS DEWS II proposed diagnostic patterns solve the problem of selecting optimal testing methods. It includes a questionnaire, such as OSDI, homeostatic marker tests, including TBUT, osmolarity and staining, and additional diagnostic tests to identify a subtype of the disease.23 The Asia Dry Eye Society recommends a simplified diagnosis based on symptoms assessed by one of the available questionnaires and unstable tear film, expressed as TBUT reduced under 5 s.24
Various criteria for the diagnosis of DED were considered in the reviewed publications. The methodology is shown in Table 3. The most popular diagnostic tests are TBUT and corneal staining, used in all the analyzed publications. A frequently used test is the Schirmer test, recommended by TFOS DEWS to classify the aqueous deficient dry eye.23 It is well recognized that it gives variable results and should not be used as the sole criterion for diagnosing dry eye.25 It is worth emphasizing that non-invasive tear film measurements, mainly OCT use, are strongly recommended in TFOS DEWS II DED diagnostic report.23 The lack of use of newer diagnostic methods, such as tear osmolarity or metalloproteinase 9 (MMP-9) levels, is surprising. These are the only biomarkers approved by the FDA that can be measured with simple bedside tests.21 The use of newer research methods could have a significant impact on the results.
 |
Table 3 Diagnostic Tests for Dry Eye Disease |
Dry Eye Disease in Patients Undergoing Cataract Surgery
DED remains an underestimated problem in the population of patients undergoing cataract surgery. There are many reports of dry eye as a consequence of refractive surgery, and the problem is being considered more frequently in this context.26–28 The preoperative presence of DED increases the risk of infection after surgery and surgical complications during these procedures.20
There are no consistent data on the incidence of DED in patients undergoing cataract surgery. The prevalence in the population is about 5–42%.8–10 Due to the age of patients, these values appear to be underestimated and cannot be directly related to the group of patients with cataract.
Gupta et al evaluated the prevalence of DED in a population of patients undergoing cataract surgery. The mean patient age at the time of cataract evaluation was 69.5 years ± 8.4 (SD) (range 44 to 91 years). Of the 120 patients, 52 (43.3%) had a known ocular surface disorder before qualifying for surgery. The study group had a history (OSDI or SANDE form) and tear tests – osmolarity and MMP-9. Fifty-four (54.0%) of the 100 patients reported symptoms suggestive of ocular surface dysfunction. In the asymptomatic group of 46 patients, 39 (85%) had at least 1 abnormal tear test result (osmolarity or MMP-9), and 22 (48%) had both tests abnormal. Overall, 96 (80%) of the 120 patients had at least 1 abnormal tear test result suggestive of ocular surface dysfunction, and 48 patients (40%) had 2 abnormal results.29
The PHACO study, conducted by Trattler et al, included 143 patients who were evaluated using the OSDI questionnaire, TBUT, corneal and conjunctival staining, and Schirmer test with anesthesia. The mean age of the patients was 70.7±7.8 years (range: 54.5–87.9 years). A total of 22% of the patients had a diagnosis of DED before qualification. Overall, 80% of all patients had TBUT shortened <7s (62.9% ≤5s), 50% showed positive central corneal staining (76.8% staining at all) 21.3% had Schirmer test ≤5mm, 46.6% ≤10mm).30
Thus, it can be suspected that most cataract patients have tear film disorders, even if the patient does not report subjective symptoms. The effect of ocular surface disease can be not only exacerbated postoperative symptoms and reduced quality of vision but also errors in patient preparation and intraocular lens selection. Intraocular lens (IOL) calculations, toric IOL axis and magnitude estimates, keratometry, and topography measurements can be disturbed.31 This is particularly important in the choice of multifocal and toric lenses.32
Recent publications emphasize the importance of properly diagnosing and treating ocular surface disorders before cataract surgery.14,31,32 These reports are already reflected in the guidelines of American Society of Cataract and Refractive Surgery (ASCRS) and American Academy of Ophthalmology (AAO). The AAO points out the need of external examination (eyelids, lashes, lacrimal apparatus, and orbit) and assessment of tear function before cataract surgery, especially in older patients.33 However, tear function testing is considered only as an additional test in these guidelines.33
In 2019, ASCRS published its own recommendation for the preoperative diagnosis of DED in patients undergoing refractive surgery.34 A preoperative visit is scheduled for a minimum of 2 weeks before surgery. Following non-invasive refractive measurements (including keratometry and optical biometry), the authors suggest screening for signs and symptoms based on the ASCRS SPEED II form, as well as assessing tear osmolarity and MMP-9 levels. If abnormalities are found, additional non-invasive tests for OSD are suggested. After a clinical slit-lamp examination, OSD can be ruled out or confirmed. In the case of visually significant OSD, surgery should be postponed, appropriate treatment should be implemented, and another evaluation should be performed after 2–4 weeks.34
Biometry and Its Role in Surgery Planning
The primary test in the preoperative preparation of a cataract patient is biometry with determination of IOL power. Given the increasingly high expectations of patients and surgeons, this moment seems critical to the entire course of surgery. A satisfactory refractive outcome is above 60% of patients with postoperative refraction within ±0.5 D and above 90% within ± 1.0D.5
Studies show that also in patients with DED, a good visual outcome is possible. In a group of 668 patients with this condition, after preoperative preparation of the ocular surface, the overall median best corrected visual acuity (BCVA) improved from 20/250 pre-operatively to 20/25 at 6 weeks post-operatively (p < 0.0001). Low vision (≤20/80) was seen in 61 (9.13%) eyes, all of which were related to keratopathy.35
The gold standard is optical coherence biometry. In the studies presented here, the IOL Master-500 or IOL Master-700 were used to calculate lens power. IOL Master-500 is a partial coherence interferometer (PCI) with a built-in automatic keratometer for measuring the flat and steep corneal meridian. The principle of working is to evaluate six peripheral measuring points, spaced hexagonally over a radius of about 2.5 mm, on the central surface of the cornea.36 Light falling on the cornea is reflected at the air/tear film interface.37 Measurement of corneal curvature is possible due to separation of images obtained by measuring cameras.38 IOL Master 700 uses OCT technology. The condition for correct measurement with the IOL Master is therefore a stable tear film. An error of 1.0 D in preoperative keratometry results in an error of 1.0 D in postoperative refraction.39
The repeatability of measuring keratometry in eyes with DED is limited. Hiraoka et al evaluated the accuracy of biometric measurements by performing this procedure twice on the same day. The repeatability of corneal steep meridian measurements was significantly worse in eyes with DED than in eyes without DED (p=0.044). Moreover, the repeatability of measurements of both keratometry and axial length (AL) of the eye was negatively correlated with TBUT with fluorescein. No such correlations were found for abnormal corneal staining or subjective symptoms reported by the patient.40
A correct keratometric reading is essential for correct calculation of IOL. In patients with DED, due to tear film instability and lack of repeatability between measurements, differences in calculated IOL powers can be significant. In studies comparing patients with normal and hyperosmolar tear films, the percentage of IOL differences above 0.5D was significantly higher in the hyperosmolar group, with a maximum difference of 5.5D.39 These studies demonstrate the importance of preoperative preparation of the ocular surface.
Attention should be focused on the order of testing during qualification for the surgery. Administration of eye drops for up to 5 min before keratometry significantly interferes with its result.36 ASCRS guidelines are more restrictive, suggesting withholding any drops for 2 hr before measurements.34 Disorders that significantly interfere with refractive measurements are primarily, in addition to DED, anterior basement membrane disease (ABMD), pterygium, and Salzmann nodules.41 These patients may require several visits before surgery, and the priority for them becomes stabilizing the ocular surface before repeat measurements are taken.32
Refractive Errors - Definitions and Approaches to Reduction
An objective presentation of the achieved results is possible by defining refractive errors. We distinguish the refraction prediction error (RPE), otherwise known as mean error (ME), and its derivatives: mean absolute error (MAE) and median absolute error (MedAE).
The RPE is the difference between the measured and predicted postoperative refractive spherical equivalent.42 Postoperative measurement is usually done 1 month after surgery.43 ME is the averaged RPE.44 Absolute prediction error (APE) means the absolute value of the RPE. MAE is defined as the mean APE, while MedAE is the median APE.44 The percentage of eyes in the error range of 0.25 D, 0.5 D, 0.75 D, and 1.0 D is also an important parameter. With modern optical biometry for the majority of patients, informed formula choice and IOL constant optimization outcomes of more than 90% within ±1.0 D and more than 60% within ± 0.5 D of target are achievable.5
In the studies presented here, the final refractive effect was mainly evaluated based on the percentage of eyes in the refractive error range of ±0.25, ±0.5, ±0.75 and ±1.0 (Table 2). However, it is difficult to refer to all the results obtained. Doga et al only reported the final values in these ranges. Both reference to the control group and statistical analysis are missing. Despite obtaining 76.5% in the ± 0.5D range and 100% in the ± 1.0D range, it is difficult to assess the effect of the drops they used before repeated biometry. They declared a mean difference in calculated IOL power of 0.87 ± 0.11 D and a maximum error of 2.25 D.
Other papers evaluate the refractive effect by comparing MAE results with the percentage of eyes in each refractive error range. The post-treatment result was compared with a control group or with measurements based on biometry performed before treatment in the same patient. As can be seen in Table 2, for all proposed therapies (cyclosporin A 0.09%, lotperednol 0.5%, and cyclosporin A 0.05%, lifitegrast 5%), significantly higher results were achieved in the ±0.25 D post-treatment range. All authors achieved >90% post-treatment for the ± 0.75D interval, but the Kim et al paper lacks information on significance. They used the parameter of refractive surprise, defined as MAE ≥ 0.75D, also obtaining statistically significant differences in favor of the treated group (3.8% vs 17.3% for SRK/T, p=0.024; 1.9% vs 15.3% for Barrett Universal II, p=0.016).
In interpreting refractive results, the methodology used by the authors is extremely important. In 2021, Hoffer and Savini proposed guidelines for research protocols for calculating the power of implantable intraocular lenses. The most important assumptions are shown in Table 4. The averaged parameter for comparing different methods is the IOL Formula Performance Index, considering standard deviation of Prediction Error (SD of PE), MedAE, AL Bias (the slope of the correlation between PE and AL), and percentage coefficient (the inverse of the percentage of eyes with a PE within ±0.50 D). These guidelines mainly apply to studies of newer formulas but can be used in all postoperative refractive studies.45
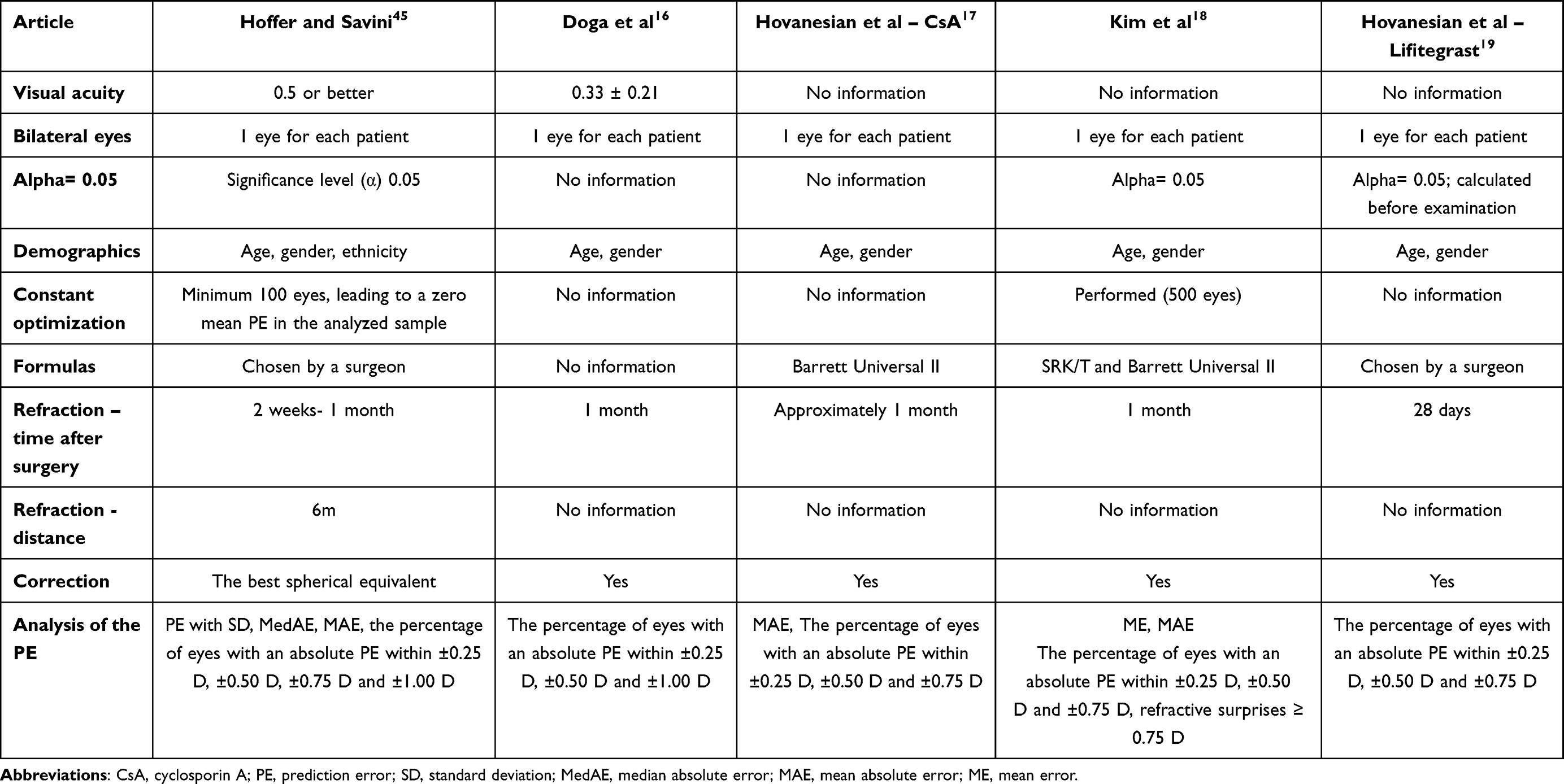 |
Table 4 Proposed Standardized Methodology in Postoperative Refractive Studies According to Hoffer and Savini |
Table 4 also shows the methodological assumptions of the analyzed studies compared to the scheme proposed by Hoffer and Savini. Notable is the lack of information on visual acuity before cataract surgery and the ethnicity of the study group. Kim et al are the only ones to write about performing a constant optimization before the actual study to eliminate the systematic error associated with an incorrect constant. The postoperative refraction examination in all cases was performed 1 month after surgery, which is in line with Hoffer and Savini, but there is no information on the distance of the examination. It is worth remembering that the incorrect method of postoperative refraction examination is responsible for up to 27% of the postoperative errors.6 Importantly, the failure to meet some of the assumptions of the refraction study must not disqualify the results obtained – Hoffer and Savini’s work is still only a proposal to standardize the methodology. More importantly, some of the presented work was written earlier than the mentioned guidelines.
Preoperative Treatment of Dry Eye Disease
As mentioned before, many variables can lead to refractive surprises after cataract surgery, including errors in biometry.46 To prevent these iatrogenic errors, all preoperative examinations should be performed by qualified technicians before placement of ophthalmic drops.41 Patients with DED may nevertheless experience errors in biometry. The aim of identifying and treating DED before cataract surgery is to obtain the most accurate measurements to ensure an optimal refractive outcome.32 Treatment is expected to primarily reduce inflammation, stabilize the tear film and alleviate symptoms prior to ophthalmic surgery.20
A variety of DED treatment options are available, such as nonprescription drops and ointments, anti-inflammatory medications or surgical procedures.32 The TFOS DEWS II algorithm involves the gradual addition of increasingly advanced treatments.47 The Asia Dry Eye Society proposes a strategy called tear film-oriented therapy, which targets the type of dry eye the patient has.31 However, in patients before cataract surgery, it is difficult to afford graded treatment and long-term follow-up. Therefore, ASCRS proposes starting treatment at a more advanced level, at least in Step 2 of the TFOS DEWS II treatment guidelines.34
All the analyzed drugs – topical corticosteroids, cyclosporin A, and liftitegrast – are proposed therapeutic options by both TFOS DEWS II and ASCRS. As mentioned before, an improved refractive effect has been demonstrated for each of these substances (Table 2). Available sources do not clearly indicate which of these drugs achieves the best results, and they are listed as equivalent options. It seems that the decision to choose a drug should be based on the results of the study and the severity of the individual patient’s disease, however treatment with cyclosporine A should last 4 to 8 weeks due to its delayed effect.
It is also worth mentioning the treatment of meibomian gland dysfunction (MGD). In addition to standard therapy with warm compresses, treatment with a thermal pulsation system (TPS) may be considered. In the study by Matossian et al, 52% of patients showed higher astigmatism after TPS, and 28% had a change in the astigmatism axis. Overall, 40% of patients required a change in therapeutic plan due to significant astigmatism on reexamination. The consideration of post-TPS measurements appears to improve the accuracy of keratometric readings and reduce refractive errors.48 However, further research is needed to optimize MGD treatment prior to cataract surgery.
Conclusion
In conclusion, DED is a significant problem in patients before cataract surgery. Adequate diagnosis and preparation of the ocular surface before biometric measurements can reduce the rate of refractive surprises after surgery. Further research is needed to optimize the treatment of DED in the preoperative period.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang W, Yan W, Müller A, He M. A global view on output and outcomes of cataract surgery with national indices of socioeconomic development. Invest Ophthalmol Vis Sci. 2017;58(9):3669–3676. doi:10.1167/iovs.17-21489
2. McCormick I, Butcher R, Evans JR, et al. Effective cataract surgical coverage in adults aged 50 years and older: estimates from population-based surveys in 55 countries. Lancet Glob Health. 2022;1(1). doi:10.1016/S2214-109X(22)00419-3
3. Rossi T, Romano MR, Iannetta D, et al. Cataract surgery practice patterns worldwide: a survey. BMJ Open Ophthalmol. 2021;6(1):e000464. doi:10.1136/bmjophth-2020-000464
4. Lundström M, Dickman M, Henry Y, et al. Risk factors for refractive error after cataract surgery: analysis of 282 811 cataract extractions reported to the European Registry of Quality Outcomes for cataract and refractive surgery. J Cataract Refract Surg. 2018;44(4):447–452. doi:10.1016/j.jcrs.2018.01.031
5. Sheard R. Optimising biometry for best outcomes in cataract surgery. Eye Lond Engl. 2014;28(2):118–125. doi:10.1038/eye.2013.248
6. Norrby S. Sources of error in intraocular lens power calculation. J Cataract Refract Surg. 2008;34(3):368–376. doi:10.1016/j.jcrs.2007.10.031
7. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
8. Marculino LGC, Hazarbassanov RM, Hazarbassanov NGT, et al. Prevalence and risk factors for dry eye disease: the Sao Paulo dry eye study. Arq Bras Oftalmol. 2022;85(6):549–557. doi:10.5935/0004-2749.202200100
9. Akowuah PK, Kobia-Acquah E. Prevalence of dry eye disease in Africa: a systematic review and meta-analysis. Optom Vis Sci off Publ Am Acad Optom. 2020;97(12):1089–1098. doi:10.1097/OPX.0000000000001610
10. Song P, Xia W, Wang M, et al. Variations of dry eye disease prevalence by age, sex and geographic characteristics in China: a systematic review and meta-analysis. J Glob Health. 2018;8(2):020503. doi:10.7189/jogh.08.020503
11. Paulsen AJ, Cruickshanks KJ, Fischer ME, et al. Dry eye in the Beaver dam offspring study: prevalence, risk factors, and health-related quality of life. Am J Ophthalmol. 2014;157(4):799–806. doi:10.1016/j.ajo.2013.12.023
12. Barabino S. Is dry eye disease the same in young and old patients? A narrative review of the literature. BMC Ophthalmol. 2022;22(1):85. doi:10.1186/s12886-022-02269-2
13. Steinmetz JD, Bourne RR, Briant PS, et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021;9(2). doi:10.1016/S2214-109X(20)30489-7
14. Naderi K, Gormley J, O’Brart D. Cataract surgery and dry eye disease: a review. Eur J Ophthalmol. 2020;30(5):840–855. doi:10.1177/1120672120929958
15. Toda I. Dry Eye After LASIK. Invest Ophthalmol Vis Sci. 2018;59(14):DES109–DES115. doi:10.1167/iovs.17-23538
16. Doga AV, Maychuk NV, Mushkova IA, Shamsetdinova LT. Prichiny, profilaktika i korrektsiia refraktsionnykh narusheniĭ posle fakoémul'sifikatsii s implantatsieĭ intraokuliarnykh linz [Causes, prevention and correction of refractive errors after phacoemulsification with intraocular lens implantation]. Vestn Oftalmol. 2019;135(6):83–90. Russian. doi:10.17116/oftalma201913506183
17. Hovanesian JA, Berdy GJ, Epitropoulos A, Holladay JT. Effect of cyclosporine 0.09% treatment on accuracy of preoperative biometry and higher order aberrations in dry eye patients undergoing cataract surgery. Clin Ophthalmol Auckl NZ. 2021;15:3679–3686. doi:10.2147/OPTH.S325659
18. Kim J, Kim MK, Ha Y, Paik HJ, Kim DH. Improved accuracy of intraocular lens power calculation by preoperative management of dry eye disease. BMC Ophthalmol. 2021;21:364. doi:10.1186/s12886-021-02129-5
19. Hovanesian J, Epitropoulos A, Donnenfeld ED, Holladay JT. The Effect of lifitegrast on refractive accuracy and symptoms in dry eye patients undergoing cataract surgery. Clin Ophthalmol Auckl NZ. 2020;14:2709–2716. doi:10.2147/OPTH.S264520
20. Schechter B, Mah F. Optimization of the ocular surface through treatment of ocular surface disease before ophthalmic surgery: a narrative review. Ophthalmol Ther. 2022;11(3):1001–1015. doi:10.1007/s40123-022-00505-y
21. Roy NS, Wei Y, Kuklinski E, Asbell PA. The growing need for validated biomarkers and endpoints for dry eye clinical research. Invest Ophthalmol Vis Sci. 2017;58(6):BIO1–BIO19. doi:10.1167/iovs.17-21709
22. Korb DR. Survey of preferred tests for diagnosis of the tear film and dry eye. Cornea. 2000;19(4):483–486. doi:10.1097/00003226-200007000-00016
23. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II diagnostic methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
24. Tsubota K, Yokoi N, Shimazaki J, et al.; Asia Dry Eye Society. New perspectives on dry eye definition and diagnosis: a consensus report by the Asia dry eye society. Ocul Surf. 2017;15(1):65–76. doi:10.1016/j.jtos.2016.09.003
25. Dry Eye Syndrome PPP. American academy of ophthalmology; 2018. Available from: https://www.aao.org/preferred-practice-pattern/dry-eye-syndrome-ppp-2018.
26. D’Souza S, James E, Swarup R, Mahuvakar S, Pradhan A, Gupta K. Algorithmic approach to diagnosis and management of post-refractive surgery dry eye disease. Indian J Ophthalmol. 2020;68(12):2888–2894. doi:10.4103/ijo.IJO_1957_20
27. Nair S, Kaur M, Sharma N, Titiyal JS. Refractive surgery and dry eye - an update. Indian J Ophthalmol. 2023;71(4):1105–1114. doi:10.4103/IJO.IJO_3406_22
28. Sharma B, Soni D, Saxena H, et al. Impact of corneal refractive surgery on the precorneal tear film. Indian J Ophthalmol. 2020;68(12):2804–2812. doi:10.4103/ijo.IJO_2296_19
29. Gupta PK, Drinkwater OJ, VanDusen KW, Brissette AR, Starr CE. Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation. J Cataract Refract Surg. 2018;44(9):1090–1096. doi:10.1016/j.jcrs.2018.06.026
30. Trattler WB, Majmudar PA, Donnenfeld ED, McDonald MB, Stonecipher KG, Goldberg DF. The prospective health assessment of cataract patients’ ocular surface (PHACO) study: the effect of dry eye. Clin Ophthalmol Auckl NZ. 2017;11:1423–1430. doi:10.2147/OPTH.S120159
31. Chuang J, Shih KC, Chan TC, Wan KH, Jhanji V, Tong L. Preoperative optimization of ocular surface disease before cataract surgery. J Cataract Refract Surg. 2017;43(12):1596–1607. doi:10.1016/j.jcrs.2017.10.033
32. Donaldson K, Parkhurst G, Saenz B, Whitley W, Williamson B, Hovanesian J. A call to action: treating dry eye disease and setting the foundation for a successful surgery. J Cataract Refract Surg. 2021. doi:10.1097/j.jcrs.0000000000000844
33. Olson RJ, Braga-Mele R, Chen SH, et al. Cataract in the adult eye preferred practice pattern®. Ophthalmology. 2017;124(2):P1–P119. doi:10.1016/j.ophtha.2016.09.027
34. Starr CE, Gupta PK, Farid M, et al. ASCRS Cornea Clinical Committee. An algorithm for the preoperative diagnosis and treatment of ocular surface disorders. J Cataract Refract Surg. 2019;45(5):669–684. doi:10.1016/j.jcrs.2019.03.023
35. Donthineni PR, Das AV, Shanbhag SS, Basu S. Cataract surgery in dry eye disease: visual outcomes and complications. Front Med. 2020;7:575834. doi:10.3389/fmed.2020.575834
36. Röggla V, Leydolt C, Schartmüller D, et al. Influence of artificial tears on keratometric measurements in cataract patients. Am J Ophthalmol. 2021;221:1–8. doi:10.1016/j.ajo.2020.08.024
37. Chen YA, Hirnschall N, Findl O. Evaluation of 2 new optical biometry devices and comparison with the current gold standard biometer. J Cataract Refract Surg. 2011;37(3):513–517. doi:10.1016/j.jcrs.2010.10.041
38. Bullimore MA, Buehren T, Bissmann W. Agreement between a partial coherence interferometer and 2 manual keratometers. J Cataract Refract Surg. 2013;39(10):1550–1560. doi:10.1016/j.jcrs.2013.03.034
39. Epitropoulos AT, Matossian C, Berdy GJ, Malhotra RP, Potvin R. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41(8):1672–1677. doi:10.1016/j.jcrs.2015.01.016
40. Hiraoka T, Asano H, Ogami T, et al. Influence of dry eye disease on the measurement repeatability of corneal curvature radius and axial length in patients with cataract. J Clin Med. 2022;11(3):710. doi:10.3390/jcm11030710
41. Kieval JZ, Al-Hashimi S, Davidson RS, et al. ASCRS refractive cataract surgery subcommittee. Prevention and management of refractive prediction errors following cataract surgery. J Cataract Refract Surg. 2020;46(8):1189–1197. doi:10.1097/j.jcrs.0000000000000269
42. Wlaź A, Kustra A, Rozegnał-Madej A, Żarnowski T. Intraocular lens power calculations in eyes with pseudoexfoliation syndrome. Sci Rep. 2021;11(1):19071. doi:10.1038/s41598-021-98675-5
43. Choi HS, Yoo HS, An Y, Yoon SY, Park SP, Kim YK. Inter-ocular and inter-visit differences in ocular biometry and refractive outcomes after cataract surgery. Sci Rep. 2020;10(1):14673. doi:10.1038/s41598-020-71545-2
44. Chung HS, Chung JL, Kim YJ, Lee H, Kim JY, Tchah H. Comparing prediction accuracy between total keratometry and conventional keratometry in cataract surgery with refractive multifocal intraocular lens implantation. Sci Rep. 2021;11(1):19234. doi:10.1038/s41598-021-98491-x
45. Hoffer KJ, Savini G. Update on intraocular lens power calculation study protocols: the better way to design and report clinical trials. Ophthalmology. 2021;128(11):e115–e120. doi:10.1016/j.ophtha.2020.07.005
46. Aristodemou P, Sparrow JM, Kaye S. Evaluating refractive outcomes after cataract surgery. Ophthalmology. 2019;126(1):13–18. doi:10.1016/j.ophtha.2018.07.009
47. Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
48. Matossian C. Impact of thermal pulsation treatment on astigmatism management and outcomes in meibomian gland dysfunction patients undergoing cataract surgery. Clin Ophthalmol Auckl NZ. 2020;14:2283–2289. doi:10.2147/OPTH.S263046
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Cataract Surgery on IOP and Ocular Structures in Normotensive Patients and Primary and Exfoliation Open-Angle Glaucoma Patients
Xirou V, Xirou T, Siganos C, Ntonti P, Georgakopoulos C, Stavrakas P, Makri OE, Kanakis M, Tsapardoni F, Fragkoulis I, Garnavou-Xirou C, Kozobolis V
Clinical Ophthalmology 2023, 17:1047-1055
Published Date: 5 April 2023
Prevalence of Dry Eye Disease Among Individuals Scheduled for Cataract Surgery in a Norwegian Cataract Clinic
Graae Jensen P, Gundersen M, Nilsen C, Gundersen KG, Potvin R, Gazerani P, Chen X, Utheim TP, Utheim ØA
Clinical Ophthalmology 2023, 17:1233-1243
Published Date: 27 April 2023
Randomized Trial Comparing Prediction Accuracy of Two Swept Source Optical Coherence Tomography Biometers
Multack S, Plummer N, Smits G, Hall B
Clinical Ophthalmology 2023, 17:2423-2428
Published Date: 17 August 2023
Safe and Effective Management of Dry Eye Symptoms with Hydroxypropyl Guar and Hyaluronic Acid Dual-Polymer Lubricating Eye Drops: A Review of Preclinical and Clinical Studies
Srinivasan S, Garofalo R, Williams R
Clinical Ophthalmology 2023, 17:3883-3898
Published Date: 13 December 2023
Efficacy of Adding Sodium Hyaluronate Eye Drops to Tobramycin and Dexamethasone in the Treatment of Post-Cataract Surgery Dry Eye Disease: A Retrospective Analysis and Prospective Questionnaire Assessment
Amer AA, Abu El Wafa Ali EG, Hamed MA, Gad Elkareem AM, Ahmed Sinjab AA, Awny I
Clinical Ophthalmology 2024, 18:613-621
Published Date: 28 February 2024