")
Back to Journals » Clinical Ophthalmology » Volume 17
Impact of Cataract Surgery on IOP and Ocular Structures in Normotensive Patients and Primary and Exfoliation Open-Angle Glaucoma Patients
Authors Xirou V , Xirou T , Siganos C , Ntonti P , Georgakopoulos C , Stavrakas P , Makri OE , Kanakis M , Tsapardoni F, Fragkoulis I, Garnavou-Xirou C, Kozobolis V
Received 17 January 2023
Accepted for publication 28 March 2023
Published 5 April 2023 Volume 2023:17 Pages 1047—1055
DOI https://doi.org/10.2147/OPTH.S402550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vasiliki Xirou,1 Tina Xirou,1 Charalambos Siganos,2 Panagiota Ntonti,3 Constantinos Georgakopoulos,4 Panagiotis Stavrakas,4 Olga E Makri,4 Menelaos Kanakis,4 Foteini Tsapardoni,4 Ioannis Fragkoulis,4 Christina Garnavou-Xirou,1 Vassilios Kozobolis3– 5
1Ophthalmology Department, Hellenic Red Cross Hospital of Athens, Athens, Greece; 2Ophthalmology Department, University Hospital of Heraklion, Heraklion, Greece; 3Ophthalmology Department, University Hospital of Alexandroupolis, Alexandroupolis, Greece; 4Ophthalmology Department, University Hospital of Patras, Patras, Greece; 5Eye Institute of Thrace, Democritus University of Thrace, Alexandroupolis, Greece
Correspondence: Vasiliki Xirou, Ophthalmology Department, Hellenic Red Cross Hospital of Athens, Athens, Greece, Email [email protected]
Purpose: The aim of this study was to evaluate and compare the changes in Intraocular Pressure (IOP) and other ocular parameters: the Anterior Chamber Angle (ACA), Anterior Chamber Volume (ACV), and Anterior Chamber Depth (ACD) during phacoemulsification surgery in Greek patients with normotensive eyes and those with well-controlled Open-Angle Glaucoma (OAG). Additionally, parameters such as the Corneal Thickness (CCT), Axial Length (AL), Central Macular Thickness (CMT), and Retinal Nerve Fibre Layer (RNFL) were also examined.
Patients and Methods: This was a prospective observational case–control study that included 50 phakic eyes, 25 normotensive (Group 1), and 25 with OAG: 15 Primary Open-Angle Glaucoma (POAG) and 10 Exfoliation Glaucoma (EXG) (Group 2). Ophthalmic assessment included IOP measurements, ocular biometry, and anterior and posterior segment optical coherence tomography evaluation of the aforementioned ocular parameters, prior and 6 months after phacoemulsification surgery.
Results: At the 6 months post-operative review, a greater IOP reduction was recorded in eyes with OAG, in comparison to normotensive ones (5.3mmHg and 1.6 mmHg respectively). In addition, a significant but similar increase was recorded in the values of the ACA, ACV, and ACD of both groups between the pre- and the post-op period. Furthermore, the CCT and AL values remained unaltered. Finally, there was a non-statistically significant change in the mean CMT and the mean average RNFL of both groups.
Conclusion: Eyes with OAG tend to undergo a greater reduction in IOP post-phacoemulsification surgery, in comparison to normotensive eyes. This reduction may not be solely attributed to ocular anatomical changes after phacoemulsification surgery but may also be due to the remodeling of the trabecular meshwork and the ciliary body. This may be especially true in the case of OAG eyes, which already start off with a compromised trabecular endothelium prior to surgery.
Keywords: cataract surgery, open angle glaucoma, biometry, axial length, intraocular pressure, corneal pachymetry
Introduction
It is a well-established fact that modern phacoemulsification surgery alters several ocular parameters, such as the anterior chamber depth (ACD) and angle (ACA), as well as the intraocular pressure (IOP). Furthermore, research has demonstrated that certain of these parameters are intertwined with one another; the ACA and its structures play a pivotal role in IOP regulation.1–4 This complicated relationship has been a research topic of several recent publications.5–19
During life, the lens thickness increases causing a decrease in ACA and ACD.1,20,21
Phacoemulsification surgery, which results in the implantation of an intraocular lens inside the capsular bag (PCIOL), leads to the modification of these anterior chambers structures, leading to the modification of the IOP.21
Although the impact of phacoemulsification on IOP mechanisms related to these changes are universally accepted in patients with closed-angle glaucoma,15–17 several theories have been given regarding the post-phacoemulsification IOP reduction in OAG eyes: (1) the increase in the anterior chamber volume (2) the changes of the ACA anatomy (3) remodeling of the endothelium of the trabecular meshwork and (4) the difference in thickness between the phakic lens and the PCIOL and its impact on the ciliary body and the ciliary processes position.2,19,22
Bearing these statements in mind – as well as the fact that an elevated IOP is associated with the progression of glaucoma – it can be assumed that phacoemulsification surgery could be considered as an early form of surgical glaucoma treatment. This is especially true in the case of patients with OAG eyes,14,18 despite the fact that on a macroscopic level the anterior chamber architecture of eyes with OAG is the same as that belonging to normotensive eyes.19,22,23
On the other hand, less information in the literature was published regarding the post-cataract anatomical changes in OAG patients, especially compared to normotensive eyes.
Patients and Methods
The study conducted is a prospective case-control study. Fifty patients from the Ophthalmology Departments from three hospital sites across Greece (Red Cross Hospital of Athens, the University Hospital of Alexandroupolis and the University Hospital of Patras) were recruited between the period January 2019 and June 2021. All patients received phacoemulsification surgery as part of the study. Inclusion criteria were as follows: age > 45 years, IOP < 23 mmHg, visual acuity ≥ 0.3 decimal, open ACA gonioscopically. Exclusion criteria were as follows: previous laser treatment or other ocular surgery, systemic pathology such as diabetes mellitus, arterial hypertension, other ocular pathology (high myopia, closed-angle glaucoma, age related macular degeneration, previous inflammatory eye diseases, ACA pathology during gonioscopy).
The patients were divided into two groups based on their glaucoma status.Group 1 consisted of 25 normotensive individuals 14 out of which were Female (56%): Table 1, whereas Group 2 consisted of 25 patients with OAG 13 out of which were Female (52%): Table 1, 15 had POAG and 10 had EXG. The OAG eyes enrolled presented mild glaucoma (Humphrey visual field test indices: Mean Deviation < 6dB and Visual Field Index > 94%), well-controlled with one anti-glaucoma medical therapy (prostaglandin or b-blocker) for at least 1 year. The same medication continued during the postoperative period. We specify that the well-controlled mild OAG eyes were those with IOP below the target IOP for each patient individually, so that no progression in the visual field was noted during the 1 year follow-up period before enrollment in the study. LOCS II (Lens Opacities Classification System II) was used to determine the nuclear sclerosis grade. All the patients enrolled presented with nuclear sclerosis of grade 1 and grade 2; meaning that they had mild-to-moderate cataract.
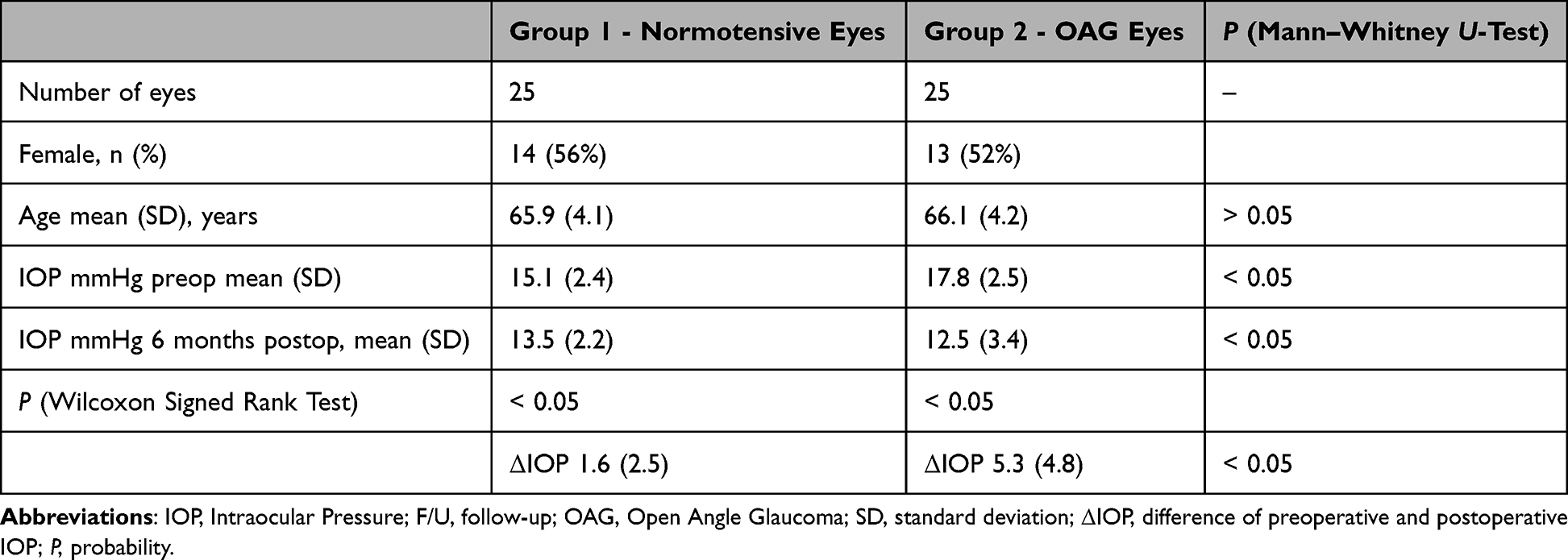 |
Table 1 Demographic Data of the Greek Population & IOP Preoperatively and Postoperatively at the End of the Follow Up Period of 6 Months |
The study was approved by the ethics committee of the Eye Institute (N 29/2018), and a written informed consent was obtained from all patients. All procedures adhered to the tenets of the Declaration of Helsinki. Ten (10) eyes in each group had exfoliation material in the anterior chamber during the preoperative examination in the slit lamp.
All 50 eyes underwent uneventful phacoemulsification surgery (Centurion Vision System, Alcon Laboratories) by two experienced surgeons (V.X. and V.K.). In all cases, a temporal clear corneal incision (2.4 mm) was made for the main wound. Viscoelastic material (Viscoat, Alcon ®), was subsequently used to complete the continuous curvilinear capsulorhexis (~5.5 mm diameter), which was followed by the hydro-dissection, phacoemulsification of the nucleus and aspiration of cortex. The capsular bag was then filled with Pro-visc ® (Alcon), prior to the insertion of the Intraocular Lens (IOL). All IOLs were inserted into the capsular bag. All the IOls used – Alcon AcrySof® IQ lenses (Alcon) and EnVista® lenses (Bausch + Lomb), were monofocal aimed at −0.50 spherical refraction. The mean IOL power was 21 (+2.1) diopters and 20.75 (+2.0) in Group 1 and Group 2, respectively. Finally, the remaining viscoelastic was meticulously removed from the eye prior to completion of the surgery.
All the IOP measurements were performed by the same ophthalmologists using the Goldmann Applanation Tonometry on each eye twice: preoperatively and 6 months postop.
All the Anterior Segment Optical Coherence Tomography: AS-OCT (Visante OCT, Carl Zeiss Meditec) and posterior – OCT (Optovue, Avanti XR, Visionix) measurements were performed by the same ophthalmologists on each eye twice: preoperatively and 6 months postoperatively.
We evaluated the following ocular biometry parameters: Central Corneal Thickness (CCT/μm), Axial Length (AL/mm), Anterior Chamber Depth (ACD/mm), Anterior Chamber Volume (ACV/mm3), Angle Opening Distance at 500 μm from scleral spur (AOD500), as well as Trabecular-Iris Space Area 500 (TISA500).
Additionally, the mean Central Macular Thickness (CMT) and the mean average Retinal Nerve Fibre Layer (RNFL) thickness were recorded pre- and postoperatively in both groups.
The SPSS Version 23.0 Program was used for statistical analysis. The normality of the sample distribution was evaluated with Kolmogorov–Smirnov test. The Mann–Whitney U-test was used for the comparison of the two non-parametric independent samples.
Finally, the Spearman Correlation Coefficient was used for non-parametric correlations. The p value was deemed to be statistically significant if it was <0.05.
Results
Twenty-five phakic, normotensive eyes (Group 1) and 25 phakic eyes with open-angle glaucoma (Group 2) were included in the study. There was no difference regarding patients’ age between the groups (Table 1).
The IOP was significantly higher in the OAG group before the surgery. At the 6 month post-operative review, there was a statistically significant reduction in the IOP of both groups (p=0.001). However, this reduction was observed to be greater in the OAG group in comparison to the normotensive one (Table 1).
As was mentioned previously, OAG patients were kept on the same anti-glaucoma drops pre- and post-operatively.
The findings of the 6 month post-operative review are summarized below
- There was no statistically significant change in the CCT and AL values pre- and post-operatively (Table 2).
- There was a statistically significant increase in the mean ACD of both groups (p=0.001). This difference between the groups was not significant (Table 2).
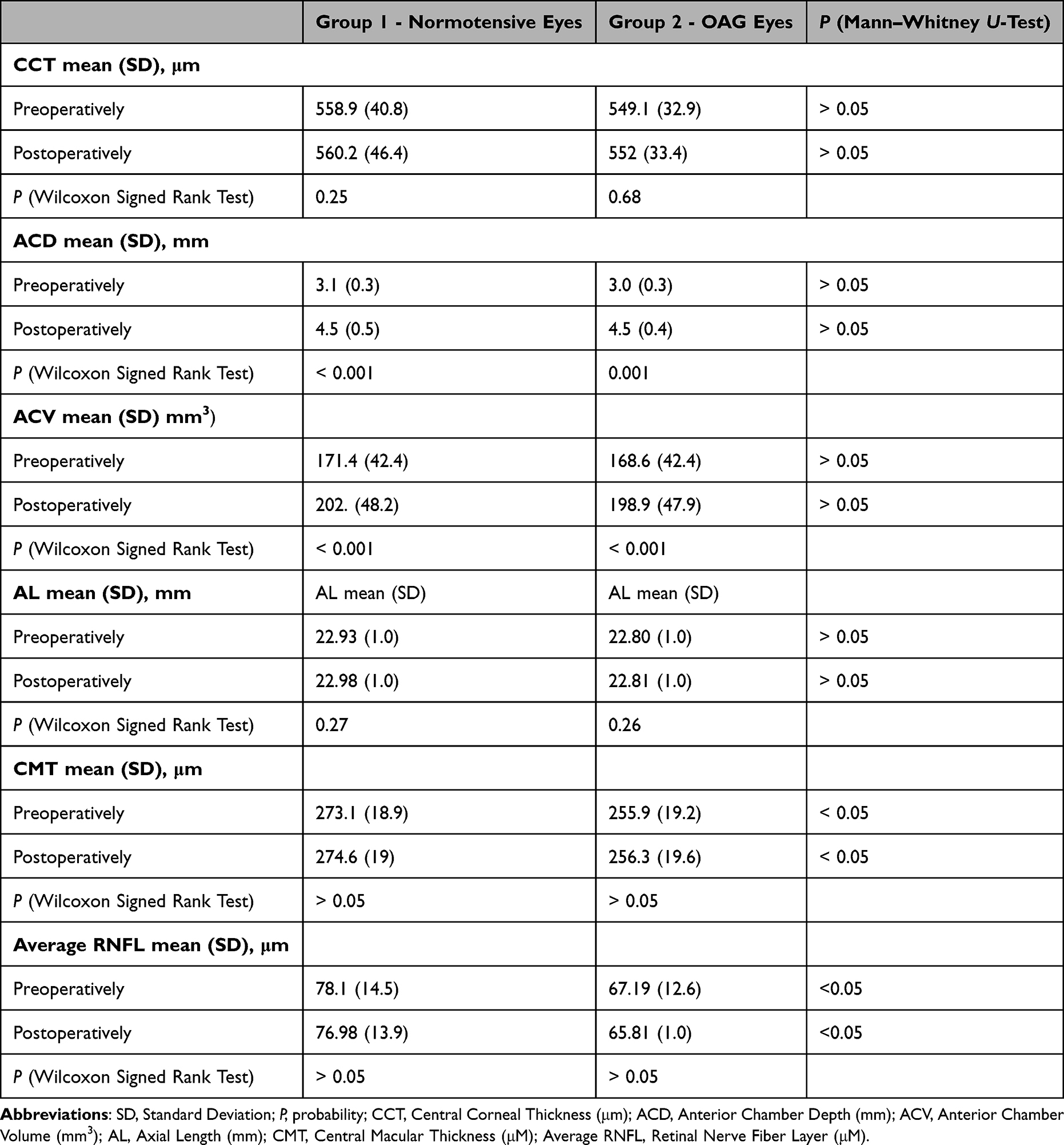 |
Table 2 Preoperatively and Postoperatively at the End of the Follow Up Period of 6 Months in Normotensive & OAG (Open-Angle Glaucoma) Eyes |
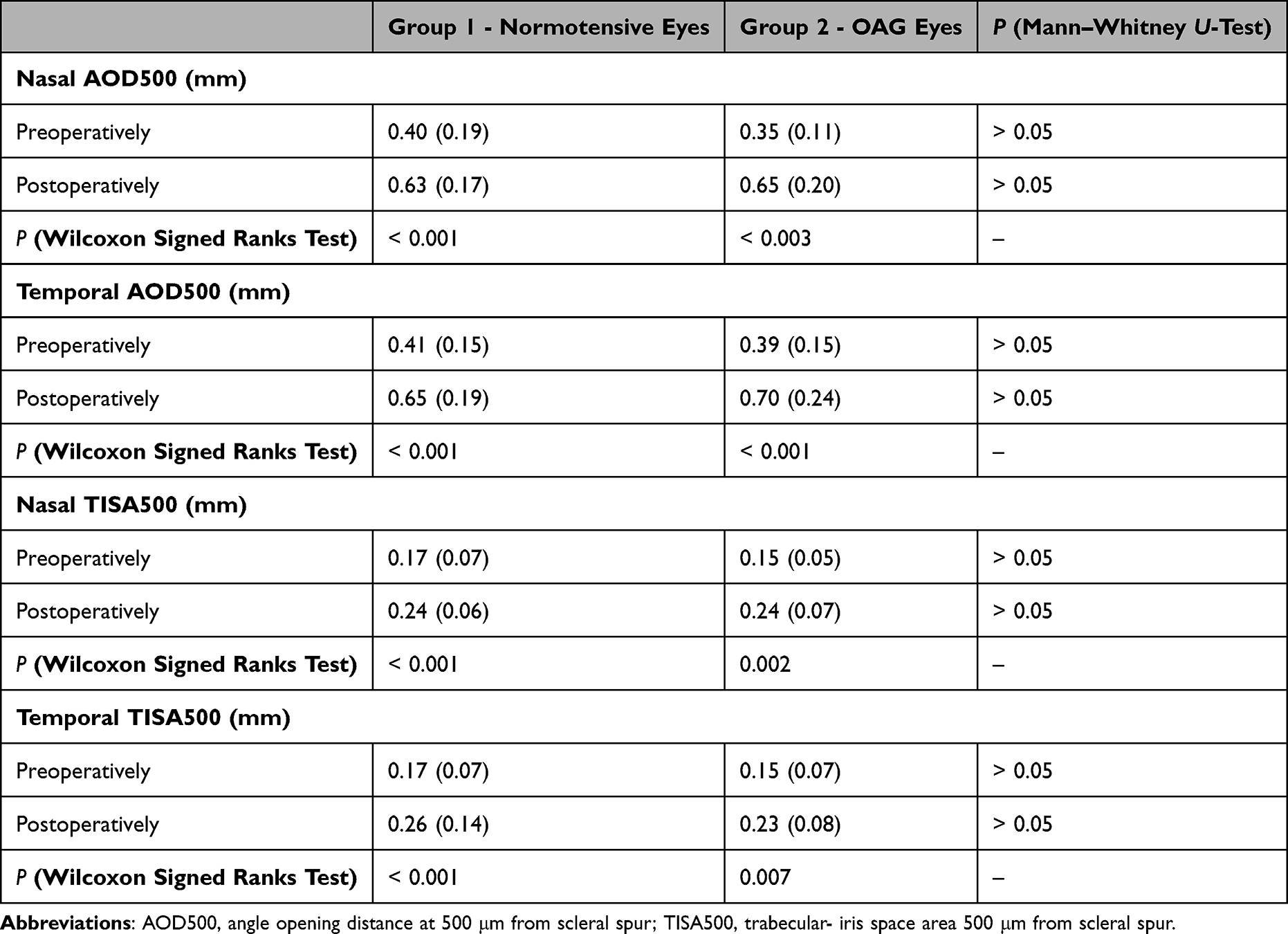 |
Table 3 Nasal & Temporal AOD500 & TISA500 Pre- and Postoperatively |
Discussion
In this study, we evaluate the impact of phacoemulsification surgery on IOP and several other ocular parameters in normotensive eyes and eyes with OAG (POAG and EXG).
Our inclusion criteria incorporated patients with eyes with mild glaucoma (MD < 6dB and VFI > 94%), well controlled with one medication (prostaglandin or b-blocker), who were then compared to normotensive patients, exhibiting the same demographic characteristics (Table 1).
Furthermore, our results recorded no change in CCT and AL, between preoperative and postoperative status in either group and no difference between the groups. In addition, no difference between the two groups was recorded with regard to the ACD, ACV while an increase in these two parameters was recorded postoperatively in both groups.
Considering the posterior segment parameters, such as the mean RNFL and the central macular thickness, we noted that there was no statistical difference in either group 6 months after the operation regarding the RNFL and the CMT, while the statistical difference between normal and glaucoma group, which was recorded preoperatively remained unaltered 6 months post-operatively.
Furthermore, our results also revealed a significantly higher IOP reduction in OAG eyes when compared to normotensive eyes. It is important to reiterate that ten (10) of the OAG eyes presented with exfoliation material in the anterior chamber during the preoperative examination in the slit lamp. Interestingly, there was no difference found between EXG eyes and POAG eyes regarding the post-op IOP reduction. Obviously, the sample population of EXG and POAG eyes in this study is too small to enable us to arrive at any concrete conclusions.
Over the past years, researchers have been looking into the relationship between IOP (reduction) and phacoemulsification surgery in normotensive and OAG eyes. However, a few have examined this topic on homogeneous populations such as the Greek one. In this study, we focus and compare the change in parameters concerning both ocular posterior and anterior chambers in normotensive and OAG eyes in patients of Greek origin.
Additionally, despite the small sample size in this study, it is important to note that the OAG group consisted of patients with mild EXG and mild POAG, who were well-controlled on one medication.
The results of IOP reduction in normotensive eyes after phacoemulsification surgery vary in several published papers (Table 4). On the other hand, Majstruk et al found that 12 months following phaco surgery, eyes with POAG underwent an IOP decrease of 10mmHg.13
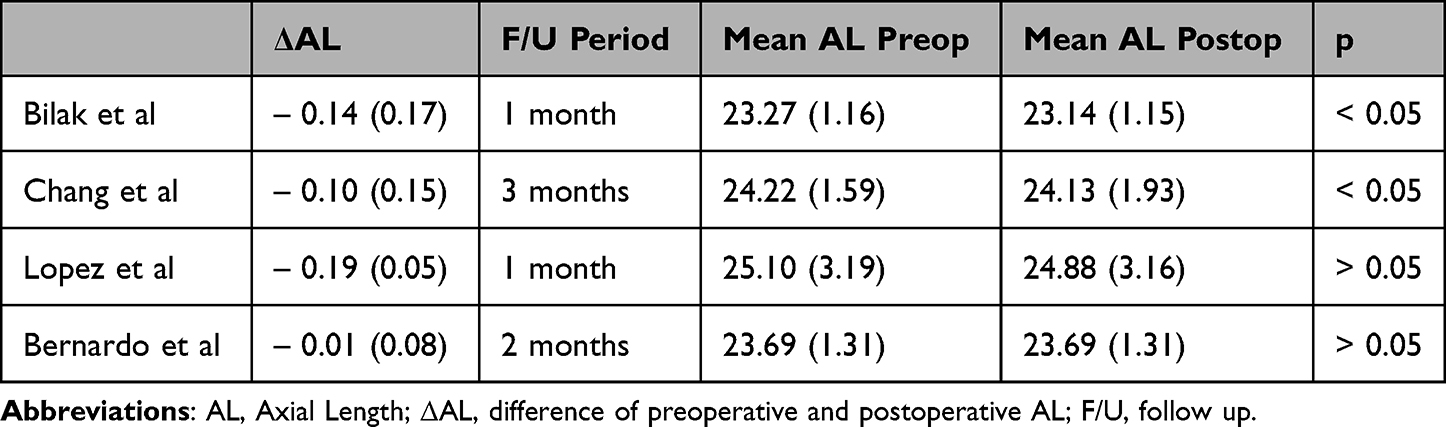 |
Table 4 Postoperative Change of AL After Cataract Phacoemulsification in Normotensive Eyes |
We evaluate the changes in IOP as well as the ACA and other ocular parameters of the anterior and posterior segment that take place 6 months following phacoemulsification surgery. We chose a period of 6 months as we deem it unlikely that any further structural changes to the eyes will take place after this period, thus other studies agree with this consideration.18,19
According to Our Results
The ACA width was found to be increased in all eyes of both groups at the end of the follow-up period. No correlation was found, in both groups, between preoperative ACA with the IOP change postoperatively. The same is valid in both groups, regarding the post-op increase of ACA and the IOP change postoperatively. This contradicts the findings of the study conducted by Lin et al, where the researchers identified that a correlation did indeed exist between the pre-phacoemulsification ACA parameters and the post-operative IOP.16
Our findings may indicate that other mechanisms other than structural AC alterations are responsible for the decrease in IOP, such as the post-operative remodeling of the trabecular meshwork or changes, which occur in the ciliary body and its processes.23–25
Our conclusion that the changes in ACA are not the only causative factor for the post-operative decrease in IOP comes in accordance with the study by Lee et al24 and not with the conclusion of Shammas et al21 in which the cataractic lens produces a reduction of the ACA depth by pushing the iris anteriorly and consequently the post-phacoemulsification ACA deepening is the main causative factor of the IOP reduction postoperatively.
Furthermore, our findings that there was a significant increase of both nasal and temporal increase AOD500 & TISA500 after the phacoemulsification surgery, are on par with the findings of Kim et al,12 whose study included only normotensive individuals and no change in IOP post-operatively was also mentioned.
Several contradictory results were published regarding AL shortening in patients who underwent phacoemulsification surgery.8,26 We found no post-phacoemulsification change regarding the AL of either group by performing measurements with IOL Master 700 (Carl Zeiss Meditec, Jena, Germany), in order to avoid errors as explained previously by Bernardo et al.27 Concerning the AL, our results are in accordance with those found by Bernardo and Lopez27,28 and not with the results published by Bilak, Chang and Kim.8,26,29
We consider our follow-up period of 6 months as an important element of our study, as previous similar research carried out had a shorter follow-up period of 1–3 months (Table 4). Additionally, no glaucoma eyes had been enrolled in these studies.
Furthermore, Pakuliene et al identified a shortening of AL in normotensive eyes and no change in OAG eyes postoperatively.30 The authors attributed this finding to the difference in scleral rigidity in glaucomatous eyes. In our present study, these findings coincide only with our arm of OAG eyes.
In a review published in 2015, Chen et al concluded that cataract phacoemulsification decreases IOP and medications in a small, moderate and marked way in eyes with POAG, EFG and Primary Angle Closure Glaucoma (PACG), respectively, using 1 to 2 medications before surgery.31
In contrast, we did not find any significant difference in IOP decrease between eyes with POAG and EFG in our study, taking into consideration that all glaucoma eyes were receiving only one medication, while no narrow-angle eyes were enrolled in our study.
Also, no significant differences were recorded regarding the central macular thickness between normotensive and OAG eyes, or between EFG and non-EFG eyes. The same applies when comparing EFG and POAG eyes at the pre- and post-op reviews. These findings are also consistent with those of Kemer Atik, who concluded that EFG is not a risk factor for a post-phaco-cataract macular thickness increase.32
Finally, the mean average RNFL was recorded without significant change between preoperative and after 6 months postoperative status. This finding is not in agreement with the findings of Erkan Celik et al33 where an increase in RNFL was recorded 1 month postoperatively. We could explain this discrepancy by the fact that our study was conducted with a follow-up of 6 months and no other measurements were performed during this postop period.
The strength of this study is the comparison of the change in IOP and the anterior chamber parameters after phacoemulsification surgery in normotensive and glaucoma eyes with the enrollment of exfoliative glaucoma eyes. Analogous studies in the literature compared IOP changes after phacoemulsification in only OAG eyes or compared only OAG and PACG eyes. Additionally, we consider as an advantage of our study the duration of the follow-up period and the evaluation of all parameters, which could be influenced after phacoemulsification surgery, in the same group of patients in a homogeneous population.
Obviously, there are limitations in our study, which are the low number of enrolled patients, the fact that no choroidal changes were assessed, the non-detailed record of all parameters characterizing macular thickness and Ganglion Cell Inner Plexiform Layer (GCIPL) and the low number of EXG and POAG eyes for a reliable conclusion.
In this study, post-phacoemulsification change in IOP was found to be significantly more pronounced in OAG-cataract eyes compared to normotensive-cataract eyes. The duration of the IOP decrease is needed to be investigated for a longer period of time, especially in OAG eyes, in order to better evaluate its role as an antiglaucoma procedure in mild OAG eyes.
Finally, our results may lead to the conclusion that not the widening of the anterior chamber angle but other factors may play a role in the reduction in IOP post phacoemulsification, such as trabecular meshwork remodeling and changes that take place at the level of the ciliary body and the ciliary processes especially in OAG, which start –off with an already compromised trabecular endothelium.
Ethics and Consent Statements
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the Helsinki Declaration and its later amendments.
The study was approved by the ethics committee of the Eye Institute (N 29/2018), and a written informed consent was obtained from all patients.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Masis Solano M, Lin SC. Cataract, phacoemulsification and intraocular pressure: is the anterior segment anatomy the missing piece of the puzzle? Prog. Retin Eye Res. 2018;64:77–83.
2. Rüfer F, Schröder A, Klettner A, et al. Anterior chamber depth and iridocorneal angle in healthy White subjects: effects of age, gender and refraction. Acta Ophthalmol. 2010;88:885–890. doi:10.1111/j.1755-3768.2009.01588.x
3. Huang G, Gonzalez E, Lee R, et al. Association of biometric factors with anterior chamber angle widening and intraocular pressure reduction after uneventful phacoemulsification for cataract. J Cataract Refract Surg. 2012;38:108–116. doi:10.1016/j.jcrs.2011.06.037
4. Kim M, Park KH, Kim TW, Kim DM. Changes in anterior chamber configuration after cataract surgery as measured by anterior segment optical coherence tomography. Korean J Ophthalmol. 2011;25:77. doi:10.3341/kjo.2011.25.2.77
5. DeVience E, Chaudhry S, Saeedi O. Effect of intraoperative factors on IOP reduction after phacoemulsification. Int Ophthalmol. 2017;37:63–70. doi:10.1007/s10792-016-0230-7
6. Bilak S, Simsek A, Capkin M, Guler M, Bilgin B. Biometric and intraocular pressure change after cataract surgery. Optom Vis Sci. 2015;92:464–470. doi:10.1097/OPX.0000000000000553
7. Baek SU, Kwon S, Park IW, Suh W. Effect of phacoemulsification on intraocular pressure in healthy subjects and Glaucoma patients. J Korean Med Sci. 2019;34:1294–1307. doi:10.3346/jkms.2019.34.e47
8. Coh P, Moghimi S, Chen RI, et al. Lens position parameters as predictors of intraocular pressure reduction after cataract surgery in glaucomatous versus nonglaucomatous eyes. Investig Ophthalmol Vis Sci. 2016;57:2593–2599.
9. Guan H, Mick A, Porco T, Dolan BJ. Preoperative factors associated with IOP reduction after cataract surgery. Optom Vis Sci. 2013;90:179–184. doi:10.1097/OPX.0b013e31827ce224
10. Yoo C, Amoozgar B, Yang KS, Park JH, Lin SC. Glaucoma severity and intraocular pressure reduction after cataract surgery in eyes with medically controlled glaucoma. Med. 2018;97:e12881.
11. Jimenez-Roman J, Lazcano-Gomez G, Martínez-Baez K, et al. Effect of phacoemulsification on intraocular pressure in patients with primary open angle glaucoma and pseudoexfoliation glaucoma. Int J Ophthalmol. 2017;10:1374–1378. doi:10.18240/ijo.2017.09.07
12. Kim M, Park KH, Kim T-W, Kim DM. Anterior chamber configuration changes after cataract surgery in eyes with glaucoma. Korean J Ophthalmol. 2012;26:97–103. doi:10.3341/kjo.2012.26.2.97
13. Majstruk L, Leray B, Bouillot A, et al. Long term effect of phacoemulsification on intraocular pressure in patients with medically controlled primary open-angle glaucoma. BMC Ophthalmol. 2019;19:1–7. doi:10.1186/s12886-019-1157-3
14. Iancu R, Corbu C. Intraocular pressure after phacoemulsification in patients with uncontrolled primary open angle glaucoma J. Med Life. 2014;7:11–16.
15. Siak J, Quek D, Monisha E, et al. Anterior chamber angle and intraocular pressure changes after phacoemulsification: a comparison between eyes with closed-angle and open-angle glaucoma. J Glaucoma. 2016;25:e259–e264. doi:10.1097/IJG.0000000000000271
16. Lin SC, Masis M, Porco TC, Pasquale LR. Predictors of intraocular pressure after phacoemulsification in primary open- angle glaucoma eyes with wide versus narrower angles (an American ophthalmological society thesis). Trans Am Ophthalmol Soc. 2017;115:1–13.
17. Brown RH, Zhong L, Whitman AL, et al. Reduced intraocular pressure after cataract surgery in patients with narrow angles and chronic angle-closure glaucoma. J Cataract Refract Surg. 2014;40:1610–1614. doi:10.1016/j.jcrs.2014.01.038
18. Shingleton BJ, Pasternack JJ, Hung JW, O’Donoghue MW. Three and five years changes in intraocular pressures after clear corneal phacoemulsification in open angle glaucoma patients, glaucoma suspects, and normal patients. J Glaucoma. 2006;15:494–498. doi:10.1097/01.ijg.0000212294.31411.92
19. Cetinkaya S, Dadaci Z, Acir N, et al. The effect of phacoemulsification surgery on intraocular pres- sure and anterior segment anatomy of the patients with cataract and ocular hypertension. Indian J Ophthalmol. 2015;743:745.
20. Wang D, Meng Q, He M, et al. Ethnic difference of the anterior chamber area and volume and its association with angle width. Invest Ophthalmol Vis Sci. 2012;53(6):3139–3144. doi:10.1167/iovs.12-9776
21. Shammas HJ, Shammas MC. Measuring the cataractous lens. J Cart Refract Surg. 2015;41:1875–1879. doi:10.1016/j.jcrs.2015.10.036
22. Zoroquiain P, Mastromonaco C, Balaszi M, et al. Histopathological trabecular meshwork remodeling after cataract surgery detected with an advanced image analyzer. J Cataract Refract Surg. 2018;44:98–102. doi:10.1016/j.jcrs.2017.09.034
23. Woo-Jin K, Ju-Mi K, Kyoung Nam Kim CK. Effect of preoperative factors and gonioscopy on intraocular pressure reduction after phacoemulsification in glaucoma. J Korean Ophthalmol Soc. 2019;60:463–469. doi:10.3341/jkos.2019.60.5.463
24. Lee H, Zukaite I, Juniat V, et al. Changes in symmetry of anterior chamber following routine cataract surgery in non-glaucomatous eyes. Eye Vis. 2019;6:1–8. doi:10.1186/s40662-019-0144-3
25. Liu XQ, Zhu HY, Su J, Hao XJ. Effects of phacoemulsification on intraocular pressure and anterior chamber depth. Exp Ther Med. 2013;5:507–510. doi:10.3892/etm.2012.835
26. Chang SW, Yu CY, Chen DP. Comparison of intraocular lens power calculation by the IOLMaster in Phakic and eyes with hydrophobic acrylic lenses. Ophthalmology. 2009;116:1336–1342. doi:10.1016/j.ophtha.2009.01.035
27. De Bernardo M, Salerno G, Cornetta P, Rosa N. Axial length shortening after cataract surgery: new approach to solve the question. Transl Vis Sci Technol. 2018;7:34. doi:10.1167/tvst.7.6.34
28. García López C, García López V. Change in axial length pre and post cataract surgery measured with IOL master. J Clin Exp Ophthalmol. 2016;7:1–5. doi:10.4172/2155-9570.1000544
29. Kim YC, Koo YH, Bin-Hwang H, Kang KD. The shape of posterior sclera as a biometric signature in open angle glaucoma. J Glaucoma. 2020;29:890–898. doi:10.1097/IJG.0000000000001573
30. Pakuliene G, Kuzmiene L, Siesky B, et al. Changes in ocular morphology after cataract surgery in open angle glaucoma patients. Sci Rep. 2021;11(1):12203. doi:10.1038/s41598-021-91740-z
31. Chen PP, Lin SC, Junk AK, et al. The effect of phacoemulsification on intraocular pressure in glaucoma patients: a report by the American Academy of Ophthalmology. Ophthalmology. 2015;122:1294–1307. doi:10.1016/j.ophtha.2015.03.021
32. Atik BK, Kirmaci A, Garip R. Comparison of macular thickness change by optical coherence tomography after uncomplicated cataract surgery in eyes with and without exfoliation syndrome. Int Ophthalmol. 2021;41(2):519–526. doi:10.1007/s10792-020-01602-2
33. Celik E, Cakır B, Turkoglu EB, et al. Effect of cataract surgery on subfoveal choroidal and ganglion cell complex thicknesses measured by enhanced depth imaging optical coherence tomography. Clin Ophthalmol. 2016;10:2171–2177. doi:10.2147/OPTH.S105992
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.