Back to Journals » Clinical Ophthalmology » Volume 17
Safe and Effective Management of Dry Eye Symptoms with Hydroxypropyl Guar and Hyaluronic Acid Dual-Polymer Lubricating Eye Drops: A Review of Preclinical and Clinical Studies
Authors Srinivasan S, Garofalo R, Williams R
Received 29 July 2023
Accepted for publication 6 November 2023
Published 13 December 2023 Volume 2023:17 Pages 3883—3898
DOI https://doi.org/10.2147/OPTH.S428725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sruthi Srinivasan,1 Renee Garofalo,2 Ravaughn Williams2
1Alcon Research LLC, Johns Creek, GA, 30097, USA; 2Alcon Research, LLC, Fort Worth, TX, 76134, USA
Correspondence: Sruthi Srinivasan, Alcon Research LLC, 11460 Johns Creek Parkway, Johns Creek, GA, 30097, USA, Tel +1 678 415 5315, Email [email protected]
Abstract: Dry eye disease (DED) is a chronic ocular surface disorder often characterized by decreased tear production and rapid tear evaporation that affect tear film stability and homeostasis. The common symptoms of DED include ocular discomfort, visual disturbances, dryness, and itching. Artificial tears are the mainstay of DED management and supplement one or more layers of the tear film. Artificial tear drops are available as a combination of viscosity-enhancing agents (demulcents/lubricants), humectants, and buffers either with or without preservatives. Artificial tears, as a combination of components (polymers/demulcents/viscosity-enhancing agents), can provide synergistic action compared with a single component for the management of multifactorial signs and symptoms of DED. This review describes the formulation components, physicochemical properties, mechanism of action, and summary of preclinical and clinical evidence on the hydroxypropyl guar-hyaluronic acid (HPG-HA) dual-polymer lubricant eye drops (SYSTANE™ HYDRATION). The dual-polymer eye drops consist of dual demulcents (propylene glycol and polyethylene glycol 400) and the polymers hydroxypropyl guar (HPG) and hyaluronic acid (HA). When instilled on the ocular surface, HPG forms a cross-linked gel matrix with borate ions that prolongs the retention of demulcents, thus providing long-lasting lubrication and ocular surface protection. Additionally, HA stabilizes the tear film, increases corneal wettability, and reduces friction during blinks due to its hygroscopic and viscoelastic properties. Preclinical evidence demonstrates that HPG HA dual-polymer lubricant eye drops provide protection against desiccation by cell hydration and surface retention, cell barrier protection, prolonged lubrication, and promotion of corneal re-epithelialization. Clinical scientific evidence demonstrates that HPG HA dual-polymer lubricant eye drops are safe and effective in the management of DED. Specifically, they reduce the signs and symptoms of DED, reduce dry eye symptoms post-cataract surgery, and improve tear film quality in healthy eyes.
Keywords: artificial tears, cataract surgery, demulcent, dry eye disease, lubrication, symptom relief
Introduction
Dry Eye Disease
Dry eye disease (DED) is a multifactorial inflammatory ocular disease that affects tear film stability and homeostasis.1 DED is characterized by signs such as decreased tear production, rapid tear evaporation, and ocular surface damage;2,3 with common symptoms such as ocular discomfort, visual disturbances, dryness, burning, itching, and redness.2,4 The global overall prevalence of DED involving symptoms, either with/without signs, is approximately 5%–50% depending on age, sex, and geographic location.2
DED is classified as aqueous-deficient dry eye (ADDE), evaporative dry eye (EDE), and mixed dry eye.5 ADDE occurs due to reduced lacrimal gland function, resulting in decreased tear production.5,6 EDE, the most common type, occurs due to conditions affecting eyelids (eg, meibomian gland dysfunction and blink abnormalities) or ocular surface (eg, mucin deficiency and contact lens wear) that lead to tear film instability and excessive evaporation of the tear film.5,6 As DED progresses, both ADDE and EDE may occur concurrently as the mixed DED.5,7
As DED is a multifactorial disease, the management of dry eye is planned according to the type and etiology of the disease. DED management aims to relieve the symptoms of dry eye, restore homeostasis of the tear film and ocular surface, and improve the quality of life (QoL) of patients with DED. Additionally, treatment depends on the severity of the disease and can be either conservative or aggressive, thus helping to effectively manage multifaceted DED presentation.8,9
Currently, several treatments are available to manage and alleviate the symptoms of DED, including artificial tear substitutes (for aqueous and/or lipid supplementation), biological tear substitutes (eg, autologous serum), tear conservation approaches (eg, punctal occlusion), antibiotics, and anti-inflammatory drugs.7
Management of DED: Artificial Tears
Artificial tears are considered the mainstay of DED treatment.7 They constitute the class of topical eye formulations that supplement the aqueous and/or lipid layers of the tear film, reduce tear evaporation, stabilize the tear film, and provide lubrication to the eyes to reduce ocular complications.7,10 Several artificial tear products of varying compositions and viscosities are available in the form of gels, ointments, and drops.9
Artificial tears are specifically designed as a combination of viscosity-enhancing agents (demulcents/lubricants), humectants, electrolytes, osmoprotectants, antioxidants, preservatives, and buffers.11 Viscosity-enhancing agents constitute the most frequently used component of artificial tears. Demulcents or viscosity enhancing agents increase tear film thickness, improve corneal surface wettability, and provide lubrication to the ocular surface, thereby relieving symptoms of DED.11 Some widely used demulcents or viscosity enhancing agents include cellulose derivatives (eg, carboxymethylcellulose [CMC]), polyol liquids (eg, polyethylene glycol and polypropylene glycol), and povidone.11 Commonly available artificial tear eye drops in the market are also based on CMC, polyethylene glycol/propylene glycol/hydroxypropyl guar (HPG), hydroxypropyl methylcellulose (HPMC), hyaluronic acid (HA), and combination products such as HPG and HA.11
A key challenge with artificial tear eye drops is their low retention time on the ocular surface.12 To overcome this challenge, various viscosity-enhancing agents are incorporated in the eye drops, which prolong the retention time of artificial tear formulations.7 For example, hydroxypropyl guar (HPG), a polymer, that undergoes a solution-gelation transition at the ocular surface and forms an in-situ gelling system with tears.11 HPG has bioadhesive gel-forming property at the ocular pH and has viscoelastic property.12,13 Hence, it prolongs the retention of demulcents on the ocular surface, increases tear film stability, and provides sustained lubrication in patients with DED.14 In addition, HPG has been shown to exhibit mucomimetic properties and therefore improves precorneal mucous layer retention offering fast relief from symptoms of DED.15
Furthermore, sodium hyaluronate (HA), a naturally occurring polymer in human tears, has inherent viscoelastic and hygroscopic (water-retaining) properties, and thus provides enhanced lubrication.7,16 HA-based eye drops have been demonstrated to be safe and effective in alleviating the signs and symptoms of dry eye in patients with DED.17,18
Thus, artificial tears designed as a combination of components (eg, demulcents/viscosity-enhancing agents) can provide synergistic or dual action as compared with a single component for the management of multifactorial signs and symptoms of DED.12 An artificial tear product of the SYSTANE™ family, SYSTANE™ HYDRATION (hydroxypropyl guar-hyaluronic acid [HPG-HA] dual-polymer lubricating eye drop), is indicated for the temporary relief of burning and irritation in persons experiencing dry eye symptoms.19 In this review, we describe the composition, mechanism of action, and preclinical and clinical scientific evidence of the HPG-HA dual-polymer containing lubricating eye drops (Alcon Laboratories, Inc., Fort Worth, TX, USA).
HPG-HA Dual-Polymer Containing Lubricating Eye Drops
Formulation Components and Physicochemical Properties
HPG-HA dual-polymer lubricating eye drops are artificial tear products containing dual demulcents (propylene glycol and polyethylene glycol) and dual viscosity-enhancing agents and polymers (HPG and HA).20
The lubricating eye drops are composed of the following ingredients: polyethylene glycol 400, propylene glycol, HPG, HA, sorbitol, aminomethyl propanol, boric acid, sodium borate, potassium chloride, purified water, and sodium chloride (preserved formulation contains polyquad [polidronium chloride] preservative, sodium citrate, and disodium ethylenediamine tetraacetic acid [EDTA]).14 HPG-HA dual-polymer eye drops are available as unit-dose preservative-free, multi-dose preservative-free (MDPF), and multi-dose preserved formulations.
Studies evaluating the physicochemical properties of the HPG-HA dual-polymer have shown that the average molecular weight (MW) of the HPG-HA dual-polymer is 1334 kDa (2233 kDa post-hyaluronidase treatment), with the average MW of HA (0.15%) being <500 kDa.21 Further, the HPG-HA dual-polymer eye drops have a polydispersity index of 1.44, pH of 7.90, sodium concentration of 121 mM, and a coefficient of friction of 0.07 ± 0.01.21,22 The average osmolality for HPG-HA dual-polymer eye drops ranges between 240 and 280 mOsm/kg (mmol/kg).21,23
Mechanism of Action
In the eye drop bottle (pH 7.9), sorbitol/borate/HPG complexes remain in a state of dynamic equilibrium, where sorbitol competes with borate ions to form complexes with HPG; this reduces the cross-linking of HPG and results in a droppable gel.20,24 During instillation of eye drops, the pressure exerted on the bottle causes a reduction in the viscosity of the gel via shear thinning.25 The low viscosity of the HPG not only diminishes the risk of visual blurring on instillation but also improves migration of the eye drops for the cornea, providing protection to the epithelial and mucoaqueous layer.26 On the ocular surface, sorbitol is diluted due to its water solubility, thereby allowing the borate/HPG cross-links to be fortified.24 The change in pH (normal eye: 7.5; dry eye: 7.8) and the natural divalent ions in the tear film (eg, calcium, zinc, and magnesium) help in the fortification of the borate/HPG cross-linking. The sorbitol/HPG interactions weaken, thereby increasing the density of borate/HPG cross-links.20,25 The increased density of borate/HPG cross-links forms a matrix on the damaged regions of the ocular surface.20 This matrix, in turn, prolongs the retention of demulcents on the ocular surface to provide long-lasting lubrication and comfort, reduce friction during blinking, and increase ocular surface protection, thus helping in reducing clinical signs associated with DED.20,25 HPG-based artificial tear formulations have shown to relieve symptoms and improve signs in patients with DED.27,28 Additionally, clinical studies encompassing over a decade on HPG-based formulations have shown improvements not only in individual symptoms13,27,29 and ocular surface disease index score (OSDI) but also in signs such as reduction in corneal staining,27,29,30 total ocular surface staining (TOSS),13 and tear break up time (TBUT);27,30 thereby maintaining the integrity and stability of the corneal surface.29
Role of HA
HA is a naturally occurring polysaccharide with hygroscopic (water-absorptive) and viscoelastic properties.20,31 HA has a higher viscosity on the ocular surface between blinks and hence is retained on the ocular surface and provides protection.16,32 The viscosity of HA reduces during blinks due to shear force, which enables HA to spread across the ocular surface, thus increasing tear film stability, adhesion to the corneal epithelium, and reducing friction.16 Further, due to the abundance of hydroxyl groups, HA attracts water molecules and helps in increasing the tear film thickness, stabilizing the tear film, and increasing corneal wettability.33–35 HA has also been shown to help in corneal wound healing through the activation of corneal epithelial cell migration.36 These properties make HA a valuable component in an artificial tear formulation.34 Hence, the combination of both HPG and HA polymers in eye drops provides better hydration, spreading and retention of demulcents, and lubrication of the ocular surface.20
HPG-HA Dual-Polymer Preservative-Free Lubricating Eye Drops
Due to the chronic nature of DED, repeated instillation of artificial tear eye drops is required throughout the day, over a long-term period.37 The multi-dose eye drops typically need to be protected with a preservative to prevent microbial growth.37 Some of the commonly used preservatives include benzalkonium chloride and polyquaternium-1.37 However, use of certain preservative-containing artificial tear formulations, especially when used over a long term, can have undesirable effects such as ocular symptoms and cytotoxicity.37–39 Therefore, preservative-free eye drops are desirable in patients with chronic dry eye requiring multiple instillations of artificial tear formulations over long periods.37 Switching from preserved to preservative-free formulations has been shown to improve ocular surface by preventing preservative-induced complications and improving clinical signs and symptoms of the disease.37,40
HPG-HA dual-polymer preservative-free artificial tear drops, which are similar to the formulation with preservatives, are designed as both unit-dose and multi-dose formulations. However, certain unit-dose preservative-free formulations are not easy to handle and are expensive.41 Preservative-free multi-dose eye drop formulations require a mechanism to maintain the sterility of the solution once the bottle is opened.37 HPG-HA dual-polymer MDPF drops are designed with Novelia® PureFlow® technology.42,43 This design utilizes a silicone membrane (PureFlow Technology) that filters air; it also comprises a non-return one-way valve that allows air but not contaminated liquid to enter the bottle, thus avoiding bacterial contamination.43,44 Furthermore, the Novelia system has been shown to be easy to use and has eye drop control with an efficient residual drop removal from the tip of the bottle.42
The specific composition, properties, and mechanism of action of HPG and HA highlight their potential as artificial tear lubricants in relieving dry eye symptoms. Further, preclinical and clinical scientific evidence as described below will elucidate and provide support for the role of HPA-HA dual-polymer eye drops.
Preclinical and Clinical Studies of HPG-HA Dual-Polymer Lubricant Eye Drops in the Management of DED
A literature search was performed in PubMed to identify preclinical and clinical studies reporting the efficacy and safety of HPG-HA dual-polymer lubricant eye drops in relieving the signs and symptoms of DED. The following predefined search strings were used.
1. ((Dry eye) OR (dry eye syndrome) OR DES OR (dry eye disease) OR DED) AND ((artificial tears) OR (lubricant) OR (lubricant eye drops))
2. ((Dry eye) OR (dry eye syndrome) OR DES OR (dry eye disease) OR DED) AND ((artificial tears) OR (lubricant) OR (lubricant eye drops) OR (eye drops)) AND ((Systane Hydration) OR (polyethylene glycol 400) OR (PEG 400) OR (polyethylene glycol) OR PEG OR (propylene glycol) OR PG OR (HP guar) OR (hydroxypropyl guar) OR HPG)
3. ((Dry eye) OR (dry eye syndrome) OR DES OR (dry eye disease) OR DED) AND ((artificial tears) OR (lubricant) OR (lubricant eye drops) OR (eye drops)) AND ((Systane Hydration) OR (polyethylene glycol 400) OR (PEG 400) OR (polyethylene glycol) OR PEG OR (propylene glycol) OR PG OR (HP guar) OR (hydroxypropyl guar) OR HPG) AND ((hyaluronic acid) OR (sodium hyaluronate))
4. ((Dry eye) OR (dry eye syndrome) OR DES OR (dry eye disease) OR DED) AND ((polyethylene glycol 400) OR (PEG 400) OR (polyethylene glycol) OR PEG) AND ((propylene glycol) OR PG) AND ((HP guar) OR (hydroxypropyl guar) OR HPG)
5. ((Dry eye) OR (dry eye syndrome) OR DES OR (dry eye disease) OR DED) AND ((polyethylene glycol 400) OR (PEG 400) OR (polyethylene glycol) OR PEG) AND ((propylene glycol) OR PG) AND ((HP guar) OR (hydroxypropyl guar) OR HPG) AND ((hyaluronic acid) OR (sodium hyaluronate))
6. ((Artificial tears) OR (lubricant) OR (lubricant eye drops) AND ((polyethylene glycol 400) OR (PEG 400) OR (polyethylene glycol) OR PEG)) AND ((propylene glycol) OR PG) AND ((HP guar) OR (hydroxypropyl guar) OR HPG)
7. ((Artificial tears) OR (lubricant) OR (lubricant eye drops) AND ((polyethylene glycol 400) OR (PEG 400) OR (polyethylene glycol) OR PEG) AND ((propylene glycol) OR PG) AND ((HP guar) OR (hydroxypropyl guar) OR HPG) AND ((hyaluronic acid) OR (sodium hyaluronate))
A flowchart detailing the literature screening strategy used for selecting publications for this review, along with the key inclusion and exclusion criteria, is shown in Figure 1. A total of 1111 articles in English published between January 01, 2010, and October 31, 2022, were identified using the search strings. After removing duplicates, 1015 articles were screened based on the inclusion and exclusion criteria. Of these, four relevant articles with preclinical and clinical evidence were included. Additionally, one article was identified through a Google search and was included (based on the same inclusion/exclusion criteria). Thus, five studies (two preclinical and three clinical) were reviewed and summarized, with consensus from all the authors.
Preclinical Evidence of HPG-HA Dual-Polymer Lubricating Eye Drops
Increased Protection Against Desiccation, Cell Barrier Protection, and Lubricity in Corneal Epithelial Cells
An in vitro study assessed the efficacy of HPG-HA dual-polymer lubricating eye drops versus control and single polymer formulations containing either HPG alone or HA alone in models of the human corneal epithelium (Table 1).22 HPG-HA dual-polymer provided significantly greater (p < 0.001) protection against desiccation as compared with media control, HPG alone, and HA alone, immediately after treatment (cell viability, 53.6% ± 10.7%) as well as after rinsing of the solution (cell viability, 44.4% ± 12.5%) (Table 1). These results indicate that HPG/HA dual-polymer eye drops provide protection against desiccation through cell hydration and surface retention in corneal cells.
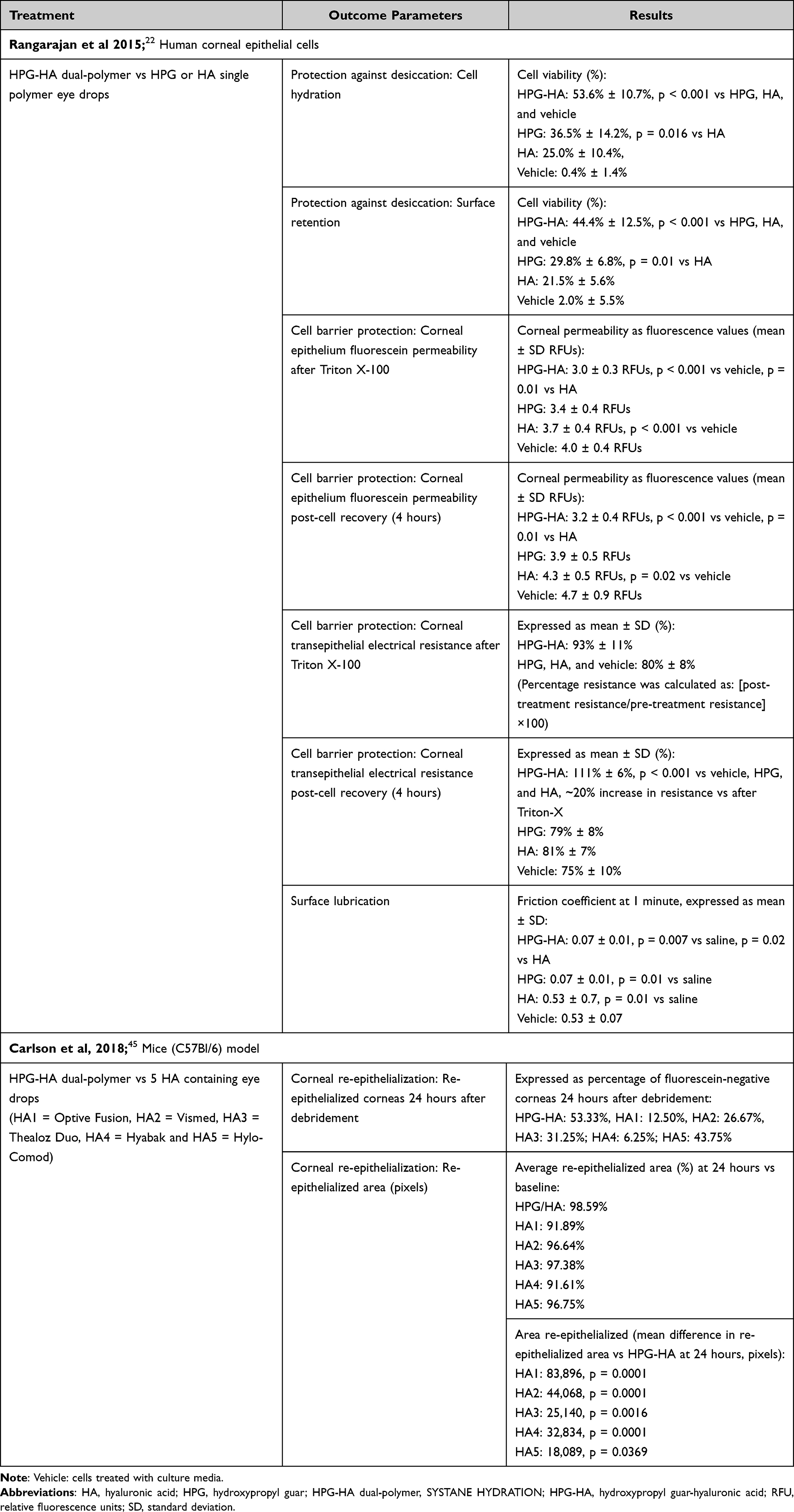 |
Table 1 Preclinical Studies on the Efficacy of HPG-HA Dual-Polymer Lubricant Eye Drops in DED Management |
Fluorescein permeability immediately after surfactant (Triton X-100) exposure was significantly lower in HPG-HA dual-polymer pretreated cells (3.0 ± 0.3 RFUs) when compared with media control (p < 0.001) and HA alone (p = 0.01); a similar trend was observed after 4 hours of recovery. Furthermore, the transepithelial electrical resistance after Triton X-100 exposure was similar across cells pretreated with HPG-HA dual-polymer, HA alone, HPG alone, and media control; however, after 4 hours of recovery, the resistance was significantly higher (p < 0.001) in cells pretreated with HPG-HA dual-polymer (111% ± 6%) than in the media control, HPG alone, and HA alone. After Triton X-100 exposure, considerably more viable cells were observed with the HPG-HA dual-polymer than with the media control, HPG alone, and HA alone (Table 1). These findings demonstrate higher cell barrier protection from surfactant exposure by the dual- polymer than by single polymer solutions.
Simulated blinking in bovine pericardial tissue showed that HPG-HA dual-polymer, HPG alone, and HA alone significantly reduced friction compared with saline (p ≤ 0.01 for all).22 Further, HPG-HA dual-polymer reduced friction to a greater extent as compared with HA alone (0.07 ± 0.01 vs 0.53 ± 0.7; p = 0.02) and also maintained lubricity post-rinsing of the solution. This finding demonstrates the effective and prolonged lubrication provided by the dual-polymer.
Increased Corneal Re-Epithelialization in an in-vivo Corneal Injury Model
A preclinical study compared the effect of HPG-HA dual-polymer lubricating eye drops versus other HA-containing eye drops (Optive Fusion™, Vismed®, Thealoz Duo®, Hyabak®, and Hylo-Comod®) on corneal re-epithelialization post-injury, in an in vivo mouse model (Table 1).45 HPG-HA dual-polymer lubricating eye drops showed the highest corneal re-epithelialization rate (fluorescein-negative corneas, 53.3%), 24 hours after epithelial debridement, as compared with the other five HA-containing eye drops. Furthermore, HPG-HA dual-polymer lubricating eye drops demonstrated a significantly higher average area and percentage area (98.6%) of re-epithelialization than the other HA-containing drops evaluated (all p < 0.05) (Table 1). These results suggest the role of dual-polymer in corneal wound healing.
Clinical Evidence of HPG-HA Dual-Polymer Lubricating Eye Drops
Reduction in Clinical Signs of Dry Eye in Patients with Dry Eye Disease
In a prospective, double-masked, parallel-group, randomized, noninferiority trial (NCT02470429), the efficacy and safety of HPG-HA dual-polymer lubricating eye drops were compared with an artificial tear formulation containing HA (Hyabak 0.15%) in patients with DED.14 Patients (n = 99) aged ≥18 years with a TOSS score ≥4 and ≤9 were randomized 1:1 to receive either HPG-HA or HA treatment, 4 times per day (1 drop in each eye) for 42 days. Changes from baseline on day 42 in TOSS, the impact of dry eye symptoms on everyday life (IDEEL) treatment satisfaction (effectiveness and inconvenience) scores, and tear film breakup time (TFBUT) were evaluated. A reduction was observed in mean TOSS scores (from baseline at day 42) in both treatment groups; however, the mean change from baseline was higher in HPG-HA dual-polymer lubricating eye drops than 0.15% HA eye drops (least square mean ± standard error [LSM ± SE]: −1.16 ± 0.24 vs −0.92 ± 0.23; treatment difference [95% CI], −0.24 [−0.90 to 0.42]; p = 0.476) (Table 2). Thus, the HPG-HA dual-polymer was found to be non-inferior to 0.15% HA eye drops (upper limit of 95% CI <2 units) in reducing the clinical signs of DED.
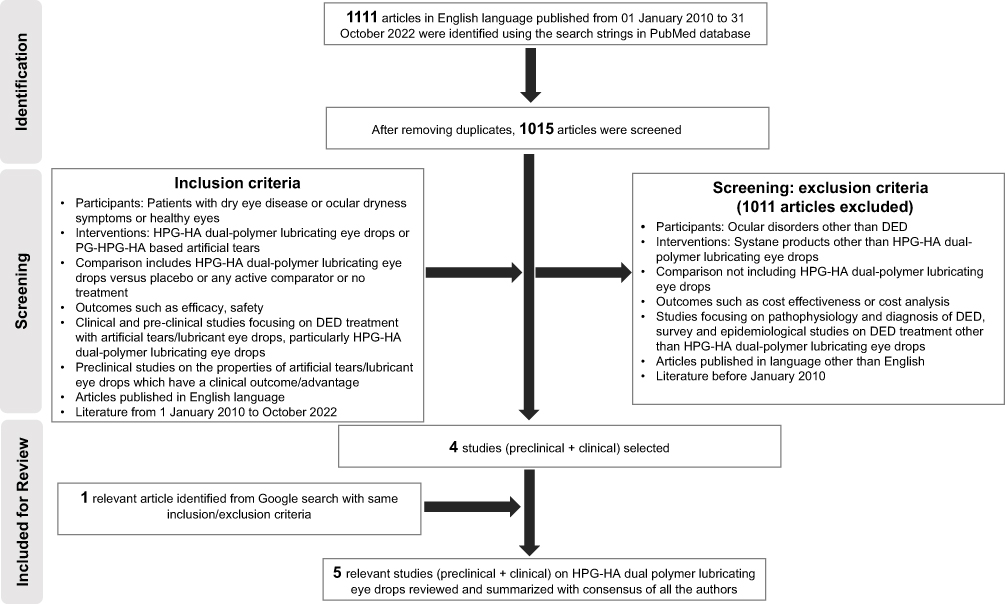 |
Figure 1 Flow chart of literature screening strategy, with key inclusion and exclusion criteria used for the selecting publications for this review. Abbreviations: DED, dry eye disease; HA, hyaluronic acid; HPG, hydroxypropyl guar; PG, propylene glycol; HPG-HA dual-polymer lubricating eye drops, SYSTANE Hydration. |
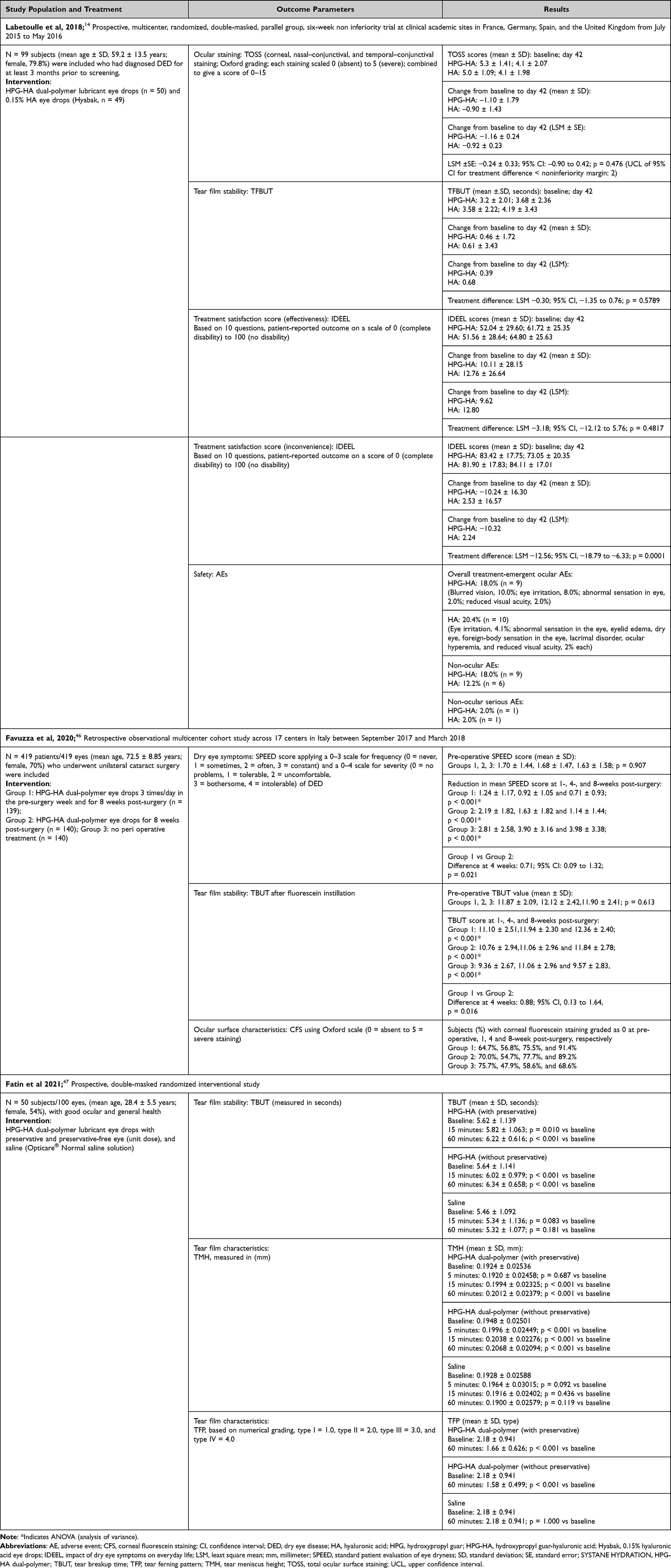 |
Table 2 Clinical Studies on the Efficacy of HPG-HA Dual-Polymer Lubricant Eye Drops in DED Management |
Improvement in the IDEEL treatment effectiveness score on day 42 (from baseline) was similar for HPG-HA and HA eye drops (LSM: 9.62 vs 12.80; treatment difference [95% CI], −3.18 [−12.12 to 5.76]; p = 0.4817). However, the IDEEL treatment inconvenience scores were lower (ie, more disability) for HPG-HA than for HA eye drops (LSM: −10.32 vs 2.24; treatment difference [95% CI], −12.56 [−18.79 to −6.33]; p = 0.0001) (Table 2). The higher treatment inconvenience observed with HPG-HA eye drops was hypothesized to be related to the transient blurred vision experienced by some patients upon instillation of eye drops with high viscosity (dual-polymer). Improvement in TFBUT values at day 42 (from baseline) was similar for HPG-HA and HA eye drops (LSM: 0.39 vs 0.68 seconds; treatment difference [95% CI], −0.30 [−1.35 to 0.76]; p = 0.5789). Transient blurred vision was the most frequently reported treatment-related adverse event with HPG-HA compared with HA eye drops. However, no major differences were observed in the frequency of ocular treatment-emergent adverse events between the HPG-HA dual-polymer and 0.15% HA eye drops (18.0% vs 20.4%), and no new safety findings were reported with the use of the HPG-HA dual-polymer lubricating eye drops (Table 2). The HPG-HA dual-polymer was well tolerated and safe in patients with DED.
Reduction in Post-Cataract Surgery Dry Eye Symptoms and Signs
A retrospective, observational, multicenter cohort study evaluated the efficacy of perioperative use of HPG-HA dual-polymer lubricant eye drops in preventing DED post-cataract surgery.46 Data of patients (n = 419) who had undergone unilateral cataract surgery and were not affected by DED previously were analyzed. Patients were divided into three groups based on the perioperative lubricating regimens used: those who had instilled HPG-HA drops (3 times/day) both pre-operatively for 1 week and post-operatively for 8 weeks, those who had only instilled HPG-HA drops post-operatively for 8 weeks, and those who had not instilled any peri-operative artificial tears. Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire scores, fluorescein TBUT, and corneal fluorescein staining scores were evaluated pre-operatively, and post-operatively at 1, 4, and 8 weeks (Table 2).
SPEED questionnaire scores were stable after surgery in the two groups treated with HPG-HA drops but increased significantly in the non-treated group, especially at week 4 (p < 0.001). Furthermore, the SPEED scores were significantly lower in the two groups treated with HPG-HA drops than in the non-treated group throughout the post-operative period (all p < 0.05). The group with both pre-operative and post-operative use of the HPG-HA drops had significantly lower SPEED scores than the group with post-operative use of drops alone, at week 1 (1.24 ± 1.17 vs 2.19 ± 1.82; p < 0.001) and week 4 (0.92 ± 1.05 vs 1.63 ± 1.82; p = 0.021) post-operatively. In the non-treated group, 25% of the patients reported mild-to-moderate dry eye symptoms at 4 and 8 weeks post-surgery (Table 2). These results suggest that the HPG-HA dual-polymer reduces ocular discomfort post-cataract surgery, especially when administered pre-operatively.
TBUT was significantly reduced (p < 0.001) 1 week after surgery compared with the pre-operative values in all three groups, but the differences were not clinically significant in the two groups treated with HPG-HA. TBUT returned to pre-operative values faster in the HPG-HA group pre- and post-operatively than in the group treated only post-operatively (week 4 vs week 8); however, TBUT remained significantly lower throughout the post-operative period in the non-treated group (p < 0.001). TBUT was significantly higher in the two groups treated with HPG-HA drops than in the non-treated group throughout the post-operative period (all p < 0.001). Furthermore, the group with both pre- and post-operative use of HPG-HA drops had a significantly higher TBUT than the group with post-operative use of drops alone at week 4 (11.94 ± 2.30 vs 11.06 ± 2.96; p = 0.016; not clinically significant) post-operatively (Table 2). These results suggest that the HPG-HA dual-polymer reduces tear film instability post-cataract surgery, particularly when administered pre-operatively. Furthermore, SPEED scores were inversely correlated with TBUT scores at week 8, indicating good correspondence between the signs and symptoms of DED.
The percentage of patients with no corneal fluorescein staining (Grade 0) was higher in the two groups treated with the HPG-HA dual-polymer than in the non-treated group throughout the post-operative period (Table 2); these results indicate less corneal damage and inflammation in patients treated with the HPG-HA dual-polymer following cataract surgery.
Improvement in Tear Film Quality in Subjects with Healthy Eyes
A prospective, randomized, double-masked study evaluated the short-term effect of HPG-HA dual-polymer lubricant eye drops (preserved and preservative-free formulations) compared with saline on tear film characteristics in subjects with normal eyes. TBUT, tear meniscus height (TMH), and tear ferning pattern (TFP) were evaluated in 50 subjects at baseline and up to 60 minutes after instillation.47 HPG-HA dual-polymer lubricant eye drops had high viscosity, with the preservative-free eye drops being more viscous than the preserved one (32.73 cP vs 26.70 cP; saline: 0.71 cP) (Table 2). The pH of both eye drop formulations was slightly basic (preserved, 7.85; preservative-free, 7.74; saline, 6.64). The pH of normal tears is 6.5 to 7.6. Both formulations of HPA-HA dual-polymer eye drops significantly increased TBUT at 15 minutes (preserved: 5.82 ± 1.063, p = 0.010; preservative-free: 6.02 ± 0.979, p < 0.001) and 60 minutes (preserved: 6.22 ± 0.616, p < 0.001; preservative-free: 6.34 ± 0.658, p < 0.001) post-instillation, whereas TBUT decreased in normal saline at 15 and 60 minutes post-instillation. These results indicated an increase in tear film stability with the dual-polymer. Similarly, significant improvements in TMH from baseline were observed with both preservative-free (5 minutes, 0.1996; 15 minutes, 0.2038; 60 minutes, 0.2068; p < 0.001 for all) and preserved (15 minutes, 0.1994; 60 minutes, 0.2012; p < 0.001 for both) formulations of HPA-HA dual-polymer eye drops; however, no significant changes were observed at 5 minutes after instillation of eye drops and with saline. These findings indicate an increase in TMH with a higher viscosity. TFP was significantly improved with both HPA-HA dual-polymer eye drop formulations at 60 minutes post-instillation (p < 0.001); however, no change was observed in the saline group (Table 2). Overall, both formulations of HPG-HA dual-polymer eye drops improved the tear film quality.
Other Reports on HPG-HA Dual-Polymer Lubricating Eye Drops
A prospective, single-center, randomized, double-masked, three-arm study evaluated the subjective responses of participants (N = 24; aged 23–40 years) to the filling solutions in the application of miniscleral contact lenses.48 The study compared the effects of instilling HPG/HA eye drops or PG-HPG nanoemulsion (SYSTANE Complete) drops into the lenses before filling with saline or filling with saline alone (control). General linear mixed model analysis demonstrated that improvement in dryness symptoms was faster with HPG/HA eye drops (estimate ± standard error [SE], −1.13 ± 0.56, p = 0.049) or with PG-HPG nanoemulsion eye drops (estimate ± SE, −1.69 ± 0.58, p = 0.005) than with saline alone. Approximately 50% of the subjects treated with the PG-HPG nanoemulsion and 42% treated with HPG/HA drops showed the greatest improvement in dryness 5 min after lens application, whereas subjects treated with saline alone showed the greatest improvement in dryness only at 4 hours.
The PG-HPG nanoemulsion eye drops were also effective in improving other symptoms (fluctuating vision, grittiness/burning/stinging, and foreign body sensation [all p < 0.05]) more quickly than saline alone, whereas the HPG/HA eye drops showed no significant improvement (all p < 0.05). There were no significant differences in subjective scores between treatments or over time for comfort, vision quality, facial recognition, and overall satisfaction (p > 0.05).
Overall, HPG/HA dual-polymer lubricating eye drops improved symptoms of dryness after application of miniscleral contact lenses and, hence, may be helpful in improving adaptation to miniscleral lenses.
A prospective, randomized, comparative study49 by Pastor-Pascual et al evaluated the effects of HPG/HA dual-polymer lubricating eye drops and CMC sodium-containing eye drops (Viscofresh) in subjects undergoing treatment with intravitreal injections of anti-vascular endothelial growth (anti-VEGF). OSDI, dry eye questionnaire-5 (DEQ-5), TMH, non-invasive keratograph tear breakup time (NIKBUT), vision breakup time (VBUT), meibography, and mean redness score were evaluated in subjects with age-related macular degeneration (N = 34; aged 51–88 years). The subjects were treated with one intravitreal injection per month (on days 0, 30, and 60) and were randomized (1:1) at baseline to receive either HPG/HA (n = 16) or CMC (n = 18) eye drops. The patients were instructed to instill the assigned eye drops 3 times a day for 30 days during the second month.
Mixed models for repeated measures showed no significant differences in the parameters (OSDI, DEQ-5, TMH, NIKBUT, redness, VBUT and meibography; p > 0.05) assessed in the study between no treatment versus treatment with either eye drops. However, the OSDI and DEQ-5 showed a trend towards lower values across the study, indicating their potential for future studies. The parameters of OSDI, DEQ-5, TMH, and meibography were not affected by the type of treatment (HPG/HA vs CMC eye drops) or the time of treatment (day 30 to day 60) but depended on the starting value (ie, value at day 30). In contrast, NIKBUT first and VBUT increased over time, regardless of the type of treatment (HPG/HA vs CMC eye drops) and the starting value (ie, at day 30). Thus, the results indicate that artificial tears may help to maintain tear film stability and thus improve the QoL in patients receiving anti-VEGF intravitreal treatment.
A 2-week study50 by Pucker et al evaluated the QoL of digital device users treated with HPG/HA dual-polymer lubricating eye drops (NCT04837807). The study recruited participants (N = 30, aged >18 years) who used digital devices (eg, computers, tablets, or smartphones) for ≥8 hours per day and had an Impact of Dry Eye on Everyday Life (IDEEL) Quality of Life (QoL) work domain score ≤80, and an OSDI questionnaire score of 13–32. Subjects attended three visits and were randomized to receive either HPA-HA dual-polymer preservative-free unit-dose or multi-dose eye drops for 1 week and switched to the alternative dosing in the second week. Subjects were instructed to use eye drops ≥4 times per day in each eye. Subjects completed the IDEEL-QoL and OSDI questionnaires at each visit. Comfort was evaluated using a visual analogue scale (VAS) of 0–100 on days 1–5, week 1, and week 2 visits. Dispensing system preferences (unit- or multi-dose) were evaluated using a Likert questionnaire.
Subjects reported significant improvements in VAS eye comfort upon waking and while they used the digital devices (start/mid/end of the day) (all p ≤ 0.003). Similarly, the IDEEL questionnaire (daily activities, feelings, and work) and OSDI scores improved significantly at week 2 (all p < 0.0001). Overall, a higher percentage of subjects (55%) preferred using the unit-dose HPG-HA dual-polymer eye drops than the multi-dose (45%) dispensing system. Overall, the results suggest that HPG-HA dual-polymer lubricating preservative-free eye drops provide symptomatic relief and improve QoL in digital device users with dry eye symptoms.
Summary
The management of DED is challenging due to the multifactorial and chronic nature of the disease. Artificial tears provide temporary relief from DED symptoms and have evolved as an integral part of DED management. Aqueous-based tears contain demulcents that improve corneal surface wettability and provide lubrication to the ocular surface, thereby relieving the symptoms of DED. HPG-HA dual-polymer lubricating eye drops, which utilize the action of the two polymers, support the retention of demulcents, protect the ocular surface, and provide lubrication to the ocular surface. Additionally, dual-polymer eye drops possess excellent hygroscopic and viscoelastic properties that help with water retention, protect against desiccation, reduce friction during blinks (lubrication), and promote corneal re-epithelialization.
Clinical medical evidence demonstrates the effects of HPG-HA dual-polymer lubricating eye drops in reducing the signs and symptoms of DED. These drops have also been demonstrated to be effective in reducing dry eye symptoms post-cataract surgery, particularly if instilled pre-operatively. Furthermore, HPG-HA dual-polymer lubricating eye drops (with and without preservative) have been shown to improve tear film quality in healthy eyes. Although HPG-HA dual-polymer eye drops are well tolerated, some patients may experience transient blurred vision immediately upon instillation due to the high viscosity of the eye drops.
Other reports on HPG-HA dual-polymer lubricating eye drops suggest that it relieves ocular dryness after application of miniscleral contact lenses and can help maintain tear film stability in patients undergoing anti-VEGF intravitreal treatment. Furthermore, HPG-HA dual-polymer preservative-free eye drops have been shown to provide symptomatic relief and improve the QoL of digital device users with dry eye symptoms.
Overall, based on the available preclinical and clinical evidence, HPG-HA dual-polymer lubricating eye drops are well tolerated, safe and effective in the management of dry eye symptoms. It also improved ocular health, tear film stability and integrity and QoL in patients with DED.
Acknowledgments
Writing, editorial, and formatting assistance were provided by Aru Singh, PhD, and Sudha Korwar, PhD, from Indegene Pvt. Ltd., which was contracted and funded by Alcon. Alcon was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Author Contributions
All authors have made a significant contribution to the work reported in the conception, study design, execution, and interpretation; took part in drafting, revising, and critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
Writing, editorial support, and formatting assistance were provided by Indegene Pvt. Ltd, which was contracted and funded by Alcon.
Disclosure
The authors are employees of Alcon. The authors received no direct compensation for the development of this manuscript. The authors declare that they have no other conflicts of interest in this work.
References
1. Pflugfelder SC, de Paiva CS. The Pathophysiology of Dry Eye Disease: what We Know and Future Directions for Research. Ophthalmology. 2017;124(11):S4–S13. doi:10.1016/j.ophtha.2017.07.010
2. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
3. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
4. Barabino S, Benitez-Del-Castillo JM, Fuchsluger T, et al. Dry eye disease treatment: the role of tear substitutes, their future, and an updated classification. Eur Rev Med Pharmacol Sci. 2020;24(17):8642–8652. doi:10.26355/eurrev_202009_22801
5. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
6. Lemp MA, Baudouin C, Baum J, et al. The definition and classification of dry eye disease: report of the definition and classification subcommittee of the international Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):75–92. doi:10.1016/s1542-0124(12)70081-2
7. Jones L, Downie LE, Korb D, et al. TFOS DEWS II Management and Therapy Report. Ocul Surf. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
8. Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II Report Executive Summary. Ocul Surf. 2017;15(4):802–812. doi:10.1016/j.jtos.2017.08.003
9. Módis L, Szalai E. Dry eye diagnosis and management. Expert Rev Ophthalmol. 2011;6(1):67–79. doi:10.1586/eop.10.89
10. Pucker AD, Ng SM, Nichols JJ. Over the counter (OTC) artificial tear drops for dry eye syndrome. Cochrane Database Syst Rev. 2016;2016(2). doi:10.1002/14651858.CD009729.pub2
11. Labetoulle M, Benitez-Del-castillo JM, Barabino S, et al. Artificial Tears: biological Role of Their Ingredients in the Management of Dry Eye Disease. Int J Mol Sci. 2022;23(5). doi:10.3390/ijms23052434
12. Agarwal P, Craig JP, Rupenthal ID. Formulation considerations for the management of dry eye disease. Pharmaceutics. 2021;13(2):1–19. doi:10.3390/pharmaceutics13020207
13. Labetoulle M, Messmer EM, Pisella PJ, Ogundele A, Baudouin C. Safety and efficacy of a hydroxypropyl guar/polyethylene glycol/propylene glycol-based lubricant eye-drop in patients with dry eye. Br J Ophthalmol. 2017;101(4):487–492. doi:10.1136/bjophthalmol-2016-308608
14. Labetoulle M, Schmickler S, Galarreta D, et al. Efficacy and safety of dual-polymer hydroxypropyl guar-and hyaluronic acid-containing lubricant eyedrops for the management of dry-eye disease: a randomized double-masked clinical study. Clin Ophthalmol. 2018;12:2499–2508. doi:10.2147/OPTH.S177176
15. Moon SW, Hwang JH, Chung SH, Nam KH. The impact of artificial tears containing hydroxypropyl guar on mucous layer. Cornea. 2010;29(12):1430–1435. doi:10.1097/ICO.0b013e3181ca636b
16. Posarelli C, Passani A, Del Re M, et al. Cross-Linked Hyaluronic Acid as Tear Film Substitute. J Ocul Pharmacol Ther. 2019;35(7):381–387. doi:10.1089/jop.2018.0151
17. Schmidl D, Schmetterer L, Witkowska KJ. Tear Film Thickness After Treatment With Artificial Tears in Patients With Moderate Dry Eye Disease. Cornea. 2015;34(4):421–426. doi:10.1097/ICO.0000000000000358
18. Park Y, Song JS, Choi CY, Yoon KC, Lee HK, Kim HS. A Randomized Multicenter Study Comparing 0.1%, 0.15%, and 0.3% Sodium Hyaluronate with 0.05% Cyclosporine in the Treatment of Dry Eye. J Ocul Pharmacol Ther. 2017;33(2):66–72. doi:10.1089/jop.2016.0086
19. Systane Hydration drug facts. Available from: https://fda.report/DailyMed/8936f66f-10fe-44ab-a26e-dd8b05dfa997.
20. Jones L, Ngo W, Yeh T SYSTANE ® HYDRATION PF’s Dual-Polymer Technology: hydroxypropyl-Guar and Sodium Hyaluronate [White Paper]. Available from: Https://Us.Alconscience.Com/Sites/g/Files/Rbvwei1736/Files/Pdf/SYSTANE-HYDRATION-PFs-Dua.
21. Aragona P, Simmons PA, Wang H, Wang T. Physicochemical Properties of Hyaluronic Acid-Based Lubricant Eye Drops. Transl Vis Sci Technol. 2019;8(6):2. doi:10.1167/tvst.8.6.2
22. Rangarajan R, Kraybill B, Ogundele A, Ketelson HA. Effects of a Hyaluronic Acid/Hydroxypropyl Guar Artificial Tear Solution on Protection, Recovery, and Lubricity in Models of Corneal Epithelium. J Ocul Pharmacol Ther. 2015;31(8):491–497. doi:10.1089/jop.2014.0164
23. Bitton E, Perugino C, Charette S. Comparison of Ocular Lubricant Osmolalities. Optom Vis Sci. 2017;94(6):694–699. doi:10.1097/OPX.0000000000001082
24. Springs CL. Novel hydroxypropyl-guar gellable lubricant eye drops for treatment of dry eye. Adv Ther. 2010;27(10):681–690. doi:10.1007/s12325-010-0052-3
25. Benelli U. Systane® lubricant eye drops in the management of ocular dryness. Clin Ophthalmol. 2011;5(1):783–790. doi:10.2147/OPTH.S13773
26. Garofalo R, Kunnen C, Rangarajan R, Manoj V, Ketelson H. Relieving the symptoms of dry eye disease: update on lubricating eye drops containing hydroxypropyl-guar. Clin Exp Optom. 2021;104(8):826–834. doi:10.1080/08164622.2021.1925208
27. Ng A, Keech A, Jones L. Tear osmolarity changes after use of hydroxypropyl-guar-based lubricating eye drops. Clin Ophthalmol. 2018;12:695–700. doi:10.2147/OPTH.S150587
28. Yeu E, Silverstein S, Guillon M, et al. Efficacy and safety of phospholipid nanoemulsion-based ocular lubricant for the management of various subtypes of dry eye disease: a Phase IV, multicenter trial. Clin Ophthalmol. 2020;14:2561–2570. doi:10.2147/OPTH.S261318
29. Davitt WF, Bloomenstein M, Christensen M, Martin AE. Efficacy in patients with dry eye after treatment with a new lubricant eye drop formulation. J Ocul Pharmacol Ther. 2010;26(4):347–353. doi:10.1089/jop.2010.0025
30. Fernandez KB, Epstein SP, Raynor GS, et al. Modulation of HLA -DR in dry eye patients following 30 days of treatment with a lubricant eyedrop solution. Clin Ophthalmol. 2015;9:1137–1145. doi:10.2147/OPTH.S81355
31. Fallacara A, Baldini E, Manfredini S, Vertuani S. Hyaluronic acid in the third millennium. Polymers (Basel). 2018;10(7). doi:10.3390/polym10070701
32. Lõpez-García JS, García-Lozano I, Rivas L, Ramírez N, Raposo R, Méndez MT. Autologous serum eye drops diluted with sodium hyaluronate: clinical and experimental comparative study. Acta Ophthalmol. 2014;92(1). doi:10.1111/aos.12167
33. Hynnekleiv L, Magno M, Vernhardsdottir RR, et al. Hyaluronic acid in the treatment of dry eye disease. Acta Ophthalmol. 2022;100(8):844–860. doi:10.1111/aos.15159
34. Rah MJ. A review of hyaluronan and its ophthalmic applications. Optometry. 2011;82(1):38–43. doi:10.1016/j.optm.2010.08.003
35. Szegedi S, Scheschy U, Schmidl D, et al. Effect of Single Instillation of Two Hyaluronic Acid-Based Topical Lubricants on Tear Film Thickness in Patients with Dry Eye Syndrome. J Ocul Pharmacol Ther. 2018;34(9):605–611. doi:10.1089/jop.2018.0069
36. Seino S, Matsuoka R, Masuda Y, Kunou M, Okada Y, Saika S. Topical hyaluronan alone promotes corneal epithelial cell migration whereas combination with benzalkonium chloride impairs epithelial wound healing. Cutan Ocul Toxicol. 2020;39(1):13–20. doi:10.1080/15569527.2019.1673402
37. Walsh K, Jones L. The use of preservatives in dry eye drops. Clin Ophthalmol. 2019;13:1409–1425. doi:10.2147/OPTH.S211611
38. Kim YH, Jung JC, Jung SY, Yu S, Lee KW, Park YJ. Comparison of the Efficacy of Fluorometholone With and Without Benzalkonium Chloride in Ocular Surface Disease. Cornea. 2015;35(2):234–242. doi:10.1097/ICO.0000000000000695
39. Goldstein MH, Silva FQ, Blender N, Tran T, Vantipalli S. Ocular benzalkonium chloride exposure: problems and solutions. Eye. 2022;36(2):361–368. doi:10.1038/s41433-021-01668-x
40. Gomes JAP, Azar DT, Baudouin C, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2017;15(3):511–538. doi:10.1016/j.jtos.2017.05.004
41. Hsu KH, Gupta K, Nayaka H, Donthi A, Kaul S, Chauhan A. Multidose Preservative Free Eyedrops by Selective Removal of Benzalkonium Chloride from Ocular Formulations. Pharm Res. 2017;34(12):2862–2872. doi:10.1007/s11095-017-2270-8
42. Kaarniranta K, Ropo A. Preferences and ease of use of preservative-free IOP-lowering eye drop containers: a comparison of two multi-dose bottles. Clin Investig. 2018;07(04). doi:10.4172/clinical-investigation.1000126
43. Davidson Z. Developing an efficient ophthalmic device combination product. ONdrugDelivery. 2020;2020(104):16–24.
44. SAIDANE, LP.B. How to deliver preservative-free eye drops in a multidose system with a safer alternative to filters ? Invest Ophthalmol Vis Sci. 2017;58,4460.
45. Carlson E, Kao WWY, Ogundele A. Impact of Hyaluronic Acid-Containing Artificial Tear Products on Reepithelialization in an In Vivo Corneal Wound Model. J Ocul Pharmacol Ther. 2018;34(4):360–364. doi:10.1089/jop.2017.0080
46. Favuzza E, Cennamo M, Vicchio L, Giansanti F, Mencucci R. Protecting the Ocular Surface in Cataract Surgery: the Efficacy of the Perioperative Use of a Hydroxypropyl Guar and Hyaluronic Acid Ophthalmic Solution. Clin Ophthalmol. 2020;14:1769–1775. doi:10.2147/OPTH.S259704
47. Che Arif FA, Hilmi MR, Mohd Kamal K, Ithnin MH. Comparison of Immediate Effects on Usage of Dual Polymer Artificial Tears on Changes in Tear Film Characteristics. IIUM Med J Malaysia. 2020;18(3 SE). doi:10.31436/imjm.v18i2.613
48. Tan J, Peguda R, Siddireddy JS, Briggs N, Stapleton F. Subjective Responses to Various Filling Solutions in the Posterior Fluid Reservoir of Miniscleral Lenses at Application. Eye Contact Lens. 2022;48(2):73–77. doi:10.1097/ICL.0000000000000855
49. Pastor-Pascual F, Pastor-Pascual R, Gálvez-Perez P, Dolz-Marco R, Gallego-Pinazo R. Use of Artificial Tears in Patients Undergoing Treatment with Anti-VEGF Intravitreal Injections. Clin Ophthalmol. 2022;16(November):3959–3972. doi:10.2147/OPTH.S391082
50. Pucker AD, Lievens C, McGwin G, Franklin QX, Logan A, Wolfe GS. Quality of Life in Digital Device Users Who are Treated with Systane Hydration PF. Clin Optom. 2023;15(March):45–54. doi:10.2147/opto.s398496
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Topical Omega-3 Polyunsaturated Fatty Acids for the Treatment of Dry Eye – Results from a Pilot Randomized Controlled Masked-Observer Study
Kaercher T, Messmer EM, Berninger T, Huber-van der Velden KK, Geiger R, Cipriano-Bonvin P, Jacobi C
Clinical Ophthalmology 2022, 16:4021-4031
Published Date: 8 December 2022
Artificial Tears: A Systematic Review
Semp DA, Beeson D, Sheppard AL, Dutta D, Wolffsohn JS
Clinical Optometry 2023, 15:9-27
Published Date: 10 January 2023
Quality of Life in Digital Device Users Who are Treated with Systane Hydration PF
Pucker AD, Lievens C, McGwin G Jr, Franklin QX, Logan A, Wolfe GS
Clinical Optometry 2023, 15:45-54
Published Date: 7 March 2023
Prevalence of Dry Eye Disease Among Individuals Scheduled for Cataract Surgery in a Norwegian Cataract Clinic
Graae Jensen P, Gundersen M, Nilsen C, Gundersen KG, Potvin R, Gazerani P, Chen X, Utheim TP, Utheim ØA
Clinical Ophthalmology 2023, 17:1233-1243
Published Date: 27 April 2023
Dry Eye Disease as a Cause of Refractive Errors After Cataract Surgery – A Systematic Review
Biela K, Winiarczyk M, Borowicz D, Mackiewicz J
Clinical Ophthalmology 2023, 17:1629-1638
Published Date: 6 June 2023