Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Does Voluntary Work Contribute to Cognitive Performance? – An International Systematic Review
Authors Keefer A ![]() , Steichele K, Graessel E, Prokosch HU, Kolominsky-Rabas PL
, Steichele K, Graessel E, Prokosch HU, Kolominsky-Rabas PL
Received 15 January 2023
Accepted for publication 9 March 2023
Published 25 April 2023 Volume 2023:16 Pages 1097—1109
DOI https://doi.org/10.2147/JMDH.S404880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anne Keefer,1 Kathrin Steichele,1 Elmar Graessel,2 Hans-Ulrich Prokosch,3 Peter L Kolominsky-Rabas1
1Interdisciplinary Center for Health Technology Assessment (HTA) and Public Health (IZPH), Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany; 2Department of Psychiatry and Psychotherapy, Center for Health Services Research in Medicine, Uniklinik Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany; 3Chair of Medical Informatics, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany
Correspondence: Anne Keefer, Friedrich-Alexander University Erlangen-Nürnberg (FAU), Interdisciplinary Centre for Health Technology Assessment (HTA) and Public Health, Schwabachanlage 6, Erlangen, 91054, Germany, Tel +49 9131 85-35855, Fax +49 9131 85-35854, Email [email protected]
Introduction: There is a need for knowledge on activities that can reduce cognitive decline and dementia risk. Volunteering is a productive activity that entails social, physical, and cognitive functions. Therefore, volunteering could be a protective factor for cognitive loss. Thus, this review aims to examine the associations between volunteering and volunteers’ cognition and to identify influencing variables.
Methods: Six international literature databases were searched for relevant articles published between 2017 and 2021 (ALOIS, CENTRAL, CINAL, Embase, PsycINFO, PubMed). Quantitative studies of all study designs were included. The primary outcome was the volunteers’ cognition measured by objective, internationally established psychometric function tests. Two authors independently assessed the eligibility and quality of the studies. A narrative synthesis was performed using all studies included in this review. The methodology was in line with the PRISMA guidelines.
Results: Fourteen studies met the inclusion criteria and were included. Seven of the included studies confirmed that volunteering positively affects the volunteers’ cognitive function. Two other studies identified an association between volunteer activity and volunteers’ cognition using cross-sectional measurements. In particular, women and people with a low level of education benefit from the positive effects and associations. The study quality of the included articles was moderate to weak.
Discussion: Our review suggests that volunteering can improve volunteers’ cognition. Unfortunately, little attention is given to specific volunteer activities and the frequency of engagement. Additionally, more attention is needed on various risk factors of cognitive impairment.
Keywords: cognitive health, social engagement, dementia prevention, health promotion
Introduction
Dementia is one of the most significant public health challenges facing today’s and future societies worldwide. Due to demographic change, the number of people with dementia more than doubled between 1990 and 2016.1 Currently, over 55 million people are affected by dementia, and 78 million people are expected to be diagnosed with dementia in 2030.2
Several risk factors contribute to the development of dementia, such as age and gender. Thus, the risk of dementia increases significantly with age, and women are more likely to develop dementia than men, especially between the ages of 80 to 99.3 Even geographic region has an impact on personal dementia risk, with higher prevalence rates in Europe and North America than in Asia, Africa, and South America.3 In addition, there are also modifiable risk factors. In early life, low education negatively affects cognitive reserve and can increase the risk of dementia by 7%.4,5 Especially in middle age, hearing loss, traumatic brain injury, hypertension, alcohol consumption, and obesity affect the incidence of dementia.4 But even in older age, some factors contribute to the cause of dementia. These include depression, social isolation, physical inactivity, smoking, air pollution, and diabetes.4 But research also discusses other potential risk factors for dementia, such as previous anesthesia in youth or stressful life events.6,7 If the three risk factors social isolation, physical inactivity, and depression are reduced in later life, the prevalence of dementia is expected to decrease by 13%.4 Volunteering is a promising approach to reducing these three important risk factors. Therefore volunteer work can be associated with better volunteer cognition.8–11
Based on estimates by the UN Volunteers, the worldwide number of volunteers is thought to be more than one billion.12 Cultural, regional, and national differences in volunteering are evident.13,14 They exist due to different value orientations and sociodemographic, socioeconomic, and political characteristics.13 The areas of volunteering are very heterogeneous. The frequency of volunteering can also vary widely. A systematic review of 40 studies reported from 30 minutes to 15 hours per week of volunteer frequency.9 It is important to note that volunteering too often can also lead to stress, which may lead to impaired cognitive function.15,16 In the context of the increasing prevalence of dementia, volunteer work in care and support for people with dementia and their caregivers is essential from a health policy perspective.
The first pathways between volunteering and cognition were first described by Fried et al17 This theory was later developed and generalized for all types of volunteer work by Anderson et al11 The basic idea is that volunteering affects different levels of cognitive, social, and physical activation depending on the characteristics of the volunteer activity. These activations stimulate various biological and psychosocial mechanisms, such as neurogenesis, self-efficacy, and physical health. This results in better psychosocial, physical, and cognitive functioning. This overall functional improvement should ultimately lead to a lower risk of dementia.11,17
Anderson et al published a critical review of the benefits of volunteering among seniors.11 Three studies identified significant effects of volunteer activity on various cognitive outcomes (mental status, memory, executive functioning, frontal lobe activity) measured by objective tests. The second review of this topic was made by Guiney & Machado.10 They searched for articles that assessed the relationship between volunteering and cognitive functions. Eleven of the fifteen included studies found significant associations of volunteering with global cognitive function or domain-specific functions.
Other reviews examined social activities, social contacts, or social leisure activities only in general, not explicitly concerning a particular social engagement, such as volunteering.18–20 Hence, this systematic review aims to build more robust evidence on the association between volunteering and the volunteers’ cognition.
Methods
This systematic review was conducted using the “Preferred Reporting Items for Systematic reviews and Meta-Analyses” (PRISMA) recommendations.21 In addition, the review was registered in PROSPERO (CRD42021246396).
Search Strategy
The following databases were searched to identify relevant articles: ALOIS, CENTRAL, CINAL, Embase, PsycINFO, and PubMed. To retrieve studies, the search term ((social engagement OR volunteer* OR voluntary OR productive activit* OR social activit*) AND (cognit* OR brain OR dementia)) was used. Qualitative studies, unpublished, or grey literature were excluded. Moreover, the search was limited to studies in German or English. The period was limited to published articles between January 2017 and April 2021 to provide an update on the existing evidence.
Study Selection
Two independent reviewers (AKE, KST) performed title and abstract screening. Based on this screening, the full text was considered if an article could not be excluded with certainty. For discrepancies, a third reviewer was consulted (PKR). We included all study designs of quantitative research that examined an association between volunteering and cognitive functions or dementia diagnosis. Volunteering was defined as a free, public welfare-oriented activity not directed towards material gain.22,23 We excluded research that 1) does not examine volunteering as a single factor, 2) does not explicitly measure volunteering, instead social activities in general, 3) does not examine cognitive functions or does not assess cognition by internationally established psychometric tests, 4) does not measure cognition as an outcome, but as a covariate. The age of study participants was not restricted.
Data Extraction
Information was extracted independently by two reviewers (AKE, KST). The following data on the study characteristics were collected: 1) author, 2) country, 3) database, 4) study design, 5) follow-up, 6) sample size, 7) percentage of volunteers, 8) setting, 9) assessment “volunteering”, 10) assessment “cognition”, and 11) results. The study participants were described with the following characteristics: 1) age, 2) sex, 3) frequency of volunteering, 4) cognitive status, 5) education, and 6) depressive symptoms. There was no process for obtaining or confirming data from study investigators.
Study Quality
Study quality was assessed with the “Quality Assessment Tool for Quantitative Studies” as recommended by the Cochrane Collaboration.24,25 Two independent reviewers did the study appraisal (AKE, KST).
Results
Included Studies
From an initial 17,040 articles, after removing duplicates and screening for eligibility, fourteen relevant studies were included in this systematic review. Figure 1 illustrates the PRISMA Flow Chart, demonstrating the study identification and screening process.
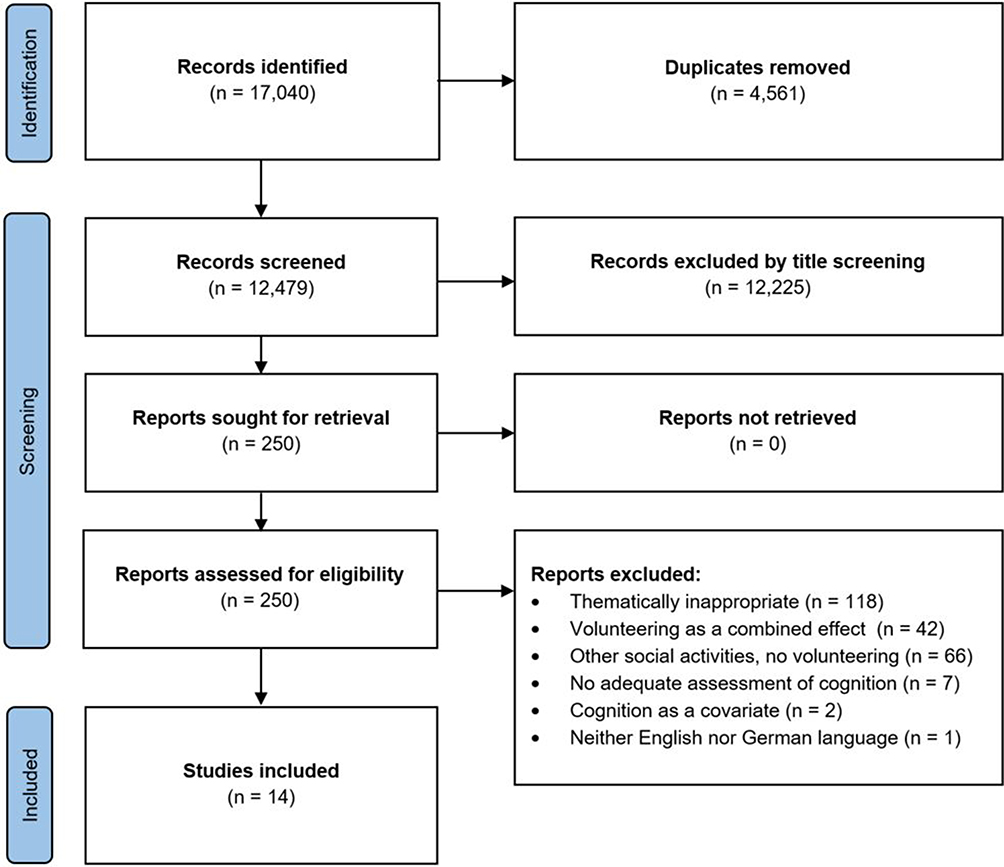 |
Figure 1 PRISMA Flow Chart illustrating the study selection process. Notes: PRISMA figure adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Medicine. 2009;6(7):e1000097. Creative Commons.21 |
Study Characteristics
Table 1 presents a detailed description of the study characteristics. All included studies are written in English. German studies could not be included. Most included articles are longitudinal studies,26–35 and only four of the articles are cross-sectional studies.36–39 Four studies are based in the USA, and all analyzed data from the US Health and Retirement Study. Three studies are based in Korea; two used the Korean National Longitudinal Study of Aging data. Further, one study each is based in Taiwan, Brazil, England, England/Scotland, New Zealand, China, and Japan.
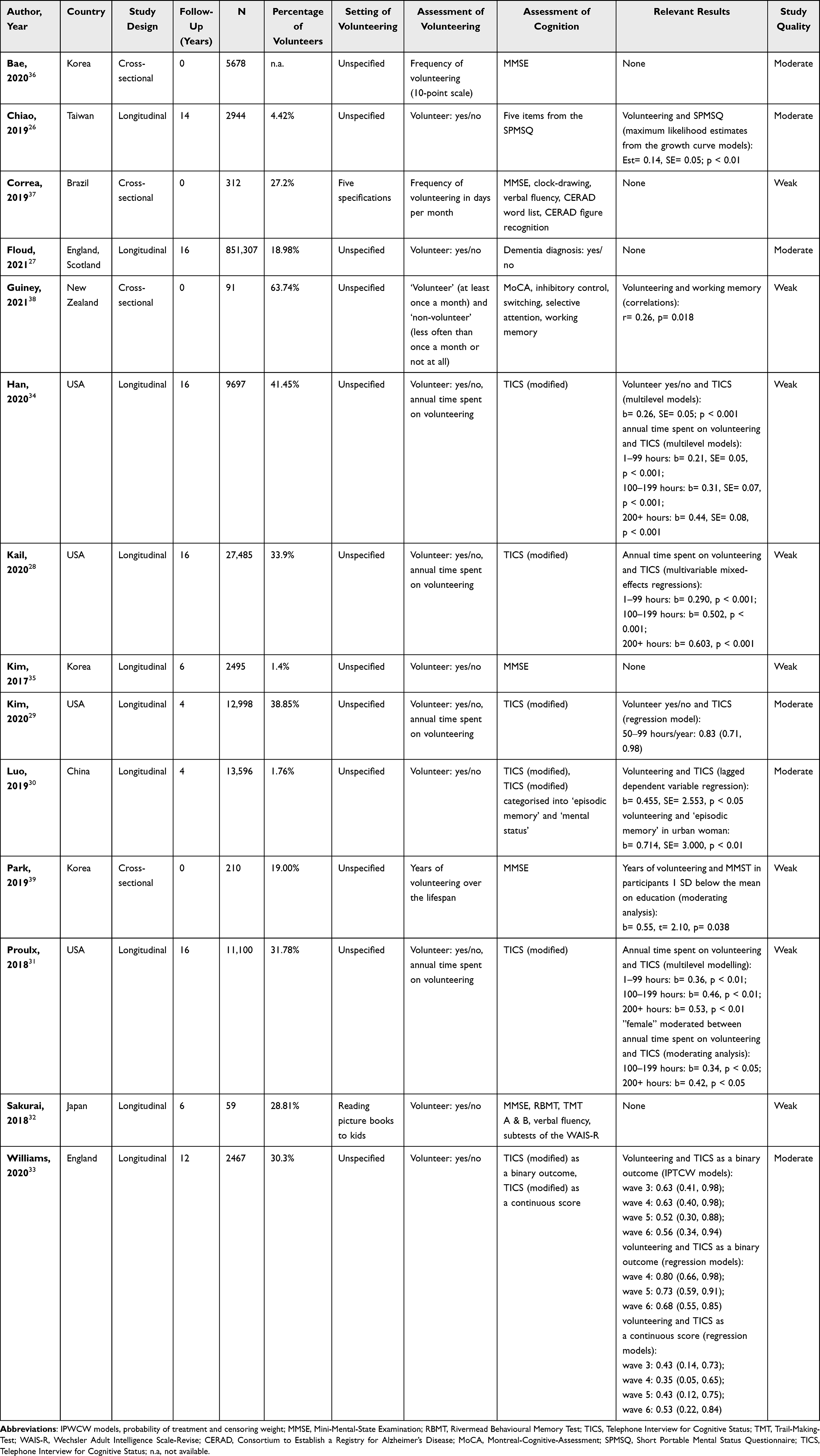 |
Table 1 Characteristics of Included Studies |
In total, ten studies are based on large cohort studies,26–31,33,34,36 three studies are observational studies,35,37–39 and one is an intervention study.32 The number of study participants varied from 5938 to 851,307.27 The volunteer setting was not specified in most cases. Only two studies analyzed specific volunteer settings. The first classified volunteering into six classifications (helping at church activities, creating handcrafts and sewing for those in need, helping needy families, visiting hospitals, visiting other institutions, and other types of volunteering).37 The second was an intervention study investigating reading (picture) books to (pre-) schoolchildren.32
Most studies assessed volunteer activities through a binary yes/no questionnaire,26,27,30,32,33,35 others used a combination of binary questionnaire and frequency of volunteering28,29,31,34,39 and others were limited to requesting the frequency of volunteer work.36,37,39 One study categorized persons as “volunteers” if they volunteered at least once a month. Others were classified as “non-volunteers” (volunteering less often than once a month or not at all).38 All studies used standardized psychometric tests to assess global cognition, with one exception that measured cognition based on an existing dementia diagnosis.27 Some studies also measured specific cognitive domains, eg working memory or verbal fluency.32,37,38 One of the included studies also measured hippocampal volume as a surrogate parameter for cognitive function.32
Six out of fourteen studies have moderate study quality,26,27,29,30,33,36 and the remaining studies have weak quality. The main reason for the poor study quality is not reporting dropouts/withdrawals. The assessment of study quality is presented in Appendix A1.
Synthesis
Table 2 presents a detailed description of the study participants regarding age, sex, frequency of volunteering, cognitive status, education, and depressive symptoms. The mean age of the study participants ranged from 61.23 ± 4.9327 to 74.14 ± 0.4939 years. Although age was not an exclusion criterion, the mean age was relatively high. Regarding sex, more women than men participated in all studies except one.26 In three studies, the proportion of women was especially high compared to men.27,32,37 Eight studies described the frequency of volunteering based on different periods. One study showed a very low frequency because no pre-selection of volunteers and non-volunteers was done, but all study participants provided a response.36 Another study reported a frequency of 1.25 ± 2.66 days per month, which is also be assumed to be low.37 Almost all studies with a percentage outcome described the largest proportion of study participants in the lower frequency range.28,31,34,39 Only one study described the largest proportion of study participants in the upper-frequency range of 200 or more hours volunteering per year.29 The participants’ cognitive status was measured in a cross-sectional design or at baseline in thirteen studies. One study assessed cognitive status only at follow-up.27 Another study collected the MMSE in a cross-sectional design, but the value cannot be reported using the published data.39 None of the studies reported a study population with identifiable cognitive impairment at baseline. In all studies, the level of education was surveyed. In one study, the education of study participants was collected but is not available based on published data.27 The total number of years of education ranged from 5.80 ± 2.5137 to 14.5 ± 3.5.38 But many studies collected years of education using other classifications. Participants’ depressive symptoms were assessed in eleven of the fourteen included studies. On average, the study participants in these studies showed no striking depressive symptoms. Some studies did not address other important risk factors for cognitive impairment. For example, five studies did not report the vascular burden in analyses.28,30,31,38,39 Also, hearing loss was only reported in three studies.33,35,37 Thus, eleven studies did not consider this important risk factor. The included studies did not consider other discussed risk factors, such as prior anesthesia or stressful events.
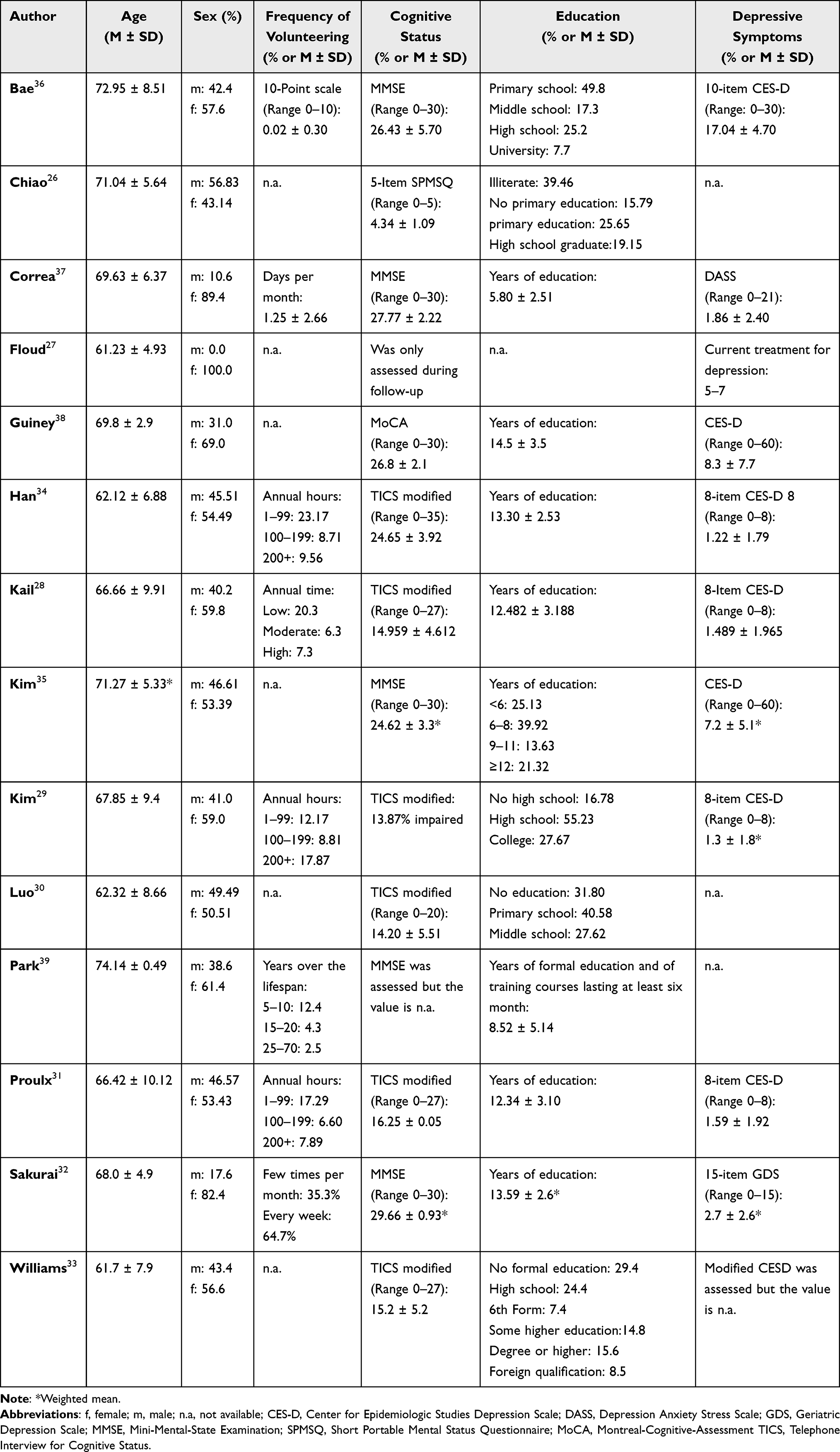 |
Table 2 Characteristics of Study Participants |
Impact of Volunteering on Global Cognitive Functions
Based on eight studies, volunteering is positively related to global cognitive function.26,28–31,33,34,39 In contrast, six of the included studies could not identify any relationship between volunteering and global cognitive ability.26,27,32,35,37,38 An influencing factor is the frequency of volunteering. On the one hand, three studies showed that the impact of volunteering on global cognitive functioning increases with the number of days volunteering per year.28,31,34 On the other hand, another study demonstrates that volunteering only shows a health-promoting effect on cognition at a frequency of 50–99 hours per year. No effects are seen with more or fewer hours per year.29 Furthermore, it makes a difference whether volunteers are female or male. Two studies indicated that women, in particular, benefit from the positive influence of volunteer activities on global cognition.30,31 In addition to frequency and sex, education also plays a crucial role. One study identified a stronger association between volunteering and cognition for persons with below-average levels of education.31 This finding is supported by another study, which found that only people with below-average education showed significant results, whereas people with above-average education did not show any positive effect of volunteering on the volunteers’ cognition.39
Impact of Volunteering on Domain-Specific Cognitive Functions
Significant associations were also established concerning specific cognitive domains in one study. A cross-sectional study assessed four domain-specific functions (inhibitory control, switching, selective attention, and working memory). Only one cognitive domain, working memory, was positively related to volunteering. No other cognitive domains showed significant associations.38 Another cross-sectional study investigated different cognitive domains using a variety of tests, eg, clock-drawing test, verbal fluency test, and word and figure recognition test. In the unadjusted model, there were several correlations, but after adjusting for different variables (eg, social support and resilience), no significant results were found.37 This study identified that altruistic behavior, rather than volunteering, is related to cognitive health.37 Two other studies that assessed different types of domain-specific cognitive functions could not identify any significant associations with volunteer activities.32,37
Discussion
This review examined associations between volunteer work and volunteers’ cognition. In total, nine out of fourteen studies identified a relationship between volunteering and cognition. The results suggest that volunteering can improve volunteers’ cognition, but the data are too heterogeneous for a clear statement. To our knowledge, this is the first systematic review focusing on objective, internationally accepted psychometric instruments for measuring cognitive performance.
The majority of our included studies are longitudinal studies, which have the potential to assess the impact of volunteering on cognition. In one longitudinal study that showed no significant effect, the survey of cognition might be the reason.27 In this study, the (non-) presence of a dementia diagnosis, not cognitive abilities, was assessed. Therefore, comparing this study with the other included studies is more difficult.
In our review, we identified four cross-sectional studies, with two describing an association between volunteering and cognition. One of the cross-sectional studies without relevant results surveyed volunteer activity on a scale, so how many study participants volunteered is not apparent.36 As the total sample in this study reported a low frequency of volunteering, an insufficient sample of volunteers could be the reason for missing results. A previous systematic review reported that most cross-sectional studies showed significant associations.10 This could indicate that the cross-sectional correlation between cognition and volunteering is lower than previously thought. The positive association might be more noticeable after a few years of volunteering. Of course, cross-sectional studies cannot determine the causality of the relationship. Accordingly, there could be a positive correlation, as people with a higher cognitive level are likelier to choose voluntary work than those cognitively impaired.
The included studies were conducted in eight different countries. Despite the significant differences in value orientations and socio-demographic, socio-economic, and political characteristics, no country-specific differences in the association between volunteering and cognition can be identified. More detailed information from the study participants is lacking to conclude statements about cultural differences.
Impact of Frequency
Concerning the frequency of volunteering, the studies are showing inconsistent results. It remains unclear whether “the more, the better” has an important influence on volunteer cognition. More frequent volunteering appears to have more positive effects on cognition, but other results suggest that volunteering, regardless of the frequency, has positive effects. Even Guiney & Machado suggest that it might be more important to do any volunteering than the amount of time spent doing it.10 They included in their review a study that only found a relationship in the binary assessment of volunteering (yes/no), while no relationship was found in the continuous assessment.10,40 We included a study in our review that confirms this theory.33 Based on the regression model, an association was only found in the binary assessment of volunteer activity (yes/no). In contrast, no connection was found in the continuous assessment. Our results also suggest that if the frequency of volunteering is too high, the positive effects on cognition may stop.29 Various stress mechanisms might be responsible for this.
Impact of Sex
Additionally, the results indicate that women, in particular, benefit from volunteering in terms of cognitive health. Large community-based studies support this finding that this review could not include.41,42 In both studies, the proportion of men and women was not balanced, with more women involved. The studies in our review that support this hypothesis included men and women in almost equal proportions (male= 49.49%, female= 50.51%;30 male= 46.57%, female= 53.43%31). Thus, the risk of selection bias is low due to a larger proportion of women in one of the groups. In general, the prevalence of dementia is higher in women than men. Therefore volunteering for dementia prevention has a great need and potential, especially among women.
Impact of Education
Two of the included studies show that people with a low level of education especially benefit from the positive effect of volunteering on cognition. This finding might be due to a low level of initial cognitive skills. As individuals with low education are at increased risk for dementia, volunteering could prevent or delay the risk of developing cognitive deficits and dementia, especially for this highly vulnerable group. The previous reviews on this topic have not yet been able to establish such a connection.10,11 Therefore, volunteering for better cognitive functioning can be particularly promoted in countries with lower levels of education.
Limitations
Due to the inclusion and exclusion criteria, some studies were not included in the analyses because they did not meet the criteria. Nevertheless, these could complement the existing evidence and provide further information. For example, one included study showed that hippocampal volume declines more slowly in volunteers than in non-volunteers. As the measurement of hippocampal volume is not an internationally established psychometric function test of cognition, this exciting result could not be included in our review.
The overall study quality measured by the Quality Assessment Tool for Quantitative Studies can be classified as moderate to weak. The relevance of the individual studies could therefore be limited due to methodological weaknesses. Moreover, in four studies, the US Health and Retirement Study was used for various research questions. Significant effects were identified in all four studies. Two other studies refer to the same database. Both studies were based on the Korean Longitudinal Study of Aging and cannot show significant results. There is a risk of selection bias in both cases because the samples were exposed to specific cultural or even socio-economic parameters.
Since almost all studies did not define volunteering precisely, it is impossible to guarantee our definition. For example, it cannot be ruled out with certainty whether there is no intention aimed at a material gain by volunteering in our included studies.
Furthermore, the included studies did not assess the volunteering setting detailed enough. Only two of the included studies describe the specific type of volunteering. Therefore, it is not known which volunteering setting is related to better cognitive functions. In addition, the frequency of volunteering is only sometimes requested. Moreover, it is poorly comparable because the frequency data were collected differently. Therefore, no recommendations can be made on the frequency of volunteering.
Positive associations between volunteering and cognition were only analyzed in study participants with an average age between 61 and 74 years. The results are therefore limited to this age group only.
Most included studies controlled outcomes for important risk factors such as age, sex, depressive symptoms, or education. However, many other risk factors for the development of cognitive impairment were not comprehensively considered in the analyses. Therefore, the results may be biased regarding unobserved risk factors, such as vascular burden or hearing loss. Independent of volunteer activity, these factors can affect cognitive abilities.
Conclusion
The fourteen included studies show very different characteristics and a moderate to weak study quality. Study participants are older, tend to volunteer less frequently, have different levels of education, and show no striking signs of depressive symptoms or cognitive impairment at baseline.
Our review supports and adds to current research that volunteer work relates to volunteers’ cognition. Therefore, volunteering should be strengthened more, not only as a benefit for society itself but also can provide cognitive abilities. On the one hand, people who already have dementia are supported in their everyday lives so that they can stay at home for longer. In addition, the burden on caregivers can be reduced. On the other hand, the volunteers’ cognition can be improved, which might lead to a lower cognitive decline.
The benefits of volunteering seem to be higher in women and people with a low level of education. In these population groups, volunteering can be promoted more intensively with the benefits for cognition. However, others should also know that volunteering is associated with better cognitive skills, making performing volunteer work even more attractive.
Since previous research has hardly examined the volunteer setting, future research should also examine this aspect. There is a wide range of volunteer activities, for example, in social, cultural, political, or ecological areas. The different volunteering settings have varying effects on cognitive, social, and physical activation. Thus, it can be assumed that certain volunteer activities influence cognition more than others. In addition, research has not focused on the frequency of volunteering. Therefore, the frequency of volunteering should be considered in future studies so that a minimum and a maximum number of volunteer hours per week/month/year can be recommended.
Some important risk factors are already considered in studies on this topic. However, more risk factors should be analyzed in future studies to ensure that the results are not affected by unobserved influencing factors.
Acknowledgments
The present work was performed by Anne Keefer in (partial) fulfillment of the requirements for obtaining the degree ‘Dr. rer. biol. hum.’ at the Medical Faculty of the Friedrich-Alexander-Universität Erlangen-Nürnberg.
Funding
This work was supported by the Bavarian State Ministry of Health and Care (StMGP) as part of the funding initiative “BAYERN DIGITAL II” (grant number G42d-G8300-2017/1606-83, project “Digital Dementia Registry Bavaria – digiDEM Bayern”). The authors are grateful to the participating experts and study participants of digiDEM Bayern.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nichols E, Szoeke CE, Vollset SE, et al. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18(1):88–106. doi:10.1016/S1474-4422(18)30403-4
2. Gauthier S, Rosa-Neto P, Morais JA, Webster C. World Alzheimer report 2021-journey through the diagnosis of dementia. Alzheimers Dis Int. 2021;314:1.
3. Cao Q, Tan -C-C, Xu W, et al. The prevalence of dementia: a systematic review and meta-analysis. J Alzheimers Dis. 2020;73(3):1157–1166. doi:10.3233/JAD-191092
4. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–446.
5. Meng X, D’arcy C. Education and dementia in the context of the cognitive reserve hypothesis: a systematic review with meta-analyses and qualitative analyses. PLoS One. 2012;7(6):e38268. doi:10.1371/journal.pone.0038268
6. Tsolaki M, Sia E, Giannouli V. Anesthesia and dementia: an up-to-date review of the existing literature. Appl Neuropsychol. 2022;2022:1–10.
7. Giannouli V, Tsolaki M. Stressful life events, general cognitive performance, and financial capacity in healthy older adults and Alzheimer’s disease patients. Neuropsychiatrie. 2023. doi:10.1007/s40211-022-00451-y
8. Milbourn B, Saraswati J, Buchanan A. The relationship between time spent in volunteering activities and quality of life in adults over the age of 50 years: a systematic review. Br J Occup Ther. 2018;81(11):613–623. doi:10.1177/0308022618777219
9. Jenkinson CE, Dickens AP, Jones K, et al. Is volunteering a public health intervention? A systematic review and meta-analysis of the health and survival of volunteers. BMC Public Health. 2013;13(1):773. doi:10.1186/1471-2458-13-773
10. Guiney H, Machado L. Volunteering in the community: potential benefits for cognitive aging. J Gerontol Series B. 2018;73(3):399–408. doi:10.1093/geronb/gbx134
11. Anderson ND, Damianakis T, Kröger E, et al. The benefits associated with volunteering among seniors: a critical review and recommendations for future research. Psychol Bull. 2014;140(6):1505. doi:10.1037/a0037610
12. Davis C. Global Synthesis Report - Plan of Action to Integrate Volunteering into the 2030 Agenda. United Nation Volunteers; 2020.
13. Aydinli A, Bender M, Chasiotis A. Helping and volunteering across cultures: determinants of prosocial behavior. ORPC. 2013;5(3):6. doi:10.9707/2307-0919.1118
14. Randle M, Dolnicar S. Does cultural background affect volunteering behavior? J Nonprofit Public Sect Mark. 2009;21(2):225–247. doi:10.1080/10495140802529649
15. Liu Z, Li T, Li P, et al. The Ambiguous relationship of oxidative stress, tau hyperphosphorylation, and autophagy dysfunction in Alzheimer’s DISEASE. Oxid Med Cell Longev. 2015;2015:352723. doi:10.1155/2015/352723
16. Yaribeygi H, Panahi Y, Sahraei H, Johnston TP, Sahebkar A. The impact of stress on body function: a review. EXCLI J. 2017;16:1057–1072. doi:10.17179/excli2017-480
17. Fried L, Carlson M, Freedman M, et al. A social model for health promotion for an aging population: initial evidence on the experience corps model. J Urban Health. 2004;81:64–78. doi:10.1093/jurban/jth094
18. Kelly ME, Duff H, Kelly S, et al. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: a systematic review. Syst Rev. 2017;6(1):1–18. doi:10.1186/s13643-017-0632-2
19. Penninkilampi R, Casey A-N, Singh MF, Brodaty H. The association between social engagement, loneliness, and risk of dementia: a systematic review and meta-analysis. J Alzheimers Dis. 2018;66(4):1619–1633. doi:10.3233/JAD-180439
20. Yates LA, Ziser S, Spector A, Orrell M. Cognitive leisure activities and future risk of cognitive impairment and dementia: systematic review and meta-analysis. Int Psychogeriatr. 2016;28(11):1791–1806. doi:10.1017/S1041610216001137
21. Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
22. Enquete Commission. Civic Engagement: Towards a Sustainable Civil Society Civil Society. German Parliament; 2002.
23. US Bureau of Labor Statistics. Volunteering in the United States - 2015. In: Bureau of Labor Statistics. United States Department of Labor Washington, DC; 2016.
24. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration; 2011.
25. Effective Public Health Practice Project. Quality Assessment Tool for Quantitative Studies. Hamilton: Effective Public Health Practice Project; 1998.
26. Chiao C. Beyond health care: volunteer work, social participation, and late-life general cognitive status in Taiwan. Soc Sci Med. 2019;229:154–160. doi:10.1016/j.socscimed.2018.06.001
27. Floud S, Balkwill A, Sweetland S, et al. Cognitive and social activities and long-term dementia risk: the prospective UK Million Women Study. Lancet Public Health. 2021;6(2):e116–e123. doi:10.1016/S2468-2667(20)30284-X
28. Kail BL, Carr DC. More than selection effects: volunteering is associated with benefits in cognitive functioning. J Gerontol Series B. 2020;75(8):1741–1746. doi:10.1093/geronb/gbaa101
29. Kim ES, Whillans AV, Lee MT, Chen Y, VanderWeele TJ. Volunteering and subsequent health and well-being in older adults: an outcome-wide longitudinal approach. Am J Prev Med. 2020;59(2):176–186. doi:10.1016/j.amepre.2020.03.004
30. Luo Y, Pan X, Zhang Z. Productive activities and cognitive decline among older adults in China: evidence from the China health and retirement longitudinal study. Soc Sci Med. 2019;229:96–105. doi:10.1016/j.socscimed.2018.09.052
31. Proulx CM, Curl AL, Ermer AE. Longitudinal associations between formal volunteering and cognitive functioning. J Gerontol. 2018;73(3):522–531. doi:10.1093/geronb/gbx110
32. Sakurai R, Ishii K, Sakuma N, et al. Preventive effects of an intergenerational program on age‐related hippocampal atrophy in older adults: the REPRINTS study. Int J Geriatr Psychiatry. 2018;33(2):e264–e272. doi:10.1002/gps.4785
33. Williams BD, Pendleton N, Chandola T. Cognitively stimulating activities and risk of probable dementia or cognitive impairment in the English longitudinal study of ageing. SSM Popul Health. 2020;12:100656. doi:10.1016/j.ssmph.2020.100656
34. Han SH, Roberts JS, Mutchler JE, Burr JA. Volunteering, polygenic risk for Alzheimer’s disease, and cognitive functioning among older adults. Soc Sci Med. 2020;253:112970. doi:10.1016/j.socscimed.2020.112970
35. Kim D, Arai H, Kim S. Social activities are associated with cognitive decline in older Koreans. Geriatr Gerontol Int. 2017;17(8):1191–1196.
36. Bae SM. The association between health‐related factors, physical and mental diseases, social activities, and cognitive function in elderly Koreans: a population‐based cross‐sectional study. Psychogeriatrics. 2020;20(5):654–662. doi:10.1111/psyg.12561
37. Correa JC, Avila MPW, Lucchetti ALG, Lucchetti G. Altruistic behaviour, but not volunteering, has been associated with cognitive performance in community-dwelling older persons. Psychogeriatrics. 2019;19(2):117–125. doi:10.1111/psyg.12372
38. Guiney H, Keall M, Machado L. Volunteering in older adulthood is associated with activity engagement and cognitive functioning. Aging Neuropsychol Cogn. 2021;28(2):253–269. doi:10.1080/13825585.2020.1743230
39. Park S, Choi B, Choi C, Kang JM, Lee J-Y. Relationship between education, leisure activities, and cognitive functions in older adults. Aging Ment Health. 2019;23(12):1651–1660.
40. Herrera AP, Meeks TW, Dawes SE, et al. Emotional and cognitive health correlates of leisure activities in older Latino and Caucasian women. Psychol Health Med. 2011;16(6):661–674. doi:10.1080/13548506.2011.555773
41. Tomioka K, Kurumatani N, Hosoi H. Social participation and cognitive decline among community-dwelling older adults: a community-based longitudinal study. J Gerontol. 2016;73(5):799–806.
42. Carlson MC, Kuo JH, Chuang Y-F, et al. Impact of the Baltimore experience corps trial on cortical and hippocampal volumes. Alzheimers Dis Assoc. 2015;11(11):1340–1348. doi:10.1016/j.jalz.2014.12.005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.