Back to Journals » Journal of Pain Research » Volume 16
Does the Association Between Psychosocial Factors and Opioid Use After Elective Spine Surgery Differ by Sex in Older Adults?
Authors Aglio LS ![]() , Mezzalira E, Corey SM, Fields KG, Hauser BM, Susano MJ, Culley DJ, Schreiber KL
, Mezzalira E, Corey SM, Fields KG, Hauser BM, Susano MJ, Culley DJ, Schreiber KL ![]() , Kelly-Aglio NJ, Patton ME, Mekary RA
, Kelly-Aglio NJ, Patton ME, Mekary RA ![]() , Edwards RR
, Edwards RR
Received 4 April 2023
Accepted for publication 1 August 2023
Published 18 October 2023 Volume 2023:16 Pages 3477—3489
DOI https://doi.org/10.2147/JPR.S415714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Linda S Aglio,1,2,* Elisabetta Mezzalira,2,3,* Sarah M Corey,1 Kara G Fields,1 Blake M Hauser,4 Maria J Susano,5 Deborah J Culley,1 Kristin L Schreiber,1 Nicole J Kelly-Aglio,2 Megan E Patton,1 Rania A Mekary,2,6 Robert R Edwards1
1Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women’s Hospital, Boston, MA, USA; 2Computational Neurosurgical Outcome Center, Department of Neurosurgery, Brigham and Women’s Hospital, Boston, MA, USA; 3Department of Diagnostics and Public Health, University of Verona, Verona, Italy; 4Harvard-Massachusetts Institute of Technology Program in Health Sciences and Technology, Cambridge, MA, USA; 5Department of Anesthesiology, Emergency and Critical Care, Centro Hospitalar do Porto, Porto, Portugal; 6School of Pharmacy, Massachusetts College of Pharmacy and Health Sciences (MCPHS) University, Boston, MA, USA
*These authors contributed equally to this work
Correspondence: Linda S Aglio, Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women’s Hospital, Boston, MA, USA, Tel +1-617-732-8280, Fax +1-617-264-5230, Email [email protected]
Purpose: Psychosocial disorders have been linked to chronic postoperative opioid use and the development of postoperative pain. The potential interaction between sex and psychosocial factors with respect to opioid use after elective spine surgery in the elderly has not yet been evaluated. Our aim was to assess whether any observed association of anxiety or depression indicators with opioid consumption in the first 72 hours after elective spine surgery varies by sex in adults ≥ 65 years.
Patients and Methods: Secondary analysis of a retrospective cohort of 647 elective spine surgeries performed at Brigham and Women’s Hospital, July 1, 2015–March 15, 2017, in patients ≥ 65. Linear mixed-effects models were used to test whether history of anxiety, anxiolytic use, history of depression, and antidepressant use were associated with opioid consumption 0– 24, 24– 48, and 48– 72 post surgery, and whether these potential associations differed by sex.
Results: History of anxiety, anxiolytic use, history of depression, and antidepressant use were more common among women (51.3% of the sample). During the first 24 hours after surgery, men with a preoperative history of anxiety consumed an adjusted mean of 19.5 morphine milligram equivalents (MME) (99.6% CI: 8.1, 31.0) more than men without a history of anxiety; women with a history of anxiety only consumed an adjusted mean 2.9 MME (99.6% CI: − 3.1, 8.9) more than women without a history of anxiety (P value for interaction between sex and history of anxiety < 0.001). No other interactions were detected between sex and psychosocial factors with respect to opioid use after surgery.
Conclusion: Secondary analysis of this retrospective cohort study found minimal evidence that the association between psychosocial factors and opioid consumption after elective spine surgery differs by sex in adults ≥ 65.
Keywords: opioids, pain, psychosocial, sex anxiety, depression
Introduction
Spine procedures are among the most frequent surgeries performed in the United States and among the procedures requiring more pain management medication after surgery.1 Postoperative pain following spine procedures is a common complaint, with persistent pain even after the immediate convalescent period, which can lead to negative impacts on health.2,3 The adult population over 65 years has various comorbidities related to age, lifestyle and genetics; they are at notable risk for experiencing worth outcomes.4 Indeed, this issue may become increasingly important, considering that the number of people in the United States aged 65 years and over was estimated to be 49.2 million in 2016 and it is projected to increase to 78.2 million people in 2035.5
Psychosocial conditions, including anxiety, depression, and catastrophizing have been linked to the development of persistent pain as well as opioid use postoperatively.6–10 Recent studies suggest that elevated indices of distress such as anxiety, depression, catastrophizing, and enhanced sensitivity to pain are among the strongest predictors of persistent post-surgical pain and that these factors are stronger predictors than surgical variables.6,9 Such findings suggest that persistent postoperative pain is associated with psychosocial factors that may promote pain sensitization.8 Moreover, post-surgical pain is a risk factor for adverse opioid-related outcomes, including persistent opioid use and misuse.11 Several risk factors have been recognized, but tools to identify high-risk patients and preventive interventions are lacking.10,12 Therefore, even if physicians are encouraged to prescribe as few opioids as possible, it remains essential to properly control post-surgical pain, especially in the first 72 hours to prevent the development of chronic pain.
In spine surgery, opioid use has been associated with greater self-reported disability and poorer function for as long as 12 months following surgery.13 Sex differences have emerged in risk factors for persistent pain and opioid use after surgery; for example, women have a higher prevalence of anxiety and depression than men and also reported more severe pain than men for a variety of clinical conditions.14,15 However, in a recent study, preoperative anxiety and depression scores have demonstrated to be better predictors of severe postoperative pain among men compared to women.16 Failure to control for these comorbid conditions may partially explain differences in pain experiences between men and women and the divergent findings among clinical studies investigating relationships between pain experience, opioid use and gender.
Recent reviews highlight the fact that known risk factors for poor outcomes after spine surgery (eg, preoperative anxiety, depression, opioid use) are unevenly distributed between men and women,17 and given that we know relatively little about the potential interactions between sex and psychosocial factors with respect to postoperative opioid use, further study is warranted to understand whether men or women patients require greater doses of opioids to ameliorate pain from standard surgical procedures, especially in the geriatric population.
In this secondary analysis of a retrospective cohort study, our aim was to assess whether any observed association of anxiety or depression indicators (history of anxiety, history of depression, anxiolytic use, antidepressant use) with our primary outcome of opioid consumption 0–24, 24–48, and 48–72 hours after elective spine surgery varies by sex in adults 65 years and older. Secondary outcomes included highest pain severity and average pain severity 0–24, 0–24, 24–48, and 48–72 hours postoperatively. Our primary hypothesis was that the association of anxiety or depression indicators with opioid consumption 0–24, 24–48, and 48–72 hours after elective spine surgery differs by sex.
Materials and Methods
Samples
This research was a secondary analysis of a retrospective cohort study that assessed the association between perioperative variables and the development of delirium in 716 men and women 65 years of age and older who underwent cervical, thoracic, lumbar, or sacral/pelvic spine surgery at the Brigham and Women’s Hospital between July 1, 2015, and March 15, 2017.18
The current study analyzed the subset of 647 patients from this cohort who underwent elective surgery and had all exposure variables of interest recorded. All patients underwent general anesthesia. Regional anesthesia was not provided to any patients. The Mass General Brigham Institutional Review Board (IRB) approved this study of existing medical records and waived the need for patient consent. This manuscript was written in accordance with the STROBE statement19 and complies with the Declaration of Helsinki.
Measures
Our four exposures of interest were preoperative history of anxiety, anxiolytic use, history of depression, and antidepressant use as documented in the pre-admission anesthesia evaluation note. Preoperative history was defined as any point in the patient’s lifetime, based on the patient report during the pre-admission anesthesia evaluation or as documented in the electronic medical record. History of anxiety, anxiolytic use, history of depression, and antidepressant use were systematically asked to all patients during the pre-op visit, regardless of gender. Patient sex, as documented in the medical record, was tested for interactions with these anxiety and depression indicators. Additional patient and surgical characteristics included as model covariates were age, BMI, American Society of Anesthesiologist (ASA) Physical Status Classification Index (a risk-stratifying system used to help predict preoperative risks; the system is used to assess a patient’s preoperative comorbid conditions and assigns a class ranging from 1 to 6), surgical invasiveness category (defined following the classification developed by Armaghani et al for surgical invasiveness20,21 with tier 1: microdiscectomy, tier 2: lumbar laminectomy, anterior cervical procedures, or minimally invasive spinal fusions, tier 3: standard or complex lumbar fusion, emergency surgery following trauma, or posterior cervical fusion procedures, and tier 4: surgeries to ameliorate tumor, infection, or deformity, or combined anterior and posterior cervical procedures), reoperation, and preoperative opioid use. The primary study outcome was opioid consumption expressed in intravenous morphine milligram equivalents (MME) 0–24, 24–48, and 48–72 hours postoperatively. Secondary outcomes included highest numeric rating scale (NRS) pain score (0 to 10 scale) and average NRS pain score 0–24, 24–48, and 48–72 hours postoperatively.
Statistical Analysis
The magnitude and direction of differences in patient and surgical characteristics between patients with and without each of the four anxiety and depression indicators and between men and women were quantified as standardized differences.22 Standardized differences with a magnitude greater than or equal to 0.1 were taken to indicate a notable difference between groups.23 Linear mixed-effects models were used to test whether the four preoperative anxiety or depression indicators of interest were associated with opioid consumption (primary outcome) or the highest or average pain severity (secondary outcomes) at 0–24, 24–48, and 48–72 hours post spine surgery, and whether these associations differed by sex (ie, whether there were any interactions between sex and anxiety or depression indicators with respect to these outcomes). Mixed-effects models were employed to account for the correlation between repeated outcome measurements on the same patient. Each mixed-effects model included a random intercept for patient ID with a first-order autoregressive (AR[1]) correlation structure. A set of four models separately tested the association of each of the four preoperative anxiety and depression indicators with postoperative opioid consumption assuming these psychosocial factors have the same effect on outcomes across both sexes. These models included terms for preoperative history of anxiety (except when testing anxiolytic use), anxiolytic use (except when testing history of anxiety), history of depression (except when testing antidepressant use), antidepressant use (except when testing history of depression), age, BMI, ASA physical status, surgical invasiveness tier, reoperation, preoperative opioid use, postoperative timepoint, and an interaction between one of the anxiety or depression indicators and postoperative timepoint. To test whether the associations of preoperative anxiety and depression indicators with postoperative opioid consumption differ by sex, a second set of four models expanded upon the first set to include all two-way interactions between sex/anxiety or depression indicator/postoperative timepoint as well a three-way interaction term for sex by anxiety or depression indicator by postoperative timepoint. The potential interaction between sex and each of the four anxiety and depression indicators with respect to postoperative opioid consumption was tested at each of the three postoperative time points, resulting in 12 comparisons. The secondary outcomes of the highest and average NRS pain scores were evaluated in an identical manner to the opioid consumption primary outcome. All multivariable model residuals were approximately normally distributed. To account for 12 comparisons of interest per outcome, all hypothesis tests were evaluated at a Bonferroni-corrected two-sided alpha level of 0.05/12 = 0.004. All statistical analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC).
Results
A total of 753 patients over 65 years of age were identified who underwent spine surgery at Brigham and Women’s Hospital between July 1, 2015, and March 15, 2017. After exclusions, the final sample included 647 patients, including 51.3% women (Figure 1). Table 1 compares patient and surgical characteristics between patients with versus without each of the four anxiety and depression indicators and Supplementary Table 1 compares these characteristics between women and men. Patients with preoperative anxiety or depression indicators tended to be younger, women, and take opioids preoperatively (Table 1, Supplementary Table 1).
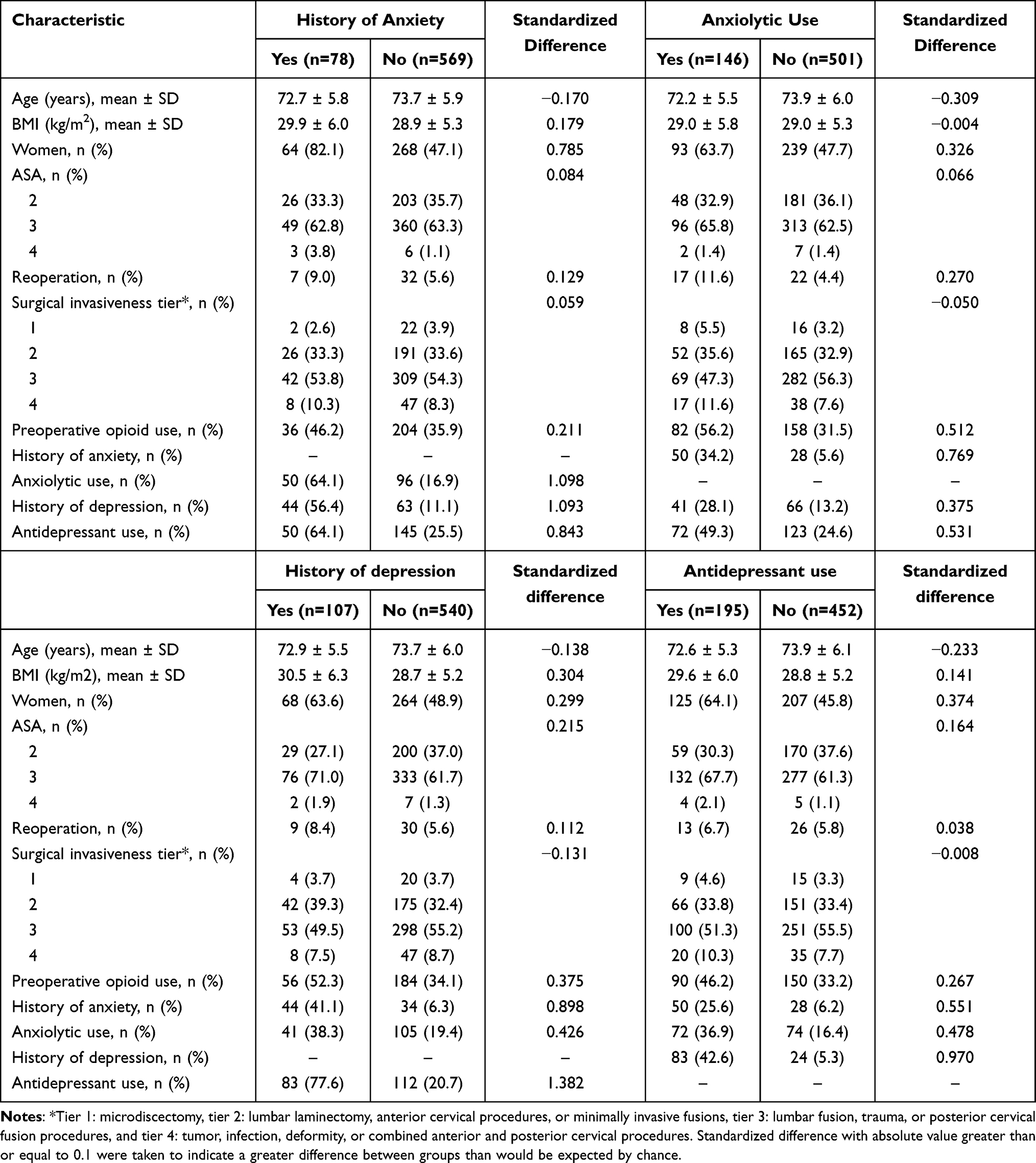 |
Table 1 Patient and Surgical Characteristics by Anxiety and Depression Indicators |
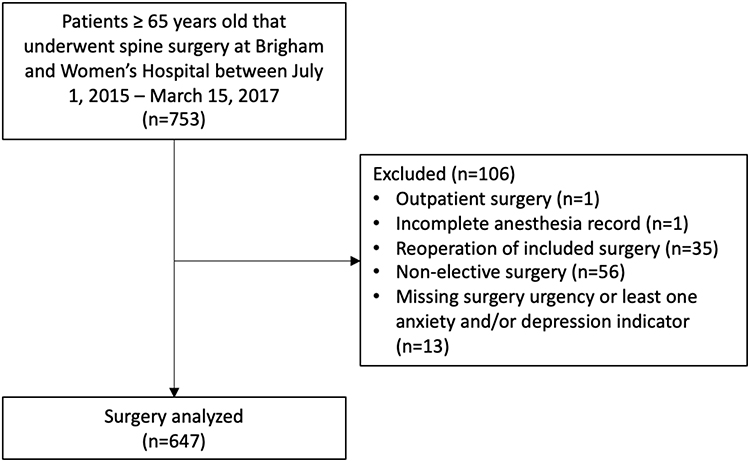 |
Figure 1 Patient inclusion flow diagram. |
Preoperative History of Anxiety
Preoperative history of anxiety was associated with an adjusted mean (99.6% confdence interval [CI]) 6.6 (1.1, 12.0) MME greater opioid consumption in men and women combined 0–24 hours post-surgery (Supplementary Table 2). No associations were detected between the preoperative history of anxiety and postoperative opioid consumption at 24–48 or 48–72 hours post-surgery, or with the highest or average pain severity at any postoperative time point (Supplementary Tables 2–4) In the subgroup analysis by sex, no association was detected between the preoperative history of anxiety and opioid consumption at 0–24 hours among women (adjusted difference in means [99.6% CI]: 2.9 [−3.1, 8.9] MME), but there was a strong association between preoperative history of anxiety and opioid consumption at 0–24 hours among men (adjusted difference in means [99.6% CI]: 19.5 [8.1, 31.0] MME) (Table 2 and Figure 2). When directly compared, the adjusted difference in mean opioid consumption (99.6% CI) between patients with and without a history of anxiety for women vs men was −16.6 (−29.2, −4.0) (P < 0.001 for the interaction between sex and history of anxiety) (Table 2 and Figure 2). No interactions between sex and history of anxiety with respect to postoperative opioid consumption at 24–48 or 48–72 hours post-surgery, or with the highest or average pain severity were detected at any postoperative time point (Tables 2–4).
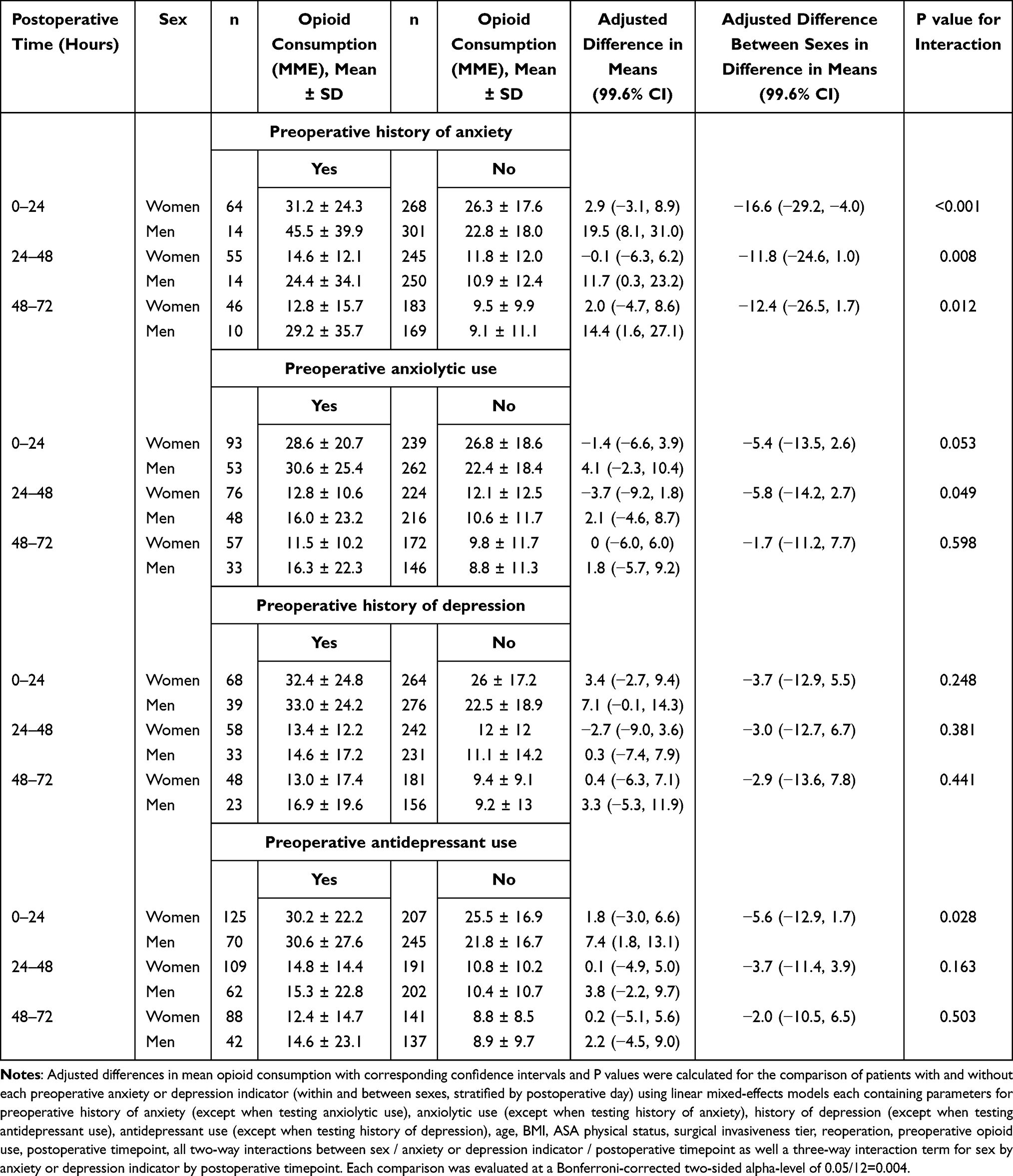 |
Table 2 Assessment of Whether the Association of Preoperative Anxiety or Depression Indicators with Opioid Consumption 0–24, 24–48, and 48–72 Hours After Elective Spine Surgery Differs by Sex |
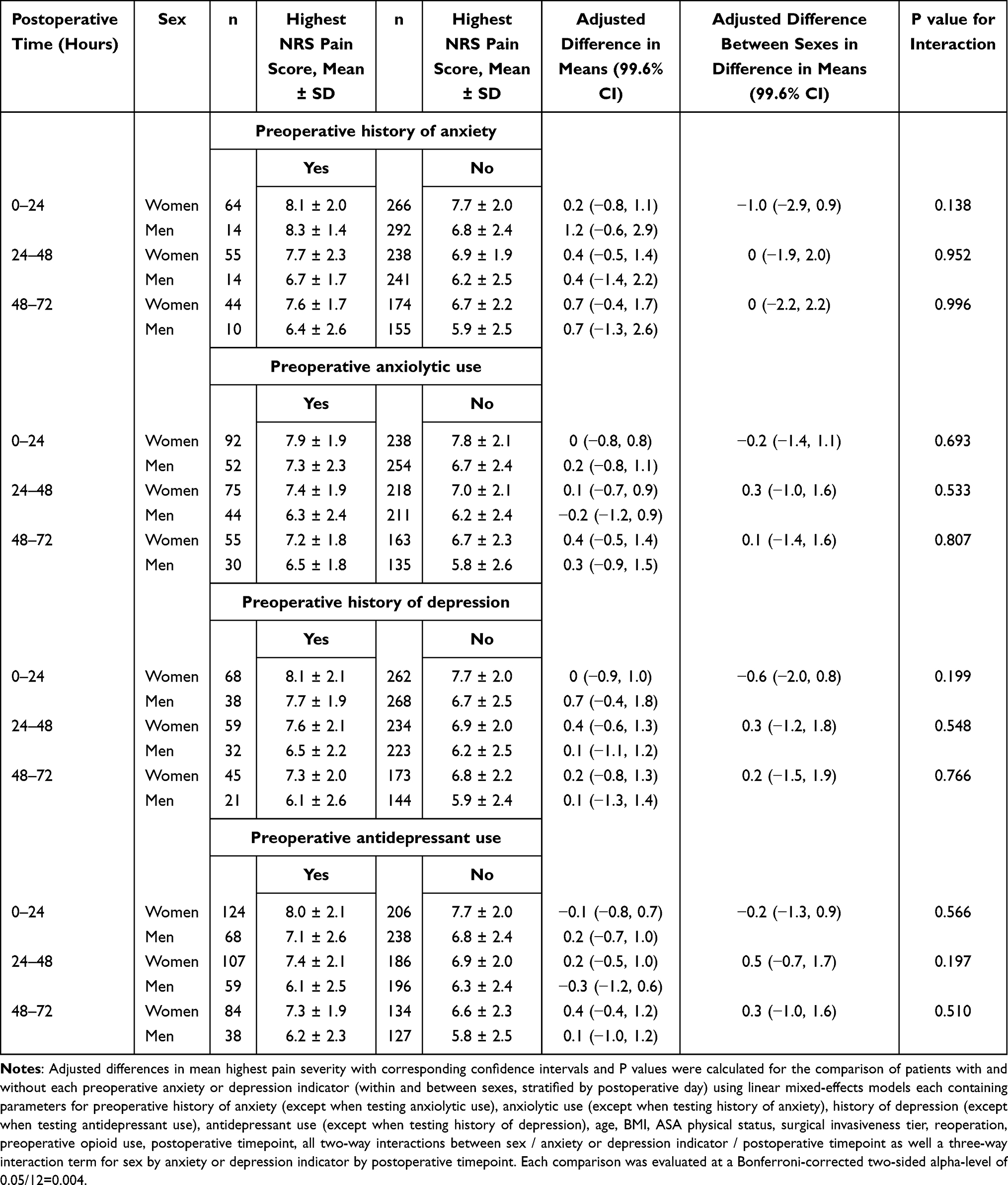 |
Table 3 Assessment of Whether the Association of Preoperative Anxiety and Depression Indicators with Highest Pain Severity 0–24, 24–48, and 48–72 Hours After Elective Spine Surgery Differs by Sex |
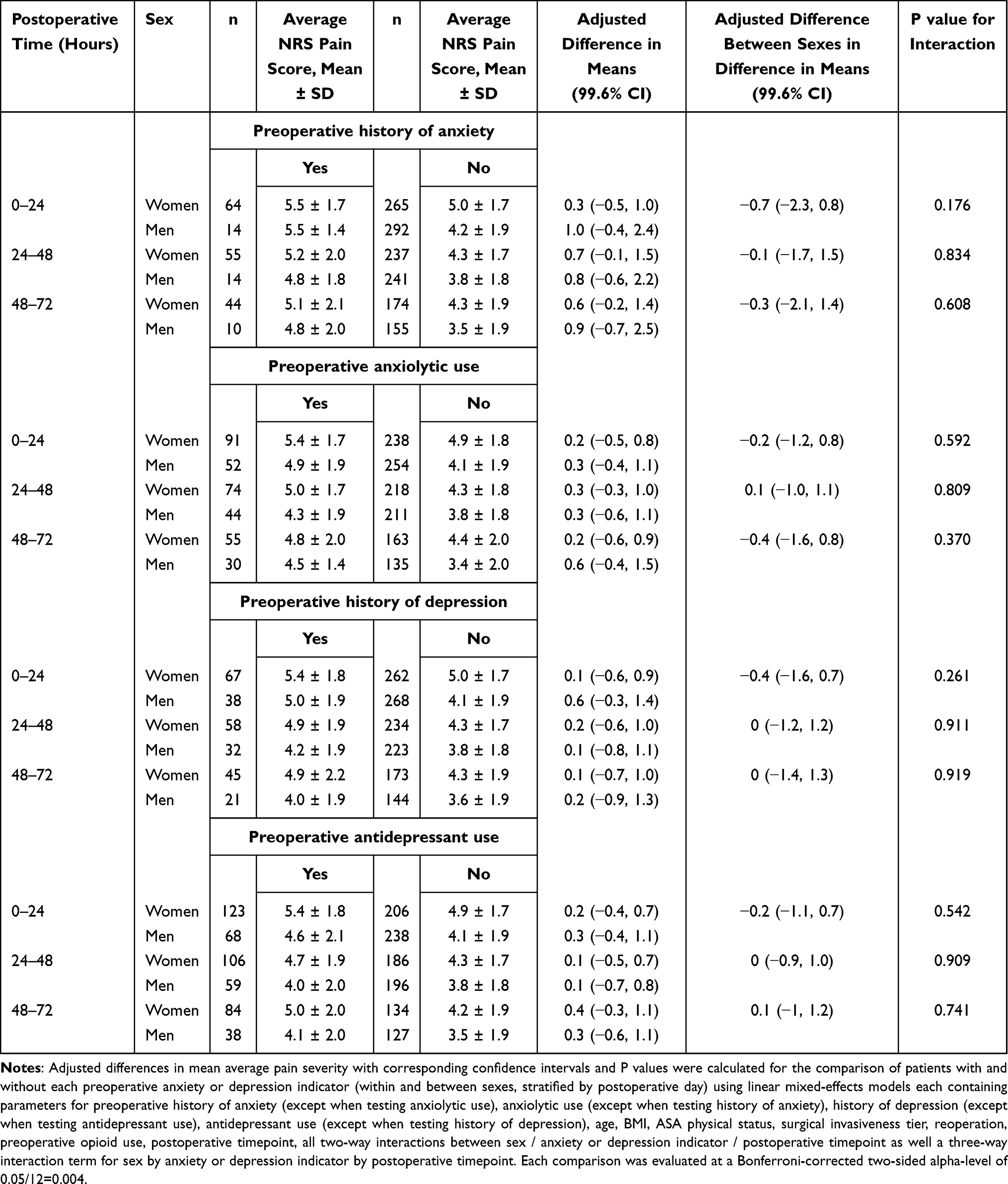 |
Table 4 Assessment of Whether the Association of Preoperative Anxiety or Depression Indicators with Average Pain Severity 0–24, 24–48, and 48–72 Hours After Elective Spine Surgery Differs by Sex |
 |
Figure 2 Boxplots of postoperative opioid consumption at 0–24, 24–48, and 48–72 hours post elective spine surgery stratified by preoperative history of anxiety and sex. Diamonds represent mean values. Boxes consist of the first quartile, median, and third quartiles. The whiskers extend to the most extreme observations within 1.5 times the interquartile range below and above the first and third quartiles, respectively. Small circles represent outliers. |
Preoperative Anxiolytic Use
No associations were detected between preoperative anxiolytic use and postoperative opioid consumption, highest pain severity, or average pain severity at any postoperative time point (Supplementary Tables 2–4). No interactions were detected between sex and preoperative anxiolytic use with respect to opioid consumption, highest pain severity, or average pain severity at any postoperative time point (Tables 2–4).
Preoperative History of Depression
Preoperative history of depression was associated with an adjusted mean (99.6% CI) 5.0 (0.3, 9.7) MME greater opioid consumption in men and women combined 0–24 hours post-surgery (Supplementary Table 2). No associations were detected between the preoperative history of depression and postoperative opioid consumption at 24–48 or 48–72 hours post-surgery, or with the highest or average pain severity at any postoperative time point (Supplementary Tables 2–4). No interactions were detected between sex and preoperative history of depression with respect to opioid consumption, highest pain severity, or average pain severity at any postoperative time point (Tables 2–4).
Preoperative Antidepressant Use
Preoperative antidepressant use was associated with an adjusted mean (99.6% CI) 4.3 (0.6, 8.0) MME greater opioid consumption in men and women combined 0–24 hours post-surgery (Supplementary Table 2). No associations were detected between preoperative antidepressant use and postoperative opioid consumption at 24–48 or 48–72 hours post-surgery, or with the highest or average pain severity at any postoperative time point (Supplementary Tables 2–4). No interactions were detected between sex and preoperative antidepressant use with respect to opioid consumption, highest pain severity, or average pain severity at any postoperative time point (Tables 2–4).
Discussion
The aim of this secondary analysis of a retrospective cohort study was to assess whether any observed association of anxiety or depression indicators with opioid consumption in the first 72 hours after elective spine surgery varies by sex in adults 65 years and older. We found that preoperative history of anxiety was associated with greater opioid consumption 0–24 hours post-surgery in men and women combined, and that this increase was much greater in men than in women. These results are consistent with research conducted by Nandi et al,16 where the association between negative affect and worse acute pain after total knee arthroplasty was stronger in men than in women. However, in our study, no other interactions were detected between sex and psychosocial factors with respect to opioid use, highest pain, or average pain 0–72 hours after elective spine surgery.
Among the exposures investigated, a history of anxiety had the strongest association with acute postoperative opioid consumption. This result is consistent with the finding of Armaghani et al that a higher preoperative Modified Somatic Perception Questionnaire (MSPQ) score, a measure of anxiety symptoms, was associated with greater opioid consumption in the post-anesthesia care unit among elective spine surgery patients.21 Beyond the acute postoperative period, Armaghani et al further found that higher preoperative MSPQ scores were associated with lower odds of opioid independence 12 months after surgery,21 along with other authors who have found an association between anxiolytics and chronic opioid use.24 The mixed-effects models analysis indicated that a history of anxiety was a stronger predictor of postoperative opioid use in men than women. This result may be partially attributable to the fact that women have higher rates of anxiolytic prescriptions. That is, assuming anxiolytic medications may help to mitigate the emotional burden of the surgery and reduce the fear of pain, the more common use of anxiolytics among women may be modestly protective. On the other hand, men are less likely to access psychological therapies than women and present different coping mechanism.25
Our study found a higher prevalence of documented preoperative history of anxiety and depression in women than men. However, we must note this finding in the context that men tend to underreport mental health issues.26 That said, we found that history of anxiety was associated with greater opioid consumption in the first 24 postoperative hours in men and women combined. This is consistent with the literature on pain, catastrophizing, and anxiety, where the evidence clearly highlights greater long-term opioid use for individuals with mental health conditions, in particular anxiety and depression.27,28
While the association between history of anxiety and opioid use was observed for men and women combined during the first 24 postoperative hours, between 24–48 and 48–72 hours post-operatively the association was statistically significant only for men (Table 2). Furthermore, men with a history of anxiety take on average more than double MME (Table 2) in the first 72 hours post-surgery. In this regard, this highlights the importance of studying the gender differences in opioid use.
Floyd et al showed that anxiety has an impact on the length of stay following lumbar spinal surgery29 with patients taking anxiolytics staying 1.8 days longer in the hospital. Another recent literature review30 highlighted how patients with the underlying psychological disease tend to present higher rates of delirium, readmission, longer hospital stays, and higher rates of nonroutine discharge following spine surgery, as well as higher rates of chronic postoperative narcotic use and may experience worse surgical outcomes.
The study by Veal et al with 20,000 elders31 indicated that the use of anxiolytics and opioids tends to be concurrent (41% of opioid users had taken anxiolytics/hypnotic medications). Regarding our population, Table 1 highlights that 56.2% of the patients declaring anxiolytics use were administered opioids preoperatively. Since we are investigating a cohort of elderly patients, this association needs to be particularly highlighted. It constitutes a combination particularly dangerous that it seems to be associated with an increased risk of falls,32 which in the older population lead to further complications and negative outcomes.33,34
A significant difference in length of stay was also found by Walid et al in patients taking antidepressants compared to the ones who were not taking antidepressants.35 However, we found that antidepressant use was associated with an increase in opioid use in the first 24 hours after surgery, albeit in minor quantities compared to patients with a history of anxiety, and this association was not confirmed 48 to 72 hours post-surgery. It appears from our study that anxiety is the most affecting issue influencing pain and postoperative consumption. Therefore, it is essential to find another way to successfully manage preoperative anxiety in older populations.
Perspectives and Significance
Women report on average twice the history of anxiety and take more anxiety medications; on the other hand, men with anxiety seem to be more prone to use opioids in the early postoperative period, leading to think that both genders would benefit from targeted strategies addressing this issue. Given the problems associated with mental health medications in the elderly, it would be key to implement non-pharmacological strategies to manage the psychosocial factors, a solution could be Cognitive Behavioral Therapy (CBT). CBT could provide a toolkit of stress management techniques to individuals experiencing chronic life stress and enhance stress management and coping skills to help patients better manage pain after surgery and reduce their need for opioid medications. Moreover, more research is needed to uncover potential sex differences in the pain management postoperative journey, to optimize the recovery of both populations.
Limitations
This study has several limitations. This was a retrospective study utilizing data from the electronic medical record, corresponding with non-ideal measurement of exposures, model covariates, and outcomes. Regarding study exposures, preoperative anxiety, and depression would ideally be measured on an ordinal or continuous scale via a validated questionnaire. However, given the retrospective nature of this study, we measured preoperative anxiety and depression as binary yes/no exposures as documented in the pre-admission anesthesia evaluation note. Analyzing anxiety and depression as binary (as opposed to ordinal or continuous) variables decreased our power to detect any existing effect. Further, the reliability of the pre-admission anesthesia evaluation note depends on accurate patient report or documentation in the medical record of mental health diagnoses and associated medications. Any misclassifications of anxiety and depression indicators (with false negatives being much more probable than false positives) would likely bias results toward a null finding. Regarding the measurement of model covariates, we only had a record of a patient who was taking preoperative opioids, not the amount. This dichotomization could have resulted in inadequate regression adjustment for preoperative opioid use. Regarding outcomes, postoperative opioid consumption, and pain scores were only available in the medical record during the inpatient stay, precluding analysis of long-term patient pain and functioning. In addition, patients discharged from the hospital prior to 72 hours led to missing outcomes for the 24–48 and 48–72 postoperative time points. However, mixed-effects models provide valid estimates when the probability of an outcome being missing is dependent only upon observed information (the data are missing at random). We posit that the missing at-random assumption, albeit not verifiable, is reasonable given that in-hospital (observed) opioid consumption and pain intensity as well as covariates like surgical invasiveness tier are associated with hospital length of stay. Furthermore, while we acknowledge that the prescribing practices in many groups have changed since the creation of this dataset, the prescribing practices are surgeon specific. In this specific group of patients, the practices have not changed, and the results are therefore still up to date.
In addition to outcome follow-up limitations, there was likely variability in how patients were queried about their postoperative pain intensity, as well as the unknown reliability of their responses. Further, our detection of an interaction between sex and a history of anxiety with respect to opioid consumption 0–24 hours after elective spine surgery was based on only 14 men with documented anxiety, minimizing the generalizability of this finding. Finally, given our observational study design, we could not draw conclusions about causal relationships between the variables studied.
Conclusion
This secondary analysis of a retrospective cohort study found that preoperative history of anxiety was associated with a greater increase in opioid consumption 0–24 hours after elective spine surgery in men than in women aged 65 and older. However, no other interactions were detected between sex and psychosocial factors with respect to opioid use, highest pain, or average pain 0–72 hours after surgery. While this retrospective study found minimal evidence that the association between psychosocial factors and opioid consumption after elective spine surgery differs by sex in older adults, it is possible that some of the null findings may be at least partly attributable to the limitations of the electronic medical record as the sole data source. Therefore, future prospective studies should utilize more sensitive, granular measurements of anxiety and depression to further explore the potential interaction between sex and psychosocial factors with respect to opioid use and pain after surgery.
Acknowledgments
Linda S Aglio and Elisabetta Mezzalira are co-first authors for this study. Thank you Nancy Axelrod for administrative assistance with the manuscript.
Funding
This study did not receive any funding.
Disclosure
Dr Deborah Culley reports grants from NIH, during the conduct of the study; personal fees from American Society of Anesthesiologists, outside the submitted work. The authors have no other competing interests in this work.
References
1. Yoshihara H. Pain medication use after spine surgery. Pain Med. 2014;15:2161–2162. doi:10.1111/pme.12597
2. Dietz N, Sharma M, Adams S, et al. Enhanced Recovery After Surgery (ERAS) for spine surgery: a systematic review. World Neurosurg. 2019;130:415–426. doi:10.1016/j.wneu.2019.06.181
3. Yoo JS, Ahn J, Buvanendran A, et al. Multimodal analgesia in pain management after spine surgery. J Spine Surg. 2019;5:S154–s159. doi:10.21037/jss.2019.05.04
4. Rajan J, Behrends M. Acute pain in older adults: recommendations for assessment and treatment. Anesth Clin. 2019;37:507–520. doi:10.1016/j.anclin.2019.04.009
5. Roberts AW, Ogunwole SU, Blakeslee L, Rabe MA. The Population 65 Years and Older in the United States: 2016. U.S. Census Bureau; 2018.
6. Schreiber KL, Martel MO, Shnol H, et al. Persistent pain in postmastectomy patients: comparison of psychophysical, medical, surgical, and psychosocial characteristics between patients with and without pain. Pain. 2013;154:660–668. doi:10.1016/j.pain.2012.11.015
7. Schreiber KL, Campbell C, Martel MO, et al. Distraction analgesia in chronic pain patients: the impact of catastrophizing. Anesth. 2014;121:1292–1301. doi:10.1097/ALN.0000000000000465
8. Edwards RR, Mensing G, Cahalan C, et al. Alteration in pain modulation in women with persistent pain after lumpectomy: influence of catastrophizing. J Pain Symp Manag. 2013;46:30–42. doi:10.1016/j.jpainsymman.2012.06.016
9. Theunissen M, Peters ML, Bruce J, et al. Preoperative anxiety and catastrophizing: a systematic review and meta-analysis of the association with chronic postsurgical pain. Clin J Pain. 2012;28:819–841. doi:10.1097/AJP.0b013e31824549d6
10. Meretoja TJ, Andersen KG, Bruce J, et al. Clinical prediction model and tool for assessing risk of persistent pain after breast cancer surgery. J Clin Oncol. 2017;35:1660–1667. doi:10.1200/JCO.2016.70.3413
11. Hah JM, Bateman BT, Ratliff J, et al. Chronic opioid use after surgery: implications for perioperative management in the face of the opioid epidemic. Anesth Analg. 2017;125:1733–1740. doi:10.1213/ANE.0000000000002458
12. Perttunen K, Tasmuth T, Kalso E. Chronic pain after thoracic surgery: a follow-up study. Acta Anaesth Scand. 1999;43:563–567. doi:10.1034/j.1399-6576.1999.430513.x
13. Lee D, Armaghani S, Archer KR, et al. Preoperative opioid use as a predictor of adverse postoperative self-reported outcomes in patients undergoing spine surgery. J Bone Joint Surg Am. 2014;96:e89. doi:10.2106/JBJS.M.00865
14. Thompson T, Correll CU, Gallop K, et al. Is pain perception altered in people with depression? A systematic review and meta-analysis of experimental pain research. J Pain. 2016;17:1257–1272. doi:10.1016/j.jpain.2016.08.007
15. Pereira MP, Pogatzki-Zahn E. Gender aspects in postoperative pain. Curr Opin Anaesth. 2015;28:546–558. doi:10.1097/ACO.0000000000000226
16. Nandi M, Schreiber KL, Martel MO, et al. Sex differences in negative affect and postoperative pain in patients undergoing total knee arthroplasty. Biol Sex Differ. 2019;10:23. doi:10.1186/s13293-019-0237-7
17. Costelloe C, Burns S, Yong RJ, et al. An analysis of predictors of persistent postoperative pain in spine surgery. Curr Pain Headache Rep. 2020;24:11. doi:10.1007/s11916-020-0842-5
18. Susano MJ, Scheetz SD, Grasfield RH, et al. Retrospective analysis of perioperative variables associated with postoperative delirium and other adverse outcomes in older patients after spine surgery. J Neurosurg Anesth. 2019;31:385–391. doi:10.1097/ANA.0000000000000566
19. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147(8):573–577. doi:10.7326/0003-4819-147-8-200710160-00010
20. Armaghani SJ, Lee DS, Bible JE, et al. Preoperative narcotic use and its relation to depression and anxiety in patients undergoing spine surgery. Spine. 2013;38:2196–2200. doi:10.1097/BRS.0000000000000011
21. Armaghani SJ, Lee DS, Bible JE, et al. Preoperative opioid use and its association with perioperative opioid demand and postoperative opioid Independence in patients undergoing spine surgery. Spine. 2014;39:E1524–1530. doi:10.1097/BRS.0000000000000622
22. Yang D, Dalton J. A unified approach to measuring the effect size between two groups using SAS; 2012.
23. Austin PC. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Comm Stat. 2009;38:1228–1234. doi:10.1080/03610910902859574
24. Skurtveit S, Furu K, Bramness J, et al. Benzodiazepines predict use of opioids--a follow-up study of 17,074 men and women. Pain Med. 2010;11:805–814. doi:10.1111/j.1526-4637.2010.00870.x
25. Liddon L, Kingerlee R, Barry JA. Gender differences in preferences for psychological treatment, coping strategies, and triggers to help-seeking. Brit J Clin Psych. 2018;57:42–58. doi:10.1111/bjc.12147
26. Affleck W, Carmichael V, Whitley R. Men’s mental health: social determinants and implications for services. Can J Psych. 2018;63:581–589. doi:10.1177/0706743718762388
27. Quinn PD, Rickert ME, Franck J, et al. Associations of mental health and family background with opioid analgesic therapy: a nationwide Swedish register-based study. Pain. 2019;160:2464–2472. doi:10.1097/j.pain.0000000000001643
28. Best MJ, Harris AB, Bansal A, et al. Predictors of long-term opioid use after elective primary total shoulder arthroplasty. Orthoped. 2020;2020:1–6.
29. Floyd H, Sanoufa M, Robinson JS. Anxiety’s impact on length of stay following lumbar spinal surgery. Perm J. 2015;19:58–60. doi:10.7812/TPP/15-022
30. Jackson KL, Rumley J, Griffith M, et al. Correlating psychological comorbidities and outcomes after spine surgery. Global Spine J. 2020;10:929–939. doi:10.1177/2192568219886595
31. Veal FC, Bereznicki LR, Thompson AJ, et al. Use of opioid analgesics in older Australians. Pain Med. 2015;16:1519–1527. doi:10.1111/pme.12720
32. Milos V, Bondesson Å, Magnusson M, et al. Fall risk-increasing drugs and falls: a cross-sectional study among elderly patients in primary care. BMC Geriat. 2014;14:40. doi:10.1186/1471-2318-14-40
33. Hartholt KA, van Beeck EF, Polinder S, et al. Societal consequences of falls in the older population: injuries, healthcare costs, and long-term reduced quality of life. J Trauma. 2011;71:748–753. doi:10.1097/TA.0b013e3181f6f5e5
34. Burns ER, Stevens JA, Lee R. The direct costs of fatal and non-fatal falls among older adults - United States. J Safety Res. 2016;58:99–103. doi:10.1016/j.jsr.2016.05.001
35. Walid MS, Zaytseva NV. Prevalence of mood-altering and opioid medication use among spine surgery candidates and relationship with hospital cost. J Clin Neurosci. 2010;17:597–600. doi:10.1016/j.jocn.2009.09.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Alleviating Excessive Worries Improves Co-Occurring Depression and Pain in Adolescent and Young Adult Cancer Patients: A Network Approach
Li W, Xu Y, Luo X, Wen Y, Ding K, Xu W, Garg S, Yang Y, Sun H
Neuropsychiatric Disease and Treatment 2022, 18:1843-1854
Published Date: 25 August 2022
Predictive Validity and Patterns of Change Over Time of the Sensitivity to Pain Traumatization Scale: A Trajectory Analysis of Patients Seen by the Transitional Pain Service Up to Two Years After Surgery
Fashler SR, Pagé MG, Svendrovski A, Flora DB, Slepian PM, Weinrib AZ, Huang A, Fiorellino J, Clarke H, Katz J
Journal of Pain Research 2022, 15:2587-2605
Published Date: 31 August 2022
The Relationship of Postoperative Pain and Opioid Consumption to Postoperative Delirium After Spine Surgery
Sica R, Wilson JM, Kim EJ, Culley DJ, Meints SM, Schreiber KL
Journal of Pain Research 2023, 16:287-294
Published Date: 28 January 2023
Perioperative Pain Management and Cancer Outcomes: A Narrative Review
Ramirez MF, Strang A, Roland G, Lasala J, Owusu-Agyemang P
Journal of Pain Research 2023, 16:4181-4189
Published Date: 5 December 2023
Suzetrigine Approval Breaks a 25-Year Silence: A New Era in Non-Opioid Acute Pain Management
Sibomana O, Okereke M, Hakayuwa CM
Journal of Pain Research 2025, 18:2805-2808
Published Date: 6 June 2025