Back to Journals » Advances in Medical Education and Practice » Volume 12
Documentation Practice and Associated Factors Among Nurses in Harari Regional State and Dire Dawa Administration Governmental Hospitals, Eastern Ethiopia
Authors Tamir T ![]() , Geda B
, Geda B ![]() , Mengistie B
, Mengistie B ![]()
Received 22 December 2020
Accepted for publication 3 April 2021
Published 10 May 2021 Volume 2021:12 Pages 453—462
DOI https://doi.org/10.2147/AMEP.S298675
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Takla Tamir,1 Biftu Geda,2 Bezatu Mengistie3
1Department of Nursing, College of Health and Medical Science, Dilla University, Dilla, Ethiopia; 2Department of Nursing, College of Health and Medical Science, Haramaya University, Harar, Ethiopia; 3Department of Public Health, College of Health and Medical Science, Haramaya University, Harar, Ethiopia
Correspondence: Takla Tamir Email [email protected]
Background: Nursing documentation is an integral and vital professional nursing practice that refers to the process of recording nursing activities concerned with the care given to individual clients to ensure continual effective, safe, quality, evidence-based, and individualized care.
Objective: To assess documentation practice and identify its associated factors among nurses in six Governmental Hospitals of Harari Regional State and Dire Dawa Administration, Eastern Ethiopia.
Methodology: An institutional-based cross-sectional study was conducted among 430 nurses and 421 medical records. Simple random sampling was employed for the selection of nurses and charts after the total sample size had been allocated proportionally for each hospital. Data were collected by using a self-administered questionnaire and review of records, and entered and analyzed by using EpiData version 3.1 and statistical package for social sciences version 20.0, respectively. Logistic regression was used to identify the associated factors.
Results: In this study, 47.5% of nurses were found to have good nursing documentation practice whereas good nursing documentation practice was found in 38.5% of medical records. Age (AOR, 95% CI 3.54, 1.170– 10.8), attitude (AOR, 95% CI 5.66, 3.17– 10.11), in-service training (AOR, 95% CI 2.53, 1.477– 4.35), nurse to patient ratio (AOR, 95% CI 2.24, 1.24– 4.047), motivation (AOR, 95% CI 4.60, 2.721– 7.76), and familiarity with standards of nursing documentation (AOR, 95% CI 1.98, 1.137– 3.44) were found to have a statistically significant positive association with documentation practice.
Conclusion: Poor documentation practice was due to the identified factors. So, it is better to put further effort toward improving documentation practice through providing training on standards of documentation and enhancing the favorable attitude of nurses toward documentation practice by motivating them regarding documentation activities.
Keywords: documentation, nursing care, practice, nursing standards, associated factors
Introduction
Nursing documentation is the process of recording1,2 and keeping evidence to have an account of what happened and when it happened.1,3,4 It is an integral, vital, and important part of professional nursing practice5 with the primary purpose of communicating patient information to the health care team.6
Nursing documentation promotes effective communication, ensures early detection of problems, quality, continuity, individuality as well as complete client care and patient safety that ultimately increase the quality of life through which it determines the standard of care rendered by nurses.1,2,7 It also enhances professional autonomy, nurses’ critical thinking skills, development of professional knowledge, and nursing education. It is a legal witness for the nurses’ act.8,9 Its contribution to the research environment, credentialing, reimbursement, and auditing clinical services is invaluable,10 which helps the profession to be advanced and visible.11,12
The quality of patient care depends on the caregiver’s ability to have an accurate, timely, and effective exchange of oral or written information, ideas, and feelings with patients and colleagues.13,14 There is no way to prove care was provided without completed documentation,2,15 as many studies indicated globally, most of the nurses’ actions are either not documented or not properly documented.2,6,16,17 In Africa as well as Ethiopia, the act of nursing documentation remains challenging due to lack of training, resources, comprehensive nursing education (CNE), time, high nurse-to-patient ratio, poor knowledge, and attitude.1,6,18
Nurses play an important role in the care of patients and what they put into writing determines the standard and quality of care rendered to the patient.2 Documentation is the tip of the iceberg of patient care issues that could expose caregivers to medico-legal suits and other forms of disciplinary action.19 So poor documentation practice creates a great problem when it comes to the evaluation of client care2 and is a key factor in miscommunication among nurses and physicians, delayed, repeated or omitted, and fragmented care that will cause preventable medical errors which may potentially affect patient outcomes.1 Ineffective documentation causes clinical mishaps and crucial issues in many malpractice cases20 and continues to be cited as a major cause of adverse events for patients.21,22 Poor nursing documentation can place patients, staff, as well as organizations at considerable risk of physical and legal harm.23
As per the review of available literature, there is a paucity of information about documentation practice and its associated factors due to few studies which were limited only to one hospital, done with small sample size, moreover, they measured the practice through self-administered questionnaire. This study aimed to determine documentation practice and identify factors associated with it by “filling in the gaps” identified from previous studies and providing relatively strong and additional baseline evidence. The findings will help to plan intervention programs for poor nursing documentation practice and to avert its effects at different levels.
Methods and Materials
Study Design and Setting
An institutional-based quantitative cross-sectional study was conducted from March 15-25, 2019 in the Governmental Hospitals of Harari Regional State and Dire Dawa Administration located in the eastern part of the country at a distance of 523 and 515 km respectively from Addis Ababa, the capital city of Ethiopia. There were 101 governmental health care facilities of which 6 were hospitals, and 2282 health care workers of whom 44.3% were nurses.
Population
All nurses working in Harari Regional State and Dire Dawa Administration Governmental Hospitals were source and study populations.
Eligibility Criteria
Nurses involved in direct patient care with work experience of at least 6 months were included.
Sample Size and Sampling Procedure
The sample size was determined by using Epinpho Version 7 for the two objectives separately. For the first objective (documentation practice), the population survey/single population proportion formula was used by considering the proportion of good practice is 47.84 with 95% confidence level and 5% marginal error; the calculated sample size was 383. For the second objective using AOR, 95% confidence level, 80% power, 1:1 ratio of unexposed to exposed and percent outcome in the unexposed group for each factor which had a statistically significant association with documentation practice from previous studies, the sample size ranged from 184 to 402. For this study, we decided to take the maximum calculated sample size (402) after comparing the sample sizes calculated for both objectives. Finally, it came to 442 after adding a 10% non-response rate.
The determined sample was allocated proportionally for each governmental hospital found in the study area using the proportional allocation formula. Each participant was selected by simple random sampling using a sampling frame from the Human Resource department of each hospital. The same sample size and sampling technique were applied to select charts with a sampling frame of the list of one-month medical registration numbers nearest to the study period from the inpatient department and again proportional allocation was done for each ward found in the hospital to increase the representativeness.
Study Variables
After reviewing existing literature, all the study variables were summarized by the conceptual framework as shown in Figure 1.
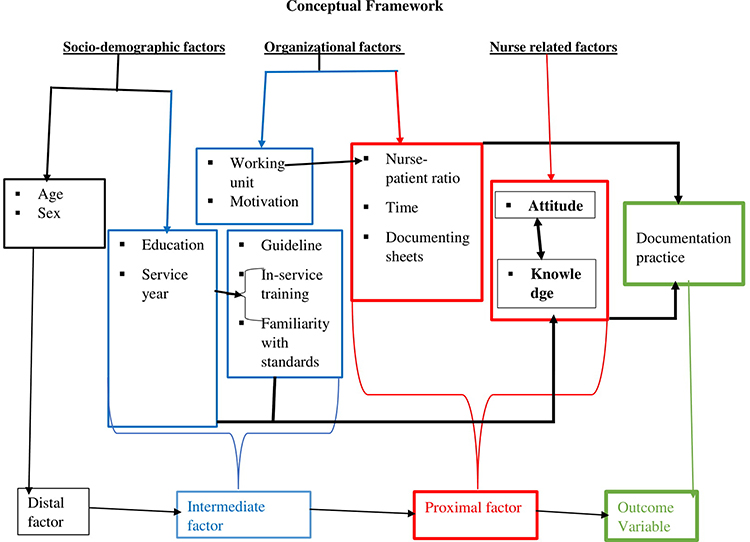 |
Figure 1 A conceptual framework of documentation practice and associated factors among nurses in Harari Region and Dire Dawa Administration Governmental Hospitals, Eastern Ethiopia 2019. Notes: Adapted from Mihiretu K, Yesuf E, Desalegn TZ. Nursing care documentation practice: The unfinished task of nursing care in the University of Gondar Hospital. Informatics for Health and Social Care. 2017;42(3):290–302.1 |
Data Collection Methods (Tool and Procedure)
A structured, self-administered English version questionnaire with 41 questions in five parts was adopted and modified from different reviewed literature.1,4 A pre-test was done on five percent of the total sample. Part-I contains 04 questions regarding the socio-demographic characteristics of the nurses; Part-II contains 10 questions regarding documentation practice with “Never”, “Sometimes”, and “Always” responses having a score of “1”, “2”, and “3” respectively, with a reliability coefficient of 0.888. Previous studies used “Yes” or “No” responses. Part III contains 08 questions regarding organizational factors; Part IV contains 10 Likert-type attitude-related questions where a score of 1, 2, 3, 4, and 5 was given for “strongly disagree”, “disagree”, “neutral”, “agree”, and “strongly agree” responses respectively. It had a reliability coefficient of 0.801. Previous studies used four scales and this study incorporated “neutral”. Part V contains 09 multiple choice type questions with multiple options where the scoring was based on the type of response, so 1 for the response of correct options and 0 for incorrect options were scored with a reliability coefficient of 0.912. Previous studies used Likert-type questions.
A structured and pretested English version standard checklist with 12 items adopted and modified from different reviewed literature and guidelines1,13,14,24 was used to review medical records separately from nurses and to collect the data regarding nursing documentation practice objectively. The checklist contained 12 items with a score of “1”, “2”, and “3” for “not”, “partially”, and “completely” responses respectively. Previously studies used “yes” or “no” checks.
Ethical clearance was obtained from Haramaya University, College of Health and Medical Sciences, Institute Health Research Ethics Review Committee. A permission letter and explanation about the aims, benefits, and risks of the study were provided. So, approval was obtained from the participating hospitals. Informed, voluntary, written and signed consent was obtained from each respondent. Confidentiality was maintained at all levels of the study through anonymous data collection. Twelve BSc nurse data collectors and two MSc nurse supervisors were employed, trained, and did the data collection activities with the principal investigators’ close supervision.
Operational Definitions
Documentation practice of study participants was measured by using 09 Likert-type self-administered questions or a structured checklist comprising 12 items. The total score for both self-administered questions and the checklist was dichotomized into good and poor practice by median score cut off point. Good practice: a score of ≥ the median score for practice questions, otherwise poor.
The total score for knowledge of study participants about nursing documentation measured by 09 multiple choice type questions was dichotomized into good and poor knowledge by median score cut off point. Good knowledge: a score of ≥ the median score for knowledge questions, otherwise poor.1
The total score for attitude of study participants toward nursing documentation measured by 10 Likert-type questions was dichotomized into favorable and unfavorable attitude by median score cut off point. Favorable attitude: ≥ the median score for attitude questions, otherwise unfavorable.1 Adequate nurse to patient ratio: if a nurse serves ≤ 2 patients in ICU or ≤ 6 patients in inpatient wards other than ICU, otherwise inadequate.25
Data Quality Control
A properly aimed data collection tool was prepared and tested on five percent of the total sample at the questionnaire level. To minimize bias, recruited data collectors and supervisors were not employees of the study hospitals, and adequate training was given to data collectors. On each data collection day, a percentage of the collected data was examined by the principal investigator and any issues were resolved immediately.
After the data had been collected, the principal investigator and supervisors checked it for completeness, accuracy, clarity, and consistency before data entry into software, and each questionnaire which was selected for analysis was properly coded. Data double entry into EpiData version 3.1 was done. The consistency of data entry was validated. After all, data screening was performed through running descriptive statistics, and data cleaning measures were taken accordingly before data analysis at the data processing stage.
Method of Data Processing and Analysis
Data were exported to SPSS Version 20 software for analysis. Variables were computed and recoded through the transform function of SPSS. Descriptive analysis was done to compute proportions and summary measures. Summary measures, tables, and figures were used to present the processed information.
Attitude toward nursing documentation was computed from summing up all relevant 10 five scale Likert attitude items, those respondents who scored median and above were labeled as having a favorable attitude. Knowledge about nursing documentation was computed from summing up all relevant 09 multiple-choice items with a total of 31 multiple options, those respondents who scored median and above were labeled as having good knowledge about nursing documentation.
The practice of nursing documentation was computed from summing up all relevant 09 Likert type practice items for self-reported and 12 Likert practice checklist items for chart review, respondents or records who scored median and above were labeled as having good nursing documentation practice. Record review was used to determine the documentation practice level of nurses and self-reported documentation practice was used in the bivariate and multivariate analysis to identify associated factors.
Bivariate analysis, crude odds ratio with 95% CI, was estimated to see the crude association between each independent variable with the dependent variable. All variables with P ≤ 0.25 at 95% confidence level during the bivariate analysis were a candidate for multivariate analysis. A multicollinearity test was carried out to see the linear correlation among independent variables by using standard error. Standard error >2 was considered as suggestive of the existence of multicollinearity. Hosmer–Lemeshow goodness-of-fit was done to check model fitness. The omnibus test was significant (p-value <0.0001) and Hosmer–Lemeshow’s test was found to be insignificant (p-value =0.476), which indicated that the model was fitted.
Adjusted odds ratios with 95% CI were estimated during multivariate analysis to identify factors associated with documentation practice. Independent variables at the level of statistical significance, P < 0.05, which does not include null value in the 95% CI were declared as significant.
Result
Socio-Demographic Characteristics
Four hundred and thirty nurses participated in the study giving a response rate of 97.3%. The age of the study participants ranged from 21 to 58 years with a median age of 29 years. The majority of the respondents were males (54.4%). Nearly eighty percent of them (79.3%) had a BSc degree and above in nursing. More than half, 224 (52.1%), of respondents had worked for 5 years and less as a nursing professional (Table 1).
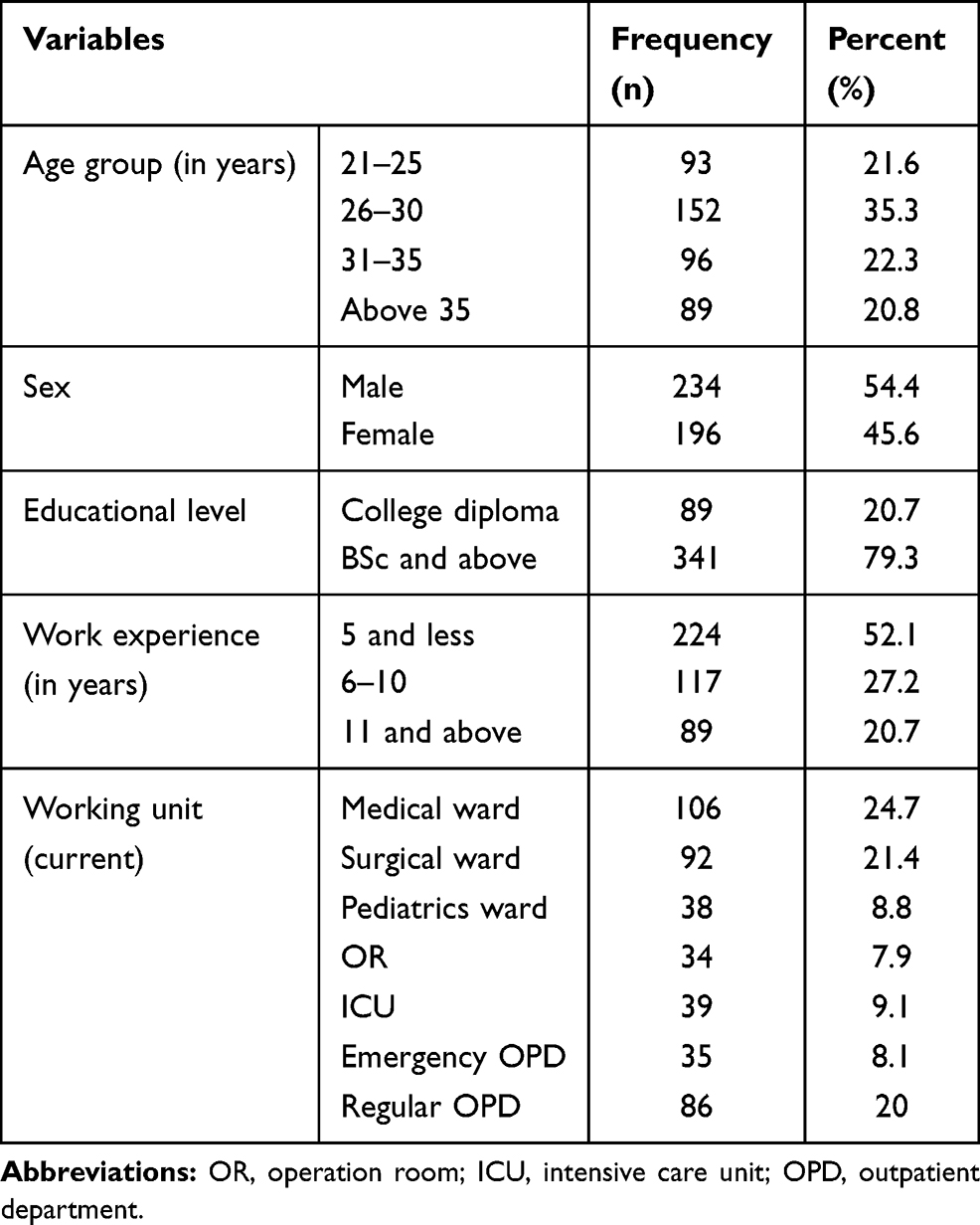 |
Table 1 Socio-Demographic Characteristics of Nurses in Governmental Hospitals of Harari Regional State and Dire Dawa Administration, Eastern Ethiopia, 2019 (n=430) |
Organizational Factors
Out of four hundred and thirty participating nurses, 49% attended in-service training on standards of nursing documentation. Only 47.9% of respondents easily obtained nursing documentation standard guidelines, and a nursing documenting sheet was available in their working unit for 59.8% of respondents. Nearly two-thirds (66%) of them reported that they were familiar with operational standards of nursing documentation. Fifty-three percent (53%) of respondents were motivated by their supervisors regarding their documentation activities and 68.8% of respondents reported that they had enough time to document their nursing activities after the care they provided (Table 2).
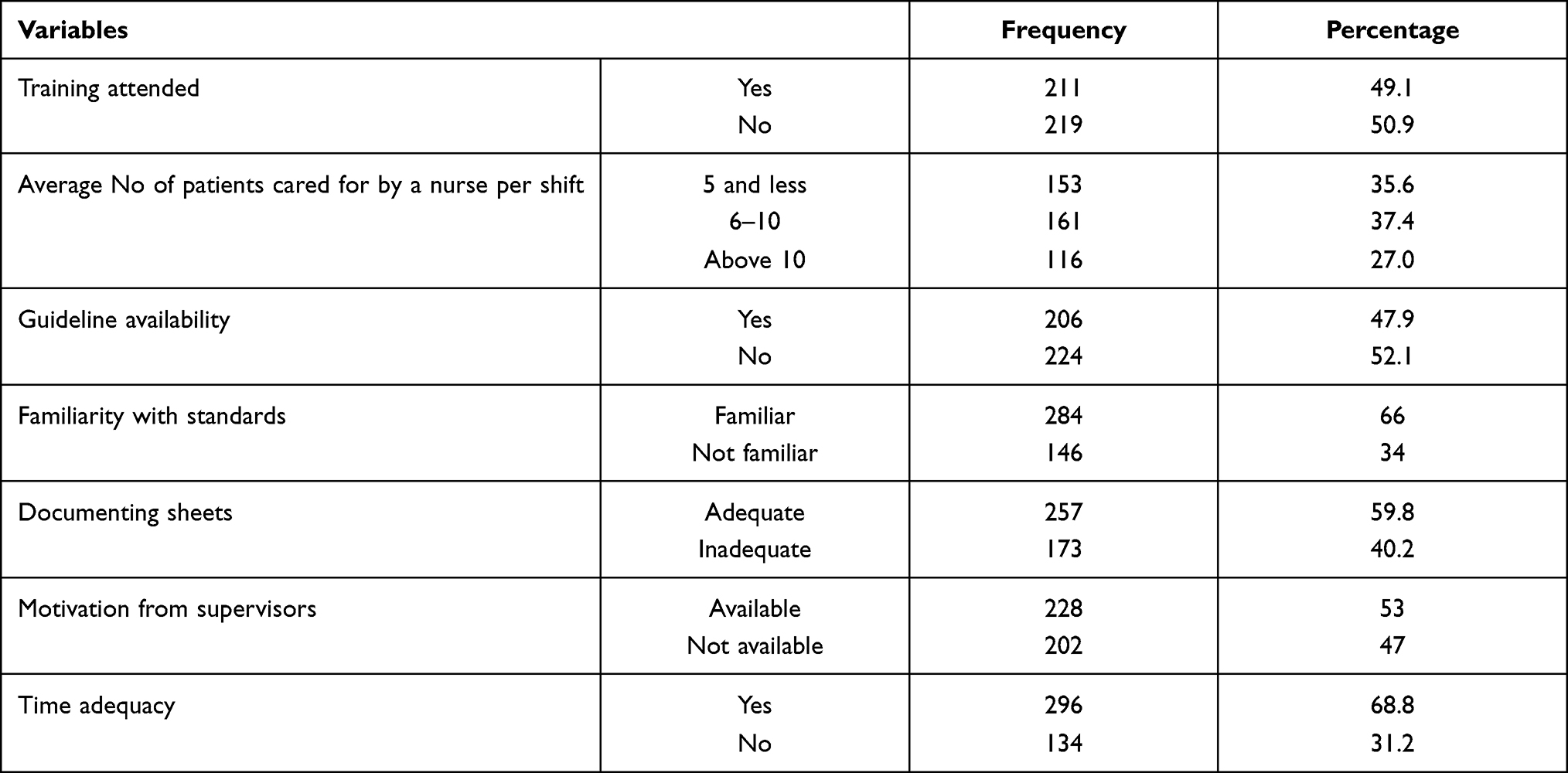 |
Table 2 Frequency and Percentage Distribution of Organizational Factors Among Nurses in Governmental Hospitals of Harari Regional State and Dire Dawa Administration, Eastern Ethiopia, 2019 (n=430) |
Knowledge and Attitude of Nurses Toward Nursing Documentation
Out of the total study participants, 50%, 95% CI (45–55%) had favorable attitude and 51.6%, 95% CI (46.7–56.5%) had good knowledge about nursing documentation.
Documentation Practice
Out of the total 430 participants, 64.6% and 51.6% of them reported that they always document the medication they administered and the assessment they did for every patient, respectively. Whereas only 30.5% of them reported that they always document the education they provided for every patient. Concerning timing parameter, all their documentation was always done immediately after the care provided for 32.6% of study participants (Table 3). Out of 430 participants, 47.9% (n=206); 95% CI (43.2–52.6%) of respondents were found to have good documentation practice.
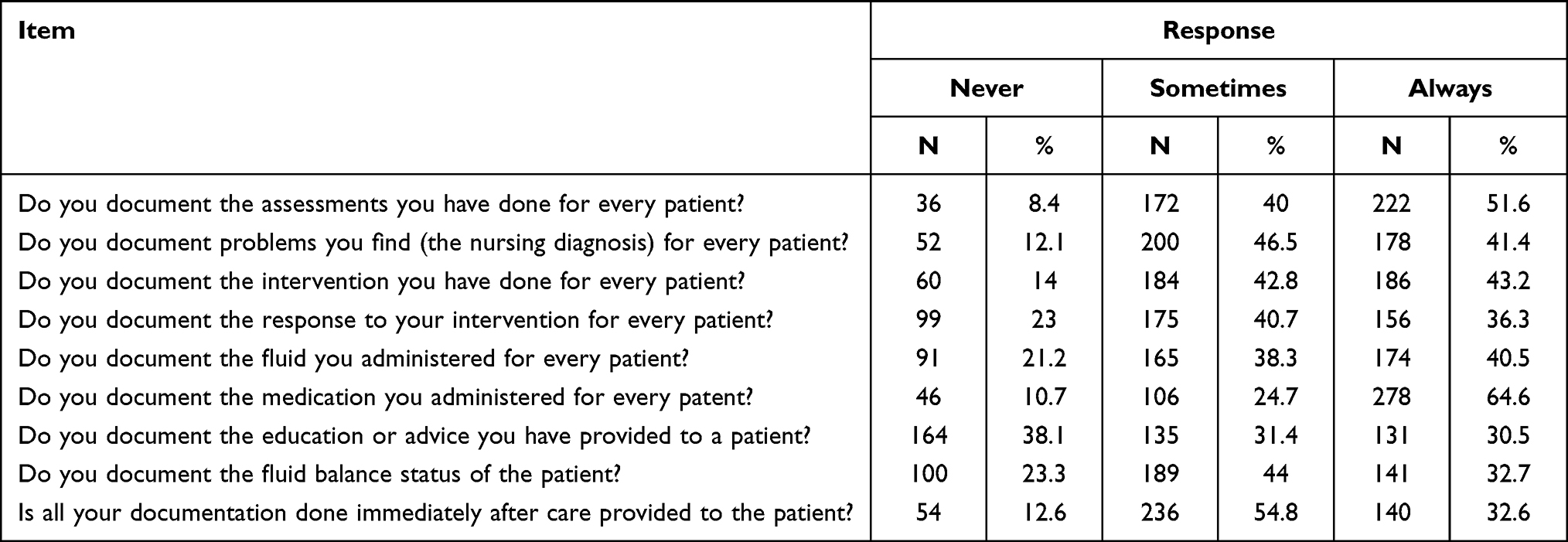 |
Table 3 Self-Reported Documentation Practice Among Nurses in Governmental Hospitals of Harari Regional State and Dire Dawa City Administration, Eastern Ethiopia, 2019 (n=430) |
Nursing documentation practice was assessed objectively through reviewing the previous one-month charts of admitted patients. Out of 442 sample charts to be reviewed, twenty-one charts were not found in their place and 421 charts were reviewed giving a retrieval rate of 95.25%. The vital sign sheet was attached to 91.9% of reviewed charts and for 61.5% of them the vital sign status of the patient was completely documented. The nursing process format was attached to only 21.1% of the charts reviewed and for 5.6% of them none of the nursing process format components were documented. Regarding their legibility, only 5.2% of the charts were not legible (Table 4). Out of 421 reviewed medical records, good nursing documentation was found to be practiced in 38.5% (n=162, 95% CI (34–43.2%) of them.
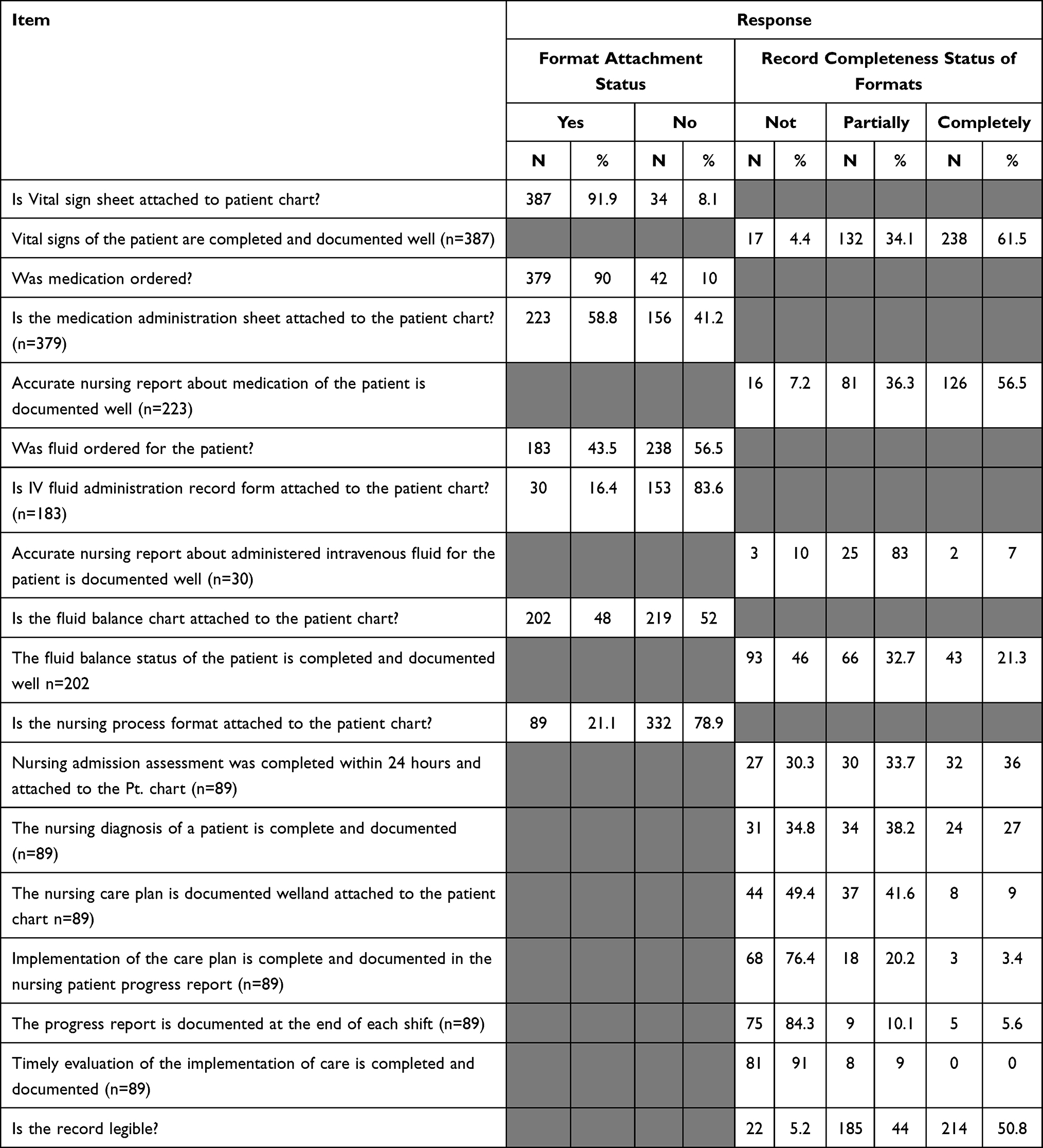 |
Table 4 Chart Review Documentation Practices Among Nurses in Governmental Hospitals of Harari Regional State and Dire Dawa City Administration, Eastern Ethiopia 2019 (n=421) |
Factors Associated with Documentation Practice
Age, standard training on nursing documentation, nurse to patient ratio, familiarity with operational standards of nursing documentation, motivation from supervisors, and attitude toward nursing documentation were positively and independently associated with nursing documentation practice (Table 5).
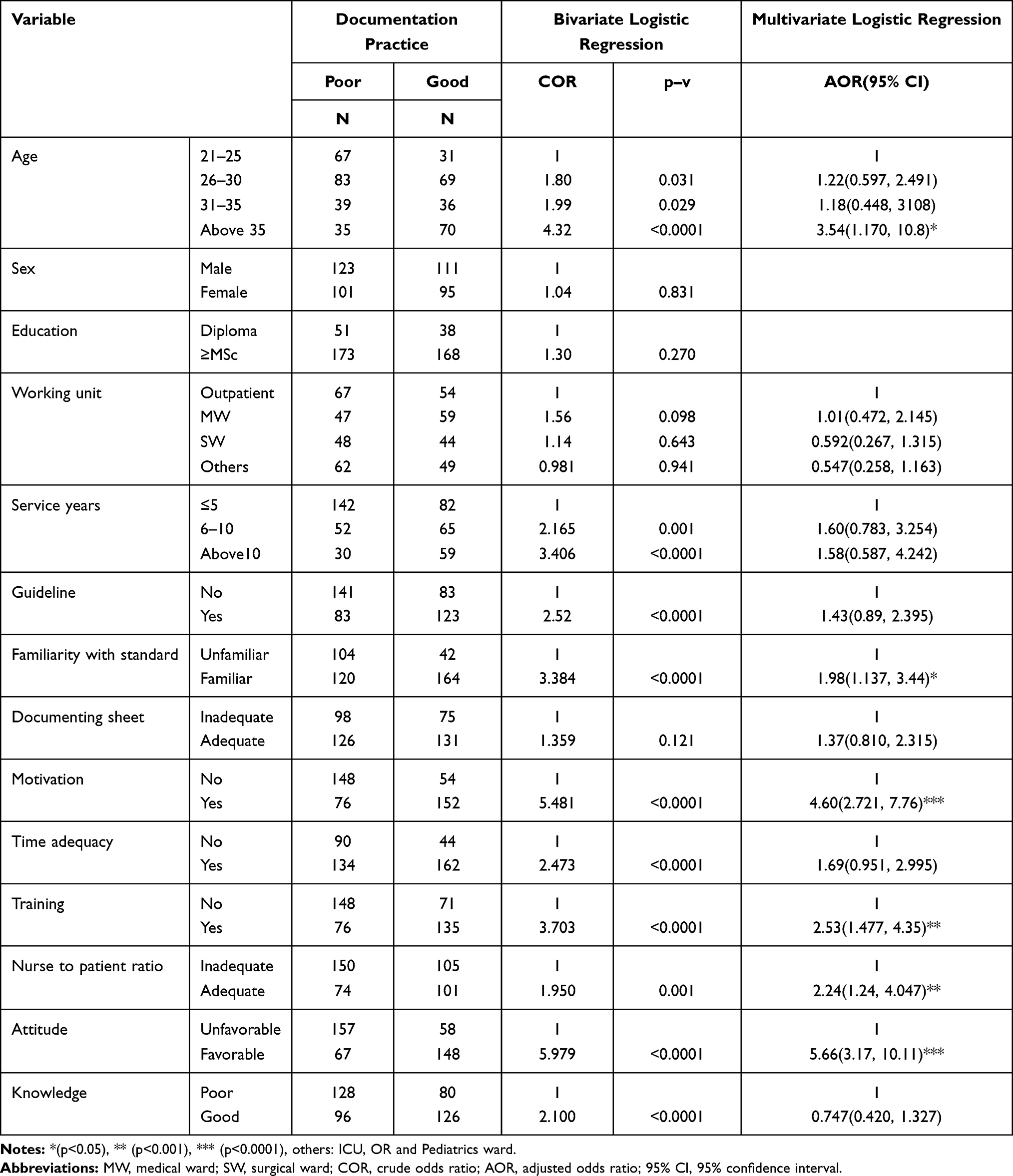 |
Table 5 Factors Associated with Documentation Practice Among Nurses in Governmental Hospitals of Harari Region and Dire Dawa Administration, Eastern Ethiopia, 2019 (n=430) |
Discussion
This study revealed that documentation practice was poor through both self-reported questions and record review. Self-reported documentation practice was supported by the chart review documentation practice, but it was higher than the chart review documentation practice. This discrepancy might be due to social desirability bias in the self-reported documentation practice.
For this study, record-reviewed documentation practice was reported as the level of documentation practice, which is almost similar to the finding of the study conducted in Gondar.1 The finding of this study was lower than the finding of the studies conducted in Jamaica,26 Nigeria,2 Ghana,19 and Jimma.18 The possible reason for this variation might be the tool utilized to determine the level of documentation practice,2,18 self-administered questionnaire was used in those studies but medical record review was used in this study, and self-reported documentation practice may be overestimated due to social desirability bias. But this finding was higher than the finding of the studies conducted in Iran,27 Europe,28 and Canada.29 This discrepancy might be due to the ward type included in the study,27 the units included in the previous study were only medical-surgical wards and the workload is high in medical-surgical wards in teaching hospitals of Iran, thus it may cause lower level of nurses’ documentation practice. The other possible reason for this discrepancy might also be due to area coverage difference,28 the study conducted in Europe covered a large scale area but this study covered a small area. Even the type of study conducted may have its role in this discrepancy,29 the study conducted in Canada was “prospective observational” but “retrospective review of records” in this study.
For this study, self-reported documentation practice was used to identify factors associated with documentation practice among nurses. A favorable attitude toward nursing documentation was positively associated with documentation practice. This finding is in line with the finding of the studies conducted in Iraq,23 Iran (Tabriz),10 Nigeria,11 and Gondar.1 This might be due to the fact that favorable attitude toward nursing documentation may be a strong and baseline internal motive of nurses to practice documentation. It is important to provide in-service training on standards of documentation and enhancing the favorable attitude of nurses toward documentation.
Attending standard training on nursing documentation had a positive association. This finding is comparable with the finding of the studies conducted in Ghana,19 Uganda,6 and Gondar.1 This might be due to the fact that training may increase their familiarity with operational standards of documentation, and may enhance their attitude toward documentation, and may also add their value of documenting what they have done. So training will be helpful to improve documentation practice.
Familiarity with operational standards of nursing documentation had a significant and positive association. This finding is consistent with the finding of the study conducted in Jimma.18 This might be due to the fact that familiarity with operational standards of nursing documentation may make tasks of documentation easy, fast, and interesting for nurses.
Nurses who were motivated by their supervisors regarding documentation activities were more likely to practice documentation when compared to nurses who were not motivated. Similarly, this evidence is in line with the finding of the study conducted in Jimma.18 This might be due to the fact that motivation may enhance nurses’ favorable attitude toward nursing documentation and encourage them to document their activity.
Adequate nurse to patient ratio was positively associated with nursing documentation practice. This finding is consistent with the finding of the studies conducted in Western Jamaica,26 Eastern Ghana,19 and Gondar.1 This might be due to the fact that an adequate nurse to patient ratio may decrease workload and increase time to document their activity, which makes documentation practice more likely. It is important to have adequate nursing human resources.
Also, in this study, age had a significantly positive association with nursing documentation practice. This finding is comparable with the finding of the study conducted in Iraq, Al Najaf Governorate.9 This might be due to the fact that most older nurses were shown to have long service years as seen from crosstab, so their exposure to training may be increased and this will make them familiar with operational standards of documentation. Again, as their age increases, they may appreciate different multi-aspect advantages of documentation that will enhance their favorable attitude toward documentation which will in turn improve their documentation practice. It is important to plan and have experience exchange within and across hospitals, about documentation practice.
Conclusion
Documentation practice among nurses was poor. Attitude toward nursing documentation, in-service training on standards of nursing documentation, familiarity with operational standards of nursing documentation, motivation from supervisors, nurse to patient ratio, and age of nurses had a statistically significant positive association with self-reported documentation practice. Therefore this study concludes that nursing documentation remains a challenge. So it is better to put further effort toward improving documentation practice through providing training on standards of documentation and enhancing the favorable attitude of nurses toward documentation by motivating them regarding their documentation activities. The hospitals need to plan and implement standard training on nursing documentation for nurses. The nursing supervisor (matron) should oversee nurses’ documentation, evaluate, and appreciate accordingly.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio.
Acknowledgments
The authors would like to thank Dilla University, Ministry of Education, Haramaya University, all study participants, data collectors, and supervisors. In addition, we would like to acknowledge the owner of the thesis and research article1,4 on which this manuscript was based.
Disclosure
The authors declared no potential conflicts of interest for this work, nor concerning the research, authorship, or publication of this article.
References
1. Mihiretu K, Yesuf E, Desalegn TZ. Nursing care documentation practice: the unfinished task of nursing care in the University of Gondar Hospital. Inform Health Soc Care. 2017;42(3):290–302. doi:10.1080/17538157.2016.1252766
2. Taiye HB. Knowledge and practice of documentation among nurses in Ahmadu Bello University Teaching Hospital (Abuth) Zaria, Kaduna State. IOSR J Nurs Health Sci. 2015;4(6):01–6.
3. Li D. The relationship between nursing documentation and incidence of pressure ulcers in intensive care units. Open Access Dissertations 1131. 2013; Available from: https://scholarlyrepositorymiamiedu/oa_dissertations/1131.
4. Hana H. Assessment of Self-Reported Practice of Nursing Documentation and Associated Factors Among Nurses in Selected Public Hospitals, Addis Ababa, Ethiopia. AAU; 2017.
5. Okaisu EM, Kalikwani F, Wanyana G, Coetzee M. Improving the quality of nursing documentation: an action research project. Curationis. 2014;38(1):1–11. doi:10.4102/curationis.v37i2.1251
6. Nakate G, Dahl D, Drake KB, Petrucka P. Knowledge and attitudes of select ugandan nurses towards documentation of patient care. Afr J Nurs Midwifery. 2015;2(1):056–65.
7. Wang N, Hailey D, Yu P. Quality of nursing documentation and approaches to its evaluation: a mixed‐method systematic review. J Adv Nurs. 2011;67(9):1858–1875. doi:10.1111/j.1365-2648.2011.05634.x
8. Hameed RY, Allo RR. Assessment of nurses’ knowledge about nursing documentation. Kufa J Nurs Sci. 2014;4(1):1–9.
9. Jebur HG, Mohammed W. Evaluation of nursing staffs’ documentation standard related to nursing procedures at medical wards in Al-Najaf Al-Ashraf Governorate. Kufa J Nurs Sci. 2017;6(3):1–11.
10. Mohajjel AA, Lak DS, Rahmani A, Hassankhani H, Ahmadizadeh A. Survey of knowledge, attitude and performance of nursing students towards nursing documentation. Eur J Sci Res. 2012;80(2):191–198.
11. Dike FM, Onasoga OA, Njoku E. Documentation in labour among midwives in Madonna university teaching hospital elele, rivers state, Nigeria. Int J Reprod Contracept Obstet Gynecol. 2015;4:1404–1409. doi:10.18203/2320-1770.ijrcog20150719
12. Kerkina B, Lennox S, Patterson J. Making midwifery work visible: multiple purpose of documentation. Women Birth. 2017;31(2018):232–239. doi:10.1016/j.wombi.2017.09.012
13. FMOH. Fedral Ministry of Health, nursing care practice standards communication in nursing. Addis Ababa, Ethiopia 2011. Available from: https://www.medbox.org/nursing-care-practice-standards-reference-manual-for-nurses-and-healthcare.
14. FMOH. Fedral Ministry of Health, Ethiopian hospital reform implementation guidelines. 2010; Available from: https://www.scribd.com/document/358431689/Ethiopian-Hospital-Reform-Implementation-Guideline-PDF.
15. Mutshatshi TE, Mothiba TM, Mamogobo PM, Mbombi MO. Record-keeping: challenges experienced by nurses in selected public hospitals. Curationis. 2018;41(1):1931–1937. doi:10.4102/curationis.v41i1.1931
16. Jasemi M, Zamanzadeh V, Rahmani A, Mohajjel A, Alsadathoseini F. Nurses’ knowledge and practice regarding nursing documentation at tabriz teaching hospitals. Thrita J Med Sci. 2012;1(4):133–138. doi:10.5812/thrita.8023
17. Suhita BM, Sutrisno J, DewiK P. Factors influencing nurses in implementing documentation of nursing at Muhammadiyah Hospital, Kediri City. Health Notions. 2017;1(4):301–307.
18. Gizaw AB, Yimamreta E, Mamo SA. Documentation practice and associated factors among nurses working in Jimma University Medical Center, Jimma Town, South West Ethiopia. Adv Res J Multidiscip Discoveries. 2018;30(10):54–61.
19. Asamanal JA, Amenorpe D, Babanawo F, Ofei AM. Nursing documentation of inpatient care in eastern Ghana. Br J Nurs. 2014;23(1):48–55. doi:10.12968/bjon.2014.23.1.48
20. DeLaune SC, Ladner PK. Fundamentals of Nursing.
21. Machudo SY, Mohidin S. Nursing Documentation Study at teaching hospital in KSA. Nurs Health. 2015;3(1):1–6. doi:10.13189/nh.2015.030101
22. Tower M, Chaboyer W, Green Q, Dyer K, Wallis M. Registered nurses’ decision-making regarding documentation in patients’ progress notes. J Clin Nurs. 2012;21(19pt20):2917–2929. doi:10.1111/j.1365-2702.2012.04135.x
23. Blair W, Smith B. Nursing documentation: frameworks and barriers. Contemp Nurse. 2012;41(2):160–168. doi:10.5172/conu.2012.41.2.160
24. Paans W, Sermeus W, Nieweg RMB, Van Der Schans CP. D-Catch instrument: development and psychometric testing of a measurement instrument for nursing documentation in hospitals. J Adv Nurs. 2010;66(6):1388–1400. doi:10.1111/j.1365-2648.2010.05302.x
25. FMOH. Fedral Ministry of Health, Ethiopian hospital reform implementation guidelines. 2012; Available from: http://www.who.int/bulletin/online_first/BLT.14.151399.pdf.
26. Blake-Mowatt C, Lindo JLM, Bennett J. Evaluation of registered nurses’ knowledge and practice of documentation at a Jamaican hospital. Int Nurs Rev. 2013;60:328–334. doi:10.1111/inr.12040
27. Aghdam AR, Jasemi M, Rahmani A. Quality of nursing documents in medical-surgical wards of teaching hospitals related to Tabriz University of medical sciences. Iran J Nurs Midwifery Res. 2009;14(2):45–50.
28. Ausserhofer D, Zander B, Busse R, et al. Prevalence, patterns and predictors of nursing care left undone in European hospitals: results from the multicountry cross-sectional RN4CAST study. BMJ Qual Saf. 2014;23(2):126–135. doi:10.1136/bmjqs-2013-002318
29. Voyer P, McCusker J, Martin G, et al. Nursing documentation in long-term care settings: newempiricalevidence demands changes be made. Clin Nurs Res. 2014;23(4):442–461. doi:10.1177/1054773813475809
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.