Back to Journals » Infection and Drug Resistance » Volume 17
Disseminated Combined Talaromyces marneffei and Enterococcus faecium Bloodstream Infection Presenting as Gastrointestinal Perforation in a Patient with CARD9 Gene Mutation
Authors Liang H ![]() , Duan X, Li T
, Duan X, Li T ![]() , Hu L, Guo J
, Hu L, Guo J
Received 24 May 2024
Accepted for publication 14 October 2024
Published 31 October 2024 Volume 2024:17 Pages 4783—4790
DOI https://doi.org/10.2147/IDR.S479629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Huicang Liang,1,* Xuehong Duan,2,* Teng Li,3 Liang Hu,3 Jian Guo3
1Department of Laboratory Medicine, Key Laboratory of Precision Medicine for Viral Diseases, Guangxi Health Commission Key Laboratory of Clinical Biotechnology, Liuzhou People’s Hospital, Liuzhou, People’s Republic of China; 2Department of Laboratory Medicine, The First People’s Hospital of Xianyang, Xianyang, People’s Republic of China; 3Department of Laboratory Medicine, Shanghai East Hospital, School of Life Sciences and Technology, Tongji University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Guo; Liang Hu, Department of Laboratory Medicine, Shanghai East Hospital, School of Life Sciences and Technology, Tongji University, Shanghai, 200123, People’s Republic of China, Email [email protected]; [email protected]
Abstract: This study presents a case of Talaromyces marneffei combined with Enterococcus faecium bloodstream infection with gastrointestinal symptoms as the sole initial clinical manifestation.The patient is a resident of Shanghai and has no recent travel history to areas with a high risk of T. marneffei infection. He was admitted to the emergency room due to severe upper abdominal pain. Laboratory tests indicated elevated levels of white blood cells, rapid C-reactive protein, and procalcitonin, while the human immunodeficiency virus (HIV) test returned negative. An abdominal CT examination revealed gas and fluid accumulation in the abdominal cavity, raising suspicion for gastrointestinal perforation and peritonitis. Initially, he received symptomatic treatment for gastrointestinal perforation and abdominal infection, but his response to the treatment was poor.Through metagenomic next-generation sequencing (mNGS) and multiple blood cultures, a mixed infection of T. marneffei and E. faecium was identified in the patient’s blood. Combination treatment with vancomycin and amphotericin B was initiated to manage the symptoms. However, we discovered genome-wide exon CARD9 mutations in the patient, complicating the treatment process. Ultimately, the delayed diagnosis of T. marneffei resulted in the patient’s severe deterioration, rendering the anti-infective treatment ineffective, and leading to the patient’s death.This report underscores the challenges associated with diagnosing T. marneffei infections in non-AIDS patients and in non-endemic regions. The diagnosis of disseminated infections poses significant difficulties, particularly when mixed infections are present, complicating clinical treatment. This highlights the critical importance of standardized blood cultures for the early diagnosis of T. marneffei. Additionally, we must prioritize timely whole-genome testing to identify potential immune gene mutations.
Keywords: Talaromyces marneffei, drug susceptibility, disseminated infection, HIV, CARD9 gene mutation, antifungal antibacterial therapy
Introduction
There is a significant body of literature on T. marneffei infections. T. marneffei infection primarily affects individuals with compromised immune systems, with most cases occurring in HIV-positive individuals.1–4 The endemic range of T. marneffei is expanding, which has led to an increased incidence rate of infections.5 Disseminated T. marneffei infection has also been reported in HIV-negative patients virus (HIV)-negative patients.4,5 However, there are few reports of T. marneffei bloodstream infection with non-respiratory symptoms as the first manifestation. Here, we report a rare case of disseminated T. marneffei combined with E. faecium infection in a non-AIDS, non-endemic area, with gastrointestinal symptoms as the first symptom. Atypical clinical symptoms are difficult to diagnose in patients. Standardizing blood cultures and mNGS can facilitate the early detection of pathogens. Additionally, it is crucial to monitor vulnerable populations with CARD9 mutations across all the exons of the genome. Currently, there are no reports of such cases of T. marneffei bloodstream infection abroad, with the majority of cases reported in China. This warrants careful study to alert clinicians regarding this particular disease.
Case
Clinical Information
The patient was a 63-year-old male from Shanghai with a medical history of hypertension for over a decade, chronic kidney disease for 6 years, stage 4 chronic renal failure, and Henoch-Schonlein purpura for 2 years. The patient presented with severe and persistent mid-upper abdominal pain of unknown etiology along with cold sweats. He was admitted to the emergency department, where examination revealed upper abdominal tenderness, radiating back pain, and no symptoms of nausea, vomiting, chills, or fever.
Routine Laboratory Testing
The patient was negative for human immunodeficiency virus antibody, hepatitis C antibody, and Treponema pallidum-specific antibody. Routine blood tests revealed 7.74 × 109/L leukocytes (reference range, 3.5–9.5×109 /L), 94.2% neutrophils (reference range, 45%-70%). The serum amyloid and C-reactive protein levels were >288.00 mg/L (reference range, <10mg/L) and 141.65 mg/L (reference range, <10mg/L), respectively. The interleukin 6 and procalcitonin were 293.0pg/mL (reference range, <7pg/mL) and 17.90ng/mL (reference range, <0.05ng/mL), respectively. The interleukin (IL)-12 level was below 2.50pg/mL (reference range, 0–3.40pg/mL), the anti-interferon-γ level was 2.83pg/mL (reference range, 0–14pg/mL), and the tumor necrosis factor (TNF)-α was below 2.50pg/mL (reference range, 740–1540pg/mL). The serum 1,3-β-D glucan test yielded a negative result, whereas the galactomannan antigen test yielded a strong positive result with I value of 3.786.
Laparoscopy and Imaging Results
Abdominal CT tomography revealed gas and fluid accumulation in the abdominal cavity. Further laparoscopic exploration revealed a large volume of white purulent turbid fluid (approximately 3000 mL) within the abdominal cavity. Purulent fur was observed adhering to the entire small intestine and forming clumps due to adhesion. Additionally, dilation of the colon was noted and the stomach and omentum appeared to be wrapped in a pie shape. Notably, lung computed tomography (CT) showed no abnormalities.
Microbial Culture
Bronchoalveolar lavage fluid was cultured and Stenotrophomonas maltophilia was detected. Sputum culture showed no fungal growth. Anaerobic and aerobic cultures of the blood culture bottle were positive, revealing gram-positive cocci identified as E. faecium using matrix-assisted laser desorption-ionization time-of-flight mass spectrometry (MALDI-TOF) EXS3000 (Zybio, China). Aerobic culture from the blood culture sample was collected, and smears were used for fluorescence and Gram staining. Microscopic examination revealed a large number of branched and septate hyphae. (Figure 1A and B). These samples were then transferred to Sabouraud dextrose agar and cultured at 35 and 25°C. After 72 h, colonies cultured at 35°C appeared round, convex, smooth, moist, and milky white with brain-like folds in the center. Colonies cultured at 25°C displayed light-gray, brown, and slightly reddish villi-like structures, producing water-soluble red pigments (Figure 1C). The central aerial hyphae were white and fluffy, and were identified as T. marneffei through mass spectrometry. In vitro antifungal drug susceptibility testing was conducted according to the CLSI M27 and CLSI M57 protocols approved by the National Clinical Laboratory Standards Committee. Tests were performed on both the yeast and mycelial phases, with consistent experimental results. MICs for itraconazole, posaconazole, voriconazole and amphotericin B were as follows: 0.015μg/mL, ≤0.008μg/mL, 0.015 μg/mL, 0.25 μg/mL, respectively. MICs for echinocandins and fluconazole were comparatively high. The distribution of MIC values in this study was consistent with the susceptibility results of 100 T. marneffei strains previously tested in our laboratory,6,7 as shown in Table 1.
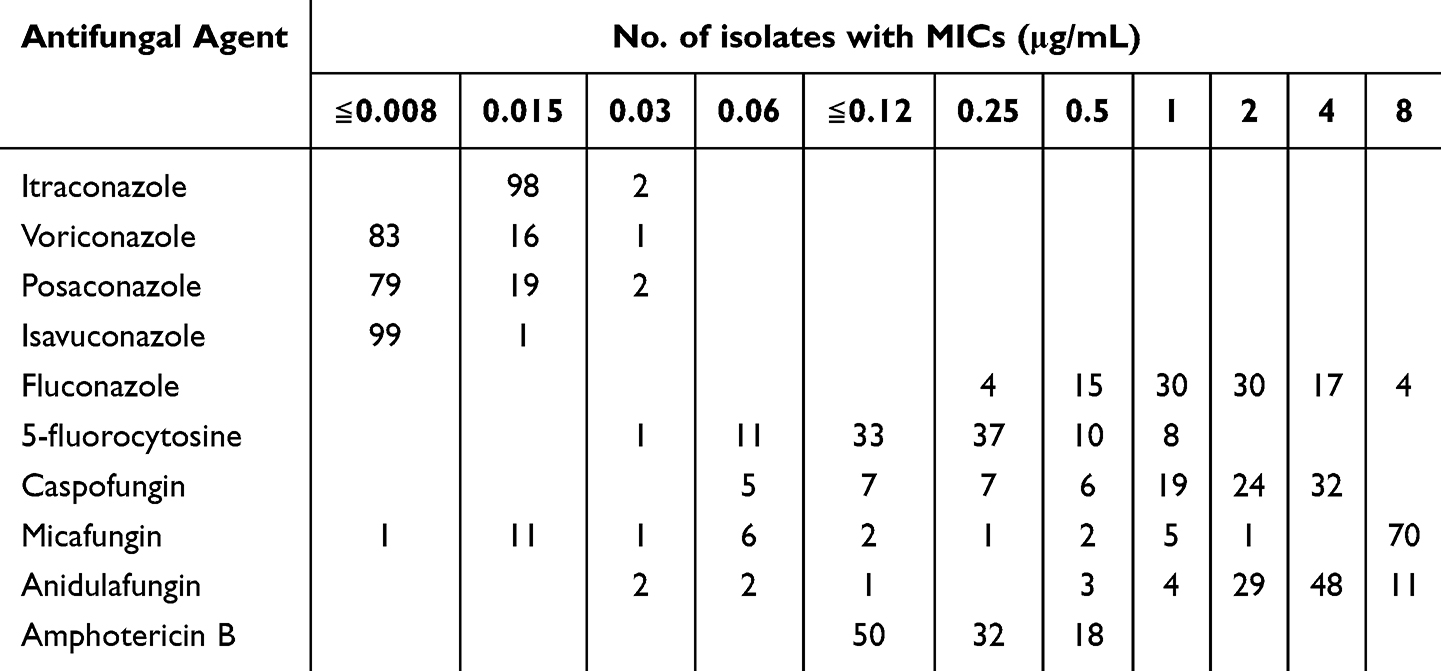 |
Table 1 In vitro MIC (μg/Ml) of the 100 T. marneffei Strains Against 10 Antifungals as Determined by YeastOne Method |
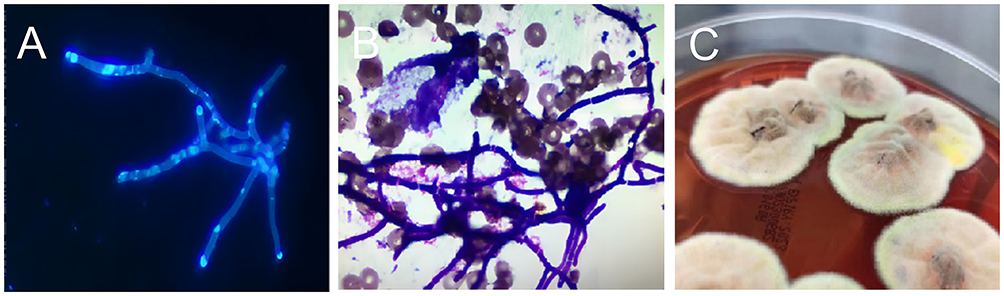 |
Figure 1 Colony morphology and microscopic morphology of T. marneffei. (A) Smear of positive blood culture sample (BaSO fluorescent staining,magnification × 1000). (B) Smear of positive blood culture sample (Gram stain,magnification × 1000). (C) Morphology of T. marneffei (Cultivated on Sabouraud dextrose agar at 25°C for 96h). |
Molecular Biology Testing
Peripheral blood samples were collected from patients for NGS. Through high-throughput sequencing and bioinformatics analysis of nucleic acids extracted from the patient’s peripheral blood, information on the types and abundance of microorganisms in the samples was obtained. Detection includes over 24,000 pathogens, including bacteria, fungi, viruses, parasites, and other pathogenic microorganisms. Quantitatively determining the ratio of human nucleic acids and the levels of pathogenic microorganisms in a sample can be achieved by introducing artificially synthesized tag sequences. The detection results included the presence of bacteria, specifically E. faecium, with a sequence reads of 1013 and a relative abundance of 38.64%. Additionally, a highly pathogenic fungus T. marneffei, was detected, with 86 sequence reads and a relative abundance of 18.98%. The test results indicated a mixed infection involving E. faecium and T. marneffei, consistent with the culture findings. The patient’s serum was analyzed using the Talaromyces marneffei antigen detection kit (colloidal gold method). The patient’s serum test was negative for T. marneffei antigen, whereas the antigen test with the T. marneffei culture yielded positive results.
Genome-Wide Exon Detection for CARD9 Gene Mutation
Samples of deoxyribonucleic acid (DNA) were meticulously extracted from the patient’s peripheral blood for in-depth analysis. Exome capture sequencing was performed using the Agilent SureSelect Human All-Exon V8 Kit, focusing on the coding exons of approximately 5000 genes associated with diseases. Medical exome sequencing (MES) was performed using the NovaSeq X Plus PE150 platform. The sequencing data obtained were aligned with the human genome sequence hg19 (GRCh37.p13) to identify potential mutations associated with the disease. To ensure the accuracy of the identified variants, those with minor allele frequencies above 0.1% were filtered out by referencing established variant databases such as the Exome Aggregation Consortium (ExAC) and the Genome Aggregation Database (gnomAD). Mutations in CARD9 were detected at four specific locations within the patient’s DNA, with c.G35A (p.S12N) identified as a non-synonymous mutation, indicating a possible impact on protein function.
The Treatment Process
Following admission, the patient was initially treated with imipenem for anti-infection purposes. Upon the identification of gram-positive bacteria in the microbial culture, intravenous vancomycin (500 mg, q12h) was initiated. Subsequently, caspofungin was added when the serum galactomannan antigen test result was strongly positive. However, the anti-infective effects were not apparent. Following the identification of T. marneffei in the blood sample culture, voriconazole tablets (400 mg bid) were administered orally, based on the minimum inhibitory concentration determined from the drug susceptibility test results provided by the laboratory. After 4 days, the treatment was switched to intravenous voriconazole (0.2 g every 12 hours). Despite these interventions, the patient’s response was unsatisfactory. The patient was switched to an amphotericin B cholesterol sulfate complex regimen of 50 mg on the first day, 100 mg on the second day, and 150 mg intravenously once daily on the third day and thereafter. Owing to the patient’s autoimmune system disease and T. marneffei combined with a mixed bacterial infection, his condition deteriorated. Despite receiving symptomatic drug treatment, the patient’s condition did not improve and he died.
Discussion
T. marneffei is an opportunistic airborne fungal pathogen that primarily affects the respiratory system of patients.1 Infection is believed to occur through the inhalation of conidia, which subsequently transform into yeast and disseminate from the lungs to other organs via the reticuloendothelial system.2 T. marneffei is classified as a facultative intracellular pathogen, with the phase transition to yeast occurring within the phagosomes of macrophages following the phagocytosis of conidia.2 To survive and proliferate within macrophages, T. marneffei yeasts have developed various adaptation and attack strategies to enhance their pathogenicity and virulence in the hostile environment of the host.2 T. marneffei was previously identified as Penicillium marneffei.3 This fungus is temperature-dependent and biphasic, and is capable of causing disseminated infection.4 Similar to other major causes of systemic mycoses, the extent of disease and outcomes are the results of complex interactions between this opportunistic human pathogen and a host’s immune response.3,8 T. marneffei is a primary pulmonary pathogen that disseminates to other internal organs through lymphatic or hematogenous routes.3,9 It can cause disseminated disease in both immunocompetent and immunocompromised individuals, however, it is most commonly observed in patients with HIV/AIDS and those with functional impairments in cellular immunity, particularly defects in CD4 T cell activity.3 However, this condition is unusual in non-AIDS patients. Disseminated T. marneffei infections typically affect the reticuloendothelial system of various organs.5 These include the skin, lungs, bones, bone marrow,8 lymph nodes, liver, and the spleen.10,11 Additionally, cases of infection of the mesentery, central nervous system,12 and trachea have been documented.13 However, there are few reports regarding the spread of infection to the digestive tract and the development of severe complications such as visceral perforation in HIV-negative individuals. The patient in our study had abdominal pain and underwent an abdominal CT examination, which revealed gas and fluid accumulation in the abdominal cavity. Laparoscopic exploration revealed a large amount of white purulent turbid fluid totaling approximately 3000 mL in the abdominal cavity. Adhesions in the form of clumps were observed on the surface of the small intestine. The colon was dilated and the stomach and omentum were wrapped in a pie shape. Initially, the clinical manifestations did not suggest T. marneffei infection. Symptomatic treatment for the gastrointestinal perforation was initiated; however, the treatment response was unsatisfactory. Ultimately, blood culture detected T. marneffei and confirmed the disseminated infection. Prior studies indicate that T. marneffei is the main pulmonary pathogen obtained through inhalation of spores.14 T. marneffei primarily infects the monocyte-macrophage system, leading to acute lung disease.15 It subsequently spreads through the bloodstream to the skin, reticuloendothelial system, bone marrow, intestine, and other organ systems.16 However, in our case, recurrent diarrhea and abdominal pain were the only early symptoms. This is a rare case of T. marneffei infection. Therefore, we considered that the intestine may be the site of primary infection via ingestion.
T. marneffei is commonly found in tropical regions, such as southern China, Hong Kong, Taiwan, and Southeast Asia.17 Bamboo rats act as natural hosts.18 However, the specific origin of human infections is still unknown. Studies have shown that a major contributing factor comes into contact with regions where T. marneffei is common,17 with a potential incubation period lasting up to a decade.16 Having underlying conditions, such as AIDS, along with a travel history to an endemic area can aid doctors in reaching the correct diagnosis. However, our patient resided in Shanghai and denied visiting any region where T. marneffei has been prevalent in the last decade. As a result, the origin of the infection in this particular case remains unknown. There have been occasional reports of T. marneffei infection in non-endemic areas in recent years. The source of infection remains unclear, highlighting the need for additional environmental investigations and future research. In cases where the clinical diagnosis is uncertain and traditional anti-infective treatments are ineffective, it is important to consider the potential for infection by unique pathogens in non-endemic regions. Previous studies indicate a potential correlation between T. marneffei infection in HIV-negative individuals and immune deficiencies.15,19 These include Th17 deficiency, CD40 ligand deficiency, STAT1 GOF deficiency, STAT3 deficiency, X-SCID, IFN-γ receptor 1 deficiency, CARD9 deficiency, ADA deficiency, RelB deficiency and NFKB2 deficiency.20 Mutations in the autosomal dominant phosphorylation signal transducer and transcription activator STAT1 and STAT3 heterozygous missense mutations.20 The patients in our study exhibited mutations in the immune gene, CARD9, which is a crucial molecule for fungal immune surveillance. CARD9 is predominantly expressed in macrophages and myeloid dendritic cells, where it plays a central role in antifungal defense by receiving signals from various C-type lectin-like receptors and triggering pro-inflammatory responses.19 After reviewing the current literature, it was posited that mutations in CARD9 could potentially elevate vulnerability to fungal infections.19,20 Patients who are HIV antibody-negative and infected with T. marneffei, particularly those with disseminated infection and no other susceptibility factors, should be vigilant regarding the potential presence of a primary immunodeficiency disease. Nonetheless, literature concerning genetic predisposition in relation to T. marneffei infection is notably sparse, thus necessitating further investigation.
Isolation of the fungus from clinical specimens is considered the gold standard for confirming the diagnosis of T. marneffei infection diagnosis.15,16 However, the extended incubation period for T. marneffei poses.18 The difficulty in cultivating microorganisms makes early clinical diagnosis difficult.21 Research indicates that a combined approach using a serum 1.3-β-D glucan detection test and galactomannan antigen detection test is a common indicator for detecting invasive fungal infections.22 These tests can yield positive results 4–7 days earlier than the clinical symptoms and imaging abnormalities.23 The patient’s serum 1.3-β-D glucan test was negative, whereas the galactomannan antigen test showed a strong positive result with I value of 3.786, which aligns with existing literature. It is important to note that 1.3-β-D glucan detection test is not specific to particular species.22 In contrast, the galactomannan antigen is a specific antigen found in the Aspergillus cell wall. This antigen detection test is sensitive to Aspergillus and T. marneffei, with a cross-reactivity rate of > 70%.23 Therefore, in this case, when the galactomannan test result was positive, invasive fungal infection was suspected and the diagnosis of T. marneffei infection could not be confirmed. The T. marneffei antigen detection kit is currently used in clinical settings because of its high specificity for plasma samples, high sensitivity, low false-positive rate, and short detection time.24 This facilitates rapid diagnosis of T. marneffei. However, some studies have indicated that this occurs during the early stages of acute T. marneffei.24 Antigens are predominantly found in the blood, with a gradual decrease to negative levels in later stages of infection.24 Consequently, false negatives may occur in T. marneffei antigen tests. The negative antigen test results in this case may be attributed to the decline of antigens in the plasma during the later stages of T. marneffei infection, a phenomenon that is consistent with the existing literature.
Traditional diagnostic methods for T. marneffei infection include fungal culture, pathological examination, or direct microscopic examination. These methods often involve lengthy culture times or struggle to accurately identify the pathogen, thereby presenting obstacles for early diagnosis. Metagenomic next-generation sequencing (mNGS) is a recently developed technology for detecting nucleic acids that can aid in identifying infectious pathogens.25 The Expert Consensus on the Clinical Application of Chinese Metagenomics Second-Generation Sequencing Technology for Detection of Infectious Pathogens’ suggests.26 If blood culture results are negative after 3 days and empiric anti-infective treatment is ineffective, mNGS testing can be conducted on stored blood samples.26 Studies have confirmed that mNGS is effective in detecting a wide range of pathogens.27 It has shown significant advantages in identifying mixed infections in patients with T. marneffei.28 The sensitivity and specificity of mNGS have been reported to be 98.3% and 98.6% respectively,28 which can provide valuable assistance in clinical decision-making. In our study, the blood samples were subjected to mNGS. Mixed infections with E. faecium and T. marneffei. These results are consistent with those of the subsequent blood cultures. This study suggests that a single detection method has limitations in the clinical diagnosis of T. marneffei infection. We need to use A combination of etiology, serology, PCR detection methods, second-generation sequencing, and other detection methods is required to quickly and effectively diagnose the pathogen. This provides assistance for early clinical diagnosis.
Currently, there is a lack of international documents and guidelines for standardized in vitro drug susceptibility testing for T. marneffei,29 including the absence of clinical breakpoints (CBPs) and critical epidemiological values (ECVs).30 Amphotericin B, itraconazole, and voriconazole are effective in treating T. marneffei infections.6,31 The recommended dose and duration of treatment for infection in HIV-positive adult patients is intravenous amphotericin B deoxycholate at a dosage of 0.6–1.0 mg/kg/day for a 2-week. Oral itraconazole (400 mg/day for 8–10 weeks.31 Treatment guidelines for HIV-negative patients have not yet been standardized. In clinical practice, we can only administer empirical medication according to previous studies. However, clinical outcomes are closely related to patients’ basic status, immune function status, and organ function. Adverse effects of amphotericin B, such as severe anemia, electrolyte imbalance, nephrotoxicity, and hepatotoxicity, occur frequently and limit its clinical application.30 The patient was treated with voriconazole and amphotericin B to relieve symptoms. Unfortunately, despite treatment, the patient experienced multiple organ failure, which was not successfully treated. The most likely reason for this may be the adverse events associated with amphotericin B use in patients with severe systemic inflammatory response syndrome and autoimmune diseases. More research is needed on treatment methods for special cases of rare pathogenic infections to reduce the mortality rate. If pathogenic bacteria can be diagnosed early, early clinical intervention may improve cure rates. Research indicates a higher fatality rate of T. marneffei infection in non-HIV-infected individuals than in those with HIV.32 This may be linked to delayed identification resulting from a lack of suspicion in the clinical settings.33 It has been observed that many non-AIDS patients with T. marneffei infection are initially misdiagnosed and treated empirically for other conditions.7,32 In these cases, the diagnosis of T. marneffei infection is often delayed by several weeks to months.33 Droplet digital PCR has emerged as a promising tool for pathogenic fungal early detection with high sensitivity.34 Consistent with previous studies, our patient also had delayed diagnosis. Initially, only symptoms of gastrointestinal perforation were present, and E. faecium was detected in the blood culture. Because the patient was not HIV-infected and had no history of travel to areas where specific pathogenic bacteria were common, T. marneffei infection was not suspected early. The effectiveness of symptomatic imipenem and caspofungin as anti-infective treatments was not statistically significant. It was only a month after admission that a mixed infection of E. faecium and T. marneffei was confirmed through mNGS and multiple blood culture results. Despite timely correction of the anti-infective treatment plan with vancomycin and amphotericin B, delayed diagnosis, spread of T. marneffei infection, delayed anti-infective intervention, and mixed infections pose significant challenges to treatment and ultimately lead to treatment failure. The challenge of diagnosing T. marneffei infection in HIV-negative patients without typical symptoms or in those living in non-endemic areas remains significant. Additionally, there are substantial difficulties in treating mixed infections involving T. marneffei and other bacteria, highlighting the need for further research.
Conclusion
Here, we report a rare case of disseminated T. marneffei and E. faecium. The only early symptom was a gastrointestinal infection. While this case study has limitations in its generalizability to a larger population, it offers valuable in-depth clinical insights into T. marneffei infections. Important aspects of this case include awareness of the potential infection in non-AIDS patients, patients with immune gene mutations, and those who are non-endemic in China. Recognizing fatal outcomes resulting from delays in diagnosis and treatment is crucial. When anti-infection treatments fail to effectively treat an infection, it may be difficult to detect the pathogen using traditional methods. Clinicians should consider opportunistic pathogenic infections. Metagenomic next-generation sequencing can quickly and accurately identify pathogens, especially mixed infections, thus supporting early clinical decision making. If there is co-infection with T. marneffei and other bacteria, timely whole-genome screening is important to identify diseases that may harbor immune gene mutations. In future clinical research, it is crucial to conduct thorough investigations into the monitoring, prevention, and treatment of T. marneffei infection in patients without AIDS. This includes exploring improved immunotherapy techniques, developing new antifungal drugs, and developing vaccines. These efforts aim to facilitate early detection and treatment, ultimately enhancing patient outcomes.
Data Sharing Statement
The original contributions of this study are as follows. Further inquiries can be directed to the corresponding authors.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Shanghai East Hospital (Tongji University School of Medicine). The patient’s wife provided written informed consent to participate in this study.
Consent for Publication
Written informed consent was obtained from the patient’s wife for the publication of this case report. The consent form is available for review by the editor, when needed.
Acknowledgments
The authors thank the patients for their cooperation in the diagnostic process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, sample culture and isolation, antibiotic susceptibility testing, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to take responsibility and be accountable for the content of the article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no competing interests to declare relevant to the content of this article.
References
1. Pongpech N, Rotjanapan P. Absence of cutaneous involvement in disseminated Talaromyces marneffei infection in an AIDS patient: a case report and literature review. Infect Drug Resist. 2019;12:1493–1499. doi:10.2147/IDR.S207819
2. Pruksaphon K, Amsri A, Thammasit P, Nosanchuk JD, Youngchim S. Extracellular vesicles derived from Talaromyces marneffei contain immunogenic compounds and modulate THP-1 macrophage responses. Front Immunol. 2023;14:1192326. doi:10.3389/fimmu.2023.1192326
3. Pruksaphon K, Nosanchuk JD, Ratanabanangkoon K, Youngchim S. Talaromyces marneffei infection: virulence, intracellular lifestyle and host defense mechanisms. J Fungi. 2022;8(2):200. doi:10.3390/jof8020200
4. Zeng W, Qiu Y, Tang M, et al. Talaromyces marneffei and Burkholderia cepacia co-infection in a HIV-uninfected patient with anti-interferon-γ autoantibodies. Infect Drug Resist. 2021;14:2173–2177. doi:10.2147/IDR.S312042
5. Sun A, Gou X, Zhu Y, et al. Identification of Talaromyces marneffei infection in an HIV-negative patient by ITS sequencing. Infect Drug Resist. 2023;16:5275–5282. doi:10.2147/IDR.S418174
6. Huang CL, He YY, Liang HC, et al. MALDI-TOF MS-based clustering and antifungal susceptibility of 99 Talaromyces marneffei strains. AIDS STDs China. 2023;29(2):146–150. doi:10.13419/j.cnki.aids.2023.02.05
7. Fang L, Liu M, Huang C, et al. MALDI-TOF MS-based clustering and antifungal susceptibility tests of Talaromyces marneffei isolates from Fujian and Guangxi (China). Infect Drug Resist. 2022;15:3449–3457. doi:10.2147/IDR.S364439
8. Liu X, Xing H, Lin J, et al. Coexisting of primary central nervous system lymphoma and Talaromyces marneffei brain abscess in an AIDS patient, a case report and review of the literature. Infect Drug Resist. 2024;17:709–718. doi:10.2147/IDR.S432697
9. Narayanasamy S, Dat VQ, Thanh NT, et al. A global call for talaromycosis to be recognised as a neglected tropical disease. Lancet Glob Health. 2021;9(11):e1618–e1622. doi:10.1016/S2214-109X(21)00350-8
10. Wang F, Han R, Chen S. An overlooked and underrated endemic mycosis-talaromycosis and the pathogenic fungus Talaromyces marneffei. Clin Microbiol Rev. 2023;36(1):e0005122. doi:10.1128/cmr.00051-22
11. Xue X, Zou J, Fang W, et al. Characteristics and prognosis of Talaromyces marneffei infection in HIV-positive children in southern China. Mycopathologia. 2022;187(2–3):169–180. doi:10.1007/s11046-021-00614-5
12. Sun J, Sun W, Tang Y, et al. Clinical characteristics and risk factors for poor prognosis among HIV patients with Talaromyces marneffei bloodstream infection. BMC Infect Dis. 2021;21(1):514. doi:10.1186/s12879-021-06232-2
13. Cao C, Xi L, Chaturvedi V. talaromycosis (penicilliosis) due to Talaromyces (penicillium) marneffei: insights into the clinical trends of a major fungal disease 60 years after the discovery of the pathogen. Mycopathologia. 2019;184(6):709–720. doi:10.1007/s11046-019-00410-2
14. He L, Mei X, Lu S, et al. Talaromyces marneffei infection in non-HIV-infected patients in mainland China. Mycoses. 2021;64(10):1170–1176. doi:10.1111/myc.13295
15. Chen D, Chang C, Chen M, et al. Unusual disseminated Talaromyces marneffei infection mimicking lymphoma in a non-immunosuppressed patient in east China: a case report and review of the literature. BMC Infect Dis. 2020;20(1):800. doi:10.1186/s12879-020-05526-1
16. Pan M, Qiu Y, Zeng W, et al. Disseminated Talaromyces marneffei infection presenting as multiple intestinal perforations and diffuse hepatic granulomatous inflammation in an infant with STAT3 mutation: a case report. BMC Infect Dis. 2020;20(1):394. doi:10.1186/s12879-020-05113-4
17. Wong SS, Wong KH, Hui WT, et al. Differences in clinical and laboratory diagnostic characteristics of Talaromyces marneffei in human immunodeficiency virus (HIV) and non-HIV-infected patients. J Clin Microbiol. 2001;39(12):4535–4540. doi:10.1128/JCM.39.12.4535-4540.2001
18. Guo P, Li L, Tang X. Advances in diagnosis and treatment of Talaromyces marneffei in patients with AIDS. Chin Med J. 2022;135(22):2687–2689. doi:10.1097/CM9.0000000000002506
19. You CY, Hu F, Lu SW, et al. Talaromyces marneffei infection in an HIV-negative child with a CARD9 mutation in China: a case report and review of the literature. Mycopathologia. 2021;186(4):553–561. doi:10.1007/s11046-021-00576-8
20. Wang L, Luo Y, Li X, et al. Talaromyces marneffei infections in 8 Chinese children with inborn errors of immunity. Mycopathologia. 2022;187(5–6):455–467. doi:10.1007/s11046-022-00659-0
21. Du R, Feng Y, Mao H. Case report: diagnosis of Talaromyces marneffei infection in an HIV-negative patient with septic shock and high-titer anti-interferon gamma autoantibodies by metagenomic next-generation sequencing. Front Cell Infect Microbiol. 2023;13:1163846. doi:10.3389/fcimb.2023.1163846
22. Huang YT, Hung CC, Liao CH, et al. Detection of circulating galactomannan in serum samples for diagnosis of Penicillium marneffei infection and cryptococcosis among patients infected with human immunodeficiency virus. J Clin Microbiol. 2007;45(9):2858–2862. doi:10.1128/JCM.00050-07
23. Zheng Y, He Y, Liu JY, et al. Diagnostic value of serum (1,3)-β-D glucan test and serum galactomannan test for Talaromyces marneffei. Chin J Mycol. 2022;17(5):385–390.
24. Chen X, Ou X, Wang H, et al. Talaromyces marneffei Mp1p antigen detection may play an important role in the early diagnosis of Talaromycosis in patients with acquired immunodeficiency syndrome. Mycopathologia. 2022;187(2–3):205–215. doi:10.1007/s11046-022-00618-9
25. Chinese Pharmacists Association; Branch of Bacterial Infection and Resisatnce Prevention of Chinese Medical Association; Expert Committee of the National Health Commission on Antimicrobial Susceptibility Testing and Standard Research. Expert consensus on clinical localization detection standards for metagenomic next generation sequencing of pathogens. Zhonghua Yu Fang Yi Xue Za Zhi. 2024;58:1–12. Chinese. doi:10.3760/cma.j.cn112150-20230720-00019
26. Chen Q, Qiu Y, Zeng W, et al. Metagenomic next-generation sequencing for the early diagnosis of Talaromyces marneffei in HIV-uninfected patients: five cases report. BMC Infect Dis. 2021;21(1):865. doi:10.1186/s12879-021-06551-4
27. Cao Q, Chen B, Chen L, et al. Expert consensus on the clinical application of metagenomics next-generation sequencing technology for detection of infectious pathogens in China. Chin J Infect Dis. 2020;38(11):681–689. doi:10.3760/cma.j.cn311365-20200731-00732
28. Liu L, Sun B, Ying W, et al. Rapid diagnosis of Talaromyces marneffei infection by metagenomic next-generation sequencing technology in a Chinese cohort of inborn errors of immunity. Front Cell Infect Microbiol. 2022;12:987692. doi:10.3389/fcimb.2022.987692
29. Huang W, Li T, Zhou C, et al. Voriconazole versus amphotericin B as induction therapy for Talaromyces marneffei in HIV/AIDS patients: a retrospective study. Mycopathologia. 2021;186(2):269–276. doi:10.1007/s11046-021-00533-5
30. Liu D, Liang L, Chen J. In vitro antifungal drug susceptibilities of Talaromyces marneffei from China. J Infect Chemother. 2013;19:776–778. doi:10.1007/s10156-012-0511-7
31. He R, Zhang CJ, Kong WJ, et al. Progress in the application of voriconazole in Talaromyces marneffei infection. Chin J Mycol. 2023;18(3):273–275.
32. Yang S, Lou L, Ma S, et al. Disseminated Talaromyces marneffei infection initially presenting as cutaneous and subcutaneous lesion in an HIV-negative renal transplant recipient: a case report and literature review. BMC Infect Dis. 2024;24(1):473. doi:10.1186/s12879-024-09351-8
33. He H, Cai L, Lin Y, et al. Advances in the understanding of talaromycosis in HIV-negative patients (especially in children and patients with hematological malignancies): a comprehensive review. Med Mycol. 2024;62(10):myae094. doi:10.1093/mmy/myae094
34. Guo J, Tian W, Lin H, et al. Analytical and clinical validation of multiplex droplet digital PCR assay for detecting pathogenic fungal infection in lungs. Mycology. 2023;15(1):110–119. doi:10.1080/21501203.2023.2296941
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis (SAPHO) Syndrome with Cutis Verticis Gyrata: Case Report and Review of Literature
Wang Y, Wang S, Zheng L, Wang X, Wang H, Zhong Z, Liu S, Zheng X, Gao M
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1415-1420
Published Date: 23 July 2022
Talaromyces marneffei is the Persistent Overwhelming Bloodstream Infection Pathogen Among HIV Inpatients in Fujian, China
Lai J, Liu Y, Ye H, Chen Y
Infection and Drug Resistance 2022, 15:5207-5214
Published Date: 5 September 2022
AIDS-Associated Talaromyces marneffei Infection with Thoracic Spinal Cord Involvement Leading to Paraplegia: A Case Report and Literature Review
Guo Y, Song Y, Peng X, Zhou X, Zhou H, Xu L, Zhu B
Infection and Drug Resistance 2025, 18:1263-1269
Published Date: 4 March 2025
Aplastic Anaemia Disease Burden From the Patient Perspective and Quality of Life in Zimbabwe by A. Maramba and J. Mupini
Maramba A, Mupini J, Munyati S, Maboreke TC, Manasa J, Gwanzura L
Journal of Blood Medicine 2025, 16:259-268
Published Date: 30 May 2025
HIV Complicated with Talaromyces Marneffei Multisystem Infection: A Case Report and Literature Review
Zhang G, Wu G, Xu Y, Yang L, Yang W
Infection and Drug Resistance 2025, 18:3561-3568
Published Date: 21 July 2025