Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis (SAPHO) Syndrome with Cutis Verticis Gyrata: Case Report and Review of Literature
Authors Wang Y, Wang S, Zheng L, Wang X, Wang H, Zhong Z, Liu S, Zheng X, Gao M
Received 29 April 2022
Accepted for publication 14 July 2022
Published 23 July 2022 Volume 2022:15 Pages 1415—1420
DOI https://doi.org/10.2147/CCID.S372522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yifan Wang,1– 3 Shan Wang,1– 3 Liyun Zheng,1– 3 Xiuli Wang,1– 3 Hui Wang,1– 3 Zhenyu Zhong,1– 3 Siqi Liu,1– 3 Xiaodong Zheng,1– 3 Min Gao1– 3
1Department of Dermatology, the First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China; 2Key Laboratory of Dermatology (Anhui Medical University), Ministry of Education, Hefei, Anhui, People’s Republic of China; 3Inflammation and Immune Mediated Diseases Laboratory of Anhui Province, Hefei, People’s Republic of China
Correspondence: Min Gao; Xiaodong Zheng, Department of Dermatology, the First Affiliated Hospital of Anhui Medical University, No. 81 Meishan Road, Hefei, Anhui, 230032, People’s Republic of China, Tel/Fax +86-0551-62923042, Email [email protected]; [email protected]
Abstract: SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) syndrome is a rare disease clinically characterized by a wide range of cutaneous and osteoarticular manifestations. Here, we report a case of SAPHO syndrome with cutis verticis gyrata (CVG) and investigated the genetic causes in the four members of this pedigree. After failure of conventional treatments, a recombinant human TNF-α receptor II:IgG Fc fusion protein (rhTNFR:Fc, YISAIPU®) achieved good control of the disease at the 2-year follow-up. We did not identify any pathogenic mutation in this pedigree. We also summarized the clinical and therapeutic characteristics of 83 patients with SAPHO syndrome through the China National Knowledge Infrastructure (CKNI) database from 2016 to 2021. Patients with acne were young and predominantly male. About 45.8% patients were treated with biological therapies or traditional Chinese medicine (TCM), 84.2% of which showed positive effects against cutaneous and osteoarticular manifestations. We report a case of SAPHO syndrome with CVG that was successfully treated with rhTNFR:Fc. Our results reveal the genetic heterogeneity involved. Biologics and TCM are likely alternative options for the treatment of SAPHO syndrome.
Keywords: cutis verticis gyrata, gene mutation, SAPHO syndrome, treatment, whole-exome sequencing
Introduction
SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) syndrome is a rare disease first described by Chamot et al in 1987.1 The prevalence of SAPHO syndrome is thought to be less than 1 in 10,000 in Caucasians.2 The most commonly affected area of osteoarticular manifestations is the anterior chest wall (ACW) (mainly the sternum, clavicles, and sternocostoclavicular joints), followed by the axial skeleton (including the spine and sacroiliac joints) and the extremities.3 The most frequent skin manifestations of SAPHO syndrome are palmoplantar pustulosis (PPP) and severe acne.4 Currently, the exact etiopathogenesis of SAPHO syndrome remains unclear, but genetic susceptibility is understood to be one of its various etiologies owing to familial clustering.5 The commonly used diagnostic criterion of SAPHO syndrome was proposed by Kahn and Khan in 1994.2
Cutis verticis gyrata (CVG) is a rare benign condition of the scalp with dermal thickening that induces rigid folds and furrows resembling the cerebral cortex.6 CVG is classified into primary and secondary forms; secondary CVG is related to various causes including inflammatory, neoplastic, and metabolic conditions.7
In this study, we described a case of SAPHO syndrome with CVG in a young Chinese male patient that was successfully treated with a tumor necrosis factor (TNF)-α antagonist at the 2-year follow-up.
Case Report
A 16-year-old Chinese male patient presented to the Department of Dermatology of our hospital in June 2019, complaining of painful inflammatory abscesses on the face and swelling on both knees. The patient had a history of relapsing facial acne since 2017. Seven months before admission, both of his lower limbs had purpura, which was diagnosed as Henoch–Schönlein purpura. He was treated with methylprednisolone and cyclosporin A in the local hospital, with no recurrence after remission. Then, he showed a gradual worsening of acne that manifested as acne conglobata. At the same time, both of his knees began to feel swollen, leading to limited activities. Physical examination on admission revealed numerous papules, pustules, cysts, draining sinus tracts, and hypertrophic scars on the face, part of which coalesced into plaques (Figure 1A). There was CVG on his head (Figure 1B). There was also swelling and tenderness on both knees (Figure 1C). The floating patella test was positive. Skin thickening, roughness, and pigmentation were observed on both legs. Clubbing fingers were not identified. His parents and sister were all normal (Figure 1D).
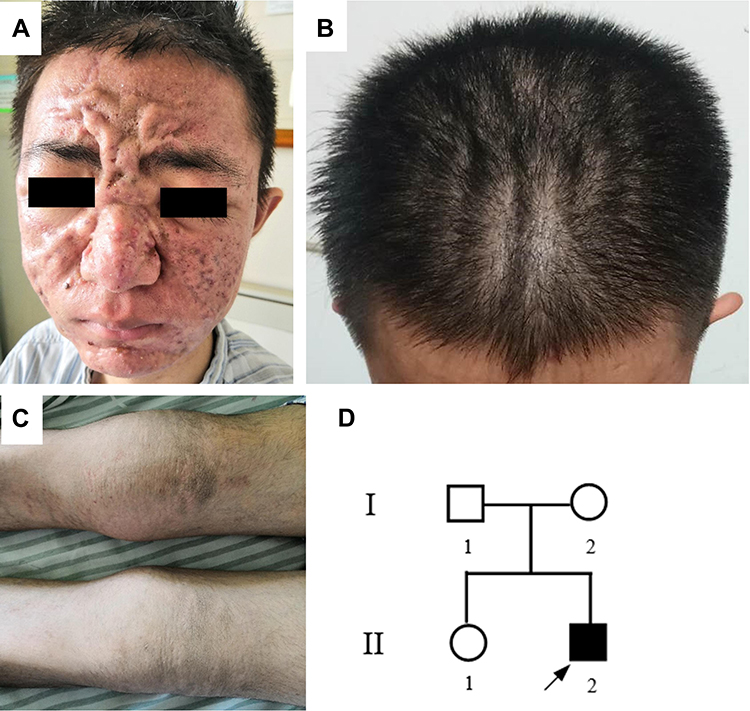 |
Figure 1 Acne conglobata (A), cutis verticis gyrata (CVG) (B), and knee arthritis (C) before treatment. (D) The pedigree gram of SAPHO family. |
Laboratory assays revealed elevated erythrocyte sedimentation rate (49 mm/h) and high-sensitivity C-reactive protein (26.40 mg/L). Rheumatoid factor, anti-streptolysin O, anti-cyclic citrullinated peptide antibody, human leukocyte antigen B27, antinuclear antibody, and parathyroid hormone were all negative. Cytochemical analysis of the synovial fluid was normal. Radiographic imaging of the lower extremities showed a low-density plaque with a sclerotic margin on the right distal tibia (Figure 2A). The magnetic resonance imaging (MRI) scans of the knee demonstrated a posterior horn tear on the medial meniscus (II°), injury on the medial collateral ligament, injury on the lateral and medial retinacula, suprapatellar bursa and joint effusion, and circumferential soft tissue edema on the right knee (Figure 2B). Whole-body bone scintigraphy revealed a diffuse, slightly increased uptake in the limb bones (Figure 2C).
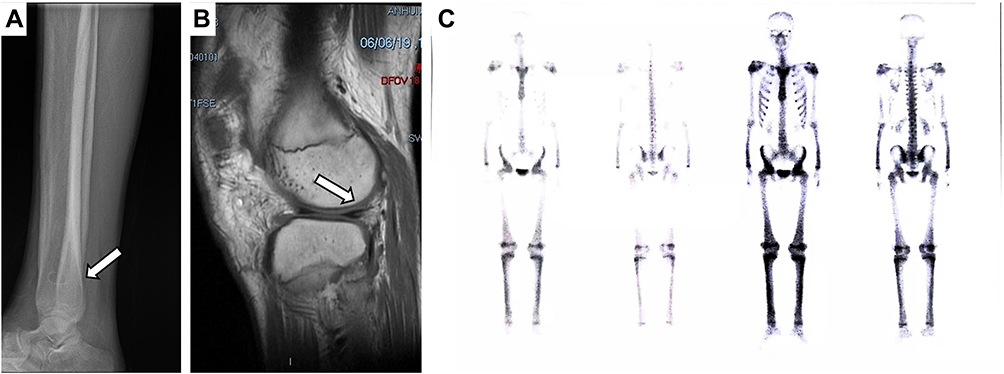 |
Figure 2 (A) Radiographic imaging showed a low-density plaque with a sclerotic margin on the right distal tibia (arrow). (B) MRI demonstrated suprapatellar bursa and joint effusion, and circumferential soft tissue edema on the right knee (arrow). (C) Whole-body bone scintigraphy revealed increased radioactivity in the limb bones. |
We did not identify any pathogenic mutation by whole-exome sequencing (WES) of this pedigree (one affected and three unaffected individuals). We also identified eight possible pathogenic genes in this pedigree, namely NCSTN, PSEN1, PSEN2, PSENEN, PSTPIP2, PSTPIP1, NLRP3, and SLCO2A1, by Sanger sequencing. No pathogenic mutation was found either.
The association of acne conglobata, osteitis, and arthritis suggested the diagnosis of SAPHO syndrome, which was in accordance with the diagnostic criteria proposed by Kahn in 2003.4 During the first 3 weeks, the patient was treated with ornidazole (50 mg, QD); azithromycin (50 mg, QD); minocycline (100 mg, QD); isotretinoin (20 mg, QD); red-blue light therapy, and boric acid wet dressing. The lesions on the face showed visible improvement, but CVG, knee swelling, and disability were not significantly relieved. Thus, a recombinant human TNF-α receptor II:IgG Fc fusion protein (rhTNFR:Fc, YISAIPU®) was administered at a dose of 25 mg twice weekly since July 2019, resulting in a gradual remission of the facial acne, knee swelling, and limited activities. Isotretinoin and rhTNFR:Fc were used until December 2020. At present, his maintenance therapy drugs are nonsteroidal anti-inflammatory drugs (NSAIDs) and glucosamine sulfate. A 2-year follow-up showed no relapse of acne and remarkable improvement of joint pain, and his CVG was also improved (Figure 3).
 |
Figure 3 Acne conglobata and knee arthritis after recombinant human TNF-α receptor II:IgG Fc fusion protein (rhTNFR:Fc) treatment: (A and F) 4 months (November 2019); (B and G) 10 months (May 2020); (C and H) 13 months (August 2020); (D and I) 21 months (April 2021). Cutis verticis gyrata (CVG) before (E) and after (J) rhTNFR:Fc treatment. |
Discussion
In our patient with SAPHO syndrome, acne had preceded the onset of knee arthritis, and it gradually worsened to acne conglobata. When conventional treatments failed to control the cutaneous and osteoarticular symptoms, our patient experienced great clinical improvement with rhTNFR:Fc administration at the 2-year follow-up. rhTNFR:Fc is an etanercept biosimilar to TNF-α antagonist and has been widely used in clinical practice in China for 15 years.8
Primary CVG usually has no known associated disorders, while secondary CVG typically has a defined cause such as inflammatory dermatoses, endocrine disorders, neoplastic diseases, or trauma. Several reports have found the links between acne and CVG,9–11 but to the best of our knowledge, the association between SAPHO syndrome and CVG has not yet been reported. We presumed that our case of SAPHO syndrome had acne conglobata, which probably led to his CVG.
To date, the precise etiopathogenesis of SAPHO syndrome remains unknown. Several studies have attempted to search for the genetic factors of SAPHO syndrome, but many of them failed to find pathogenic mutations in patients.5,12–15 Recently, an NCSTN gene mutation was identified in a patient with SAPHO syndrome and hidradenitis suppurativa,16 which provided the possible molecular linkage between SAPHO syndrome and mutations in gamma-secretase subunits. Besides, early reports found that PSTPIP2-deficient mouse models can present with SAPHO syndrome-like phenotype.17–19 In addition, pyogenic arthritis, pyoderma gangrenosum, and acne (PAPA) syndrome; pyoderma gangrenosum, acne, hidradenitis suppurativa, and spondyloarthritis (PASS) syndrome; and pachydermoperiostosis (PDP) are all rare diseases with acne and osteoarticular involvement. Therefore, the candidate genes chosen to perform Sanger sequencing were the genes of the gamma-secretase subunits (NCSTN, PSEN1, PSEN2, and PSENEN);20 PSTPIP2, PAPA-related gene (PSTPIP1);21 PASS-related gene (NLRP3);22 and PDP-related gene (SLCO2A1).23 Unfortunately, we did not identify any pathogenic mutations in this pedigree by WES or Sanger sequencing. Thus, our results reveal the genetic heterogeneity of SAPHO syndrome and the etiology of our case may be related to other factors such as immune dysfunction.
Furthermore, we searched the China National Knowledge Infrastructure (CKNI) database and reviewed Chinese publications of case reports or case series from January 1, 2016 to February 28, 2021. Our literature review found a total of 55 papers and 85 patients with SAPHO syndrome and cutaneous manifestations. There were only two patients with psoriasis pustulosa who were excluded. The remaining 83 patients were divided into three groups: 13 with acne, 59 with PPP, and 11 with more than one kind of skin lesion. Patients with acne were young and predominantly male (p<0.001), while patients with PPP were predominantly female. About 45.8% of the patients (n=38) were treated with biological therapies or traditional Chinese medicine (TCM), 84.2% (n=32) of which showed positive effects against cutaneous and osteoarticular manifestations. Further, 8.4% patients (n=7) chose TCM as their only therapy for maintenance treatment, and 85.7% (n=6) showed a significant improvement of all symptoms. Antibiotics were used mostly for patients with acne (p=0.005), while bisphosphonates were used mostly for patients with PPP (p=0.011). Patients with acne were most likely to achieve better results than other groups (p=0.028). No significant difference was observed in other variables in the three groups (Table 1).
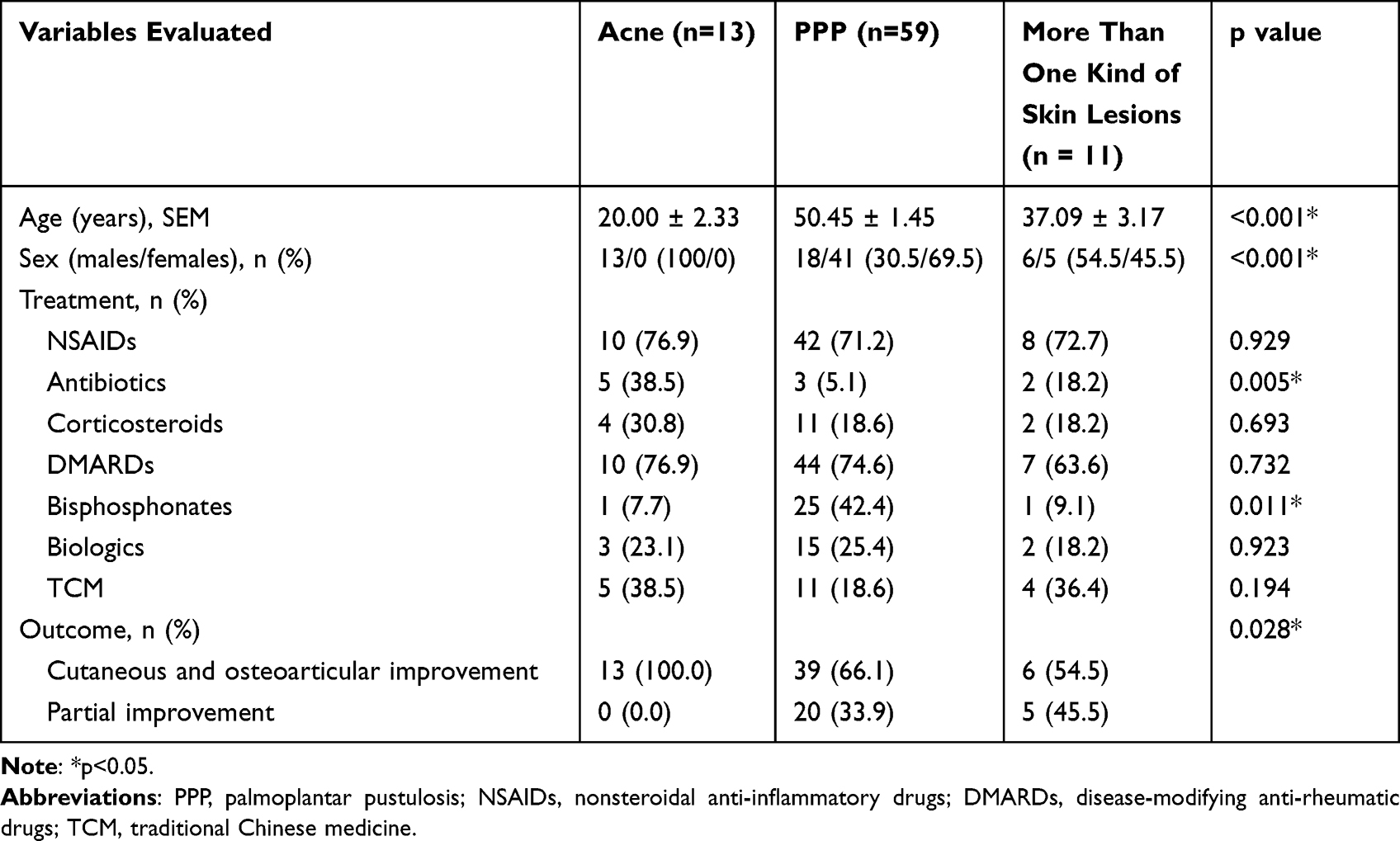 |
Table 1 Clinical and Treatment Comparison of Patients with SAPHO Syndrome and Different Cutaneous Manifestations |
Our review showed that patients with SAPHO syndrome affected by acne were young and predominantly male. This result is similar to the cohort studies conducted by Chamot and Li et al1,24 Because of the rarity of SAPHO syndrome, the treatment is challenging, and no consensus has yet been reached.25 Conventional treatments include various drugs such as NSAIDs, antibiotics, corticosteroids, disease-modifying anti-rheumatic drugs, and bisphosphonates. Moreover, the use of biologics has been proven to be a valid alternative for unresponsive cases.26 Nearly half of the cases in our review were treated with biologics or TCM, and part of them chose TCM as their only therapy, resulting in good outcome, which means that biologics and TCM might be alternative options for the treatment of SAPHO syndrome. The limitation of our study is that our review-based findings need to be confirmed in more databases.
In conclusion, we reported a case of SAPHO syndrome with CVG in a young Chinese male patient that was successfully treated with rhTNFR:Fc, and our results showed genetic heterogeneity as a cause for the disease. Biologics and TCM can be considered as alternative options for the treatment of SAPHO syndrome.
Consent
The study was approved by the Clinical Research Ethics Committee of the Anhui Medical University. Written informed consent to participate in this study was obtained from all participants. Written informed consent was obtained from all participants to have the case details and any accompanying images published. Institutional approval is not required to publish the case details.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant no. 81573065) and Natural Science Foundation of Anhui Province (grant no. 2108085MH277).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chamot AM, Benhamou CL, Kahn MF, Beraneck L, Kaplan G, Prost A. Acne-pustulosis-hyperostosis-osteitis syndrome. Results of a national survey. 85 cases. Rev Rhum Mal Osteoartic. 1987;54(3):187–196.
2. Kahn MF, Khan MA. The SAPHO syndrome. Bailliere’s Clin Rheumatol. 1994;8(2):333–362. doi:10.1016/S0950-3579(94)80022-7
3. Wang M, Li Y, Cao Y, et al. Mandibular involvement in SAPHO syndrome: a retrospective study. Orphanet J Rare Dis. 2020;15(1):312. doi:10.1186/s13023-020-01589-0
4. Gao S, Deng X, Zhang L, Song L. The comparison analysis of clinical and radiological features in SAPHO syndrome. Clin Rheumatol. 2021;40(1):349–357. doi:10.1007/s10067-020-05187-0
5. Hurtado-Nedelec M, Chollet-Martin S, Chapeton D, Hugot JP, Hayem G, Gérard B. Genetic susceptibility factors in a cohort of 38 patients with SAPHO syndrome: a study of PSTPIP2, NOD2, and LPIN2 genes. J Rheumatol. 2010;37(2):401–409. doi:10.3899/jrheum.090456
6. Rallo MS, Nosko M, Agag RL, et al. Neurosurgical and Scalp Reconstructive Challenges During Craniotomy in the Setting of Cutis Verticis Gyrata. World Neurosurg. 2019;125:392–397. doi:10.1016/j.wneu.2019.01.217
7. Zhu H, Feng ST, Zhang X, et al. Computed Tomography and Magnetic Resonance Imaging-aided Diagnosis of Primary Essential Cutis Verticis Gyrata: a Case Report with 5-year Follow-up and Review of the Literature. Curr Med Imaging Rev. 2019;15(9):906–910. doi:10.2174/1573405614666181005113448
8. Wu Q, Zhao Y, Xu D, Zhang Z, Li Z. Efficacy of methotrexate and etanercept biosimilar rhTNFR:Fc in Chinese patients with active rheumatoid arthritis: a controlled, randomized and multicenter study. Sci Rep. 2020;10(1):14270. doi:10.1038/s41598-020-64991-5
9. Ulrich J, Franke I, Gollnick H. Cutis verticis gyrata secondary to acne scleroticans capitis. J Eur Acad Dermatol Venereol. 2004;18(4):499–502. doi:10.1111/j.1468-3083.2004.00961.x
10. Jain K, Jain VK, Aggarwal K, Bansal A. Late onset isotretinoin resistant acne conglobata in a patient with acromegaly. IndJ Dermatol Venereol and Leprol. 2008;74(2):139–141. doi:10.4103/0378-6323.39699
11. Xu Y, Zhang Z, Yue H, Li S, Zhang Z. Monoallelic mutations in SLCO2A1 cause autosomal dominant primary hypertrophic osteoarthropathy. J Bone Mineral Res. 2021;36(8):1459–1468. doi:10.1002/jbmr.4310
12. Ferguson PJ, Lokuta MA, El-Shanti HI, Muhle L, Bing X, Huttenlocher A. Neutrophil dysfunction in a family with a SAPHO syndrome-like phenotype. Arthritis Rheumatism. 2008;58(10):3264–3269. doi:10.1002/art.23942
13. Colina M, Pippucci T, Moro MA, et al. Synovitis, acne, pustulosis, hyperostosis, osteitis (SAPHO) syndrome: is PTPN22 involved? Clin Exper Rheumatol. 2012;30(3):451.
14. Assmann G, Köhm M, Schuster V, et al. Genetic variants in FBLIM1 gene do not contribute to SAPHO syndrome and chronic recurrent multifocal osteomyelitis in typical patient groups. BMC Med Genetics. 2020;21(1):102. doi:10.1186/s12881-020-01037-7
15. Queiro R, Moreno P, Sarasqueta C, Alperi M, Riestra JL, Ballina J. Synovitis-acne-pustulosis-hyperostosis-osteitis syndrome and psoriatic arthritis exhibit a different immunogenetic profile. Clin Exper Rheumatol. 2008;26(1):125–128.
16. Li C, Xu H, Wang B. Is SAPHO Syndrome Linked to PASH Syndrome and Hidradenitis Suppurativa by Nicastrin Mutation? A Case Report. J Rheumatol. 2018;45(11):1605–1607. doi:10.3899/jrheum.171007
17. Liao HJ, Chyuan IT, Wu CS, et al. Increased neutrophil infiltration, IL-1 production and a SAPHO syndrome-like phenotype in PSTPIP2-deficient mice. Rheumatol. 2015;54(7):1317–1326. doi:10.1093/rheumatology/keu481
18. Ferguson PJ, Laxer RM. New discoveries in CRMO: IL-1β, the neutrophil, and the microbiome implicated in disease pathogenesis in Pstpip2-deficient mice. Sem Immunopathol. 2015;37(4):407–412. doi:10.1007/s00281-015-0488-2
19. Ferguson PJ, Bing X, Vasef MA, et al. A missense mutation in pstpip2 is associated with the murine autoinflammatory disorder chronic multifocal osteomyelitis. Bone. 2006;38(1):41–47. doi:10.1016/j.bone.2005.07.009
20. Bergmans BA, De Strooper B. gamma-secretases: from cell biology to therapeutic strategies. Lancet Neurol. 2010;9(2):215–226. doi:10.1016/S1474-4422(09)70332-1
21. Genovese G, Moltrasio C, Garcovich S, Marzano AV. PAPA spectrum disorders. Giornale italiano di dermatologia e venereologia. 2020;155(5):542–550. doi:10.23736/S0392-0488.20.06629-8
22. Schwob E, Bessis D, Boursier G, et al. PASS: a rare syndrome within the autoinflammatory diseases that still lacks a genetic marker. J Eur Acad Dermatol Venereol. 2020;34(9):e478–e480. doi:10.1111/jdv.16385
23. Seta V, Capri Y, Battistella M, Bagot M, Bourrat E. Pachydermoperiostosis: the value of molecular diagnosis. Ann Dermatol Venereol. 2017;144(12):799–803. doi:10.1016/j.annder.2017.03.027
24. Li Y, Li C, Wu N, et al. Demographic, clinical, and scintigraphic comparison of patients affected by palmoplantar pustulosis and severe acne: a retrospective study. Clin Rheumatol. 2020;39(6):1989–1996. doi:10.1007/s10067-019-04904-8
25. Liu S, Tang M, Cao Y, Li C. Synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome: review and update. Therap Adv Musculoskeletal Dis. 2020;12:1759720x20912865.
26. Figueiredo ASB, Oliveira AL, Caetano A, Moraes-Fontes MF. SAPHO: has the time come for tailored therapy? Clin Rheumatol. 2020;39(1):177–187. doi:10.1007/s10067-019-04675-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Disseminated Combined Talaromyces marneffei and Enterococcus faecium Bloodstream Infection Presenting as Gastrointestinal Perforation in a Patient with CARD9 Gene Mutation
Liang H, Duan X, Li T, Hu L, Guo J
Infection and Drug Resistance 2024, 17:4783-4790
Published Date: 31 October 2024