Back to Journals » Journal of Pain Research » Volume 14
Direct and Indirect Relationships Between Physical Activity, Fitness Level, Kinesiophobia, and Health-Related Quality of Life in Patients with Rheumatic and Musculoskeletal Diseases: A Network Analysis
Authors Courbalay A ![]() , Jobard R, Descarreaux M, Bouvard B
, Jobard R, Descarreaux M, Bouvard B
Received 15 June 2021
Accepted for publication 1 October 2021
Published 28 October 2021 Volume 2021:14 Pages 3387—3399
DOI https://doi.org/10.2147/JPR.S323424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Anne Courbalay,1 Romane Jobard,1 Martin Descarreaux,2 Béatrice Bouvard3,4
1Institut de Formation en Education Physique et en Sport d’Angers (IFEPSA-UCO), APCoSS, Les Ponts de Cé, France; 2Department of Human Kinetics, Université du Québec à Trois-Rivières Québec, Trois-Rivières, Canada; 3Univ Angers, GEROM, SFR ICAT, Angers, France; 4CHU Angers, Service de Rhumatologie, Angers, France
Correspondence: Anne Courbalay
Institut de Formation en Education Physique et en Sport d’Angers (IFEPSA-UCO), APCoSS, 49 rue des Perrins - BP 40071, Les Ponts de Cé, 49136, France
Tel +33 2 41 45 26 40
Fax +33 2 41 45 26 44
Email [email protected]
Introduction: Using a network analysis, the present study investigated the extent to which physical activity (PA), objective fitness level, kinesiophobia, and health-related quality of life (HRQoL) interact in patients with rheumatic and musculoskeletal diseases. The objectives were twofold: 1) to clarify the direct and indirect relationships between these variables while controlling for the shared variance between them, and 2) to establish a potential ranking of influence among them.
Methods: This cross-sectional design study involved patients recruited from a rheumatology unit. One hundred and twenty patients completed self-reported measures of PA, the Tampa scale of kinesiophobia and the 36-item Short-Form Health Survey, and ninety-seven of those patients performed the six-minute walking test and the thirty-second sit-to-stand test. Network analyses were conducted using bootnet and qgraph packages.
Results: Weekly time spent on PA, as well as physical fitness measures, were directly linked to kinesiophobia and the HRQoL physical dimension, but indirectly linked to HRQoL mental dimension through the mediation of kinesiophobia. Specifically, weekly PA time had direct relationships to physical functioning, vitality, and role limitations due to physical and emotional problems. Fitness measures had direct relationships with physical functioning, bodily pain, and mental health. The analyses did not clearly highlight one variable as the most influential in the network.
Discussion: The study highlights the complexities of direct and indirect biopsychosocial relationships that are at the core of patients’ daily functioning. Measurement of PA, use of a longitudinal design, and interventions are discussed.
Keywords: rheumatic and musculoskeletal diseases, health-related quality of life, physical activity, fitness level, kinesiophobia
Introduction
Rheumatic and musculoskeletal diseases (RMDs), which are recognized as one of the highest global burdens on individuals and social-care systems worldwide,1 include more than 200 commonly progressive diseases affecting joints, tendons, ligaments, bones, muscles and internal organs.2 Low back pain, neck pain, osteoarthritis, rheumatoid arthritis, and gout are the most prevalent RMDs.1 RMDs can be caused by problems of the immune system, inflammation, infections, or gradual deterioration of joints, muscles, and bones.2
These long-term and degenerative conditions are characterized by a broad range of symptoms and signs, among which persistent pain and a decrease in the range of motion potentially leading to a progressive functional disability.2 The progressive nature of these symptoms have a negative influence on individuals’ health-related quality of life (HRQoL), commonly defined as the way a person functions in their life and perceives their wellbeing in the physical, mental, and social domains of health.3 Spinal pain has been identified as the leading cause of the number of years lived with disabilities worldwide, closely followed by neck pain and musculoskeletal disorders, which are also in the top ten ranking causes of disability.1 Moreover, individuals with inflammatory rheumatic diseases, systemic connective tissue disorders, symptomatic peripheral osteoarthritis, soft tissue disorders, and osteoporosis have lower scores on HRQoL dimensions (usually studied with physical and mental summaries) as well as on HRQoL-specific sub-dimensions, namely physical functioning, role limitations due to physical function, bodily pain, general health perceptions, mental health, vitality, role limitations due to emotional health, and social functioning.4
Physical activity (PA), which includes exercise, sports and physical activities done as part of daily living, occupation, leisure and active transportation5 is highly recommended for individuals with RMDs6 considering its positive effects on HRQoL.7 Regarding the physical domain, PA is believed to limit inflammation, joint damage, pain-related symptoms, fatigue, and improve cardiovascular fitness, muscular strength and joint range of motion.6,8–11 Moreover, PA reduces psychological distress,12 depressive symptoms13 and anxiety14 in individuals with RMDs. Studies report that individuals with RMDs are less active and have more sedentary behaviors than individuals without RMDs, despite a high level of heterogeneity among participants.14,15 Among the physical, psychological, and socio-environmental auto-reported barriers to PA practice in individuals with RMDs (eg, sociodemographic factors, lack of time, fatigue, and social support), pain experiences is one of the most significant barriers reported by patients.16,17 Given the negative impact of pain experienced in PA practice, examining the way individuals with RMDs deal with their pain experience is worthy of interest when examining the relationship linking PA with HRQoL broad- and sub-dimensions.
Kinesiophobia, which is defined as an excessive, irrational, and debilitating fear of physical movement and activity,18 is negatively associated with pain intensity and disability in individuals with RMDs.19 A recent systematic review found a negative association between kinesiophobia and HRQoL with an overall moderate quality of evidence.19 Negative associations have also been highlighted between fear-avoidance beliefs (including PA-related beliefs) and the physical and psychological broad domains of HRQoL in patients with RMDs.20,21 Furthermore, negative associations have been described between kinesiophobia and self-reported PA or attitudes toward PA practice in individuals with chronic low back pain or knee osteoarthritis.16,22–24 When looking at objective measures related to PA, monitored by accelerometers or performed during fitness tests, instead of self-reported measures, the association with kinesiophobia is no longer significant.22,25 Such findings suggest that although self-reported physical function provides information about one’s pain-related beliefs, the use of objective measures offers additional information about physical capacity or ambulatory activity.
To date, and to our knowledge, no previous study has examined the relationships between kinesiophobia, self-reported measures of PA practice, objective fitness measures, and HRQoL using a systemic approach. By extension, no one has yet investigated a potential ranking of importance among these variables. Yet, considering that pain-related experience encompass multiple factors26 that exert reciprocal influences on each other, integrative approaches appear necessary when investigating the interrelated relationships between PA, psychological pain-related variables, and HRQoL in patients with RMDs. A network analysis approach can be used to map out a complex interplay of components such as psychological ones.27 During the last decade, this approach has been used in the fields of mental disorders,28 personality,29 affective regulation,30 but also in health,31 including pain.32 A partial correlation network makes it possible to visualize and analyze the global structure of a large number of interacting variables, but also to identify the most (and least) influential variable(s) in the network, while controlling for the variance shared between the studied variables. Metrics (called centrality measures) allow us to characterize the influence of each studied variable in terms of strength, closeness and betweenness. The measure of strength quantifies the extent to which a node is directly connected to other nodes, while closeness, quantifies the indirect connections between a node to other ones.33 Finally, betweenness quantifies the importance of a node in the average path between two other nodes.33 Using a partial correlation network analysis approach, the way pain intensity and psychological pain-related variables (ie, anxiety and depression symptoms, fear avoidance beliefs, pain self-efficacy, perceived disability, and perceived control) co-interact in patients with chronic pain syndromes has recently been examined.32 Analyses not only revealed direct and indirect relationships between the studied variables, but also highlighted a ranking of importance among them, with pain self-efficacy and perceived disability having the highest strength values, whereas pain intensity had the lowest one.32 As a whole, pain-related psychological variables were more directly connected to each other than to pain intensity. The structure of HRQoL measured by the 36-item Short Form Health Survey (SF-36) in individuals with and without cancer has also been investigated using a network approach.31 Beyond the expected respective relationships within the physical (eg, general health and physical functioning) and the psychological subdomains of HRQoL (eg, mental health and vitality), the authors also identified positive direct relationships between subdomains belonging more specifically to the physical and to the psychological dimensions (eg, between physical functioning and mental health), highlighting the value of examining direct and indirect relationships between PA practice, fitness measures, kinesiophobia and main or subdomains of HRQoL within the same analysis. In individuals with cancer, general health and physical functioning were found to have the highest closeness values, indicating that changes on these two variables influence the largest number of variables in the network. Conversely, bodily pain and social functioning had the lowest values for closeness, suggesting that changes in these two variables would not predict changes in other nodes and vice-versa. When investigating how self-reported PA practice, objective fitness levels, kinesiophobia, and HRQoL domains and subdomains co-interact in patients with RMDs, using a network approach could provide new insights by 1) clarifying the direct and indirect relationships between these variables, and 2) identifying centrality metrics between these interrelated variables.
This study therefore aims at addressing these two issues. The first objective was to investigate the extent to which self-reported PA practice, objective fitness levels, kinesiophobia, and HRQoL domains and subdomains interact in patients with RMDs. The second objective was to examine a potential ranking of importance among these variables. It was hypothesized that self-reported PA practice and fitness level would have more proximal relationships with kinesiophobia and HRQoL physical-related domain(s) than with the HRQoL mental-related domain(s). The relationships between self-reported PA practice, fitness level and HRQoL were expected to be positive but dependent on the level of kinesiophobia. It was finally hypothesized that bodily pain, physical functioning, and role limitations due to physical problems, which belong to the physical-related subdomains of HRQoL, would be the primary variables of the studied networks.
Materials and Methods
Participants and Procedures
Participants were eligible for inclusion in the study if they had a diagnosed RMD and were under care at a rheumatology unit at the time of the study. They also had to speak and understand French fluently. Women were excluded if they were pregnant or breastfeeding. The study protocol was systematically introduced to patients by one of the study investigators who remained available if necessary. The protocol included questionnaires, two fitness tests, as well as a short semi-structured interview (see Outcome Measures for details). Outpatients were asked to complete the protocol during one of their medical appointments, while inpatients could participate when free of clinical examinations. The protocol received approval from a French Rheumatology unit providing clinical care for numerous degenerative and inflammatory musculoskeletal disorders at Angers’ University Hospital Center. Such protocol includes questionnaires and tests that were part of the clinical routine led by rheumatologists. Since participants were not out of their care plan, no Institutional Review Board were asked for approval. Participants provided written informed consent after being assured that all data would be treated anonymously. All procedures performed in the study were in accordance with the 1964 Helsinki declaration and its later amendments.
Outcome Measures
Demographics
Current age, sex, height, weight, professional status, and information about RMDs (ie, type of pathology, years since diagnosis) were collected from the intake assessment form.
Kinesiophobia
The French version of the Tampa Scale of Kinesiophobia34 was used to measure subjective fear of movement/(re)-injury through 17 items (eg, “I am afraid that I might injure myself if I exercise”). Participants were asked to indicate the degree to which they agreed or disagreed with each item on a scale ranging from 1 (strongly disagree) to 4 (strongly agree). Items were summed to obtain a total score, possibly ranging from 17 to 68. A score equal to or greater than 40 is considered clinically relevant. Cronbach’s alpha was acceptable: α = 0.72.
Health-Related Quality of Life
The French validation of the Medical Outcome Study Short-Form 36 item health survey (SF-36),35 which is a generic measure designed to assess health status in various conditions including RMDs,4 was used to assess HRQoL. The SF-36 comprises eight domains: physical functioning (PF; ie, feeling able to do common daily tasks and activity such as walking, carrying loads, bending, practicing PA), role limitations due to physical health problems (RP; ie, loss of efficacy and accomplishment at work or in daily tasks due to physical health problems), bodily pain (BP; ie, pain intensity and frequency), general health (GH; ie, health perception), vitality (VT; ie, feeling of energy or fatigue), social functioning (SF; ie, social participation or restriction due to health condition), role limitations due to emotional problems (RE; ie, loss of efficiency and accomplishment at work or in daily tasks due to emotional problems) and general mental health (MH; ie, positive and negative emotion). Raw scores were converted to respective 0–100 scales, with higher scores indicating better health. A physical dimension (ie, Physical Component Summary (PCS)) and a mental dimension (ie, Mental Component Summary (MCS)) were respectively calculated by a proper weighting of the eight subscales, with a larger weighting of PF, RP, BP, and GH for PCS and a larger weighting of VT, SF, RE and MH for MCS. The SF-36 also comprises an additional item named health transition (HT), corresponding to the difference between the current perceived health status in comparison with one last year. This item was not included in the analyses because it did not seem relevant to examine the relationship between patients’ current PA practice, which is time dependent, and a global perception of health status from about one year ago. Cronbach’s alphas were good for PF, RP, BP, and RE: 0.90> α ≥ 0.80, and acceptable for GH, VT, SF: 0.80> α ≥ 0.78. MH’s alpha was only acceptable when item 9d was dropped, αexcluding9d = 0.73, αincluding9d = 0.28. Following the missing value procedure, item 9d was suppressed from the analysis and its score was substituted by the mean score of the remaining items. In these conditions, Cronbach’s alpha became good (α = 0.85).
Self-Reported Physical Activity
The Saltin-Grimby physical activity scale36 was used to categorize participants according to their level of weekly PA practice. Participants were asked to indicate among four items describing sedentary behaviors, light, moderate and vigorous activities, the one that corresponded the best to their weekly PA routine. Validity of this categorical measure is supported in the field of health research.37 In addition, participants were also asked to report the weekly time spent on active transportation, supervised and unsupervised light to vigorous physical activity or sport. A total weekly PA practice score summing the time spent for all these practices was calculated in minutes per week. Barriers to PA practice were also assessed during a 4-question semi-structured interview targeting one’s pain experience, motivation toward physical activity, accessibility and financial cost.
Objective Fitness Level
Two relevant fitness tests for individuals with RMDs were selected.38 The six-minute walking test was used to assess functional performance (FP) at a submaximal level. Participants had to walk the longer distance possible going back and forth in a quiet hallway that met the following prerequisites: hard, flat, and indoor. The distance each participant was able to walk in 6 minutes was recorded by the experimenter. Standardized verbal encouragement were provided at minute intervals, and rest was allowed. The 30-second sit-to-stand test (30STS) was used to assess participants’ muscular strength (MS) in legs. Participants were asked to sit and stand as quickly and safely as possible in 30 seconds. The total number of completed chair stands within 30 seconds was recorded.
Data Analysis
Descriptive statistics and Pearson correlations were first performed between the studied variables. Then, network analyses were performed on R, using bootnet and qgraph packages.27,33 In the present study, the estimated partial correlation network was computed using the Extended Bayesian Information Criterion Graphical Least Absolute Shrinkage and Selection Operator (ie, EBICglasso), which is a regularized estimation method. This method efficiently estimates parsimonious and interpretable network structure in psychological data, avoids spurious correlations, and handles relatively small datasets.27 The network model used was a Gaussian graphical model, in which nodes represent variables (ie, for the present study, self-reported PA, functional performance, muscular strength, kinesiophobia, and HRQoL scores) and edges indicate nonzero partial correlation coefficients between two nodes while controlling for the shared variance between all other nodes in the network. Regularized partial correlations were computed and depicted in an edge weighted structure in which the sign of the edge weight (ie, positive or negative) indicates the nature of the relation, and the absolute value of the edge weight indicates the strength of the effect. Regularized partial correlations range from −1 to 1, with a coefficient of zero, indicating that two variables are independent after controlling for all other variables in the network.
The respective importance of nodes was assessed using three indices of centrality: strength (called degree in unweighted networks), which “quantifies the sum of absolute partial correlation coefficients between a node and all other nodes”;33 closeness, which “measures how strongly a node is indirectly connected to other nodes in the network”;33 and betweenness, which “is related to how often a node is in the shortest paths between other nodes”.33 The stability of centrality indices as well as edge weights and nodes’ significant differences were estimated using bootstrap analyses.27 To examine the stability of centrality metrics, a case-dropping subset bootstrap was used to investigate the extent through which the order of indices remained the same after re-estimating the network with only a subset of the data. To do so, we relied on the correlation stability coefficient (ie, the CS-coefficient) representing the proportion of participants that can be dropped from the original sample while maintaining a correlation of 0.70 or above for centrality metrics between the full and subset sample. According to the recommendations, the CS-coefficient should not be below 0.25, and preferably above 0.5 to ensure sufficient stability of the centrality metrics.27 Respective edge weights and nodes differences were examined with nonparametric bootstrapped difference tests.
Psychological networks estimated on cross-sectional data are computed as undirected networks, indicating mutual relationships between the nodes instead of a causal structure.33 Thus, no statement can be done about the direction of the effect.
Results
Sample Characteristics
One hundred and twenty patients were recruited for the present study (49 men, 71 women; mean age = 56.21 years; standard deviation [SD] = 13.64; number of years lived since diagnosis = 10.23, SD = 10.02; BMI = 27.74, SD = 6.09), including 68 outpatients and 52 patients hospitalized for one week. RMDs varied among participants: 65% (N = 78) were diagnosed with chronic inflammatory rheumatism (ie, rheumatoid polyarthritis, ankylosing spondylitis, and gout), 28.3% (N = 34) diagnosed with spinal disorder (ie, non-specific chronic low back pain, herniated disc, sciatica), 5.8% (N = 7) diagnosed with osteoporosis and 0.8% (N = 1) diagnosed with fibromyalgia. Regarding their professional status, 31.6% (N = 38) of participants were employed, 6.7% (N = 8) were unemployed, 20% (N = 24) were on medical leave, and 41.7% (N = 50) were retired. Among the 120 patients who agreed to participate in the study, 23 did not perform the fitness tests.
Preliminary Analyses
Results revealed that 41.7% (N = 50) of the participants were sedentary, 47.5% (N = 57) had a light PA practice, 9.2% (N = 11) had a moderate PA practice, and 1.7% (N = 2) had a vigorous PA practice. Among the reported barriers to PA practice, pain was mentioned by 93.3% (N = 112) of the participants, lack of motivation in 27.5% (N = 33), accessibility problems in 14% (N = 17), and cost were mentioned by 1.7% (N = 2).
Descriptive statistics revealed heterogeneity in the weekly time in PA practice (M = 189.42, SD = 154.82), as well as during the six-minute walking test (M = 330.40, SD = 95.20) and the 30-second sit-to-stand test (M = 8.25, SD = 4.02). The mean kinesiophobia score was greater than 40 (M = 41.35, SD = 7.16), and thus clinically relevant.
Correlation analyses showed negative relationships between kinesiophobia and the weekly time spent doing PA (r = −0.37, p < 0.001), functional performance (r = −0.41, p < 0.001), and muscular strength (r = −0.25, p < 0.001). The weekly time spent doing PA practice, as well as both fitness measures were all positively correlated with the physical component summary (0.46 <r < 0.62, p < 0.001), and with all HRQoL subdomains excepting mental health (0.21 <r < 0.45, 0.05 <p < 0.001). These three variables were not significantly correlated with the mental component summary (p > 0.05). Kinesiophobia was negatively correlated with each HRQoL domain, with small to large effect sizes (−.27 <r <-.45, 0.05 <p <0.001). The correlation between the weekly time spent doing PA practice and social functioning was close to significance (p = 0.06). Except for general health perceptions and role limitations due to emotional problems (p < 0.05), all HRQoL domains were positively correlated among each other, with small to large effect sizes (0.21 <r < 0.60, 0.05 < p < 0.001). Because the number of years since diagnosis was not significantly correlated with the weekly time spent doing PA practice, functional performance, muscle strength, or with kinesiophobia (all p> 0.05), this variable was not included in the network analyses. The descriptive statistics of the studied variables are presented in Table 1 while the Pearson correlations between them are presented in Table 2.
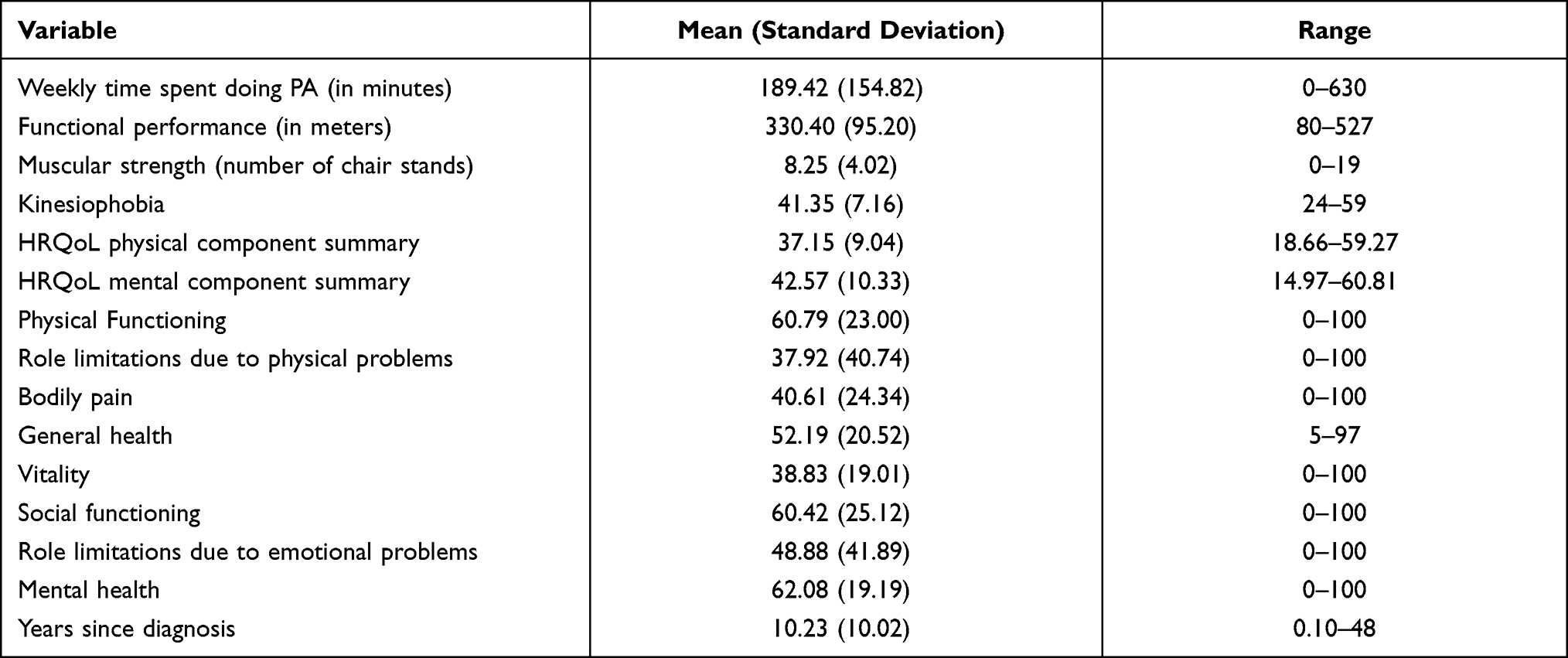 |
Table 1 Participants’ Characteristics Among the Studied Variables |
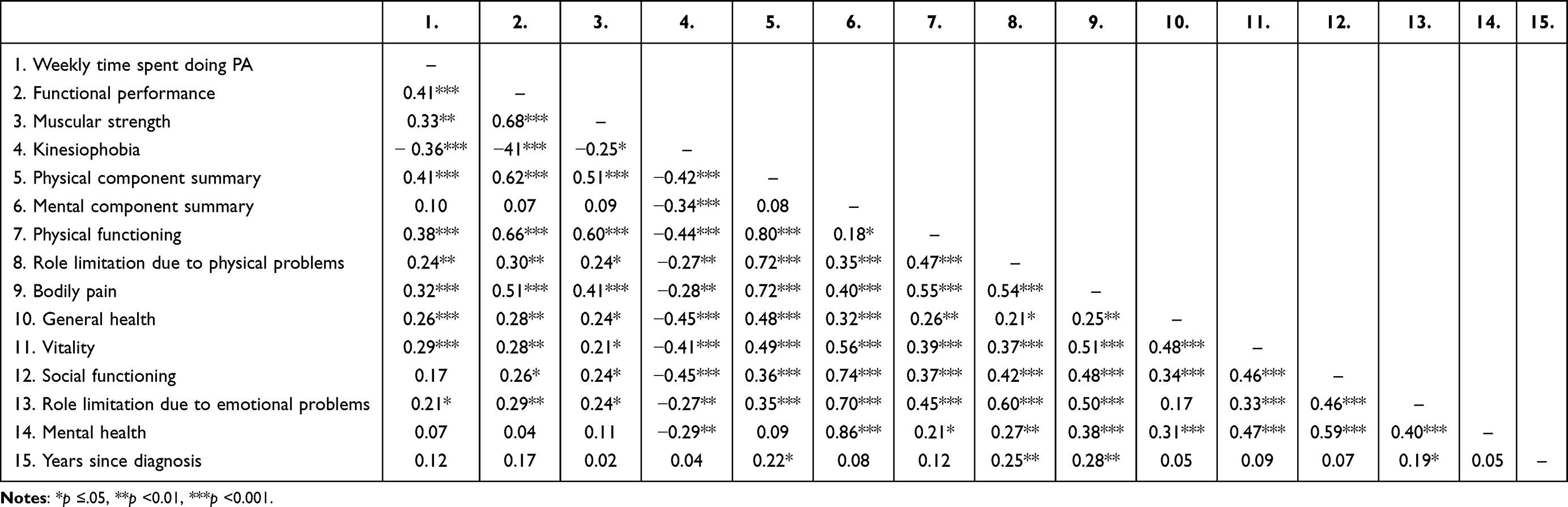 |
Table 2 Matrix of Pearson Correlations Between the Studied Variables |
Network Analyses
Network Analysis Including HRQOL Broad Domains
Results from the network analysis showed that all nodes are interrelated. Figure 1 shows the modelled network, including partial correlation coefficients. All regularized partial correlation coefficients between all nodes are presented in Table 3. When controlling for other variables in the model, analyses revealed that the physical component summary had direct positive connections with the weekly time spent doing PA practice, functional performance and muscular strength, and a negative one with kinesiophobia. Although the weekly time spent doing PA had a direct connection with results from the functional performance, it was indirectly connected with muscular strength. All physical-related variables had an indirect connection with the mental component summary through the mediation of kinesiophobia. Network analyses highlighted proximal relationships between the physical component summary, the weekly time spent doing PA practice, functional performance and muscular strength, and distal relationships with kinesiophobia.
 |
Table 3 Weights Matrix of the First Network Analysis |
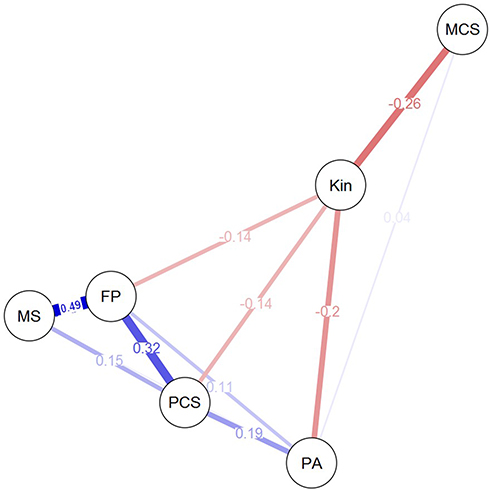 |
Figure 1 Modelled network of the studied variables. Blue lines (edges) between the studied variables (nodes) represent positive partial correlations, whereas red edges represent negative partial correlations. The size and color density of the edges vary to reflect the strength of the partial correlations, with thicker and deeper blue/red-colored edges representing the stronger partial correlation coefficients. Partial correlation coefficients are indicated on their respective edge. Variables which are not graphically connected among each other are not significantly connected when controlling for other variables in the model. Abbreviations: MCS, mental component summary; Kin, kinesiophobia; PA, weekly time spent doing PA; FP, functional performance; PCS, physical component summary; MS, muscular strength. |
Results from the bootstrapped difference tests between edge weights are presented in Figure 2A. The edges respectively linking the physical component summary, with the weekly time spent doing PA, functional performance, and muscular strength did not differ significantly from each another, highlighting similar weights between them. The edge between muscular strength and functional performance was significantly stronger than those linking muscular strength with the weekly time spent doing PA and the physical component summary. In addition, the edge connecting kinesiophobia with the mental component summary was not significantly stronger than all the other edges linked with kinesiophobia, indicating that kinesiophobia is similarly associated with the mental- and physical-related components. Moreover, the edge linking kinesiophobia with the physical component summary was significantly lower than those linking the physical component summary with the weekly time spent doing PA and functional performance.
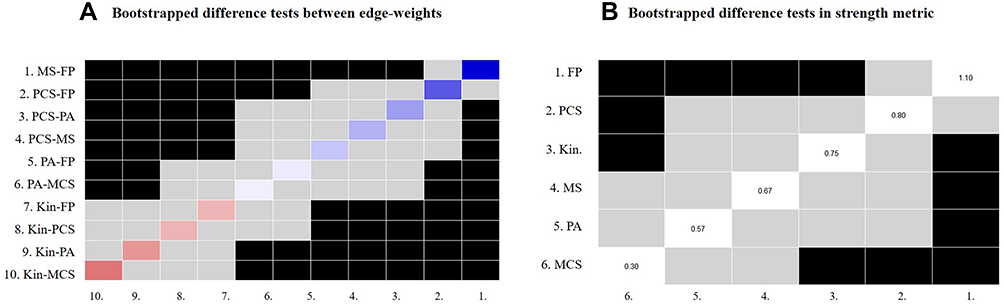 |
Figure 2 Results of the bootstrapped difference tests (α = 0.05) between edge weights that were nonzero in the estimated network (A) and between nodes in terms of strength metric (B). In (A), edge weights are presented in abscissa and ordinate axes. Black boxes represent edge weights (partial coefficient correlations) that significantly differ from one another while gray boxes indicate edge weights (partial coefficient correlations) that do not significantly differ. Red to blue colored boxes correspond to the color of the edge in Figure 1, with red boxes highlighting negative partial coefficient correlations and blue boxes positive partial coefficient correlations. In (B), nodes’ related strength are presented in abscissa and ordinate axes. Black boxes represent nodes that significantly differ from one another in terms of direct connections with the other nodes while gray boxes indicate non-significant differences. For each node, its strength value is indicated in the white box. Abbreviations: MCS, mental component summary; Kin, kinesiophobia; PA, weekly time spent doing PA; FP, functional performance; PCS, physical component summary; MS, muscular strength. |
Finally, centrality-related analyses revealed that the strength metric was stable under subsetting cases (CS (cor = 0.7) = 0.44), but that metrics of closeness (CS (cor = 0.7) = 0.21) and betweenness (CS (cor =0.7) = 0.12) were not. Therefore, significant nodes’ differences were only examined in terms of strength. Analyses revealed that functional performance shares the most numerous direct connections compared to the other nodes, while the mental component summary shares the less numerous ones. Results from the bootstrapped difference tests in strength metrics are presented in Figure 2B.
Network Analysis Including HRQOL Subdomains
Figure 3 shows the second network analysis, including partial correlation coefficients. All partial correlation coefficients are presented in Table 4. Results from the second network analysis showed that the weekly time spent doing PA, functional performance, muscular strength, kinesiophobia, and all HRQoL subdomains were all interrelated. Controlling for other variables in the model, all HRQoL subdomains were directly or indirectly associated with each other in such a way that the higher or lower the scores were in one subdomain, the higher or lower they were in the other subdomains. The weekly time spent doing PA shared edges with physical functioning, role limitations due to emotional and physical health problems, vitality and general health perceptions, but did not share edges with mental health or with bodily pain. Functional performance was directly connected with physical functioning and bodily pain, while muscular strength was only connected with physical functioning. The weekly time spent doing PA was distally linked with any HRQoL subdimensions, contrary to functional performance and muscular strength.
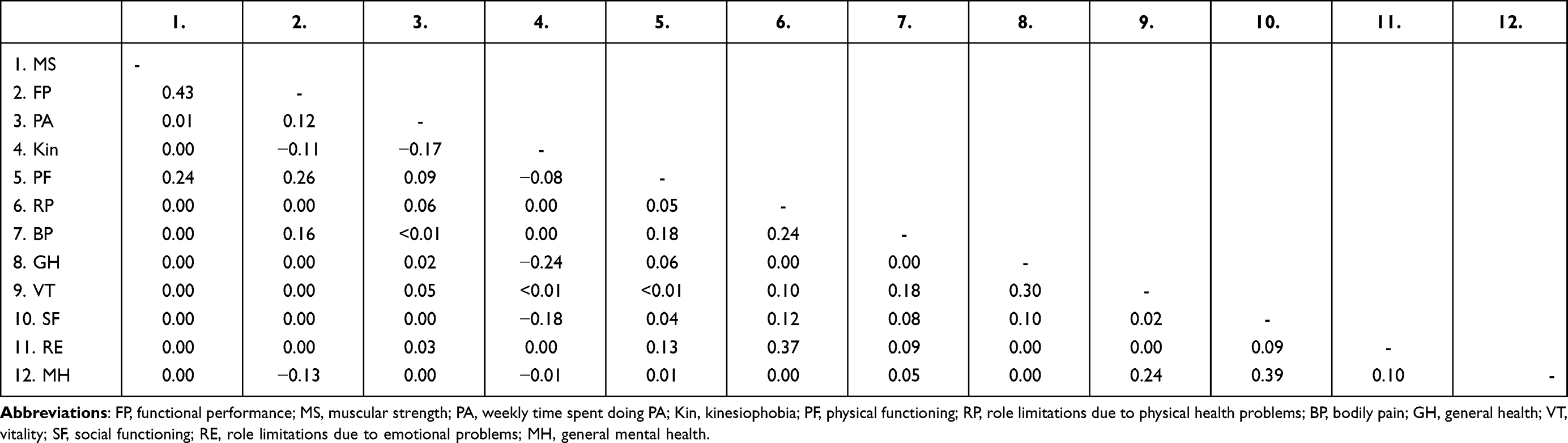 |
Table 4 Weights Matrix of the Second Network Analysis |
 |
Figure 3 Modelled network of the studied variables. Blue lines (edges) between variables (nodes) in the network represent positive partial correlations, whereas red edges represent negative partial correlations. The size and color density of the edges vary to reflect the strength of the partial correlations, with thicker and deeper blue/red-colored edges representing the stronger partial correlation coefficients. Partial correlation coefficients are indicated on their respective edge. Variables which are not graphically connected among each other are not significantly connected when controlling for other variables in the model. Abbreviations: PA, weekly time spent doing PA; FP, functional performance; MS, muscular strength; Kin, kinesiophobia; PF, physical functioning; RP, role limitations due to physical health problems; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, role limitations due to emotional problems; MH, general mental health. |
Furthermore, analyses showed that kinesiophobia was directly and negatively connected with physical functioning, social functioning and general health, acting as a partial mediator between these HRQoL subdomains and functional performance on the one hand, and the weekly time spent doing PA on the other hand. Finally, kinesiophobia did not share any edge with bodily pain, vitality, nor with role limitations due to physical and mental problems, while sharing an edge with mental health.
Due to the large number of nonzero edges in the second network, we only focused on direct and indirect relationships between the nodes of importance, and did not compare their weights.
Analyses of the CS-coefficients showed that centrality metrics did not reach the cutoff of 0.25 (all CS (cor = 0.7) <0.21). Therefore, no conclusions were drawn about importance ranking of nodes in terms of strength, betweenness and closeness metrics.
Discussion
Using a network approach, the current study is the first to examine and model the extent to which weekly time spent doing PA practice, objective fitness levels, kinesiophobia, and HRQoL are interrelated in patients with RMDs. We expected positive relationships between the time spent doing PA, objective fitness levels, and HRQoL, primarily with the major domains and subdomains of HRQoL related to physical activity, but also that these relationships would be conditioned by the level of kinesiophobia. Furthermore, it was hypothesized that bodily pain, physical functioning, and role limitations due to physical problems would be the most central variables of the networks studied.
The first hypothesis was supported by the results, as the weekly time spent doing PA and objective fitness level had strong associations with the HRQoL physical component summary, which were mainly driven by strong positive links with physical functioning. As expected, these results are in line with previous studies showing positive relationships between time spent doing PA, objective fitness levels and physical components of HRQoL such as functional capacity, general health, and fatigue.6–8 Interestingly, the results showed that levels of pain experienced within one month were directly connected to functional performance and physical functioning, but only indirectly connected with the weekly time spent doing PA practice and muscular strength. Although no causal relationship can be established, this suggests that the time dedicated to PA and muscular strength are not sufficiently informative to account for bodily pain, but that their positive effects on abilities such as being able to walk, carry loads, bend forward, and engage in efforts of different intensities promote pain management.
Moreover, although the weekly time spent doing PA practice was only indirectly related to HRQoL mental component summary, it showed a direct positive association with vitality, supporting reciprocal interactions between PA practice and the subsequent feeling of vitality,39 as well as the influence of vitality on PA.40
Furthermore, by highlighting that kinesiophobia shares negative relationships with HRQoL physical and mental main and sub-dimensions, the results are consistent with previous findings,20 but also extend them by clarifying the subdomains which are proximally and distally linked to kinesiophobia. Although kinesiophobia has previously been associated with physical functioning, disability and depression,20 the present results show that kinesiophobia is also associated with social functioning, suggesting that the more kinesiophobia a person has, the more his/her social life is restricted. Combined with depression and anxiety,20,32 fear-avoidance beliefs such as the levels of kinesiophobia might partly explain why individuals with RMDs have lower social functioning than individuals without RMDs.4 These results, however, contrast with previous findings indicating no significant relationship between kinesiophobia and objective characteristics22 of daily PA, walking endurance,41 and aerobic fitness using a cycling test42 in patients with chronic low back pain, which suggests that individuals with clinical levels of fear of movement would mainly avoid spinal-related functions, but would remain physically active during their daily routine.22 Since our sample covers a broad range of RMDs, it seems plausible that the measures of objective fitness chosen for the present study were not specifically tailored for the heterogeneity of our sample.
Finally, although the benefits of the time spent doing PA and fitness levels were conditional on the kinesiophobia level, the relationships linking the weekly time spent doing PA and functional performance with the physical component summary were significantly stronger than those linking these two variables with kinesiophobia. Therefore, although kinesiophobia is a component to target when the overall therapeutic goal includes improving the functioning of both physical and mental components of HRQoL, improving physical functioning appears a relevant clinical management strategy to reduce the maladaptive effect of kinesiophobia on daily functioning. To that end, and taking a patient-centered approach, examining patients-reported barriers and motivation,14 relying on the satisfaction of basic psychological needs, such as the feelings of competence, relatedness and autonomy43, and offering the opportunity to take part in supervised, group-adapted physical activities44 or multidisciplinary task-oriented exercise program,45 appear to be interesting ways to promote PA and to some extent, to develop physical functioning.
The second hypothesis was not supported by the results. In the first network analyses, the assessed functional performance was the variable most directly linked to the other variables of the network, suggesting that changes in this variable would have a great influence in one’s functioning, especially in physical functioning. However, according to the results of the second network, the stability of the centrality metrics was not sufficient to identify one or a few variables as the most influential. In light of the many interrelationships among the studied variables, the aim of increasing physical functioning combined with the perspective of developing social functioning, vitality43 and decreasing bodily pain (eg, by combining PA and relaxation46) when wishing to develop HRQoL in patients with RMDs using physical activity seems relevant.
Consistent with a recent study,32 the findings of this study reinforce the value of using network analyses when investigating interactions between biopsychosocial components of patients functioning. Beyond these results, the current study presents some limitations that should be considered. First, the cross-sectional design of the study did not allow for causal nor reciprocity inferences, although some can be theoretically hypothesized. In light of previous studies investigating the dynamic network structure of affect30 or depressive symptoms,47 this limitation could be overcome by longitudinal study designs to highlight the dynamic nature of HRQoL according to fluctuations in PA practice, fitness level and clinical condition. In addition, since individuals with RMDs generally do not meet the recommendations for moderate to vigorous PA,13 the present study only focused on the amount of PA performed weekly, and did not investigate its intensity. Given the benefits of moderate to vigorous PA practice on pain, fatigue, inflammation and stiffness,8,48 the use of questionnaires such as the Global Physical Activity Questionnaire49 or the International Physical Activity Questionnaire50 would have been relevant to specify the potential relationships between the intensity of PA practice, kinesiophobia and HRQoL. Finally, since RMDs share common symptoms but also because PA practice is recommended for each RMD (as well as for the general population), no expectations were made about potential network structure variations across the RMDs. Nevertheless, we recognized that our sample could have been more equally distributed among the different RMDs.
Conclusion
The results emphasize the positive direct and indirect relationships associating self-reported PA practice and objective fitness levels on HRQoL main and subdomains, while showing their negative relationships with kinesiophobia. These findings demonstrate the complexity of interacting biopsychosocial components in patients with RMD’s daily functioning. All components being interrelated and at a fairly similar importance ranking, the findings suggest that an effective clinical intervention targeting one of them may have positive effects, whether directly or indirectly, on the entire network. Further studies are needed to investigate the dynamic of such a network in relation to the RMDs characteristics.
Data Sharing Statement
The data set on which our analyses were based is contained in an open-access file available at: https://osf.io/pc6m5/quickfiles.
Ethics Approval and Informed Consent
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki declaration and its subsequent amendments or comparable ethical standards. The authors confirm that all mandatory laboratory health and safety procedures have been complied with in the course of conducting any experimental work.
Consent for Publication
All authors provide consent for the publication of this article.
Acknowledgments
The authors thank Geneviève Côté for the English proofreading. The authors also thank the rheumatology unit from Angers University Hospital for hosting the research project.
Author Contributions
All authors have:
- Contributed significantly to the reported work, whether in conception, study design, execution, data acquisition, analysis and interpretation, or in all these areas.
- Drafted or written the article, or substantially revised or critically reviewed it.
- Agreed on the journal to which the article will be submitted.
- Reviewed and agreed on all versions of the article before submission.
- Agreed to take responsibility and be accountable for the contents of the article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. doi:10.1016/S0140-6736(17)32154-2.
2. van der Heijde D, Daikh DI, Betteridge N, et al. Common language description of the term rheumatic and musculoskeletal diseases (RMDs) for use in communication with the lay public, healthcare providers and other stakeholders endorsed by the European League Against Rheumatism (EULAR) and the American College of Rheumatology (ACR). Ann Rheum Dis. 2018;77(6):829–832. doi:10.1136/annrheumdis-2017-212565
3. World Health Organization. Basic Documents of the World Health Organization.
4. Salaffi F, Di Carlo M, Carotti M, Farah S, Ciapetti A, Gutierrez M. The impact of different rheumatic diseases on health-related quality of life: a comparison with a selected sample of healthy individuals using SF-36 questionnaire, EQ-5D and SF-6D utility values. Acta Biomed. 2019;89(4):541–557. doi:10.23750/abm.v89i4.7298
5. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–131.
6. Rausch Osthoff AK, Niedermann K, Braun J, et al. 2018 EULAR recommendations for physical activity in people with inflammatory arthritis and osteoarthritis. Ann Rheum Dis. 2018;77(9):1251–1260. doi:10.1136/annrheumdis-2018-213585
7. Cuesta-Vargas AI, González-Sánchez M, Casuso-Holgado MJ. Effect on health-related quality of life of a multimodal physiotherapy program in patients with chronic musculoskeletal disorders. Health Qual Life Outcomes. 2013;11:19. doi:10.1186/1477-7525-11-19
8. Sveaas SH, Smedslund G, Hagen KB, Dagfinrud H. Effect of cardiorespiratory and strength exercises on disease activity in patients with inflammatory rheumatic diseases: a systematic review and meta-analysis. Br J Sports Med. 2017;51(14):1065–1072. doi:10.1136/bjsports-2016-097149
9. Metsios GS, Kitas GD. Physical activity, exercise and rheumatoid arthritis: effectiveness, mechanisms and implementation. Best Pract Res Clin Rheumatol. 2018;32(5):669–682. doi:10.1016/j.berh.2019.03.013
10. Gordon R, Bloxham S. A systematic review of the effects of exercise and physical activity on non-specific chronic low back pain. Healthcare (Basel). 2016;4:2. doi:10.3390/healthcare4020022
11. Krumov J, Obretenov V, Vodenicharova A, et al. The benefits to functional ambulation and physical activity of group-based rehabilitation in frail elderly Bulgarians undergoing total knee arthroplasty. Preliminary results. J Frailty Sarcopenia Falls. 2019;4(1):20–25. doi:10.22540/JFSF-04-020
12. Hurwitz EL, Morgenstern H, Chiao C. Effects of recreational physical activity and back exercises on low back pain and psychological distress: findings from the UCLA low back pain study. Am J Public Health. 2005;95(10):1817–1824. doi:10.2105/AJPH.2004.052993
13. Kelley GA, Kelley KS, Hootman JM. Effects of exercise on depression in adults with arthritis: a systematic review with meta-analysis of randomized controlled trials. Arthritis Res Ther. 2015;17(1):21. doi:10.1186/s13075-015-0533-5
14. Iversen MD, Frits M, von Heideken J, Cui J, Weinblatt M, Shadick NA. Physical activity and correlates of physical activity participation over three years in adults with rheumatoid arthritis. Arthritis Care Res (Hoboken). 2017;69(10):1535–1545. doi:10.1002/acr.23156
15. Pinto AJ, Roschel H, de sá pinto AL, et al. Physical inactivity and sedentary behavior: overlooked risk factors in autoimmune rheumatic diseases? Autoimmun Rev. 2017;16(7):667–674. doi:10.1016/j.autrev.2017.05.001
16. Boutevillain L, Dupeyron A, Rouch C, Richard E, Coudeyre E. Facilitators and barriers to physical activity in people with chronic low back pain: a qualitative study. PLoS One. 2017;12(7):e0179826. doi:10.1371/journal.pone.0179826
17. Liu S-H, Morais SA, Lapane KL, Kay J. Physical activity and attitudes and perceptions towards physical activity in patients with spondyloarthritis: a systematic review. Semin Arthritis Rheum. 2020;50(2):289–302. doi:10.1016/j.semarthrit.2019.10.002
18. Kori S, Miller R, Todd D. Kinesiophobia: a new view of chronic pain behavior. Pain Manage. 1990;3(1):35–43.
19. Luque-Suarez A, Martinez-Calderon J, Falla D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: a systematic review. Br J Sports Med. 2019;53(9):554–559. doi:10.1136/bjsports-2017-098673
20. Shim E-J, Hahm B-J, Go DJ, et al. Modeling quality of life in patients with rheumatic diseases: the role of pain catastrophizing, fear-avoidance beliefs, physical disability, and depression. Disabil Rehabil. 2018;40(13):1509–1516. doi:10.1080/09638288.2017.1300691
21. Comachio J, Magalhães MO, de Campos Carvalho e Silva APM, Marques AP. A cross-sectional study of associations between kinesiophobia, pain, disability, and quality of life in patients with chronic low back pain. Advan Rheumatol. 2018;58(1):8. doi:10.1186/s42358-018-0011-2
22. Carvalho FA, Maher CG, Franco MR, et al. Fear of movement is not associated with objective and subjective physical activity levels in chronic nonspecific low back pain. Arch Phys Med Rehabil. 2017;98(1):96–104. doi:10.1016/j.apmr.2016.09.115
23. Combs MA, Thorn BE. Yoga attitudes in chronic low back pain: roles of catastrophizing and fear of movement. Complement Ther Clin Pract. 2015;21(3):160–165. doi:10.1016/j.ctcp.2015.06.006
24. Kilinç H, Karahan S, Atilla B, Kinikli Gİ. Can fear of movement, depression and functional performance be a predictor of physical activity level in patients with knee osteoarthritis? Arch Rheumatol. 2019;34(3):274–280. doi:10.5606/ArchRheumatol.2019.7160
25. Greenberg J, Mace RA, Popok PJ, et al. Psychosocial correlates of objective, performance-based, and patient-reported physical function among patients with heterogeneous chronic pain. J Pain Res. 2020;13:2255–2265. doi:10.2147/JPR.S266455
26. Craig KD. The social communication model of pain. Can Psychol. 2009;50(1):22–32. doi:10.1037/a0014772
27. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
28. Fried EI, van Borkulo CD, Cramer AOJ, Boschloo L, Schoevers RA, Borsboom D. Mental disorders as networks of problems: a review of recent insights. Soc Psychiatry Psychiatr Epidemiol. 2017;52(1):1–10. doi:10.1007/s00127-016-1319-z
29. Costantini G, Richetin J, Preti E, Casini E, Epskamp S, Perugini M. Stability and variability of personality networks. A tutorial on recent developments in network psychometrics. Pers Individ Dif. 2019;136:68–78. doi:10.1016/j.paid.2017.06.011
30. Pavani JB, Le Vigouroux S, Kop JL, Congard A, Dauvier B. A network approach to affect regulation dynamics and personality trait‐induced variations: extraversion and neuroticism moderate reciprocal influences between affect and affect regulation strategies. Eur J Pers. 2017;31(4):329–346.
31. Kossakowski JJ, Epskamp S, Kieffer JM, van Borkulo CD, Rhemtulla M, Borsboom D. The application of a network approach to Health-Related Quality of Life (HRQoL): introducing a new method for assessing HRQoL in healthy adults and cancer patients. Qual Life Res. 2016;25(4):781–792. doi:10.1007/s11136-015-1127-z
32. Thompson EL, Broadbent J, Fuller-Tyszkiewicz M, Bertino MD, Staiger PK, Network A. Analysis of the links between chronic pain symptoms and affective disorder symptoms. Int J Behav Med. 2019;26(1):59–68. doi:10.1007/s12529-018-9754-8
33. Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, Borsboom D. qgraph: network visualizations of relationships in psychometric data. J Stat Softw. 2012;48(1):1–18. doi:10.18637/jss.v048.i04
34. French DJ, Roach PJ, Mayes S. Peur du mouvement chez des accidentés du travail: L’Échelle de Kinésiophobie de Tampa (EKT). Can J Behav Sci. 2002;34(1):28–33. doi:10.1037/h0087152
35. Leplege A, Ecosse E, Coste J, Pouchot J, Perneger T. Le questionnaire MOS SF-36: Manuel de l’utilisateur et guide d’interprétation des scores. Paris,France: Éditions ESTEM; 2001.
36. Rödjer L, Jonsdottir IH, Rosengren A, et al. Self-reported leisure time physical activity: a useful assessment tool in everyday health care. BMC Public Health. 2012;12(1):693. doi:10.1186/1471-2458-12-693
37. Grimby G, Börjesson M, Jonsdottir IH, Schnohr P, Thelle DS, Saltin B. The “Saltin-Grimby Physical Activity Level Scale” and its application to health research. Scand J Med Sci Sports. 2015;25 Suppl 4:119–125. doi:10.1111/sms.12611
38. Klokkerud M, Dagfinrud H, Uhlig T, et al. Developing and testing a consensus-based core set of outcome measures for rehabilitation in musculoskeletal diseases. Scand J Rheumatol. 2018;47(3):225–234. doi:10.1080/03009742.2017.1347959
39. Liao Y, Shonkoff ET, Dunton GF. The acute relationships between affect, physical feeling states, and physical activity in daily life: a review of current evidence. Front Psychol. 2015;6. doi:10.3389/fpsyg.2015.01975.
40. Schöndube A, Kanning M, Fuchs R. The bidirectional effect between momentary affective states and exercise duration on a day level. Front Psychol. 2016;7:1414. doi:10.3389/fpsyg.2016.01414
41. Vincent HK, Vincent KR, Seay AN, Conrad BP, Hurley RW, George SZ. Back strength predicts walking improvement in obese, older adults with chronic low back pain. PM R. 2014;6(5):418–426. doi:10.1016/j.pmrj.2013.11.002
42. Smeets RJ, van Geel KD, Verbunt JA. Is the fear avoidance model associated with the reduced level of aerobic fitness in patients with chronic low back pain? Arch Phys Med Rehabil. 2009;90(1):109–117. doi:10.1016/j.apmr.2008.07.009
43. Yu C, Rouse PC, Van Zanten JVJ, et al. Motivation-related predictors of physical activity engagement and vitality in rheumatoid arthritis patients. Health Psychology Open. 2015;2(2):1–9. doi:10.1177/2055102915600359-
44. Paolucci T, Morone G, Iosa M, et al. Efficacy of group-adapted physical exercises in reducing back pain in women with postmenopausal osteoporosis. Aging Clin Exp Res. 2014;26(4):395–402. doi:10.1007/s40520-013-0183-x
45. Monticone M, Ambrosini E, Rocca B, Cazzaniga D, Liquori V, Foti C. Group-based task-oriented exercises aimed at managing kinesiophobia improved disability in chronic low back pain. Eur J Pain. 2016;20(4):541–551. doi:10.1002/ejp.756
46. Shariat A, Alizadeh R, Moradi V, et al. The impact of modified exercise and relaxation therapy on chronic lower back pain in office workers: a randomized clinical trial. J Exerc Rehabil. 2019;15(5):703–708. doi:10.12965/jer.1938490.245
47. Bringmann LF, Lemmens LHJM, Huibers MJH, Borsboom D, Tuerlinckx F. Revealing the dynamic network structure of the Beck Depression Inventory-II. Psychol Med. 2015;45(4):747–757. doi:10.1017/S0033291714001809
48. Pinto RZ, Ferreira PH, Kongsted A, Ferreira ML, Maher CG, Kent P. Self-reported moderate-to-vigorous leisure time physical activity predicts less pain and disability over 12 months in chronic and persistent low back pain. Eur J Pain. 2014;18(8):1190–1198. doi:10.1002/j.1532-2149.2014.00468.x
49. Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J Public Health. 2006;14:66–70. doi:10.1007/s10389-006-0024-x
50. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.