")
Back to Journals » Journal of Pain Research » Volume 14
Direct and Indirect Pathways for Health-Related Quality of Life Change from Pain Improvement in Neuropathic Pain Patients with Spine Diseases: Path Analysis with Structural Equation Modeling Using Non-Interventional Study Results of Pregabalin
Authors Taguchi T, Nozawa K, Zeniya S , Murata T, Laurent T, Hirano T, Fujii K
Received 29 October 2020
Accepted for publication 28 April 2021
Published 1 June 2021 Volume 2021:14 Pages 1543—1551
DOI https://doi.org/10.2147/JPR.S289396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michael A Ueberall
Toshihiko Taguchi,1 Kazutaka Nozawa,2 Shigeki Zeniya,3 Tatsunori Murata,3 Thomas Laurent,4 Takahiro Hirano,4 Koichi Fujii2
1Japan Organization of Occupational Health and Safety, Yamaguchi Rosai Hospital, Sanyo-Onoda, Yamaguchi, Japan; 2Medical Affairs, Pfizer Japan Inc, Tokyo, Japan; 3CRECON Medical Assessment Inc., Tokyo, Japan; 4Clinical Study Support, Inc, Nagoya, Japan
Correspondence: Kazutaka Nozawa
Pfizer Japan Inc., Shibuya Bunka Quint Bldg., 22-7, Yoyogi 3-chome, Shibuya-ku, Tokyo, 150-8589, Japan
Tel +81-3-5309-7000
Email [email protected]
Background: Chronic low back pain or chronic cervical pain often has a neuropathic pain (NeP) component and patients with these conditions complain of sleep deprivation, loss of physical function, and reduced productivity due to pain. The objective of this study was to clarify the pathway by which pain, sleep disturbance due to pain, and physical function status influence QOL measures in chronic low back pain patients with NeP associated with lumbar spine diseases (CLBP-NeP) and in chronic cervical pain patients with NeP associated with cervical spine diseases (CCP-NeP).
Methods: A model assuming pain numeric rating scale (NRS), pain-related sleep interference scale (PRSIS), and functional indices (Roland Morris Disability Questionnaire [RMDQ], Neck Disability index [NDI]) as factors that can affect outcomes such as QOL (calculated using EuroQoL 5 Dimensions (EQ-5D)), the Patient Global Impression of Change (PGIC), and the Clinical Global Impression of Change (CGIC) was developed using structural equation modeling.
Results: Overall trends were frequently observed in both patients with CLBP-NeP and CCP-NeP. Pain NRS had the largest comprehensive direct impact on QOL based on EQ-5D and an overall impression of changing symptoms. The effects of pain NRS on each outcome were largely due to direct pain-related effects; however, for EQ-5D, an indirect effect via functional improvement was the primary factor.
Conclusion: Although the results of this study suggest that the indirect functional improvement of pain relief may not be recognized as a significant component of therapeutic effects by both physicians and patients, the pain-relieving intervention contributes directly to improvement of patients’ overall QOL and also indirectly via functional improvement in Japanese primary care settings. Accordingly, to achieve the therapeutic goal for patients with NeP and minimize the impact of pain burden, our findings indicate that pain relief interventions are also crucial from the perspective of the patient’s HRQOL.
Keywords: neuropathic pain, spine diseases, pregabalin, function, structural equation modeling, EuroQoL 5 Dimensions
Introduction
Low Back Pain (LBP), and neck pain are worldwide health concerns, especially in industrialized countries. Back and neck pain is the 11th highest leading cause of disability-adjusted life years (DALYs) in global, the fourth in high income countries and the third in Japan in the Global Burden of Disease studies 2019.1 In epidemiological studies,2,3 including those conducted in the Japanese general population,4 the number of adults reporting neck or shoulder pain represented almost one half of the surveyed population. Additionally, in a cross-sectional postal survey that included more than 6000 Japanese adults, 8% of respondents who reported experiencing severe chronic pain (defined as pain that lasted for more than 3 months) also reported chronic pain in their neck region, which adversely affected their quality of life.5 According to the Comprehensive Survey of Living Conditions in 2019 by Japan’s Ministry of Health, Labour and Welfare, LBP and shoulder pain were the most common symptoms in both men and women.6
Suka et al conducted a survey among a Japanese adult population who underwent health examinations to estimate the degree to which LBP decreased their quality of life (QOL) and reported the results in terms of reductions in QOL.7 Additionally, Sadosky et al analyzed the Japan National Health and Wellness Survey to clarify the effect of pain severity on health status (using SF-36), work productivity, healthcare resource use, and cost among Japanese respondents with LBP. LBP patients reported considerable and significant sleep disturbance and impairment of QOL at high pain severity levels.8 Previous studies conducted in other countries also reported similar results to those of the Japanese studies – that chronic LBP (CLBP), defined as LBP lasting ≥3 months, significantly increased patients’ burden in comparison with nonchronic LBP.9
In patients with cervical radiculopathy10,11 or cervical spondylotic myelopathy,12 neuropathic pain (NeP), which is well observed in CLBP through nerve root involvement,13,14 is a common symptom. In addition, in patients with NeP conditions, high pain severity is reported to be associated with poor sleep as well as reduced function and productivity;15 both the pain and the sleep disturbance affect the ability to function effectively and perform daily activities.
Pain improvement may have a positive impact on quality of life, however, no verification has yet been made as to whether simply improving pain is sufficient to achieve the therapeutic goal of chronic pain management, which aims to minimize its burden. Hence, in this study of patients with CLBP-NeP or CCP-NeP, we aimed to clarify how the pathways of pain, sleep disorders caused by pain, and the state of physical function influence indicators of patient health-related QOL in primary care settings using non-interventional study results of pregabalin in Japan.
Methods
Study Design and Data Source
This study is based on the secondary use of data from two observational studies on CLBP-NeP and CCP-NeP patients undergoing conventional analgesic care. As the objective of this analysis was to examine the comprehensive effects of pain improvement on QOL, only data from the pregabalin arm were used. The design of these studies is detailed below.
The original studies were a multicenter, prospective non-interventional observational study. Subjects with CLBP with accompanying lower limb radiating pain (with a neuropathic component)16 or chronic cervical pain with accompanying upper limb radiating pain (with a neuropathic component)17 – who met all other entry criteria – were enrolled at baseline for the duration of the study. The analgesic treatment was determined by the clinical judgment of the physician in charge of patient management; therapeutic choice was not related to the decision to take part in the study. All enrolled subjects received analgesic treatment. The study required 3 visits: Baseline/enrollment visit, Week 4 visit and Week 8 visit (or discontinuation). The studies were performed in accordance with the Declaration of Helsinki and received approval from the Byoin-Godo Ethical Review Board; all patients provided written informed consent prior to participation (Clinicaltrials.gov identifier: NCT02273908, NCT02868359)
Study Population in the Original Studies
Inclusion Criteria
In the original studies of CLBP-NeP patients16 and CCP-NeP patients,17 the following inclusion criteria were necessary for subjects to be eligible for the study: 1) Received adequate study information and then provided a signed informed consent form; 2) had CLBP accompanied by lower limb pain (with a neuropathic component) from the knee to the ankle (for CCP-NeP patients, subject required chronic pain with accompanying radiating pain to the superior limb beyond the elbow); 3) male or female and aged ≥18 years old (for CCP-NeP patients, ≥20 years old); 4) complained of LBP for 3 months or more before Visit 1 (for CCP-NeP patients, subject required cervical pain with accompanying radiating pain to superior limb [for a duration of ≥12 weeks at Visit 0]); 5) refractory to prior analgesics for ≥3 months; 6) was able and willing to complete all study related assessments and comply with the study schedule and clinical procedures at clinic; 7) had pain numerical rating scale (NRS) ≥5 at baseline (based on recall for the past week) (for CCP-NeP patients, subjects required pain NRS ≥5 and Pain Related Sleep Interference Scale (PRSIS) ≥1 at baseline [based on recall for the past week]).
Exclusion Criteria
In the original studies,16,17 patients meeting any of the following criteria were not included in the study: 1) Subjects who, in the opinion of the investigator, were not likely to complete the trial for whatever reason; 2) subjects previously treated with pregabalin.
Outcome
The EQ5D-5L, the Clinical Global Impression of Change (CGIC) and the Patient Global Impression of Change (PGIC) in the pregabalin arm of the original studies were used as outcomes, and the pain NRS, PRSIS and measures of disability (the Roland Morris Disability Index [RMDI] for CLBP-NeP and the neck disability index (NDI) for CCP-NeP, respectively) were evaluated to examine the magnitude of direct or indirect effects of pain improvement on QOL.16,17 However, we have recognized that the score measured by EQ-5D-5L reflects the general population’s sense of value, not patients. Since it focuses not only on symptoms, such as pain and numbness, but also on the overall health of patients, the EQ-5D-5L can be viewed as a comprehensive tool for evaluating changes in the overall health condition of patients with NeP (that patients in the original study may have experienced). Therefore, EQ-5D-5L was adopted as a method of measuring overall health-related QOL in this study with caution.
Endpoint
The primary endpoint was to investigate the direct and indirect pathways between pain NRS, PRSIS, and QOL using Structural Equation Modeling (SEM). QOL was considered as an observed variable based on Japanese index values. For each equation, study (as fixed effect), sex and age were included as covariates. These analyses were performed for PRO measurements at 8 weeks. It should be noted that the interactions between variables, either observed or latent, and the direction of interactions were assessed in an exploratory manner, based on model fitting. The purpose of the exploratory endpoint was to investigate the direct and indirect pathways between pain NRS, PRSIS, and either CGIC or PGIC using SEM. This was evaluated in the same manner as the primary endpoint.
Statistical Analysis
The primary and exploratory endpoints were investigated on a basis using structural equation modeling (SEM). Patients in whom any of the model parameters were missing were excluded from the analysis.
The pain NRS, PRSIS, and functional indices (RMDQ and NDI) were assumed as factors that would affect outcomes such as QOL calculated using the EQ-5D-5L, PGIC, and CGIC. According to the information obtained from interviews with clinical experts and preliminary data fitting tests, it was assumed that the effects of individual factors on outcomes may be direct or indirect, and a virtual model was created with age and sex as covariates (Figure 1). After parameter estimation, the model was updated with a modification index indicating the degree of improvement of the model at the time of the addition of a particular path, and the model was finalized to show the relationship between pain and various outcomes.
 |
Figure 1 Virtual model on which the analysis was based. Abbreviations: NRS, numeric rating scale; PGIC, Patients’ Global Impression of Change; PRSIS, pain-related sleep interference scale; RMDQ, Roland-Morris Disability Questionnaire. |
Final model fit was evaluated using the chi-square test. Briefly, if P>0.05 and the ratio of chi-square statistics divided by the degree of freedom were shown to be <1.5, the model was considered to be adequate. Then, to support the quality of the model further, the following statistics were also estimated: Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), Comparative Fit Index (CFI>0.95 considered acceptable),18 the Tucker-Lewis Index (TLI>0.95 considered acceptable),19 the Root Mean Square Error of Approximation (RMSEA<0.05 considered acceptable), and the Standardized Root Mean Square Residual (SRMR<0.05 considered acceptable).20 For final models, unstandardized regression coefficients along the corresponding p-values were presented. Additionally, this analysis was performed separately in patients with CLBP-NeP and in patients with CCP-NeP.
Results
A flow diagram of CLBP-NeP patients and CCP-NeP patients is shown in Figure 2; a total of 138 patients with CLBP-NeP and 138 patients with CCP-NeP were evaluated.
 |
Figure 2 Flow diagram of the patients. Abbreviations: CCP-NeP, chronic cervical pain patients with neuropathic pain associated with disease of the cervical spine; CLBP-NeP, chronic low back pain patients with neuropathic pain associated with disease of the lumbar spine; NRS, numeric rating scale; PRSIS, pain-related sleep interference scale. Notes: *Choice of therapy as determined by the clinical judgment of the treating physician. |
In terms of patient characteristics, CLBP-NeP patients were older (mean age at baseline: 69.1 years vs 58.3 years) and had a longer duration of pain (70.3 months vs 28.8 months) than CCP-NeP patients (Table 1). The pain NRS, PRISIS, and RMDQ/NDI scores at baseline did not differ significantly between CLBP-NeP and CCP-NeP patients (Table 1). At 8 weeks after administration of pregabalin, both CLBP-NeP and CCP-NeP patients showed similar improvements in the pain NRS and PRSIS (pain NRS: 2.4 for CLBP-NeP patients and 2.3 for CCP-NeP patients; PRSIS: 1.6 for CLBP-NeP patients and 1.5 for CCP-NeP patients) (Table 1).
 |
Table 1 Patient Characteristics |
Regarding the paths added following model update with the modification index, paths from age to PRSIS and from age to RMDQ were added when the EQ-5D was the outcome in CLBP-NeP patients, whereas no addition of paths was necessary when PGIC and CGIC were the outcomes in CLBP-NeP patients. In CCP-NeP patients, paths from age to PRSIS, from age to NDI, and from sex to NDI were added when the EQ-5D was the outcome, whereas no addition of paths was necessary when PGIC and CGIC were the outcomes. The statistics following the above corrections are shown in Table 2.
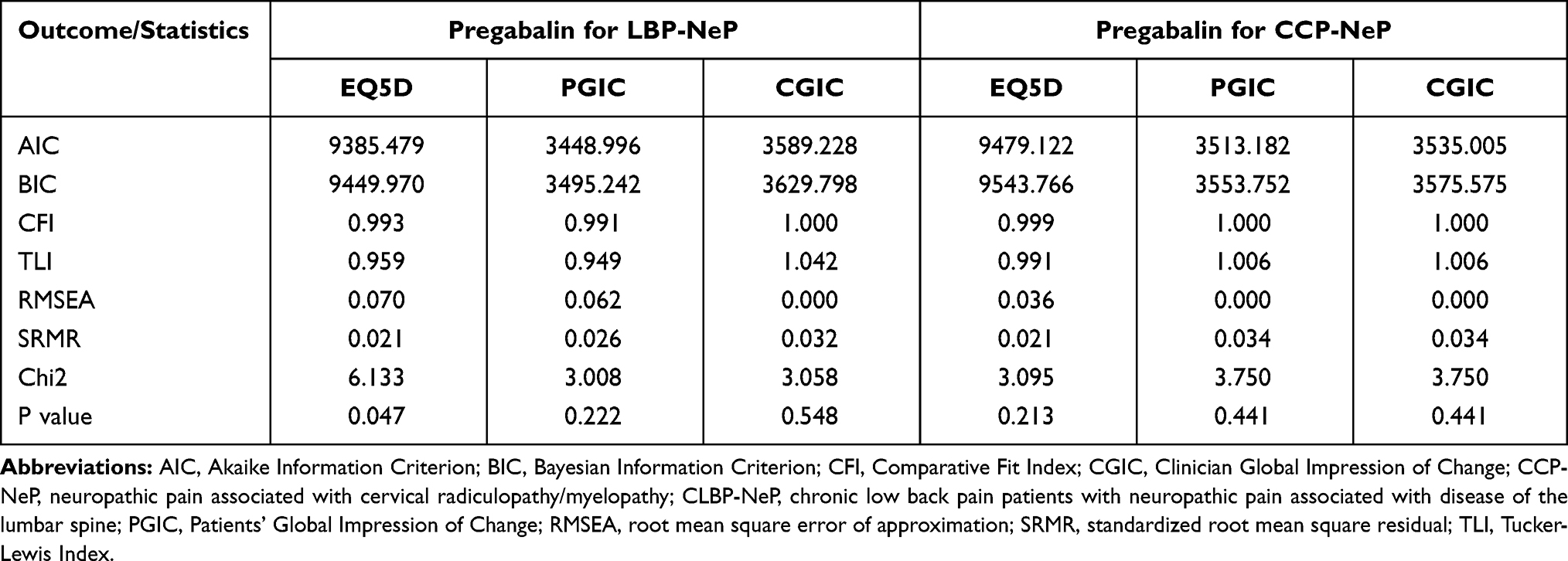 |
Table 2 Goodness-of-Fit Statistics |
The effects of pain, sleep, and function on each outcome are shown in Figure 3 for overview, and Figures S1 and S2 for details. In CLBP-NeP patients, the effects of pain NRS on each outcome were largely indirect via function in the EQ-5D (−0.0269), with an increase of one in the pain NRS resulting in a worsening of 0.0269 in QOL as measured by the EQ-5D via function. For PGIC and CGIC, in contrast, direct pain-related effects were greater (−0.165 and −0.158, respectively), with an increase of one in the pain NRS resulting in decreases of 0.165 and 0.158 in PGIC and CGIC, respectively. In CCP-NeP patients, the effects of pain NRS on each outcome were due to indirect effects via functional improvement in the EQ-5D (−0.0332), whereas direct pain-related effects were greater in PGIC and CGIC (−0.230 and −0.237, respectively). The indirect effects via sleep from pain were not significant in both patient groups.
 |
Figure 3 Direct and indirect effects on EQ-5D, PGIC and CGIC from Pain NRS in CLBP-NeP, CCP-Nep patients, and those with severe pain. Abbreviations: CGIC, Clinician Global Impression of Change; CLBP-NeP, chronic low back pain patients with neuropathic pain associated with disease of the lumbar spine; CCP-NeP, chronic cervical pain patients with neuropathic pain associated with disease of the cervical spine; NRS, numeric rating scale; PGIC, Patients’ Global Impression of Change; PRSIS, pain-related sleep interference scale; RMDQ, Roland-Morris Disability Questionnaire. Notes: *Negative value items with small changes were shown only in the Figures S1, Figures S2 and Figures S3 and excluded from calculation of total effects in order to present the reader with the main impact of indicators such as Pain NRS. |
The effects of pain, sleep, and function on each outcome in patients with severe pain are also shown in Figure 3, and Figure S3. In patients with severe pain, the effects of individual factors on each outcome were increased; the rate of increase was approximately 1.5 times greater when the EQ-5D was the outcome in both patient groups (CLBP-NeP: −0.0624/-0.0429=1.45, CCP-NeP: −0.0607/-0.0397=1.52), and it was relatively small when PGIC and CGIC were the outcomes (Figures S4 and S5).
Discussion
The objective of this study was to clarify the pathway through which pain, sleep disturbance due to pain, and physical function status influenced the indices of overall impression to changing symptoms, such as the EQ-5D, PGIC, and CGIC in neuropathic pain patients with lumbar and cervical radiculopathy in Japanese primary care settings.
Some trends were commonly present in both patients with CLBP-NeP and those with CCP-NeP. Pain NRS had the largest comprehensive impact on QOL based on the EQ-5D and the overall impression to changing symptoms (PGIC and CGIC). Suka et al also reported QOL reduction in EQ-5D due to LBP in a Japanese adult population who underwent health examinations. Since QOL – as measured by the EQ-5D – reflects overall health condition, patients with LBP have, in addition to the pain itself, other factors potentially affecting QOL such as pain-related anxiety and difficulty moving the lower back. The effects of pain on QOL noted in our study are in agreement with the previous study.8 Furthermore, the effects of pain NRS on the above outcomes were largely due to direct pain-related effects, but in the EQ-5D, indirect effects via functional improvement were equal to direct pain-related effects. This may reflect the fact that the EQ-5D includes items related to function such as self-care and the degree of mobility, and that pain causes inconveniences in daily activities such as housework and dressing, which result in a decline in QOL. In contrast, the effects on PGIC and CGIC largely consisted of direct pain-related effects, and minimally comprised indirect effects via functional improvement. These indices are used to assess changes in symptoms and may reflect the fact that changes in pain are more easily perceived by patients and evaluated by physicians than changes in neck or lower back movement. This result may reflect that patients easily perceive improvement in pain as improvement in symptoms and that the physicians’ evaluation of symptoms is influenced by the patients’ claims. In addition, when considering the degree of indirect effects via functional improvement of pain NRS in EQ-5D, patients and physicians may not recognize a significant component of the therapeutic effects. A stratified analysis limited to patients whose pain was severe showed an increase in the unit impact of each factor on each outcome (the amount of change in outcome such as EQ-5D when pain NRS or PRSIS increased by one).
Previous studies reported that pregabalin improves sleep disturbance among CLBP-NeP and CCP-NeP patients.16,17 Therefore, we presumed pregabalin has a positive effect via sleep on EQ-5D; however, the indirect effect via PRSIS had no large effect on EQ-5D. We think that EQ-5D would not be sensitive to improvement via sleep due to lack of questions related to sleep and it could be one of limitations of the evaluation.
The structures of each impact of direct and indirect pain-related effect on EQ5D were consistent between CLBP-NeP and CCP-NeP patients in the evaluation of total score across all five dimensions. However, the significant dimensions in EQ5D should be different between CLBP-NeP and CCP-NeP patients; for instance, mobility for CLBP-NeP and self-care for CCP-NeP patients. A further investigation would therefore be informative for clinical interpretation to clarify the structural difference of pain impact on each individual dimension in EQ5D (ie mobility, self-care, usual activity, pain/discomfort, and anxiety/depression) according to the different location of pain.
The present study suggests that the impact of neck and LBP on the EQ-5D consist of direct and indirect effects, therefore, it is possible that the pain-focused treatment not only reduces the pain but also improves the function of the low back and neck, which contributes to the improvement of the patient’s QOL.
This study has several limitations. The first limitation concerns generalizability. In this study, as the subject is limited to NeP patients with spine diseases, the results cannot be applied to diseases chiefly comprising nociceptive pain such as cervical-shoulder-arm syndrome.
The second limitation concerns internal validity. The score measured by EQ-5D-5L reflects the general population’s sense of value, not patients, which may be different from the values of patients with chronic pain, a population studied in this study. If this is the case, the magnitude of the effects of pain and sleep indices on the EQ-5D may have been underestimated.
In addition to function-related factors, the pain-related factors that indirectly affect outcomes include psychological states such as pain-induced anxiety and catastrophic thinking. Moreover, in this study, the analysis was performed assuming linearity between outcomes such as EQ-5D and dependent variables such as pain NRS and PRSIS. According to indicators that judge the excellence of the model such as AIC, BIC, and CFI, the best fit model was used. However, non-linear effects may remain between outcomes and parameters. This study may have underestimated the indirect effects of pain on outcomes because these factors were not measured. Despite the above limitations, we believe that the results of this study generally reflect the effects of pain on the overall health condition and therapeutic effects in patients with NeP of middle-age and older (a population in which NeP is prevalent). In addition, since the EQ-5D comprises items concerning self-care, daily activities, and the degree of movement, as well as pain, further research will reveal the details of indirect effects of pain on EQ-5D such as which dimensions are affected.
Conclusion
Although the results of this study suggest that the indirect functional improvement for pain relief may not be recognized as a significant component of therapeutic benefit by both physicians and patients, it could be concluded that not only does a pain-relieving intervention contribute to improvement of patients’ overall HRQOL directly, but it also does so indirectly via functional improvement in Japanese primary care settings.
Accordingly, to achieve the therapeutic goal for patients with NeP leading to minimized pain, our findings support the notion that interventions for pain relief are also crucial from the perspective of the patient’s HRQOL.
Disclosure
This study was sponsored by Pfizer Japan Inc. Kazutaka Nozawa and Koichi Fujii are employees of Pfizer Japan Inc. Shigeki Zeniya and Tatsunori Murata are employees of CRECON Medical Assessment Inc. Thomas Laurent and Takahiro Hirano are employees of Clinical Study Support, Inc. Toshihiko Taguchi was not financially compensated for their collaboration in this project or for the development of this manuscript, although Toshihiko Taguchi has received honorarium from Pfizer Japan Inc. outside of this work. The authors report no other conflicts of interest in this work.
References
1. World Health Organization (WHO). The global health observatory, 2021. World Health Organization; 2021. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/global-health-estimates-leading-causes-of-dalys.
2. Cote P, Kristman V, Vidmar M, et al. The prevalence and incidence of work absenteeism involving neck pain: a cohort of Ontario lost-time claimants. Spine (Phila Pa 1976). 2008;33(4Suppl):S192–198. doi:10.1097/BRS.0b013e3181644616
3. Croft PR, Lewis M, Papageorgiou AC, et al. Risk factors for neck pain: a longitudinal study in the general population. Pain. 2001;93(3):317–325. doi:10.1016/S0304-3959(01)00334-7
4. Takasawa E, Yamamoto A, Kobayashi T, et al. Characteristics of neck and shoulder pain in the Japanese general population. J Orthop Sci. 2015;20(2):403–409. doi:10.1007/s00776-014-0676-2
5. Inoue S, Kobayashi F, Nishihara M, et al. Chronic pain in the Japanese community—prevalence, characteristics and impact on quality of life. PLoS One. 2015;10(6):e0129262. doi:10.1371/journal.pone.0129262
6. Ministry of Health, Labour and Welfare. Comprehensive survey of living conditions, 2019. Tokyo, Japan: Ministry of Health, Labour and Welfare; 2019. Available from: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa19/dl/14.pdf.
7. Suka M, Yoshida K. Low back pain deprives the Japanese adult population of their quality of life: a questionnaire survey at five healthcare facilities in Japan. Environ Health Prev Med. 2008;13(2):109–115. doi:10.1007/s12199-007-0011-z
8. Sadosky AB, DiBonaventura M, Cappelleri JC, et al. The association between lower back pain and health status, work productivity, and health care resource use in Japan. J Pain Res. 2015;8:119–130. doi:10.2147/JPR.S76649
9. Becker A, Held H, Redaelli M, et al. Low back pain in primary care. Costs of care and prediction of future health care utilization. Spine (Phila Pa 1976). 2010;35(18):1714–1720. doi:10.1097/brs.0b013e3181cd656f
10. Tampin B, Slater H, Briffa NK. Neuropathic pain components are common in patients with painful cervical radiculopathy, but not in patients with nonspecific neck-arm pain. Clin J Pain. 2013;29(10):846–856. doi:10.1097/AJP.0b013e318278d434
11. Tsunoda D, Iizuka Y, Iizuka H, et al. Associations between neck and shoulder pain (called katakori in Japanese) and sagittal spinal alignment parameters among the general population. J Orthop Sci. 2013;18(2):216–219. doi:10.1007/s00776-012-0341-6
12. Yamashita T, Takahashi K, Yonenobu K, Kikuchi S. Prevalence of neuropathic pain in cases with chronic pain related to spinal disorders. J Orthop Sci. 2014;19(1):15–21. doi:10.1007/s00776-013-0496-9
13. Dionne CE, Dunn KM, Croft PR, et al. A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine (Phila Pa 1976). 2008;33(1):95–103. doi:10.1097/BRS.0b013e31815e7f94
14. Webb R, Brammah T, Lunt M, Urwin M, Allison T, Symmons D. Prevalence and predictors of intense, chronic, and disabling neck and back pain in the UK general population. Spine (Phila Pa 1976). 2003;28(11):1195–1202. doi:10.1097/01.BRS.0000067430.49169.01
15. Sadosky A, Hopper J, Parsons B. Painful diabetic peripheral neuropathy: results of a survey characterizing the perspectives and misperceptions of patients and healthcare practitioners. Patient Center Outcomes Res. 2014;7:107–114. doi:10.1007/s40271-013-0038-8
16. Taguchi T, Igarashi A, Watt S, et al. Effectiveness of pregabalin for the treatment of chronic low back pain with accompanying lower limb pain (neuropathic component): a non-interventional study in Japan. J Pain Res. 2015;8:487–497. doi:10.2147/JPR.S88642
17. Taguchi T, Nozawa K, Parsons B, et al. Effectiveness of pregabalin for treatment of chronic cervical radiculopathy with upper limb radiating pain: an 8-week, multicenter prospective observational study in Japanese primary care settings. J Pain Res. 2019;12:1411–1424. doi:10.2147/JPR.S191906
18. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–246. doi:10.1037/0033-2909.107.2.238
19. Tucker LR, Lewis C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika. 1973;38:1–10. doi:10.1007/BF02291170
20. Marsh HW, Hau KT, Wen Z. In search of golden rules: comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) findings. Struct Equ Modeling. 2004;11(3):320–341. doi:10.1207/s15328007sem1103_2
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.