Back to Journals » OncoTargets and Therapy » Volume 19
Diffuse Sclerosing Variant of Papillary Thyroid Carcinoma: A Single-Center Case Series of Five Patients
Authors Sun X, Liu Y, Peng J, Liu J
Received 10 January 2026
Accepted for publication 28 March 2026
Published 7 April 2026 Volume 2026:19 595202
DOI https://doi.org/10.2147/OTT.S595202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr John Maher
XiaoYu Sun,1,* Yanze Liu,2,* Jie Peng,1 Jiaqi Liu2
1Department of Pathology, Zibo Central Hospital, Shandong Zibo, People’s Republic of China; 2Department of Breast and Thyroid Surgery, Zibo Central Hospital, Shandong Zibo, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiaqi Liu, Department of Breast and Thyroid Surgery, Zibo Central Hospital, Shandong Zibo, People’s Republic of China, Email [email protected]
Background: Diffuse sclerosing variant papillary thyroid carcinoma (DSVPTC) is a rare subtype of papillary thyroid carcinoma characterized by diffuse intrathyroidal involvement and frequent cervical lymph node metastasis. This study aims to delineate the clinicopathologic features, treatment outcomes, and recurrence patterns of DSVPTC.
Methods: We retrospectively reviewed five patients with histopathologically confirmed DSVPTC treated at Zibo Central Hospital between 2009 and 2025. Follow-up data were collected until December 30, 2025.
Results: Patients were aged 22– 54 years (median: 41 years) and 60% (3/5) were female. Hashimoto’s thyroiditis was present in 80% (4/5). All patients presented with diffuse microcalcifications on ultrasound (100%, 5/5). Thyroid FNA was performed in 80% (4/5) and all aspirates were Bethesda category VI. Cervical lymph node metastasis was observed in all patients: central compartment in 100% (5/5) and lateral neck in 60% (3/5). TNM staging (8th edition) included: pT1aN1aM0 (n=1), pT1aN1bM0 (n=1), pT3bN1aM0 (n=1), pT3bN1bM0 (n=2). According to ATA risk stratification, 3 patients were classified as high risk and 2 as intermediate risk. All patients underwent total thyroidectomy with bilateral central neck dissection. Lateral neck dissection was performed in 3 patients with radiologic evidence of lateral nodal disease. All patients received TSH suppression therapy (TSH < 0.1 mIU/L) and two courses of I-131 therapy (100 mCi per course) at 3 and 6 months postoperatively. With a median follow-up of 2 years (range: 1– 16 years), structural recurrence occurred in 2 patients (40%, 2/5) in the ipsilateral lateral neck at 1 and 4 years, respectively. No distant metastasis or disease-specific death occurred.
Conclusion: In this small series of five patients, DSVPTC commonly presented as a nodule-negative “snowstorm” microcalcification phenotype with high nodal burden. Despite aggressive multimodal therapy including total thyroidectomy, TSH suppression, and scheduled radioiodine, lateral neck recurrence occurred in 40% of patients. Meticulous preoperative lateral neck assessment and long-term imaging-based surveillance remain essential.
Keywords: diffuse sclerosing variant, papillary thyroid carcinoma, microcalcification, lymph node metastasis, recurrence, radioiodine, TSH suppression
Introduction
Papillary thyroid carcinoma (PTC) is the most common endocrine malignancy with an excellent prognosis overall; however, significant heterogeneity exists among its histologic variants. Diffuse sclerosing variant papillary thyroid carcinoma (DSVPTC) is an uncommon subtype characterized histologically by diffuse thyroid involvement, prominent stromal sclerosis, abundant psammoma bodies, marked lymphocytic infiltration, and frequent squamous metaplasia.1 Lacking a discrete space-occupying lesion, DSVPTC often evades detection during screening, potentially compromising preoperative staging and surgical planning.2
The pathogenesis of DSVPTC remains incompletely understood. While high-dose radiation exposure has been proposed as a potential risk factor, DSVPTC also occurs in patients without radiation history. Notably, autoimmune thyroid disease—particularly Hashimoto’s thyroiditis—frequently coexists with DSVPTC, suggesting that the immune-activated microenvironment may contribute to its distinctive phenotype.3 However, the relationships among inflammation, molecular events, and clinical outcomes require further investigation.
Ultrasonographically, DSVPTC typically presents with diffuse parenchymal heterogeneity and widespread microcalcifications, frequently described as a “snowstorm” appearance, often accompanied by suspicious cervical lymphadenopathy. In contrast to conventional PTC presenting as a solitary hypoechoic nodule, DSVPTC lacks a definitive mass effect, which may lead to diagnostic delay.4,5
Fine-needle aspiration cytology (FNAC) diagnostic yield in DSVPTC depends heavily on target selection, as tumors present as diffuse microcalcifications rather than discrete nodules. Sampling from densely calcified regions and concurrent lymph node aspiration may improve diagnostic accuracy.6
Therapeutically, DSVPTC demonstrates higher propensity for cervical lymph node metastasis than conventional PTC, making preoperative mapping and surgical planning critical. Despite TSH-suppressive therapy and radioiodine adjuvant treatment, locoregional recurrence may still occur, necessitating imaging-led follow-up with cytologic confirmation of suspicious nodes.7
Given the rarity of DSVPTC, evidence remains limited to small cohorts. Herein, we retrospectively analyzed five patients with pathologically confirmed DSVPTC to delineate clinicopathologic and imaging features, summarize compartment-oriented surgical management and outcomes, and describe recurrence patterns to inform preoperative staging and long-term surveillance.
Methods
This study was a single-center, retrospective case series of patients with diffuse sclerosing variant papillary thyroid carcinoma (DSVPTC) treated at Zibo Central Hospital between January 1, 2009 and December 1, 2025. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. All patient data were anonymized, and patient confidentiality was strictly maintained. The study protocol was approved by the Institutional Review Board (IRB) of Zibo Central Hospital. Given the retrospective nature of the study, the requirement for informed consent was waived.
Participants
Patients were eligible if they (1) underwent primary thyroid surgery at our institution, (2) had a postoperative histopathologic diagnosis of DSVPTC, and (3) had available perioperative imaging (Figures 1–3)/cytology and follow-up data sufficient for outcome assessment. Patients with incomplete key clinicopathologic information were excluded. Five patients met the inclusion criteria and were included in this analysis.
 |
Figure 1 Representative preoperative ultrasonography demonstrating a “nodule-negative” diffuse thyroid involvement pattern with extensive sand-like microcalcifications in DSVPTC. (Patient 1, Patient 3, Patient 5). |
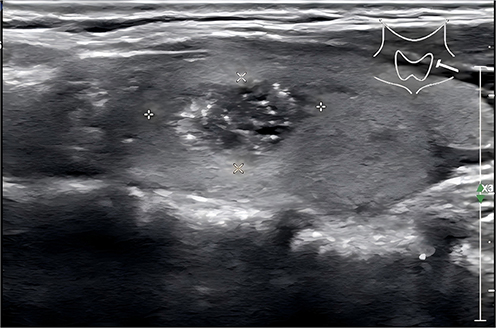 |
Figure 2 Representative preoperative ultrasonography demonstrating a “nodule-negative” diffuse thyroid involvement pattern with topical type sand-like microcalcifications in DSVPTC. (Patient 2 and Patient 4). |
 |
Figure 3 Contrast-enhanced neck CT demonstrated heterogeneous or decreased thyroid attenuation in all cases (100%). |
Data Collection
Clinical data were extracted from electronic medical records, including demographics, clinical presentation, comorbid thyroid disease (Hashimoto’s thyroiditis and hyperthyroidism), preoperative imaging, cytology, operative and pathology reports, immunohistochemistry (IHC), molecular testing results, postoperative management, and oncologic outcomes. Pathological specimens were processed as follows: surgical specimens were fixed in 4.0% neutral buffered formalin, sectioned at 5-mm intervals, and embedded routinely. H&E staining was performed on 4-μm sections. IHC was conducted using the EnVision two-step method with antibodies against CK19, TG, and TTF-1 (Dako). All slides were independently evaluated by two associate chief pathologists in a double-blind manner for diagnostic confirmation.
Molecular Testing
Multigene testing was performed in 3 of 5 patients using a thyroid cancer 12-gene detection kit (fluorescence PCR method). The remaining 2 patients did not undergo molecular testing because this test was not available at our institution’s pathology department during their treatment period.
For the testing procedure, tumor tissue obtained from surgery was placed into centrifuge tubes containing 10 volumes of RNAstore preservation solution (Hangzhou Scieasy Diagnostics Co., Ltd.) to ensure the sample was completely immersed in the preservation solution, then stored at −20°C or −80°C. RNA extraction was performed weekly in batches using a commercial RNA extraction kit.
The following gene alterations were detected: BRAF V600E point mutation; TERT promoter region (TERTp) C228T/C250T mutations; KRAS gene G12C/G12V/Q61R mutations; NRAS gene Q61R mutation; HRAS gene Q61R mutation; CCDC6 (exons 1 or 8)-RET (exon 12) gene fusion (RET/PTC1); PAX8 (exon 10)-PPARG (exon 2) gene fusion; and ETV6 (exon 4)-NTRK3 (exon 14) gene fusion.
Kit performance validation: (1) Stability: the kit maintained satisfactory performance after 6 months of storage under specified conditions; (2) Reference sample detection: all variant sites showed positive results for positive reference samples and negative results for negative reference samples, with positive results for precision reference samples; (3) Detection limit: at least 1% mutation could be detected in a background of 5 ng/μL wild-type genomic DNA for BRAF, RAS (KRAS/NRAS/HRAS), and TERT gene mutations; at least 500 copies of fusion mutations could be detected at the RNA level.
Surgical Procedures
All five patients underwent surgical treatment: (1) Management of the primary tumor: Because preoperative fine-needle aspiration indicated metastatic disease in the level VI (central compartment) lymph nodes, total thyroidectomy was performed in all patients after detailed discussion with the patients and their families. (2) Central compartment lymph node management: Bilateral central neck dissection was routinely performed for all patients. (3) Lateral neck lymph node management: Therapeutic lateral neck dissection was performed in patients with suspected lateral cervical lymph node metastasis on preoperative ultrasonography or CT, including lymph node levels II, III, IV, and V. Prophylactic lateral neck dissection was not performed in patients without radiologic evidence of lateral nodal disease.
Postoperative Management
All patients received suppressive levothyroxine therapy with serum TSH maintained at <0.1 mIU/L. Thyroid function tests (TSH, Free T4, Free T3) were monitored monthly after surgery until TSH suppression was stably achieved, after which testing was performed every 3–6 months.
Radioiodine (I-131) therapy was administered according to a standardized protocol: the first course was given at 3 months postoperatively, and the second course at 6 months. All patients received a fixed dose of 100 mCi (3.7 GBq) per course. Preparation for I-131 therapy included thyroid hormone withdrawal for 4 weeks to achieve TSH >30 mIU/L before each treatment. A post-therapy whole-body scan was performed 5–7 days after each administration. No significant adverse reactions were observed in any patient during or after I-131 therapy. Adverse events were monitored and recorded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Serum thyroglobulin (Tg) was assessed during follow-up using the Roche Cobas e601 immunoassay analyzer. Anti-thyroglobulin antibodies (TgAb) were measured concurrently to interpret Tg values when applicable. In patients with Hashimoto’s thyroiditis (n=4), Tg monitoring was not routinely performed due to potential interpretative limitations from interfering antibodies.
Follow-up
Patients were followed up with neck ultrasound every 6 months. Suspicious lymph nodes were evaluated with ultrasound-guided FNA for cytology. The last follow-up date was December 30, 2025. Patient-level follow-up times were: Patient 1: 1 year; Patient 2: 2 years (with recurrence at 1 year); Patient 3: 16 years; Patient 4: 1 year; Patient 5: 9 years (with recurrence at 4 years). Median follow-up was 2 years (range: 1–16 years).
Statistical Analysis
Due to the small sample size (n=5), descriptive statistics were used to summarize the data. Categorical variables were presented as n (%). Continuous variables were presented as median (range).
Results
Oncologic Summary
Of five DSVPTC patients, all (100%) presented with cervical lymph node metastasis at diagnosis, including central (n=5, 100%) and lateral compartment involvement (n=3, 60%). With a median follow-up of 2 years (range: 1–16 years), structural recurrence occurred in 2 patients (40%), both in the lateral neck. No distant metastasis or disease-specific death was observed.
Clinicopathologic Characteristics
Among the five patients with DSVPTC, four (80%) had coexisting Hashimoto’s thyroiditis and one (20%) had hyperthyroidism. Diffuse thyroid calcification involved a single lobe in two cases (40%) and both lobes in three cases (60%). All patients were asymptomatic, with thyroid abnormalities detected during routine health screening. Cervical lymphadenopathy was present in all cases (100%): level VI in all five patients and lateral neck in three patients (60%).
Ultrasound-guided fine-needle aspiration cytology (FNAC) of calcified thyroid areas and suspicious lymph nodes was performed in four patients (80%). Thyroid aspirates were classified as Bethesda category VI, and lymph node cytology suggested metastatic carcinoma. Contrast-enhanced neck CT demonstrated heterogeneous or decreased thyroid attenuation in all cases (100%). No distant metastasis was identified at initial staging.
Postoperative pathology confirmed cervical lymph node metastasis in all patients (100%), including central compartment metastasis in five (100%) and lateral neck metastasis in three (60%). Extrathyroidal extension was observed in three patients (60%). Immunohistochemistry showed tumor cell positivity for thyroglobulin (TG, Figure 4), CK19 (Figure 5), and TTF-1 (Figure 6) in all cases, with squamous metaplasia (Figure 7) identified in four patients (80%). Multigene testing in three patients revealed RET mutation in one case and BRAF V600E mutation in two cases (Table 1 and Table 2).
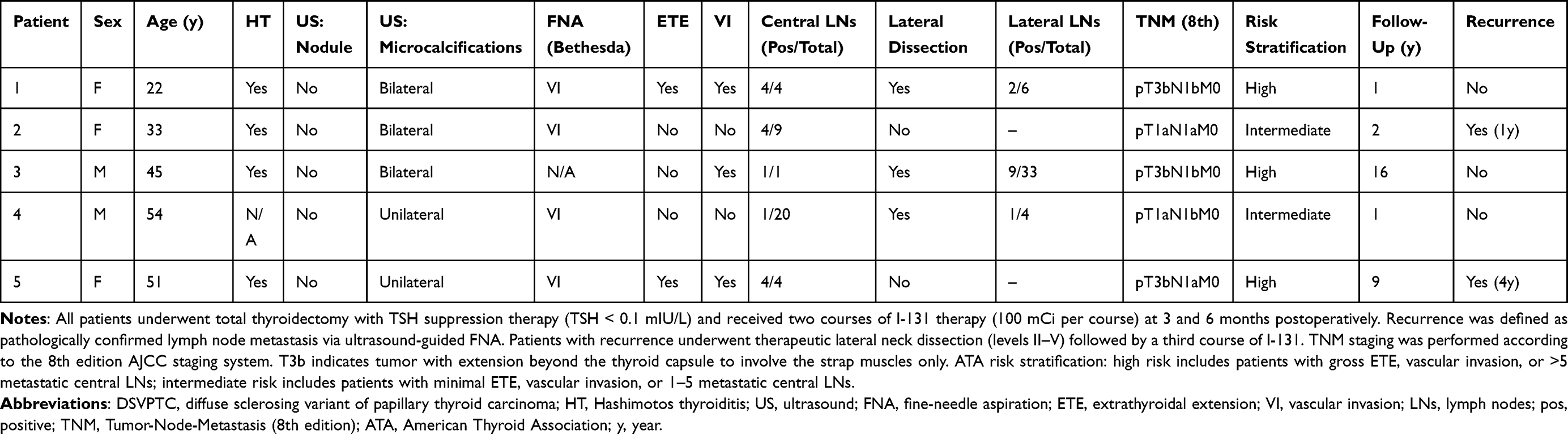 |
Table 1 Clinicopathologic Characteristics and Treatment Outcomes of Patients with DSVPTC (n = 5) |
 |
Table 2 Summary of Key Features and Outcomes (n = 5) |
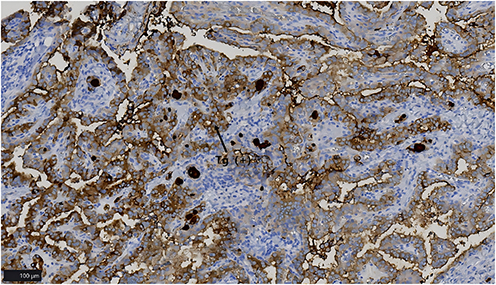 |
Figure 4 Immunohistochemistry for thyroglobulin (TG) showing diffuse tumor cell positivity in DSVPTC in all cases. |
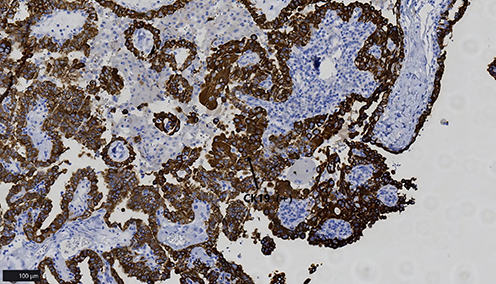 |
Figure 5 Immunohistochemistry for CK19 showing strong tumor cell positivity in all cases. |
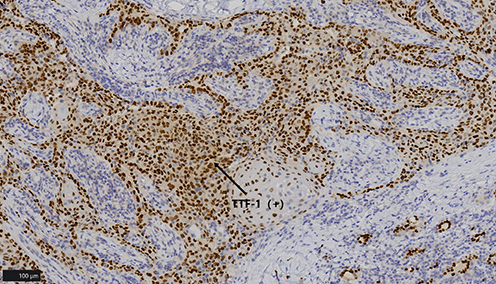 |
Figure 6 Immunohistochemistry for TTF-1 showing nuclear positivity consistent with thyroid origin in all cases. |
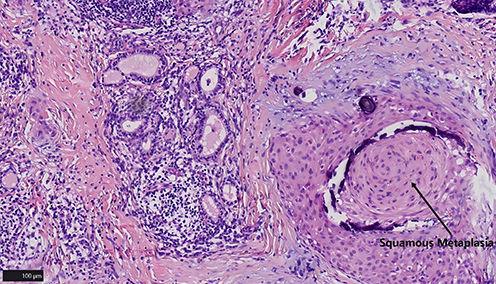 |
Figure 7 Histopathology demonstrating squamous metaplasia (arroe) within DSVPTC in four patients (Patient 4 was excluded). |
Postoperative Management and Oncologic Outcomes
All patients received strict TSH suppression (TSH <0.1 mIU/L) and standardized radioiodine therapy (I-131 at 3 months postoperatively, with a second course at 6 months). No significant adverse reactions were observed during or after I-131 therapy.
During follow-up (median: 2 years; range: 1–16 years), two patients (40%) developed structural recurrence in the lateral neck. Specifically, Patient 2 experienced lateral neck lymph node recurrence at 1 year postoperatively, and Patient 5 developed lateral neck recurrence at 4 years postoperatively. Both recurrences were confirmed by ultrasound-guided fine-needle aspiration cytology showing metastatic carcinoma. These patients subsequently underwent therapeutic lateral neck dissection (levels II–V) followed by a third course of I-131 radioiodine therapy. No disease-specific death occurred during the observation period.
Discussion
In this single-center case series of five patients with diffuse sclerosing variant papillary thyroid carcinoma (DSVPTC), several clinically meaningful patterns were observed. First, DSVPTC frequently manifested as a diffuse, “nodule-negative” thyroid phenotype on ultrasonography, dominated by widespread microcalcifications rather than a discrete mass. Second, the cohort exhibited a high regional nodal disease burden, with universal central compartment metastasis and a substantial prevalence of lateral neck involvement. Third, despite an intensive postoperative strategy—stringent TSH suppression (TSH <0.1 mIU/L) combined with scheduled radioiodine therapy—ipsilateral lateral neck nodal recurrence occurred in 40% of patients, underscoring the need for meticulous lateral neck assessment and sustained imaging-based surveillance in DSVPTC.
Clinical Phenotype, Putative Risk Factors, and Inflammatory Background
DSVPTC is an uncommon histologic subtype of papillary thyroid carcinoma (PTC), and its pathogenesis remains incompletely defined. Prior studies have suggested an association with high-dose radiation exposure,8 yet none of our patients reported a clear history of radiation exposure, indicating that radiation is not a prerequisite for disease occurrence. DSVPTC has been described as occurring more commonly in younger females and frequently coexisting with autoimmune thyroid disease and elevated thyroid autoantibodies. In our cohort, Hashimoto’s thyroiditis was present in 80% (4/5), which is notably higher than the rates reported in previous studies (typically 20–40%).9,10 This finding supports the concept that DSVPTC frequently develops within an immune-activated thyroid microenvironment. The persistent lymphoid infiltration and chronic inflammation in Hashimoto’s thyroiditis may contribute to epithelial-mesenchymal transition and tumor development through various cytokine pathways. This high coexistence rate also has important clinical implications: (1) diffuse echotexture changes may delay DSVPTC diagnosis; (2) Tg monitoring may be unreliable in these patients due to interfering antibodies; and (3) imaging-based surveillance becomes particularly important.
Imaging Hallmarks and the Diagnostic Challenge
A key diagnostic challenge of DSVPTC is its frequent departure from the classic nodule-forming presentation of conventional PTC. In our series, no patient had a discrete dominant thyroid nodule on ultrasonography, whereas diffuse microcalcifications were present in 100%, consistent with the classic “snowstorm” appearance.4,5 These findings have direct clinical implications: diffuse echotexture alteration and microcalcifications may be misattributed to benign inflammatory disease, especially when Hashimoto’s thyroiditis is present, resulting in under-recognition or delayed diagnosis. Therefore, when diffuse microcalcifications coexist with abnormal cervical lymph nodes, DSVPTC should be strongly considered.
Cytology and Molecular Testing
Fine-needle aspiration cytology (FNAC) is widely used for thyroid malignancy assessment; however, DSVPTC poses unique challenges because the lesion is often diffuse and non-mass-forming. Target selection is therefore crucial. In our cohort, thyroid FNAC was performed in 80% (4/5) and uniformly resulted in Bethesda VI, supporting the value of targeted sampling in clinically suspected cases. Given the high nodal metastatic propensity of DSVPTC, concurrent FNAC of suspicious lymph nodes can further improve staging accuracy and inform surgical planning.
Molecular findings in our series (RET alteration in one tested case and BRAF V600E in two) highlight potential molecular heterogeneity in DSVPTC. While BRAF V600E testing is widely applied in PTC, its diagnostic specificity for DSVPTC may be limited compared with alterations such as RET rearrangements reported in this subtype.11 Clinically, a negative BRAF result should not lower suspicion when the imaging phenotype is highly suggestive; broader multigene testing may be considered to support diagnosis and future risk stratification. However, it should be emphasized that DSVPTC remains a histopathologic diagnosis, and molecular testing does not establish the diagnosis.
Nodal Disease Burden and Surgical Management
DSVPTC is recognized for a high frequency of cervical lymph node metastasis.12 Consistent with this, all patients in our cohort had nodal metastasis, with central compartment involvement in 100% and lateral neck metastasis in 60%. Among those who underwent lateral neck dissection at the index operation, the lateral positivity rate was 100%, supporting the appropriateness of therapeutic lateral dissection when radiologic suspicion is present. Our management strategy followed compartment-oriented principles: routine central neck dissection and selective therapeutic lateral neck dissection, avoiding prophylactic lateral dissection in patients without radiologic evidence of lateral disease to limit surgical morbidity.
Nevertheless, our outcomes emphasize that the lateral compartment remains a critical site for disease control. The observation that recurrence occurred exclusively in the lateral neck (40%, 2/5) suggests that preoperative lateral neck mapping must be particularly rigorous in DSVPTC. High-quality ultrasound with systematic evaluation of lateral levels, selective CT, and cytologic confirmation of suspicious nodes may reduce occult disease and subsequent recurrence.
Comparison with Published Literature
Previous studies have reported that DSVPTC is associated with more aggressive behavior and poorer outcomes compared with conventional PTC.13,14 However, in our small series, no distant metastasis or disease-specific death occurred during follow-up. This favorable outcome may be attributed to several factors: (1) early detection through routine health screening allowed for timely intervention before distant spread occurred; (2) all patients underwent total thyroidectomy with comprehensive central and therapeutic lateral neck dissection; (3) stringent TSH suppression was maintained in all patients; (4) standardized radioiodine therapy was administered to all patients; and (5) close imaging-based surveillance (every 6 months) enabled early detection and timely salvage treatment of recurrence. These factors may explain the discrepancy between our findings and reports of worse prognosis in DSVPTC.
Limitations
This study is limited by its small sample size and single-center retrospective design, precluding inferential statistics and limiting generalizability. Molecular testing was performed in only 3 of 5 patients because this test was not available at our institution’s pathology department during the treatment period for the other 2 patients. Biochemical monitoring (Tg) was constrained in those with autoimmune thyroiditis due to interfering antibodies. Larger multicenter cohorts with standardized imaging, surgical, molecular, and follow-up protocols are warranted to refine risk stratification and optimize lateral neck management in DSVPTC.
Conclusions
In this small series of five patients, DSVPTC commonly presented with a diffuse, nodule-negative ultrasonographic phenotype characterized by widespread microcalcifications and was commonly associated with autoimmune thyroiditis. The subtype carried a high burden of cervical nodal disease, particularly in the central compartment, with frequent lateral neck involvement. Even with stringent TSH suppression and scheduled radioiodine therapy, ipsilateral lateral neck nodal recurrence occurred in 40% of patients. Meticulous preoperative lateral neck evaluation, compartment-oriented surgery, and long-term imaging-based surveillance with cytologic confirmation of suspicious nodes remain essential.
Abbreviations
AHNS, American Head and Neck Society; CK19, Cytokeratin 19; DSVPTC, Diffuse sclerosing variant papillary thyroid carcinoma; FNA, Fine-needle aspiration; FNAC, Fine-needle aspiration cytology; I-131, Iodine-131 (radioiodine); IHC, Immunohistochemistry; MAPK, Mitogen-activated protein kinase; PTC, Papillary thyroid carcinoma; RET, Rearranged during transfection; Tg/TG, Thyroglobulin (Tg typically for serum marker; TG for IHC staining); TSH, Thyroid-stimulating hormone; TTF-1, Thyroid transcription factor-1; US, Ultrasonography.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request. The transparency in data reporting in accordance with journal requirements.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. All patient data were anonymized, and patient confidentiality was strictly maintained. The study protocol was approved by the Institutional Review Board (IRB) of Zibo Central Hospital. We confirm that all experiments were performed in accordance with relevant guidelines and regulations. The transparency in data reporting and conflict of interest disclosures in accordance with journal requirements. Given the retrospective nature of the study, the requirement for informed consent was waived.
Acknowledgments
XiaoYu Sun and Yanze Liu are co-first authors for this study. We are grateful to all patients and their families for their cooperation and participation. We also thank the clinical staff of Zibo Central Hospital for their assistance with patient management, data collection, and follow-up.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Zhang Y, Ding T, Cheng R, et al. Exploring the molecular features and clinicopathological correlations of diffuse sclerosing papillary thyroid carcinoma. Clin Endocrinol. 2025;103(5):729–11. PMID: 40785448. doi:10.1111/cen.70013
2. Prasad P, Jain S, Chand G. Diffuse sclerosing variant of papillary thyroid carcinoma in an euthyroid 13-year-old girl: a rare thyroid malignancy. J Indian Assoc Pediatr Surg. 2025;30(2):238–240. PMID: 40191475; PMCID: PMC11968041. doi:10.4103/jiaps.jiaps_210_24
3. Cavaco D, Martins AF, Cabrera R, et al. Diffuse sclerosing variant of papillary thyroid carcinoma: outcomes of 33 cases. Eur Thyroid J. 2022;11(1):e210020. PMID: 34981753; PMCID: PMC9142808. doi:10.1530/ETJ-21-0020
4. Kang B, Yu HW, Kong Y, et al. Diagnostic accuracy of preoperative ultrasound in predicting diffuse sclerosing variant papillary thyroid carcinoma: a retrospective diagnostic accuracy study. Ann Surg Treat Res. 2025;109(1):35–43. PMID: 40688265; PMCID: PMC12270920. doi:10.4174/astr.2025.109.1.35
5. Wang Q, Chang Q, Zhang R, et al. Diffuse sclerosing variant of papillary thyroid carcinoma: ultrasonographic and clinicopathological features in children/adolescents and adults. Clin Radiol. 2022;77(5):e356–e362. PMID: 35197192. doi:10.1016/j.crad.2022.01.051
6. Li W, Wang Y, Gao L, et al. Sonographic characteristics of diffuse sclerosing variant of papillary thyroid carcinoma with histopathological correlation: a preliminary study. Orphanet J Rare Dis. 2024;19(1):136. PMID: 38532506; PMCID: PMC10967076. doi:10.1186/s13023-023-02867-3
7. Chou A, Qiu MR, Crayton H, et al. A detailed histologic and molecular assessment of the diffuse sclerosing variant of papillary thyroid carcinoma. Mod Pathol. 2023;36(12):100329. PMID: 37716505. doi:10.1016/j.modpat.2023.100329
8. Yang L, Zhao M, Xiao L, et al. Diffuse sclerosing variant of papillary thyroid carcinoma is related to a poor outcome: a comparison study using propensity score matching. Endocr Pract. 2023;29(10):779–786. PMID: 37169176. doi:10.1016/j.eprac.2023.05.003
9. Crayton H, Wu K, Leong D, et al. Diffuse sclerosing variant papillary thyroid carcinoma has worse survival than classic papillary thyroid carcinoma: a meta-analysis. Endocr Relat Cancer. 2023;30(6):e220348. PMID: 36952650. doi:10.1530/ERC-22-0348
10. Vuong HG, Kondo T, Pham TQ, et al. Prognostic significance of diffuse sclerosing variant papillary thyroid carcinoma: a systematic review and meta-analysis. Eur J Endocrinol. 2017;176(4):433–441. PMID: 28183787. doi:10.1530/EJE-16-0863
11. Baek HJ, Kim DW, Shin GW, et al. Ultrasonographic features of papillary thyroid carcinomas according to their subtypes. Front Endocrinol. 2018;9:223. PMID: 29867759; PMCID: PMC5951938. doi:10.3389/fendo.2018.00223
12. Malandrino P, Russo M, Regalbuto C, et al. Outcome of the diffuse sclerosing variant of papillary thyroid cancer: a meta-analysis. Thyroid. 2016;26(9):1285–1292. PMID: 27349273. doi:10.1089/thy.2016.0168
13. Chereau N, Giudicelli X, Pattou F, et al. Diffuse sclerosing variant of papillary thyroid carcinoma is associated with aggressive histopathological features and a poor outcome: results of a large multicentric study. J Clin Endocrinol Metab. 2016;101(12):4603–4610. PMID: 27626975. doi:10.1210/jc.2016-2341
14. Liu Y, Fu N, Liu H, et al. Risk factors of lymph node metastasis in the diffuse sclerosing variant of papillary thyroid carcinoma compared with conventional papillary thyroidcarcinoma in pediatric populations. Oral Oncol. 2025;160:107120. Erratum in: Oral Oncol. 2025;161:107135. doi:10.1016/j.oraloncology.2024.107135. PMID: 39591694. doi:10.1016/j.oraloncology.2024.107120
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Younger Than 55 Years Old and BRAF V600E Mutation are Risk Factors for Lymph Node Metastasis in Papillary Thyroid Carcinomas ≤1.0 cm but Not in >1.0 cm
Lai Y, Gu Y, Yu M, Deng J
International Journal of General Medicine 2023, 16:1403-1414
Published Date: 19 April 2023
Development of a Clinical-Radiomics Nomogram That Used Contrast-Enhanced Ultrasound Images to Anticipate the Occurrence of Preoperative Cervical Lymph Node Metastasis in Papillary Thyroid Carcinoma Patients
Wei T, Wei W, Ma Q, Shen Z, Lu K, Zhu X
International Journal of General Medicine 2023, 16:3921-3932
Published Date: 29 August 2023
The Association of Pretreatment Systemic Immune Inflammatory Response Index (SII) and Neutrophil-to-Lymphocyte Ratio (NLR) with Lymph Node Metastasis in Patients with Papillary Thyroid Carcinoma
Gu Y, Yu M, Deng J, Lai Y
International Journal of General Medicine 2024, 17:2887-2897
Published Date: 1 July 2024
Preoperative High Level of Circulating Tumor Cells is an Independent Risk Factor for Central Lymph Node Metastasis in Papillary Thyroid Carcinoma with Maximum Lesion Diameter ≤1.0 cm
Yu M, Deng J, Gu Y, Lai Y
International Journal of General Medicine 2024, 17:4907-4916
Published Date: 25 October 2024