Back to Journals » Journal of Inflammation Research » Volume 14
Diet-Related Inflammation is Associated with Major Depressive Disorder in Bahraini Adults: Results of a Case-Control Study Using the Dietary Inflammatory Index
Authors Chen W, Faris AIE ![]() , Bragazzi NL
, Bragazzi NL ![]() , AlGahtani HMS, Saif Z
, AlGahtani HMS, Saif Z ![]() , Jahrami A, Shivappa N, Hebert JR, Jahrami H
, Jahrami A, Shivappa N, Hebert JR, Jahrami H ![]()
Received 16 February 2021
Accepted for publication 26 March 2021
Published 15 April 2021 Volume 2021:14 Pages 1437—1445
DOI https://doi.org/10.2147/JIR.S306315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monika Sharma
Wen Chen,1 Mo’ez Al-Islam E Faris,2 Nicola Luigi Bragazzi,3 Haifa MS AlGahtani,4,5 Zahra Saif,6 Ahmed Jahrami,7 Nitin Shivappa,8,9 James R Hebert,8,9 Haitham Jahrami4,6
1Department of Psychiatry, Xiamen Xianyue Hospital, Xiamen, 361000, People’s Republic of China; 2Department of Clinical Nutrition and Dietetics, College of Health Sciences/Research Institute for Medical and Health Sciences (RIMHS), University of Sharjah, Sharjah, United Arab Emirates; 3Laboratory for Industrial and Applied Mathematics (LIAM), Department of Mathematics and Statistics, York University, Toronto, ON, Canada; 4College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain; 5Renewal and Reward Center, Dammam, Saudi Arabia; 6Ministry of Health, Manama, Bahrain; 7Bahraini Association for Intellectual Disabilities and Autism, Sanad, Bahrain; 8Cancer Prevention and Control Program, University of South Carolina, Columbia, SC, 29208, USA; 9Department of Epidemiology and Biostatistics, Arnold School of Public Health, University of South Carolina, Columbia, SC, USA
Correspondence: Haitham Jahrami
Ministry of Health, PO Box 12, Manama, Bahrain
Tel +973 17286334
Fax +973 17286335
Email [email protected]
Purpose: This case-control study aimed to examine the association between the inflammation potential of the diet and depression.
Patients and Methods: Ninety-six patients with major depression disorder were matched with 96 age- and sex-matched healthy controls. Energy-adjusted DII (E-DIITM) scores were calculated based on the participants’ responses to a detailed nutritional assessment using a quantitative food frequency questionnaire. Descriptive results were reported. Logistic regression was used to estimate odds ratios and 95% confidence intervals associated with E-DII scores and depression adjusting for covariates including age, sex, body mass index, comorbidities, level of education, and employment.
Results: The mean E-DII score of participants in the study was 1.32± 1.08, indicating a generally pro-inflammatory diet. Patients with depression had elevated E-DII scores compared to age- and sex-matched controls with E-DII scores of 1.72± 1.09 vs 0.90± 0.90, respectively (P=0.001). Results of logistic regression analysis revealed that patients with depression were nearly three times more likely to be in the extreme ends of pro-inflammatory diet (OR 2.75; 95% CI 1.82– 4.15).
Conclusion: Adult Bahraini patients with depression have higher dietary inflammation potential compared to the general population controls. Further research is needed to confirm these results and provide effective interventions to reduce the burden of this dietary inflammation.
Keywords: inflammation, depression, case-control study, mental health, Arabian population groups
Introduction
Worldwide, psychiatric disorders including depression are among the most common forms of noncommunicable diseases (NCDs) with significant etiologic factors of death, comprising 14.3% of global deaths. This is reflected in about 8 million deaths each year, with a potential life loss of a median of 10 years.1 Several recent systematic reviews and meta-analyses examined the association between low-grade inflammation, depression, and risk of mortality.2–4 Results of these reviews suggest that a substantial association between excess mortality and depression was found in a review of 293 analyses including 135,007 depressed and about 1.7 million non-depressed subjects distributed over 35 countries.5 This increased risk of mortality is associated with depression and depressive symptoms in subclinical populations.6
Furthermore, a meta-analysis of data from 21 published articles from 10 countries involving more than 117,000 participants revealed that dietary behaviors involving high intakes of olive oil, whole grains, vegetables, fruits, low-fat dairy, antioxidants, and fish, and accompanied with low intakes of animal foods were associated with a reduced incidence of depression. By contrast, a dietary behavior of excessive consumption of red meats, refined grains, sweets, butter, potatoes, high-fat dairy products, and high-fat gravies, and accompanied with low intakes of vegetables and fruits is linked with an increased risk of having depression.7 More than one meta-analysis indicated that the increased risk of mortality attributed to CVD, cancer, and chronic obstructive pulmonary disease among people with severe mental illness is associated with excessive intakes of inflammation-triggering processed foods.8,9 As with other chronic diseases, the role of inflammatory processes in the pathophysiology of mental health disorders is well established.10–12 This association between inflammation and mental ailments is described as a bidirectional comorbid relationship, meaning that increased bodily inflammation is associated with increased risk of developing the mental problem (such as depression), while depression itself is associated with increased inflammation-triggering behaviors such as unhealthy eating patterns and smoking or drug addiction.13 These findings are consistent with the observation that C-reactive protein (CRP) predicted future depression.13 Psychotropic medications are essential components in the management of severe mental illnesses.14 However, many of these medications are associated with undesirable side effects including obesity and weight gain, and, concomitantly, the progression of metabolic disorders.14
The Dietary Inflammatory Index (DII®) is a standardized scoring algorithm developed to quantify the overall effect of diet on bodily inflammatory status.15 The energy-adjusted DII (E-DIITM)] was developed to account for the strong negative correlation between the DII and total energy intake observed in many populations.16 Both the DII and the E-DII are designed to assess the quality of diet stand on its ability to trigger bodily inflammation, by assessing the intakes of different essential nutrients and commonly consumed bioactive phytochemicals. Other than that total energy consumed is in the denominator of the E-DII, the DII and E-DII are scored similarly and scaled identically; so, the scores are comparable across studies. The DII/E-DII were both developed based on the published literature related to a group of inflammatory markers related to dietary factors, namely TNF-α, CRP, IL-1β, IL-6, IL-4, and IL-10.15 While an elevated DII/E-DII score reflects an elevated intake of pro-inflammatory foods, lower DII scores indicate an anti-inflammatory diet.15,16 The DII/E-DII has been validated against a list of inflammatory markers including CRP, TNF-α, IL-6, homocysteine.16–19 High DII/E-DII scores have been reported to be associated with anxiety,20 declined cognitive function,21,22 and severe mental disorders, including depression.8,9,23,24
It is known that differences exist in age and sex concerning the development of depression.25 In addition, it is known that cultural26 and sociodemographic27 factors also influence the development of the disease. Due to the unique sociodemographic and cultural background of the Gulf Cooperation Council (GCC) region of the Middle East, this case-control study was designed to examine the association between the inflammatory potential of diet, as measured by the E-DII, and depression in Bahraini adults.
Patients and Methods
TheStrengthening the Reporting of Observational Studies in Epidemiology statement was used to design and report this study.28 Our sample consisted of two groups; the first group was cases (n=96) with major depression disorder diagnosed according to the International Classification of Diseases version 10 (ICD-10) by a multi-disciplinary psychiatry team in the Psychiatric Hospital in the Kingdom of Bahrain; the second group (n=96) was age- and sex-matched healthy controls recruited from local health centers during non-emergency visits. The sample of depression cases was selected by simple random sampling from the case registry of the study site. Recruitment occurred in the out-patient department of the Psychiatric Hospital/Bahrain.
Data were collected in the year 2019 between the months of March and December. Inclusion criteria included: out-patients diagnosed with depression, both sex, adults (20–60 years), able to provide consent, and willing to participate in the research. Exclusion criteria were: those with serious medical comorbidity (cancer, motor neuron diseases, and chronic kidney disease), patients with depression with a psychiatric morbidity, pregnant women, those who are involved in other experimental controls. We projected that a sample of 70 patients would be needed for case-control analysis based on previous similar research29 that suggested the patients with serious mental illness are twofold (odd ratio=2.0) more likely to be in the extreme end of pro-inflammatory diet. Sample size calculation included the following assumptions α=5%, β=20% (corresponding to power of 80%). To further increase the power, we aimed to include about 100 patients per arm.
Research ethical approval was obtained from the Research Ethics Committee, Ministry of Health, Kingdom of Bahrain (No. Year 2018/CC REC/ID EF023). Written informed consent was secured from all participants before data collection. The study followed the declaration of Helsinki ethical principles for medical research involving human subjects.
Data were collected during a clinical interview and involved the following assessments: demographics, anthropometrics (weight and height), detailed assessment of dietary habits and other lifestyle factors and assessment of depressive symptoms for patients with depression using a psychometric scale by a qualified research assistant. Based on weight and height, body mass index (BMI= weight (kg)/height(m)2) was calculated. The BMI was then categorized as per the World Health Organization categories of underweight, normal, overweight, or obese.30 The Mosteller formula was used to compute body surface area (BSA).31 Total body water (TBW) in liters, body fat percent (BFP) in percentage, lean mass (LM) in kilograms, and fat mass (FM) in kilograms were estimated using bioelectrical impedance analysis device.
Assessment of dietary habits was performed using a validated food frequency questionnaire (FFQ), with Cronbach alpha and McDonald omega of >0.9,32,33 a complete description of the FFQ is published elsewhere.29,32,33 To further standardize data collection models were used to determine a standard unit for portions. Briefly, the FFQ assessed food consumption of five main food groups categorized into 32 items during the past 4 weeks. Recent systematic review and meta-analysis showed that the use of FFQs (typically the past month) is robust approach in nutritional epidemiological studies.34
Dietary analysis of the FFQ was performed using dietary software ESHA’s Food Processor® nutrition analysis software and DII/E-DII were subsequently computed. We used the food parameters included in the DII/E-DII that consist of up to 45 items. In this study 29 parameters were available. The pro-inflammatory food parameters were 8 items: B12 (Cobalamin)(mcg), Carbohydrates (g), Cholesterol (mg), Energy (Kcal), Fats (g), Protein (g), SFA (g), and Trans-fats (g). The anti-inflammatory food parameters were 21 items: Alcohol (g), B1 (Thiamin) (mg), B2 (Riboflavin) (mg), B3 (Niacin) (mg), B6 (Pyridoxine) (mg), Caffeine (mg), Fibers (g), Folic acid (µg), Iron (mg), Magnesium (mg), MUFA (g), Omega-3 (g), Omega-6 (g), PUFA (g), Selenium (µg), Vitamin A (IU), Vitamin C (mg), Vitamin D (IU), Vitamin E (mg), Zinc (mg), and β-carotene (µg).
The individual intakes of food item parameters that constitute the DII are compared to a world-wide standard database. Detailed description of the DII and calculation algorithm is available elsewhere.15 Briefly, to estimate DII for the participants of this study, the data on food intakes were obtained from the FFQ. Then, the following steps were used: First, the intake of food data is related to the regionally representative world database that offered a strong estimate of a mean and standard deviation for each food parameter. Second, Z-score normalization was used using the standard Z-score formula to estimate each participant’s exposure in reference to the global mean. Third, the Z-scores were converted to proportions to reduce the effect of skewing to the right. Fourth, these proportions were multiplied by 2 and then 1 was subtracted to achieve a normal distribution with values centered on 0 (null) and bounded between −1 (maximally anti-inflammatory) and +1 (maximally pro-inflammatory). Fifth, the centered proportion value for each food item was then multiplied by its respective parameter-specific inflammatory effect score to obtain the parameter-specific DII score. Sixth, all of the food parameters-specific DII scores were summed to compute the overall DII score.
Using a method identical to that employed for the DII, but using amounts of foods consumed per 1000 kcal/day, energy-adjusted DII (E-DIITM) scores were derived for each participant in this study. Calculating E-DII scores entailed using a specially constructed referent database of energy-adjusted parameter-specific scores on the basis of data from the same countries used to compute the DII. Further details on E-DII are available elsewhere.16
Participants were categorized into tertiles based on E-DII scores. Tertiles of E-DII scores were calculated based on the distribution of E-DII scores among controls: according to the following ranges Tertile 1 ≤0.59, Tertile 2 0.60 to 1.20, and Tertile 3 ≥1.21. Tertile 3 is the most pro-inflammatory.
The Beck Depression Inventory II (BDI-II) was used to estimate depressive symptoms. Scores were computed and classified into 0–13 (minimal range - no sign of depression), 14–19 (mild depression), 20–28 (moderate depression), and 29–63 indicate severe depression.35
Data were checked for normality using visualization and formally using Shapiro–Wilk test before beginning the analyses. For continuous variables, the means and standard deviations are reported, and for categorical variables, counts and percentages are reported. To compare the two independent groups, the independent sample t-test was used for continuous variables and Chi-square was used for categorical variables. Multinomial logistic regression analysis was performed to assess the effect of the E-DII on depression as the outcome variable. E-DII scores were fit as tertiles. Models were adjusted for age, sex, body mass index, comorbidities, level of education, and employment. E-DII as continuous score also was used in linear multiple regression analysis adjusting for the same covariates. The E-DII was chosen in place of the DII because it produced better goodness of fit statistics. E-DII was used for all subsequent analyses because it takes into the account the total energy consumed per participants.
All data analytics were performed using STATA 16.0 software; significant P value was set at 0.05.
Results
Table 1 represents anthropometric, socio-demographic, and health markers for both cases and controls. Cases and controls did not exhibit significant differences concerning age and anthropometric measurements. Nonetheless, cases with depression were more likely, but not significantly, to be obese (37.5% vs 26.0%), physically inactive (67.7% vs 49%), currently, smokers (37.2% vs 10.4%), less educated, and have significantly higher rates of comorbidity with type 2 diabetes mellitus (27.1% vs 7.3%), and hypertension (28.1% vs 11.5%). Moreover, cases presented lower socioeconomic status based on their lower education levels and being more likely to be single and unemployed.
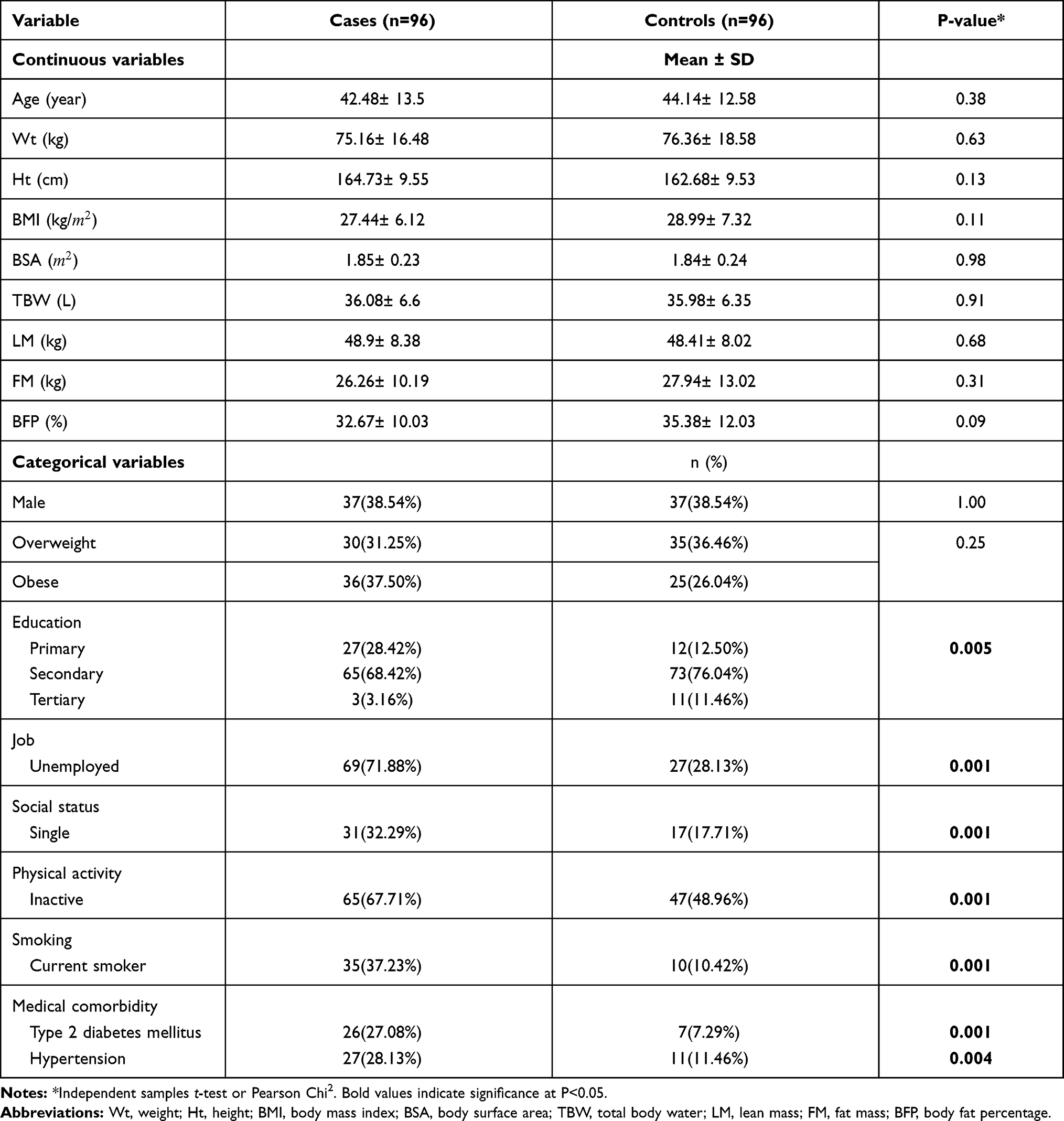 |
Table 1 Anthropometric and Sociodemographic Characteristics of Cases with Depression and Their Counterpart Healthy Controls |
Supplemental Table 1 describes the distribution of anthropometric, sociodemographic, and health indicators characteristics across tertiles of E-DII for the control participants, while Supplemental Table 2 describes the distribution of the same characteristics across tertiles of E-DII for cases with depression. According to Supplemental Table 1, controls were slightly trending towards the pro-inflammatory direction. For the patients with depression (Supplemental Table 2), more than 50% of the patients were in Tertile 3. The characteristics of patients in Tertile 3 included being more obese; active smoker, less physically active, and having a higher prevalence of medical comorbidities specifically muscular and joints diseases.
The overall E-DII for all of the participants in this study was 1.32±1.08. Table 2 shows that cases with depression had a statistically significant E-DII compared to matched controls; 1.72±1.09 and 0.90±0.90, respectively. Table 2 also shows the difference in dietary intake between cases and control participants. Cases with depression showed significantly (P<0.05) higher intakes of calories, saturated fats, total fats, mono, and poly-unsaturated fats, dietary cholesterol, protein, β-carotene, riboflavin (B2), vitamin E, sodium, iron, zinc, and overall normal and E-DII, while reported fewer intakes from caffeine and vitamin C.
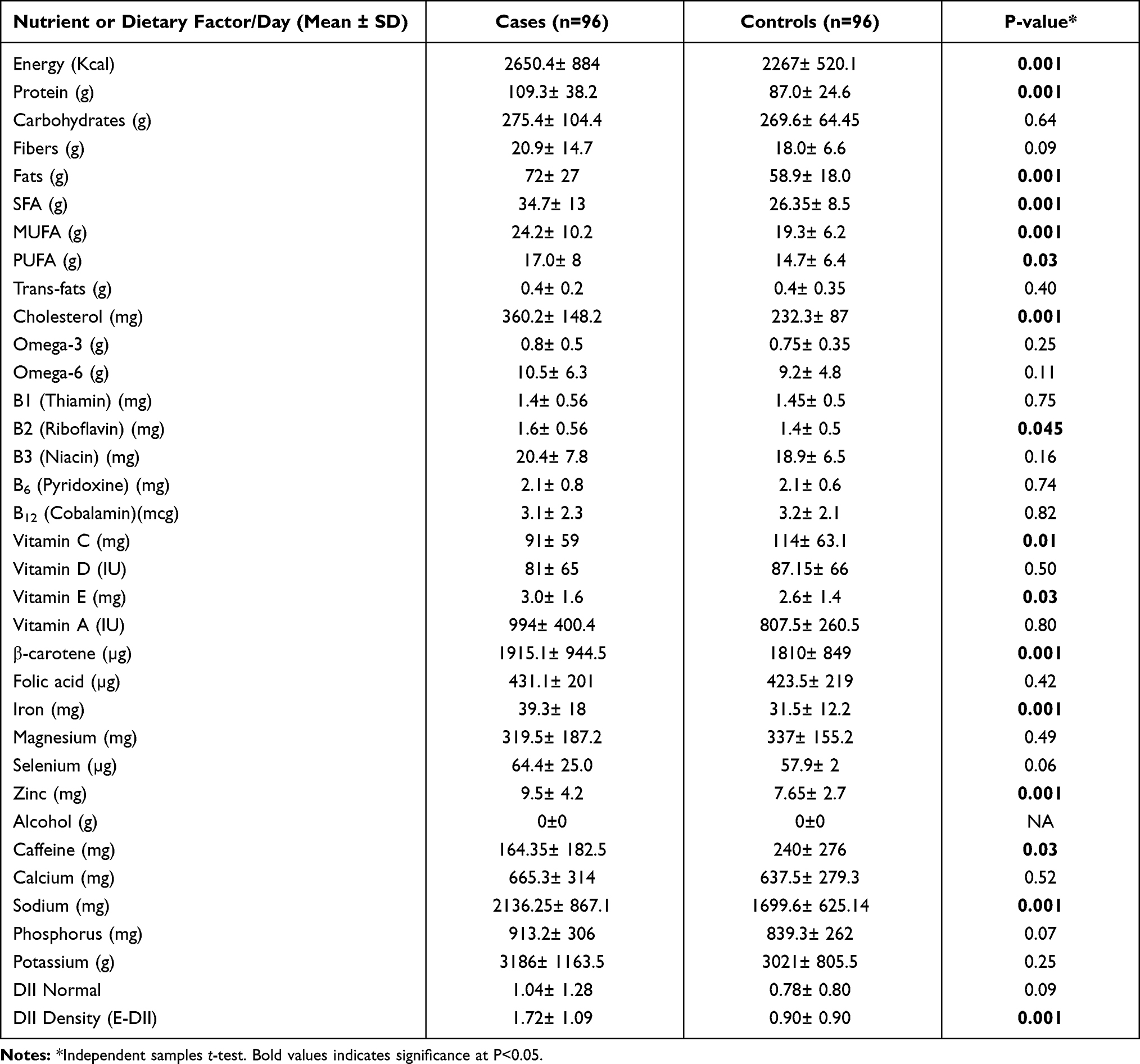 |
Table 2 Distribution of Dietary Factors, Nutrients, and Energy-Adjusted Dietary Inflammatory Index (E-DII) for Cases and Control Subjects |
As shown in Supplemental Table 3, most pro- and anti-inflammatory nutrients or food components decreased linearly across the tertiles of E-DII for controls. Unexpectedly, the same trend was shown for the dietary intakes for both pro-and anti-inflammatory dietary factors and food components for the cases with depression across the tertiles of the E-DII (Supplemental Table 4). However, this trend is reversed across the tertiles of E-DII depression cases categorized by depression severity according to BDI-2 (Supplemental Table 5). As shown in Supplemental Table 5, energy, carbohydrates, protein, fats, saturated fats, and cholesterol were the most pro-inflammatory food components. Folic acid fiber, carotene, vitamins C, and A, Mg, and Zn were the anti-inflammatory components that decreased across tertiles. Subjects in the fourth quartile reported higher consumption for the pro-inflammatory components such as protein, energy, fat carbohydrates, PUFA, MUFA saturated fat, trans-fat, cholesterol, omega-6 FAs, and niacin.
Table 3 shows the proportion (and ratio) of patients and cases in each tertile, the ORs and 95% CIs for depression status according to tertiles of E-DII. When E-DII was expressed as tertiles, results obtained from modeling E-DII as a continuous variable about depression indicated a direct association, with participants in the most pro-inflammatory group (Tertile 3) being almost three times more likely to be depressed than participants in the most anti-inflammatory group (Tertile 1) (OR 2.75; 1.82–4.15; P-trend=0.01).
 |
Table 3 Odds Ratios (OR) and Confidence Intervals for Tertiles of Energy-Adjusted Dietary Inflammatory Index (E-DII) (and E-DII as Continuous) Associated with the Diet of Patients with Depression |
Discussion
This case-control study tested the inflammatory potential of diet in relation to depression. We found that cases with depression had higher E-DII scores when compared to depression-free controls. The observed association observed in this study between the E-DII and cases of depression suggests that the inflammatory potential of diet plays an important role in depression. The findings of this research are consistent with those of the available four case-control studies on the relationship between dietary behaviors and depression among adolescents and adults in Korea,36 Iran,37,38 and China.39 It also falls in line with results from three meta-analyses.40–42
The observed significant association between E-DII and depression in the current study broadly supports a relevant study conducted on 254 patients with depression in the UK who were found to have higher DII/E-DII scores in comparison with their disease-free controls (after adjusting for total energy intake, sex, and age).9 Other reports found that patients with depression have elevated levels of dietary inflammation and were more likely to exhibit profoundly worse physical health indicators than other classes of severe mental illness.43
This is the first observational study in the GCC region of the Middle East investigating the association between depression and DII/E-DII as a representative indicator of the inflammatory potential of diet. Other studies on depression explored various aspects related to the inflammation–depression relationship. It is important to note that depression is an inflammation-related mental disorder.44
The two-way relationship between mental disorders, including depression, and inflammation is well established. While neuropsychiatric disorders (eg, depression) promote inflammatory reactions; inflammation promotes neuropsychiatric disorders including depression.44 It has been repeatedly reported that neuropsychiatric disorders patients demonstrate all classical characteristics of inflammation. Pro-inflammatory cytokines regulate cognition and mood behavior by lowering brain monoamine levels, inhibiting neuroendocrine responses, promoting excitotoxicity.44 Changes in neuroendocrine regulation,45 metabolism,46 and diet/microbiota47 are the main triggering factors that account for inflammation and predispose to developing depression. Additionally, recent reports indicate that stress in early life is associated with elevated inflammation before the progression to neuropsychiatric disorders such as depression.46
Our findings are consistent with the hypothesis that increasing the consumption of low-DII, anti-inflammatory foods and reducing the intake of high-DII, pro-inflammatory dietary components would decrease the risk of depression and could serve as the basis for an effective supportive therapy for patients with depression.47,48 It is important to note that nutrients involved in the calculation of DII/E-DII are essential for promoting neuroplasticity which is essential for enhancing healthy brain function, and, thereby, hindering its severity in diagnosed patients or delaying the progression of depression.49 These nutrients include vitamin D, vitamin E, B vitamins (B6, B12, folate), omega-3 polyunsaturated fatty acids, and carotenoids.49
Our findings are reinforced by the findings of cross-sectional studies reporting that subjects with severe mental illnesses, particularly depression, consume fewer anti-inflammatory nutrients and more pro-inflammatory foods than the general population.8,9 Our findings are also consistent with accumulating evidence on the relationship between diet-associated inflammation and depression18–25 and is reflected in 3 meta-analyses40–42 exploring the relationship between diet-induced inflammation and depression. The pathogenesis of psychiatric disorders, including depressive symptoms, is directly influenced by environmental factors, with dietary behaviors having been shown to regulate the inflammatory state; thus, signifying their potential role both as or etiologic factor and as a potential therapeutic tool in disorders with an inflammatory basis.9,20,50,51 Indeed, recent review highlights that diet-associated inflammation may be linked with severe mental ailments, including depression.8
This case-control study design, which permits for a relatively large sample size, resulting in the ability to control for variable covariates and having relatively high statistical power represents one strong point of the current work. Besides, the use of DII/E-DII as a research tool allowed to study the overall diet rather than focusing on individual dietary components. Third, the E-DII score was calculated using data from a food frequency questionnaire that was specifically tailored to cover the broad range of diets in Bahrain. However, more than one limitation should be considered when interpreting the findings of the current work. These include the increased likelihood of both information and selection biases. The lack of validation for DII with inflammatory markers in this study also is a limitation to be considered.
To deepen understanding of the mechanisms of action, future research should include follow-up studies that examine both dietary inflammatory potential and inflammatory cytokines measured in biosamples of individuals with and without depression. The effectiveness of an anti-inflammatory diet should be tested in suitable experimental trials including randomized controlled clinical trials and pragmatic/adaptive trials, as appropriate.
Conclusions
This case-control study conducted among Bahraini adults showed that cases with depression had higher dietary inflammation potential, as estimated by the E-DII, compared to depression-free controls. Further research is needed to confirm these results and provide effective interventions to reduce the burden of this dietary inflammation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Dr. James R. Hébert owns controlling interest in Connecting Health Innovations LLC (CHI), a company that has licensed the right to his invention of the dietary inflammatory index (DII®) from the University of South Carolina in order to develop computer and smart phone applications for patient counseling and dietary intervention in clinical settings. Dr. Nitin Shivappa is an employee of CHI and also reports non-financial support from Connecting Health Innovations. The subject matter of this paper will not have any direct bearing on that work, nor has that activity exerted any influence on this project. The authors report no other conflicts of interest in this work.
References
1. Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications. JAMA Psychiatry. 2015;72(4):334. doi:10.1001/jamapsychiatry.2014.2502
2. Osimo EF, Baxter LJ, Lewis G, Jones PB, Khandaker GM. Prevalence of low-grade inflammation in depression: a systematic review and meta-analysis of CRP levels. Psychol Med. 2019;49(12):1958–1970. doi:10.1017/S0033291719001454
3. Osimo EF, Pillinger T, Rodriguez IM, Khandaker GM, Pariante CM, Howes OD. Inflammatory markers in depression: a meta-analysis of mean differences and variability in 5166 patients and 5083 controls. Brain Behav Immun. 2020;87:901–909. doi:10.1016/j.bbi.2020.02.010
4. Yuan N, Chen Y, Xia Y, Dai J, Liu C. Inflammation-related biomarkers in major psychiatric disorders: a cross-disorder assessment of reproducibility and specificity in 43 meta-analyses. Transl Psychiatry. 2019;9(1):233. doi:10.1038/s41398-019-0570-y
5. Cuijpers P, Vogelzangs N, Twisk J, Kleiboer A, Li J, Penninx BW. Comprehensive meta-analysis of excess mortality in depression in the general community versus patients with specific illnesses. Am J Psychiatry. 2014;171(4):453–462. doi:10.1176/appi.ajp.2013.13030325
6. Cuijpers P, Smit F. Excess mortality in depression: a meta-analysis of community studies. J Affect Disord. 2002;72(3):227–236. doi:10.1016/s0165-0327(01)00413-x
7. Li Y, Lv M-R, Wei Y-J, et al. Dietary patterns and depression risk: a meta-analysis. Psychiatry Res. 2017;253:373–382. doi:10.1016/j.psychres.2017.04.020
8. Teasdale SB, Ward PB, Samaras K, et al. Dietary intake of people with severe mental illness: systematic review and meta-analysis. Br J Psychiatry. 2019:1–9. doi:10.1192/bjp.2019.20.
9. Firth J, Stubbs B, Teasdale SB, et al. Diet as a hot topic in psychiatry: a population-scale study of nutritional intake and inflammatory potential in severe mental illness. World Psychiatry. 2018;17(3):365–367. doi:10.1002/wps.20571
10. Hong H, Kim BS, Im H-I. Pathophysiological role of neuroinflammation in neurodegenerative diseases and psychiatric disorders. Int Neurourol J. 2016;20(Suppl 1):S2. doi:10.5213/inj.1632604.302
11. Müller N. The role of anti-inflammatory treatment in psychiatric disorders. Psychiatr Danub. 2013;25(3):0–298.
12. Najjar S, Pearlman DM, Alper K, Najjar A, Devinsky O. Neuroinflammation and psychiatric illness. J Neuroinflammation. 2013;10(1):43. doi:10.1186/1742-2094-10-43
13. Mac Giollabhui N, Ng TH, Ellman LM, Alloy LB. The longitudinal associations of inflammatory biomarkers and depression revisited: systematic review, meta-analysis, and meta-regression. Mol Psychiatry. 2020. doi:10.1038/s41380-020-00867-4
14. Tayem YI, Jahrami HA, Ali MK, Hattab SW. Ambulatory pharmacotherapy of five psychiatric disorders in Bahrain: a Descriptive Study. Psychiatr Q. 2020;91(2):289–298. doi:10.1007/s11126-019-09705-5
15. Shivappa N, Steck SE, Hurley TG, Hussey JR, Hebert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–1696. doi:10.1017/S1368980013002115
16. Hebert JR, Shivappa N, Wirth MD, Hussey JR, Hurley TG. Perspective: the Dietary Inflammatory Index (DII)-lessons learned, improvements made, and future directions. Adv Nutr. 2019;10(2):185–195. doi:10.1093/advances/nmy071
17. Wirth MD, Shivappa N, Davis L, et al. Construct validation of the dietary inflammatory index among African Americans. J Nutr Health Aging. 2017;21(5):487–491. doi:10.1007/s12603-016-0775-1
18. Vahid F, Shivappa N, Faghfoori Z, et al. Validation of a dietary inflammatory index (DII) and association with risk of gastric cancer: a case-control study. Asian Pac J Cancer Prev. 2018;19(6):1471.
19. Vahid F, Shivappa N, Hekmatdoost A, Hebert JR, Davoodi SH, Sadeghi M. Association between Maternal Dietary Inflammatory Index (DII) and abortion in Iranian women and validation of DII with serum concentration of inflammatory factors: Case-Control Study. Appl Physiol Nutr Metab. 2017;42(5):511–516. doi:10.1139/apnm-2016-0274
20. Phillips CM, Shivappa N, Hébert JR, Perry IJ. Dietary inflammatory index and mental health: a cross-sectional analysis of the relationship with depressive symptoms, anxiety and well-being in adults. Clin Nutr. 2018;37(5):1485–1491. doi:10.1016/j.clnu.2017.08.029
21. Shin D, Kwon SC, Kim MH, et al. Inflammatory potential of diet is associated with cognitive function in an older adult Korean population. Nutrition. 2018;55–56:56–62. doi:10.1016/j.nut.2018.02.026
22. Hayden KM, Beavers DP, Steck SE, et al. The association between an inflammatory diet and global cognitive function and incident dementia in older women: the Women’s Health Initiative Memory Study. Alzheimers Dement. 2017;13(11):1187–1196. doi:10.1016/j.jalz.2017.04.004
23. Shivappa N, Hebert JR, Veronese N, et al. The relationship between the dietary inflammatory index (DII((R))) and incident depressive symptoms: a longitudinal cohort study. J Affect Disord. 2018;235:39–44. doi:10.1016/j.jad.2018.04.014
24. Shivappa N, Hebert JR, Neshatbini Tehrani A, et al. Is associated with an increased odds of depression symptoms among Iranian female adolescents: a Cross-Sectional Study. Front Psychiatry. 2018;9:400. doi:10.3389/fpsyt.2018.00400
25. Zavaglia E, Bergeron L. Systematic review of comorbidity between DSM disorders and depression according to age and sex in youth. Can Psychol. 2017;58(2):124. doi:10.1037/cap0000085
26. Kessler RC, Bromet EJ. The epidemiology of depression across cultures. Annu Rev Public Health. 2013;34(1):119–138. doi:10.1146/annurev-publhealth-031912-114409
27. Akhtar-Danesh N, Landeen J. Relation between depression and sociodemographic factors. Int J Ment Health Syst. 2007;1(1):4. doi:10.1186/1752-4458-1-4
28. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
29. Jahrami HA, Faris M-IE, Saif ZQ, Hammad LH. Assessing dietary and lifestyle risk factors and their associations with disease comorbidities among patients with schizophrenia: a Case–Control Study from Bahrain. Asian J Psychiatr. 2017;28:115–123. doi:10.1016/j.ajp.2017.03.036
30. World Health Organization. Body mass index – BMI; 2020. Available from: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi#:~:text=BMI%2C%20formerly%20called%20the%20Quetelet,have%20a%20BMI%20of%2022.9.
31. Redlarski G, Palkowski A, Krawczuk M. Body surface area formulae: an alarming ambiguity. Sci Rep. 2016;6(1):27966. doi:10.1038/srep27966
32. Jahrami H, Alekri E, BaHammam AS, et al. The association between micronutrient status and sleep quality in patients with depression: a case-control study. Sleep Breath. 2020. doi:10.1007/s11325-020-02228-5
33. Jahrami H, Bragazzi NL, Grant WB, et al. Vitamin D doses from solar ultraviolet and dietary intakes in patients with depression: results of a Case-Control Study. Nutrients. 2020;12(9):2587. doi:10.3390/nu12092587
34. Cui Q, Xia Y, Wu Q, Chang Q, Niu K, Zhao Y. A meta-analysis of the reproducibility of food frequency questionnaires in nutritional epidemiological studies. Int J Behav Nutr Phys Act. 2021;18(1):12. doi:10.1186/s12966-020-01078-4
35. Smarr KL, Keefer AL. Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire‐9 (PHQ‐9)†. Arthritis Care Res. 2011;63(S11):S454–S466. doi:10.1002/acr.20556
36. Kim T-H, Choi J-Y, Lee H-H, Park Y. Associations between dietary pattern and depression in Korean adolescent girls. J Pediatr Adolesc Gynecol. 2015;28(6):533–537. doi:10.1016/j.jpag.2015.04.005
37. Khosravi M, Sotoudeh G, Majdzadeh R, et al. Healthy and unhealthy dietary patterns are related to depression: a Case-Control Study. Psychiatry Investig. 2015;12(4):434. doi:10.4306/pi.2015.12.4.434
38. Rashidkhani B, Gargari BP, Ranjbar F, Zareiy S, Kargarnovin Z. Dietary patterns and anthropometric indices among Iranian women with major depressive disorder. Psychiatry Res. 2013;210(1):115–120. doi:10.1016/j.psychres.2013.05.022
39. Xia Y, Wang N, Yu B, et al. Dietary patterns are associated with depressive symptoms among Chinese adults: a Case–Control Study with propensity score matching. Eur J Nutr. 2017;56(8):2577–2587. doi:10.1007/s00394-016-1293-y
40. Wang J, Zhou Y, Chen K, et al. Dietary inflammatory index and depression: a meta-analysis. Public Health Nutr. 2019;22(4):654–660. doi:10.1017/S1368980018002628
41. Lassale C, Batty GD, Baghdadli A, et al. Healthy dietary indices and risk of depressive outcomes: a systematic review and meta-analysis of observational studies. Mol Psychiatry. 2019;24(7):965–986. doi:10.1038/s41380-018-0237-8
42. Molendijk M, Molero P, Ortuno Sanchez-Pedreno F, Van der Does W, Angel Martinez-Gonzalez M. Diet quality and depression risk: a systematic review and dose-response meta-analysis of prospective studies. J Affect Disord. 2018;226:346–354. doi:10.1016/j.jad.2017.09.022
43. Vancampfort D, Correll CU, Galling B, et al. Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: a systematic review and large scale meta-analysis. World Psychiatry. 2016;15(2):166–174. doi:10.1002/wps.20309
44. Bauer ME, Teixeira AL. Inflammation in psychiatric disorders: what comes first? Ann N Y Acad Sci. 2019;1437(1):57–67. doi:10.1111/nyas.13712
45. Appiah-Kusi E, Leyden E, Parmar S, Mondelli V, McGuire P, Bhattacharyya S. Abnormalities in neuroendocrine stress response in psychosis: the role of endocannabinoids. Psychol Med. 2016;46(1):27–45. doi:10.1017/s0033291715001786
46. Fair DA, Graham AM, Mills B. A role of early life stress on subsequent brain and behavioral development. Wash UJL Poly. 2018;57:89.
47. Huang Q, Liu H, Suzuki K, Ma S, Liu C. Linking what we eat to our mood: a review of diet, dietary antioxidants, and depression. Antioxidants (Basel). 2019;8(9):376. doi:10.3390/antiox8090376
48. Firth J, Marx W, Dash S, et al. The effects of dietary improvement on symptoms of depression and anxiety: a meta-analysis of randomized controlled trials. Psychosom Med. 2019;81(3):265. doi:10.1097/PSY.0000000000000673
49. Mitra S, Natarajan R, Ziedonis D, Fan X. Antioxidant and anti-inflammatory nutrient status, supplementation, and mechanisms in patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2017;78:1–11. doi:10.1016/j.pnpbp.2017.05.005
50. Oddy WH, Allen KL, Trapp GSA, et al. Dietary patterns, body mass index and inflammation: pathways to depression and mental health problems in adolescents. Brain Behav Immun. 2018;69:428–439. doi:10.1016/j.bbi.2018.01.002
51. Bergmans RS, Malecki KM. The association of dietary inflammatory potential with depression and mental well-being among U.S. adults. Prev Med. 2017;99:313–319. doi:10.1016/j.ypmed.2017.03.016
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.