Back to Journals » International Journal of General Medicine » Volume 18
Diaphragm Contraction Pressure Index: A New Forecasting Indicator for Weaning from Mechanical Ventilation
Authors Zhang P, Jiang H, Li Z, Zhou Q, Wu J, Wang M, Wu J ![]() , Jiang X
, Jiang X
Received 24 May 2025
Accepted for publication 21 November 2025
Published 2 December 2025 Volume 2025:18 Pages 7163—7173
DOI https://doi.org/10.2147/IJGM.S542365
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Reynold Panettieri Jr
Peng Zhang,* Haijiao Jiang,* Zheng Li,* Quan Zhou, Jiaofeng Wu, Mengquan Wang, Jingyi Wu, Xiaogan Jiang
Department of Critical Care Medicine, Yijishan Hospital, First Affiliated Hospital of Wannan Medical College, Wuhu, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaogan Jiang, Department of Critical Care Medicine, Yijishan Hospital, First Affiliated Hospital of Wannan Medical College, 2# Zheshan Road, Wuhu, Anhui, 241000, People’s Republic of China, Email [email protected]
Purpose: Failure to wean from mechanical ventilation can lead to prolonged hospital stays, increased incidence of ventilator-associated pneumonia, and higher mortality rates. This study aimed to explore the effectiveness of the diaphragm contraction pressure index (DCPI) in predicting weaning outcomes in patients undergoing mechanical ventilation, providing a scientific basis for successful weaning in clinical practice.
Patients and Methods: This prospective observational study included 286 individuals in the derivation cohort and 104 patients in the validation cohort, all of whom completed the spontaneous breathing trial (SBT). During SBT, ultrasound was used to quantify the right hemidiaphragm excursion (DE), diaphragm thickness (DTF) after inspiration and expiration, and DCPI. MIP values were gathered from the mechanical ventilator when the patients breathed peacefully. The derivation cohort determined the cut-off value of DCPI and compared these ultrasound diaphragm parameters. The validation cohort contributes to verifying the accuracy of DCPI.
Results: The weaning success group’s DCPI in the derivation cohort was significantly higher than that of the weaning failure group (36.67% ± 7.02% vs 24.03% ± 5.78%, P < 0.001). While the area under the receiver operating characteristic curve (ROC) (AUC) of DE, DTF, and MIP was 0.698 (95% CI, 0.615– 0.771, P < 0.001), 0.770 (95% CI, 0.693– 0.837, P < 0.01), and 0.811 (95% CI, 0.737– 0.872, P < 0.001), the ROC of DCPI was 0.954 (95% CI, 0.905– 0.982, P < 0.001), indicating good predictive performance for weaning success. The DCPI had a sensitivity of 94.1% and a specificity of 90.8%, with the ideal cut-off value set at ≥ 30.0%. Similarly, in the validation cohort, the AUC of DCPI for the predicted value is 0.952 (95% CI, 0.854– 0.992, P < 0.001).
Conclusion: Compared with DTF, DE, and MIP, DCPI dramatically improves the accuracy of predicting successful weaning.
Trial Registration: No. ChiCTR2100052470, Registered 28 October 2021.
Keywords: ultrasound, diaphragm, DCPI, predictive performance, mechanical ventilation, weaning
Take Home Message
We developed the diaphragm contraction pressure index (DCPI), a novel sonographic assessment indicator for diaphragm function, for this observational cohort study. The DCPI’s ROC for predicting the effectiveness of weaning off mechanical ventilation was 0.954 (95% CI, 0.905–0.982), higher than the maximal inspiratory pressure, diaphragm thickness, and diaphragm excursion.
Introduction
Although mechanical ventilation rescues plenty of patients with critical illness, difficulties in weaning from that confront 20–30% of patients1–3 which may induce ventilator-associated pneumonia, lengthen the duration in ICU, and increase mortality.4–6 The respiratory muscle dysfunction mainly contributes to the difficulty in weaning, of which the diaphragm frequently takes the central role.7 Hence, the assessment of the diaphragm has been employed to predict the odds of successful weaning.
Compared to the other respiratory muscles, the diaphragm undertakes a dominating workload during the inspiration period.8 The feeble diaphragm consequently compels the other accessory respiratory muscles to do more work, resulting in these muscles’ fast fatigue, shortening the spontaneous breathing persistence time, and even leading to weaning failure.9 Therefore, the proportion of the diaphragm workload during the breathing cycle could be an important indication of the weaning effort. Nevertheless, in the context that the maximum inspiratory pressure (MIP) has been developed to assess the whole endeavor of all respiratory muscles, which represents accurately inspiratory muscle strength,10 the transdiaphragmatic pressure (Pdi), being a potential indicator of the diaphragm work, remains difficult to measure directly at the ICU bedside.11
Recently, transthoracic ultrasound has been increasingly applied in the intensive care setting to assess diaphragmatic function. Measurements of diaphragm thickness during PSV mode have been shown to correlate strongly with Pdi,12 which is considered the gold standard for evaluating diaphragmatic workload. However, direct measurement of Pdi requires invasive procedures such as esophageal and gastric balloon catheter placement, which are technically demanding and not always feasible in critically ill patients. In contrast, ultrasound assessment of diaphragm thickness offers a simple, non-invasive, and reproducible method that can be performed at the bedside. Building upon these findings, we propose the DCPI, a novel parameter derived from changes in diaphragm thickness relative to inspiratory muscle strength. DCPI provides an indirect yet practical representation of the proportion of diaphragmatic work within the overall respiratory muscle effort, thereby offering clinicians a more comprehensive and less invasive tool to predict weaning outcomes.
The objective of this study is to investigate the application value of the Diaphragm Contractile Pressure Index (DCPI) in predicting weaning outcomes in mechanically ventilated patients. By evaluating the predictive performance of DCPI, this study seeks to provide clinicians with a scientific and reliable tool to more accurately assess the likelihood of successful weaning, thereby improving weaning success rates, reducing the incidence of ventilator-associated pneumonia, shortening hospital stays, and lowering patient mortality.
Methods
Study Design
This prospective observational cohort study was conducted in an adult Intensive Care Unit (ICU) of a teaching hospital (Yijishan Hospital, First Affiliated Hospital of Wannan Medical College, Anhui, China). Patients who met the inclusion criteria and underwent SBT between June 2021 and December 2023 were selected as the derivation cohort, and those admitted between January and December 2024 were selected as the validation cohort. The hospital ethics committee approved the study protocol (Approval Number 2018–03), which was registered on chictr.gov (Registration No. ChiCTR2100052470). The participants or their relatives endorsed the informed consent. Two researchers accepted standardized point-of-care ultrasound training before the initiation of the study, which focused on lung and diaphragm ultrasound imaging. The study process was designed into two phases: the derivation section, which determined the cut-off value of DCPI, and the validation section to appraise the prediction performance of DCPI in the appropriate patients. This study was conducted in accordance with the Declaration of Helsinki.
Study Subjects
The study included each participant who completed the spontaneous breathing test (SBT) and had been intubated and ventilated for at least 48 hours. In the derivation cohort, patients were divided into the successful weaning group and the weaning failure group based on the weaning outcomes. However, patients who were younger than 18 years, with diaphragmatic paralysis or who were pregnant, were excluded. The inclusion and exclusion criteria of both section cohorts are the same.
Scheme of Weaning from Ventilation
A senior clinician and a respiratory therapist (RT) decided that the patients should try a spontaneous breathing trial (SBT). The ventilation parameters were as follows: FiO2 was set at 35%, positive end-expiratory pressure (PEEP) was set at 3 cmH2O, pressure support ventilation mode (PSV) was set at 5 cmH2O, and pressure support level (PS) was set at 5 cmH2O. The patient was lying down in a semi-supine position when the diaphragm ultrasound pictures were taken, and MIP was also recorded, following 30 minutes of SBT. Clinicians and respiratory therapists responsible for the patient’s care were unaware of the ultrasonography and MIP measures. The patients who fulfilled the criteria for the tolerance of SBT discontinued from the ventilator and were extubated.13 Failure of the SBT was based on predefined criteria: Subjective criteria include neuropsychiatric symptoms like anxiety, stress, or mental inhibition, excessive perspiration, cyanosis, dyspnea, respiratory difficulty, and increased amplitude of the auxiliary breathing muscles. Objective criteria: ①FiO2≥ 0.5, PaO2 between 50~60 mmHg and PaO2 less than 50 mmHg or SaO2< 90%; PaCO2> 50 mmHg or PaCO2 increased by >8 mmHg; ②PH < 7.32 or pH decrease > 0.07; ③F/VT > 105 breaths/(min • L); ④RR > 35 breaths/min or increase ≥50%, HR > 140 beats/min or increase ≥20%; ⑤Systolic blood pressure >180mmHg or diastolic blood pressure <90 mmHg or increase ≥20%; ⑥Arrhythmia. If the patient exhibits any of the criteria mentioned above, and it persists for some time (3~5 minutes), the SBT test fails. The SBT test is successful if none of the previously listed conditions are met. Weaning failure is defined as the need for reintubation within 48 hours of extubation due to unstable vital signs, such as altered mental status, respiratory rate greater than 35 beats per minute, and hemodynamic instability (heart rate greater than 140 beats per minute, systolic pressure greater than 180 or less than 90 mmHg). Patients may need mechanical and non-invasive positive pressure ventilation to support respiratory function.
Measurement of Diaphragmatic Excursion
A 3.5-MHz ultrasound probe was placed at the junction of the midclavicular or anterior axillary line and the costal margin, with the probe marker directed outward and downward so that the ultrasound beam was perpendicular to the posterior diaphragm. On the two-dimensional ultrasound image, the hyperechoic diaphragmatic line around the liver could be clearly visualized.12 At this point, the mode was switched to M-mode ultrasound, and the measurement line was adjusted to be as perpendicular to the diaphragm as possible. The diaphragmatic motion trajectory was displayed along the measurement line, and diaphragmatic excursion was defined as the vertical distance from the baseline to the highest point of the curve (Figure 1A). Three respiratory cycles were measured, and the average value was recorded.
 |
Figure 1 Schematic diagrams of the ultrasound assessments. Notes: (A) The DE was the vertical distance from the baseline to the highest point of the curve. (B) The anatomical structure of the diaphragm includes the visceral pleura, parietal pleura, and muscle tissue between them. The distance between the pleura and peritoneum determined the thickness of the diaphragm. (a) After inspiration, the diaphragm’s thickness was measured. (b) The diaphragm thickness was measured at the end of expiration. |
Measurement of Diaphragmatic Thickness
A high-frequency 10-MHz probe was positioned in the 8th or 9th intercostal space between the anterior and mid-axillary lines, either along the intercostal space or with the probe marker oriented toward the patient’s head, ensuring the ultrasound beam was perpendicular to the diaphragm. On the two-dimensional ultrasound image, the hyperechoic pleural and peritoneal layers could be seen, with the hypoechoic diaphragmatic muscle layer in between. Diaphragm thickness was defined as the distance between the pleural and peritoneal layers.14 After localizing the diaphragm in two-dimensional mode, the probe was switched to M-mode, and the measurement line was adjusted to be perpendicular to the diaphragm. M-mode displayed variations in diaphragm thickness along the measurement line throughout the respiratory cycle. The diaphragm thickness at end-expiration during quiet breathing and at end-inspiration during quiet breathing were measured (Figure 1B). Three respiratory cycles were recorded, and the average values were used to calculate the diaphragm thickening fraction (DTF).

Measure MIP
When the patients were breathing normally and the head of the bed was raised 45 degrees, MIP data were obtained from the mechanical ventilator (Puritan BennettTM 840, Medtronic, Minneapolis, USA). The respiratory therapist set the PEEP as 0 cmH2O to decrease the measuring error, held the button “Negative Inspiratory Force, NIF” and recorded the maximum value during the three inspiratory efforts or continuous 20 seconds. The mean value of the three measurements was chosen.
All ultrasound measurements in this study were performed by a respiratory therapist and a physician, both certified in standardized ultrasound training. Inter-observer reliability testing was conducted to ensure the consistency of the measurements. The formula for calculating DCPI is defined as follows;

Statistical Analysis
The sample size of the derivation section was calculated via PASS software, version 15.0. Based on the data of DE and DTF, the area under the ROC curve (AUC) for prediction performance was approximately 70%. The data from our pilot work, which included ten patients and yielded the AUC of 0.75, we estimate 143 patients for the derivation cohort, with a power of 80%, at the 5% two-sided significance level.
The statistical program SPSS 20.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. The mean ± standard deviation is the expression for normally distributed measurement data, and independent sample t-tests were employed to compare the two groups. The median (M) and interquartile range (IQR) are used to express data with non-normal distributions, and Mann–Whitney U-tests were employed to compare the groups. Enumeration data were expressed as frequencies (percentages) [n (%)], and the groups were compared using either Fisher’s exact tests or chi-square testing. The threshold for statistical significance was set at P < 0.05. To assess the effectiveness of the DTF and MIP for the prediction of successful weaning, a receiver operating characteristic (ROC) curve was created, and the ideal critical value was used to compute the sensitivity and specificity.
Results
We screened a consecutive sample of 2394 patients in the derivation cohort to build the predicted cut-off value of DCPI from June 2021 to December 2023, and 286 patients met the inclusion criteria and underwent SBT. To verify the reliability of the DCPI formula, we screened another 986 patients from January 2024 to December 2024 for the validation cohort, and 104 patients were finally retained in the subsequent SBT process. The two recruitment flows are shown in Figure 2, and both cohorts’ characteristics are presented in Table 1.
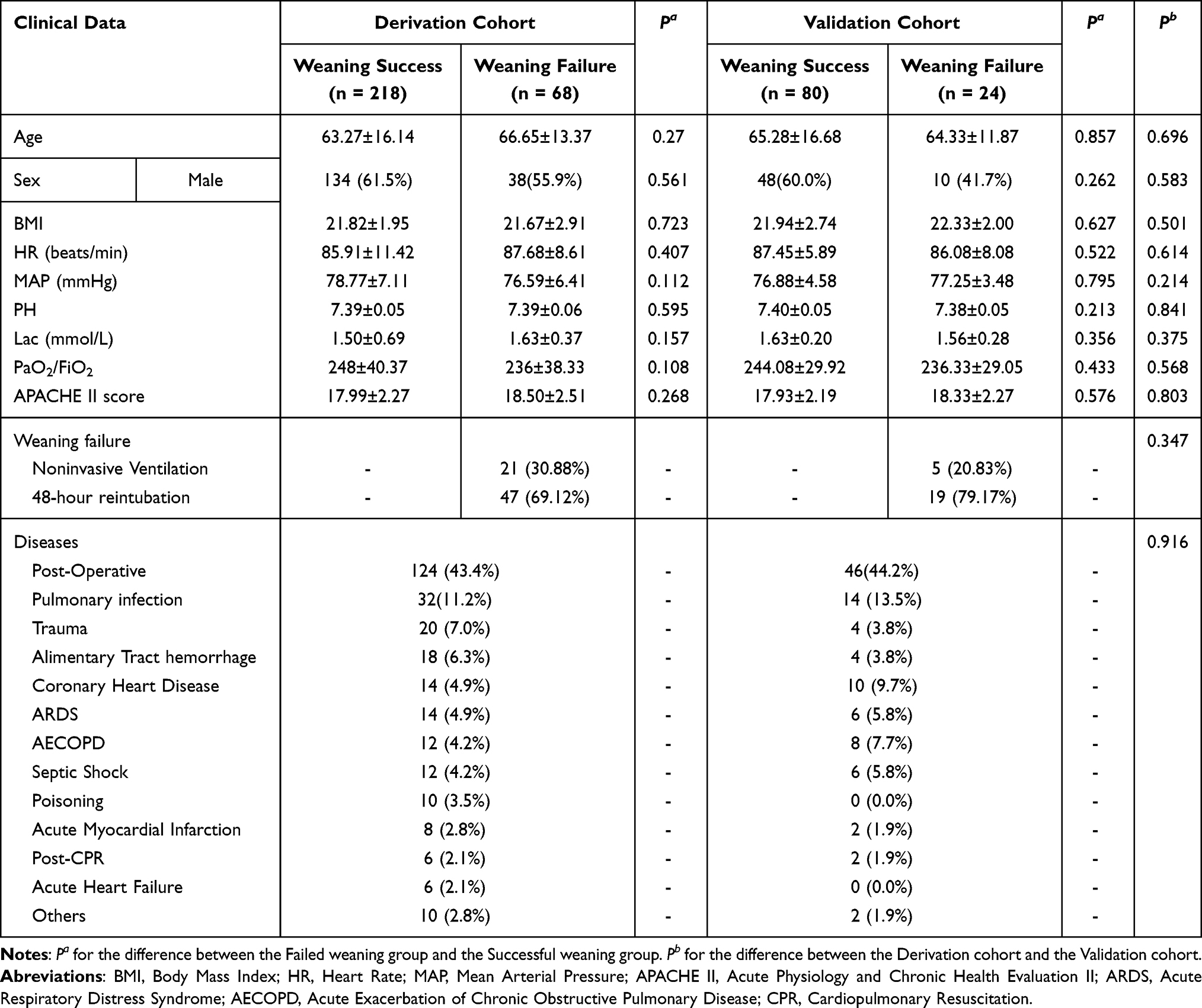 |
Table 1 Patient Characteristics of the Derivation and Validation Cohorts |
 |
Figure 2 Recruitment flows of the derivation and validation cohorts. Notes: (A) Screening protocol of the prospective cohort and (B) screening protocol of the prospective validation cohort. |
All the diaphragm assessment parameters in the derivation cohort, including DCPI, DE, DTF and MIP, were significantly higher in weaning success group (36.67% ± 7.02%, 1.85 ± 0.38, 34.75% ± 7.82%, and 33.57 ± 8.50) than those in weaning failure group (24.03% ± 5.78%, 1.64 ± 0.23, 24.81% ± 4.50%, and 25.72 ± 4.28, P < 0.001), as shown in Table 2.
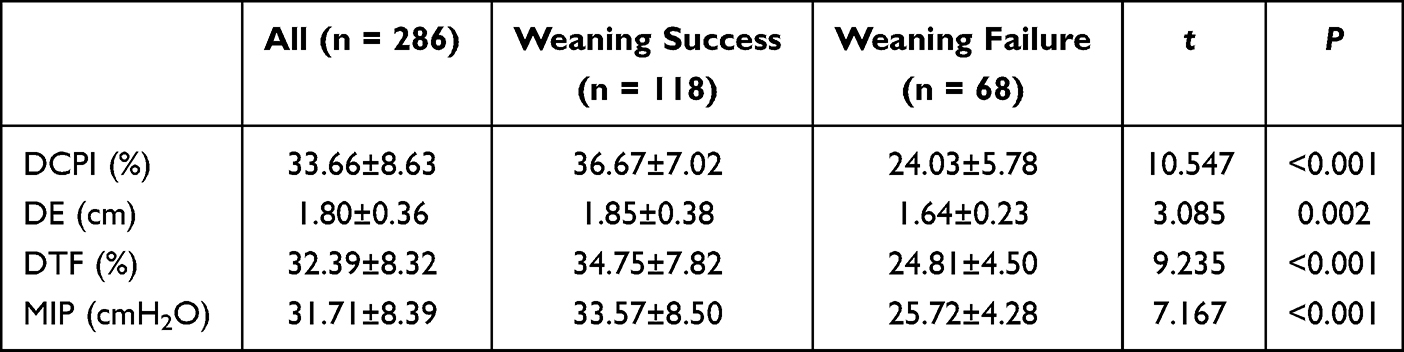 |
Table 2 Weaning Parameters Between Success and Failure Groups in the Derivation Cohort |
Table 3 shows the duration of MV, the time of endotracheal intubation, the period of ICU stay, and the rate of tracheotomy was considerably lower in the weaning success group than in the weaning failure group (P < 0.05), even though there was no difference in the mortality rate or total hospital days between the two groups in the derivation cohort (P > 0.05).
 |
Table 3 Clinical Characteristics Between Success and Failure Groups in the Derivation Cohort |
The ROC curves demonstrate the predictive performance of DCPI, DE, DTF, and MIP in the derivation cohort’s weaning success group, shown in Figure 3 and Table 4. At a cut-off value of 30.0%, the DCPI showed excellent diagnostic performance, with an AUC of 0.954 (95% CI: 0.905–0.982, P < 0.001), and corresponding sensitivity and specificity of 94.1% and 90.8%, respectively. For DE, a cut-off value of 1.7 cm yielded an AUC of 0.698 (95% CI: 0.615–0.771, P < 0.001), with sensitivity and specificity of 76.2% and 61.8%. The DTF, with a cut-off of 29.5%, produced an AUC of 0.770 (95% CI: 0.693–0.837, P < 0.01), sensitivity of 88.2%, and specificity of 71.6%. Lastly, the MIP demonstrated an AUC of 0.811 (95% CI: 0.737–0.872, P < 0.001) at a cut-off of 26.5 cmH2O, with sensitivity and specificity of 84.4% and 73.5%, respectively.
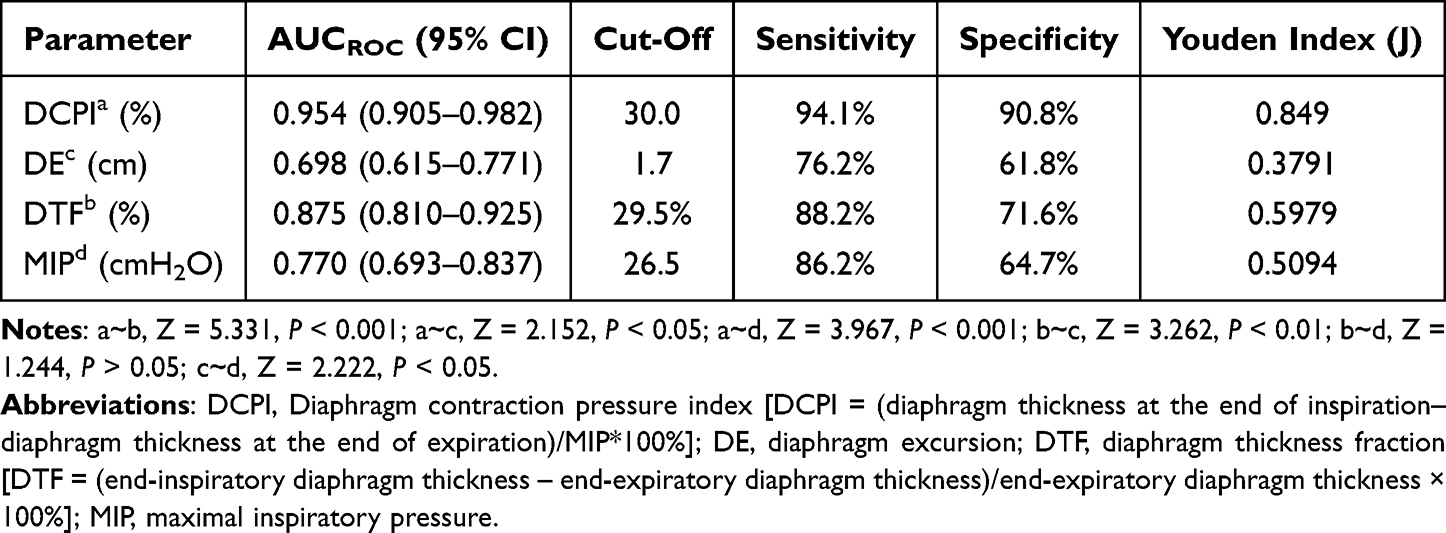 |
Table 4 AUCROC of Prediction Performance of DCPI, DTF, MIP and DE for Weaning Success |
 |
Figure 3 ROC curves for weaning parameters in the derivation cohort. Notes: In the derivation cohort’s weaning success group, the AUCs for the predictive performance of DCPI, DE, DTF, and MIP were 0.944 (95% CI: 0.893–0.975), 0.698 (95% CI: 0.615–0.771), 0.890 (95% CI: 0.827–0.936), and 0.811 (95% CI: 0.737–0.872). |
With an AUC of 0.952 (95% CI, 0.854–0.992, P < 0.001), DCPI’s predictive performance in the prospective validation cohort was similar to that of the derivation cohort, as shown in Figure 4. When the cut-off value was 30.0%, the DCPI’s sensitivity and specificity were 0.93 and 0.92, respectively, with a PPV of 0.91 and an NPV of 0.89.
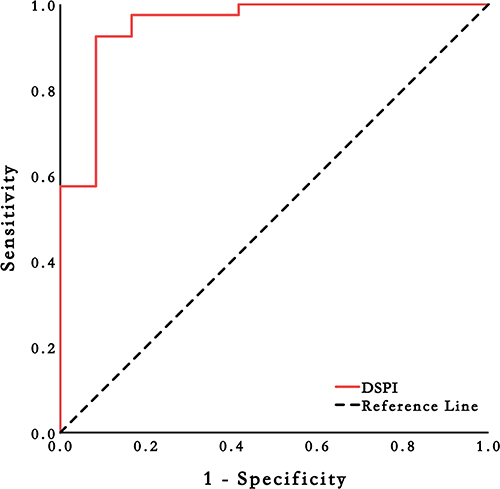 |
Figure 4 ROC curves for weaning parameters in the validation cohort. Note: The prospective validation cohort’s DCPI AUC was 0.952 (95% CI, 0.854−0.992, P < 0.001); |
Discussion
In this work, we introduced the novel parameter – DCPI – instead of Pdi, which represents the differential value of diaphragm thickness after inspiration and expiration, and is more readily obtainable via ultrasonography. When the best cut-off value was equal to or greater than 30.0 mm/cmH2O, the AUC of DCPI for prediction performance was 0.954, markedly superior to DE, DTF, and MIP. With the prominent sensitivity (94.1%) and specificity (90.8%), similar results were obtained in the prospective validation cohort. DCPI could help the clinician estimate who can sweep through the weaning procedure.
In this single-center observational study, we have innovatively established DCPI as a new parameter to predict whether the patients can successfully separate from the ventilator and verified the superiority of that over the other indicators, such as DE, DTF, and MIP.
During the past decades, clinicians were increasingly enthusiastic about applying ultrasound at the ICU bedside, as the methodological superiority of low cost, non-invasive, and easy reproducibility,15,16 as if it had been a matter of course that ultrasonographically visual assessment of pathological diaphragm could effectively assist in disconnecting from the ventilator in critically ill subjects.17,18 Nevertheless, that is not the end of the controversy.
In a recent systematic review, twenty studies on diaphragm ultrasound availability were thoroughly examined and revealed the optimistic value.19 Although four studies underlined the superiority of DE or DTF in predicting extubation odds, several intrinsic vulnerabilities confined the extension of these ultrasonic indicators. On the one hand, the best cut-off of DE and DTF to identify the diaphragm dysfunction remained in doubt. On the other hand, the prediction performance, represented as the AUC, fell short of being immensely satisfying. In this study, the best cut-off values calculated for DE and DTF were 1.7 cm and 29.5%, a more demanding standard than the previous studies. They merely yielded the reluctant diagnostic capability (AUCs were 0.698 and 0.770).20–22 When the spotlight was turned on the more rigorous methodology and the cut-off value, for instance, multiple-centered study design, diaphragmatic dysfunction was defined as DE < 10 mm or DTF < 30%, the reliability of these parameters is more frustrating.23
On the other hand, previous research on weaning has also focused on analyzing the effects of the rapid shallow breathing index during weaning, and it performed excellently.24–26 However, we did not include RSBI as a direct weaning index in our comparative analysis, as all patients underwent evaluation through a spontaneous breathing trial (SBT), which indirectly reflects RSBI. Notably, all patients had an RSBI of less than 105 breaths/min/L. SBT also evaluated whether the patient exhibited symptoms such as cyanosis and difficulty breathing, indirectly indicating that the patient did not experience respiratory distress.
Based solely on the data from patients who meet the inclusion criteria of this study, the 48-hour reintubation rate after extubation is high (>15%). However, because the study covered patients on mechanical ventilation for more than 24 hours and the actual number of patients on mechanical ventilation significantly exceeds the number of cases in this study, the 48-hour reintubation rate at our center is much lower than the data presented.
Moreover, even more importantly, when the diaphragm’s core status has been highly prized, the accessory respiratory muscles, including the intercostal muscle, should not be ignored as the essential contributors to the whole breathing process. Despite the primary breathing workload undertaken by the diaphragm during normal breathing, the accessory muscles engage more breathing effort after diaphragm dysfunction.8
Therefore, in a small-sized observational study, including healthy volunteers and critically ill patients, Dres et al presented the parasternal muscle thickening correlated with diaphragm dysfunction and could similarly predict failure of the spontaneous breathing trial as DTF.9
We know that during normal breathing, the diaphragm mainly works. When the function of the diaphragm is abnormal, increased work is done by the accessory respiratory muscles during breathing. However, compared with the diaphragm in physiology, these accessory muscles possess weak respiratory endurance and are more liable to fatigue. When the respiratory capacity load from the accessory muscles accounts for a relatively high proportion during the entire respiratory effort, the patients are not capable of persevering in prolonged spontaneous breathing, which always leads to weaning failure.27 When the ratio of diaphragmatic work is high, the patient maintains better spontaneous breathing, and the success rate of weaning is higher. Hence, evaluation of the diaphragm and the whole accessory respiratory muscles workload should be regarded as the more appropriate paradigm, which MIP has usually appraised in previous studies.10,11 The value of MIP reflects the pressure generated by all breathing muscles; the pressure generated by the work of the diaphragm can be expressed as transdiaphragmatic pressure (Pdi). Therefore, the ratio of Pdi to MIP indicates the proportion of diaphragmatic work done by the patient during breathing. When Pdi is well-represented as the diaphragm’s workload, the higher proportion of Pdi to MIP indicates that the patients are more likely to achieve successful weaning. However, the measurement of Pdi requires precise catheter placement technology, specific materials, and a ventilator, and the clinical application rate of Pdi is not high. Studies have shown that the diaphragm thickness measured using ultrasound in PSV mode highly correlates with Pdi.12
Study Limitations
Several limitations exist in our study. First, as a preliminary exploration, this study is still inevitably a monocentric and small-scale research. However, the outstanding reliability of the new parameter will encourage us to verify it further in multicenter research. Second, the convenient acquisition of high-quality images prompted all ultrasound procedures to be performed on the right side. Third, except for diaphragm appraisement, we did not adequately investigate the patients’ cardiac function, consciousness level and cough, which also contribute to weaning failure. Finally, the limitations of ultrasound measurements, including operator-dependence and poor reproducibility, should be explicitly mentioned.
Conclusion
DCPI of right diaphragm ≥30.0% is used as the threshold, it has potential or better predictive value than traditional parameters, but it still needs to be verified in multi-center and large sample studies.
Abbreviations
DCPI, diaphragm contraction pressure index; MIP, maximum inspiratory pressure; SBT, spontaneous breathing trial; DE, diaphragm excursion; Pdi, transdiaphragmatic pressure; DTF, diaphragm thickness; ROC, receiver operating characteristic curve.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Informed Consent
The protocol was approved by the Human Ethics Committee of Yijishan Hospital, First Affiliated Hospital of Wannan Medical College (Approval Number 2018-03), and informed consent was obtained from all patients or their relatives. The consent to participate was applicable.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the University Scientific Research Program of Wannan Medical College in 2024 (WK2024LC07; SJD202407).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Thille AW, Arrivé F, Le Pape S. Spontaneous breathing trials: how and for how long? Curr Opin Crit Care. 2025;31(1):86–92. doi:10.1097/MCC.0000000000001227
2. Thille AW, Cortés-Puch I, Esteban A. Weaning from the ventilator and extubation in ICU. Curr Opin Crit Care. 2013;19(1):57–64. doi:10.1097/MCC.0b013e32835c5095
3. Jaber S, Quintard H, Cinotti R, et al. Risk factors and outcomes for airway failure versus non-airway failure in the intensive care unit: a multicenter observational study of 1514 extubation procedures. Crit Care. 2018;22(1):236. doi:10.1186/s13054-018-2150-6
4. Damuth E, Mitchell JA, Bartock JL, Roberts BW, Trzeciak S. Long-term survival of critically ill patients treated with prolonged mechanical ventilation: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(7):544–553. doi:10.1016/S2213-2600(15)00150-2
5. Dettmer MR, Damuth E, Zarbiv S, Mitchell JA, Bartock JL, Trzeciak S. Prognostic factors for long-term mortality in critically ill patients treated with prolonged mechanical ventilation: a systematic review. Crit Care Med. 2017;45(1):69–74. doi:10.1097/CCM.0000000000002022
6. Dres M, Estellat C, Baudel JL, et al. Reseau Européen de Recherche en Ventilation Artificielle (REVA) research network. Comparison of a preventive or curative strategy of fluid removal on the weaning of mechanical ventilation: a study protocol for a multicentre randomised open-label parallel-group trial. BMJ Open. 2021;11(8):e048286. doi:10.1136/bmjopen-2020-048286
7. Doorduin J, Roesthuis LH, Jansen D, van der Hoeven JG, van Hees HWH, Heunks LMA. Respiratory muscle effort during expiration in successful and failed weaning from mechanical ventilation. Anesthesiology. 2018;129(3):490–501. doi:10.1097/ALN.0000000000002256
8. Ricoy J, Rodríguez-Núñez N, Álvarez-Dobaño JM, Toubes ME, Riveiro V, Valdés L. Diaphragmatic dysfunction. Pulmonology. 2019;25(4):223–235. doi:10.1016/j.pulmoe.2018.10.008
9. Dres M, Dubé BP, Goligher E, et al. Usefulness of parasternal intercostal muscle ultrasound during weaning from mechanical ventilation. Anesthesiology. 2020;132(5):1114–1125. doi:10.1097/ALN.0000000000003191
10. Bien Udos S, Souza GF, Campos ES, et al. Maximum inspiratory pressure and rapid shallow breathing index as predictors of successful ventilator weaning. J Phys Ther Sci. 2015;27(12):3723–3727. doi:10.1589/jpts.27.3723
11. Supinski GS, Westgate P, Callahan LA. Correlation of maximal inspiratory pressure to transdiaphragmatic twitch pressure in intensive care unit patients. Crit Care. 2016;20:77. doi:10.1186/s13054-016-1247-z
12. Goligher EC, Laghi F, Detsky ME, et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity. Intensive Care Med. 2015;642–649. doi:10.1007/s00134-015-3687-3
13. MacIntyre NR, Cook DJ, Ew E, et al. American College of Chest Physicians; American Association for Respiratory Care; American College of Critical Care Medicine. Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest. 2001;120(6 Suppl):375S–95S. doi:10.1378/chest.120.6_suppl.375s
14. Theerawit P, Eksombatchai D, Sutherasan Y, Suwatanapongched T, Kiatboonsri C, Kiatboonsri S. Diaphragmatic parameters by ultrasonography for predicting weaning outcomes. BMC Pulm Med. 2018;18(1):175. doi:10.1186/s12890-018-0739-9
15. Pivetta E, Cara I, Paglietta G, et al. Diaphragmatic point-of-care ultrasound in COVID-19 patients in the emergency department-a proof-of-concept study. J Clin Med. 2021;10(22):5291. doi:10.3390/jcm10225291
16. Fossat G, Daillet B, Desmalles E, Boulain T. Does diaphragm ultrasound improve the rapid shallow breathing index accuracy for predicting the success of weaning from mechanical ventilation? Aust Crit Care. 2022;35(3):233–240. doi:10.1016/j.aucc.2021.05.008
17. Kilaru D, Panebianco N, Baston C. Diaphragm ultrasound in weaning from mechanical ventilation. Chest. 2021;159(3):1166–1172. doi:10.1016/j.chest.2020.12.003
18. Dres M, Similowski T, Goligher EC, et al. Dyspnoea and respiratory muscle ultrasound to predict extubation failure. Eur Respir J. 2021;58(5):2100002. doi:10.1183/13993003.00002-2021
19. Parada-Gereda HM, Tibaduiza AL, Rico-Mendoza A, et al. Effectiveness of diaphragmatic ultrasound as a predictor of successful weaning from mechanical ventilation: a systematic review and meta-analysis. Crit Care. 2023;27(1):174. doi:10.1186/s13054-023-04430-9
20. Kannan S, Khanna P, Kayarat B, et al. Assessment of respiratory muscles, lung parenchyma, and cardiac function by ultrasound for predicting weaning failure in critically ill adults: a prospective observational study. J Ultrasound Med. 2025;44(2):195–207. doi:10.1002/jum.16596
21. Demoule A, Fossé Q, Mercat A, et al. Operator independent continuous ultrasound monitoring of diaphragm excursion predicts successful weaning from mechanical ventilation: a prospective observational study. Crit Care. 2024;28(1):245. doi:10.1186/s13054-024-05003-0
22. Yoo JW, Lee SJ, Lee JD, Kim HC. Comparison of clinical utility between diaphragm excursion and thickening change using ultrasonography to predict extubation success. Korean J Intern Med. 2019;34(3):686. doi:10.3904/kjim.2016.152.e1
23. Vivier E, Muller M, Putegnat JB, et al. Inability of diaphragm ultrasound to predict extubation failure: a multicenter study. Chest. 2019;155(6):1131–1139. doi:10.1016/j.chest.2019.03.004
24. Jia D, Wang H, Wang Q, et al. Rapid shallow breathing index predicting extubation outcomes: a systematic review and meta-analysis. Intensive Crit Care Nurs. 2024;80:103551. doi:10.1016/j.iccn.2023.103551
25. Chu Y, Guo C, Fu H. Correlation between diaphragmatic-rapid shallow breathing index and lung ultrasound score in elderly patients with mechanical ventilation and its predictive value for weaning results. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024;36(2):
26. Er B, Mızrak B, Aydemir A, et al. Is diaphragm ultrasound better than rapid shallow breathing index for predicting weaning in critically ill elderly patients? Tuberk Toraks. 2023;71(3):197–202. doi:10.5578/tt.20239701
27. Diao S, Li S, Dong R, et al. The diaphragmatic electrical activity during spontaneous breathing trial in patients with mechanical ventilation: physiological description and potential clinical utility. BMC Pulm Med. 2024;24(1):263. doi:10.1186/s12890-024-03077-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diaphragm Assessment by Multimodal Ultrasound Imaging in Healthy Subjects
Zhang T, Liu Y, Xu D, Dong R, Song Y
International Journal of General Medicine 2024, 17:4015-4024
Published Date: 12 September 2024
Advances in Machine Learning for Mechanically Ventilated Patients
Xu Y, Xue J, Deng Y, Tu L, Ding Y, Zhang Y, Yuan X, Xu K, Guo L, Gao N
International Journal of General Medicine 2025, 18:3301-3311
Published Date: 21 June 2025
Retrospective Comparison of Extrafascial versus Intrafascial Interscalene Brachial Plexus Block with Reduced Volume: Impact on Hemidiaphragmatic Paralysis and Hemodynamic Effects in Shoulder Surgery Patients
Coviello A, Ranieri G, Coppola F, Damonte R, Cirillo D, De Siena AU, Fattorini F, Scimia P, Castellano G, Rucci F, Servillo G
Local and Regional Anesthesia 2025, 18:87-102
Published Date: 17 September 2025
Circulating and Respiratory Biomarkers in Sepsis-Induced ARDS: Diagnostic and Prognostic Insights – A Narrative Review
Muhoza BG, Liu S, Niyonkuru E, Sun T
Journal of Inflammation Research 2026, 19:571504
Published Date: 25 March 2026