Back to Journals » Infection and Drug Resistance » Volume 16
Diagnostic Performance of Metagenomic Next-Generation Sequencing in Central Nervous System Cryptococcosis Using Cerebrospinal Fluid
Authors Zhang X, Lin Y, Chen H, Hu J, Zhao H, Yang M, Han D ![]()
Received 9 July 2023
Accepted for publication 1 September 2023
Published 13 September 2023 Volume 2023:16 Pages 6175—6183
DOI https://doi.org/10.2147/IDR.S425463
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xuan Zhang,1 Yaqing Lin,2 Huixin Chen,1 Jianhua Hu,1 Hong Zhao,1 Meifang Yang,1 Dongsheng Han3– 5
1State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, National Medical Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Shulan (Hangzhou) Hospital Affiliated to Zhejiang Shuren University Shulan International Medical College, Hangzhou, Zhejiang, People’s Republic of China; 3Department of Laboratory Medicine, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 4Key Laboratory of Clinical in vitro Diagnostic Techniques of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China; 5Institute of Laboratory Medicine, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Dongsheng Han, Centre of Clinical Laboratory, First Affiliated Hospital, College of Medicine, Zhejiang University, 79 Qingchun Road, Hangzhou, 310003, People’s Republic of China, Tel +86-571-87236394, Fax +86-571-87236394, Email [email protected]
Purpose: Metagenomic next-generation sequencing (mNGS) has been widely used to diagnose infectious diseases. However, there are few studies on its diagnostic performance in the central nervous system (CNS) cryptococcosis. This study examined the diagnostic efficacy of mNGS in identifying Cryptococcus spp. in cerebrospinal fluid (CSF) samples.
Patients and Methods: From March 2021 to March 2023, 290 patients with suspected CNS infection were recruited from the First Affiliated Hospital, School of Medicine, Zhejiang University, and 74 patients were ultimately included in the study. Lastly, 22 patients with CNS cryptococcosis were included. Of these patients, 25 CSF samples were enrolled. The diagnostic performance of conventional assays [including India ink, cryptococcal antigen (CrAg) testing, and culture] and mNGS was evaluated for CNS cryptococcosis.
Results: In the 25 samples collected, the coincidence rates of mNGS with India ink, CrAg, and culture were 64.0% (16/25), 80.0% (20/25), and 80.0% (20/25), respectively. Without antifungal drug exposure, the coincidence rates were increased to 66.7% (10/15), 100.0% (15/15), and 93.3% (14/15), respectively. The coincidence rates after antifungal therapy were all decreased to 60.0% (6/10), 50.0% (5/10), and 60.0% (6/10), respectively. Moreover, in the 25 samples, the sensitivity of mNGS reached 80.0%, and of India ink, CrAg testing, and culture were 68.0, 100.0, and 60.0%, respectively. The mNGS showed an excellent positive rate (100.0%) in the 15 samples collected without antifungal drug exposure, which was significantly higher than the antifungal drug-exposed group (n = 10) (50.0%) (P = 0.005). The reads of Cryptococcus spp. before antifungal therapy were significantly higher than after it (median, 25,915 vs 2, P = 0.008).
Conclusion: mNGS is an effective tool for diagnosing CNS cryptococcosis using CSF; however, its sensitivity decreases considerably in patients who have been effectively treated with antifungal drugs.
Keywords: metagenomic next-generation sequencing, central nervous system cryptococcosis, cerebrospinal fluid, invasive fungal infection
Introduction
Central nervous system (CNS) cryptococcosis is an invasive fungal infection caused by Cryptococcus spp. Although the infection is preventable and treatable, its morbidity and mortality rates are still high.1 Global cryptococcal meningitis accounts for 15% of acquired immune deficiency syndrome-related deaths, with an estimated 181,100 deaths annually.2 In the Asia and Pacific region, approximate 44,000 HIV-infected adults developed cryptococcal meningitis, and 26,000 cryptococcal-related deaths occurred annually.3 Consequently, effective prevention, prompt and accurate diagnosis, and early treatment are critical.
Traditional diagnostic methods of CNS cryptococcosis include cerebrospinal fluid (CSF) culture, India ink, and cryptococcal antigen (CrAg) testing. Among them, CSF culture is considered the diagnostic gold standard.2 However, it takes several days, or even a week, for fungus to develop, which can delay diagnosis and treatment. Cultures may also produce false-negative results when the fungal burden is low.4 India ink microscopy has historically been a rapid and low-resource technique for detecting Cryptococcus spp. in the CSF.5 It demonstrates relatively low sensitivity (86% in cryptococcal meningitis)6 and is technician-dependent.7,8 CrAg testing was an effective method to detect cryptococcosis, which was more sensitive than CSF culture.9 The summary estimates of sensitivity and specificity of CSF CrAg for detecting cryptococcal meningitis were 98.8 and 99.3%, respectively, and summary sensitivity and specificity of serum CrAg were 99.7% and 94.1%, respectively.10
Metagenomic next-generation sequencing (mNGS) is a method where all the nucleic acid (DNA and/or RNA) of a specimen is sequenced in parallel, which is highly effective in diagnosing infectious diseases.11–13 Previous studies14–16 demonstrated that, in some cases, mNGS improved the diagnosis of neurologic infections and provided actionable information on CSF obtained from patients with meningitis. However, only a few studies have focused on CNS cryptococcosis.17–19 Therefore, this retrospective study evaluated the diagnostic performance of mNGS in identifying CNS cryptococcosis compared to traditional culture, India ink, and CrAg testing of CSF.
Materials and Methods
Study Design and Participants
A retrospective observational study was performed in patients with suspected CNS infections from March 2021 to March 2023. The inclusion criteria of patients were as follows: (1) patients aged over 18 years; (2) patients who visited the First Affiliated Hospital, School of Medicine, Zhejiang University, from March 2021 to March 2023; (3) patients had symptoms of meningitis or encephalitis, including fever, headache, nausea/vomiting, seizures, alteration in consciousness/ coma; and (4) patients received lumbar puncture for CSF test, included mNGS, culture, India ink, and CrAg testing. Exclusion criteria were: (1) patients with incomplete clinical data; (2) patients without mNGS, culture, India ink, or CrAg testing on CSF. The diagnosis of CNS cryptococcosis was based on the guideline of European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium (2019).20 The enrollment and screening process of patients is depicted in Figure 1.
 |
Figure 1 Flowchart of patient enrollment and grouping (CNS, central nervous system; CrAg, cryptococcal antigen; mNGS, metagenomic next-generation sequencing). |
Data were extracted from the electronic patient record system of the hospital. Demographic characteristics (age and gender), comorbidities, laboratory results (CSF routine test, biochemical tests, mNGS, culture, India ink, and CrAg testing), clinical manifestations, intensive care unit treatment history, and ventriculoperitoneal shunts were collected.
Culture, India Ink, and CrAg Testing
All samples were cultured on Sabouraud dextrose agar (SDA) at 37°C for 2–5 days. The growing colonies were purified for culture, and a single colony was selected for strain identification using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). Cryptococcus neoformans was shown as a yeast-like fungus with a thick, clear capsule through Indian ink staining. CSF-based CrAg lateral flow immunoassay tests (Immy Diagnostics, Norman, Oklahoma, USA) were performed on each sample according to the manufacturer’s instructions.
mNGS on CSF Samples
CSF mNGS testing was performed in the clinical laboratory of our hospital. The steps included sample processing, nucleic acid extraction, library construction, high-throughput sequencing, and bioinformatics analysis (result interpretation). First, total DNA was extracted from 300 μL of CSF samples using a commercial kit (QIAamp® UCP Pathogen DNA Kit, catalog number: 50,214, Qiagen, Germany). Each sample was spiked with an internal control after nucleic acid extraction in a manner described in detail in our recently published study.21 Subsequently, 30 μL of the nucleic acid solution was used to generate a sample library using a commercial library construction kit (Nextera DNA Flex kit, Illumina, San Diego, CA, USA). The synthesized library was single-end sequenced (SE-75) using an Illumina Nextseq CN500 sequencer. In each run, negative and no-template control samples were tested alongside clinical samples to identify potential test failures and microbial contaminations. After sequencing, we used the same analysis software and algorithms as in our published studies to filter the raw data into clean data, then remove the human sequence by mapping the clean data to the human reference genome (hg38), and the remaining non-human sequence are finally aligned to the microbial reference database to complete the identification of microorganisms.21
Statistical Analysis
All statistical analyses were conducted with SPSS software version 25.0 (IBM, Armonk, NY, USA). Continuous variables with a normal distribution were expressed as mean ± standard deviation (SD), while continuous variables with a non-normal distribution were represented as median. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and the Youden index were used to evaluate the diagnostic performance of India ink, CrAg, culture and mNGS for CNS cryptococcosis. The χ2 test was used to compare categorical data obtained from various tests. The reads of Cryptococcus spp. between various antifungal drug exposure states were analyzed by the Mann–Whitney U-test. P < 0.05 was considered to be statistically significant. Figures were drawn using GraphPad Prism 8.0 (GraphPad Software, San Diego, CA, USA) and online website (https://bioinfogp.cnb.csic.es/tools/venny/index.html).
Results
Patient Characteristics
As displayed in Figure 1, 290 patients with suspected CNS infections were selected from March 2021 to March 2023. However, 212 patients were excluded due to the absence of CSF sample analysis (including mNGS, culture, India ink, and CrAg testing), and four patients were excluded due to incomplete clinical data. Consequently, 74 patients were ultimately included in the study. Based on the CSF sample analysis results, the patients were divided into the CNS cryptococcosis group (22 patients) and the non-CNS cryptococcosis group (52 patients). Three of the 22 patients with CNS cryptococcosis received CSF tests twice (including mNGS). A total of 25 CSF samples were collected. The mNGS and culture results suggested that all samples contained Cryptococcus neoformans.
Table 1 enlists the patient characteristics of the CNS cryptococcosis group and non-CNS cryptococcosis group. In CNS cryptococcosis group, the number of immunocompromised patients (P = 0.003) and patients with ventriculoperitoneal shunts (P < 0.001) increased significantly. Of the 25 CSF samples, 15 (60.0%) cases were collected without antifungal therapy exposure, while 10 (40.0%) were under antifungal therapy. The CSF assays in various stages of antifungal treatment are shown in Table 2, and none of them differed significantly (P > 0.05).
 |
Table 1 Clinical Features of Patients with CNS Cryptococcosis and Non-CNS Cryptococcosis |
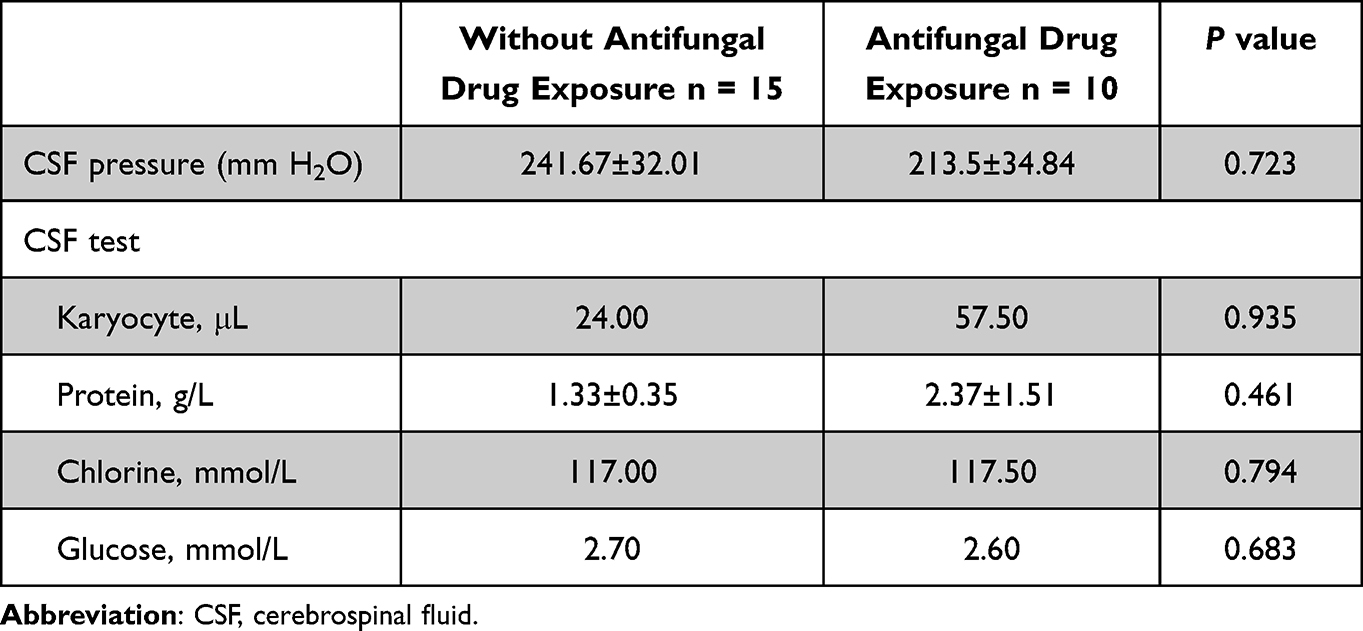 |
Table 2 The Cerebrospinal Fluid Tests for Central Nervous System Cryptococcosis in Various Antifungal Treatment States |
The Results of mNGS and Conventional Tests for Cryptococcus Spp.
The results of mNGS and conventional tests (India ink, CrAg, and culture) in the 25 CSF samples collected are shown in Figure 2A. The 11 samples were diagnosed positive by all the methods, however, seven samples were positive by three methods [4 samples (CrAg, culture, mNGS), 3 samples (India ink, CrAg, mNGS)]. Five samples were identified as positive by two distinct methods [2 samples (CrAg, mNGS), 3 samples (India ink, CrAg)]. Only two samples tested positive using a single method (CrAg).
 |
Figure 2 The Venn diagram of results of metagenomic next-generation sequencing (mNGS) and conventional tests [including India ink, cryptococcal antigen (CrAg) testing, and culture] in central nervous system cryptococcosis. Figure (A) depicts the results of all 25 CSF samples, Figure (B) shows the results of 15 CSF samples collected before antifungal drug exposure, and Figure (C) depicts the results of 10 samples collected after antifungal drug exposure. |
Before antifungal drug exposure, ten of fifteen samples (10/15) were positive by all methods, four by three methods (CrAg, culture, mNGS), and one by CrAg and mNGS (Figure 2B). Under antifungal drug exposure, one sample was positive by all methods, three samples were positive by three methods (India ink, culture, mNGS), four samples were positive by two methods [1 samples (CrAg, mNGS), 3 samples (India ink, CrAg)], and two samples were positive by CrAg (Figure 2C).
Comparison of the Detection Capabilities of mNGS and Conventional CNS Cryptococcosis Tests
Table 3 displays the diagnostic efficacy of India ink, CrAg, culture, and mNGS using CSF in CNS cryptococcosis. The detection efficiency of mNGS for the 25 collected samples reached 80.0%, and the results of the four detection methods differed statistically (χ2 = 12.818, P = 0.005). Among the 15 samples collected without antifungal drug exposure, mNGS and CrAg showed excellent detection efficiency (100.0%), and culture also had 93.3% detection efficiency, which was significantly higher than India ink (66.7%, χ2 = 12.593, P = 006). However, mNGS (50.0%) did not perform than CrAg and India ink in antifungal drug exposure samples (100.0% vs 70.0%), and culture was the worst (10.0%, χ2 = 17.494, P = 0.001).
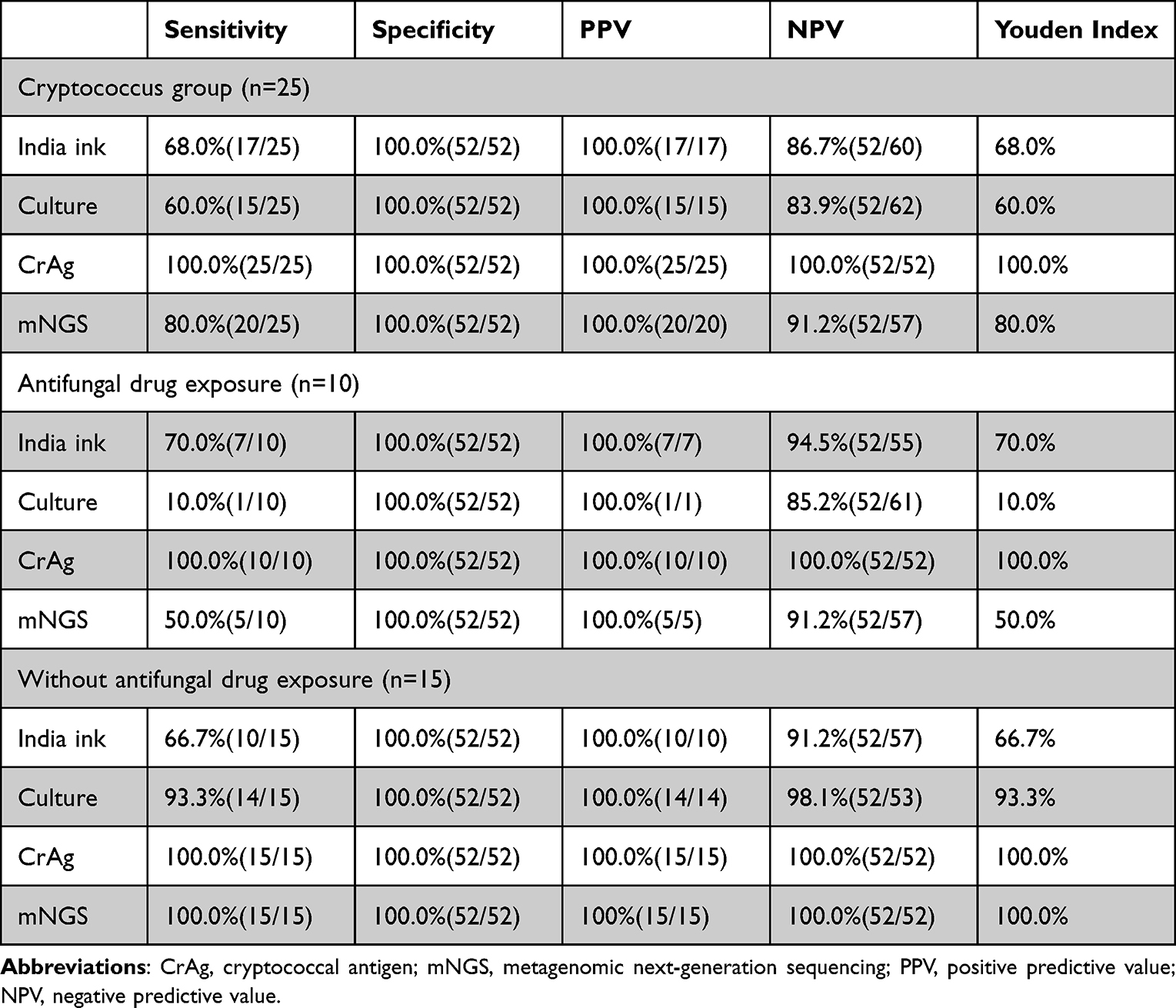 |
Table 3 Diagnostic Performance of India Ink, CrAg, Culture, and mNGS in Central Nervous System Cryptococcosis |
The coincidence rates of mNGS with India ink, CrAg, and culture in 25 CSF samples were 64.0% (16/25), 80.0% (20/25), and 80.0% (20/25), respectively. Without antifungal drug exposure, the coincidence rates of mNGS with India ink, CrAg, and culture were increased to 66.7% (10/15), 100.0% (15/15), and 93.3% (14/15), respectively. The coincidence rates of mNGS with India ink, CrAg, and culture after antifungal therapy were all decreased to 60.0% (6/10), 50.0% (5/10), and 60.0% (6/10), respectively.
Effect of Antifungal Drug Exposure on Cryptococcus Spp. Detection Using mNGS
There was a significant difference in the positive detection rate by mNGS between CNS cryptococcosis patients receiving antifungal therapy and those not receiving treatment (100.0 vs 50.0%, P = 0.005). However, in patients receiving antifungal drugs for > 3 months, the rate of Cryptococcus spp. detection by mNGS was lower than in cases receiving drugs for < 3 months [60.0% (3/5) vs 40.0% (2/5)]. Moreover, there was no statistical difference (P = 0.573). Antifungal regimens and duration of antifungal therapy in patients with CNS cryptococcosis were detailed in Table S1.
Of the 25 CSF samples, the reads of Cryptococcus spp. before antifungal therapy were significantly higher than after it (median, 25,915 vs 2, P = 0.008) (Figure 3). Among the samples with antifungal drug exposure, two samples had only one read, and one had two reads. Three patients underwent CSF testing before and after antifungal therapy. According to mNGS, the sequence of Cryptococcus spp. decreased significantly after antifungal treatment of two cases was undetectable, and that of one case was significantly reduced (217,218 vs 2060).
 |
Figure 3 Comparison of Cryptococcus spp. reads measured by metagenomic next-generation sequencing in the cerebrospinal fluid of patients with central nervous system cryptococcosis with or without antifungal drug exposure. The difference was statistically significant (P = 0.008). |
Discussion
Our study enrolled 22 patients with CNS cryptococcosis and 25 CSF samples. Some samples were collected after antifungal treatment, resulting in intriguing variations in the results. There was no significant difference in the routine tests of CSF before and after antifungal therapy. The reason may be that mNGS was examined to confirm the diagnosis again due to poor response to antifungal treatment or suspicion of a mixed infection.
Tests used in CNS cryptococcosis, an exceedingly severe disease with a high fatality, must be highly sensitive to ensure the timely initiation of induction antifungal therapy.22 We evaluated the diagnostic performance of conventional tests (India ink, CrAg testing, and culture) and mNGS in detecting CNS cryptococcosis using CSF. The sensitivity of mNGS was slightly lower than CrAg testing, however, higher than India ink and culture; its specificity was identical to conventional methods. Interestingly, before antifungal drug exposure, the sensitivity of mNGS and CrAg reached 100.0%, superior to India ink and culture. It indicated excellent diagnostic efficacy of mNGS in CNS cryptococcosis using CSF. Similar to our findings, Gan Z et al18 reported that in 46 cases of cryptococcal meningitis in HIV-negative patients, the sensitivity and specificity of mNGS reached 93.5 and 96.0%, respectively.
The role of CrAg testing in cryptococcosis diagnosis has been established by guidelines.20,23 In this study, the CrAg test performed well, and its sensitivity in CSF reached 100.0% regardless of antifungal drug exposure. It is well known that antifungal drug exposure can significantly alter the results of conventional etiological tests because a decrease in cryptococcal load and cryptococcal activity may result in negative fungal culture and India ink staining results. However, it is unclear whether exposure to antifungal drugs affects the results of mNGS. Our study provided a conclusive answer. After antifungal treatment, the detection rate of Cryptococcus spp. with mNGS decreased from 100.0 to 50.0% (P = 0.005), even lower than CrAg and India ink and higher than culture. With the extension of antifungal drug application time, the rate of mNGS detection decreased. In addition, Cryptococcus spp. reads decreased substantially following antifungal therapy, confirming the efficacy of antifungal therapy. Therefore, antifungal therapy can considerably reduce the detection rate and reads of Cryptococcus spp. using mNGS detection. The cost of mNGS was expensive, and the time performance was not as good as India ink and CrAg testing. Therefore, mNGS was no longer suitable as a diagnostic tool for CNS cryptococcosis after antifungal drug exposure, with a significant decrease in sensitivity.
Our research has several limitations. First, this retrospective, single-center study had a limited sample size, which may have introduced statistical bias. Therefore, a large-scale multicenter prospective study is warranted to further elucidate the diagnostic utility of mNGS in CNS cryptococcosis. Second, the study’s conclusion may be influenced by the inconsistent duration of antifungal exposure during sample collection. Consistent sampling intervals are essential for future studies. Furthermore, CrAg was only tested qualitatively, however, the specific titer was unclear.
Conclusion
The diagnostic performance of conventional tests (including India ink, CrAg testing, and culture) and mNGS was evaluated for detecting CNS cryptococcosis using CSF. The mNGS was less sensitive than CrAg, however, it was more sensitive than India ink and culture. Before antifungal drug exposure, mNGS and CrAg sensitivity reached 100.0%. After exposure to antifungal drugs, the Cryptococcus spp. detection rate and reads using mNGS significantly decreased, and the sensitivity of mNGS were worse than CrAg and India ink. Therefore, mNGS is an effective tool for diagnosing CNS cryptococcosis using CSF; however, its sensitivity decreases considerably in patients effectively treated with antifungal drugs, CrAg and India ink may be the better detection methods than mNGS.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This investigation was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang University. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Because this was a retrospective observational study, informed consent to participate was waived in accordance with the ethics approval. The patients’ privacy will be kept strictly confidential.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Key R&D Program of China (2022YFC2304500, 2022 YFC2304505) and Zhejiang Province Natural Science Foundation (LY23H200001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stott KE, Loyse A, Jarvis JN, et al. Cryptococcal meningoencephalitis: time for action. Lancet Infect Dis. 2021;21(9):e259–e271. doi:10.1016/S1473-3099(20)30771-4
2. Rajasingham R, Smith RM, Park BJ, et al. Global burden of disease of HIV-associated cryptococcal meningitis: an updated analysis. Lancet Infect Dis. 2017;17:873–881. doi:10.1016/S1473-3099(17)30243-8
3. Rajasingham R, Govender NP, Jordan A, et al. The global burden of HIV-associated cryptococcal infection in adults in 2020: a modelling analysis. Lancet Infect Dis. 2022;22(12):1748–1755. doi:10.1016/S1473-3099(22)00499-6
4. Abassi M, Boulware DR, Rhein J. Cryptococcal Meningitis: diagnosis and Management Update. Curr Trop Med Rep. 2015;2(2):90–99. doi:10.1007/s40475-015-0046-y
5. Kambugu A, Meya DB, Rhein J, et al. Outcomes of cryptococcal meningitis in Uganda before and after the availability of highly active antiretroviral therapy. Clin Infect Dis. 2008;46:1694–1701. doi:10.1086/587667
6. Boulware DR, Rolfes MA, Rajasingham R, et al. Multisite validation of cryptococcal antigen lateral flow assay and quantification by laser thermal contrast. Emerg Infect Dis. 2014;20:45–53. doi:10.3201/eid2001.130906
7. Makadzange AT, McHugh G. New approaches to the diagnosis and treatment of cryptococcal meningitis. Semin Neurol. 2014;34(1):47–60. doi:10.1055/s-0034-1372342
8. Góralska K, Blaszkowska J, Dzikowiec M. Neuroinfections caused by fungi. Infection. 2018;46(4):443–459. doi:10.1007/s15010-018-1152-2
9. Rajasingham R, Wake RM, Beyene T, Katende A, Letang E, Boulware DR. Cryptococcal meningitis diagnostics and screening in the era of point-of-care laboratory testing. J Clin Microbiol. 2019;57(1):e01238–18. doi:10.1128/JCM.01238-18
10. Temfack E, Rim JJB, Spijker R, et al. Cryptococcal antigen in serum and cerebrospinal fluid for detecting cryptococcal meningitis in adults living with human immunodeficiency virus: systematic review and meta-analysis of diagnostic test accuracy studies. Clin Infect Dis. 2021;72(7):1268–1278. doi:10.1093/cid/ciaa1243
11. Chiang AD, Dekker JP. From the pipeline to the bedside: advances and challenges in clinical metagenomics. J Infect Dis. 2020;221(Suppl 3):S331–S340. doi:10.1093/infdis/jiz151
12. Simner PJ, Miller S, Carroll KC. Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases. Clin Infect Dis. 2018;66(5):778–788. doi:10.1093/cid/cix881
13. Zhang X, Chen H, Han D, Wu W. Clinical usefulness of metagenomic next-generation sequencing for Rickettsia and Coxiella burnetii diagnosis. Eur J Clin Microbiol Infect Dis. 2023;42(6):681–689. doi:10.1007/s10096-023-04586-w
14. Zhang Y, Cui P, Zhang HC, et al. Clinical application and evaluation of metagenomic next-generation sequencing in suspected adult central nervous system infection. J Transl Med. 2020;18(1):199. doi:10.1186/s12967-020-02360-6
15. Wilson MR, Sample HA, Zorn KC, et al. Clinical metagenomic sequencing for diagnosis of meningitis and encephalitis. N Engl J Med. 2019;380(24):2327–2340. doi:10.1056/NEJMoa1803396
16. Ramachandran PS, Ramesh A, Creswell FV, et al. Integrating central nervous system metagenomics and host response for diagnosis of tuberculosis meningitis and its mimics. Nat Commun. 2022;13(1):1675. doi:10.1038/s41467-022-29353-x
17. Xing XW, Zhang JT, Ma YB, Zheng N, Yang F, Yu SY. Apparent performance of metagenomic next-generation sequencing in the diagnosis of cryptococcal meningitis: a descriptive study. J Med Microbiol. 2019;68(8):1204–1210. doi:10.1099/jmm.0.000994
18. Gan Z, Liu J, Wang Y, et al. Performance of metagenomic next-generation sequencing for the diagnosis of cryptococcal meningitis in HIV-negative patients. Front Cell Infect Microbiol. 2022;12:831959. doi:10.3389/fcimb.2022.831959
19. Jin K, Wang X, Qin L, et al. Nanopore sequencing of cerebrospinal fluid of three patients with cryptococcal meningitis. Eur J Med Res. 2022;27(1):1. doi:10.1186/s40001-021-00625-4
20. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
21. Han D, Yu F, Zhang D, et al. The real-world clinical impact of plasma mNGS testing: an observational study. Microbiol Spectr. 2023;11(2):e398322. doi:10.1128/spectrum.03983-22
22. Jarvis JN, Bicanic T, Loyse A, et al. Determinants of mortality in a combined cohort of 501 patients with HIV-associated cryptococcal meningitis: implications for improving outcomes. Clin Infect Dis. 2014;58:736–745. doi:10.1093/cid/cit794
23. Liu ZY, Wang GQ, Zhu LP, et al. <atl>Expert consensus on the diagnosis and treatment of cryptococcal meningitis. Zhonghua Nei Ke Za Zhi. 2018;57(5):317–323. doi:10.3760/cma.j.issn.0578-1426.2018.05.003.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diagnosis of Mycoplasma hominis Meningitis with Metagenomic Next-Generation Sequencing: A Case Report
Dong Y, He Y, Zhou X, Lv X, Huang J, Li Y, Qian X, Hu F, Zhu J
Infection and Drug Resistance 2022, 15:4479-4486
Published Date: 12 August 2022
Exploring the Spectrum of Microbiota in Central Nervous System Infections Through Metagenomic Next-Generation Sequencing
Wang JM, Pan YY, Hong JC, Jiang ZJ, Zhang SY, Fan RJ, Yang BH, Wang ZQ, Zhu JT, Yao XP
Infection and Drug Resistance 2025, 18:6019-6033
Published Date: 17 November 2025