Back to Journals » International Medical Case Reports Journal » Volume 18
Diagnostic and Management Challenges of Rheumatoid Arthritis-Associated Interstitial Lung Disease in a Ugandan Patient: A Case Report
Authors Adan AH, Hirsi Snr AM ![]() , Jayte M
, Jayte M
Received 18 June 2025
Accepted for publication 26 November 2025
Published 10 December 2025 Volume 2025:18 Pages 1569—1573
DOI https://doi.org/10.2147/IMCRJ.S547951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Abshir Hassan Adan, Abishir Mohamud Hirsi Snr, Mohamed Jayte
Department of Internal Medicine, Kampala International University, Kampala, Uganda
Correspondence: Mohamed Jayte, Internal Medicine Department at Kampala International University, Kampala, P.O. Box 7062, Uganda, Tel +256 55272543, Email [email protected]
Introduction: Rheumatoid arthritis (RA)-associated interstitial lung disease (ILD) is a serious complication of RA, characterized by progressive pulmonary fibrosis. Diagnosing and managing RA-ILD can be particularly challenging in resource-limited settings, where access to advanced diagnostic tools and treatment options may be limited. Early detection and intervention are critical for improving outcomes.
Case Presentation: A 40-year-old female with a six-year history of RA (rheumatoid factor positive) presented with a three-month history of worsening cough, shortness of breath, and chest pain. On examination, she exhibited signs of respiratory distress and digital clubbing. Baseline oxygen saturation was 81% on 5 L/min supplemental oxygen. Chest X-ray revealed bilateral reticular opacities, while a CT scan showed bilateral fibrotic changes and ground-glass opacities, suggestive of an NSIP-like pattern, although formal HRCT classification could not be confirmed. Anti-CCP testing and pulmonary function tests were unavailable due to resource limitations. The patient was managed with supplemental oxygen therapy, corticosteroids, and methotrexate, along with lifestyle modifications and pulmonary rehabilitation. Follow-up over two months showed marked symptomatic improvement.
Conclusion: This case emphasizes the challenges of diagnosing and managing RA-associated ILD in resource-limited settings. It highlights the importance of clinical suspicion, pragmatic use of available resources, and the need to strengthen diagnostic capacity in low-resource environments.
Keywords: interstitial lung disease, rheumatoid arthritis, respiratory complications, case report, Uganda
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disease that primarily affects the joints but is also associated with extra-articular manifestations, including interstitial lung disease (ILD). ILD, one of the most severe pulmonary complications of RA, has a prevalence ranging from 5% to 10% in RA patients globally, though estimates vary by population and methodology used in detection.1 RA-ILD is characterized by inflammatory and fibrotic changes in the lung parenchyma, leading to a progressive decline in respiratory function, with nonspecific interstitial pneumonia (NSIP) and usual interstitial pneumonia (UIP) being the most common histopathologic patterns.2
The incidence and clinical course of RA-ILD are influenced by factors such as smoking, age, and serologic status.3,4 In Africa, and Uganda in particular, little data is available on RA-associated ILD, partly due to limited access to advanced diagnostic tools like high-resolution computed tomography (HRCT).4,5 This case highlights the diagnostic and management challenges of RA-ILD in Uganda, where health resources are constrained and suggests the need for improved awareness and early diagnosis to optimize patient outcomes.
RA-ILD is estimated to occur in up to 10% of patients with RA, with smoking, older age, and seropositivity being major risk factors.3,5 Recent guidelines (ATS/ERS 2018; ERJ 2019) emphasize HRCT pattern recognition and antifibrotic therapy in management.6 In sub-Saharan Africa, however, the lack of HRCT and biologics significantly limits diagnosis and treatment, making individual case documentation important for awareness.
Recent large cohort studies and guidelines have advanced understanding of RA-ILD, identifying UIP and NSIP as prognostically distinct patterns, with UIP conferring poorer survival.5,6 Antifibrotics such as nintedanib are now recommended in progressive fibrosing ILD, including RA-ILD.7–9 However, these advances remain largely inaccessible in African settings, where HRCT and antifibrotics are rarely available. This context justifies case documentation to draw attention to both clinical and systemic challenges.
Documenting such cases in Uganda is important because the true prevalence of RA-ILD is unknown, and underdiagnosis is likely due to limited access to HRCT and specialist care. A case study approach is justified in this context as it allows detailed documentation of the diagnostic reasoning and management pathway in a resource-limited setting, highlighting both systemic challenges and potential lessons for similar environments.
Case History/Examination
A 40-year-old Ugandan woman, diagnosed with RA six years prior, presented to Kayunga Regional Referral Hospital with a three-month history of dry cough, shortness of breath upon exertion, and intermittent chest pain. She reported no fever, night sweats, or recent infections. Her medical history was notable for RA without prior respiratory disease, and there was no history of smoking or alcohol use. She worked as a farmer and had no family history of chronic respiratory or autoimmune diseases.
Clinical Examination
On examination, the patient appeared acutely ill, requiring 5 liters of supplemental oxygen to maintain oxygen saturation. She had grade 2 digital clubbing and mild bilateral lower limb edema. Her vital signs were as follows: blood pressure 135/82 mmHg, pulse rate 102 beats per minute, respiratory rate 30 breaths per minute, oxygen saturation 81% on oxygen, and temperature 37°C. Respiratory examination revealed bilateral coarse crackles in the upper and lower lung zones, with decreased chest expansion bilaterally.
Diagnostic Evaluation
Due to resource constraints, the diagnostic options available for the patient were limited. A complete blood count was performed and found to be within normal limits, providing no additional evidence for an underlying infection or hematologic abnormalities. The chest X-ray (Figure 1) revealed a bilateral reticular pattern, which suggested interstitial pneumonitis, a potential sign of lung involvement in rheumatoid arthritis (RA). A more detailed CT angiography (Figure 2) with contrast was conducted, showing bilateral fibrotic changes and ground-glass opacities, which are characteristic of interstitial lung disease (ILD). These imaging findings were consistent with interstitial pneumonitis, supporting the diagnosis of RA-associated ILD. Additionally, the patient tested positive for rheumatoid factor (RF), which further reinforced the clinical suspicion of ILD related to RA. The combination of the patient’s clinical presentation, imaging findings, and known history of rheumatoid arthritis led to the diagnosis of RA-associated ILD.
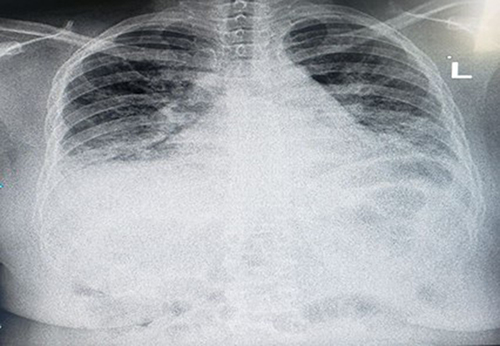 |
Figure 1 Chest Xray showed nodular reticular pattern of both lung fields. |
 |
Figure 2 Showing CTA with contrast showing fibrotic lung, ground glass appearance suggestive of interstitial pneumonitis with Positive RF, Rheumatoid Arthritis patients. |
Further diagnostic work-up was limited by unavailability of anti-CCP testing, pulmonary function testing (PFT/DLCO), and serial HRCT follow-up. These limitations constrained our ability to fully characterize disease severity and trajectory.
Management
Managing RA-ILD is complex, particularly in resource-constrained settings. For this patient, a combination of corticosteroids and conservative care was implemented, along with antifibrotic and immunosuppressive therapy to manage the lung fibrosis and halt disease progression.
The patient was initially placed on supplemental oxygen to address hypoxia and alleviate respiratory distress. She was prescribed a moderate dose of corticosteroids to control inflammation, which is commonly associated with rheumatoid arthritis-related interstitial lung disease (RA-ILD).
Considering her persistent respiratory symptoms and fibrosis on imaging, an antifibrotic agent, such as nintedanib, was introduced to slow the progression of lung fibrosis. Additionally, low-dose methotrexate, a standard immunosuppressant, was added to her regimen to control RA and prevent further joint and lung damage. Given the potential adverse effects, her liver and kidney functions were closely monitored.
The patient was also advised on pulmonary rehabilitation exercises to improve lung capacity and reduce breathlessness. Lifestyle modifications, including avoiding environmental respiratory irritants and maintaining a balanced diet, were emphasized to support her recovery.
Outcome and Follow-Up
Two-Week Follow-Up
At her two-week follow-up, the patient reported some improvement in breathlessness and cough. Her oxygen saturation was stable with supplemental oxygen, and she was tolerating corticosteroids and methotrexate without adverse effects. Blood tests showed no abnormalities in liver or renal functions. The patient was encouraged to continue with her medications and pulmonary exercises.
One-Month Follow-Up
After one month, the patient showed notable improvement. Her need for supplemental oxygen decreased, and she experienced less dyspnea on exertion. The corticosteroid dose was gradually tapered, and her response to antifibrotic therapy was positive, with no signs of disease exacerbation. Methotrexate was continued, with regular monitoring of blood parameters. The patient’s adherence to pulmonary rehabilitation exercises appeared to support her respiratory function.
Two-Month Follow-Up
At her two-month follow-up, the patient was significantly improved, requiring no supplemental oxygen at rest. She reported minimal cough and no significant dyspnea with daily activities. Physical examination revealed stable respiratory function, and her vital signs remained within normal limits. She was advised to continue methotrexate at a maintenance dose, and corticosteroids were tapered further. Pulmonary rehabilitation and lifestyle modifications remained an essential part of her ongoing care plan.
Discussion
This study presents a case of interstitial lung disease (ILD) in a 40-year-old Ugandan woman with a six-year history of rheumatoid arthritis (RA). The patient, who presented with a persistent cough, exertional dyspnea, and chest pain, was diagnosed with RA-related interstitial lung disease (RA-ILD) after imaging studies revealed fibrotic changes and ground-glass opacities consistent with nonspecific interstitial pneumonia (NSIP), a common subtype of RA-ILD. This case underscores the need for heightened clinical suspicion and timely diagnosis of RA-ILD, especially in resource-limited settings where access to advanced diagnostic tools may be restricted.
RA-ILD is a significant extra-articular manifestation of RA, with an incidence reported between 5% to 10% among RA patients.5 The most common subtypes are usual interstitial pneumonia (UIP) and nonspecific interstitial pneumonia (NSIP), both of which are characterized by progressive fibrosis and declining pulmonary function.5 In this case, the patient’s CT findings of fibrotic changes and ground-glass opacities are typical of the NSIP pattern associated with RA.6
Contemporary literature emphasizes that HRCT pattern recognition (UIP vs NSIP) has prognostic value, with UIP associated with a 3–5 year median survival and NSIP more favorable outcomes.5,6 Antifibrotics such as nintedanib have shown benefit in slowing disease progression in progressive fibrosing ILDs, including RA-ILD.9 These were not accessible in our setting. Our discussion is therefore limited to symptomatic and immunosuppressive management. Limitations of this case include absence of anti-CCP testing, lack of PFT/DLCO measurements, inability to confirm HRCT-based pattern, no follow-up imaging, and incomplete exclusion of alternative causes such as infection or environmental exposures. Despite these limitations, this case contributes a valuable perspective on real-world management in resource-limited settings.
A study by Kelly et al emphasized that the presence of ILD in RA patients is associated with poor prognosis, with a 10-year mortality rate reaching up to 50%.6 The study also highlighted that seropositivity for rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies is significantly associated with an increased risk of ILD in RA patients. While our patient was RF-positive, limitations in testing prevented us from assessing anti-CCP, highlighting a gap in resource-limited settings where diagnostic capabilities are restricted.
Moreover, RA-ILD remains underreported in many African countries, likely due to limited access to diagnostic tools such as high-resolution computed tomography (HRCT) and a lack of awareness among healthcare providers.6 A study from South Africa revealed that only a small percentage of RA patients were screened for ILD, contributing to underdiagnosis and delayed treatment.7 This case adds to the growing recognition of RA-ILD in African patients and emphasizes the need for increased clinical awareness and improved access to diagnostic resources.
Management of RA-ILD typically involves immunosuppressive therapies such as corticosteroids, disease-modifying anti-rheumatic drugs (DMARDs), and biologic agents targeting pro-inflammatory cytokines. However, in resource-limited settings, these treatments are often inaccessible. Studies suggest that early intervention with corticosteroids and DMARDs may help slow the progression of fibrosis in RA-ILD, but in this case, the patient only received corticosteroids due to the unavailability of advanced therapies.8 Pulmonary rehabilitation and regular monitoring of pulmonary function are additional interventions that have been shown to improve outcomes in RA-ILD patients.1,8
In settings like Uganda, where healthcare resources are limited, the focus of management often shifts to symptomatic care and prevention of disease progression through lifestyle modifications. Improving access to diagnostic tools like HRCT and increasing healthcare providers’ awareness of RA-ILD are crucial steps toward earlier diagnosis and more effective intervention.9
In high-income countries, advanced therapies such as methotrexate, rituximab, and TNF inhibitors are commonly employed to manage RA-ILD, though their use requires careful monitoring due to the risk of adverse effects.5,9 However, the applicability of these therapies in sub-Saharan Africa is limited by high costs and limited availability. As awareness and resources improve in the region, future research could focus on developing cost-effective, region-specific treatment protocols that can be used safely in low-resource settings.
Conclusion
This case demonstrates that clinicians must maintain a high index of suspicion for ILD in RA patients presenting with unexplained respiratory symptoms. In low-resource settings, where HRCT and biologics are inaccessible, pragmatic use of chest radiography, clinical judgment, and supportive therapy can still yield meaningful improvement. Beyond clinical practice, the case highlights the need for health system strengthening in Africa to improve access to advanced diagnostics and therapies, and calls for regional research to develop cost-effective approaches for RA-ILD.
Key Clinical Message
Rheumatoid arthritis-associated interstitial lung disease (RA-ILD) poses significant diagnostic and management challenges in resource-limited settings. Early recognition through clinical and imaging findings, combined with timely symptomatic management, can improve patient outcomes even in constrained environments.
Ethical Approval
Ethical approval to report this case was obtained from the Ethics Committee at Kayunga Regional Referral Hospital (Approval Number: KRRH-EC-2024-011). In addition, Kayunga Regional Referral Hospital provided institutional approval for the publication of the case details.
Consent For Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest associated with this study.
References
1. Assayag D, Elicker BM, Urbania TH, et al. Rheumatoid arthritis-associated interstitial lung disease: radiologic identification of usual interstitial pneumonia pattern. Radiology. 2014;270:583–588. doi:10.1148/radiol.13130187
2. Olson AL, Swigris JJ, Sprunger DB, et al. Rheumatoid arthritis-interstitial lung disease-associated mortality. Am J Respir Crit Care Med. 2011;183:372–378. doi:10.1164/rccm.201004-0622OC
3. Bongartz T, Nannini C, Medina-Velasquez YF, et al. Incidence and mortality of interstitial lung disease in rheumatoid arthritis - A population-based study. Arthritis Rheum. 2010;62:1583–1591. doi:10.1002/art.27405
4. Zamora-Legoff JA, Krause ML, Crowson CS, Ryu JH, Matteson EL. Patterns of interstitial lung disease and mortality in rheumatoid arthritis. Rheumatology. 2017;56. doi:10.1093/rheumatology/kew391
5. Spagnolo P, Lee JS, Sverzellati N, Rossi G, Cottin V. The lung in rheumatoid arthritis: focus on interstitial lung disease. Arthritis Rheumatol. 2018;70(10):1544–1554. doi:10.1002/art.40574
6. Jacob J, Hirani N, Van Moorsel CHM, et al. Predicting outcomes in rheumatoid arthritis related interstitial lung disease. Eur Respir J. 2019;53(1):1800869. doi:10.1183/13993003.00869-2018
7. Nurmi HM, Purokivi MK, Kärkkäinen MS, Kettunen HP, Selander TA, Kaarteenaho RL. Variable course of disease of rheumatoid arthritis-associated usual interstitial pneumonia compared to other subtypes. BMC Pulm Med. 2016;16. doi:10.1186/s12890-016-0269-2
8. Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis An Official ATS/ERS/JRS/ALAT Clinical practice guideline. Am J Respir Crit Care Med. 2018;198:e44–e68. doi:10.1164/rccm.201807-1255ST
9. Flaherty KR, Wells AU, Cottin V, et al. Nintedanib in PROGRESSIVE FIBROSING INTERSTITIAL LUNG DISEases. New England Journal of Medicine. 2019;381:1718–1727. doi:10.1056/nejmoa1908681
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Rapidly Progressive Felty Syndrome After Sudden Discontinuation of Methotrexate: A Case Report and Review of Literature
Hamsho S, Alannouf I, Ashour AA
International Medical Case Reports Journal 2022, 15:473-477
Published Date: 2 September 2022
Overview on the Link Between the Complement System and Auto-Immune Articular and Pulmonary Disease
Triggianese P, Conigliaro P, De Martino E, Monosi B, Chimenti MS
Open Access Rheumatology: Research and Reviews 2023, 15:65-79
Published Date: 15 May 2023
Clinical Features and Prognosis of Double-Positive Anti-MDA5 and Anti-CCP Antibodies in Dermatomyositis: A Retrospective Study
Xu X, Zhu L, Li S, Wang G, Ge Y
Journal of Inflammation Research 2025, 18:1929-1939
Published Date: 10 February 2025
The Value of NLR and PLR in the Diagnosis of Rheumatoid Arthritis Combined with Interstitial Lung Disease and Assessment of Treatment Effect: A Retrospective Cohort Study
Cui P, Cheng T, Yan H, Xu D, Ren G, Ma S
International Journal of General Medicine 2025, 18:867-880
Published Date: 19 February 2025
From Gut to Lung: The Role of Bile Acids in Rheumatoid Arthritis-Associated Interstitial Lung Disease (RA-ILD)
Shi YJ, Lin S, Shi YC, Xie J
Journal of Inflammation Research 2025, 18:10331-10340
Published Date: 2 August 2025