Back to Journals » Advances in Medical Education and Practice » Volume 17
Diagnostic Accuracy and Educational Value of the RIPASA Score in Suspected Acute Appendicitis: A Prospective Study in an Emergency Department Training Setting
Authors Zaouche K ![]() , Chamekh S, Yousfi R, Saidani A, Rezgui E
, Chamekh S, Yousfi R, Saidani A, Rezgui E ![]() , Kallel E, El Ayech F, Chebbi F, Kallel M
, Kallel E, El Ayech F, Chebbi F, Kallel M
Received 27 January 2026
Accepted for publication 10 March 2026
Published 30 March 2026 Volume 2026:17 593782
DOI https://doi.org/10.2147/AMEP.S593782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Khedija Zaouche,1 Sourour Chamekh,2 Rahma Yousfi,3 Ahmed Saidani,3 Emna Rezgui,1 Emna Kallel,1 Fedia El Ayech,1 Faouzi Chebbi,3 Manel Kallel1
1Emergency Department, Mahmoud El Matri Hospital, Faculty of Medicine of Tunis, University of Tunis El Manar, Tunis, Tunisia; 2Faculty of Medicine of Tunis, University of Tunis El Manar, Tunis, Tunisia; 3Surgery Department, Mahmoud El Matri Hospital, Faculty of Medicine of Tunis, University of Tunis El Manar, Tunis, Tunisia
Correspondence: Khedija Zaouche, Emergency Department, Mahmoud El Matri Hospital, Faculty of Medicine of Tunis, University of Tunis El Manar, Tunis, Tunisia, Tel +216.29873030, Email [email protected]
Background: Clinical scoring systems are increasingly used in emergency departments for decision support and risk stratification. This prospective observational study evaluated the diagnostic performance of the RIPASA score in suspected acute appendicitis and explored its potential role as a structured decision-support tool within a training environment.
Methods: We conducted a prospective observational study in a university emergency department including patients aged ≥ 18 years presenting with suspected acute appendicitis. The RIPASA score was calculated during routine clinical assessment by physicians with varying levels of experience. Histopathological findings served as the reference standard for operated patients, while non-operated patients were followed for one month. Diagnostic performance was assessed using receiver operating characteristic analysis.
Results: Among 135 included patients (median age 28 years), acute appendicitis was confirmed in 55 cases (40.7%). The RIPASA score demonstrated moderate diagnostic accuracy, with an area under the curve of 0.79 (95% CI, 0.72– 0.87). The negative predictive value in the low-probability group reached 86.4%, whereas the positive predictive value in the high-probability group was 67.4%.
Conclusion: The RIPASA score demonstrated moderate diagnostic performance for risk stratification in suspected acute appendicitis. While it may support structured clinical reasoning in training settings, it should not be used as a standalone tool for discharge decisions.
Plain Language Summary: Clinical scoring systems help emergency doctors make decisions and train junior staff. This study evaluated the RIPASA score in patients with suspected appendicitis to see how well it works as a diagnostic and teaching tool. The score successfully grouped patients into low and high-risk categories. However, it was not reliable enough to be used alone to send patients home without further clinical review or tests. These results suggest that the RIPASA score provides a helpful structure for teaching clinical reasoning to young doctors, though more research is needed to measure its full educational impact.
Keywords: appendicitis, clinical decision support, emergency medicine, medical education, risk assessment
Introduction
Acute appendicitis is one of the most common abdominal surgical emergencies worldwide, with a lifetime risk estimated at 6.7–8.6%.1 Although diagnosis is primarily based on clinical assessment, definitive confirmation relies on histopathological findings. Atypical presentations are frequent and represent a major source of diagnostic uncertainty, particularly for physicians in training.2 In high-volume emergency departments, this uncertainty may result in unnecessary imaging, delayed diagnosis, or inappropriate discharge decisions.
To address these challenges, several clinical scoring systems have been developed to structure diagnostic reasoning and optimize the use of diagnostic resources.3 Among them, the Alvarado and modified Alvarado scores remain widely used. However, systematic reviews and meta-analyses have demonstrated variability in their diagnostic accuracy across different populations and clinical settings.4,5 Differences in demographic characteristics and symptom presentation may limit their reliability, particularly outside Western contexts.
The RIPASA score, introduced in 2010, incorporates additional demographic and clinical parameters intended to improve diagnostic performance across diverse populations.6 It has demonstrated high sensitivity and specificity in both Asian and Western settings7 and may therefore offer improved applicability in resource-constrained emergency departments. Beyond diagnostic performance, structured clinical scores may also support systematic assessment and supervised clinical reasoning in training environments. However, data regarding the applicability and potential educational relevance of the RIPASA score in North African emergency departments remain limited.
The objective of this study was to evaluate the diagnostic performance of the RIPASA score and to explore its role as a structured decision-support tool for risk stratification and discharge planning in an emergency department training setting.
Methods
Ethics Statement
The study was approved by the Ethics Committee of Mahmoud El Matri Hospital (Ariana, Tunisia), the clinical institution where the study was conducted and where patient data were collected (approval number 11/2023). The committee operates independently of the universities with which the authors are affiliated. The study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants, and patient confidentiality and data protection were ensured throughout the study.
Study Design
This was a prospective observational study.
Setting
The study was conducted in a university-affiliated emergency department in Tunis, Tunisia, between October 1, 2022, and March 31, 2023. The department serves as a clinical training site for emergency medicine and family medicine residents.
Participants
Patients aged 18 years or older presenting with abdominal pain suggestive of acute appendicitis were eligible for inclusion. Exclusion criteria included post-traumatic abdominal pain, pregnancy, shock, and incomplete clinical evaluation.
Variables
The primary outcome was the final diagnosis of acute appendicitis, established by histopathological examination, which served as the reference standard for operated patients. Secondary outcomes included the diagnostic performance of the RIPASA score and its clinical utility as an educational and decision-support tool to exclude acute appendicitis in patients classified as low risk.
Data Sources and Measurement
Clinical data were collected prospectively using a standardized form during routine patient care. The RIPASA score was calculated during the initial clinical assessment by physicians with varying levels of experience. In addition to its diagnostic purpose, the score was used as a structured educational tool to support clinical reasoning among physicians in training by encouraging a systematic evaluation of symptoms, physical findings, and laboratory results.
The RIPASA score was calculated based on 14 clinical and laboratory parameters, as detailed in Figure 1. In accordance with previously published thresholds,5–7 the RIPASA score was interpreted as follows: a score <5 indicated a low probability of acute appendicitis, scores between 5 and 7 a moderate probability, and scores ≥7 a high probability.
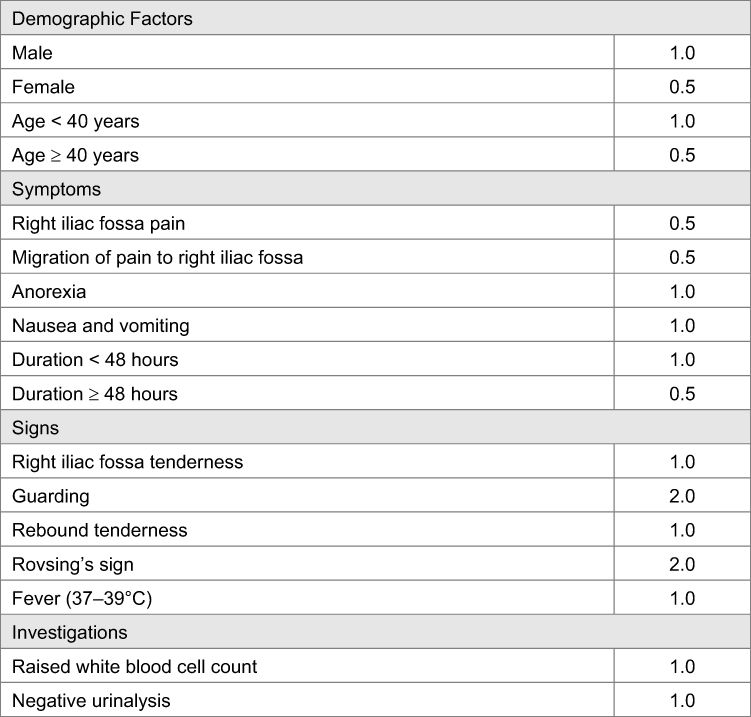 |
Figure 1 Components of the RIPASA scoring system. |
The score was used to assist diagnostic decision-making and to evaluate the feasibility of safe discharge from the emergency department. Patients in whom acute appendicitis was considered unlikely were discharged with written instructions for home surveillance. A follow-up phone call was conducted within one month to identify any subsequent emergency visits, hospital admissions, or surgical interventions.
Bias
Variability in clinical assessment and RIPASA score calculation related to differences in physician experience was considered a potential source of bias. No formal interobserver agreement analysis was performed. However, the score was calculated according to predefined objective criteria, and physicians were familiarized with the scoring system prior to study initiation, reflecting routine practice in a teaching emergency department.
Study Size
Sample size was calculated using Buderer’s method, based on expected sensitivity, specificity, and disease prevalence. Institutional data estimated the prevalence of acute appendicitis among patients presenting with abdominal pain at 15%. Using pooled sensitivity (0.95) and specificity (0.71) values from a recent meta-analysis of the RIPASA score,5 and assuming a confidence interval width of ±10%, the required sample size was determined using the larger estimate derived from sensitivity and specificity calculations. This resulted in a minimum sample size of 122 patients.
Statistical methods
Statistical analyses were performed using SPSS version 20. Quantitative variables were expressed as means ± standard deviations or medians with interquartile ranges, as appropriate, while qualitative variables were expressed as frequencies and percentages. Diagnostic performance was assessed using sensitivity, specificity, positive and negative predictive values, and receiver operating characteristic (ROC) curve analysis with calculation of the area under the curve (AUC). Diagnostic accuracy indices were calculated focusing on extreme probability categories (low <5 and high >7) to assess the rule-out and rule-in performance of the score. Patients in the intermediate probability group (score 5–7) were excluded from these specific analyses because this category represents diagnostic uncertainty and cannot be reliably classified as either positive or negative. Their distribution is reported separately to ensure transparency and to minimize potential spectrum bias. This study is reported in accordance with the STROBE statement for observational studies (Supplementary Material 1).
Results
Participants
A total of 135 patients were included in the analysis. Figure 2 illustrates the study flow. Acute appendicitis was confirmed in 55 of the 135 included patients (40.7%).
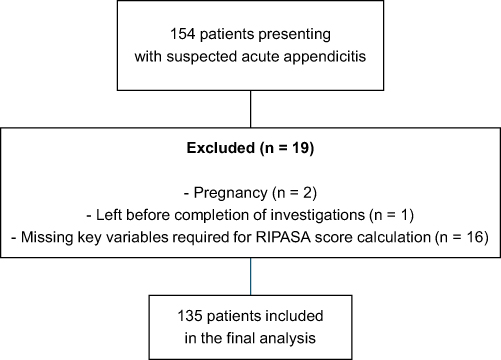 |
Figure 2 Flowchart of the study. |
Main results
The sex ratio was 0.43. The median age of the patients was 28 years (range 13–70 years), with an interquartile range (IQR 25–75) of [22–40]. The median temperature was 36.9°C (range 36–40°C; IQR [36.6–37.6]). Duration of symptoms was less than 48 hours in 61.5% of patients.
On physical examination, right iliac fossa pain was observed in 91% of patients, Blumberg’s sign was positive in 12%, Rovsing’s sign in 14.8%, and guarding in 8%.
The median white blood cell (WBC) count was 9150 cells/mm3 (interquartile range [7,540–12,370]).
Table 1 presents the distribution of patients according to RIPASA probability categories. Forty-four patients (32.6%) were classified as low probability (<5), 48 (35.6%) as intermediate probability (5–7), and 43 (31.9%) as high probability (>7).
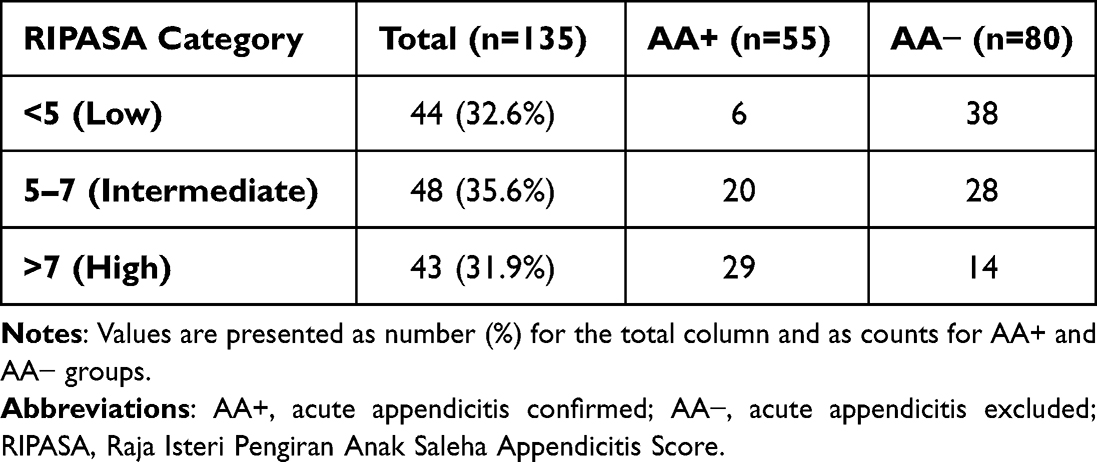 |
Table 1 Distribution of Patients According to RIPASA Probability Categories |
Abdominal ultrasound was performed in 52 patients, confirming the diagnosis in 21 cases and excluding it in 16. In 15 patients with inconclusive ultrasound results, a complementary abdominal CT scan was conducted, confirming the diagnosis in 9 cases and excluding it in 8. Additionally, 46 patients underwent abdominal CT as the initial imaging modality, resulting in 20 confirmed cases and 16 exclusions. Overall, radiological imaging confirmed acute appendicitis in 50 patients.
Surgery was performed in 55 patients with histologically confirmed acute appendicitis. Among the remaining patients, 54 were discharged with alternative, non-serious diagnoses explaining their abdominal pain, and 26 were discharged due to low suspicion of appendicitis and followed up. No cases of appendicitis were identified during follow-up in discharged patients. Table 2 summarizes alternative diagnoses among patients without acute appendicitis.
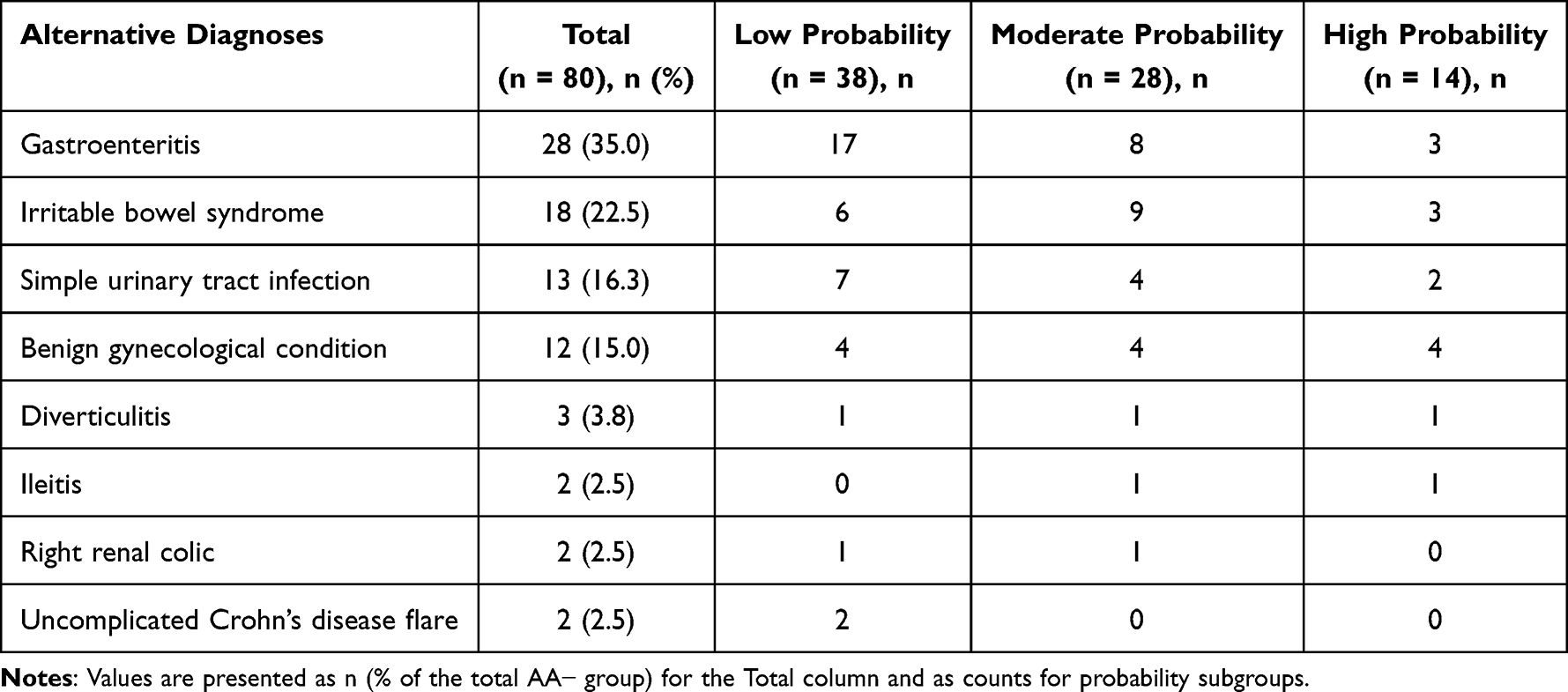 |
Table 2 Alternative Diagnoses Among Patients Without Acute Appendicitis According to RIPASA Probability Groups |
Table 3 compares clinical characteristics between patients with and without acute appendicitis.
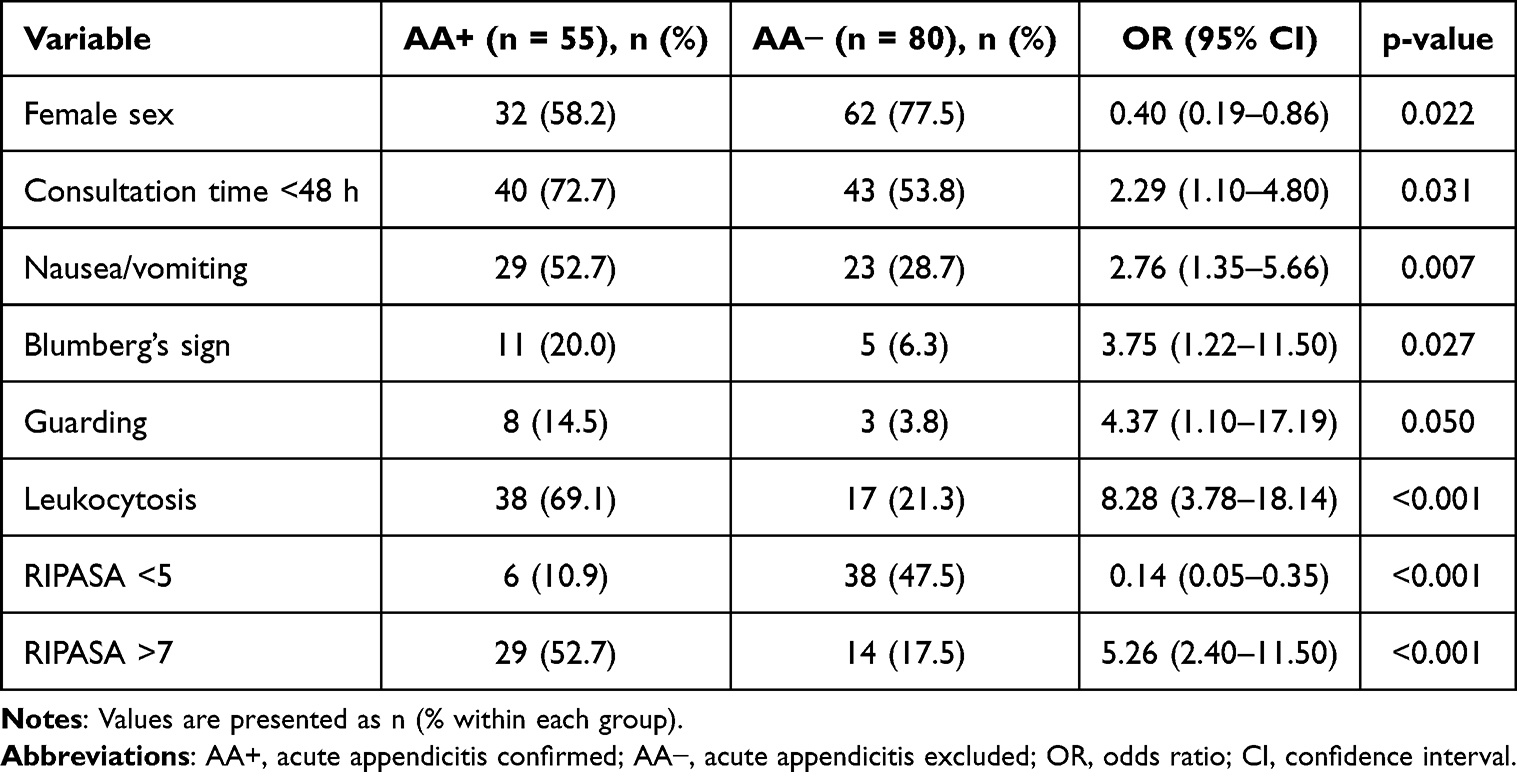 |
Table 3 Comparison of Clinical Characteristics Between Patients with and without Acute Appendicitis |
The RIPASA score demonstrated moderate diagnostic accuracy. Figure 3 illustrates the ROC curve analysis, showing an area under the curve (AUC) of 0.79 (95% CI [0.72–0.87], p<0.001). When evaluating its clinical utility for decision-making, the score showed a high negative predictive value (NPV) of 86.4% in the low-probability group (<5), supporting its role in helping to exclude acute appendicitis. Conversely, in the high-probability group (>7), the score achieved a positive predictive value (PPV) of 67.4%, providing a useful tool for risk confirmation. Detailed diagnostic performance indices, including sensitivity and specificity for each category, are reported in Table 4.
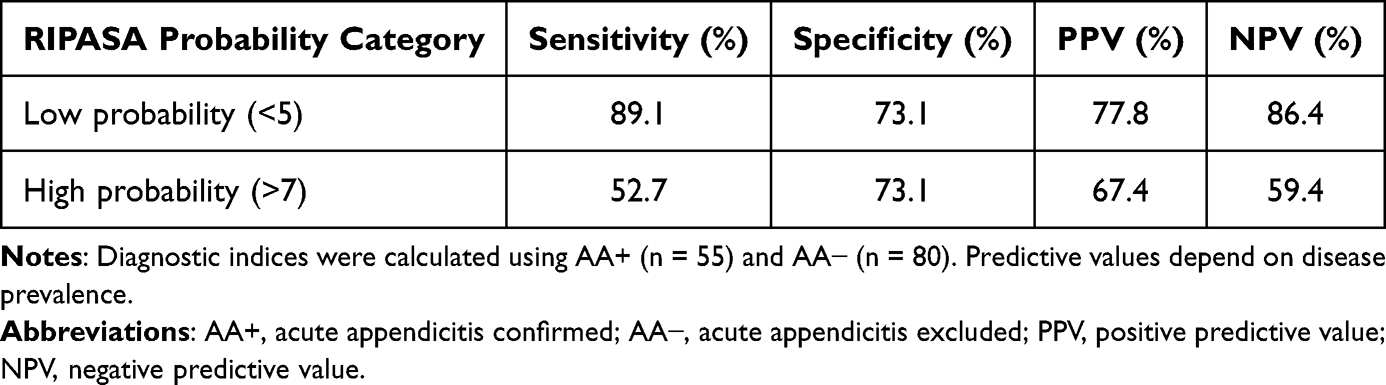 |
Table 4 Diagnostic Accuracy of the RIPASA Score According to Probability Categories |
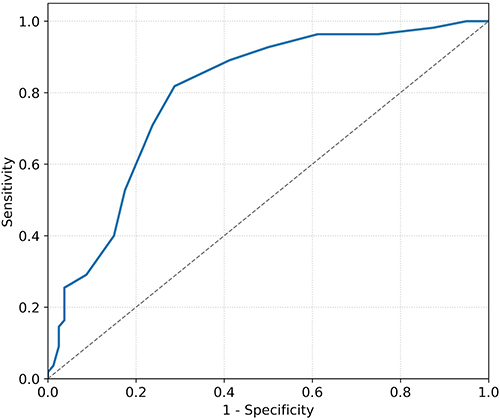 |
Figure 3 The ROC curve of RIPASA SCORE. |
From an educational perspective, the RIPASA score appeared to provide a structured framework for categorizing patients into probability groups during initial assessment. However, formal educational outcomes were not directly measured in this study.
Discussion
Diagnostic Performance and Educational Relevance of the RIPASA Score
The primary objective of this study was to evaluate the diagnostic performance of the RIPASA score in suspected acute appendicitis within an emergency department training environment, while also exploring its educational value as a decision-support tool. Our findings indicate that the RIPASA score demonstrated moderate overall diagnostic accuracy, with an area under the ROC curve of 0.79 (95% CI [0.72–0.87]).8,9 Increasing RIPASA scores were associated with a higher likelihood of confirmed acute appendicitis, supporting its role in clinical risk stratification.
In emergency departments, clinical scoring systems serve three complementary purposes: risk stratification, guidance for imaging decisions, and support for discharge planning. In patients classified as low probability, such tools may contribute to reducing unnecessary imaging when combined with repeated clinical evaluation. Conversely, higher scores may support early surgical consultation or prompt advanced imaging. In this context, RIPASA may contribute to more rational use of diagnostic resources, particularly in settings where access to computed tomography is limited.
Although sensitivity decreased slightly at higher cut-off values (>7), specificity improved, suggesting that higher scores may be particularly useful for identifying patients at increased risk of acute appendicitis. These results are consistent with previous studies reporting comparable or superior diagnostic performance of the RIPASA score compared with other commonly used scoring systems, including the Alvarado score.4–6,9,10
Recent high-level evidence further strengthens this interpretation. A contemporary systematic review and meta-analysis evaluating appendicitis scoring systems reported that the RIPASA score demonstrated among the highest pooled diagnostic accuracy compared with traditional clinical scores, although heterogeneity across populations persists.11 These findings enhance the external validity of our results and situate our data within the broader international evidence base.
Population Characteristics and Implications for Diagnostic Complexity
The demographic profile of our cohort was characterized by a median age of 28 years and a predominance of female patients (69.6%). While sex is not considered an independent risk factor for acute appendicitis.12 This female predominance has been similarly reported in Middle Eastern populations13,14 and contrasts with findings from Western Europe and Asia, where male predominance is more common.15,16 These differences likely reflect regional healthcare-seeking behaviors and referral patterns rather than true epidemiological variation.
From a training standpoint, such population characteristics may increase diagnostic complexity, particularly in female patients with overlapping gynecological conditions. This underscores the importance of interpreting clinical scores within the broader clinical context rather than relying solely on numerical thresholds.
Limitations of the RIPASA Score for Exclusion and Discharge Decisions
A key finding of this study was the presence of confirmed acute appendicitis cases within the low-probability RIPASA group. This observation raises important concerns regarding the reliability of the score for safely excluding acute appendicitis. Although RIPASA has been proposed as a tool to reduce unnecessary imaging and hospital admissions, particularly in resource-limited emergency departments, its ability to rule out acute appendicitis remains limited.17,18
With a negative predictive value of 86.4%, the RIPASA score alone does not provide sufficient reassurance to support autonomous discharge decisions in patients classified as low risk. Clinical reassessment, appropriate follow-up instructions, and contextual judgment remain essential components of safe emergency care. These findings reinforce that scoring systems should complement—but not replace—clinical reasoning and supervision.
Educational Considerations in Emergency Medicine Training
In training environments, structured clinical scores such as RIPASA may contribute to making diagnostic reasoning more explicit and reproducible. When appropriately integrated into clinical teaching, the score can facilitate case-based discussions, encourage systematic data gathering, and support reflective decision-making. Structured observation-based educational approaches have been shown to enhance clinical reasoning and reflective practice in medical training, particularly when embedded within guided clinical practice.19 However, the educational implications observed in this study remain interpretative, as formal educational outcomes were not directly measured.
Therefore, while RIPASA may serve as a supportive framework for introducing structured diagnostic reasoning, it should not promote algorithm-driven decision-making detached from clinical judgment. Ongoing mentorship, feedback, and iterative assessment remain central to emergency medicine training.
Limitations and Generalisability
This study has several limitations. Clinical assessments and RIPASA score calculations were performed by physicians from different specialties and with varying levels of experience, which may have introduced interobserver variability. Additionally, the study was conducted in a single center with a relatively small sample size and a predominantly young and female population, potentially limiting generalisability to other emergency department settings.
Despite these limitations, the study reflects real-world emergency practice and provides insight into the strengths and constraints of the RIPASA score when used in a training environment.
Future Perspectives
Future multicenter prospective studies including larger and more diverse populations are needed to improve external validity. Standardized training in RIPASA score calculation may reduce interobserver variability. In addition, combining the RIPASA score with biomarkers or point-of-care ultrasound may enhance diagnostic performance and further support structured clinical reasoning in settings with limited access to advanced imaging.
Conclusion
The RIPASA score demonstrated moderate diagnostic accuracy for suspected acute appendicitis in this emergency department setting. Clinically, while the score supports risk stratification and may guide imaging decisions when integrated with clinical assessment, it does not provide sufficient reliability to be used as a standalone tool for the definitive exclusion of appendicitis or for autonomous discharge decisions.
Regarding its role in medical training, our findings suggest that the structured nature of the RIPASA score may provide a useful framework to facilitate supervised clinical reasoning. However, as formal educational outcomes were not directly measured, these implications remain interpretative. Further prospective studies are required to formally evaluate the impact of such clinical scoring systems on the learning curves and decision-making skills of junior clinicians.
Use of Artificial Intelligence Tools
Artificial intelligence–based tools were used exclusively for language editing and clarity improvement. All content was reviewed and approved by the authors, and the use of these tools did not influence the study design, data analysis, or conclusions.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Guan L, Liu Z, Pan G, et al. The global, regional, and national burden of appendicitis in 204 countries and territories, 1990–2019: a systematic analysis from the Global Burden of Disease Study 2019. BMC Gastroenterol. 2023;23:44. doi:10.1186/s12876-023-02678-7
2. Chaudhary SR, Jeevika, Roy SG. Diagnostic uncertainties and legal precedents in appendicitis malpractice. Acad Radiol. 2025;32(suppl 1):S109–9. doi:10.1016/j.acra.2025.05.034
3. Jayanand D, Jayalal JA, Kumar ASJ, Manovah JA, Vivek MR. Appendicitis inflammatory response score and Alvarado score: comparison with preoperative computed tomography and postoperative histopathology—a prospective cohort study. Int J Surg Open. 2024;54:100708.
4. Dezfuli SAT, Yazdani R, Khorasani M, Hosseinikhah SA. Comparison between the specificity and sensitivity of the RIPASA and Alvarado scoring systems in the diagnosis of acute appendicitis among patients with right iliac fossa pain. AIMS Public Health. 2020;7(1):1–9. doi:10.3934/publichealth.2020001
5. Favara G, Maugeri A, Barchitta M, Ventura A, Basile G, Agodi A. Comparison of RIPASA and Alvarado scores for risk assessment of acute appendicitis: a systematic review and meta-analysis. PLoS One. 2022;17(9):e0275427. doi:10.1371/journal.pone.0275427
6. Chong CF, Adi MIW, Thien A, et al. Development of the RIPASA score: a new appendicitis scoring system for the diagnosis of acute appendicitis. Singapore Med J. 2010;51(3):220–225.
7. Malik MU, Connelly TM, Awan F, et al. The RIPASA score is sensitive and specific for the diagnosis of acute appendicitis in a western population. Int J Colorectal Dis. 2017;32:491–497. doi:10.1007/s00384-016-2713-4
8. Zeb M, Khattak SK, Samad M, Shah SS, Shah SQA, Haseeb A. Comparison of Alvarado score, appendicitis inflammatory response score, and Raja Isteri Pengiran Anak Saleha appendicitis score in predicting acute appendicitis. Heliyon. 2023;9(1):e13013. doi:10.1016/j.heliyon.2023.e13013
9. Chong CF, Thien A, Mackie AJ, et al. Comparison of RIPASA and Alvarado scores for the diagnosis of acute appendicitis. Singapore Med J. 2011;52(5):340–345.
10. Sinha S, Ahmed S, Ansari M. Evaluation of RIPASA score compared to modified Alvarado score. Int J Pharm Clin Res. 2023;15(6):1470–1478.
11. Alvarez-Lozada LA, Fernandez-Reyes BA, Arrambide-Garza FJ, et al. Clinical scores for acute appendicitis in adults: a systematic review and meta-analysis of diagnostic accuracy studies. Am J Surg. 2025;240:116123. doi:10.1016/j.amjsurg.2024.116123
12. Kollias TF, Gallagher CP, Albaashiki A, Burle VS, Slouha E. Sex differences in appendicitis: a systematic review. Cureus. 2024;16(5):e60055. doi:10.7759/cureus.60055
13. Musa A, Alelyani M, Hadadi I, et al. Comparison between computed tomography and ultrasonography to diagnose acute appendicitis in a Saudi population. J Radiat Res Appl Sci. 2024;17(1):100827.
14. Afifi HS, Abdelrahman EM, Abdelfattah MF, Elhady AM, Sakr AE. RIPASA score in diagnosis of acute appendicitis: to what extent is it accurate? Egypt J Hosp Med. 2023;90(2):2195–2198. doi:10.21608/ejhm.2023.285508
15. Buderer NM. Statistical methodology: i. Incorporating the prevalence of disease into the sample size calculation for sensitivity and specificity. Acad Emerg Med. 1996;3(9):895–900. doi:10.1111/j.1553-2712.1996.tb03538.x
16. Gan DEY, Nik Mahmood NRK, Chuah JA, Hayati F. Performance and diagnostic accuracy of scoring systems in adult patients with suspected appendicitis. Langenbecks Arch Surg. 2023;408(1):267. doi:10.1007/s00423-023-02991-5
17. Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020;15(1):27. doi:10.1186/s13017-020-00306-3
18. Abourizk MI, Abdel-Hafez EM, Abdelrahman EM, El Hantery MM, Waly MA. Accuracy and sensitivity of the RIPASA score in the diagnosis of acute appendicitis versus the Alvarado score. Benha Med J. 2024;41(1):1–8.
19. Bhat R. Reviving observation-based learning for Zoomers in medical education. Adv Med Educ Pract. 2025;14:1401–1412.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Physicians’ Knowledge of the Systematic ABCDE Approach in Riyadh, Saudi Arabia
Qutob R, Almutairy LS, Altamimi AM, Almehaideb LA, Alshehri KA, Alaryni A, Alghamdi A, Alsolamy E, Al Harbi K, Alammari Y, Alanazi A, Bukhari A, Ababtain A, Alburakan A, Hakami OA
Journal of Multidisciplinary Healthcare 2024, 17:1179-1188
Published Date: 15 March 2024
When Clinical AI and Learner Reasoning Conflict: An Emerging Educational Blind Spot and a Framework for Pedagogical Response
Heslin SM
Advances in Medical Education and Practice 2026, 17:592114
Published Date: 7 May 2026