")
Back to Journals » Patient Related Outcome Measures » Volume 13
Development of the Breast Cancer Survivors Symptom Checklist for Use in Follow-Up Multidisciplinary Appointments
Authors Schou-Bredal I , Sørensen EM, Kraglund KH, Jensen VS, Drageset S
Received 9 May 2022
Accepted for publication 24 August 2022
Published 7 October 2022 Volume 2022:13 Pages 199—208
DOI https://doi.org/10.2147/PROM.S364625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Lynne Nemeth
Inger Schou-Bredal,1 Elin Myklebust Sørensen,2 Kari Heitmann Kraglund,2 Vibeke Schou Jensen,2 Sigrunn Drageset3
1Faculty of Medicine, Institute for Health and Science, University of Oslo, Oslo, Norway; 2Department of Cancer, Unit for Breast and Endocrine Surgery, Oslo University Hospital, Oslo, Norway; 3Faculty of Health Social Sciences, Institute for Health and Caring Sciences, Western Norway University of Applied Sciences, Bergen, Norway
Correspondence: Sigrunn Drageset, Faculty of Health Social Sciences, Institute for Health and Caring Sciences, Western Norway University of Applied Sciences, HVL, Postbox 7030, Bergen, 5020, Norway, Tel + 47 55 58 56 32, Email [email protected]
Background: Breast cancer survivors are primarily followed up to monitor the effectiveness of treatment and complications and to detect recurrences. Many breast cancer survivors may experience prolonged adverse physical and psychological effects, which should also be addressed at follow-ups. The objective of this study was to develop a brief symptom assessment tool for breast cancer survivors to be used as a guideline for the survivors and all health care professionals conducting the routine follow-up. The second objective was to describe the women’s individual experiences with follow-ups.
Methods: A literature review, a focus group of 6 healthcare professionals using a nominal group technique process, and the experience and feedback via qualitative interviews with 16 breast cancer survivors was used to develop the Breast Cancer Survivors Symptom Assessment Checklist (BCS-SC).
Results: The BCS-SC consists of a set of 13 symptoms/burdens and one question. On a scale from 0 (no symptom) to 10 (worst imaginable), survivors indicated the extent to which they experience each symptom. All survivors perceived the annual follow-ups as important, but none prepared for them. Eight of the 16 survivors reported that they had 2 or more of the symptoms/burdens listed in the BCS-SC. However, only one of the survivors had mentioned her symptom to the doctor at follow-up.
Conclusion: The BCS-SC is a comprehensive assessment tool for symptoms/burdens that are common among breast cancer survivors and can aid efforts to optimize their follow-up. Furthermore, the BCS-SC allows for a more patient-initiated and focused consultation, leading to more patient-centered quality care.
Keywords: breast cancer, checklist, personalized approach, survivorship, symptoms assessment tool
Introduction
Due to advances in early detection, treatment, and follow-up care, relative 5-year survival rates in Norway are currently estimated at 92%.1 Breast cancer patients are followed up annually for 10 years. The follow-ups include evaluation of any ongoing treatment, side effects, and disease status and detection of recurrence; information is also provided.2 The breast cancer patients survival rate has increased dramatically in recent decades, therefore quality of life (QoL) has become a major focus in research and clinical practice. The type of follow-up the survivors receive may affect their level of reassurance and have an impact on their QoL. It has been suggested that worsening QoL might be related to worsened prognosis and an increase in the risk of recurrence.3
Over the past decades, research has shown that breast cancer and its treatment have a significant emotional and social impact on patients,4 their QoL5,6 as well as their capacity for work.7–9 Many survivors experience prolonged adverse physical, cognitive, and psychological effects.4,10,11 Furthermore, survivors may experience multiple symptoms concurrently, which compounds the impact on functions in daily life, yet these symptoms often remain underdiagnosed and untreated because the patient’s report of symptom severity is rarely part of routine cancer care and validated symptom assessment tools are not readily available to clinicians.12 Some brief symptom inventories exists that allow for simple and rapid documentation of multiple patient-reported symptoms at the same time.13 However, not all symptoms screened by these instruments are relevant for breast cancer survivors and some symptoms that are relevant, are not covered. Therefore, based on previous symptom assessment tools, research, clinical experience, and patient involvement, we decided to develop an assessment tool for breast cancer survivors to be used at routine follow-ups. Effective care for breast cancer patients after treatment depends on recognition of the patients’ psychosocial as well as physical needs.14,15 Better assessment is a prelude to successful treatment of symptoms.
The aim of the present study was (1) to develop a brief symptom assessment tool that provides an adequate summation of symptoms/burdens described by breast cancer survivors, (2) to describe women’s individual experiences with follow-ups consultations without the aid of an assessment tool.
Materials and Methods
A focus group of 6 healthcare professionals (oncology nurses, clinical nurse specialist) with expertise in breast cancer symptom management was convened. First, the group conducted a search of the literature to identify existing symptom assessment scales for cancer symptoms using PubMed, CINAHL, and Cochrane Library databases. MeSH terms (eg, “checklist”, “assessment tool”, “breast cancer”) were combined with keywords (eg, “follow-up”, “ treatment”, “late effects”, “symptoms”, “survivorship”). All search results were scanned for possible relevant content based on titles and abstracts. Next, the optimal properties of a symptom screening tool for breast cancer survivors and symptom assessment scales were identified and evaluated. A nominal group technique (NGT) was used to identify the most important symptoms for inclusion. NGT is a process that is designed to promote group participation in identifying problems, generating solutions, and decision-making. The structure of NGT has 5 stages: introduction, idea generation, sharing ideas, group discussion, voting. It helps groups to make fast and informed decisions, taking everyone’s opinion into account.16 The NGT resulted in a final ranking of items according to the sum of votes from all participants. A consensus approach in face-to-face discussion was then implemented to produce an initial draft of the checklist we named the Breast Cancer Survivors Symptom Checklist (BCS-SC).
The next step was to involve the breast cancer consumers to assess the checklist. Before their follow-up appointment, patients were asked if they were willing to be interviewed immediately after the follow-up at the hospital. The follow-ups were conducted without the use of the BCS-SC. One-to-one semi-structured interviews were conducted with 16 patients to explore their experiences and perceptions of follow-up. The interviews lasted from 30 to 45 minutes. A semi-structure interview guide was developed. The following questions were included:
- How have you been since treatment was completed?
- Did you receive information regarding the possibility of experiencing late side effects?
- At the last consultation, after treatment was complete, did the doctor talk about getting back to work?
- Did the doctor talk about the importance of adherence with regard to endocrine therapy?
- Do you prepare for your annual follow-up (eg, write down questions, you want to ask the doctor)?
- How important are these annual follow-ups for you?
After the interview, the patient was asked to fill out and assess the BCS-SC, with the interviewer present. The following topics were covered: views and feasibility of using the BCS-SC during routine follow-up, were any symptoms or ailments missing, presentation of the data on a one-page sheet, usefulness, length of time to fill out the BCS-SC. If the patient scored 4 or more on an item(s), they were asked if they had mentioned that particular symptom(s) to the doctor. Finally, patients were asked if they thought that the BCS-SC would be a helpful tool for the annual follow-ups.
Data Analysis
Descriptive statistics are presented as means, standard deviations (SD), and frequencies where appropriate. The interviews were conducted, audio-taped, and transcribed verbatim by the first author. The interviews were analyzed using thematic analysis in 6 steps: familiarization, coding, generating themes, reviewing themes, defining and naming themes. The transcripts were carefully reviewed independently by 2 researchers to identify categories, which were then compared and a set of core themes was derived.17
Results
The focus group and the interviews both contributed to the development of the BCS-SC.
Results from the Focus Group
The focus group found that the optimal properties for a breast cancer survivor symptoms screening tool were: (1) capture of both physical and psychosocial symptoms; 2) minimal burden for the respondent, (3) focus on subjective types of symptoms rather than objective symptoms, and (4) focus on the severity of symptoms.
The 2 most suitable screening tools found were the M.D. Anderson Symptom Inventory (MDASI), which includes 13 cancer-related symptoms that are common for most cancers,18 and the Edmonton Symptom Assessment System (ESAS), which was developed to assist in the assessment of 9 symptoms that are common in palliative care.19 However, the group concluded that not all symptoms screened by the ESAS or MDASI are relevant for breast cancer survivors and many symptoms are not covered.
The NGT process resulted in identification of 13 symptoms/burdens. The symptoms were fatigue, pain, problems sleeping, body image, menopausal burdens/symptoms, sexuality, weight gain, lymphedema, cognitive functioning, and emotional distress. The burdens were social network, work situation, financial. In addition, one question was added and possibility to add symptoms/burdens that were not on the checklist was included (Table 1).
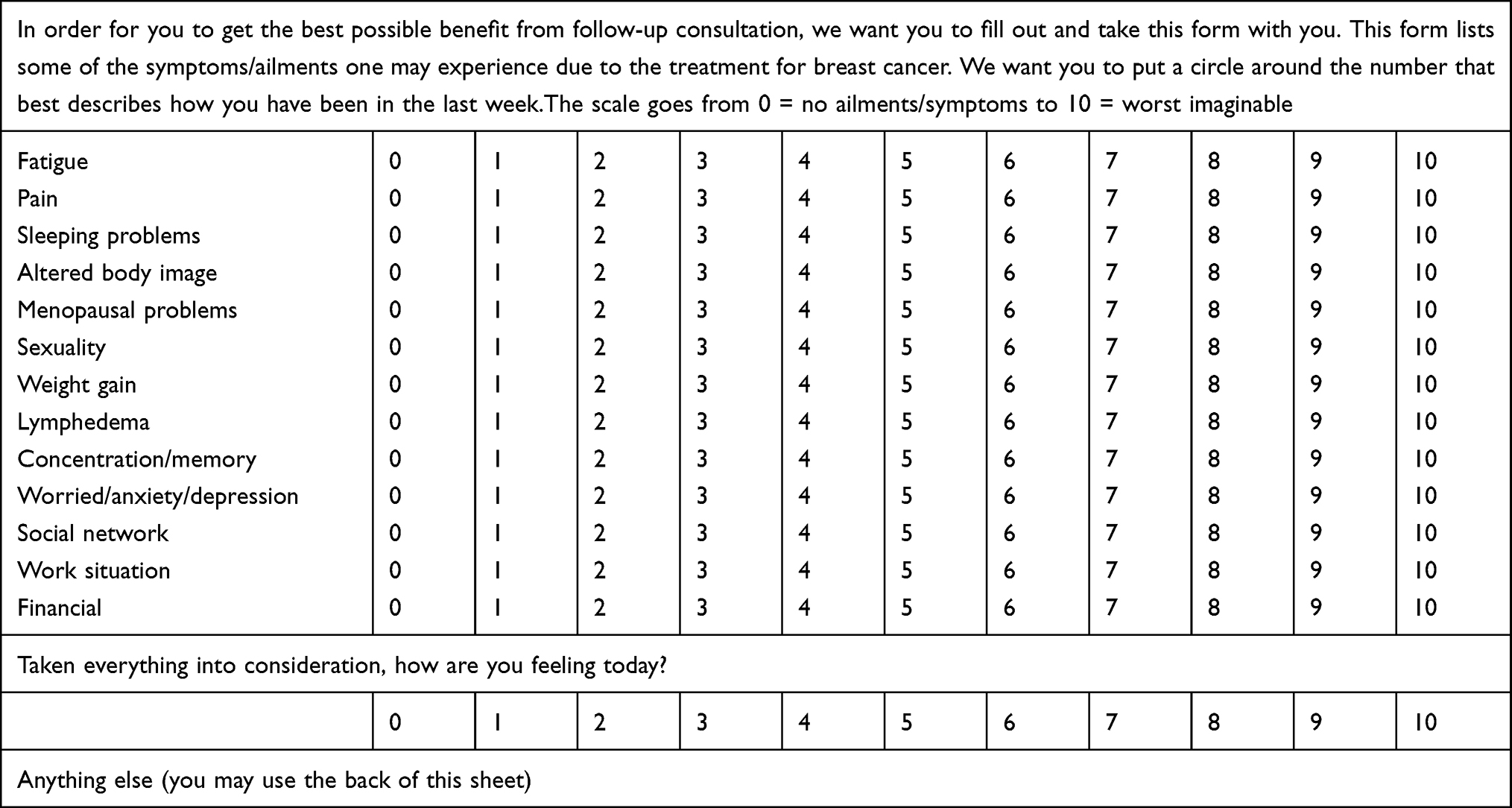 |
Table 1 The Breast Cancer Survivors Symptom Checklist |
The group had a significant dialogue on social network, work situation, and finances. The health professionals cannot provide assistance with these items, but can make suggestions or refer to other professionals that may be of help. Because these items were viewed as important for the individual’s QoL, and this view is supported by research,20–22 the consensus of the group was to retain them.
The group decided to adapt the layout of the ESAS, using a visual analog scale from 0 (no burden/symptom) to 10 (worst imaginable). A score of 4 or more for pain was considered to have an impact on daily life;23 for all other items, a score of 5 or more was considered to have an impact on daily life and as a threshold level for medical intervention.24
A short introduction was formulated as a heading for the BCS-SC. The respondents were asked to indicate the extent to which they experienced each symptom/burden listed on the BCS-SC, The time frame used was “now”.
Results from Patient Interviews
Demographic and medical data of the patients are shown in Table 2. Three patients had their first-annual follow-up, 2 their second, 3 their fourth, 4 their fifth, 1 her eighth, and 3 their tenth.
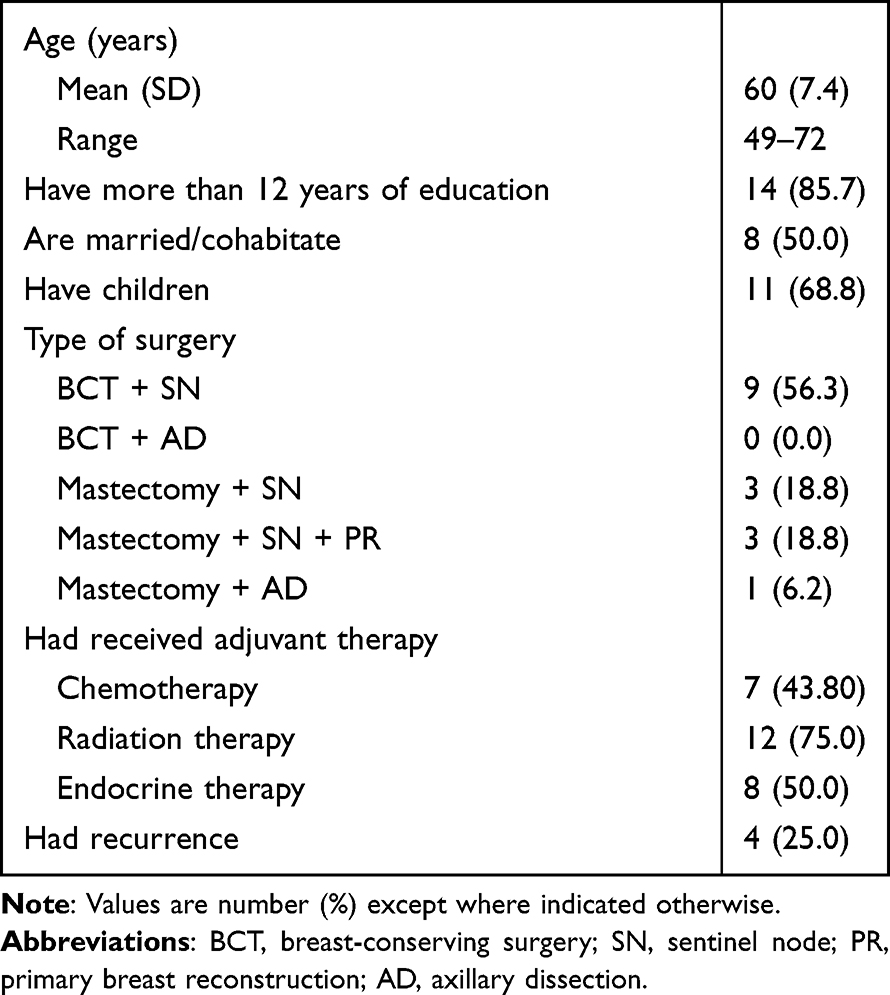 |
Table 2 Demographic and Medical Data (N = 16) |
How Have You Been Since Your Treatment Was Completed?
The women’s illness experiences varied, but most reported that they felt fine when interviewed. However, several of the participants had experienced physical and psychological symptoms, burdens, or worries.
“My pain due to arthritis worsened after treatment”. [Participant 1]
“I have had my ups and downs. I have some control, but then everything gets black…ups and downs.” [Participant 7]
“In the beginning I had lots of pain due to the expanding prosthesis, but then it was changed to a permanent prosthesis. I have less pain now”. [Participant 16]
I had both breasts removed, one due to cancer and the other prophylactically and both were reconstructed. I am pleased that the doctor listened to my worries. I have no genetic defect, but breast cancer is hereditary in my family. [Participant 2]
“The first year was very bad, I was sick, not good at all, but since then I have been fine.” [Participant 13]
“It has gone smoothly, no traumatic treatment…but I always feel some tension at follow-ups.” [Participant 12]
Did You Receive Information Regarding the Possibility of Experiencing Late Side Effects?
In general, most believed that they had received good information. The information regarding side effects was mostly related to the possibility of experiencing pain due to endocrine treatment. Only a few patients had been informed about side effects or late effects due to the treatment. A couple expressed that they had the opportunities to get the information they needed.
“Most of the information was regarding side effects of the tablets I have to use.” [Participant 5]
“I was informed that some have more pain than others…” [Participant 7]
There were so many doctors…I encountered many doctors when receiving chemotherapy… they seemed more occupied with blood results and they like…so no…not much information [Participant 8]
We got some explanations, but I think in some cases they can be afraid to say too much.so it is up to each person to read. find out for themselves…but I did receive some information. [Participant 9]
At the Last Consultation After the Treatment Was Complete Did the Doctor Talk to You About Getting Back to Work?
Some women were working during treatment, and others started working when they finished the treatment. Some could not remember if the doctors had talked about getting back to work; 2 confirmed that was talked about.
“Yes. we talked about how I felt and how to proceed” [Participant 10]
“Yes we had a dialogue all the time. I went back to work, but am retired now.” [Participant 14]
“Yes we probably did…I cannot remember…but I did get the information I wanted.” [Participant 12]
Did the Doctor Talk About the Importance of Adherence with Regard to Endocrine Therapy?
Six participant had received anti-hormone treatment. Some said that the doctor emphasized the importance of adherence, and others could not remember if the doctor had mentioned it.
Yes, but it did not go well. I contacted the doctor and was encouraged to try 3 months more, but in the end it was horrible. I got depressed, developed anxiety, and had trouble sleeping.had pain in my joints. I contacted my doctor …I told her I had to stop taking them and she understood, but said I could start with them again at any time. [Participant 7]
I am finished taking the tablets, but I took them all the years I should because I knew how important they were, but there were many side effects….yes especially mood swings and I was in such a bad mood. [Participant 13]
Do You Prepare for Your Annual Follow-Up? (Eg, Write Down Questions You Wanted to Ask the Doctor)
Most women did not prepare for the follow-up checks, but said that they had discussed what they wanted. Topics that were raised by the participants included concerns about feeling pain in the operated area, the risk of experiencing relapse, why they experienced pain all over their body, and the results from the mammography.
“Yes I think about what I want to ask. I experience pain at times, and I asked about the pain.” [Participant 10]
“Yes I do, I ask about why I experience pain in the operating area…what the risks for relapse are….why I ache all over my body.” [Participant 14]
“She (the doctor) was very informative, she took her time, yes it is often the case that when they (doctors) start talking about things, questions may arise.” [Participant 5]
How Important are These Annual Follow-Up for You?
All women perceived the follow-ups as important and reassuring. Most preferred follow-ups at the hospital instead with their general practitioner (GP), because they experienced that the hospital took the follow-ups more seriously.
The first 5 years I went to follow-ups at the hospital, but later follow-ups were with the GP. I received appointments for mammography every year, but neither the GP nor I knew who requisitioned it or who received the results. The GP finally found out that it was the hospital that had requisitioned the mammography and received the results. I would have preferred to have all my follow-ups at the hospital. Now I had my last follow-up at the hospital. [Participant 11]
“I think the follow-ups are very good, but I prefer having them at the hospital. I do not think the GP takes them seriously.” [Participant 6]
“I feel secure that any relapse will be detected early and it is good to have regular communication with the hospital.” [Participant 5]
I am happy I can continue to have my follow-ups at the hospital. After 5 years one is supposed to go to the GP, but my GP does not even know that I have had the operation. [Participant 13]
Results from the Patients’ Assessment of the BCS-SC
The patients questioned what was meant by the time frame “now”. The time frame was therefore changed to “during the last week”. One woman thought there should be one item for “fear of recurrence”. However, the others thought that the item “feeling blue/worried/anxiety” covered fear of recurrence. The patients were asked which term should be used: “fatigue or tired/exhausted”. They all agreed that the term fatigue should be used. All of the patients considered the BCS-SC easy to understand and use. The final version of the BCS-SC is presented in Table 1.
Table 3 presents the BCS-SC scores for the individual women and the most persisting symptoms/burdens were fatigue and sleeping problems, followed by sexuality, concentration/memory. Four of the 16 women answered “all things considered, they did not feel good today”.
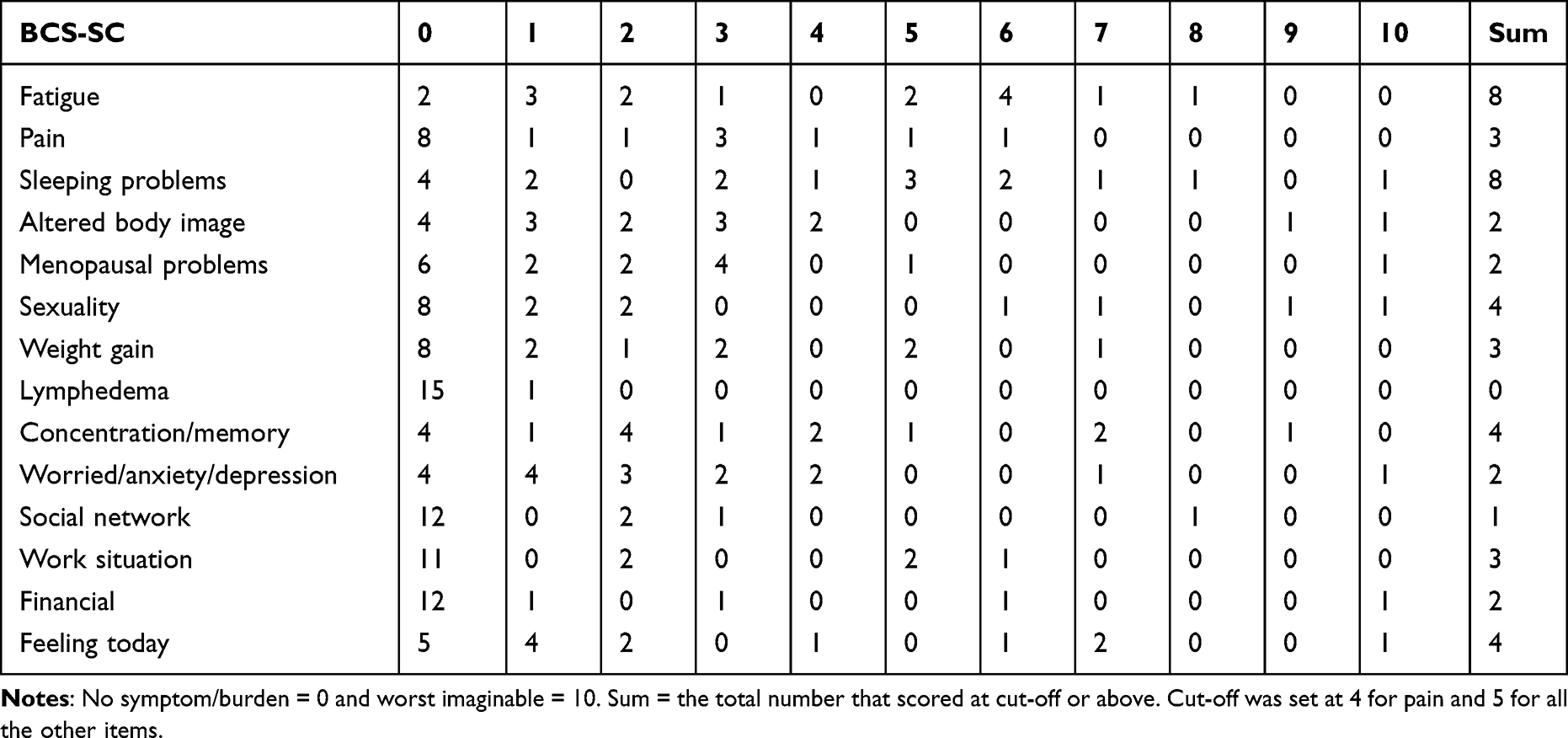 |
Table 3 The Breast Cancer Survivors Symptom Checklist Scores for the 16 Women |
Women who had scored 4 or more on any of the BCS-SC items were asked if they had discussed this topic with the doctor during the follow-up consultation. Participant 5 scored had scored more than 5 on several symptoms/problems (fatigue, sleeping problems, and concentration/memory). When asked if she had mentioned these to the doctor at follow-up she answered:
No maybe my sleeping problems are due to my age. I don’t know if my poor memory is due to my age or treatment…no I did not mention it…Yes I mentioned that I was tired…fatigue…because that has to do with the tablets…they take your energy away…. [Participant 5]
The patients were asked if they thought that the BCS-SC would be a helpful tool for the annuals follow-ups. All patients thought the BCS-SC was helpful and that it was wise to use it. Filling out the BCS-SC made them think and prepare for the follow-up. Some mentioned that the BCS-SC probably also was a good working tool for the doctor and made it easier for them as well.
“Yes.I definitely think it can be helpful before follow-ups….I because…yes …the point about sexuality….I had not thought about it…but I could have asked …” [Participant 7]
Absolutely wise – it’s much easier…yes…such a form makes it easier…it’s not easy to remember everything on a busy day…it’s probably easier for the doctor also as a work tool… [Participant 13]
The final version of the BCS-SC after the patients had given their feedback was presented to 2 breast cancer surgeons for their feedback. Based on both patients’ and surgeons’ feedback, the BCS-SC was finalized.
Discussion
The Breast Cancer Survivors Symptom Checklist
We develop the BCS-SC assessment tool for breast cancer survivors for use as a guideline for survivors and all health care professionals conducting routine follow-ups. The final version of the checklist consists of a set of 13 symptoms/burdens, and one question. The patients are asked to indicate the extent to which they experience each symptom/burden on a scale from 0 (no symptom/burden) to 10 (worst imaginable). The time frame used was in the last week. The content of this checklist is based on a review of the literature, clinical experiences, an NGT process, feedback from breast cancer surgeons and patients regarding the usability and validity. In view of the rigorous development process, we believe that the checklist is a comprehensive assessment tool for symptoms/burdens that are common among breast cancer survivors and can aid efforts to optimize their follow-up.
Patients’ Experience of Follow-Ups
Most of the patients believed that they had received good information, but not all were informed regarding possible side effects or late effects. This finding is similar to previous findings that breast cancer survivors often express unmet needs for information on the effects of cancer treatment, emotional distress, and lifestyle changes.12
When one considers the increase in the incidence of breast cancer, the age at time of diagnosis, and the decrease in mortality, the return to work issue is important. Thus, this should be a topic that is routinely addressed at follow-ups, and factors that could get in the way of return to work or ease it should be discussed. A systematic research and meta-analysis including studies from Europa and Asia found that the overall rate of return to work was 57%.25 In the present study, some of the patients worked during their treatment, whereas others started to work after treatment was completed. However, few could remember if the doctor had talked about getting back to work at follow-ups.
The experience of the illness varied among the breast cancer survivors. Most said that they did not experience any problems. Thus, it was interesting to note that half of the survivors reported that they had 2 or more of the symptoms/burdens listed in the BCS-SC. This is consistent with previous research that shows cancer survivors may experience symptoms/burdens related to cancer and its treatments years after the treatment has been completed.6,26,27 There is evidence that indicates that the psychological needs of cancer survivors often go underdiagnosed during routine medical follow-up.28
The most persisting symptoms/burdens found in the present study were fatigue and insomnia, followed by sexuality, concentration/memory. These are the same as found previously to be the most persisting symptoms/burdens experienced by survivors.8,26,29 However, although many of the survivors in the present study experienced symptoms/burdens, they did not discuss these with the doctors at follow-up.
The primary goal of follow-up after breast cancer treatment is to detect recurrences or second primary breast cancer and to monitor side effects related to treatment.2 Concern for long-term QoL and psychological adjustment of cancer survivors has increased because improved treatments have resulted in a growing population of cancer survivors in Norway.1 However, it appears that both the women and the doctors are mostly concerned regarding the results of mammography or other tests. Monitoring side effects is an important issue of the follow-up, but our experience is that when doctors ask patients if they want to discuss anything or how they are feeling, most patients say that they feel fine and have nothing to discuss. A reason for not addressing other issues could be that the participants were unaware that breast cancer follow-up care extends beyond surveillance for recurrence.
Adjuvant hormonal therapy is important in the treatment of receptor-positive breast cancer. However, non-adherence rate to hormonal treatment is estimated to be between 30% and 60%.30–32 In the present study, only 1 in 6 women said that the doctor had emphasized the importance of adherence. The BCS-SC lists the most prominent side effects of adjuvant hormonal treatment. Thus, we propose that the BCS-SC could contribute to remind the doctors to inquire about the adherence to endocrine therapy.
All the survivors in the present study perceived the annual follow-ups as important and reassuring. They preferred follow-ups at the hospital instead of with the GP because they experienced that the hospital took the follow-ups more seriously. This is similar to previous findings regarding patients’ follow-up preference with cancer-related specialists.33 In addition, it has been found that patients are more positive about nurse practitioner-led follow-up than GP-led-follow-up.34 It appears that patients valued the expertise of specialists in hospital settings more than GPs.
Breast Cancer Survivors’ Assessment of the BCS-SC
None of the survivors had prepared for their follow-up consultation, even though they all perceived them as important. However, when asked if the BCS-SC could be a helpful tool for the annual follow-ups, all answered yes. They argued that if they had received and filled in the checklist before their follow-up, they would be better prepared. Furthermore, the BCS-SC would insure that the symptoms/burdens they experienced would be discussed. They reported that the BCS-SC was brief and easy to fill out. Furthermore, some also commented that the BCS-SC would be a helpful tool for the doctors at follow-up.
Clinical Implications
There has been a paradigm change from reactive to predictive, preventive, and personalized medicine, which has been declared as an essential transformation of the overall health care approach to benefit the patient and society at large.35 This implies that follow-ups should also be personalized. Thus, the BCS-SC may be considered a cost-effective tool to individualize follow-ups and provide tailored care to improve the patient’s health outcome and QoL. The BCS-SC is simple and quick to administer. It supports subjective decision-making in resource-limited settings or primary care, and may improve outcomes. We propose that all breast cancer survivors should fill out the BCS-SC routinely before their follow-up at the hospital or with the GP. Including the patient’s BCS-SC score in the follow-up routinely would help to elicit patient concerns and allow discussion of issues that could otherwise be missed.
Strengths and Limitations
The development of the BCS-SC was based on a literature review, clinical experience and patient input. Limitations of the literature review include the possibility of missing articles and errant evidence interpretation. The use of the qualitative analysis technique utilized may be prone to biases of subjective interpretation. In addition, there may have been a bias in the types of patients who agreed to participate, and the sample size for the study was small. Thus, this study should be viewed as a small-scale preliminary study. Future research with a larger sample is needed to better evaluate the feasibility and validity of the BCS-SC. In addition, it remains uncertain as to which scores on the BCS-SC (except pain) comprise the optimal cut-off to determine symptom severity for breast cancer survivors. Further research should explore the optimal cut-off for each BCS-SC item to determine symptom/burden severity. Future research could also investigate the doctors’ evaluation of the utility of the BCS-SC.
Conclusion
The BCS-SC appears to be a promising brief screening tool for symptoms/burdens and could be incorporated into routine follow-ups for breast cancer survivors. This would help to elicit patient concerns and allow discussion of issues that could otherwise be missed. This can improve clinician–patient communication and symptom management, as well as provide the opportunity for multi-professional support and more personalized follow-up. This is supportive of the paradigm change from reactive medicine to predictive, preventive, and personalized medicine.
Abbreviations
BCS-SC, the Breast Cancer Survivors Symptom Assessment Checklist; ESAS, the Edmonton Symptom Assessment System; GP, general practitioner; NGT, nominal group technique; MDASI, the M.D. Anderson Symptom Inventory; SD, standard deviation.
Data Sharing Statement
The data (interview transcripts) reported in this paper are not publicly available, because the participants did not consent to public data sharing. The quantitative data are available upon reasonable request from the corresponding author after permission from the Hospital’s Privacy Officer has been obtained.
Ethical Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki and approved by The Regional Committee for Medical and Health Research Ethics South East Norway (REC 2014/730) and the Data Inspectorate, Oslo University Hospital. All participants received oral information on the purpose of the study. They were informed that the interview would be taped and that all data would be de-identified. All participants were required to review the consent form before signing. All participants gave their written informed consent.
Acknowledgments
The authors thank the patients for their contribution to the evaluation and testing of the BCS-SC.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of the data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Cancer Registry of Norway. Cancer in Norway 2019 - Cancer Incidence, Mortality, Survival and Prevalence. Oslo: Cancer Registry of Norway; 2020.
2. Norwegian Directorate for Health Services. National Guidelines for a National Action Program with Guidelines for Diagnosis, Treatment and Follow-Up of Patients with Breast Cancer. Norwegian Directorate for Health Services; 2020.
3. Souza APS, Silva LCD, Fayh APT. Nutritional intervention contributes to the improvement of symptoms related to quality of life in breast cancer patients undergoing neoadjuvant chemotherapy: a randomized clinical trial. Nutrients. 2021;13(2):589. doi:10.3390/nu13020589
4. Knobf MT. Clinical update: psychosocial responses in breast cancer survivors. Semin Oncol Nurs. 2011;27(3):e1–e14. doi:10.1016/j.soncn.2011.05.001
5. Iioka Y, Iwata T, Yamauchi H. Symptoms and QOL in breast cancer patients receiving hormone therapy in Japan. Breast Cancer. 2020;27:62–69. doi:10.1007/s12282-019-00993-0
6. Wu HS, Harden JK. Symptom burden and quality of life in survivorship: a review of the literature. Cancer Nurs. 2015;38(1):E29–E54. doi:10.1097/NCC.0000000000000135
7. Drageset S, Lindstrom TC, Ellingsen S. ”I have both lost and gained”. Norwegian survivors’ experiences of coping 9 years after primary breast cancer surgery. Cancer Nurs. 2020;43(1):E30–E37. doi:10.1097/NCC.0000000000000656
8. Drageset S, Lindstrom TC, Ellingsen S. ”Cancer changed my life.” Women’s experiences 1 and 9 years after primary breast cancer surgery. Nordisk Sygeplejeforskning. 2020;10(2):20–33. doi:10.18261/issn.1892-2686-2020-01-03
9. Sun Y, Shigaki CL, Armer JM. Return to work among breast cancer survivors: a literature review. Support Care Cancer. 2017;25(3):709–718. doi:10.1007/s00520-016-3446-1
10. Binkley JM, Harris SR, Levangie PK, et al. Patient perspectives on breast cancer treatment side effects and the prospective surveillance model for physical rehabilitation for women with breast cancer. Cancer. 2012;118(8 Suppl):2207–2216. doi:10.1002/cncr.27469
11. Pillai US, Kayal S, Cyriac S, et al. Late effects of breast cancer treatment and outcome after corrective interventions. Asian Pac J Cancer Prev. 2019;20(9):2673–2679. doi:10.31557/APJCP.2019.20.9.2673
12. Vuksanovic D, Sanmugarajah J, Lunn D, Sawhney R, Eu K, Liang R. Unmet needs in breast cancer survivors are common, and multidisciplinary care is underutilised: the Survivorship Needs Assessment Project. Breast Cancer. 2021;28(2):289–297. doi:10.1007/s12282-020-01156-2
13. Recklitis CJ, Rodriguez P. Screening childhood cancer survivors with the brief symptom inventory-18: classification agreement with the symptom checklist-90-revised. Psychooncology. 2007;16(5):429–436. doi:10.1002/pon.1069
14. Brandao T, Schulz MS, Matos PM. Psychological adjustment after breast cancer: a systematic review of longitudinal studies. Psychooncology. 2017;26(7):917–926. doi:10.1002/pon.4230
15. Antoni MH, Jacobs JM, Bouchard LC, et al. Post-surgical depressive symptoms and long-term survival in non-metastatic breast cancer patients at 11-year follow-up. G–n Hosp Psychiatry. 2017;44:16–21. doi:10.1016/j.genhosppsych.2016.10.002
16. Van de Ven AH, Delbecq AL. The nominal group as a research instrument for exploratory health studies. Am J Public Health. 1972;62(3):337–342. doi:10.2105/AJPH.62.3.337
17. Kvale S, Brinkman S. InterViews: Learning the Craft of Qualitative Research Interviewing. Los Angeles, CA: SAGE; 2015.
18. Cleeland CS, Mendoza TR, Wang XS, et al. Assessing symptom distress in cancer patients: the M.D. Anderson Symptom Inventory. Cancer. 2000;89(7):1634–1646. doi:10.1002/1097-0142(20001001)89:7<1634::AID-CNCR29>3.0.CO;2-V
19. Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K. The Edmonton Symptom Assessment System (ESAS): a simple method for the assessment of palliative care patients. J Palliat Care. 1991;7(2):6–9. doi:10.1177/082585979100700202
20. Michael YL, Berkman LF, Colditz GA, Holmes MD, Kawachi I. Social networks and health-related quality of life in breast cancer survivors: a prospective study. J Psychosom Res. 2002;52(5):285–293. doi:10.1016/S0022-3999(01)
21. Schmidt ME, Scherer S, Wiskemann J, Steindorf K. Return to work after breast cancer: the role of treatment-related side effects and potential impact on quality of life. Eur J Cancer Care. 2019;28(4):e13051. doi:10.1111/ecc.13051
22. Toledo G, Ochoa CY, Farias AJ. Exploring the role of social support and adjuvant endocrine therapy use among breast cancer survivors. Support Care Cancer. 2020;28(1):271–278. doi:10.1007/s00520-019-04814-0
23. Schou Bredal I, Smeby NA, Ottesen S, Warncke T, Schlichting E. Chronic pain in breast cancer survivors: comparison of psychosocial, surgical, and medical characteristics between survivors with and without pain. J Pain Symptom Manage. 2014;48(5):852–862. doi:10.1016/j.jpainsymman.2013.12.239
24. Klinkhammer-Schalke M, Koller M, Ehret C, et al. Implementing a system of quality-of-life diagnosis and therapy for breast cancer patients: results of an exploratory trial as a prerequisite for a subsequent RCT. Br J Cancer. 2008;99(3):415–422. doi:10.1038/sj.bjc.6604505
25. Tavan H, Azadi A, Veisani Y. Return to work in cancer patients: a systematic review and meta-analysis. Indian J Palliat Care. 2019;25(1):147–152. doi:10.4103/IJPC.IJPC_114_18
26. Liou KT, Ahles TA, Garland SN, et al. The relationship between insomnia and cognitive impairment in breast cancer survivors. JNCI Cancer Spectr. 2019;3(3):pkz041. doi:10.1093/jncics/pkz041
27. Mandelblatt JS, Zhai W, Ahn J, et al. Symptom burden among older breast cancer survivors: the Thinking and Living With Cancer (TLC) study. Cancer. 2020;126(6):1183–1192. doi:10.1002/cncr.32663
28. Absolom K, Holch P, Pini S, et al. The detection and management of emotional distress in cancer patients: the views of health-care professionals. Psychooncology. 2011;20(6):601–608. doi:10.1002/pon.1916
29. Bjerkeset E, Röhrl K, Schou-Bredal I. Symptom cluster of pain, fatigue, and psychological distress in breast cancer survivors: prevalence and characteristics. Breast Cancer Res Treat. 2020;180(1):63–71. doi:10.1007/s10549-020-05522-8
30. Hershman DL, Kushi LH, Shao T, et al. Early discontinuation and nonadherence to adjuvant hormonal therapy in a cohort of 8769 early-stage breast cancer patients. J Clin Oncol. 2010;28(27):4120–4128. doi:10.1200/JCO.2009.25.9655
31. Gotay C, Dunn J. Adherence to long-term adjuvant hormonal therapy for breast cancer. Expert Rev Pharmacoecon Outcomes Res. 2011;11(6):709–715. doi:10.1586/erp.11.80
32. Dunn J, Gotay C. Adherence rates and correlates in long-term hormonal therapy. Vitam Horm. 2013;93:353–375. doi:10.1016/B978-0-12-416673-8.00003-4
33. Kwast AB, Drossaert CH, Siesling S. Breast cancer follow-up: from the perspective of health professionals and patients. Eur J Cancer Care. 2013;22(6):754–764. doi:10.1111/ecc.12094
34. Lewis R, Neal RD, Williams NH, et al. Nurse-led vs. conventional physician-led follow-up for patients with cancer: systematic review. J Adv Nurs. 2009;65(4):706–723. doi:10.1111/j.1365-2648.2008.04927.x
35. Zhan X, Li J, Guo Y, Golubnitschaja O. Mass spectrometry analysis of human tear fluid biomarkers specific for ocular and systemic diseases in the context of 3P medicine. EPMA J. 2021;12(4):449–475. doi:10.1007/s13167-021-00265-y
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.