Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Development of Emerging Infectious Diseases Preventive Health Behavior (EID-PHB) Scale and Validation of the Complex Models
Received 23 October 2023
Accepted for publication 24 January 2024
Published 1 February 2024 Volume 2024:17 Pages 445—460
DOI https://doi.org/10.2147/JMDH.S446006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Wee Kyung Lee, Sung Rae Shin
Department of Nursing, Sahmyook University, Seoul, South Korea
Correspondence: Sung Rae Shin, Department of Nursing, Sahmyook University, 815 Hwarang-ro, Nowon-gu, Seoul, 01795, South Korea, Tel +82-2-3399-1588, Fax +82-2-3399-1594, Email [email protected]
Introduction: Emerging Infectious Diseases are one of the world’s leading causes of death, and preventive measures must be implemented to minimize human casualties. Research on preventive behavior relies on the preventive behavior scale and it has an impact on the findings.
Purpose: This study aimed to develop an Emerging Infectious Diseases Preventive Health Behavior (EID-PHB) Scale and verify the validity and reliability of the complex models.
Methods: Initial items were generated through a literature review and interviews, based on the proposed conceptual framework of transmission-based precautions. 14 experts reviewed the preliminary items for content validity and 20 adults for face validity. Data were collected online by a research company from April 28 to May 3, 2023. A total of 533 participants completed the survey, and subjects were assigned through simple random sampling. The first sample (n = 330) was used for item analysis and Exploratory Factor Analysis (EFA), and the second sample (n = 203) was used for Confirmatory Factor Analysis (CFA), convergent validity, discriminant validity, criterion validity, and reliability. The test-retest reliability was assessed in 34 adults.
Results: The final instrument derived six components (droplet, contact, airborne, bloodborne, environmental prevention, and psychological coping), nine indicators, and 34 items. The CFA indicated that all the complex models had a good fit and the integrated factors were confirmed through validity tests. The Cronbach’s alpha for the 34 items was 0.92, and the criterion validity was verified (r = 0.85, p < 0.001).
Conclusion: The EID-PHB is a valid and reliable tool that can be used to determine preventive behaviors against emerging infectious diseases. This tool is expected to provide a conceptual framework for future research, contribute to the clinical practice and education, and establish strategies and policies for improving individual and public health.
Keywords: emerging infectious disease, health behavior, primary prevention, validation studies as topic
Introduction
Since the turn of the 21st century, the world has been exposed to a wide range of emerging infectious diseases. An emerging infectious disease poses the threat of increased human incidence in the near future as a new, previously unknown pathogen spreading geographically or expanding its influence.1 Such infections caused by biofilm-forming pathogens affect both human and animals but the host immune system finds it difficult to eradicate these infections, and the prevalence of antimicrobial resistance is rising globally. These challenges pose a serious public health threat.2 Despite ongoing attempts to develop adequate preventive and quarantine measures, infectious diseases continue to be one of the world’s major leading causes of death, accounting for millions of casualties annually.3 The mortality rates of recently emerging infectious diseases were SARS 9.5%, MERS 34.4%, and Ebola VIrus 63.0%.4 Therefore, non-pharmacological preventive efforts to avoid human deaths have become crucial quarantine measures from a public health perspective before identifying a novel infectious disease and developing a remedy.
Preventive health behaviors are a series of actions performed by asymptomatic individuals who perceive themselves as healthy to prevent or identify disease in an asymptomatic state.5 In order to successfully carry out preventive health behaviors, understanding the factors that affect preventive health behaviors in a pandemic crisis as well as tracking compliance with preventive practice guidelines have been key aims in the field of social science research.6,7 Such studies rely on instruments that ensure validity and reliability,7 and these tools significantly impact the research findings. Due to the lack of standardized scales, different approaches exist to quantify preventive behaviors against emerging infectious diseases. Some survey questions directly reflect government regulations,6,8 apply tools used in previous studies,9,10 or exclusively assess particular behaviors, such as wearing masks, washing hands, and coughing etiquette.11 However, standardized measurement tools that enable accurate communication via theory verification studies, repeated research, and cross-study comparisons are needed, rather than using non-standardized measuring tools that rely on subjective assessment.12
Assessing preventive behavior is challenging until a novel infectious disease’s lesions, symptoms, and infection routes are identified. Research on preventive behavior against novel infectious diseases is insufficient until the government announces specific guidelines for preventive behaviors. Consequently, very little research focuses on establishing a standardized novel infectious disease preventive behavior scale for the general public. Previous research on emerging infectious disease prevention practices has generally focused on medical professionals13 and nursing students,14 applying isolation and standard precautions15,16 to prevent infection. As public awareness has grown through the recent widespread promotion of quarantine guidelines, research on COVID-19 among the general public is progressing.6–10 Hence, this study aimed to develop a standardized prevention behavior scale for emerging infectious diseases for the general public in preparation for future outbreaks of novel infectious diseases. Its scope is to minimize the future damage caused by emerging infectious diseases and aid local governments in developing policies and regulations by strengthening research on preventive behavior compliance or identifying factors affecting preventive behaviors.
Materials and Methods
Research Design
This methodological study aimed to develop a preventive behavior scale for emerging infectious diseases and evaluate its validity and reliability following the eight-step tool development guidelines presented by Devellis (Figure 1).17
 |
Figure 1 Phase of development and validation of the scale. |
Development of the Scale
Conceptual Framework
The proposed conceptual framework was built by extracting concepts related to preventive behaviors and infection transmission through a literature review, and then constructing specific factors based on the infection transmission route through a mixed process of deductive and inductive methods. An infection spreads through the sources of infectious agents, susceptible hosts, and modes of transmission. However, since controlling the source of infectious agents that harbor microorganisms infiltrating the human body, objects, and surrounding environment, as well as susceptible hosts infected by these infectious agents, may be challenging, infection prevention is crucial for blocking the spread of infection. Infection transmission routes include droplets, contact, air, biology, and common vectors.18,19 Hence this study devised a conceptual framework for blocking community infection transmission routes based on transmission precautions and isolation guidelines. The components of the conceptual framework are referred to as droplet prevention, contact prevention, airborne prevention, bloodborne prevention, and environmental prevention.
Composition of Preliminary Items
We searched the DBpia (https://www.dbpia.co.kr/), Google Scholar, KISS (https://kiss.kstudy.com/), Kmbase (https://kmbase.medric.or.kr/), NDSL (http://www.ndsl.kr/), and RISS (http://www.riss.or.kr/) databases for literature to review existing preventive behavior scales against emerging infectious diseases in Korea over the last ten years. In addition, we searched the CINAHL, MEDLINE, and Google Scholar databases for worldwide literature by entering keywords using a combination of “and/or” in “emerging infectious diseases”, “preventive behaviors”, “infectious diseases”, “scale”, and “tool”. Exclusion criteria for the literature included: 1) infectious diseases that were not classified as emerging infectious diseases; 2) studies that did not target adults; 3) studies that targeted specific genders, age groups, and occupational groups; 4) studies in which the instrument question content was not clearly described; and 5) studies that were not in Korean or English. The final analysis included 16 domestic and 21 international studies that addressed the definitions and attributes of these concepts. We conducted qualitative content analysis through two focus group interviews with 15 adults aged 19~69 to discuss their experiences in preventing of emerging infectious diseases. Then, we confirmed the conceptual underpinning of the notion through a literature review. Consequently, new variables such as health care and emotional support that were not included in the components were discovered. These components are referred to as daily life prevention and psychological coping.
Reduction of the Scale
Content Validity
Based on Lynn’s (1986) opinion that verifying the content validity of preliminary items with at least three to ten experts is desirable, the researcher sent emails or letters to nine experts with backgrounds in medicine and nursing on infection control. The Content Validity Index (CVI) was used to determine validity. Previous evidence suggests that the Item-level Content Validity Index (I-CVI) should be 0.78 or higher when there are six to ten evaluators.20,21 Items with an I-CVI of less than 0.78 were therefore excluded. The items’ relevancy was evaluated on a four-point scale. The I-CVI was calculated using items with three or four points. The items with ratings of one or two points were left out of the computation, however, experts gave their opinions regarding potential modifications of the items.
Face Validity
A pilot study was conducted on April 14~15, 2023 with 20 adults aged 19~69 living in the Seoul and Gyeonggi regions using refined preliminary questions to test face validity through the validity and comprehensibility. Furthermore, opinions were openly shared, and modifications and supplements to the questions, font size, question length, question placement, and survey time were considered.
Evaluation of the Scale
Participants and Data Collection
The main survey was conducted nationwide, targeting adults residing in Korea, aged 19~69 years, who could communicate, understood the purpose of the study, and voluntarily agreed to participate. Based on the rationale that the number of participants should be more than five times the number of questions or at least 200 cases,17,21,22 the total number of participants was calculated by combining Exploratory Factor Analysis (EFA, n = 330) and Confirmatory Factor Analysis (CFA, n = 203). The survey was conducted online by a professional research company between April 28 and May 3, 2023. A total of 533 people responded to the online survey; only those who accepted the consent form were allowed to participate. The second survey was performed online on May 23, 2023, 20 days after the first survey, on the basis that a time interval of two to four weeks was appropriate for the study’s subjects’ memories to fade. Thirty-four participants were randomly selected and tested repeatedly for test-retest reliability.
Research Tools
The questionnaire included 64 questions on the EID-PHB, 10 on general characteristics for tool validation, and 12 on the Infection Prevention Behavior Scale of Individuals (IPBS-I) to verify criterion validity. The IPBS-I is a tool developed by Heo and Jang23 to assess individual infection prevention behaviors in adults. Permission to use the tool was obtained to verify the criterion validity.
Data Analysis Method
Data were analyzed using IBM SPSS Statistics version, 29.0 and R version 4.1.2 for Windows software. The adjusted correlation coefficients between the items and the overall score were reviewed as well as the items analyzed below 0.30 were discarded.22 Construct validity was verified using EFA and CFA. The suitability of the EFA was confirmed using Kaiser-Meyer-Olkin (KMO) and Bartlett’s sphericity tests. The Principal Component Analysis (PCA) approach and the Varimax rotation method were utilized for factor extraction. The criteria for determining the number of factors were a communality and factor loading value of 0.50 or greater, and a total cumulative variance of 60% or greater. Through CFA, the model’s goodness of fit was confirmed by χ²/degree of freedom, Standardized Root Mean Residual (SRMR), Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), and Tucker Lewis Index (TLI).24 Convergent validity was assessed using standardized factor loadings, Construct Reliability (CR), and Average Variance Extracted (AVE) values. Discriminant validity was determined based on whether the AVE value exceeded the squared value of the correlation coefficient. According to the validity criteria, CR was applied at 0.70 or higher and AVE at 0.50 or higher,24,25 and the standard for obtaining stable findings if one factor has at least three questions.26 The Pearson correlation coefficient between the EID-PHB and IPBS-I was used to assess criterion validity. Cronbach’s alpha was employed to calculate the tool’s internal consistency, and test-retest reliability was examined using Cronbach’s alpha and intraclass correlation coefficient criteria.27
Ethical Considerations
This study obtained approval from the Institutional Review Board of the researcher’s affiliation (IRB No. SYU 2021–12-007-001). The survey was designed to voluntarily agree to participate after being informed of the purpose of the study, method, procedure, time required, issues related to the provision of personal information, data confidentiality, management of collected data, and the possibility of withdrawal from research participation, among others via an online questionnaire. A professional research company rewarded those who completed the survey with a few points.
Results
Development of the Scale
The study derived seven components and 18 indicators, which included 147 preliminary items based on the tools from the reviewed literature, guidelines,19,28–31 and qualitative content analysis. The components are referred to as droplet prevention, contact prevention, airborne prevention, bloodborne prevention, environmental prevention, daily life prevention, and psychological coping. The item-response scale of the tool was assessed using a five-point Likert scale.
Reduction of the Scale
Following the first content validity verification, 52 items were deleted, and 11 questions were added, resulting in 106 items, reorganizing the second preliminary questions. For the second round, three experts from the first round were included, and a total of six experts evaluated resulting in the deletion of 44 items and addition of 2 items. A total of 64 items were chosen as the third preliminary questions. After the second content validity verification, the I-CVI was 0.83~1.00, and the S-CVI/Average was 0.97. In the third round, the accuracy and readability were confirmed in line with the components and indicators. The selected items were forwarded to a Korean literary professional for feedback, and advice was sought regarding on the appropriateness of grammar, spelling, vocabulary accuracy, spacing, and sentence flow.
As a result of the pilot study, the time required to complete the questionnaire ranged from six to 15 minutes. The I-CVI for validity was 0.70~1.00 and S-CVI was 0.95, the I-CVI for comprehensibility was 0.90~1.00 and S-CVI was 0.99. Modification were made based on the feedback.
Confirmation of Validation Items
A total of 64 items were finalized and were classified by attributes: eight items on droplet prevention, 20 on contact prevention, six on airborne prevention, seven on bloodborne prevention, four on environmental prevention, 10 on daily life prevention, and nine on psychological coping (Supplementary 1).
Evaluation of the Scale
General Characteristics of the Subjects
After randomly extracting data from the 533 respondents, they were divided into two samples, with the first (n = 330) chosen for EFA and the second (n = 203) chosen for CFA (Table 1).
 |
Table 1 Characteristics of Participants (N = 533) |
Item Analysis
According to the data analysis of the 330 EFA participants, the mean and standard deviation of the items ranged from 2.92 ± 1.11 to 4.70 ± 0.53. The skewness and kurtosis were −1.99~0.13, and −0.94~4.25, respectively, and the criteria32 of skewness and kurtosis of less than two and seven were met, indicating the normality of the distribution. Two items with adjusted correlation coefficients overall score of less than 0.30 were evaluated as having a poor contribution to the scale22 and eliminated. In addition, the correlation between the remaining items and the overall score ranged from r = 0.31 to 0.58. The Cronbach’s a for all 62 items was 0.95.
Exploratory Factor Analysis
PCA using the Varimax rotation approach was repeatedly conducted to confirm the construct validity of the chosen 62 items. EFA was carried out with the factors set to ten based on the conceptual framework. Twenty-seven analyses were performed, and 28 of the 62 items were discarded. The eliminated items were one with a communality of less than 0.50 and 22 items with factor loadings less than 0.50, and three with common loadings. In addition, based on the standard,26 a factor must consist of at least three questions to obtain stable results, and two additional items must be reviewed and removed. The EFA was repeated three times in the same manner, and the results were consistent. The KMO value of the selected 34 questions was 0.88, and Bartlett’s test of sphericity was statistically significant at χ²=5521.41 (p < 0.001). The communality of the 34 items ranged from 0.49 to 0.86, while the factor loadings were between 0.42 and 0.86. The three items with a communality and factor loadings below 0.50 were considered essential questions for the tool and were not eliminated. Nine factors exhibited eigenvalues greater than 1.0, and the overall cumulative variance was 63.0% (Table 2).
 |
Table 2 Exploratory Factor Analysis (N = 330) |
Confirmatory Factor Analysis, Convergent, and Discriminant Validity
CFA was performed with a new sample of 203 participants, and the model was developed using nine extracted subfactors based on the EFA result. The model resulted in a good fit, with the χ²/degree of freedom of the model equal to 1.25, CFI was 0.94, TLI was 0.94, and RMSEA was 0.04 (90% confidence interval, 0.03~0.05), and SRMR was 0.08 (Table 3 and Supplementary 2). However, in this study we developed another model based on the proposed conceptual framework, resulting in six components and nine indicators. The model resulted in a good fit, with the χ²/degree of freedom of the model equal to 1.37, CFI was 0.91, TLI was 0.91, and RMSEA was 0.05 (90% confidence interval, 0.04~0.06), and SRMR was 0.09, all of which met the standards. CR was 0.73~0.93 (≥ 0.70) and AVE was 0.41~0.61 (≥ 0.50), indicating that AVE values for bloodborne and environmental prevention were slightly below the recommended levels.24,25 To verify discriminant validity, the correlation coefficient between factors was proven to be r = 0.21~0.60 (p < 0.001) and the AVE values exceeded all squared correlation coefficients, confirming that discriminant validity was established (Table 4 and Supplementary 3).
 |
Table 3 Confirmatory Factor Analysis of the Models |
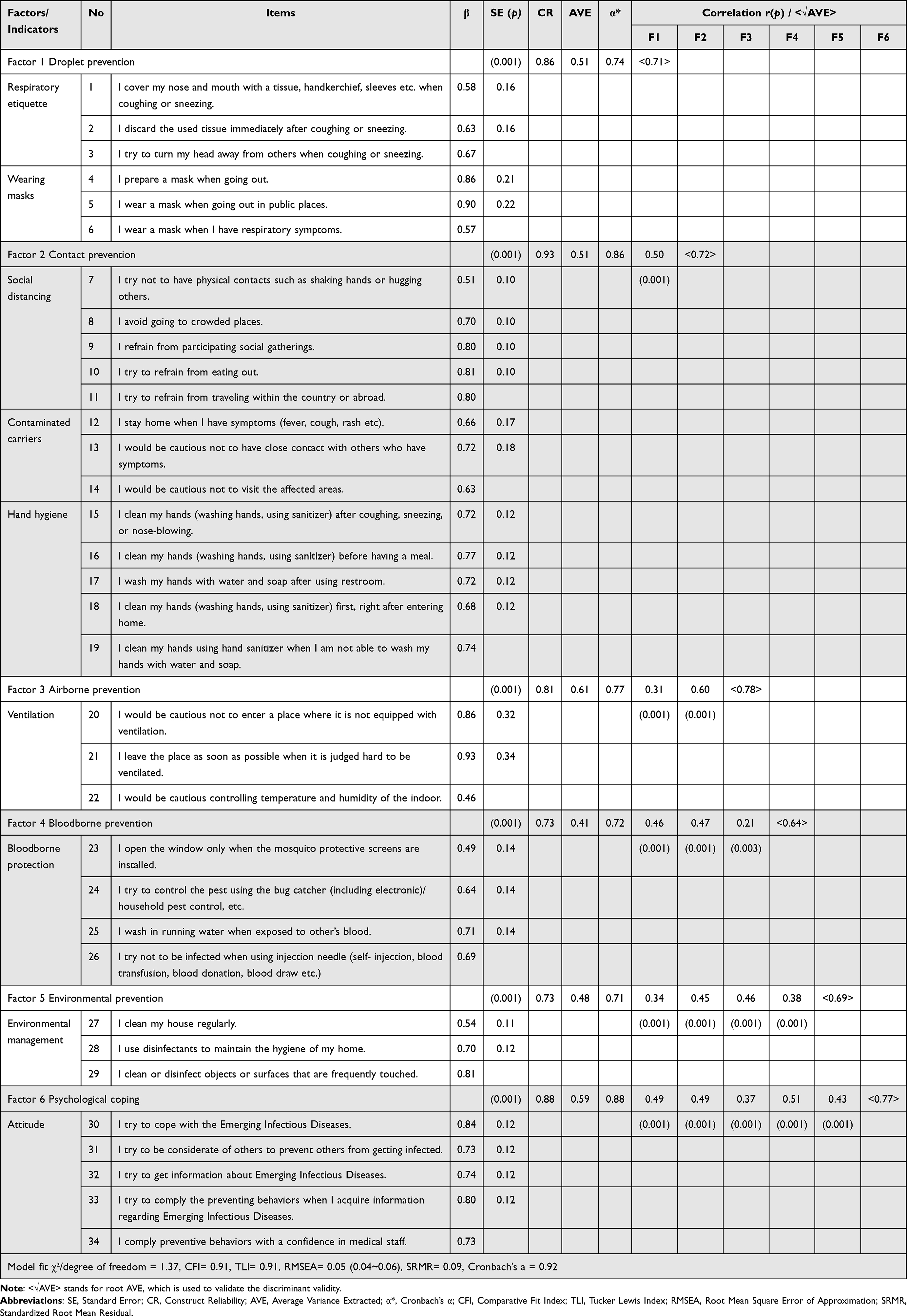 |
Table 4 Confirmatory Factor Analysis, Convergent & Discriminant Validity of the Six-Factor Model (N = 203) |
Criterion Validity
Heo and Jang’s (2021) IPBS-I scale and EID-PHB scales showed a significant positive correlation (r = 0.85, p < 0.001). The correlation between the six components of EID-PHB and IPBS-I was r =0.50~0.73 (p < 0.001), suggesting a substantial positive association and verifying criterion validity.
Reliability
The Cronbach’s a of 34 items was 0.92, along with droplet prevention equal to 0.74, contact prevention at 0.86, airborne prevention at 0.77, bloodborne prevention at 0.72, environmental prevention at 0.71, and psychological coping at 0.88. All these values were above 0.70, the reliability criterion for the new tools.33 For the test-retest reliability, 34 participants took part in the second survey, and Cronbach’s a was 0.93; we observed a slight difference from the first test for each component. The intraclass correlation coefficient was r = 0.88 (95% CI = 0.81~0.93), p < 0.001, meeting the criteria,27 ensuring stability and reliability.
Confirmation of Final Scale
The EID-PHB scale consists of six components and nine indicators: droplet prevention (respiratory etiquette, wearing masks), contact prevention (social distancing, contaminated carriers, hand hygiene), airborne prevention (ventilation), bloodborne prevention (blood protection), environmental prevention (environmental management), and psychological coping (attitude). The measurement range was a five-point Likert scale from one (not at all) to five (very much), with higher scores indicating more preventive behaviors.
Additional Research and Applicability of Complex Model
The preventive behavior path analysis of the final model showed that all six components had a significant positive correlation with preventive behaviors (r = 0.67~0.80, p < 0.001) and had an influence on preventive behaviors (β = 0.24, p = 0.032~0.45, p < 0.001) (Supplementary 4). According to general characteristics, the 60s (3.63 ± 0.79) were found to do more airborne prevention (F = 5.17, p < 0.001) than the 20s (2.87 ± 1.00), and those with higher income performed more environmental prevention (3.76 ± 0.67, 3.10 ± 0.75) and psychological coping (4.04 ± 0.63, 3.83 ± 0.78) than those with lower income (F = 9.47, p < 0.001, F= 5.21, p = 0.006). Individuals perceived as healthy engaged in more environmental prevention (3.88 ± 0.80, 3.44 ± 0.69), psychological coping (4.26 ± 0.46, 3.96 ± 0.68), and overall preventive behaviors (4.00 ± 0.40, 3.78 ± 0.68) than those who were uncertain (F = 6.21, p = 0.002, F = 4.32, p = 0.015, F = 4.11, p = 0.018). Additionally, those with experience of being quarantined due to an emerging infectious disease (3.68 ± 0.69) were found to engage more in environmental prevention (t = 2.15, p = 0.033) than those without the experience of being quarantined (3.45 ± 0.81). The model fit was confirmed to be good, and its reliability was verified.
The preventive behavior scale needed for emerging infectious diseases differs depending on the infection transmission route and the purpose of the research. Hence a complex model was built by grouping the components according to the conceptual framework to assess preventive behaviors’ fit, validity, and reliability (Table 5). In addition, daily life prevention excluded from the study was analyzed independently using EFA. Three items were selected, and their model fit was confirmed through CFA (Supplementary 5).
 |
Table 5 Model Fit of the Additional Complex Model Scale (N = 203) |
Discussion
This study’s factor classification process of blocking infection transmission routes based on the conceptual framework contributed to further subdividing preventive behaviors against emerging infectious diseases. Through interviews, the qualitative research content analysis identified daily life prevention and psychological coping that could not be extracted from the conceptual framework.
The droplet prevention factor is constructed by integrating two indicators which are respiratory etiquette and wearing masks. The first model, which includes these components, is confirmed to be a good fit. However, we reconstructed the model based on the transmission route, and the indirect contribution of the the two indicators was validated using CFA. The average for droplet prevention was relatively high but the adjusted item-total correlation coefficient was relatively low, at r = 0.32~0.43 in the item analysis. Although the droplet prevention performance level was high, the relationship with the overall preventive behavior items required improvement in constructing the questions. The question “I completely cover my nose, mouth, and chin when wearing a mask” had a relatively high average of 4.65 ± 0.62 but was removed as the factor loading value was less than 0.50. On the other hand, in the earlier investigation,8 the result was 0.67. As the debate and interest in proper mask wear continue, the item included in a previous study highlights the need for additional research on wearing masks.
The contact prevention factor is developed by integrating three indicators which are social distancing, contaminated carriers, and hand hygiene. CFA was used to verify the indirect influence of the three components. Items related to social distancing were included in several prior studies34,35 and were discovered to be an inevitable component. During the interviews, most participants emphasized the value of social isolation, and dining out. Some even claimed that they avoided using shared utensils with family members in favor of disposable or personal ones. In contrast, the average level of social distancing in this survey was considered low, ranging from 2.92 ± 1.11 to 3.41 ± 0.98, and was lower than the previous studies (4.07 ± 0.64, 4.68 ± 0.64)34,35 relatively. It was assumed due to the difference in the interval between the interview period (October~November, 2022) and the main survey period (April~May, 2023), which accounted for the difference in the social distancing stage and the social atmosphere and environment. Since it can be presumed that the difference affected the number of preventative behaviors taken into account, quarantine rules and policies should be developed. Previous research6,35 covered all components of the contaminated carrier index, and both the average value in this study (4.08 ± 0.83 to 4.22 ± 0.72), and the previous one (4.72 ± 0.57 to 4.75 ± 0.61)35 were typically high. This result implies that avoiding contact with symptomatic individuals and their surroundings is crucial to preventing the spread of infectious diseases. Therefore, when developing quarantine strategies, significant efforts must be made to develop efficient isolation plans. It is challenging to discern between social distancing and contaminated carriers. Keeping a distance from a symptomatic individual was subcategorized as contaminated carriers rather than social distancing. In practice, contact prevention is a common preventive measure. However, it included large number of items to be evaluated as a single factor. As a result, three indicators are covered in this study: social distancing, contaminated carriers, hand hygiene. In order to generate a simple tool, we suggest merging the indicators into one, and reducing the items in further study.
The average airborne prevention was relatively low, indicating that ventilation and air conditioning were not easy to implement. Despite the fact that ventilation is a subject of government guidelines,30 only few researches34 included ventilation-related items.The item “I use an air purifier/air sterilizer/ air purifier”, which had the highest mean of 3.48 ± 1.20, was eliminated owing to common loading. Because air prevention requires not only ventilation and air conditioning but also wearing a mask, an indicator of droplet prevention, this overlapping tendency is believed to limit the classification of air prevention as a single component. Therefore, we recommend reclassifying airborne prevention-related items in future research due to shortcomings in clarifying the boundaries of the items.
The public’s awareness of and implementation of bloodborne prevention could not be determined because it was not included in Korea’s most recent emerging infectious disease (COVID-19) prevention guidelines. However, the average in this study was considered significant in confirming the level of interest in bloodborne prevention and deriving as a component. The item “I try to use condom for a safe sexual life” was deleted as the item-total correlation coefficient was less than 0.30, whereas the average was 3.95 ± 0.98. Considering the differences in awareness and culture of sexual relations within the country and overseas, issues pertaining to condom use are challenging to employ as a domestic survey item. It is nevertheless, a significant query in terms of EID bloodborne prevention. Hence, condom use and sextual intercourse should be taken into account in future studies.
Although the majority of interviewees stated that they often used alcohol to disinfect their surroundings or their possessions, the associated item’s average score was low. Because society, the environment, and quarantine regulations all have an impact on infection spreads. Environmental management was defined as the dissemination of common vectors, and included items such as keeping the environment clean and using disinfectants. Ventilation, air quality management, and water and food-related queries were not categorized as environmental prevention. These may be accounted for as environmental factors, whereas were reclassified during content validity. Future research should focus on developing items and conducting research on environmental prevention in the future to safeguard the environment, which has a significant effect on public health.
The psychological coping items were developed through qualitative research, and the explanatory power was the highest at 10.4%, indicating the importance of the public’s attitude toward emerging infectious diseases. The average of psychological coping was relatively high, and it was proven that individuals had a caring attitude toward themselves and others. Many interviewees described their experiences of causing harm to others due to infection, giving insight into their thoughts and attitudes toward family members and acquaintances. This result demonstrates how challenging it is to isolate oneself from community life and take preventive actions perceived as inevitable The previous finding9 proved that the impact on others of not performing preventive measures influences an individual’s willingness to take preventive action. Nonetheless, another study36 ascertained that social groups are influenced by our society and what others think affect in decision-making when it comes to engaging in preventive behavior. In either circumstance, it highlights the influence of others on an individual’s decision to comply preventive action.In addition, results35 indicated that information seeking influences preventive behavior. Thus, it has been determined that each item is appropriate for use as psychological coping factor. Furthermore, future studies should focus on community prevention actions and public attitudes and design plans to promote the government’s efforts to prevent emerging infectious diseases.
All items regarding daily life prevention, including those found in earlier studies,10,23 were eliminated. In line with the accepted approach of removing one item each time an EFA was carried out after one item was eliminated, the factor loading values of the related items changed continuously, leading to the removal of several items in a row. An individual’s immunity must be strengthened through daily life prevention. However, maintaining a healthy lifestyle and devoting time to health management is often challenging in today’s hectic world. Furthermore, because infections mediated by vital elements such as water and food may impact the prevention of emerging infectious diseases in the future, the components were reanalyzed based on conceptual framework as an extra study, and a complex model verification was undertaken.
This study demonstrated that scales may be adequately set up and used following the research requirements. Hence, six- and nine-factor scales were introduced. Therefore, a practical tool that can be used in various fields was developed. Overall, the study’s findings suggest the need for conducting additional research and developing scales based on conceptual frameworks.
Finally, caution is needed in generalizing the findings to adults because the proposed survey was conducted online. In addition, one component could not be assessed since relevant questions were eliminated during the verification procedure.
Conclusion
This study developed a 34-item scale consisting of six components and nine indicators of an emerging infectious disease prevention behavior (EID-PHB), and it’s validity and reliability were verified. This approach provides information for future research on preventing new infectious diseases, contributing to the government’s quarantine policy preparation and promotion strategy, and provides helpful primary data for developing theories or tools for preventive behaviors against emerging infectious diseases.
This study has addresses specific and practical questions by subdividing preventive behaviors by transmission route. However, some items were discarded when processing content validity or EFA. Hence, additional analyses are presented in the the Supplementary Material. Furthermore, due to the large number of items, a complex model of contact prevention was designed. Therefore, further study should be conducted to develop a revised version of the EID-PHB in order to simplify the scale.
Ethics Approval and Consent to Participate
The study was conducted following the Declaration of Helsinki, and approved by the Institutional Review Board of Sahmyook University (IRB No. SYU 2021-12-007-001).
Acknowledgments
We thank all the medical staff and professors for the support in content validity.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weiss RA, McMichael AJ. Social and environmental risk factors in the emergence of infectious diseases. Nature Med. 2004;10(12):S70–S76. doi:10.1038/nm1150
2. Cangui-Panchi SP, Nacato-Toapanta AL, Enriquez-Martinez LJ, Salinas-Delgado GA, Reyes J, Garzon-Chavez D. Battle royale: immune response on biofilms - host-pathogen interactions. Curr Res Immunol. 2023;4:1000057. doi:10.1016/j.crimmu.2023.1000057
3. Fauci AS. Infectious diseases: considerations for the 21st century. Clinl Infect Dis. 2021;32(5):675–685. doi:10.1086/319235
4. Munster VJ, Koopmans M, van Doremalen N, van Riel D, de Wit E. A novel coronavirus emerging in China - Key questions for impact assessment. New Engl J Med. 2020;382(8):692–694. doi:10.1056/NEJMp2000929
5. Kasl SV, Cobb S. Health behavior, illness behavior and sick role behavior. I. health and illness behavior. Arch Enviro Health. 1966;12(2):246–266. doi:10.1080/00039896.1966.10664365
6. Plohl N, Musil B. Modeling compliance with COVID-19 prevention guidelines: the critical role of trust in science. Psychol Health Med. 2021;26(1):1–12. doi:10.1080/13548506.2020.1772988
7. Breakwell GM, Fino E, Jaspal R. The COVID-19 preventive behaviors index: development and validation in two samples from the United Kingdom. Eval Health Professions. 2021;44(1):77–86. doi:10.1177/0163278720983416
8. Kim SJ, Kim EY, Yang HR, Chae YJ. Gyeongnam inhabitants’ effects of COVID-19 infection prevention behavior: focus on anxiety and health belief. J Korean Public Health Nurs. 2021;35(1):19–32. doi:10.5932/JKPHN.2021.35.1.19
9. Hong DY, Jeon MA, Cho CH. Predicting preventive behavior intention in COVID-19 pandemic context: application of social variables to health belief model. J Korea Contents Assoc. 2021;21(5):22–35. doi:10.5392/JKCA.2021.21.05.022
10. Yildirim M, Gecer E, Akgul O. The impacts of vulnerability, perceived risk, and fear on preventive behaviours against COVID-19. Psychol Health Med. 2021;26(1):35–43. doi:10.1080/13548506.2020.1776891
11. Yoo W, Choi D, Park K. The effects of SNS communication: how expressing and receiving information predict MERS-preventive behavioral intentions in South Korea. Comput Human Behavior. 2016;62:34–43. doi:10.1016/j.chb.2016.03.058
12. Yoo I. Selection and development of a research measurement. J Nurs Query. 2005;14(1):33–45.
13. Almutairi KM, Alohayani AA, Moussa M, Aboshaiqah AE, Tumala RB, Vinluan JM. Ebola outbreak preparedness and preventive measures among healthcare providers in Saudi Arabia. J Infect Developing Countries. 2016;10(8):829–836. doi:10.3855/jidc.6941
14. Kim JS, Choi JS. Middle East Respiratory syndrome-related knowledge, preventive behaviours and risk perception among nursing students during outbreak. J Clin Nurs. 2016;25(17–18):2542–2549. doi:10.1111/jocn.13295
15. Askarian M, Honarvar B, Tabatabaee HR, Assadian O. Knowledge, practice and attitude towards standard isolation precautions in Iranian medical students. J Hosp Infect. 2004;58(4):292–296. doi:10.1016/j.jhin.2004.07.004
16. Hong SY, Kwon YS, Park HO. Nursing students’ awareness and performance on standard precautions of infection control in the hospital. J Korean Acad Soc Nurs Educ. 2012;18(2):293–302. doi:10.5977/jkasne.2012.18.2.293
17. DeVellis RF. Scale Development: Theory and Applications.
18. Jung SY. How to prevent transmission of infectious agents in healthcare settings. Hany Med Rev. 2011;31(3):190–199. doi:10.7599/hmr.2011.31.3.190
19. Korean Hospital Nurses Association (KHNA). Guideline for isolation precautions in healthcare settings; 2016. Available from: https://khna.or.kr/home/data/khna_guide_ebp08.pdf.
20. Lynn MR. Determination and quantification of content validity. Nursing Res. 1986;35(6):382–385. doi:10.1097/00006199-198611000-00017
21. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Research in Nursing & Health. 2007;30(4):459–467. doi:10.1002/nur.20199
22. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis: A Global Perspective.
23. Heo ML, Jang YM. Development and validation of the infection prevention behavior scale of individuals (IPBS-I) for the general population. J Multidiscipl Health. 2021;14:2791–2802. doi:10.2147/JMDH.S334154
24. Woo JP. Concept and Understanding of Structural Equation Model: AMOS 4.0-20.0. Seoul: Hannarae; 2012:150–176.
25. Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Market Res. 1981;18(1):39–50. doi:10.2307/3151312
26. MacCallum RC, Widaman KF, Zhang S, Hong S. Sample size in factor analysis. Psychological Methods. 1999;4(1):84–99. doi:10.1037/1082-989X.4.1.84
27. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chirop Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
28. Siegel JD, Rhinehart E, Jackson M, Chiarello L. Health care infection control practices advisory committee. 2007 Guideline for isolation precautions: preventing transmission of infectious agents in health care settings. Am J Infect Control. 2007;35(10):S65–S164. doi:10.1016/j.ajic.2007.10.007
29. Korea Disease Control and Prevention Agency (KDCA). Standard prevention guidelines for medical-related infections (2017); 2017. Available from: https://www.kdca.go.kr/board/board.es?mid=a20507020000&bid=0019&act=view&list_no=138061.
30. Korean Disease Control and Prevention Agency. Daily life prevention guidelines 6-2 edition; 2022. Available from: https://www.kdca.go.kr/board/board.es?mid=a20507020000&bid=0019&act=view&list_no=719392..
31. Korea Disease Control and Prevention Agency (KDCA). Infectious disease homepage. guidelines for infectious diseases; 2022. Available from: https://npt.kdca.go.kr/npt/biz/npp/portal/nppPblctDtaMain.do?pblctDtaSeAt=7.
32. Curran PJ, West SG, Finch JF. The robustness of test statistics to nonnormality and specification error in confirmatory factor analysis. Psychological Methods. 1996;1(1):16–29. doi:10.1037/1082-989X.1.1.16
33. Nunnally JC. Psychometric Theory.
34. Lee WK. The Effects of Perception of COVID-19 Campaign on Respiratory Infection Preventive Behavior: Mediated by Health Belief Model(HBM) [master’s thesis]. Seoul: Sahmyook University; 2021:129.
35. Liu PL. COVID-19 information seeking on digital media and preventive behaviors: the mediation role of worry. Cyberpsychol Behav Soc Net. 2020;23(10):677–682. doi:10.1089/cyber.2020.0250
36. Lee WK, Shin SR. Integrated factors affecting intention of COVID-19 preventive behaviours including vaccination in Korea. Nursing Open. 2023;10(5):3424–3431. doi:10.1002/nop2.1597
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.