Back to Journals » Journal of Pain Research » Volume 19
Development of an Expert Consensus on Electroacupuncture for Trigeminal Neuralgia Using the Delphi Method: A Study Protocol
Authors Xu MR ![]() , Chen NS, Wang JY, Wang D, Fan WW, Hao YB, Liu F, Yang ZH, Jiang J, Wu YY
, Chen NS, Wang JY, Wang D, Fan WW, Hao YB, Liu F, Yang ZH, Jiang J, Wu YY ![]() , Chen K
, Chen K
Received 26 August 2025
Accepted for publication 17 December 2025
Published 8 January 2026 Volume 2026:19 563427
DOI https://doi.org/10.2147/JPR.S563427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Mo-Ran Xu,1,* Ni-Sang Chen,1,* Jun-Yi Wang,1 Dong Wang,2 Wei-Wei Fan,3 Ya-Bo Hao,4 Fan Liu,2 Zhang-Hui Yang,2 Ji Jiang,2 Kun Chen,3 Yuan-yuan Wu1
1The Third Affiliated Hospital, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2Zhejiang Greentown Cardiovascular Hospital, Hangzhou, Zhejiang, People’s Republic of China; 3Pingyang Research Institute, Zhejiang Chinese Medical University, Wenzhou, Zhejiang, People’s Republic of China; 4Jiaxing Hospital of Traditional Chinese Medicine, Jiaxing, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kun Chen, Pingyang Research Institute Zhejiang Chinese Medical University XX Chezhan Avenue, Aojiang Town, Pingyang County, Wenzhou, Zhejiang, 325401, People’s Republic of China, Email [email protected] Yuan-yuan Wu, The Third Affiliated Hospital Zhejiang Chinese Medical University, 219 Moganshan Road, Xihu District, Hangzhou, Zhejiang, 310005, People’s Republic of China, Email [email protected]
Introduction: Electroacupuncture (EA) is increasingly used in the management of trigeminal neuralgia (TN), yet treatment approaches vary widely across clinical practice. Standardized guidelines are currently lacking. This protocol describes a Delphi study designed to develop expert consensus on EA use for TN.
Methods and Analysis: A multi-round Delphi process will be conducted with a multidisciplinary panel of clinicians in acupuncture, and neurology. Survey items will be developed from a systematic review, and experts will rate them to evaluate their relevance and level of agreement. Consensus will be determined using predefined criteria following the ACcurate COnsensus Reporting Document (ACCORD) guideline.
Ethics and Dissemination: This protocol has received ethics approval from the relevant institutional review boards and has been registered on the Open Science Framework (OSF). The findings will be disseminated through peer-reviewed publications and academic conferences.
Conclusion: This study outlines a modified Delphi process designed to develop a structured expert consensus on the use of EA for TN. Its primary aim is to address the considerable heterogeneity in current EA practice by establishing a standardized framework for clinical and research parameters.
Contribution to the Literature: This study addresses the lack of standardized recommendations for EA in TN and aims to provide structured expert guidance to support more consistent clinical practice.
Keywords: electroacupuncture, trigeminal neuralgia, Delphi method, expert consensus
Introduction
Clinical Status of Trigeminal Neuralgia and Electroacupuncture Management
Trigeminal neuralgia (TN) is a rare neuropathic facial pain disorder characterized by recurrent, paroxysmal attacks along one or more branches of the trigeminal nerve. According to the International Association for the Study of Pain, TN is classified into three etiological subtypes: classical, idiopathic, and secondary.1
First-line pharmacological therapy, including carbamazepine and oxcarbazepine, provides initial pain relief in most patients; however, long-term benefit frequently diminishes.2–5 Treatment is further limited by tolerance, adverse effects such as dizziness, ataxia, hyponatremia, and hepatotoxicity, and the common need for dose escalation, which increases the risk of toxicity.6–8 Discontinuation often leads to rapid recurrence of pain.
For patients who are unresponsive or intolerant to medication, surgical interventions such as microvascular decompression (MVD), radiofrequency thermocoagulation, glycerol rhizolysis, and gamma knife radiosurgery are available. MVD offers the most durable relief, but it is invasive and carries risks including cranial nerve deficits, hearing loss, cerebrospinal fluid leakage, and stroke.9,10 Recurrence occurs in approximately 30–50% of patients within 10–20 years, especially in those without evident vascular compression.11,12 Other minimally invasive procedures may provide short-term relief but are associated with sensory deficits, delayed analgesic onset, and substantial recurrence rates.13,14 Consequently, there remains a critical unmet need for therapies that are effective, durable, and well tolerated, particularly for elderly individuals and those with comorbidities seeking to avoid invasive procedures.
Electroacupuncture (EA), which combines manual acupuncture with controlled electrical stimulation, has emerged as a promising non-invasive modality. EA allows more precise control over stimulation parameters such as frequency and intensity and may enhance analgesic outcomes. Preclinical studies indicate that EA can reduce pain behaviors and modulate molecular pathways within the trigeminal system that are relevant to neuropathic pain.15,16 Neuroimaging research is also expanding; for example, a 2021 randomized protocol using resting-state functional magnetic resonance imaging aims to investigate central responses to EA in TN.17
Clinical evidence is gradually increasing. A multicenter randomized controlled trial in 2024 reported that EA combined with low-dose carbamazepine produced superior pain reduction compared with either therapy alone, with fewer adverse effects than carbamazepine monotherapy.18 Recent systematic reviews and meta-analyses have further suggested that acupuncture, including EA, may reduce pain severity and attack frequency in TN compared with pharmacological treatment, although methodological heterogeneity and potential bias remain concerns.19,20 Collectively, available evidence suggests that EA may reduce medication burden and delay or prevent the need for surgery in selected patients. A detailed analysis of its peripheral and central analgesic mechanisms will be presented in a later section to contextualize the rationale for developing technical consensus.
Current Evidence Gaps and Study Rationale
Despite encouraging findings, the clinical application of EA in TN remains inconsistent. Stimulation parameters such as waveform, frequency, current intensity, pulse width, and duration substantially influence outcomes but are often selected empirically.21–23 This heterogeneity limits reproducibility and complicates the interpretation of clinical trial data, underscoring the need for standardized and evidence-based guidance.24,25
To address these gaps, we will employ a modified Delphi method to develop expert-informed recommendations. This approach provides anonymized, iterative feedback to mitigate groupthink and authority bias, ensuring balanced contributions from specialists in neurology, pain medicine, and acupuncture.26
Our primary objective is to establish a clinically actionable expert consensus covering four domains: (1) diagnosis and patient stratification, (2) EA technical specifications, (3) therapeutic efficacy and combination therapy, and (4) long-term management and prevention.25,26 Key components will include diagnostic criteria, acupoint selection, parameter optimization, treatment schedule, and core outcome measures. The consensus targets clinicians and researchers across China, incorporating perspectives from seven major geographic regions to reflect national clinical practices.27,28
Through multi-rounds of structured questionnaires, we will refine expert responses to achieve formal agreement. The goal is to produce practical recommendations for standardizing EA in TN and to provide a methodological framework for future Delphi studies in this field.
Methods
Registration and Ethics
This study has received ethical approval. The study protocol was registered on the Open Science Framework (OSF; https://DOI.org/10.17605/OSF.IO/EJRNF). Any significant protocol amendments will be submitted for ethical committee approval and updated on the OSF registry. The study will adhere to the Conducting and Reporting of Delphi Studies (CREDES) guidelines and the ACCURATE CONSENSUS REPORTING DOCUMENT(ACCORD) for implementation, conducting at least three Delphi survey rounds. An online questionnaire will be distributed for a minimum of three rounds to an expert panel comprising clinical specialists in acupuncture and neurology from within China.
Study Design
This study will use a multiround Delphi method to develop consensus on clinical and technical recommendations for electroacupuncture treatment of trigeminal neuralgia. The Delphi method allows anonymous feedback, structured iteration, and controlled refinement of expert opinion, making it appropriate for consensus formation in interdisciplinary pain management research. Each Delphi round will include quantitative ratings and qualitative feedback, followed by aggregated group-level summaries to inform subsequent rounds.
Expert Selection
Steering Committee
A Steering Committee has been established to oversee the research methodology. The committee reviewed preliminary survey items synthesized through systematic literature review and advised on the design of the first and subsequent questionnaires. It comprises one chief physician in acupuncture, one chief physician in neurology, and one methodological expert. Committee members were selected based on (1) at least ten years of clinical or research experience in acupuncture or trigeminal neuralgia, and (2) leadership of at least two relevant projects as principal investigator.
Expert Inclusion Criteria
This study aims to produce a clinically robust and methodologically sound consensus guideline. To achieve this, a multidisciplinary expert panel will be formed by recruiting experienced specialists in acupuncture and neurology. Experts will be recruited according to the following prespecified inclusion criteria:
(1) at least ten years of experience in clinical practice, research, or education relevant to trigeminal neuralgia;
(2) a mid-level or higher professional title; and
(3) willingness to provide informed consent and complete all Delphi rounds.
Experts must demonstrate substantial clinical experience with trigeminal neuralgia diagnosis and management. All experts must commit to full participation across all planned rounds.
Expert Panel Composition
The study will be designed to maximize professional, socioeconomic, and geographical diversity, ensuring comprehensive representation across clinical settings. At least seventy percent of the experts will hold senior professional titles such as associate chief physician, associate professor, or higher, reflecting the authority and expertise required for consensus formation.
The Steering Committee will aim to recruit experts from major regions of China, including both urban medical centers and rural medical institutions. This broad inclusion strategy ensures that diverse clinical environments and resource levels are represented. Experts from different socioeconomic contexts will also be included to capture a wide range of practical experiences and decision-making strategies. All expert identities will remain strictly confidential during the survey. After the study concludes, contributing experts will be acknowledged in the final guideline.
To mitigate the potential impact of attrition, a 25% oversampling strategy will be implemented during Round 1 recruitment. This ensures that the final sample size remains adequate, even if some experts withdraw. A minimum of 40 experts will be recruited in the first round. Previous studies have shown that each subgroup in a multidisciplinary Delphi study should include at least 10 participants.11 Accordingly, the protocol will ensure a minimum of 10 experts in each of the two subgroups: acupuncture and neurology/pain medicine.29 This approach guarantees that at least 20 experts will remain by the final round. To maintain data consistency and avoid introducing heterogeneous perspectives that could compromise the consensus-building process,30 no additional experts will be recruited throughout the study.
Expert Recruitment Process
Experts will be invited through email, accompanied by an invitation letter and study information document. Candidate experts will be identified through three primary strategies: (1) systematic screening of corresponding authors who published relevant studies on trigeminal neuralgia or acupuncture in the last five years in major databases such as PubMed, Web of Science, and China National Knowledge Infrastructure; (2) distribution of invitations through professional academic societies, including the China Association of Acupuncture-Moxibustion and the Society for Neuroscience; (3) recommendations from Steering Committee members to address potential gaps in regional or disciplinary representation.
Two rounds of invitations will be conducted to meet recruitment targets. Potential experts will receive a demographic questionnaire for eligibility assessment. Before the first Delphi round, participants must provide basic demographic information (age, gender, current institution/clinic, professional title, years of experience) and detailed information on professional qualifications, clinical practice, academic background, and specific experience in managing trigeminal neuralgia. The Steering Committee will conduct uniform eligibility screening of all nominees based on pre-defined criteria. Following confirmation of participation intent and eligibility, questionnaires will be distributed via email. Each confirmed expert will be asked to commit to completing all Delphi rounds. Participation is entirely voluntary, and experts may withdraw at any time without reason. All participants will receive a Delphi study information sheet detailing the types of data collected and the study rationale.
Confidentiality and Conflict of Interest Disclosure
To ensure objectivity, only the principal investigator and data manager will have access to experts’ personally identifiable information. All Delphi questionnaires will display only anonymous expert ID codes.31 Prior to the first survey round, all invited experts must complete a conflict of interest disclosure statement using the International Committee of Medical Journal Editors (ICMJE) uniform form (Supplementary Materials 1). Collected information spans multiple dimensions, including research funding, speaker fees, consultancy fees, patents, equity, and academic affiliations. All declared conflicts will be categorically recorded. An anonymized summary table of conflicts of interest will be published as supplementary material alongside the final study results. Items meeting the “significant relevant conflict of interest” criterion (defined as a single transaction ≥ USD 10,000 or an equity share >5%) will be individually annotated via footnotes in the main research text.
The Delphi panel will not include patient or public representatives because the study addresses highly specialized clinical and technical parameters that require expert knowledge. Nonetheless, patient perspectives may be incorporated in later stages, such as external review of the completed guideline.
Questionnaire Development
Item Generation
The initial questionnaire items will be developed through a systematic synthesis of multi-source evidence to ensure completeness, clinical relevance, and methodological rigor. Item development will cover four major modules.
a) Diagnosis and Patient Stratification Module:
We will derive items from authoritative clinical guidelines, including the International Classification of Headache Disorders Third Edition published by the International Headache Society and relevant diagnostic and therapeutic guidelines issued by the Chinese Society of Neurology. The team will extract key content such as diagnostic criteria, differential diagnoses, indications, contraindications, and disease staging and will convert this information into structured statements suitable for expert rating.
b) Electroacupuncture Technical Specification Module:
We will generate items through a systematic literature review. Two independent reviewers will extract clinical parameters including core acupoints, electroacupuncture stimulation characteristics, session duration, and treatment frequency from eligible studies. The team will conduct qualitative synthesis and frequency analysis to identify commonly used regimens, controversial areas, and evidence gaps. We will then transform these results into draft technical specification items. Figure 1 shows the localization of commonly used acupoints on the upper limb, Figure 2 shows the localization of acupoints commonly selected along the affected branches of the trigeminal nerve.
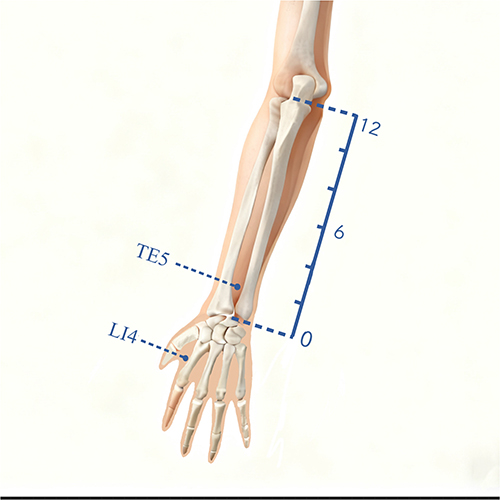 |
Figure 1 Upper limb acupoint indication. |
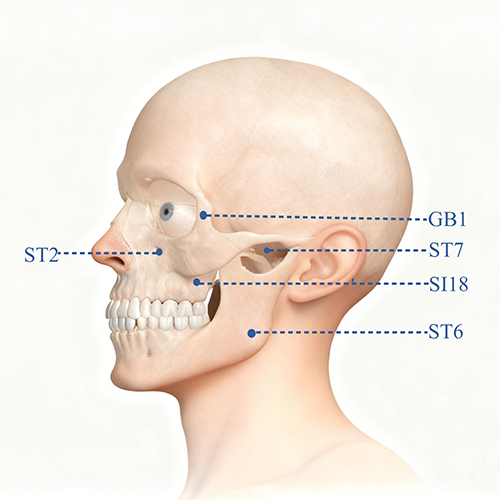 |
Figure 2 Facial acupoint indication. |
c) Efficacy and Adjunctive Therapy Module:
We will develop items by integrating evidence from systematic reviews and clinical guidelines. The team will collect core outcome indicators from high-quality studies reporting pain relief, functional improvement, patient-reported outcomes, and reductions in medication usage. We will base items related to dose reduction or discontinuation of analgesic medications on neuropharmacological principles and patterns identified in acupuncture research. Safety items will draw on adverse event reporting standards from the Standards for Reporting Interventions in Clinical Trials of Acupuncture checklist.
d) Long-Term Management and Prevention Module:
The team will formulate items through secondary analysis of systematic reviews and guideline recommendations. We will synthesize indirect evidence regarding relapse prevention, lifestyle modification, prognosis, and patient education and will convert this evidence into structured consensus items.
The core research team will review all initially generated items to ensure clarity, eliminate redundancy, and maintain consistency before forming the preliminary item pool for the Delphi survey.
Systematic Search Design
A systematic search strategy was used to identify literature supporting item generation. An initial search using “electroacupuncture AND trigeminal neuralgia” produced 204 articles. Because electroacupuncture is a subset of acupuncture, the search was expanded to include acupuncture studies related to trigeminal neuralgia and facial pain, yielding a total of 4863 articles. The study screening flow will be presented in a flowchart following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. As shown in Figure 3.
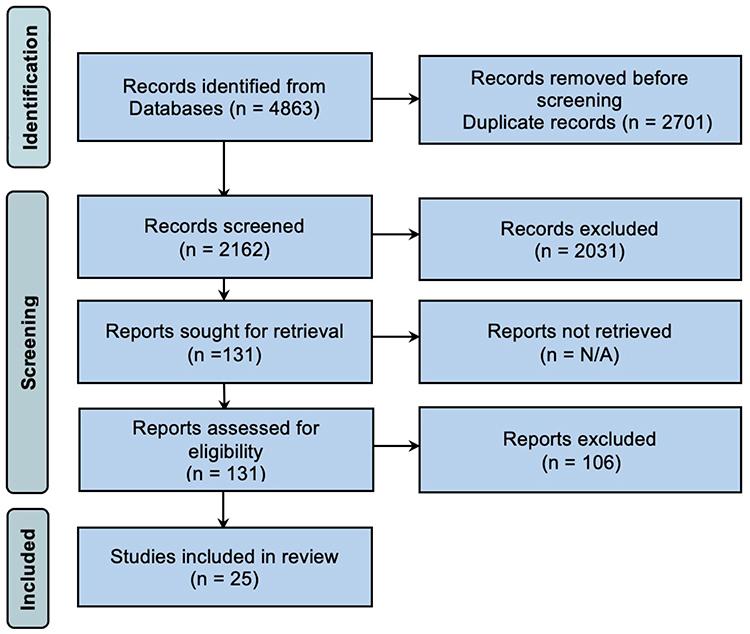 |
Figure 3 PRISMA Flow Diagram. |
Databases and Timeframe
The following databases were searched from inception to December 13, 2024: PubMed, CNKI, Wanfang Data (WF), China Biology Medicine disc (CBM), VIP Database (VIP), Web of Science Core Collection (WOS CC), Cochrane Library, and Embase.
Sample Search Strategy (for Example, CNKI and PubMed)
CNKI: Topic 1: trigeminal neuralgia + facial pain + primary trigeminal neuralgia + classical trigeminal neuralgia + secondary trigeminal neuralgia; Topic 2: acupuncture + acupuncture-moxibustion + electroacupuncture; connected with “AND”.
PubMed: (“trigeminal neuralgia” [MeSH]) AND ((acupuncture [MeSH]) OR (electroacupuncture [MeSH]))
Inclusion Criteria
(a) Language: Chinese or English; (b) Article type: systematic review of observation studies, meta-analysis, or randomized controlled trial; (c) Inclusion of acupoint and explicit electroacupuncture parameters; (d) Statistically significant primary outcome measures. Publication date was not restricted.
All retrieved records were imported into EndNote 20 for automatic deduplication. To maximize identification of relevant literature, a rigorous dual-reviewer independent screening process was employed. After deduplication, 2,162 articles remained. Following title and abstract screening, 2,031 records were excluded, leaving 131 for full-text review. Based on pre-defined eligibility criteria, articles were excluded during full-text assessment for: (a) animal studies, case reports, narrative reviews, and study protocols were excluded; (b) electroacupuncture not being the primary intervention; (c) ineligible population; (d) full text unavailable; (e) inappropriate statistical methods. If the same study was published in different languages, the version with the most detailed content was retained. If methodological discrepancies existed between different reports, the version with more rigorous methodological description was prioritized. Any disagreements between reviewers during screening were first resolved through discussion. If consensus was not reached, a third reviewer was consulted for arbitration. Ultimately, 25 articles fully met the inclusion criteria.18,32–55 The study screening flow will be presented in a flowchart following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A summary of the included studies, including acupoint selection and electroacupuncture parameters, is presented in Table 1.
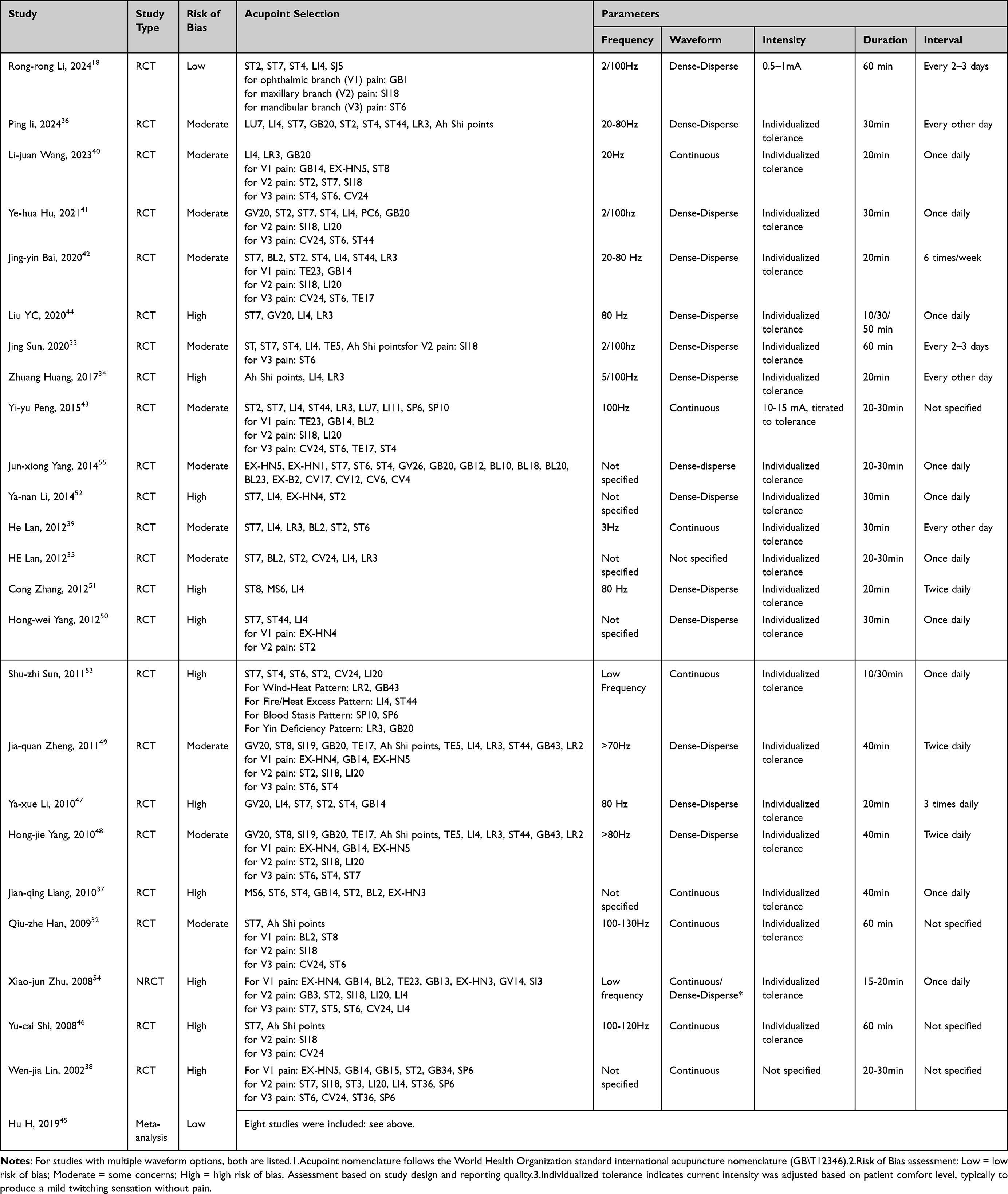 |
Table 1 Summary of Studies from the Literature Review |
Evidence Synthesis and Quality Assessment
Data Extraction
Based on the 25 studies included in the aforementioned systematic review, evidence synthesis will employ a systematic approach combining both quantitative and qualitative methods. The data extraction process will be conducted in the following steps:
- Independent Data Extraction:
Two independent reviewers will extract data on electroacupuncture technical parameters, including acupoint selection, stimulation parameters, and treatment courses. Each reviewer will work independently to minimize bias. They will use a standardized data extraction form developed for this purpose to ensure consistency across all included studies. The form will capture relevant details such as study design, sample size, acupuncture techniques, and clinical outcomes.
- Use of Tools and Software:
The data extraction will be performed using Microsoft Excel 2019. This tool will help organize and manage the data systematically. For quality control, the reviewers will cross-check their extractions, and discrepancies will be resolved through discussion or consultation with a third reviewer if needed.
- Quantitative and Qualitative Analysis:
Following data extraction, quantitative analysis will describe the distribution characteristics of electroacupuncture parameters (eg, the most commonly selected acupoints, stimulation frequencies, and treatment durations). Concurrently, qualitative methods will summarize the theoretical rationales, differentiated treatment strategies, and long-term management approaches as documented in clinical guidelines and high-quality studies. These findings will be synthesized into structured consensus statements for the initial questionnaire.
- Role of Reviewers:
The two reviewers will independently extract data, assess the quality of studies, and ensure that the extracted data is consistent with the objectives of the review. In case of any disagreements, the reviewers will resolve them through discussion, or consult a senior methodological expert for arbitration if necessary. This ensures the accuracy and integrity of the data extraction process.
Evidence Quality Assessment
The Grading of Recommendations Assessment, Development and Evaluation framework (GRADE) will be used to assess evidence quality. Randomized controlled trials will be assessed using the Cochrane Risk of Bias 2.0 (ROB 2.0) tool, and observational studies will be evaluated using the ROBINS I tool. Two independent reviewers will conduct all assessments. Disagreements will be resolved through discussion or consultation with a senior expert. Evidence will be graded as high, moderate, low, or very low, with justifications attached to each consensus item to maintain transparency.
Questionnaire Implementation
Delphi questionnaires will be administered through the Questionnaire Star electronic platform. Experts will receive personalized survey links, informed consent documents, and instructions via email. Participation will begin after experts submit electronic consent.
The platform supports anonymous responses and independent rating to minimize conformity bias. Response progress will be monitored by the research team. Automated reminders will be sent to manage non-response bias. Each round will remain open for two to three weeks. Reasons for mid-survey withdrawal will be documented to ensure process transparency.
Delphi Process
A minimum of three Delphi rounds will be conducted according to the Conducting and Reporting of Delphi Studies guideline and established methodological recommendations. Rounds will be spaced approximately 4–6 weeks apart to allow for analysis and questionnaire revision. As shown in Figure 4.
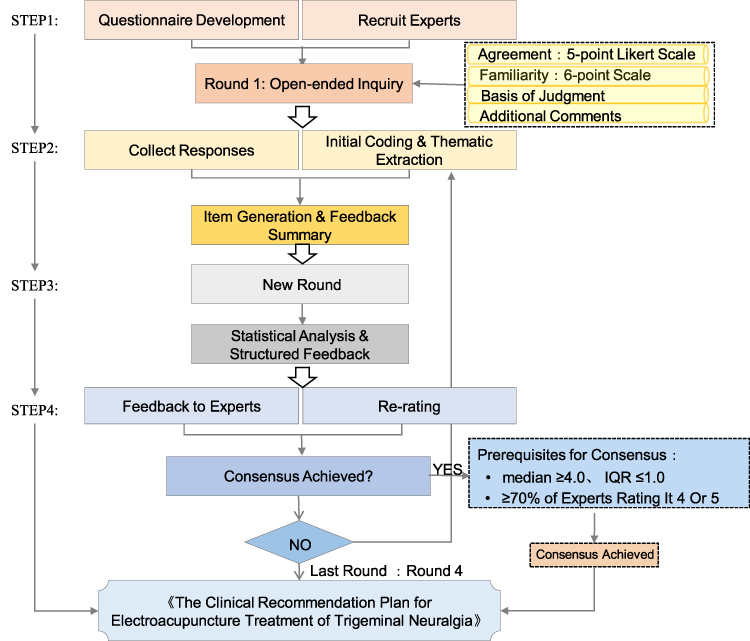 |
Figure 4 Delphi Study Schema. |
Round Procedures
Round 1: In addition to initial open-ended questions, experts will rate their level of agreement with all other items using a 5-point Likert scale (1=Strongly Disagree, 2=Disagree, 3=Neutral, 4=Agree, 5=Strongly Agree). Questionnaire items will also be assessed across four dimensions: familiarity, consensus level, basis of judgment, and additional comments with detailed scoring (Supplementary Table 1 for detailed scoring criteria). Familiarity is rated on a six-point scale (very unfamiliar to very familiar), corresponding to scores of 0–1.0. Consensus level uses a five-point Likert scale (strongly disagree to strongly agree), corresponding to scores of 1–5. Experts will also select the primary basis for their judgment from four categories (practical experience, theoretical analysis, literature / peer consensus, intuition), assigning corresponding weights. All items and open-ended questions include a comment field for supplementary feedback. Responses to open-ended questions will undergo cross-coded thematic analysis by the writing team to extract core concepts; these themes will be compiled and synthesized into new closed-ended items for subsequent rounds through iterative discussion with the Steering Committee.
The pre-defined consensus threshold will be: within each expert panel, an item will need to meet all three criteria—median ≥4.0, interquartile range (IQR) ≤1.0, and ≥70% of experts rating it 4 or 5 (Agree/Strongly Agree). Items meeting this threshold in Round 1 will be retained and excluded from subsequent questionnaires. Items with a median ≤2.0, IQR ≤1.0, and ≥70% of experts scoring 2 or 1 (Disagree/Strongly Disagree) will be deleted. Items receiving a significant proportion of “no opinion” ratings or a combined “Agree”/“Strongly Agree” percentage ≤50% will be reviewed, revised if necessary by the Steering Committee, and retained for the next round. The Committee may also revise and retain items slightly below the consensus threshold if deemed valuable, provided sufficient rationale is given. All revisions will be documented. After each round, the Steering Committee will review all data and feedback, and the writing team will adjust subsequent questionnaires accordingly.
Round 2: The second-round questionnaire will be developed based on the thematic analysis results of Round 1 open-ended responses and structured item data. In this round, experts may modify their previous responses based on the aggregated Round 1 results and feedback. They can also view information on the consensus status of each item from the previous round and compare their own response distribution with that of the panel. Items reaching the pre-set consensus threshold in this round will be excluded from the third-round questionnaire. Items meeting the deletion threshold will be removed. Items that consecutively receive a significant proportion of overall “no opinion” ratings or a combined “Agree” / “Strongly Agree” percentage still ≤50% across the first two rounds will be identified for further review. These items will be revised by the Steering Committee based on expert feedback and included in the next round. A summary table detailing revised items and the rationale for changes will be provided to the expert panel.
Round 3: In the third round, experts may modify their responses based on the aggregated second-round results and feedback. They can also view information on the consensus status of each item from the previous round and compare their personal response distribution with that of the panel. If any items remain below the pre-set consensus threshold after this round, the writing team and Steering Committee will review and revise them according to pre-defined criteria and may initiate a fourth survey round. Conversely, if all items achieve consensus after the third round, the Delphi survey process concludes.
Round 4 (Optional): When necessary, a fourth round will be conducted to allow final confirmation of revised items. Experts will vote on the Clinical Recommendation Plan for Electroacupuncture Treatment of Trigeminal Neuralgia containing all consensus items. This round focuses purely on final confirmation and does not include iterative revision or new item development.
If items still fail to reach consensus after Round 4, they will be classified as “No Consensus Reached”.
Consensus Process Description
The study will implement a structured, transparent consensus development process. In each round, experts will be able to: (1) Compare their current ratings with aggregated panel results. (2) View the consensus status of each item. (3) Assess how their own judgments align with the distribution of peer opinions.
This transparent feedback mechanism encourages informed reconsideration without compromising independent expert judgment. Experts may revise their ratings if they reconsider their perspective based on group-level insights or qualitative themes. This iterative adjustment process reflects core principles of the Delphi method.
Consensus Establishment and Item Decision Rules
Consensus will be defined using three quantitative criteria simultaneously: Median ≥ 4; interquartile range (IQR) ≤ 1; At least 70% of experts scoring the item as 4 or 5.
These thresholds will apply within each expert subgroup (acupuncture and neurology/pain medicine). An item must satisfy the criteria in both subgroups to be considered “consensus achieved.”
Deletion Threshold
Items will be deleted if they meet the following criteria:
- Median ≤ 2
- IQR ≤ 1
- At least 70% scoring 1 or 2
Based on this operational definition, item processing follows these rules:
Retention: Items achieving consensus in both expert subgroups in any round are directly retained and excluded from subsequent questionnaires.
Further Review
Items that do not meet either consensus or deletion criteria will be carried forward to the next round. Before carry-forward:
- The Steering Committee will review clarity, evidence base, clinical applicability, and qualitative feedback.
- Items may be revised before inclusion in the next round.
For items close to consensus (for example, agreement between 65% and 69%), the Steering Committee may employ a reconsideration mechanism to determine whether they merit revision and re-evaluation. All revisions and decisions will be logged for transparency.
Stopping Criteria
The Delphi process will follow a multi-stage stopping rule:
- If all items reach consensus by Round 3, the Delphi survey ends.
- If a small number of clinically important items do not reach consensus, they may be revised and included in Round 4.
- After Round 4, no additional survey rounds will be conducted.
- Items failing to reach consensus will be labeled “No Consensus Reached” and reported transparently in the final output.
Following completion of all rounds, all consensus items will be compiled into a Clinical Recommendation Plan for Electroacupuncture Treatment of Trigeminal Neuralgia. The complete plan will be circulated to experts for final confirmation.
Missing Data Handling
Systematic strategies have been established to address potential missing data during the data collection process, ensuring the reliability and validity of the study results. A minimum completion standard is set for questionnaire response rates, requiring a valid response rate of over 70% per survey round. Rounds failing to meet this standard will be excluded from final analysis, and supplementary data collection procedures (such as extending the survey period or re-inviting experts) will be initiated to maintain representativeness.
For item-level missing values, we will apply the complete case analysis principle in each round. Consensus levels will be calculated based solely on data from experts who have answered each specific item, thus avoiding the introduction of estimation bias through data imputation. No imputation will be applied to missing data at the item level; only valid responses will be considered in the analysis. This approach ensures the integrity of the consensus process and prevents the distortion of results due to missing data.
To mitigate potential declines in expert engagement over time, proactive measures will be implemented to maintain panel participation. These measures include providing personalized feedback reports after each round and sending regular follow-up communications (such as Email reminders or phone contact) to encourage continued participation.
Expert Attrition Management
This study employs a proactive strategy to manage expert attrition. During the protocol design phase, an attrition rate of approximately 25% per round is anticipated. To counteract this, an oversampling mechanism has been implemented in the first round to ensure an adequate expert reserve for subsequent rounds.
To maintain expert engagement, personalized feedback reports will be provided after each survey round, which will include a comparative analysis between individual expert ratings and the panel’s opinion distribution. In addition, systematic Email reminders and telephone follow-ups will be used to maintain active interaction.
Reasons for mid-study withdrawal will be carefully documented to analyze attrition patterns. The representativeness of the remaining panel will be continuously monitored with regard to professional background, institutional affiliation, and geographical distribution to ensure that the findings are not biased by attrition.
To maintain consistency in the expert authority coefficient and ensure data continuity, no new experts will be recruited after the second round. All analyses will be based solely on data from experts who complete all rounds, ensuring the rigor and reliability of the consensus-building process.
Questionnaire Pretesting
Before the Delphi survey begins, the Steering Committee will conduct a pretest of the questionnaire. They will independently complete the draft questionnaire in a simulated environment, evaluating:
- Clarity and readability
- Content validity
- Logical structure
- Functionality of the electronic platform
After evaluation, the committee will meet to resolve issues and implement revisions. Ambiguous or unclear items will be modified or removed. The finalized version of the Round 1 questionnaire will then be approved for distribution.
Expert Feedback Design
Following each Delphi round, experts will receive individualized feedback reports. These reports will include:
- Group-level agreement percentages
- Distribution of panel responses
- Comparison between the expert’s own rating and panel distribution
- Key qualitative themes summarizing open-ended comments
The Questionnaire Star platform will generate feedback reports automatically. Templates will be reviewed by the Steering Committee to ensure neutrality and accuracy.
Anonymity Mechanism Safeguards
A strict anonymity protocol will be implemented to protect independence of judgment:
- Experts will not have access to the identities of their peers
- Only the principal investigator and data manager will have access to identifiable information
- Steering Committee members (except the principal investigator) will not communicate directly with experts regarding study content
- All data will be encrypted and stored securely, with access restricted to authorized personnel
Identifiable data will be removed immediately upon export and replaced with unique anonymous codes.
Response Collection
The Questionnaire Star online platform will be used for data collection. Each round will be distributed through a unique link sent to each expert. Responses will be automatically encrypted and stored on the platform’s secure servers. The system will record timestamps and close access after the deadline. After each round, anonymized data will be exported for statistical analysis.
Data Analysis
All data processing procedures will follow the Appraisal of Guidelines Research and Development Conference (ACCORD) guideline to ensure transparent, reproducible, and high quality conduct of this Delphi study. All returned questionnaires will be anonymized before entry by removing personal identifiers and assigning a unique study code to each expert.
Data Entry and Verification
Two trained data managers will independently enter all questionnaire data into a prespecified electronic database. A comparison procedure will then identify any discrepancies between the two entries. A senior researcher will adjudicate each discrepancy by checking the original questionnaire. This will generate a verified master dataset for every Delphi round.
Data Cleaning and Preprocessing
After verification, the dataset will undergo systematic cleaning. We will examine completeness, out of range values, and logical inconsistencies. We will handle missing data according to the prespecified analysis plan. All required derived variables will be created at this stage, including the authority coefficient (Cr). Experts will rate their familiarity (Cs) on a zero to one scale and their basis of judgment (Ca) on a zero to ten scale. To avoid scale inconsistency and to comply with standard Delphi methodology, we will rescale Ca to a zero to one range before computing Cr. The authority coefficient will be calculated as Cr = (Ca + Cs) / 2. Higher values will represent greater credibility of expert judgment.
Statistical Analysis
Microsoft Excel 2019 will be used only for preliminary data checking and basic descriptive statistics. No formal statistical analyses will be conducted using Excel. All formal statistical analyses will be conducted in IBM SPSS Statistics version 31.0.1 to ensure reproducibility.
Expert demographic characteristics will be summarized with counts and percentages. Since item ratings are ordinal, all core variables will be described using medians and interquartile ranges, consistent with methodological guidance for Delphi research. Authority coefficients and response rates will also be summarized in this manner.
After each round, we will provide structured feedback to all experts. The feedback will include their own previous rating for each item, the group median, the group interquartile range, and anonymized qualitative comments from the panel. Feedback will be structured to ensure expert anonymity while providing sufficient information for experts to reassess their previous ratings in light of the group consensus, thus supporting controlled iteration—a defining feature of the Delphi technique.
Predefined decision rules will guide the retention, deletion, modification, or carry forward of items. An item will be retained if the median rating is at least four, the interquartile range is no greater than one, and at least seventy percent of experts assign ratings of four or five. An item will be deleted if the median rating is no greater than two, the interquartile range is no greater than one, and at least seventy percent of experts assign ratings of one or two. Items that do not meet either threshold will be carried forward to the next round. When an item receives substantial qualitative disagreement or has a wide interquartile range, we may modify the wording according to the anonymous comments and present the revised item in the next round. All modifications and their rationale will be documented in the protocol audit file.
Consensus across items will be evaluated with the Kendall coefficient of concordance W. SPSS will be used to compute W values, their ninety-five percent confidence intervals, and p-values. Kendall’s W will be calculated separately for each subgroup (acupuncture and neurology/pain medicine experts) and for the full panel to assess within-group and overall consensus. Differences between subgroups will be carefully considered to identify any significant discrepancies in ratings. This planned analytic approach will allow transparent reporting of agreement within and across disciplines and aligns with recommended practice for Delphi protocols.
Disagreement Resolution
A structured disagreement resolution procedure will ensure objectivity, methodological rigor, and consistency.
Initial Discussion
If discrepancies arise between the two independent reviewers or between a reviewer and the data manager, the involved individuals will first engage in direct discussion to clarify differences in interpretation or data extraction. This step aims to achieve mutual understanding and consensus.
Escalation to Senior Methodological Expert
If initial discussion does not resolve the disagreement, the issue will be escalated to a senior methodological expert. This expert will evaluate the evidence, examine the positions of both parties, and provide an independent, methodological judgment to resolve the disagreement.
Reevaluation and Reassessment
For disagreements involving data discrepancies or interpretation issues, the data manager may be asked to reexamine raw data. Additional statistical consultation or secondary review may be performed if needed. Revised outputs will be shared with all reviewers to ensure agreement on the final interpretation.
Final Arbitration
If disagreements remain unresolved after expert evaluation, a final arbitration will be conducted. This may involve a broader expert panel or an external advisor. All decisions made during arbitration will be final and binding.
All steps and outcomes will be fully documented to maintain transparency and accountability.
Participation Incentives
To promote sustained engagement across multiple Delphi rounds, the study will implement ethically appropriate participation incentives.
Experts who complete all Delphi rounds will receive formal acknowledgment as contributors in the final academic publication. After study completion, each expert will receive a personalized summary report describing how individual contributions influenced the final recommendations.
Periodic updates about study progress will be shared to maintain open communication and foster a sense of involvement. These incentives aim to respect and affirm expert contributions, in alignment with the Accurate Consensus Reporting Document guideline.
Questionnaire Accessibility Adjustments
All Delphi questionnaires will be administered electronically using the Questionnaire Star platform, chosen for its accessibility across devices and operating systems. The platform requires no installation and is compatible with Windows, macOS, Android, and iOS devices. A responsive design will allow optimal display on different screen sizes.
Questionnaires will include:
- Clear step-by-step instructions
- A progress indicator
- User-friendly navigation
A dedicated technical support channel, including a designated Email and telephone hotline, will be available during office hours to resolve participants’ technical issues. These measures aim to minimize barriers to participation and ensure efficient, reliable data collection.
Study Implementation and Timeline
The study will follow a predefined seven-month timeline. During the first two months, the Steering Committee will review and finalize the study protocol, supervise development and pretesting of the first-round questionnaire, and confirm expert eligibility.
The first Delphi round will begin in month three and remain open for three weeks. After each round, the research team will allocate approximately two weeks for data cleaning, statistical analysis, and preparation of individualized feedback reports, after which the next round will be launched. Subsequent rounds will follow the same schedule, with data collection lasting two to three weeks and analysis lasting two weeks. All survey rounds are expected to be completed by the end of month five.
The final two months will be dedicated to comprehensive data analysis, interpretation of consensus results, and preparation of the final report and related academic outputs. The Steering Committee will oversee progress at key stages. If challenges arise, such as low response rates, predefined contingency measures—including staged reminder emails or moderate extension of data collection windows—will be activated to ensure timely and successful completion of the study.
Anticipated Methodological Strengths and Limitations
This study employs a modified Delphi method adhering to ACCORD guidelines, presenting several notable methodological strengths. These strengths are primarily reflected in its pre-registered analysis protocol and systematic consensus-building process. By pre-specifying data management procedures, statistical analysis methods, and item decision criteria, the protocol effectively reduces arbitrariness during analysis.
However, the study also possesses some inherent limitations. The primary limitations relate to the composition and representativeness of the expert sample: despite quality control measures such as authority and response coefficients, participant selection may be constrained by geographical and disciplinary accessibility, potentially failing to fully represent expert views from all relevant fields. Secondly, the potential for group conformity effects inherent in the Delphi method itself must be considered. While anonymous feedback mechanisms aid consensus formation, they may inadvertently marginalize innovative or critical perspectives held by a minority of participants. Furthermore, although pre-defined quantitative consensus criteria (for example, median and IQR thresholds) provide operational clarity, their establishment involves a degree of subjective judgment. These criteria may not fully capture the nuanced dynamics of the consensus development process. These limitations will be thoroughly discussed in the final study report, carefully defining the boundaries within which conclusions can be generalized.
Additional Information
Supporting Institutions and Their Roles
This study was primarily conducted by the Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, which was responsible for core research tasks including expert recruitment and data collection. Pingyang County Hospital of Traditional Chinese Medicine, Zhejiang Chinese Medical University, served as a collaborating institution, undertaking auxiliary research work such as systematic literature searches and data extraction. Ethical review and procedural supervision of the study protocol were independently managed by the Ethics Committees of The Third Affiliated Hospital of Zhejiang Chinese Medical University and Pingyang County Hospital of Traditional Chinese Medicine, Zhejiang Chinese Medical University. No other supporting or endorsing institutions were involved in the design, implementation, or decision-making processes of this study.
Conflict of Interest Statement and Management
To uphold the objectivity of the research process and the credibility of its findings, a systematic mechanism for declaring and managing conflicts of interest has been established. Prior to agreeing to participate, all invited experts were required to complete a standardized conflict of interest disclosure form. This form mandates the disclosure of all potential conflicts within the scope of the study, including financial interests, academic rivalries, and any other non-financial interests.
The Steering Committee will confidentially review all disclosed conflicts of interest to assess whether they might substantially compromise an expert’s impartiality. If a conflict is deemed significant, appropriate measures will be taken, such as adjusting their consultation weight, limiting their participation in discussions on specific topics, or, if necessary, excluding them from the study.
To ensure transparency, a de-identified summary of the disclosed conflicts of interest will be made publicly available alongside the final research outputs. This summary will aggregate the nature of the conflicts but will ensure expert anonymity to maintain the integrity of the research process.
Funding Sources and Their Role
This study was supported by the Joint TCM Science & Technology Projects of National Demonstration Zones for Comprehensive TCM Reform in 2025, including the Major Project (Grant No. GZX-KJS-ZJ-2025-006) and its Sub-project (Zhejiang Province’s Traditional Chinese Medicine Science and Technology Plan in 2025 No. 2025ZS043), as well as the Hangzhou Natural Science Foundation Project of 2026 (Grant No. 2025SZRJJ0464). The funders provided financial support only and were not involved in any aspect of the research, including study design, expert selection, questionnaire development, data collection and analysis, or consensus formation. No medical writing assistance was received; all aspects of the research design, implementation, and output were independently completed by the research team.
Results
This study protocol describes a Delphi-based approach to develop an expert consensus on EA for TN, addressing the current lack of standardized treatment protocols. A multidisciplinary panel of experts in acupuncture, neurology, and pain medicine will participate in multiple survey rounds focusing on four domains: diagnosis and stratification, EA technical specifications, therapeutic efficacy and combination therapy, and long-term management. The process follows predefined consensus criteria (median ≥4, IQR ≤1, ≥70% agreement) and adheres to international reporting guidelines, for example, ACCORD and CREDES, to ensure methodological rigor and transparency. The expected output is a structured consensus document intended to standardize EA practice for TN and inform future clinical research.
Discussion
This study protocol details a modified Delphi approach to establish the first structured expert consensus on electroacupuncture (EA) for trigeminal neuralgia (TN). The anticipated consensus aims to standardize key clinical and research parameters, addressing a major source of heterogeneity in current practice. If successful, its core value lies in providing a foundational “reference standard” to enhance methodological rigor in future trials and support clinical decision-making.
The significance of standardizing EA for TN is further underscored by its distinct mechanism of action within the broader landscape of neuromodulation therapies. Unlike pharmacologic agents or single-target interventions, EA employs a sophisticated, dual-mode mechanism integrating peripheral signal modulation with central nervous system (CNS) regulation. This integrated approach may underlie its potential clinical advantages.
Peripherally, EA delivers targeted intervention at the site of pain signal initiation. Evidence suggests it can downregulate hyperpolarization-activated cyclic nucleotide-gated (HCN) channels in the trigeminal ganglion, directly reducing neuronal hyperexcitability.56 It also modulates key pain mediators like Calcitonin Gene-Related Peptide (CGRP), potentially inhibiting neuro-immune interactions.57 Emerging research points to a novel role in suppressing ferroptosis in sensory neurons via the SAT1/ALOX15 pathway, thereby mitigating oxidative damage and promoting neuronal survival.58 These multi-target actions at the ganglion level help attenuate the primary drive of neuropathic pain.
Centrally, EA induces multi-level neuromodulation that filters and modulates ascending nociceptive signals. Its analgesic effect is frequency-dependent: low-frequency stimulation promotes the release of enkephalins and endomorphins, while high-frequency stimulation triggers dynorphin, engaging diverse opioid receptors. Beyond the opioid system, EA robustly activates descending inhibitory pathways from the periaqueductal gray (PAG) and brainstem nuclei, increasing spinal serotonin and norepinephrine to gate pain transmission. Neuroimaging studies indicate it can also modify activity in higher-order pain processing regions like the anterior cingulate cortex (ACC) and insula.59 Notably, the sustained effects observed after a treatment course imply the induction of beneficial neuroplasticity within these central circuits. This central modulation may also extend to limbic areas, such as the ventral tegmental area (VTA), potentially explaining improvements in the anxiety and depression often comorbid with chronic TN.60
This dual “peripheral targeting + central multi-level modulation” profile positions EA uniquely. It contrasts with systemic medications that often carry broad side effects and differs from invasive surgeries that carry procedural risks. Specifically, regarding safety, EA’s most common adverse events (for example, minor local bleeding) are typically transient, presenting a favorable profile compared to the systemic toxicity of drugs like carbamazepine or the risk of permanent neurologic deficits from surgery.61 In terms of cost-effectiveness, as a form of acupuncture, EA shows promise for favorable long-term value in managing chronic pain, potentially reducing reliance on continuous medication or repeat procedures.62
An important anatomical consideration is the significant inter-individual variability in trigeminal nerve anatomy,63 which likely contributes to heterogeneous treatment responses. Therefore, the expert consensus sought in this study carries deeper significance: it represents a collective empirical framework to navigate this variability, offering a “common denominator” for identifying effective stimulation parameters amidst anatomical uncertainty.
The primary contribution of this research is to directly address the urgent challenge of protocol heterogeneity. A standardized consensus will provide a reference framework for future high-quality trials, enabling reliable comparison and meta-analysis—essential steps for elevating the evidence base. Clinically, it could standardize strategies for “medication reduction” or “surgery delay,” providing a structured non-pharmacological alternative. Limitations of EA itself, such as practitioner dependency and unclear optimal long-term regimens, are acknowledged and are precisely the issues the consensus’s “long-term management” module seeks to guide.
We also acknowledge limitations of this consensus-building exercise. The panel, while nationally representative within China, may limit global generalizability. The Delphi method, while minimizing bias, may still marginalize minority viewpoints. These boundaries will be explicitly discussed in the final report.
In conclusion, this Delphi study is a necessary foundational step to formalize expert knowledge and reduce procedural variability. Establishing this consensus is not merely an answer to current heterogeneity but a prerequisite for definitive clinical trials, personalized strategy exploration, and deeper mechanistic investigation into EA for TN.
Conclusion
This protocol outlines a modified Delphi study designed to establish a structured expert consensus on applying EA to TN. Its primary aim is to address the significant heterogeneity in current EA practices by developing a standardized framework for key clinical and research parameters.
The successful implementation of this Delphi process may contribute to the development of a foundational “reference standard.” This consensus is intended to enhance the methodological rigor and comparability of future clinical trials, potentially facilitating the generation of higher-level evidence. Clinically, it seeks to provide practitioners with a synthesized, expert-informed protocol that could support decision-making in the application of EA for TN.
We explicitly acknowledge the inherent limitations of this consensus-building approach. The outcomes will reflect expert opinion derived through a structured process, rather than direct clinical evidence. Their applicability may be influenced by factors such as the composition of the expert panel and the regional context in which this study is conducted. Additionally, variability in expert opinions may introduce some degree of uncertainty in the final recommendations.
Furthermore, the clinical value and efficacy of any consensus recommendations must be prospectively validated through subsequent research. The potential for variation in expert perspectives and the need for clinical validation highlight the importance of ongoing investigation to confirm the relevance and applicability of these recommendations in diverse clinical settings.
In summary, this Delphi study represents a necessary foundational step in formalizing expert knowledge and reducing procedural variability. It aims to establish a common framework that is essential for advancing definitive clinical research and optimizing EA therapy for TN, while recognizing that the true clinical impact will only be determined through further validation.
Abbreviations
EA, Electroacupuncture; TN, Trigeminal Neuralgia; ACCORD, ACcurate COnsensus Reporting Document; CREDES, Conducting and REporting of DElphi Studies; OSF, Open Science Framework; ICMJE, International Committee of Medical Journal Editors; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; GRADE, Grading of Recommendations Assessment, Development and Evaluation; ROB 2.0, Risk of Bias tool 2.0; ROBINS-I, Risk Of Bias In Non-randomized Studies - of Interventions; MVD, Microvascular Decompression; CNS, Central Nervous System; ACC, Anterior Cingulate Cortex; PAG, Periaqueductal Gray; VTA, Ventral Tegmental Area; CGRP, Calcitonin Gene-Related Peptide; HCN channels, Hyperpolarization-activated Cyclic Nucleotide-gated channels; CNKI, China National Knowledge Infrastructure; WF, Wanfang Data; CBM, China Biology Medicine; VIP, VIP Database; WOS CC, Web of Science Core Collection; SPSS, Statistical Package for the Social Sciences; IQR, Interquartile Range; Cr, Authority Coefficient; Cs, Familiarity; Ca, Basis of judgment; SAT1, Spermidine/Spermine N1-Acetyltransferase 1; ALOX15, Arachidonate 15-Lipoxygenase; CCL2, C-C Motif Chemokine Ligand 2 Other Study Terms; RCT, Randomized Controlled Trial; NRCT, None-Randomized Controlled Trial.
Data Sharing Statement
The original data presented in this study are included in the article; further inquiries can be directed to the corresponding author, Yuan-yuan Wu.
Statement of Ethics
The study was approved by the Third Affiliated Hospital of Zhejiang Chinese Medical University (ZSLL-KY-2025-055-01) and received ethics approval from Pingyang County Hospital of Traditional Chinese Medicine (Ethics Approval Number: 2025-I-003).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Joint TCM Science & Technology Projects of National Demonstration Zones for Comprehensive TCM Reform in 2025, including the Major Project (Grant No. GZX-KJS-ZJ-2025-006) and its Sub-project (Zhejiang Province’s Traditional Chinese Medicine Science and Technology Plan in 2025 No. 2025ZS043), as well as the Hangzhou Natural Science Foundation Project of 2026 (Grant No. 2025SZRJJ0464).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lambru G, Zakrzewska J, Matharu M. Trigeminal neuralgia: a practical guide. Pract Neurol. 2021;21(5):392–22. doi:10.1136/practneurol-2020-002782
2. Chisari CG, Sgarlata E, Arena S, et al. An update on the pharmacological management of pain in patients with multiple sclerosis. Expert Opin Pharmacother. 2020;21(18):2249–2263. doi:10.1080/14656566.2020.1757649
3. Montano N, Conforti G, Di Bonaventura R, et al. Advances in diagnosis and treatment of trigeminal neuralgia. Ther Clin Risk Manag. 2015;11:289–299. doi:10.2147/TCRM.S37592
4. Deng Z, Hou R, Zhai X, et al. Expert consensus on non-surgical diagnosis and treatment methods of traditional Chinese and Western medicine for primary trigeminal neuralgia. J Pract Stomatol. 2022;38(2):149–161.
5. Di Stefano G, De Stefano G, Leone C, et al. Real-world effectiveness and tolerability of carbamazepine and oxcarbazepine in 354 patients with trigeminal neuralgia. Eur J Pain. 2021;25(5):1064–1071. doi:10.1002/ejp.1727
6. Berghuis B, Hulst J, Sonsma A, et al. Symptomatology of carbamazepine- and oxcarbazepine-induced hyponatremia in people with epilepsy. Epilepsia. 2021;62(3):778–784. doi:10.1111/epi.16828
7. Chong MS, Bahra A, Zakrzewska JM. Guidelines for the management of trigeminal neuralgia. Cleve Clin J Med. 2023;90(6):355–362. doi:10.3949/ccjm.90a.22052
8. Zhou J, Ma R, Jin Y, et al. Molecular mechanisms of opioid tolerance: from opioid receptors to inflammatory mediators (Review). Exp Ther Med. 2021;22(3):1004. doi:10.3892/etm.2021.10437
9. Liu H, Wang C, Zhang H, et al. Exploring acupuncture as a therapeutic approach for tic disorders: a review of current understanding and potential benefits. Front Neurol. 2025;16:1447818. doi:10.3389/fneur.2025.1447818
10. Luo W, Wu Y, Wang K, et al. Research progress of traditional Chinese medicine treatment of trigeminal neuralgia in recent three years. Clin J Tradit Chin Med. 2020;32(5):987–991.
11. Edwards JW, Shaw V. Acupuncture in the management of trigeminal neuralgia. Acupunct Med. 2021;39(3):192–199. doi:10.1177/0964528420924042
12. Ichida MC, Zemuner M, Hosomi J, et al. Acupuncture treatment for idiopathic trigeminal neuralgia: a longitudinal case-control double blinded study. Chin J Integr Med. 2017;23(11):829–836. doi:10.1007/s11655-017-2786-0
13. Sun J, Fang JQ, Shao XM, et al. Staged treatment of trigeminal neuralgia by Prof. Jianqiao Fang. Chin Acupunct Moxibust. 2016;36(2):191–193.
14. Jin Z, Feng X, Wang YL, et al. Therapeutic efficacy of electroacupuncture with blood-stabbing in the treatment of trigeminal neuralgia. Shanghai J Acupunct Moxibust. 2012;31(10):719–720.
15. Shen ZQ, Chang WQ, Liang LF, et al. Electroacupuncture effects on trigeminal neuralgia with comorbid anxiety and depression: the role of frequency and acupoint specificity. FASEB J. 2025;39(2):e70337. doi:10.1096/fj.202402461RR
16. Yang L, Ding W, You Z, et al. Alleviation of trigeminal neuropathic pain by electroacupuncture: the role of hyperpolarization-activated cyclic nucleotide-gated channel protein expression in the Gasserian ganglion. Acupunct Med. 2019;37(3):192–198. doi:10.1177/0964528419841614
17. Tang D, Zhang X, Xu Y, et al. The central response of electroacupuncture on trigeminal neuralgia based on resting-state functional magnetic resonance imaging: a protocol for a pre-experimental, single-centre, randomized, controlled trial. J Pain Res. 2021;14:3321–3331. doi:10.2147/JPR.S334078
18. Li R, Sun J, Luo K, et al. Electroacupuncture and carbamazepine for patients with trigeminal neuralgia: a randomized, controlled, 2 × 2 factorial trial. J Neurol. 2024;271(8):5122–5136. doi:10.1007/s00415-024-12433-x
19. Ang L, Kim HJ, Heo JW, et al. Acupuncture for the treatment of trigeminal neuralgia: a systematic review and meta-analysis. Complement Ther Clin Pract. 2023;52:101763. doi:10.1016/j.ctcp.2023.101763
20. He HX, Li YX, Xiao YS, et al. The efficacy of acupuncture for trigeminal neuralgia: an overview of systematic reviews. Front Neurol. 2024;15:1375587. doi:10.3389/fneur.2024.1375587
21. Gu CY, Hu J, Cai YB, et al. Advances of studies on stimulating parameters of electroacupuncture. Chin Acupunct Moxibust. 2003;23(8):489–491.
22. Huang GF, Zhang HX, Zhang TF, et al. Analgesic duration and intervention on plasma-related factors in the treatment of lumbar disc herniation by electroacupuncture at pinch point. Chin J Clin Rehabil. 2006;10(43):1–6.
23. Yan LJ, Fu HW, Zhao Y, et al. Research progress of the mechanism of acupuncture analgesia based on electroacupuncture frequency. Shanghai J Acupunct Moxibust. 2016;35(1):121–124.
24. Fang K, Cheng W, Yu B. Effects of electroacupuncture at varied frequencies on analgesia and mechanisms in sciatic nerve cuffing-induced neuropathic pain mice. J Mol Neurosci. 2024;74(4):98. doi:10.1007/s12031-024-02276-6
25. Yin Z, Wang F, Sun M, et al. Acupuncture methods for primary trigeminal neuralgia: a systematic review and network meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2022;2022:3178154. doi:10.1155/2022/3178154
26. Diamond IR, Grant RC, Feldman BM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–409. doi:10.1016/j.jclinepi.2013.12.002
27. Bendtsen L, Zakrzewska JM, Abbott J, et al. European academy of neurology guideline on trigeminal neuralgia. Eur J Neurol. 2019;26(6):831–849. doi:10.1111/ene.13950
28. Chinese Medical Doctor Association. Expert consensus on the diagnosis and treatment of idiopathic and secondary trigeminal neuralgia. Chin Med J. 2025;105(25):2058–2071.
29. Schifano J, Niederberger M. How Delphi studies in the health sciences find consensus: a scoping review. Syst Rev. 2025;14(1):14. doi:10.1186/s13643-024-02738-3
30. Humphrey-Murto S, Varpio L, Wood TJ, et al. The use of the delphi and other consensus group methods in medical education research: a review. Acad Med. 2017;92(10):1491–1498. doi:10.1097/ACM.0000000000001812
31. International Committee of Medical Journal Editors. ICMJE Form for Disclosure of Potential Conflicts of Interest. Available from: https://www.icmje.org/disclosure-of-interest/.
32. Han QZ. Clinical observation on 30 cases of primary trigeminal neuralgia treated by electroacupuncture. Guid J Tradit Chin Med Pharm. 2009;15(9):35.
33. Sun J, Li R, Li X, et al. Electroacupuncture therapy for change of pain in classical trigeminal neuralgia. Medicine. 2020;99(16):e19710. doi:10.1097/MD.0000000000019710
34. Huang Z, Huo J, Zhao J. Efficacy on primary trigeminal neuralgia treated with triple puncture technique and electroacupuncture at trigger points. Zhongguo Zhen Jiu. 2017;37(1):31–34. doi:10.13703/j.0255-2930.2017.01.007
35. He L, Zhou WY, Zhang XM. Trigeminal neuralgia of hyperactive of liver yang type treated with acupuncture at Xiaguan (ST 7) at different depth: a randomized controlled trial. Zhongguo Zhen Jiu. 2012;32(2):107–110.
36. Li P, Li Z. Liver-sparing and Shen-tuning acupuncture combined with electroacupuncture in the treatment of primary trigeminal neuralgia combined with depression. Mod J Integr Tradit Chin West Med. 2024;33(13):1836–1840.
37. Liang JQ. Efficacy of cephalic needle parietal anterior temporal oblique in the treatment of central trigeminal neuralgia. Shanghai J Acupunct Moxibust. 2010;29(8):528.
38. Lin WJ. Treatment of 62 cases of trigeminal neuralgia with prolonged retention of needles. Acupunct Moxibust Clin J. 2002;(12):38–39.
39. He L, Zhang XM. Clinical effect of sphenopalatine ganglion needling in treating primary trigeminal neuralgia of Liver-yang upsurge syndrome type. Chin J Integr Med. 2012;18(3):214–218. doi:10.1007/s11655-012-1021-2
40. Wang LJ, Li C, Wang F. Observations on the efficacy of snap acupuncture combined with electroacupuncture in the treatment of primary trigeminal neuralgia. J Pract Chin Med. 2023;39(3):586–588.
41. Hu YH, Dong P, Feng XX, et al. Clinical study of electroacupuncture combined with repetitive transcranial magnetic stimulation in the treatment of primary trigeminal neuralgia. Chin J Geriatr Dent. 2021;19(6):325–330.
42. Bai JY, Zheng ZY. Observation on the efficacy of the treatment of primary trigeminal neuralgia by combining electroacupuncture with Xia Guan acupoint as the main point. Electron J Cardiovasc Dis Integr Tradit Chin West Med. 2020;8(21):145.
43. Peng YY, Luan L. Efficacy of electroacupuncture at different intensities in the treatment of primary trigeminal neuralgia. Hubei J Tradit Chin Med. 2015;(2):61–62.
44. Liu YC, Zhao N, Mu JL, et al. Effect of electroacupuncture on the efficacy of trigeminal neuralgia with different needle retention times. China Herald Med. 2020;17(9):138–144.
45. Hu H, Chen L, Ma R, et al. Acupuncture for primary trigeminal neuralgia: a systematic review and PRISMA-compliant meta-analysis. Complement Ther Clin Pract. 2019;34:254–267. doi:10.1016/j.ctcp.2018.12.013
46. Shi YC. Electroacupuncture “trigger point” method in the treatment of trigeminal neuralgia. Clin J Acupunct Moxibust. 2008;24(12):32–33.
47. Li YX, Huang XY, Liu X, et al. Observation on the clinical efficacy of electroacupuncture in the treatment of patients with trigeminal neuralgia. J Tradit Chin Med. 2010;38(1):90–91.
48. Yang HJ. Observation on the efficacy of acupuncture combined with electroacupuncture in the treatment of primary trigeminal neuralgia. Hebei Tradit Chin Med. 2010;32(6):891–892.
49. Zheng JQ, Shi JP. Observation on the efficacy of electroacupuncture in the treatment of primary trigeminal neuralgia. Inn Mong Tradit Chin Med. 2011;30(1):62–64.
50. Yang HW, Gao WB. Clinical journal of acupuncture and moxibustion in the treatment of primary trigeminal neuralgia. Clin J Acupunct Moxibust. 2012;28(4):10–11.
51. Zhang C. Efficacy of electroacupuncture in the treatment of primary trigeminal neuralgia. Liaoning J Tradit Chin Med. 2013;40(6):1214–1215.
52. Li YN. Clinical observation of the combination of traditional Chinese and Western medicine in the treatment of primary trigeminal neuralgia. China Health Ind. 2014;11(5):189–190.
53. Sun SZ, Cui ZY. Effect of different needle retaining times of electroacupuncture on trigeminal neuralgia. Chin Acupunct. 2011;31(3):213–215.
54. Zhu XJ, Wang XZ. Electro-acupuncture combined with the trigger point needle-embedding for treatment of primary trigeminal neuralgia in 31 cases. J Tradit Chin Med. 2008;28(1):13–14. doi:10.1016/s0254-6272(08)60005-9
55. Yang JX, Zhang JP, Yu JC, et al. A clinical study of the combination of air-street electroacupuncture intervention and spinal balance in the treatment of primary trigeminal neuralgia. Chin Acupunct. 2014;34(8):763–768.
56. Mason B, Boyd K, Doubal F, et al. Core outcome measures for palliative and end-of-life research after severe stroke: mixed-method delphi study. Stroke. 2021;52(11):3507–3513. doi:10.1161/STROKEAHA.120.032650
57. Li YK, Liu Y, Jia WB, et al. Construction of cough reflex intensity score for critically ill patients based on the Delphi method. World J Emerg Med. 2023;14(3):235–237. doi:10.5847/wjem.j.1920-8642.2023.045
58. Wan K, Jia M, Zhang H, et al. Electroacupuncture alleviates neuropathic pain by suppressing ferroptosis in dorsal root ganglion via SAT1/ALOX15 signaling. Mol Neurobiol. 2023;60:6121–6132. doi:10.1007/s12035-023-03463-z
59. Qi P, Li Q, Han M, et al. The analgesic mechanism of electroacupuncture at the central level for neuropathic pain: a review of studies based on animal experiments. Front Neurol. 2025.
60. Ma X, Chen W, Yang -N-N, et al. Potential mechanisms of acupuncture on neuropathic pain based on somatosensory system. Front Neurosci. 2022.
61. Kong S, S·h J, Koo S, et al. Electroacupuncture alleviates neuropathic pain by inhibiting spinal CCL2-driven microglial activation. Int J Mol Sci. 2025;26(18):9049. doi:10.3390/ijms26189049
62. Cong W, Peng Y, Meng B, et al. The effect of electroacupuncture on regulating pain and depression-like behaviors induced by chronic neuropathic pain. Annals of Palliative Medicine. 2021;10:104–113. doi:10.21037/apm-20-1900
63. Ogut E, Armagan K, Barut C. Reappraisal of the types of trigeminal porus and importance in surgical applications. Surg Radiol Anat. 2021;43(7):1169–1178. doi:10.1007/s00276-020-02651-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Electroacupuncture for Trigeminal Neuralgia: Study Protocol for a Multicenter Randomized Controlled Trial
Chen N, Xu M, Wang J, Wang D, Luo K, Hao YB, Chen K, Yang X, Ren H, Fang J, Wu Y
Journal of Pain Research 2026, 19:616735
Published Date: 3 June 2026