Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Development of a Cardiac Catheterization Laboratory Nursing Program Targeting Patients Undergoing Percutaneous Coronary Intervention for Acute Myocardial Infarction: A Delphi Study
Authors Shan F, Xie N, Peng Y, Yang S, Zhou Y, Wang X, Zhou S, Huang P, Yang X
Received 29 January 2026
Accepted for publication 5 June 2026
Published 17 June 2026 Volume 2026:19 599696
DOI https://doi.org/10.2147/JMDH.S599696
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Fang Shan,1– 3 Nan Xie,1 Yanqiong Peng,1 Sen Yang,4 Yuanyuan Zhou,1 Xiao Wang,5 Shiheng Zhou,5 Ping Huang,6 Xinyu Yang6
1Nursing Department, Suining Central Hospital, Suining, 629000, People’s Republic of China; 2Qinggang Senior Care Center, the First Affiliated Hospital of Chongqing Medical University, Chongqing, 402761, People’s Republic of China; 3School of Nursing, Zunyi Medical University, Zunyi, 563003, People’s Republic of China; 4Medical Affairs Department, Suining Central Hospital, Suining, 629000, People’s Republic of China; 5Cardiology Department, Suining Central Hospital, Suining, 629000, People’s Republic of China; 6Medical Records Department, Suining Central Hospital, Suining, 629000, People’s Republic of China
Correspondence: Nan Xie, Nursing Department, Suining Central Hospital, Suining, 629000, People’s Republic of China, Email [email protected]
Purpose: To construct a cardiac catheterization laboratory nursing program for patients undergoing percutaneous coronary intervention (PCI) with acute myocardial infarction, providing nurses with scientific and practical behavioral guidance.
Methods: A literature review and intra-group discussions were employed to preliminarily construct a nursing program in the cardiac catheterization laboratory. The program content underwent two rounds of expert consultation involving 15 specialists to refine the proposal, ultimately forming the final version of the cardiac catheterization laboratory nursing program. The scientific and practical validity of the program is evaluated using the following metrics: expert positivity, expert authority coefficient, Kendall’s coefficient of concordance, and concentration of expert opinions.
Results: The final cardiac catheterization laboratory nursing program consists of three phases, encompassing a total of 30 items. The response rate for two rounds of expert consultation reached an impressive 100%. Expert authority coefficients were 0.983 and 0.980, respectively. The Kendall’s coefficient of concordance was 0.206 and 0.162 (P < 0.001), with high importance scores ranging from 4.13 to 5.00. Concurrently, acceptable coefficients of variation and full-score rates were achieved, indicating substantial expert consensus.
Conclusion: The cardiac catheterization laboratory nursing program for patients undergoing PCI with acute myocardial infarction is a scientific and reliable approach, demonstrating practical significance and specialized characteristics. It helps ensure patient safety and improves the quality of care in the cardiac intervention laboratory.
Keywords: nurse, cardiac catheterization laboratory, acute myocardial infarction, percutaneous coronary intervention, Delphi technique
Introduction
Acute myocardial infarction has emerged as one of the leading causes of cardiovascular disease mortality worldwide, with a substantial disease burden in China.1–3 According to statistics, the crude incidence of acute myocardial infarction among residents aged 18 and above in China is 87.6/100,000 (age-standardized rate is 93.9/100,000).4 This prevalence is expected to continue rising in line with China’s accelerated population aging. By 2030, the number of acute myocardial infarction patients in China is projected to reach 22.6 million.5 Currently, percutaneous coronary intervention (PCI) can open infarct-related arteries and significantly reduce patient mortality during hospitalization to 6.3%.6 It is an emergency treatment for ST-segment elevation myocardial infarction and high-risk non-ST-segment elevation myocardial infarction when clinically indicated. The cardiac catheterization laboratory is the core PCI site for acute myocardial infarction and represents about 45% of total hospitalization costs.7 Clearly, the surgical safety of the cardiac catheterization laboratory is directly linked to both the quality of medical care and the financial burden faced by patients undergoing PCI for acute myocardial infarction.
Despite the high success rate of PCI procedures, patients with acute myocardial infarction often encounter safety risks during catheterization laboratory interventions due to factors such as hemodynamic instability, rapid disease progression, and the psychological distress associated with near-death experiences.8,9 Particularly when performing direct PCI on patients with acute ST-segment elevation myocardial infarction, the pressing demands of door-to-balloon time combined with complex clinical conditions present a formidable challenge.10,11 Nurses manage patients with highly complex conditions in a short period of time, which may lead to insufficient care or nursing gaps.12 It significantly increases the risk of postoperative complications, including heart failure, malignant arrhythmias, respiratory failure, and even cardiogenic shock. As such, it is essential to develop a systematic nursing program for patients undergoing PCI for acute myocardial infarction in the cardiac catheterization laboratory. Such a program would help nurses mitigate the risk of oversights in nursing procedures and facilitate the early identification of potential complications.
In the context of nursing practice, there have been significant efforts to define and standardize interventional nursing care. The Interventional Nurses Council (INC) clarified the scope of interventional cardiac care, while the Australian College of Critical Care (ANCC) issued a consensus on interventional nursing practice, identifying its educational categories and seven areas of competence to ensure patient safety.13 This consensus provides interventional nurses with the general knowledge and skill requirements for performing PCI on patients with acute myocardial infarction. However, despite these efforts, no systematic nursing program has been developed to address the specific pathophysiological and psychological needs of acute myocardial infarction patients undergoing PCI. In China, specialized nursing programs for this purpose remain limited. The Southern China Cardiovascular Nursing Alliance has issued consensus guidelines for atrial fibrillation care in cardiac catheterization laboratories, which emphasize the importance of standardized programs to ensure patient safety.14 Nevertheless, this guidance is difficult to apply in assisting clinical nurses with cardiac catheterization laboratory care for patients undergoing PCI for acute myocardial infarction, owing to differences in the mechanisms of cardiovascular disease, management priorities, and surgical approaches. Currently, the management of cardiac catheterization laboratories for patients undergoing PCI for acute myocardial infarction is largely clinician-focused, with nursing guidance remaining generalized and lacking specific, actionable directives for nursing practice.15,16 This study aims to bridge this gap by using the Delphi method to formulate a specialized nursing program through literature review and group discussion. This program will guide cardiac catheterization laboratory nursing practice during PCI for acute myocardial infarction, thereby enhancing patient safety and nursing quality.
Methods
The Delphi method is widely used in nursing research to develop programs and assessment tools.17 This technique uses structured questionnaires to synthesize expert judgments on complex and uncertain issues.18 It is characterized by anonymity, multiple rounds of controlled iterative feedback, and quantitative statistical analysis. The Delphi method relies exclusively on questionnaire-based communication, ensuring complete anonymity among experts and minimizing the influence of authority. It also enables multiple rounds of feedback to reach expert consensus. Our study developed a draft nursing program through a literature review and group discussions, which was then revised using the Delphi method over two rounds to reach consensus. This methodology enhances the reliability and content validity of clinical practice programs.
Establishment of the Research Team
The research team comprised 12 members, including 3 nursing management specialists, 4 cardiac nursing specialists, 3 cardiology medical specialists, and 2 graduate students. Team members were responsible for drafting preliminary documents, developing expert consultation questionnaires, recruiting and contacting experts, compiling and analyzing expert feedback, and revising materials accordingly.
Preliminary Draft Based on Literature Review
In this study, we used a literature review and intra-group discussions to construct a preliminary draft of the program. The research team members conducted a comprehensive search of various databases, including PubMed, Web of Science, ScienceDirect, Embase, CINAHL, BMJ Full Text Database, China Biomedical Database, China National Knowledge Infrastructure (CNKI), Wanfang, and VIP Database. We also searched guideline websites and professional association sites such as the American Heart Association, American College of Cardiology, European Society of Cardiology, and the Cardiac Society of Australia and New Zealand, as well as Medline. English search terms: “acute myocardia* infarction”, “care path*”, “clinical nursing path*”, “critical path*”, “care map”, AMI, PCI, etc. The same or adapted search terms were used for the Chinese databases (e.g., CNKI, Wanfang, VIP). A combination of subject headings and free-text terms was employed to retrieve literature published between January 2012 and May 2022. Based on literature review and group discussions, a preliminary nursing program was developed for patients undergoing PCI for acute myocardial infarction in the cardiac catheterization laboratory.
Developing an Expert Consultation Questionnaire
The draft nursing program was designed as the first-round Delphi consultation questionnaire. It comprised three sections: the consultation letter introduction, nursing program content and scoring, and expert information survey. (1) Consultation letter introduction: Explained the purpose of the consultation, research background, main content, questionnaire return deadline, submission method, and contact personnel. (2) Nursing program content and scoring: The nursing program was comprised of three sections: preoperative preparation, intraoperative cooperation and monitoring, and postoperative management. A five-point Likert scale was used to assess the importance of each item. Each item was followed by a comment column for the experts’ suggestions on modifying, adding, or deleting items. (3) Expert Information Survey: This primarily gathered basic expert details, self-assessed familiarity with questionnaire content, and the perceived influence of information sources on judgment. The Delphi questionnaire underwent readability testing by two experienced nursing experts within the research team.
Selection of Consulting Experts
The study employed purposive sampling to recruit clinical nursing experts, medical experts, and management experts specializing in cardiovascular interventional procedures. Expert inclusion criteria were: (1) at least 10 years of experience working in cardiovascular medicine or cardiac catheterization laboratories; (2) holding an associate senior or higher professional title; (3) holding at least a bachelor’s degree or higher; (4) demonstrating sufficient interest in the research topic and voluntarily agreeing to participate. As consensus on the optimal sample size for experts remains unresolved, prior literature suggests that 5–20 experts may suffice.19 This study ultimately selected 15 experts for the survey. In the catheterization laboratory, patients with acute myocardial infarction undergoing PCI were mostly under local anesthesia, and care was co-managed by the interventional cardiologist and the catheterization laboratory nurse. The cardiologists held institutional privileges for prescribing anesthetic agents, and the nurses had completed dedicated training in moderate-to-deep sedation. Through long-term catheterization laboratory practice, the expert panelists had developed substantial expertise in perioperative sedation, analgesia, and respiratory management. Additionally, the consultation questionnaire was completed by the same group of experts. They were informed during recruitment that completing the first-round survey would signify their willingness to participate in the second round of the Delphi study.
Expert Consultation and Program Development
The study employed a two-round expert consultation process, distributing questionnaires via Email or WeChat according to participants’ communication preferences. In the first round, experts provided feedback on a preliminary questionnaire, which was then reviewed, synthesized, and analyzed by the research team. The revised version formed the basis for the second-round questionnaire. In the second round, participants could view the first-round findings, including the consensus level for each item and anonymous suggestions from other experts. Experts reconsidered the revised questionnaire using the same methodology to reach a negotiated consensus. The two Delphi rounds were spaced two weeks apart, with each round requiring responses within one week. Researchers sent reminder emails two days before the response deadline. Experts who did not respond to the questionnaire or emails for over one week were considered unwilling to continue participating and were not contacted further. Throughout the process, researchers maintained ongoing communication with experts while ensuring the privacy and confidentiality of all participants. Following the completion of both rounds of expert consultation, consensus was reached on the care program for PCI patients in the cardiac catheterization laboratory. Two items were subsequently refined against the latest evidence to finalize the program.
Statistical Methods
Data entry and statistical analysis were conducted using Excel and SPSS 29.0, with a significance level of α=0.05. (1) General expert information: Quantitative data were presented as mean and standard deviation, while categorical data were expressed as frequency and percentage; (2) Expert engagement level was indicated by the questionnaire response rate. (3) Expert authority was represented by the authority coefficient (Cr), which was calculated as the arithmetic mean of the judgment coefficient (Ca) and the familiarity coefficient (Cs).20 (4) Expert consensus was assessed using Kendall’s coefficient of concordance and the coefficient of variation (CV). Kendall’s W ranges from 0 to 1; a statistically significant value indicates that the experts have reached consensus. The CV is calculated as CV = standard deviation / mean; a lower CV indicates greater expert consensus (CV ≤ 0.25 is acceptable).21 (5) The concentration of expert opinions was represented by the mean, standard deviation, and full-score rate of each item’s importance rating. Generally, the mean importance score should not be below 3.5 points, and the full-score rate should not be less than 20%.22
Ethics Statement
This study was approved by the Medical Research Ethics Committee of Suining Central Hospital (No. LLSNCH20210035) and conducted in accordance with the principles of the Declaration of Helsinki. The research and participants’ rights were explained to experts via telephone or email. Completion of the survey constituted informed consent.
Results
Expert Demographics
A total of 15 specialists from seven tertiary hospitals completed two rounds of expert consultation. Their average age was (42.93 ± 4.93) years, with an average professional experience of (20 ± 6.82) years. They specialized in cardiac nursing, nursing management, cardiology, and healthcare management, all holding associate senior or higher professional titles. The demographic characteristics and professional details of participants are presented in Table 1.
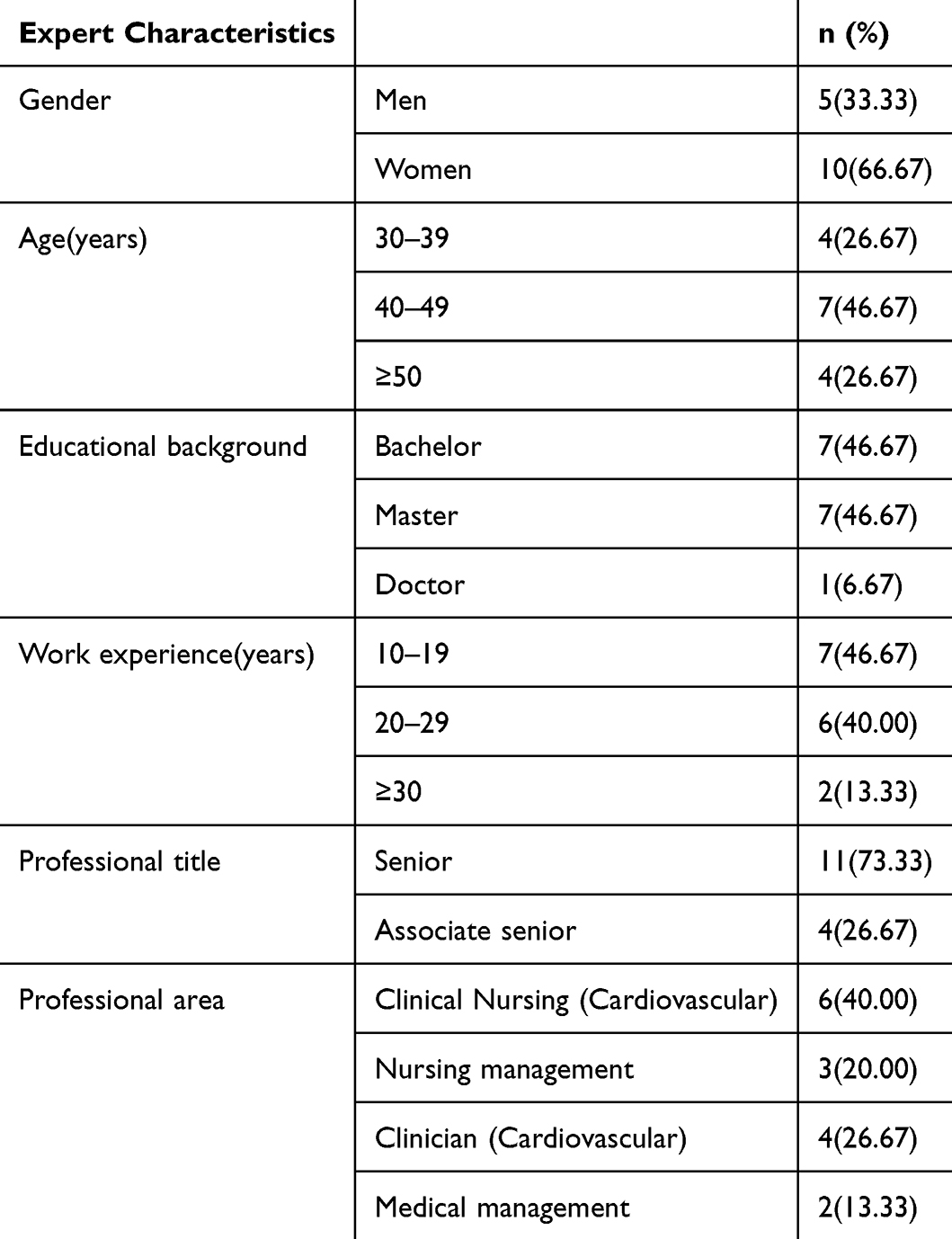 |
Table 1 Sociodemographic Characteristics of the Expert Panel |
Degree of Enthusiasm and Authority of Experts
Each round of expert consultation involved the distribution of 15 questionnaires, with a 100% response rate achieved in both rounds. Notably, five experts contributed revision suggestions, and three experts engaged in telephone discussions with members of the research team. It indicates a high level of engagement among experts with the study. The expert authority coefficients (Cr) were 0.983 and 0.980 in the first and second rounds, respectively (with Cs = 0.973/0.987 and Ca = 0.993/0.973). These scores correspond to a high degree of expert authority on the subject.
Degree of Coordination of Expert Opinions
The degree of coordination between the two rounds of expert consultation was expressed using Kendall’s coefficient of concordance, yielding values of 0.206 and 0.162, respectively. The observed difference between the two sets was statistically significant (P < 0.001), as shown in Table 2. This indicates a statistically significant concordance among experts.
 |
Table 2 Coordination Factors of Expert Consultations |
Expert Opinion Concentration and Sorting
In the first round of expert consultation, the mean importance scores for each item ranged from 4.13 to 5.00, with coefficient of variation (CV) values ranging from 0.00 to 0.30 and full-mark rates ranging from 53.33% to 100%. Detailed results are shown in Table 3. Based on the scoring outcomes and feedback from this round of experts, items were revised to remove non-essential measures, amend content, and consolidate duplicated entries. In this consultation questionnaire, the item “Assist physicians in putting on and taking off radiation protection lead aprons and surgical isolation gowns” received an importance rating of 4.13, but its CV exceeded 0.25. Items with a coefficient of variation exceeding 0.25 are typically considered for deletion. Following an in-depth discussion by the research team, this item was deleted as it pertains to the personal protection of the operating surgeon and does not require additional assistance from nurses. Meanwhile, based on expert feedback, the content “Assist the physician with skin disinfection and draping” was removed. Additionally, in accordance with expert recommendations, the items “For patients undergoing radial artery puncture, assist the physician in removing the surgical sheath” and “Assist the doctor in applying pressure to the puncture site to stop bleeding” were revised to “Apply pressure to the puncture site to stop bleeding, then observe for any signs of bleeding”. We also accepted the experts’ suggestion to merge the duplicate entries “Perform a surgical inventory and conduct patient safety verification before surgery” and “Recheck the surgical instruments”. However, after careful deliberation, the research team did not adopt two further expert suggestions. One suggestion to add “check or establish left-hand venous access” duplicated the existing item “check venous access”, and clinical practice may preclude left-hand access due to individual patient conditions. The other was to add “Allen test”, which was not adopted as performing this test in the cardiac catheterization laboratory could prolong the surgical time for acute myocardial infarction patients. Consequently, the revised proposal was formulated as a consultation questionnaire and resent to 15 experts in the second round.
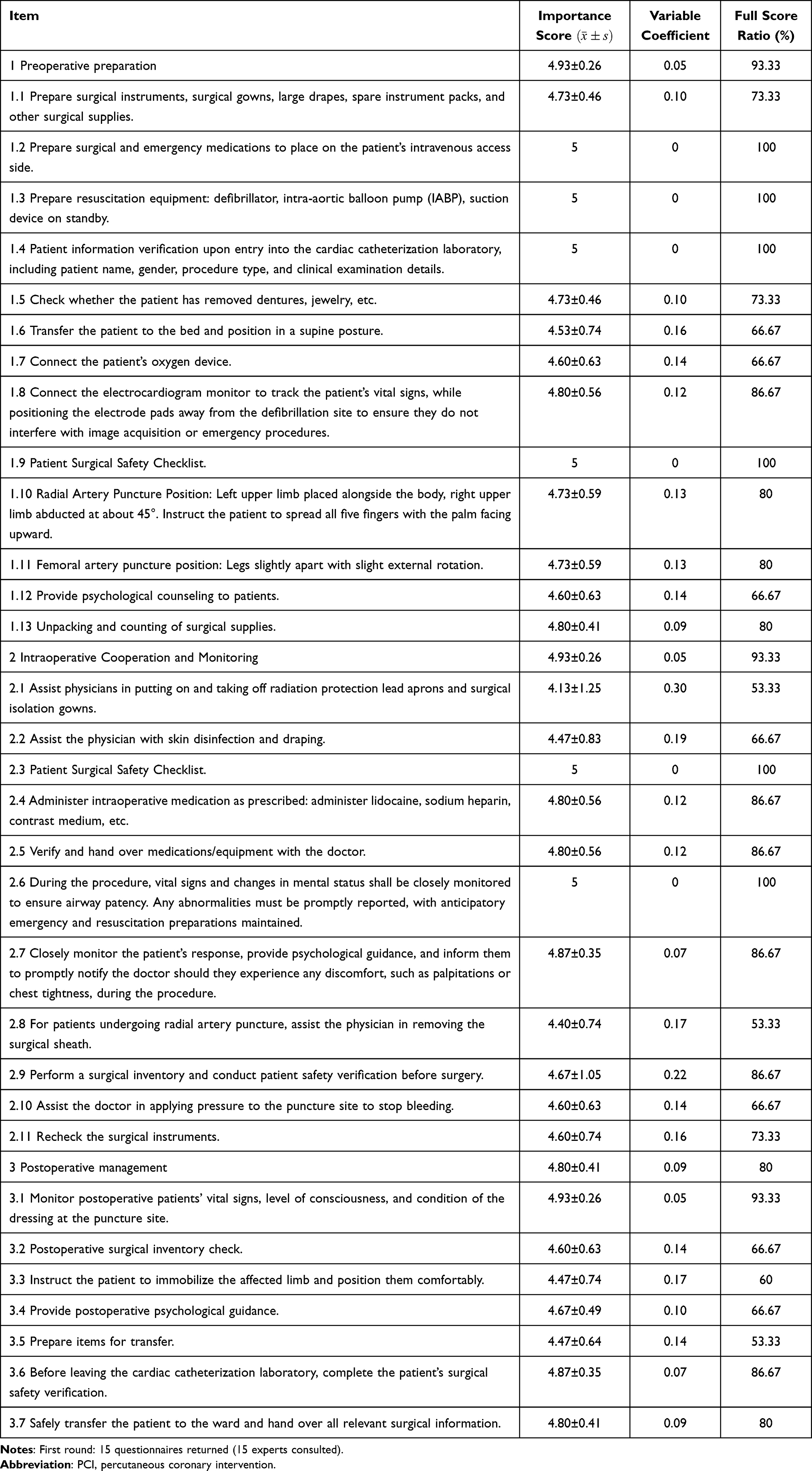 |
Table 3 First Delphi Round: Nursing Program for Acute Myocardial Infarction Patients Undergoing PCI |
In the second round of expert consultation, the mean importance scores for each item ranged from 4.53 to 5.00, with CV values ranging from 0.00 to 0.16 and full-mark rates ranging from 66.67% to 100%. Detailed results are shown in Table 4. Compared to the first round, expert opinions in this round were more concentrated, with no items or opinions meeting the deletion criteria, indicating the formation of stable and consistent content. Language descriptions were revised solely based on expert recommendations to emphasize nursing priorities or refine phrasing. The phrase “immobilize affected limb” was refined to “maintain the joint in a neutral extended position and immobilize the puncture site”; “Apply pressure to the puncture site to stop bleeding, then observe for any signs of bleeding” was amended to “Apply pressure to the puncture site for hemostasis, and observe for any bleeding or limb swelling”. Streamlined language descriptions include replacing “Perform a surgical inventory and conduct patient safety verification before surgery” with “Count surgical instruments”. Subsequently, based on feedback and supporting evidence, two items were further specified beyond the original Delphi consensus: the item “administer intraoperative medication orders” was refined to explicitly list “analgesics and vasoactive agents”; and the item “connect patient to oxygen delivery device” was refined to explicitly list “bag-valve-mask resuscitator, tracheal intubation kit, and suction apparatus”. The finalized catheterization laboratory nursing program for patients undergoing PCI for acute myocardial infarction comprises 30 items structured across three core domains: 13 for preoperative preparation, 7 for intraoperative coordination and monitoring, and 7 for postoperative management (Box 1).
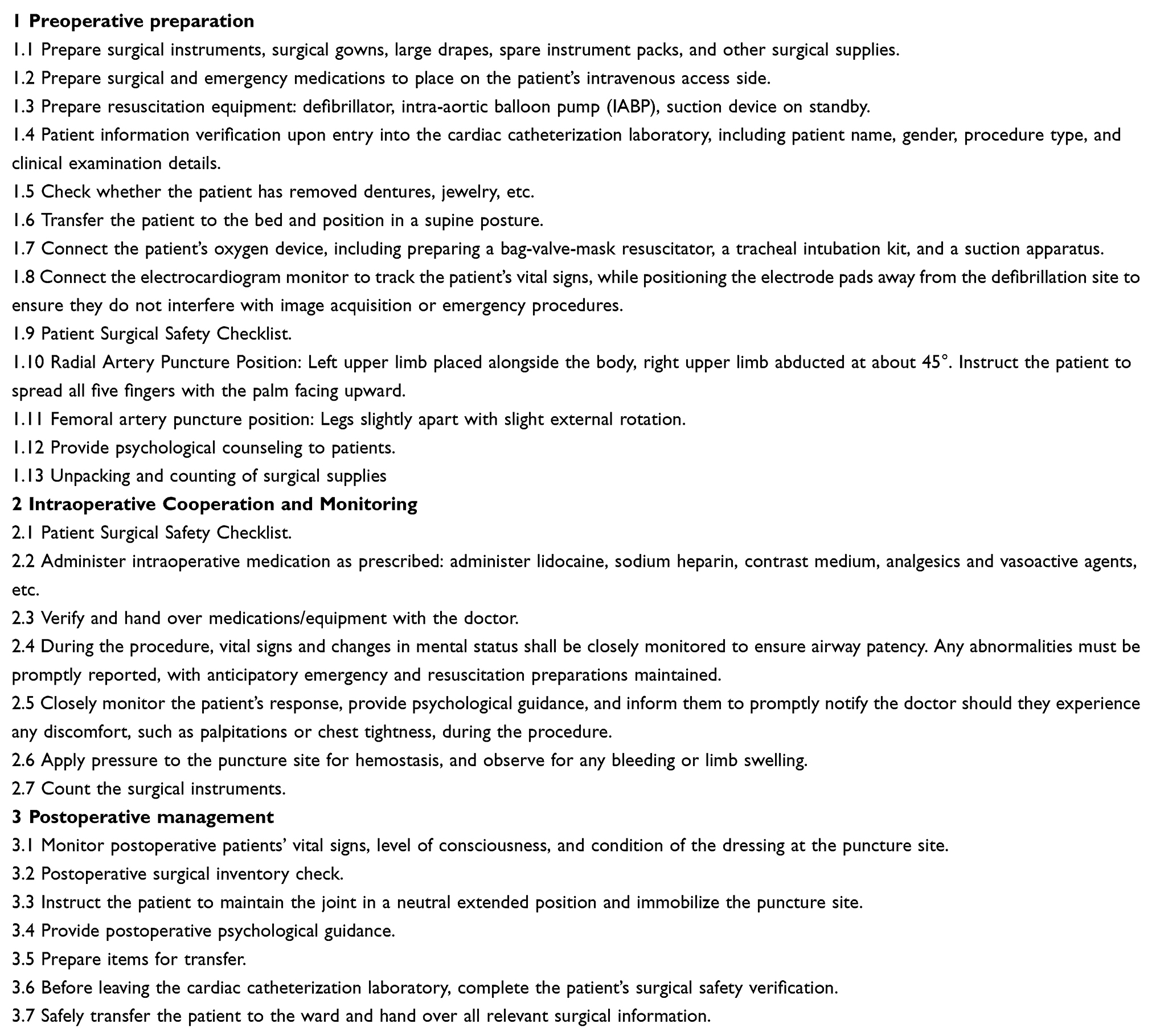 |
Box 1 Cardiac Catheterization Laboratory Nursing Program for Patients Undergoing PCI for Acute Myocardial Infarction |
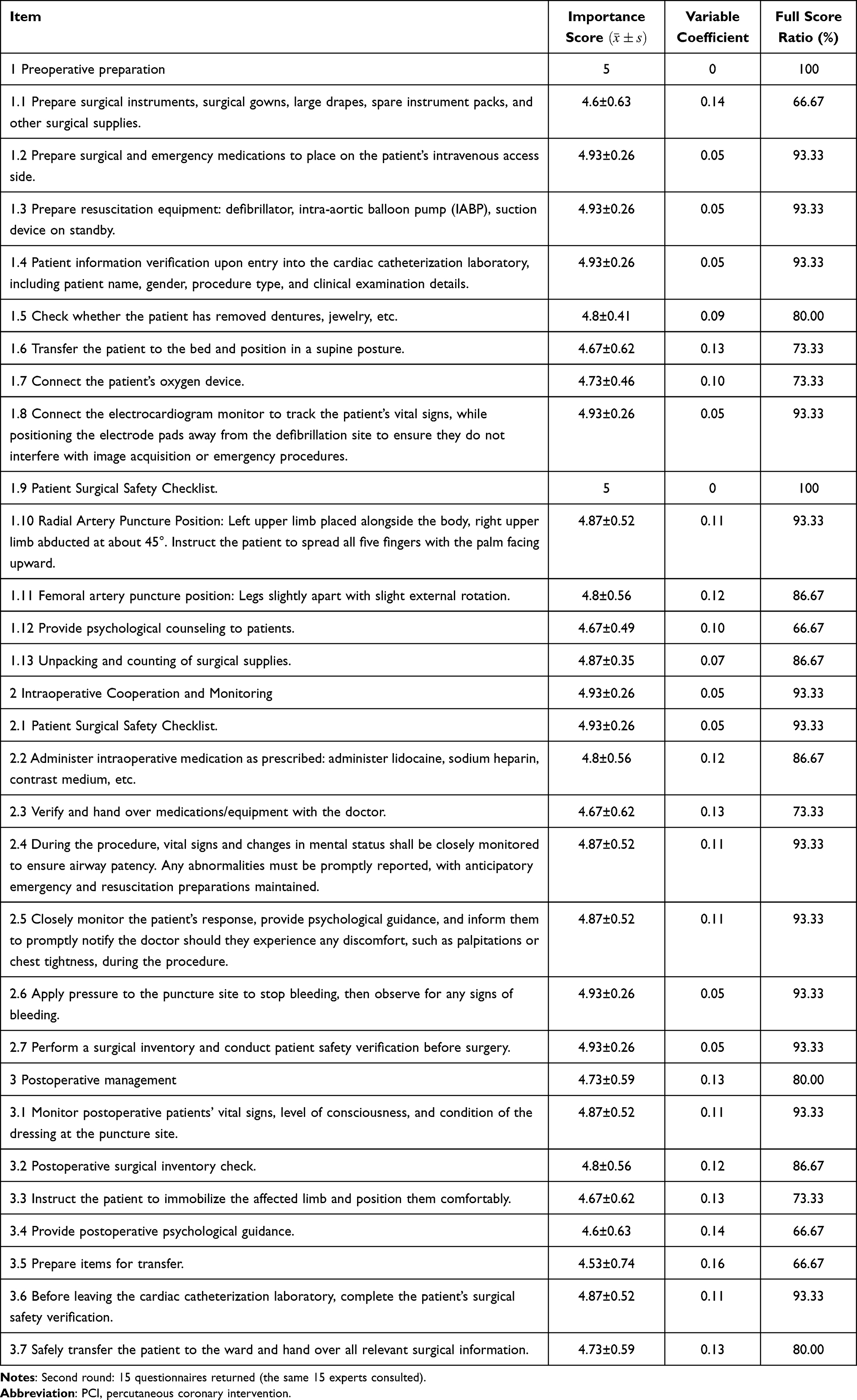 |
Table 4 Second Delphi Round: Nursing Program for Acute Myocardial Infarction Patients Undergoing PCI |
Discussion
In this study, a research team was established to develop a cardiac catheterization laboratory nursing program for patients with acute myocardial infarction undergoing PCI, based on a literature review and expert consultation, thereby ensuring the scientific rigor of the program. The selection of representative, proactive, and authoritative experts is key to the success of the expert consultation approach.23 A total of 15 experts were chosen from seven hospitals across different regions of China, with an average of 20 or more years of professional experience in their respective fields. These experts possessed extensive theoretical knowledge and clinical experience, ensuring high representativeness and minimizing potential evaluation bias. The reliability of the expert consultation results was evaluated using indicators such as expert enthusiasm, authority coefficient, Kendall’s W value, and degree of consensus. The effective questionnaire return rate for both rounds of expert consultation reached 100%, indicating considerable interest among experts in the content of the nursing programs. Previous studies indicate that an expert authority coefficient exceeding 0.7 is considered reliable and capable of achieving a certain degree of predictive accuracy.24,25 In this study, the authority coefficients for both rounds of expert consultation were exceptionally high, at 0.983 and 0.980, respectively. These values demonstrate the experts’ strong authority and reliability in their evaluations. Both rounds of expert consultation yielded statistically significant Kendall’s W values (P<0.001), with the CV for retained items remaining below 0.25. Furthermore, the mean importance scores and full-score rates for the entries showed varying degrees of increase during the second round of consultation. These findings indicate a high degree of consistency among expert opinions regarding the nursing program content, and the expert consultation process demonstrated satisfactory scientific validity and reliability.
PCI is an effective and life-saving invasive treatment for patients with acute myocardial infarction.26 Despite its success in alleviating the immediate threat of ischemia, patients undergoing PCI remain at risk of intraoperative complications such as malignant arrhythmias, hemorrhage, and hypotension during the procedure.27,28 The safety of intraoperative care greatly affects the patient’s physical recovery in the ward and subsequent cardiac rehabilitation programs. In China, however, there is currently a lack of standardized nursing programs for PCI in the cardiac catheterization laboratory, a gap that could potentially compromise patient safety and nursing care quality. During PCI procedures in the cardiac catheterization room, nurses typically follow a routine interventional checklist to guide their actions. It should not be overlooked that patients with acute myocardial infarction continue to experience myocardial ischemia throughout the procedure. Any oversight in nursing procedures may prolong surgical duration and result in failed reperfusion during the procedure, potentially leading to hemodynamic instability or even mortality. Given the high-pressure nature of the catheterization laboratory environment, nurses often rely on personal experience and individual training to manage these critical situations. This study formulated a standardized nursing program for such patients in the cardiac catheterization laboratory. Upon patient admission to the cardiac catheterization laboratory, the program addresses three key components: preoperative preparation, intraoperative coordination and monitoring, and postoperative management. For each of these domains, specific and detailed nursing guidelines have been established. The program transforms decentralized, experience-based nursing practices into a standardized, reviewable, and predictable protocol, which is essential for ensuring medical safety and quality. Our research program emphasizes core elements such as surgical safety verification at each stage, prepositioning of resuscitation equipment, and continuous vital sign monitoring. It aims to standardize the procedures of cardiac catheterization laboratory nurses performing PCI on patients with acute myocardial infarction, thereby helping to prevent nursing omissions and facilitating early detection of clinical changes. It complies with the guidelines’ requirements for rigorous monitoring and safety programs, elevating the nurse’s role from a supporting operator to an active risk manager and guardian of patient safety.29 Furthermore, with the rapid development and emergence of artificial intelligence and surgical robotics, this nursing program may also serve as preliminary behavioral guidance in future protocols, offering not only clinical utility but also potential for broader application.
The cardiac catheterization laboratory nursing program for patients undergoing PCI with acute myocardial infarction is formulated by integrating clinical characteristics based on conventional interventional procedure nursing content. Its content is more practical in nature. The content of the nursing program we studied included three aspects. In the preoperative preparation process, Nicholson et al advocate a preoperative preparation checklist for the cardiac catheterization laboratory, based on the globally recognized surgical checklist, a view consistent with the present study.30 In our study, preoperative preparations emphasized the routine provision of resuscitation drugs and circulatory support equipment, such as defibrillators and aortic balloon pumps. This practice directly responds to guideline recommendations to minimize the response time to resuscitation in the event of hemodynamic collapse during surgery in patients with acute myocardial infarction.31 It should be noted that the percutaneous ventricular assist device Impella is currently recommended as a Class IIa intervention for ST-segment elevation myocardial infarction complicated by severe cardiogenic shock.32 Given the varying availability across countries, institutions where resources permit may prioritize its use over the intra-aortic balloon pump.33 Our nursing program has limited effectiveness in extremely high-risk patients with acute myocardial infarction who have impending hemodynamic and respiratory collapse. Such patients require not only escalated circulatory support with extracorporeal membrane oxygenation but also a comprehensive airway rescue system, including video laryngoscopy, supraglottic airways, and emergency front-of-neck access.34,35 Building on our program, this requires the mobilization of a multidisciplinary team including the ICU team, perfusionists, and the operating theatre anesthesia team. In addition to focusing on the preparation of equipment, the program incorporates rigorously enforced patient identification verification and surgical safety checklists, representing the specific application of the World Health Organisation’s Surgical Safety Checklist within the catheterization laboratory setting. This system has been demonstrated to significantly reduce the incidence of serious adverse events, including wrong-site surgery.36 Furthermore, this program combines the surgical characteristics of patients with acute myocardial infarction with clear behavioral guidance on positioning for radial and femoral artery puncture, helping to standardize nurses’ operative behavior. The program further integrates physiological preparation with psychological guidance, mandating preoperative psychological counselling. This approach aligns with the contemporary biopsychosocial medical model. It can reduce the emotional stress response in patients, playing a positive role in stabilizing vital signs and facilitating postoperative recovery.37
In the context of intraoperative cooperation and monitoring, the research program not only encompasses assisting surgeons with basic surgical support but also emphasises dynamic safety management focused on nurses’ continuous physiological monitoring, medication preparedness in the cardiac catheterization laboratory, and proactive patient communication. Our nursing program requires close monitoring of patients’ vital signs. Basic parameters such as heart rate, blood pressure, electrocardiogram, respiratory rate, and pulse oximetry can be continuously monitored via an electrocardiogram monitor, and mainstream monitors also support optional end-tidal carbon dioxide modules. The latter is the most reliable method for confirming endotracheal tube placement and monitoring the adequacy of ventilation.38 In recent years, emerging intraoperative monitoring techniques such as near-infrared spectroscopy (cerebral oxygen monitoring) and the nociception level index have mainly been used in general anesthesia settings in the operating theatre.39,40 However, their routine adoption in the cardiac catheterization laboratory remains to be validated. Regarding medication in the cardiac catheterization laboratory, our research suggests that sedatives (such as lidocaine), analgesics (such as morphine), and vasoactive agents (including inotropes such as dobutamine, vasopressors such as noradrenaline, and inodilators such as milrinone) must be readily available at all times. Staff in the cardiac catheterization laboratory, including nurses and surgeons, should be fully aware of the location and indications for these medications to ensure that initial emergency management can be carried out in the event of abrupt hemodynamic changes or signs of cardiogenic shock. Our standardized nursing program alone is insufficient to fulfil the comprehensive treatment requirements of patients with acute myocardial infarction undergoing PCI who develop cardiogenic shock with respiratory failure, or those with multiple critical comorbidities leading to high procedural complexity and profound hemodynamic instability. We strongly recommend that the cardiac catheterization laboratory team engage anesthesiology, ICU, and other multidisciplinary teams early for comprehensive airway and anesthesia management. Regular multidisciplinary simulation training is essential to enhance team coordination. Notably, our intraoperative program also emphasizes that nurses should provide psychological support and encourage patients to promptly report symptoms such as chest tightness and palpitations. This operational guidance has both clinical and humanistic value. On the one hand, symptom reporting by patients with acute myocardial infarction provides crucial early warning signs of intraoperative complications. On the other hand, sustained therapeutic communication effectively alleviates patients’ fear and anxiety within specialized treatment settings, enhancing their cooperation and surgical experience.41 Our research findings indicate that nurses in the cardiac catheterization laboratory need to monitor not only patients’ vital signs and puncture sites but also their subjective experiences during the procedure. This aspect is rarely emphasized, as most studies focus on postoperative psychological counseling for negative emotions or symptoms.42 Future research may explore the use of virtual reality technology to relieve negative emotions during surgery in critically ill patients with diseases similar to acute myocardial infarction.
Our nursing program focuses on early prevention of complications and safe transport management during the postoperative phase to ensure continuity of nursing care in the cardiac catheterization laboratory. During the postoperative phase, cardiac catheterization laboratory nurses prioritize systematic assessment of vital signs, level of consciousness, the affected limb, and puncture sites. This approach mitigates the risk of bleeding and vascular complications following PCI in patients with acute myocardial infarction. This is consistent with the guideline’s recommendation that routine postoperative monitoring of puncture sites and vital signs constitutes a core measure for the early detection of hemorrhagic complications.29 Our nursing program stipulates that nurses complete the surgical safety checklist before leaving the catheterization laboratory, with patient handover as a mandatory step during ward transfer. This handover must encompass intraoperative hemodynamic parameters, administered sedatives and analgesics, and any intraoperative complications to ensure continuity of care. In addition, compression hemostasis is generally recognized as an effective evidence-based method for preventing bleeding after radial artery puncture.43 On this basis, the nursing program explicitly outlines health guidance for joint immobilization at the puncture site, further underscoring the responsibility of cardiac catheterization laboratory nurses to ensure patient safety in the postoperative period.
Strengths and Limitations
A major strength of this study is the initial standardization of PCI nursing procedures for patients with acute myocardial infarction in the cardiac catheterization laboratory. To our knowledge, existing research has largely focused on nursing programs within emergency departments,44 inpatient wards,45 and post-discharge settings,46 while relatively little attention has been paid to nursing practices specific to the catheterization laboratory. Our nursing program adheres to procedural guidelines for nurses performing PCI in patients with acute myocardial infarction in the catheterization laboratory. It not only prioritizes patient safety during procedures but also emphasizes compassionate care throughout the surgical process, thereby enhancing the overall quality of nursing services in this critical care setting. However, the study has several limitations. One notable limitation was the inclusion of only 15 experts in the Delphi survey, a sample size constrained by time and funding considerations. Although this number of experts is feasible, and the panel members demonstrated authority, reliability, and representativeness, they may not fully represent the broader nursing profession. Furthermore, the invited experts primarily hailed from a specific region within China, potentially introducing regional bias. The Delphi survey findings warrant cautious interpretation, as their generalizability is limited. Following the initial Delphi consensus, two items in the final program were refined based on feedback and supporting evidence to specify a bag-valve-mask resuscitator, tracheal intubation kit, and suction apparatus, and to include analgesics and vasoactive drugs. These refinements were not evaluated by the Delphi panel; they therefore warrant further assessment before implementation. Given these constraints, future implementation of this approach requires further refinement and tailoring to specific national and cultural contexts.
Conclusion
Catheterization laboratory nursing for patients undergoing PCI for acute myocardial infarction is a critical topic, requiring specialized and meticulously designed care programs to ensure patient safety and the quality of interventional care. Our study has preliminarily established key procedures for a standardized care program for PCI in the catheterization laboratory for acute myocardial infarction patients. This program not only serves as a guide for delivering high-quality surgical care in clinical programs but also provides a foundation for comparing outcomes in future research. By using the Delphi method, we found that integrating the perspectives of professionals, medical specialists, and administrators can form a patient-centered care program suitable for the hospital environment. Future studies will conduct a pilot clinical study to evaluate patient outcomes and care quality, allowing for iterative revisions based on clinical feedback. The refined program will then be reviewed by an independent panel of experts who did not participate in the Delphi process to provide external validation and facilitate further optimization. More importantly, given the rapid development and proliferation of intelligent robots, this program can provide an initial operational framework.
Acknowledgments
The authors would like to express their sincere gratitude to all participants from all locations who participated in the Delphi study.
Funding
This study was supported by the Sichuan Hospital Management and Development Research Center, Southwest Medical University (SCYG2022-08) and the scientific research project of Suining Central Hospital (2022yg103).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: update From the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–15. doi:10.1016/j.jacc.2020.11.010
2. Roth GA, Mensah GA, Fuster V. The Global Burden of Cardiovascular Diseases and Risks: a Compass for Global Action. J Am Coll Cardiol. 2020;76(25):2980–2981. doi:10.1016/j.jacc.2020.11.021
3. Saito Y, Oyama K, Tsujita K, Yasuda S, Kobayashi Y. Treatment strategies of acute myocardial infarction: updates on revascularization, pharmacological therapy, and beyond. J Cardiol. 2023;81(2):168–178. doi:10.1016/j.jjcc.2022.07.003
4. Liu MB, He XY, Yang XH, Wang ZW. Key points interpretation of the 2024 China cardiovascular health and disease report. J Cardiovasc Pulm Dis. 2025;44(9):899–917. doi:10.3969/j.issn.1007-5062.2025.09.001
5. Wang S, Marquez P, Langenbrunner J, Niessen L, Suhrcke M, Song F. Toward a Healthy and Harmonious Life in China: stemming the Rising Tide of Non-Communicable Diseases. Human Development Unit, East Asia and Pacific Region. 2011. Available from: https://documents.worldbank.org/en/publication/documents-reports/documentdetail/618431468012000892/toward-a-healthy-and-harmonious-life-in-china-stemming-the-rising-tide-of-non-communicable-diseases.
6. Kruk M, Przyłuski J, Kalińczuk Ł, et al. ANIN Myocardial Infarction Registry Group. Association of non-specific inflammatory activation with early mortality in patients with ST-elevation acute coronary syndrome treated with primary angioplasty. Circ J. 2008;72(2):205–211. doi:10.1253/circj.72.205
7. Martin SS, Aday AW, Allen NB, et al. 2025 Heart Disease and Stroke Statistics: a Report of US and Global Data From the American Heart Association. Circulation. 2025;151(8):e41–e660. doi:10.1161/CIR.0000000000001303
8. Basir MB, Lemor A, Gorgis S, et al. Early Utilization of Mechanical Circulatory Support in Acute Myocardial Infarction Complicated by Cardiogenic Shock: the National Cardiogenic Shock Initiative. J Am Heart Assoc. 2023;12(23):e031401. doi:10.1161/JAHA.123.031401
9. Schmitz T, Harmel E, Raake P, et al. Association Between Acute Myocardial Infarction Symptoms and Short- and Long-term Mortality After the Event. Can J Cardiol. 2024;40(7):1355–1366. doi:10.1016/j.cjca.2024.01.019
10. Hassan MO, Ahmed SA, Hassan MS, Köprülü D. Door-to-Balloon Time and Mortality Among Patients Undergoing Primary PCI, Challenges and Experience from Somalia’s Largest PCI Center. Int J Gen Med. 2024;17:237–244. doi:10.2147/IJGM.S448750
11. Nishio R, Ogita M, Suwa S, et al. Shorter door-to-balloon time, better long-term clinical outcomes in ST-segment elevation myocardial infarction patients: j-MINUET substudy. J Cardiol. 2023;81(6):564–570. doi:10.1016/j.jjcc.2023.01.008
12. El-Sayed AAI, Asal MGR, Shaheen RS, Abdelaliem SMF. Job embeddedness and missed nursing care at the operating theatres: the mediating role of polychronicity. BMC Nurs. 2023;22(1):458. doi:10.1186/s12912-023-01628-8
13. White K, Macfarlane H, Hoffmann B, et al. Consensus Statement of Standards for Interventional Cardiovascular Nursing Practice. Heart Lung Circ. 2018;27(5):535–551. doi:10.1016/j.hlc.2017.10.022
14. Huang SP, Gong B, Shen TM, et al. Guangdong Nurses Association Cardiovascular Disease Nursing Branch, Southern Cardiovascular Nursing Alliance. Expert Consensus on Perioperative Nursing Care of Patients With Atrial Fibrillation Undergoing Interventional Surgery. Chin J Inter Rad. 2024;12(1):1–9. doi:10.3877/cma.j.issn.2095-5782.2024.01.001
15. Schlotter F, Huber K, Hassager C, et al. Ventricular septal defect complicating acute myocardial infarction: diagnosis and management. A Clinical Consensus Statement of the Association for Acute CardioVascular Care (ACVC) of the ESC, the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC and the ESC Working Group on Cardiovascular Surgery. Eur Heart J. 2024;45(28):2478–2492. doi:10.1093/eurheartj/ehae363
16. Tamis-Holland JE, Abbott JD, Al-Azizi K, et al. SCAI Expert Consensus Statement on the Management of Patients With STEMI Referred for Primary PCI. J Soc Cardiovasc Angiogr Interv. 2024;3(11):102294. doi:10.1016/j.jscai.2024.102294
17. Wilkes L. Using the Delphi technique in nursing research. Nurs Stand. 2015;29(39):43–49. doi:10.7748/ns.29.39.43.e8804
18. Hasson F, Keeney S, McKenna H. Revisiting the Delphi technique - Research thinking and practice: a discussion paper. Int J Nurs Stud. 2025;168:105119. doi:10.1016/j.ijnurstu.2025.105119
19. Grime MM, Wright G. Delphi Method. In: Wiley StatsRef: Statistics Reference Online. Balakrishnan N, Colton T, Everitt B, Piegorsch W, Ruggeri F, Teugels JL editors. John Wiley & Sons Inc; 2016:1–6. doi:10.1002/9781118445112.stat07879.
20. Li Z, He W, Tian D, Sun Y, Yang Q, Cao L. Developing an ultrasound-guided enteral nutrition protocol for critically ill patients based on the Delphi method. Nurs Crit Care. 2025;30(3):e70023. doi:10.1111/nicc.70023
21. Niederberger M, Spranger J. Delphi Technique in Health Sciences: a Map. Front Public Health. 2020;8:457. doi:10.3389/fpubh.2020.00457
22. Banerjee A, Splieth C, Breschi L, et al. When to intervene in the caries process? A Delphi consensus statement. Br Dent J. 2020;229(7):474–482. doi:10.1038/s41415-020-2220-4
23. Humphrey-Murto S, Wood TJ, Gonsalves C, Mascioli K, Varpio L. The Delphi Method. Acad Med. 2020;95(1):168. doi:10.1097/ACM.0000000000002887
24. Banno M, Tsujimoto Y, Kataoka Y. The majority of reporting guidelines are not developed with the Delphi method: a systematic review of reporting guidelines. J Clin Epidemiol. 2020;124:50–57. doi:10.1016/j.jclinepi.2020.04.010
25. Varndell W, Fry M, Elliott D. Applying real-time Delphi methods: development of a pain management survey in emergency nursing. BMC Nurs. 2021;20(1):149. doi:10.1186/s12912-021-00661-9
26. Ozaki Y, Hara H, Onuma Y, et al. CVIT expert consensus document on primary percutaneous coronary intervention (PCI) for acute myocardial infarction (AMI) update 2022. Cardiovasc Interv Ther. 2022;37(1):1–34. doi:10.1007/s12928-021-00829-9
27. Schmidbauer ML, Rizas KD, Tiedt S, Dimitriadis K. Low rate of intracerebral hemorrhage after cardiac catheterization in patients with acute ischemic stroke in a large case series. Clin Neurol Neurosurg. 2020;198:106159. doi:10.1016/j.clineuro.2020.106159
28. Frampton J, Ortengren AR, Zeitler EP. Arrhythmias After Acute Myocardial Infarction. Yale J Biol Med. 2023;96(1):83–94. doi:10.59249/LSWK8578
29. ESC Scientific Document Group, Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393.
30. Nicholson P, Kuhn L, Manias E, Sloman M. The design and evaluation of a pre-procedure checklist specific to the cardiac catheterisation laboratory. Aust Crit Care. 2021;34(4):350–357. doi:10.1016/j.aucc.2020.10.005
31. Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: an Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation. 2016;134(10):e123–e155. doi:10.1161/CIR.0000000000000404
32. Rao SV, O’Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2025;85(22):2135–2237. doi:10.1016/j.jacc.2024.11.009
33. Chinese Society of Cardiology, Editorial Board of Chinese Journal of Cardiology. Chinese expert consensus on clinical application of percutaneous mechanical circulatory support devices in interventional therapy for patients with complex cardiovascular disease. Zhonghua Xin Xue Guan Bing Za Zhi. 2022;50(10):959–972. doi:10.3760/cma.j.cn112148-20220104-00004.
34. Mishkin J, Paquette J, Couper M, Peltz J, Foster T. A Novel Cardiogenic Shock Management Structure Improves Outcomes and Facilitates Growth. J Card Fail. 2024;30(1):247–248. doi:10.1016/j.cardfail.2023.10.479
35. Szczykutowicz TP, Bujila R, Yin Z, Slavic S, Maltz J. Photon count rates estimated from 1980 clinical CT scans. Med Phys. 2022;49(12):7458–7468. doi:10.1002/mp.15997
36. Sotto KT, Burian BK, Brindle ME. Impact of the WHO Surgical Safety Checklist Relative to Its Design and Intended Use: a Systematic Review and Meta-Meta-Analysis. J Am Coll Surg. 2021;233(6):794–809. doi:10.1016/j.jamcollsurg.2021.08.692
37. Haddad NE, Saleh MN, Eshah NF. Effectiveness of nurse-led video interventions on anxiety in patients having percutaneous coronary intervention. Int J Nurs Pract. 2018;24(4):e12645. doi:10.1111/ijn.12645
38. Snyder A, Binda D, Germany J-L, et al. Capnography: video in Clinical Anesthesia. Anesth Analg. 2023;137(5):943–946. doi:10.1213/ANE.0000000000006684
39. Navarro-Perez R, Romero-García N, Paolessi C, Robba C, Badenes R. Cerebral oximetry in high-risk surgical patients: where are we? Curr Opin Crit Care. 2024;30(6):672–678. doi:10.1097/MCC.0000000000001204
40. Sogut MS, Kalyoncu I, Karakaya MA, Manici M, Darçin K. Does Nociception Level Index-Guided Opioid Administration Reduce Intraoperative Opioid Consumption? A Systematic Review and Meta-Analysis. Anesth Analg. 2024;139(5):978–985. doi:10.1213/ANE.0000000000007180
41. Holzer KJ, Bollepalli H, Carron J, et al. The Impact of Compassion-Based Interventions on Perioperative Anxiety and Depression: a Systematic Review and Meta-Analysis. J Affect Disord. 2024;365:476–491. doi:10.1016/j.jad.2024.08.110
42. Tigges-Limmer K, Sitzer M, Gummert J. Perioperative Psychological Interventions in Heart Surgery. Dtsch Arztebl Int. 2021;118(19–20):339–345. doi:10.3238/arztebl.m2021.0116
43. Rodrigues DJT, Teixeira C, Parola V, Marques P. Radial Artery Haemostasis After Coronary Angiography: a Scoping Review. J Vasc Access. 2025;26(5):1466–1475. doi:10.1177/11297298241290567
44. Zègre-Hemsey JK. Optimizing Patient Outcomes in Emergency Cardiac Care Through Advances in Technology: nurse Scientists in Action. J Emerg Nurs. 2020;46(2):136–138. doi:10.1016/j.jen.2020.01.007
45. Fry C, Engel J, Granger B, Komada M, Lovins J. Evidence-Based Clinical Decision Support to Improve Care for Patients Hospitalized With Acute Myocardial Infarction. Comput Inform Nurs. 2023;41(5):323–329. doi:10.1097/CIN.0000000000000959
46. Radaideh A, Rababah JA, Al-Hammouri MM, Ta’an W, Suliman M. The Association of Health Literacy With the Quality of Discharge Planning and Readiness for Hospital Discharge in Jordanian Acute Myocardial Infarction Patients. J Clin Nurs. 2025;34(9):3745–3752. doi:10.1111/jocn.17543
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Emergency Percutaneous Coronary Intervention Combined with Sacubitril and Valsartan on the Cardiac Prognosis in Patients with Acute Myocardial Infarction
Fan H, Wang Y, Wang X, Dong X, Shao X, Yang F
International Journal of General Medicine 2023, 16:499-505
Published Date: 7 February 2023
Clinical Application of PINK1 and ACSL4 Protein Levels in the Acute Myocardial Infarction Patients and Prognosis Evaluation After PCI
Ao W, Duan P, Luo P, Xiang D, Wang Q, Ren Y, He Q
Research Reports in Clinical Cardiology 2024, 15:45-53
Published Date: 4 June 2024
The Association Between Mitral Regurgitation and Long-Term Outcomes in Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention: A Retrospective Large Sample Cohort Study
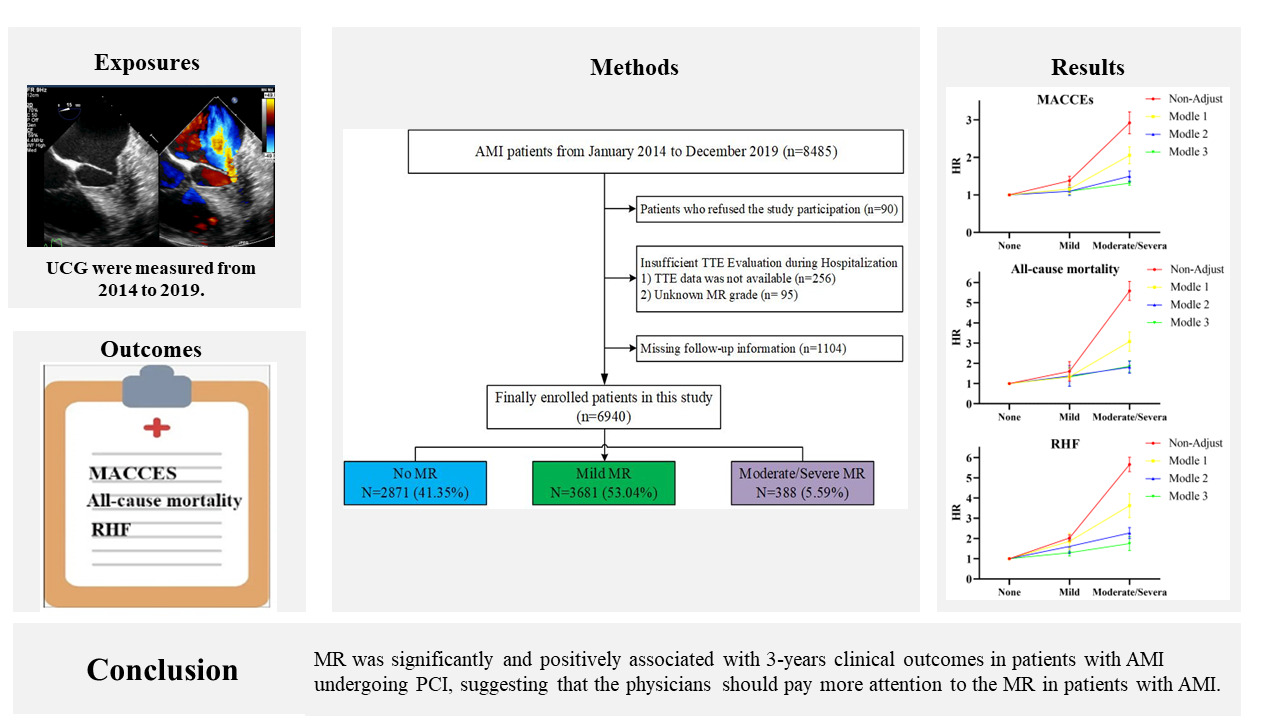
Yan N, Wu P, Zhu B, Ma A, Wang X, Hai X, Ma X, Jiang H, Yang S
International Journal of General Medicine 2025, 18:703-715
Published Date: 11 February 2025