Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Development and Validation of Novel Models Including Tumor Micronecrosis for Predicting the Postoperative Survival of Patients with Hepatocellular Carcinoma
Authors Sun X, Wang Y, Ge H, Chen C, Han X, Sun K, Wang M, Wei X, Ye M, Zhang Q, Liang T
Received 31 May 2023
Accepted for publication 20 July 2023
Published 25 July 2023 Volume 2023:10 Pages 1181—1194
DOI https://doi.org/10.2147/JHC.S423687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Jörg Trojan
Xuqi Sun,1,* Yangyang Wang,2,3,* Hongbin Ge,2,3 Cao Chen,2,3 Xu Han,2,3 Ke Sun,4 Meng Wang,4 Xiaobao Wei,2,3 Mao Ye,2,3 Qi Zhang,2,3,5,6 Tingbo Liang2,3,5,6
1Department of Medical Oncology, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Department of Hepatobiliary and Pancreatic Surgery, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 3Zhejiang Provincial Key Laboratory of Pancreatic Disease, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 4Department of Pathology, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 5Zhejiang University Cancer Center, Hangzhou, People’s Republic of China; 6Zhejiang Clinical Research Center of Hepatobiliary and Pancreatic Diseases, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tingbo Liang; Qi Zhang, Department of Hepatobiliary and Pancreatic Surgery, the First Affiliated Hospital, Zhejiang University School of Medicine, No. 79 Qingchun Road, Hangzhou, 310003, People’s Republic of China, Tel/Fax +86-0571-87236601, Email [email protected]; [email protected]
Background: The heterogeneity of hepatocellular carcinoma (HCC) leads to the unsatisfying predictive performance of current staging systems. HCC patients with pathological tumor micronecrosis have an immunosuppressive microenvironment. We aimed to develop novel prognostic models by integrating micronecrosis to predict the survival of HCC patients after hepatectomy more precisely.
Methods: We enrolled 765 HCC patients receiving curative hepatic resection. They were randomly divided into a training cohort (n= 536) and a validation cohort (n = 229). We developed two prognostic models for postoperative recurrence-free survival (RFS) and overall survival (OS) based on independent factors identified through multivariate Cox regression analyses. The predictive performance was assessed using the Harrell concordance index (C-index) and the time-dependent area under the receiver operating characteristic curve, compared with six conventional staging systems.
Results: The RFS and OS nomograms were developed based on tumor micronecrosis, tumor size, albumin-bilirubin grade, tumor number and prothrombin time. The C-indexes for the RFS nomogram and OS nomogram were respectively 0.66 (95% CI, 0.62– 0.69) and 0.74 (95% CI, 0.69– 0.79) in the training cohort, which was significantly better than those of the six common staging systems (0.52– 0.61 for RFS and 0.53– 0.63 for OS). The results were further confirmed in the validation group, with the C-indexes being 0.66 and 0.77 for the RFS and OS nomograms, respectively.
Conclusion: The two nomograms could more accurately predict RFS and OS in HCC patients receiving curative hepatic resection, thereby aiding in formulating personalized postoperative follow-up plans.
Keywords: hepatocellular carcinoma, micronecrosis, postoperative survival
Introduction
Hepatocellular carcinoma (HCC), one of the most common malignancies, is the third leading cause of cancer-related mortality.1 Curative hepatectomy remains the most effective treatment for HCC patients. Unfortunately, the postoperative recurrence rate can reach up to 70% in five years, which causes the dismal survival of HCC patients.2 Due to the high heterogeneity of HCC, it is challenging to develop clinical models to predict precisely the postoperative prognosis of patients. Several conventional staging systems have been developed to stratify HCC patients with different survival such as the American Joint Committee on Cancer (AJCC) tumor node metastasis (TNM) staging system, Barcelona Clinic Liver Cancer (BCLC) staging classification, Chinese University Prognostic Index (CUPI), Hong Kong Liver Cancer (HKLC) staging system, Japan Integrated Staging (JIS) score, Tokyo score, and Cancer of the Liver Italian Program (CLIP) scoring system; however, there has been no consensus on which system is the optimal.3–8 Besides, these models have limited accuracy in predicting prognosis owing to inherent limitations as the heterogeneity of HCC comprises not only tumor burden and liver function, but also other distinctive factors such as microvascular invasion (MVI).
MVI, a sign for aggressive biology, has been recognized as a predictor of HCC recurrence other than tumor size and number.9 However, some patients still suffer from early recurrence even without these high-risk factors, indicating the necessity to detect other factors to reflect the behavior and heterogeneity of HCC more comprehensively. Unlike massive necrosis, micronecrosis can only be detected under the microscope and is caused by abnormal angiogenesis and chronic ischemic injury.10,11 Our previous studies have found that micronecrosis, a poor prognostic factor for HCC, can identify HCC patients who can benefit from adjuvant transarterial chemoembolization (TACE).12 We have further explored the potential mechanism with mass cytometry and found that the proportions of exhausted T cells and regulatory T cells are substantially high in HCCs with micronecrosis, which indicates an immunosuppressive microenvironment.12 Further research is required to determine whether micronecrosis can complement existing clinicopathologic factors in predicting the prognosis of HCC patients.
We aimed to explore and validate the prognostic value of micronecrosis in predicting the risk of recurrence and mortality in HCC patients after hepatic resection by developing two novel prognostic models. We also compared the predictive performance of our models with that of other conventional staging systems.
Methods
Patient Selection and Study Design
To construct the predicting models for postoperative survival, we consecutively enrolled HCC patients receiving hepatic resection from June 2014 to April 2018 at the First Affiliated Hospital, Zhejiang University School of Medicine (FAHZU). The inclusion criteria were: 1) pathologically diagnosed as HCC; 2) curative hepatectomy with R0 resection and 3) conserved liver function with Child-Pugh class A or B. Patients were excluded for 1) with macrovascular invasion or extrahepatic metastasis; 2) receiving other anti-tumor treatments such as TACE or systemic drugs; 3) with other primary cancers; 4) incomplete follow-up data or 5) without sufficient formalin-fixed, paraffin-embedded (FFPE) specimens for micronecrosis evaluation. A total of 765 patients were finally included in this study. The patients were randomly divided into training and validation cohorts (n = 536 and 229, respectively). We identified independent prognostic factors for recurrence-free survival (RFS) and overall survival (OS) in the training cohort and constructed corresponding nomograms, which were further tested in the validation cohort. Moreover, we stratified all patients according to common staging systems including TNM, BCLC, CUPI, HKLC, JIS, Tokyo score, and CLIP, and compared the predictive performance of our nomograms with these staging systems. This study was approved by the institutional review board of FAHZU (approved ethics number: IIT20220798A).
Tumor Micronecrosis Assessment
The FFEP specimens were cut into 5-μm-thick slides and stained with hematoxylin and eosin (H&E). We took specimens from at least five regions for each tumor, including the central zone of the tumor. The grades of tumor micronecrosis were evaluated by two experienced pathologists based on our previously reported scoring system.12 In summary, the grades of micronecrosis were determined based on the proportion of necrotic area microscopically as follows: grade = 0, ≤5%; grade = 1, 5%-20%; grade = 2, 20%-50%; and grade = 3, >50%. Patients with grade 3 were excluded, as grade 3 micronecrosis was nearly gross necrosis and only existed in a quite small proportion of patients. All the specimens were assessed by two pathologists independently who were blinded to the clinical data of patients. Any inconsistency of assessment results was resolved by consensus after discussion.
Statistical Analyses
RFS and OS were the main endpoints in this study. The RFS was calculated from the date of surgical resection to the date of recurrence or last follow-up. The OS was defined as the period from the surgery date to the date of death or last follow-up. Chi-square or Fisher’s exact test was performed to compare baseline characteristics between the training and validation cohorts. The univariate and multivariate analyses were adopted to identify independent prognostic factors for RFS and OS, respectively. Nomograms were constructed based on the results of multivariate analyses. The predictive performance of our models was assessed using the Harrell’s concordance index (C-index), the time-dependent area under the receiver operating characteristic curve (td AUROC) and decision curve analyses (DCA). Bootstrapping with 1000 samples was performed for calculation. We also compared the discriminatory ability of our nomograms with that of other conventional staging systems (TNM, BCLC, CUPI, HKLC, JIS, Tokyo score, and CLIP) in terms of the aforementioned two parameters. The compareC R package was used to compare the C indexes of different prognostic models.13 To further validate the discriminatory ability of our models, we stratified patients into three subgroups with low, medium and high risk for postoperative recurrence or death by the 50th and 85th percentiles of the corresponding risk scores in the training and validation cohorts based on a previously reported statistical approach for the validation of the Cox proportional hazards regression model.14 The Kaplan-Meier (K-M) method with the Log rank test was adopted to compare the survival curves among subgroups with different risks. All statistical analyses and plotting were performed with the R software, version 3.5.0. A two-sided P-value less than 0.05 was considered statistically significant.
Results
Baseline Characteristics of Patients
The detailed clinicopathological characteristics are listed in Table 1. The median age was 56.5 and 57.0 years old in the training and validation cohorts, respectively. Most patients were infected with hepatitis B virus (HBV), with 83.0% in the training cohort and 83.8% in the validation cohort. MVI was detected in 27.6% of patients in the training cohort, while 27.9% of patients in the validation cohort had MVI. In the training cohort, 28.9% of patients had grade 1 micronecrosis, and 13.8% had grade 2 micronecrosis, whereas, in the validation cohort, the corresponding proportions of which were 35.8% and 12.7% respectively. Patients with MVI tended to have micronecrosis. Among the whole cohort, 15.2% (116/765) patients had co-occurrence of MVI and micronecrosis, 12.5% (96/765) patients had MVI only, 29.3% (224/765) had micronecrosis only, and 43.0% (329/765) patients had neither MVI nor micronecrosis. Most patients had solitary HCC and albumin-bilirubin (ALBI) grade I. There was no significant difference between the training and validation cohorts in terms of baseline characteristics. The median RFS was 35.8 months for the whole cohort, which was 38.4 and 31.0 months in the training and validation cohorts respectively. The median OS did not reach in both cohorts. The survival curves are shown in Supplementary Figure 1.
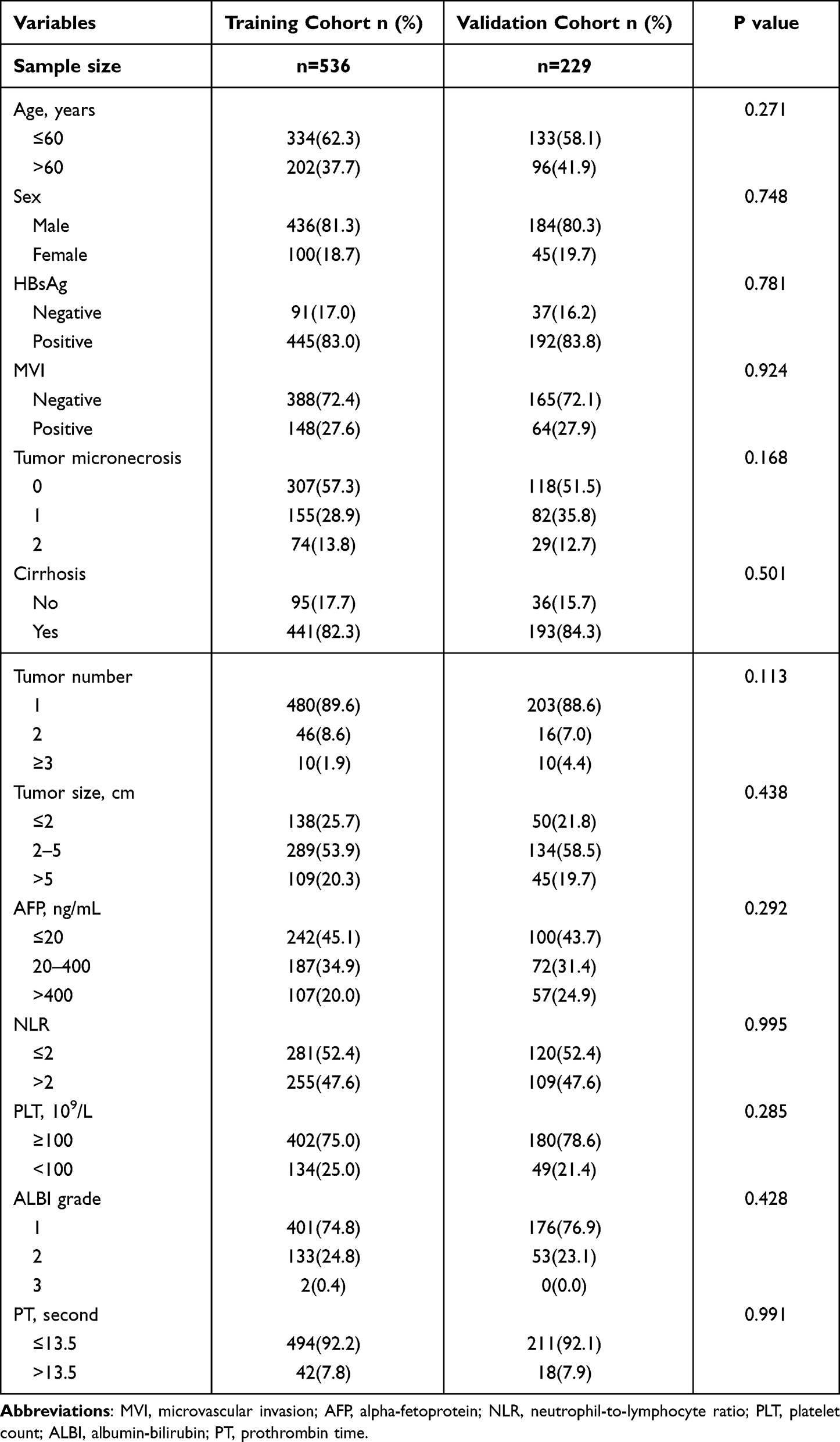 |
Table 1 Baseline Characteristics of the Training and Validation Cohorts |
Development of RFS and OS Predicting Nomograms
To identify independent prognostic factors for RFS and OS after hepatic resection, we performed univariate and multivariate Cox regression analyses in the training cohort, and the results are shown in Table 2. Although MVI was statistically significant in the univariate analyses for both RFS and OS, it was not an independent factor after multivariate analyses. Micronecrosis, tumor number, tumor size and ALBI grade were independently associated with recurrence. In term of OS, micronecrosis, tumor size, ALBI grade and prothrombin time (PT) were independent prognostic factors. Based on these results, we constructed the corresponding nomograms to predict the prognosis of HCC patients after curative hepatic resection (Figure 1).
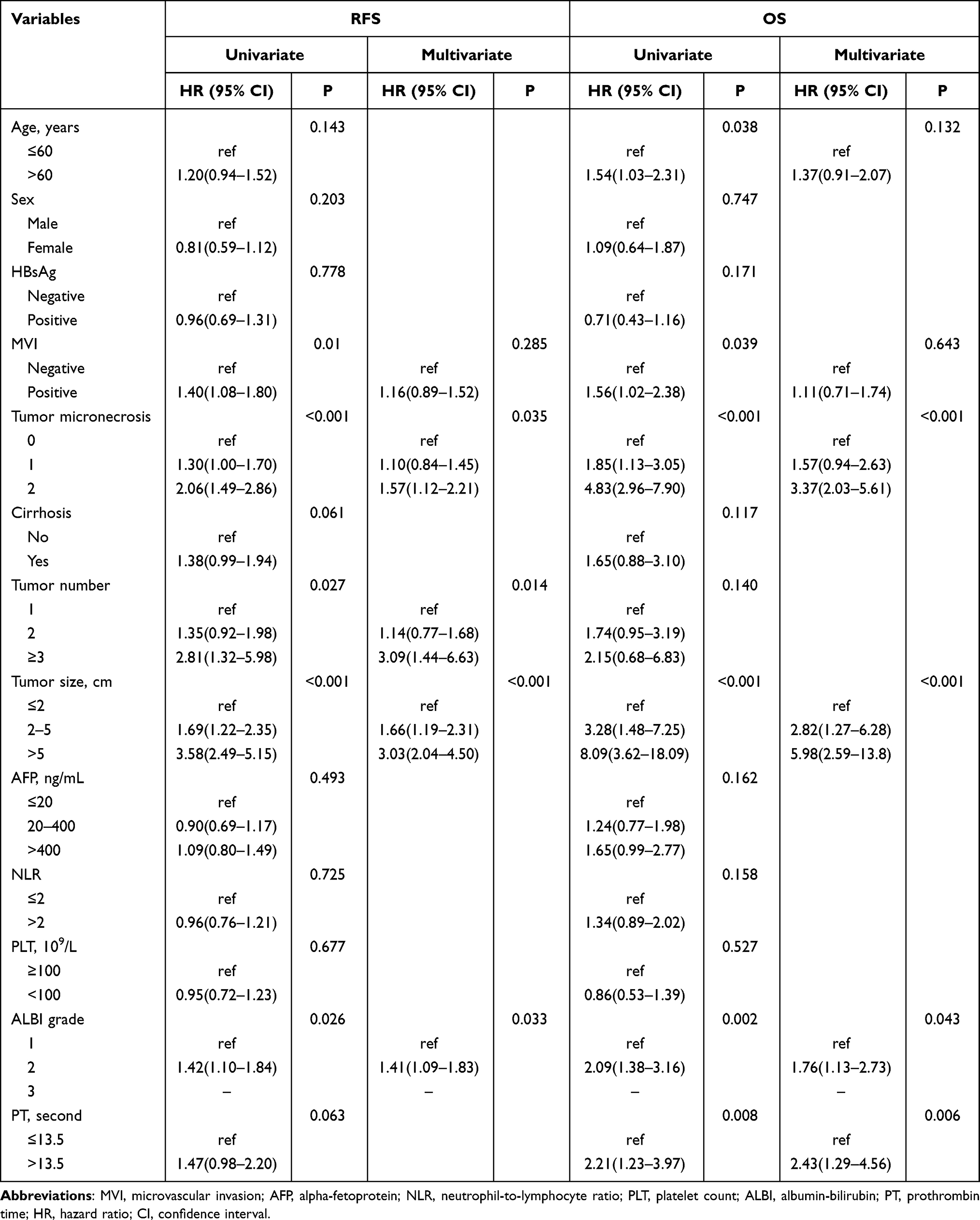 |
Table 2 Univariate and Multivariate Analyses for RFS and OS in the Training Cohort |
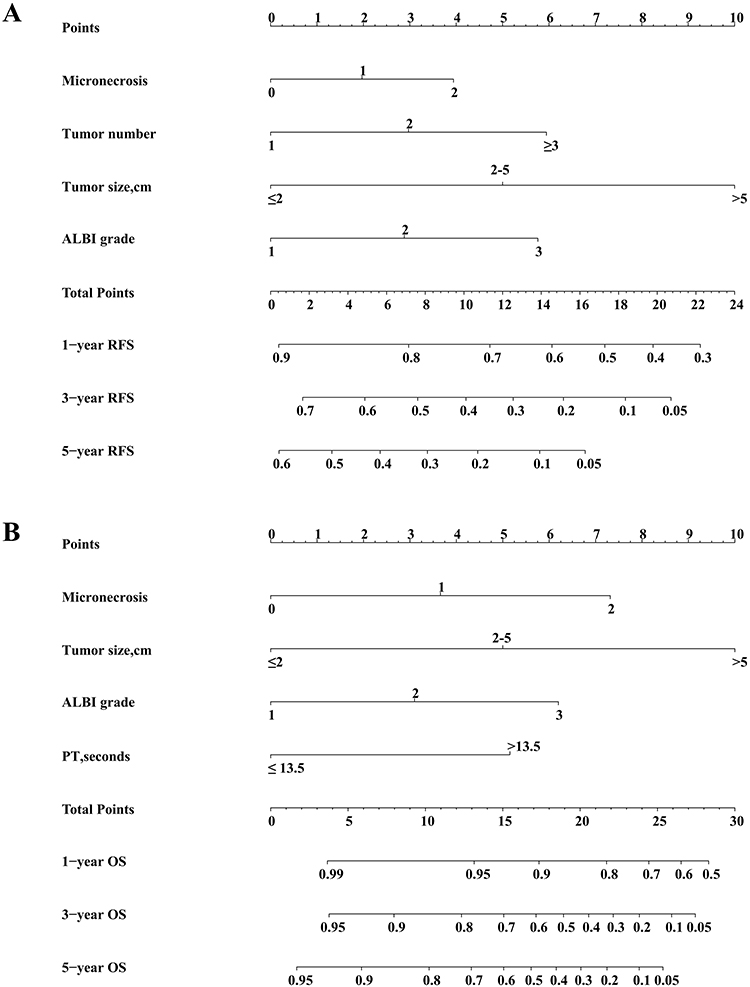 |
Figure 1 The recurrence-free survival (RFS) nomogram (A) and overall survival nomogram (OS) nomogram (B) for predicting postoperative recurrence and death in HCC patients. |
Calibration and Validation of RFS and OS Nomograms
The C-indexes of RFS and OS nomograms were 0.66 (95% CI, 0.62–0.69) and 0.74 (95% CI, 0.69–0.79), respectively, in the training cohort. In the validation cohort, the C-indexes of RFS and OS nomograms were 0.66 (95% CI, 0.62–0.71) and 0.77 (95% CI, 0.70–0.83), respectively. As shown in Figure 2A–C, the RFS predicted by the nomogram correlated well with the actual RFS in the training cohort. The training cohort also demonstrated an excellent agreement between the predicted and actual OS (Figures 3A–C). In the validation cohort, our nomograms presented good correlations between the predicted and actual prognosis in both RFS and OS (Figures 2D–F and 3D–F). We further calculated and plotted the area under the receiver operating characteristics curves (AUROC) of 1-, 2-, 3-, 4- and 5-year RFS and OS in training and validation cohorts. In terms of RFS, for the training cohort, the 1-year AUROC was 0.73; the 2-year AUROC, 0.71; the 3-year AUROC, 0.68; the 4-year AUROC, 0.76; and the 5-year AUROC, 0.66 (Figure 4A). For the validation cohort, the 1-year AUROC was 0.72; the 2-year AUROC, 0.71; the 3-year AUROC, 0.72; the 4-year AUROC, 0.68; and the 5-year AUROC, 0.65 (Figure 4B). In terms of OS, for the training group, the 1-year AUROC was 0.71; the 2-year AUROC, 0.77; the 3-year AUROC, 0.74; the 4-year AUROC, 0.75; and the 5-year AUROC, 0.76 (Figure 4C). For the validation group, the 1-year AUROC was 0.78; the 2-year AUROC, 0.81; the 3-year AUROC, 0.80; the 4-year AUROC, 0.76; and the 5-year AUROC, 0.71 (Figure 4D). In addition, the DCA curves showed good positive net benefits in training and validation cohorts for RFS and OS at different time points (recurrence and death at 1, 3, 5 years) (Supplementary Figure 2). As shown in the DCA, “all” and “none” represented that all the patients were recurrence-free and recurrent (Supplementary Figure 2A and B) or alive and dead (Supplementary Figure 2C and D).The net benefit of RFS nomogram was higher than that of treat none or treat all strategies within a threshold probability range of 0.13 to 0.72. In terms of OS, the net benefit of the prognostic model was better within a threshold probability range of 0.02 to 0.50. After stratifying the patients based on the risk scores calculated with independent factors for recurrence or death, the survival curves were plotted with the K-M method. As shown in Supplementary Figures 3A and B, patients with different risk scores for recurrence had significantly different RFS in either training or validation cohort (P < 0.001). Similarly, the OS differed significantly among patients with varying scores for death in both training and validation cohorts (P < 0.001) (Supplementary Figures 3C and D).
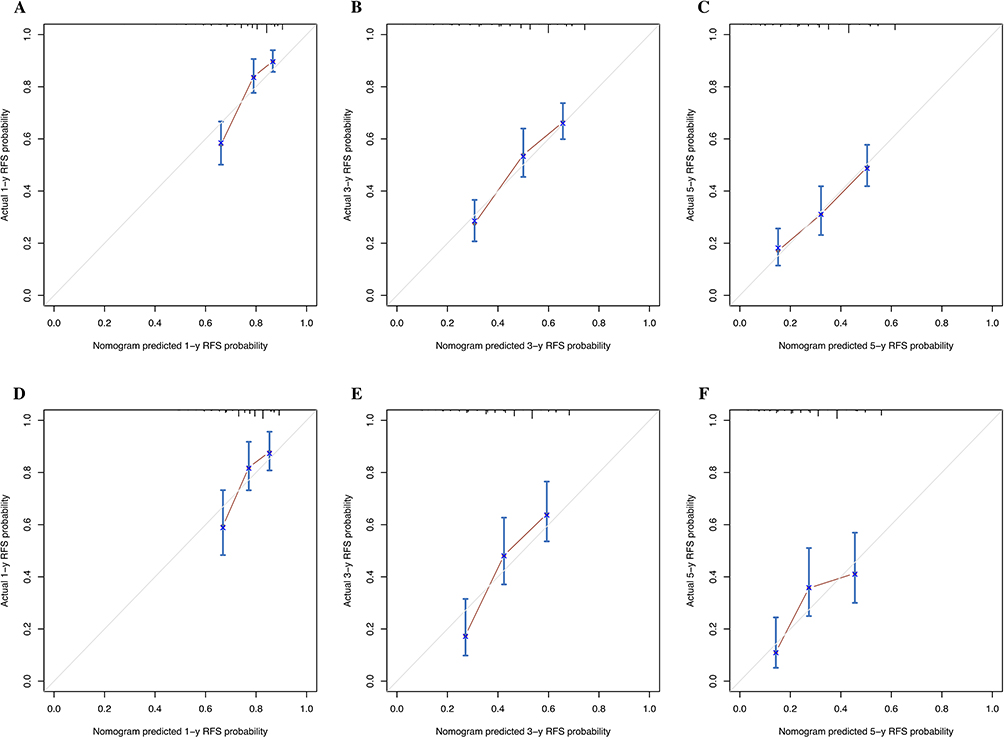 |
Figure 2 The calibration curves for predicting the 1-, 3- and 5-year recurrence-free survival (RFS) in the training (A–C) and validation (D–F) cohorts. |
 |
Figure 3 The calibration curves for predicting the 1-, 3- and 5-year overall survival (OS) in the training (A–C) and validation (D–F) cohorts. |
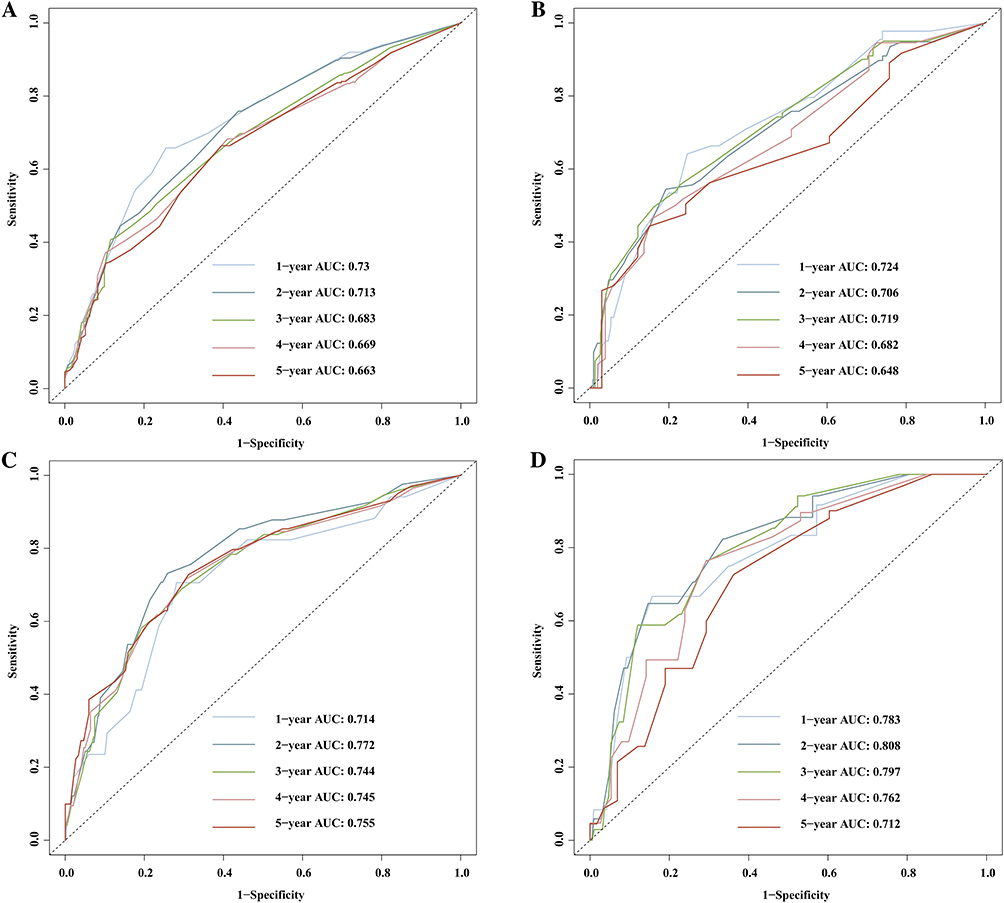 |
Figure 4 The receiver operating characteristics curves (AUROC) of 1-, 2-, 3-, 4- and 5-year recurrence-free survival (RFS) in the training (A) and validation (B) cohorts, and the AUROCs of 1-, 2-, 3-, 4- and 5-year overall survival (OS) in the training (C) and validation (D) cohorts. |
Comparing Predictive Performance with Conventional Staging Systems
We further compared the predictive performance of our nomograms with that of conventional staging systems (TNM, BCLC, CUPI, HKLC, JIS, Tokyo score, and CLIP). For the RFS nomogram, the C-index was substantially higher than that of TNM (0.61, 95% CI: 0.58–0.64, P < 0.001), BCLC (0.58, 95% CI: 0.56–0.61, P < 0.001), CUPI (0.52, 95% CI: 0.49–0.55, P < 0.001), HKLC (0.59, 95% CI: 0.56–0.62, P < 0.001), JIS (0.57, 95% CI: 0.66–0.60, P < 0.001), Tokyo score (0.60, 95% CI: 0.57–0.63, P < 0.001), and CLIP (0.55, 95% CI: 0.52–0.58, P<0.001). The superiority of the RFS nomogram in predicting recurrence was confirmed in the validation cohort. The detailed data are listed in Table 3. As demonstrated by the td AUROC, our RFS nomogram had a better ability to predict postoperative recurrence than other staging systems in both training and validation cohorts (Figures 5A and B). The superiority of the OS nomogram was also assessed. The C-index of our OS nomogram was significantly higher than that of TNM (0.61, 95% CI: 0.56–0.67, P < 0.001), BCLC (0.61, 95% CI: 0.57–0.65, P < 0.001), CUPI (0.53, 95% CI: 0.48–0.58, P < 0.001), HKLC (0.61, 95% CI: 0.56–0.66, P < 0.001), JIS (0.59, 95% CI: 0.55–0.63, P < 0.001), Tokyo score (0.62, 95% CI: 0.57–0.68, P < 0.001) and CLIP (0.57, 95% CI: 0.51–0.62, P < 0.001) in the training cohort. These results were verified in the validation cohort. The corresponding td AUROCs are shown in Figures 5C and 5D.
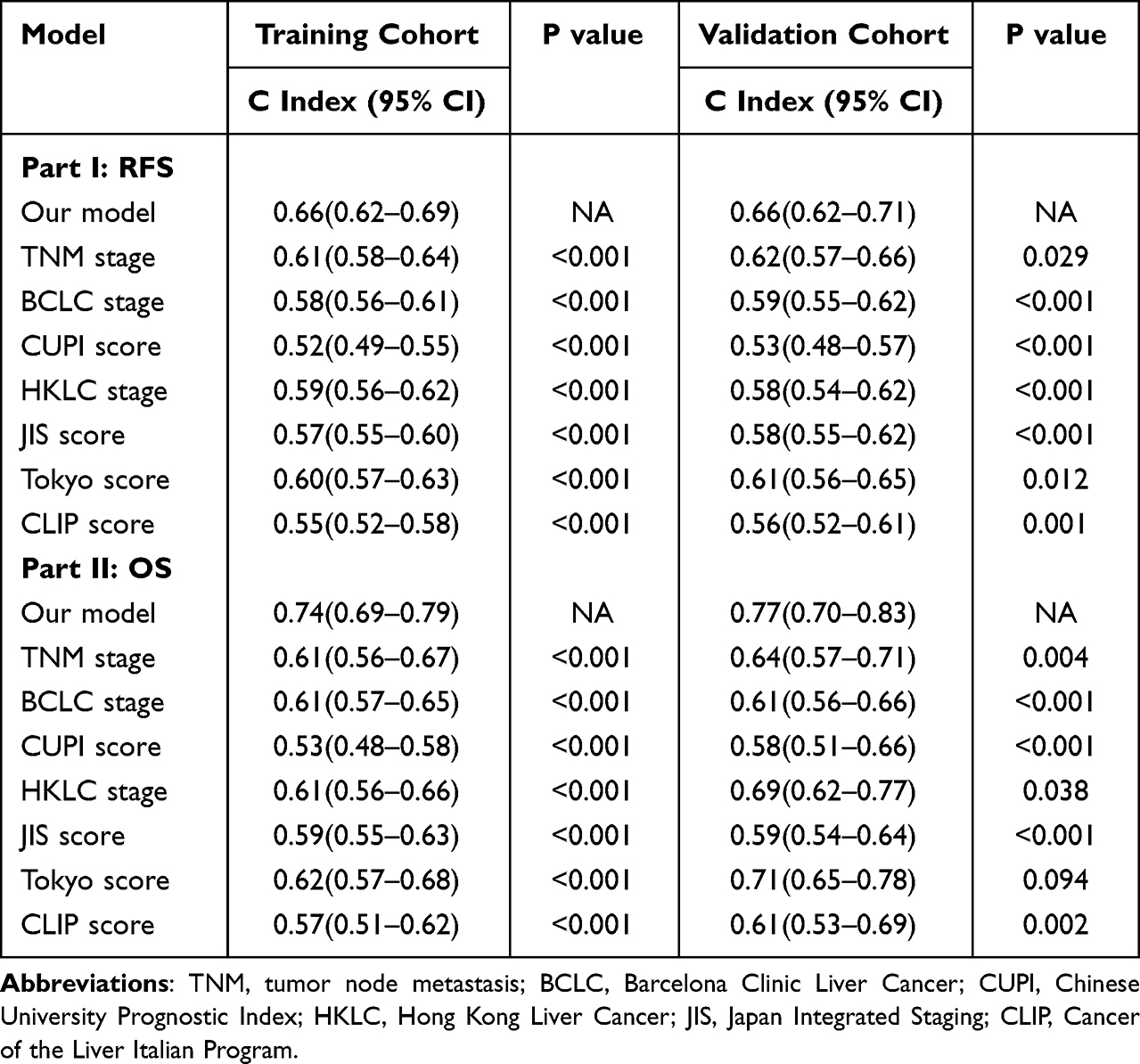 |
Table 3 C-Indexes of Different Prognostic Models for RFS and OS in the Training and Validation Cohorts |
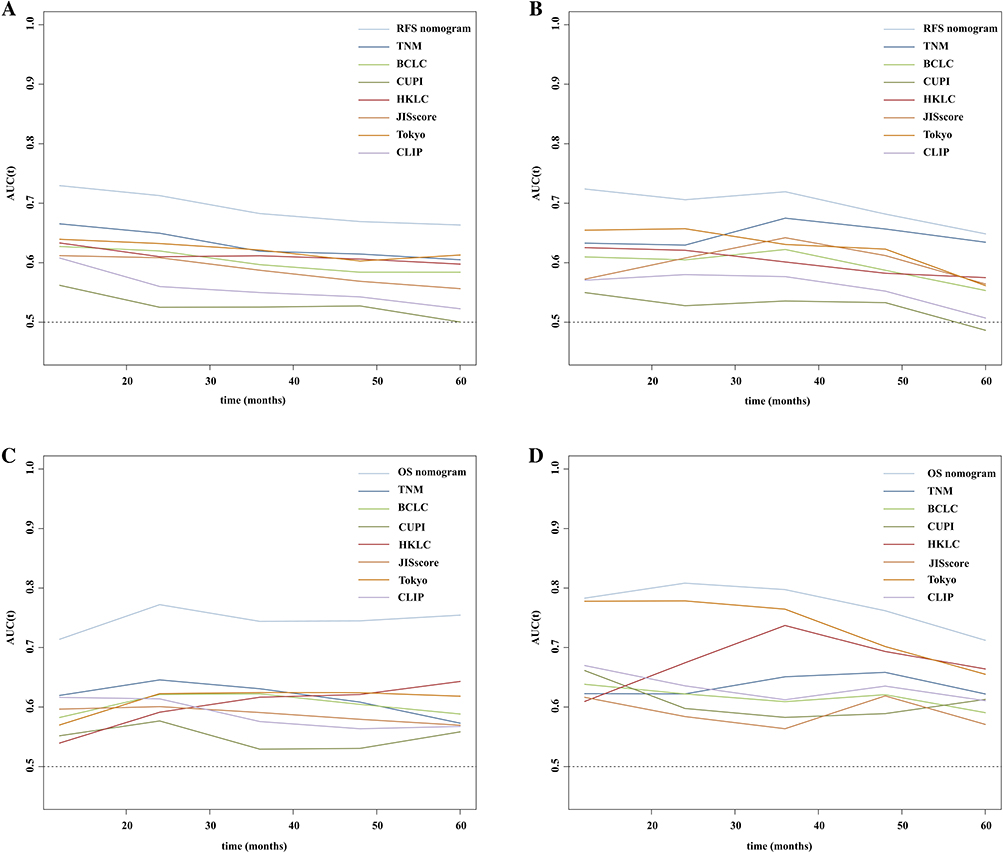 |
Figure 5 The time-dependent area under the receiver operating characteristic curves (td AUROC) of recurrence-free survival (RFS) nomogram and other staging systems (TNM, BCLC, CUPI, HKLC, JIS, Tokyo score and CLIP) since hepatic resection over time in the training (A) and validation (B) cohorts, and the td AUROCs of overall survival (OS) nomogram and other staging systems in the training (C) and validation (D) cohorts. |
Discussion
Hepatic resection remains the most effective treatment modality for HCC, but the high rate of postoperative recurrence impedes survival improvement. Studies have found that curative local ablative therapy can achieve comparable survival in primary and recurrent HCC patients, highlighting the necessity for timely prediction and detection of recurrent HCCs.15,16 In this study, we developed and validated two prognostic models for RFS and OS by integrating micronecrosis and other conventional variables for HCC patients receiving curative hepatic resection. The C-indexes in the training and validation cohorts were, respectively, 0.66 and 0.66 for RFS prediction and 0.74 and 0.77 for OS prediction. The RFS and OS nomograms had superior predictive performance compared with conventional staging systems (TNM, BCLC, CUPI, HKLC, JIS, Tokyo score, and CLIP), which remained consistent during follow-up. The risk scores could stratify patients with distinct prognoses. The RFS and OS nomograms in this study could be potential useful tools for predicting postoperative survival in HCC patients during clinical practice.
For HCC patients, recurrence severely hampers the improvement of their survival. Although some clinicopathological characteristics have been identified as common risk factors for poor prognoses, such as high tumor burden and MVI, patients without these poor prognostic indicators still suffer from early recurrence and dismal survival, which indicates the necessity for further exploring related factors to reflect the biological characteristics of HCC comprehensively. Several staging systems, commonly consisting of tumor burden and liver function, have been developed to classify HCC patients and provide suitable treatments; however, the prognostic performance of these models remains to be improved. Researchers have developed prognostic models by integrating genomic factors to stratify better and predict HCC patients with different survival; however, these models usually require expensive and complex technologies.17,18 H&E specimens are routinely necessary after surgery and require low cost, so exploring biological characteristics based on H&E specimens will be highly cost-effective. Micronecrosis, a common pathological alternation, has been proven to be associated with metastasis and poor prognosis in colorectal cancer and pancreatic cancer.19,20 We previously found that tumor micronecrosis had negative effects on the prognosis of HCC patients and could be an indicator for selecting suitable candidates to receive adjuvant TACE.12,21 We graded micronecrosis based on the proportion of necrosis in the surgical specimens from HCC patients, which was negatively correlated with prognosis. However, whether micronecrosis can be adopted as a predictor in prognostic models for HCC patients after curative hepatic resection needs to be further evaluated. The present study assessed the prognostic performance of MVI and micronecrosis in postoperative HCC patients. Compared with MVI, micronecrosis is more common in HCC patients. Although MVI had significant effects on RFS and OS in the univariate analyses, it was not an independent factor for survival after multivariate analyses, while micronecrosis remained essential for RFS and OS. After combining micronecrosis with other independent prognostic factors, the developed RFS and OS nomograms had good predictive performance, substantially better than the other six conventional staging systems over time.
The prognosis of postoperative HCC patients is affected by many factors, including tumor burden and liver function. Tumor size was identified as an independent factor for recurrence and death in this study, which is universally recognized.22 Although tumor number was the predictor only for recurrence in this study, this could be caused by several factors. Nearly 90% of patients enrolled in this study had solitary HCC, so the effect of tumor number might be undervalued with the low proportion of patients with multiple tumors. Besides, patients receiving hepatectomy tend to be at an early stage, and they can receive various subsequent treatments during the course of the disease, which can cause confounding effects on the evaluation of prognostic factors for OS.23 Preoperative liver function is an important factor for the survival of HCC patients, and the ALBI grade has been proven to be more objective and accurate than the conventional Child-Pugh grade.24,25 Compared with the aforementioned clinical factors, PT has been less reported as the independent factor for the survival of HCC patients, but studies have confirmed its prognostic value in HCC patients.26–28 As is known, the coagulation is a reflection of liver function. Therefore, prolonged PT can be a potential risk factor for poor prognosis in HCC patients. Overall, our prognostic models had good predictive performance by incorporating common clinical factors and a newly proposed factor- micronecrosis, which can be conveniently applied in clinical practice with high cost-effectiveness. With the development of medical technology, more treatment modalities can be adopted for recurrent or advanced HCC such as intensity-modulated radiotherapy and Gamma knife radiosurgery.29,30 In this circumstance, the impact of different treatment modalities after recurrence on survival might can be further explored. Besides, new prognostic biomarkers are constantly being discovered such as programmed cell death-Ligand 1 expression on circulating tumor cells and Heat-shock protein 90α, whether these biomarkers can assist to better stratify HCC patients with different survival needs further exploration.31–33
This study has several limitations except for its retrospective nature. First, the predictive nomograms were developed based on the patients from the endemic area of HBV; it remains to be determined whether these prognostic models can be applied to HCC patients with other etiologies. Second, although we have assessed the predictive performance of these nomograms by internal validation, these prognostic models need to be further evaluated by external validation. Third, the models were developed using the data from patients with primary HCC receiving hepatic resection; their applicability to patients with recurrent HCC needs further assessment. Forth, micronecrosis is currently assessed based on surgical specimens, but numerous early-stage HCC patients receive radiofrequency or microwave ablation, among whom there are no sufficient specimens. How to assess micronecrosis based on routine computer tomography or magnetic resonance imaging remains to be solved.
Conclusions
In this study, we developed two prognostic models that could accurately predict postoperative RFS and OS in HCC patients receiving curative hepatic resection. Our models can assist in formulating personalized postoperative follow-up plans, which can contribute to improving the survival of HCC patients.
Abbreviations
HCC, hepatocellular carcinoma; AJCC, the American Joint Committee on Cancer; TNM, tumor node metastasis; BCLC, Barcelona Clinic Liver Cancer; CUPI, Chinese University Prognostic Index; HKLC, Hong Kong Liver Cancer; JIS, Japan Integrated Staging; CLIP, Cancer of the Liver Italian Program; MVI, microvascular invasion; TACE, transarterial chemoembolization; FAHZU, The First Affiliated Hospital, Zhejiang University School of Medicine; FFPE, formalin-fixed, paraffin-embedded; RFS, recurrence-free survival; OS, overall survival; H&E, hematoxylin and eosin; C-index, the Harrell’s concordance index; tdAUROC, time-dependent area under the receiver operating characteristic curve; K-M, the Kaplan-Meier; HBV, hepatitis B virus; ALBI, albumin-bilirubin; PT, prothrombin time.
Data Sharing Statement
The datasets used during the current study are available from the corresponding authors on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the institutional review board of The First Affiliated Hospital, Zhejiang University School of Medicine as a retrospective study (approved ethics number: IIT20220798A), and the requirement for informed consent was waived since the data were obtained from previous medical record and it did not cause adverse effects on the rights and health of subjects. All patients’ data assessed complied with relevant data protection and privacy regulation. All procedures performed in studies involving human participants were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments.
Acknowledgments
We thank Chao Huang and Jingsong Li (from Research Center for Healthcare Data Science, Zhejiang Lab, Hangzhou, China) for their advice and help on statistical analyses.
Funding
This work was financially supported by the National Natural Science Foundation of China (Nos. 82202875, 82071865 and 82188102), Zhejiang Provincial National Science Foundation of China (No. LQ23H160029 and LR20H160002), the National Key Research & Development Program (No. 2020YFA0804300 and 2020YFA0804301), and the Fundamental Research Funds for the Central Universities (No. 226-2022-00144).
Disclosure
The authors declare that they have no competing interests.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Ercolani G, Grazi GL, Ravaioli M, et al. Liver resection for hepatocellular carcinoma on cirrhosis: univariate and multivariate analysis of risk factors for intrahepatic recurrence. Ann Surg. 2003;237(4):536–543. doi:10.1097/01.SLA.0000059988.22416.F2
3. Edge SB, Compton CC. The American joint committee on cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
4. Kudo M, Chung H, Osaki Y. Prognostic staging system for hepatocellular carcinoma (CLIP score): its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J Gastroenterol. 2003;38(3):207–215. doi:10.1007/s005350300038
5. Leung TW, Tang AM, Zee B, et al. Construction of the Chinese University Prognostic Index for hepatocellular carcinoma and comparison with the TNM staging system, the Okuda staging system, and the Cancer of the Liver Italian Program staging system: a study based on 926 patients. Cancer. 2002;94(6):1760–1769. doi:10.1002/cncr.10384
6. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
7. Tateishi R, Yoshida H, Shiina S, et al. Proposal of a new prognostic model for hepatocellular carcinoma: an analysis of 403 patients. Gut. 2005;54(3):419–425. doi:10.1136/gut.2003.035055
8. Yau T, Tang VY, Yao TJ, Fan ST, Lo CM, Poon RT. Development of Hong Kong Liver Cancer staging system with treatment stratification for patients with hepatocellular carcinoma. Gastroenterology. 2014;146(7):1691–1700 e1693. doi:10.1053/j.gastro.2014.02.032
9. Shindoh J, Andreou A, Aloia TA, et al. Microvascular invasion does not predict long-term survival in hepatocellular carcinoma up to 2 cm: reappraisal of the staging system for solitary tumors. Ann Surg Oncol. 2013;20(4):1223–1229. doi:10.1245/s10434-012-2739-y
10. Karsch-Bluman A, Benny O. Necrosis in the tumor microenvironment and its role in cancer recurrence. Adv Exp Med Biol. 2020;1225:89–98.
11. Vaupel P, Mayer A. Hypoxia in cancer: significance and impact on clinical outcome. Cancer Metastasis Rev. 2007;26(2):225–239. doi:10.1007/s10555-007-9055-1
12. Wang Y, Ge H, Hu M, et al. Histological tumor micronecrosis in resected specimens after R0 hepatectomy for hepatocellular carcinomas is a factor in determining adjuvant TACE: a retrospective propensity score-matched study. Int J Surg. 2022;105:106852. doi:10.1016/j.ijsu.2022.106852
13. Kang L, Chen W, Petrick NA, Gallas BD. Comparing two correlated C indices with right-censored survival outcome: a one-shot nonparametric approach. Stat Med. 2015;34(4):685–703. doi:10.1002/sim.6370
14. Royston P, Altman DG. External validation of a Cox prognostic model: principles and methods. BMC Med Res Methodol. 2013;13:33. doi:10.1186/1471-2288-13-33
15. Wang K, Liu G, Li J, et al. Early intrahepatic recurrence of hepatocellular carcinoma after hepatectomy treated with re-hepatectomy, ablation or chemoembolization: a prospective cohort study. Eur J Surg Oncol. 2015;41(2):236–242. doi:10.1016/j.ejso.2014.11.002
16. Yamamoto J, Okada S, Shimada K, et al. Treatment strategy for small hepatocellular carcinoma: comparison of long-term results after percutaneous ethanol injection therapy and surgical resection. Hepatology. 2001;34(4 Pt 1):707–713. doi:10.1053/jhep.2001.27950
17. van Malenstein H, van Pelt J, Verslype C. Molecular classification of hepatocellular carcinoma anno 2011. Eur J Cancer. 2011;47(12):1789–1797. doi:10.1016/j.ejca.2011.04.027
18. Villanueva A, Hoshida Y, Toffanin S, et al. New strategies in hepatocellular carcinoma: genomic prognostic markers. Clin Cancer Res. 2010;16(19):4688–4694. doi:10.1158/1078-0432.CCR-09-1811
19. Chatzopoulos K, Kotoula V, Koliou GA, et al. Genotype-phenotype associations in colorectal adenocarcinomas and their matched metastases. Hum Pathol. 2021;107:104–116. doi:10.1016/j.humpath.2020.10.009
20. Hiraoka N, Ino Y, Sekine S, et al. Tumour necrosis is a postoperative prognostic marker for pancreatic cancer patients with a high interobserver reproducibility in histological evaluation. Br J Cancer. 2010;103(7):1057–1065. doi:10.1038/sj.bjc.6605854
21. Ye Q, Zhang Q, Tian Y, et al. Method of tumor pathological micronecrosis quantification via deep learning from label fuzzy proportions. IEEE J Biomed Health Inform. 2021;25(9):3288–3299. doi:10.1109/JBHI.2021.3071276
22. Vogel A, Cervantes A, Chau I, et al. Hepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv238–iv255. doi:10.1093/annonc/mdy308
23. Zhao F. Surrogate end points and their validation in oncology clinical trials. J Clin Oncol. 2016;34(13):1436–1437. doi:10.1200/JCO.2016.66.4581
24. Kudo M. Newly developed modified ALBI grade shows better prognostic and predictive value for hepatocellular carcinoma. Liver Cancer. 2022;11(1):1–8. doi:10.1159/000521374
25. Pinato DJ, Sharma R, Allara E, et al. The ALBI grade provides objective hepatic reserve estimation across each BCLC stage of hepatocellular carcinoma. J Hepatol. 2017;66(2):338–346. doi:10.1016/j.jhep.2016.09.008
26. Mao M, Wang X, Song Y, et al. Novel prognostic scores based on plasma prothrombin time and fibrinogen levels in patients with AFP-negative hepatocellular carcinoma. Cancer Control. 2020;27(1):1073274820915520. doi:10.1177/1073274820915520
27. Takaya H, Namisaki T, Takeda S, et al. The combination of albumin-bilirubin score and prothrombin time is a useful tool for predicting liver dysfunction after transcatheter arterial chemoembolization in Child-Pugh class A patients with hepatocellular carcinoma within up-to-seven criteria. J Clin Med. 2021;10(21):4838. doi:10.3390/jcm10214838
28. Wang XP, Mao MJ, He ZL, et al. A retrospective discussion of the prognostic value of combining prothrombin time(PT) and fibrinogen(Fbg) in patients with Hepatocellular carcinoma. J Cancer. 2017;8(11):2079–2087. doi:10.7150/jca.19181
29. Su K, Gu T, Xu K, et al. Gamma knife radiosurgery versus transcatheter arterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombus: a propensity score matching study. Hepatol Int. 2022;16(4):858–867. doi:10.1007/s12072-022-10339-2
30. Su K, Guo L, Ma W, et al. PD-1 inhibitors plus anti-angiogenic therapy with or without intensity-modulated radiotherapy for advanced hepatocellular carcinoma: a propensity score matching study. Front Immunol. 2022;13:972503. doi:10.3389/fimmu.2022.972503
31. Su K, Guo L, He K, et al. PD-L1 expression on circulating tumor cells can be a predictive biomarker to PD-1 inhibitors combined with radiotherapy and antiangiogenic therapy in advanced hepatocellular carcinoma. Front Oncol. 2022;12:873830. doi:10.3389/fonc.2022.873830
32. Su K, Huang W, Li X, et al. Evaluation of lactate dehydrogenase and alkaline phosphatase as predictive biomarkers in the prognosis of hepatocellular carcinoma and development of a new nomogram. J Hepatocell Carcinoma. 2023;10:69–79. doi:10.2147/JHC.S398632
33. Su K, Liu Y, Wang P, et al. Heat-shock protein 90α is a potential prognostic and predictive biomarker in hepatocellular carcinoma: a large-scale and multicenter study. Hepatol Int. 2022;16(5):1208–1219. doi:10.1007/s12072-022-10391-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.