Back to Journals » Patient Preference and Adherence » Volume 19
Developing a Nomogram Prediction Model for Dietary Behavior Adherence in Hemodialysis Patients
Received 28 August 2025
Accepted for publication 26 November 2025
Published 5 December 2025 Volume 2025:19 Pages 3889—3900
DOI https://doi.org/10.2147/PPA.S559708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yanyan Liu, Xiurong Wen
Department of Nephrology, Ganzhou People’s Hospital, Ganzhou City, Jiangxi Province, 341000, People’s Republic of China
Correspondence: Xiurong Wen, Department of Nephrology, Ganzhou People’s Hospital, No. 16, Meiguan Avenue, Zhanggong District, Ganzhou City, Jiangxi Province, 341000, People’s Republic of China, Tel +8615170615680, Email [email protected]
Objective: To develop a nomogram prediction model for dietary behavior adherence in hemodialysis (HD) patients, providing a simple and accurate tool for individualized risk prediction and supporting effective intervention strategies.
Methods: A total of 236 HD patients admitted from January 2022 to January 2024 were retrospectively included as the modeling group, and another 121 HD patients admitted from January 2024 to May 2025 served as the validation group. Patients in both groups were classified into compliance and non-compliance groups according to their dietary adherence. Lasso regression and multivariate logistic analysis were used to identify independent predictors and construct the nomogram. Internal and external validation were performed using ROC curves, the Hosmer–Lemeshow (H–L) test, calibration curves, and decision curve analysis (DCA).
Results: Among the 236 patients in the modeling group, 73 (30.93%) showed dietary non-compliance. Age, years on dialysis, educational level, dietary knowledge, social support, family support, and self-care ability significantly differed between the two groups (P< 0.05). Seven variables selected by Lasso regression were entered into logistic analysis. Age, years on dialysis, and poor self-care ability were risk factors for non-adherence, whereas higher educational level, better dietary knowledge, stronger social support, and family support were protective factors (P< 0.05). The internal validation yielded an AUC of 0.884 and an H–L χ2 of 7.346 (P=0.713), while the external validation showed an AUC of 0.902 and an H–L χ2 of 7.342 (P=0.726). DCA indicated high clinical utility within threshold probabilities of 0.10– 0.83 (internal) and 0.15– 0.84 (external).
Conclusion: Age, years on dialysis, educational level, dietary knowledge, social support, family support, and self-care ability are key factors influencing dietary adherence in HD patients. The nomogram based on these variables demonstrated good discrimination and clinical benefit, aiding early identification of high-risk patients and supporting individualized dietary management.
Keywords: hemodialysis, dietary behavior, compliance, influencing factors, nomogram
Introduction
Hemodialysis (HD) is one of the life-sustaining treatments for patients with end-stage chronic kidney disease. It can reduce the accumulation of waste and toxins in the body, thereby improving the acid-base imbalances and electrolyte disturbances caused by renal failure. In recent years, the incidence of chronic kidney disease has been increasing annually, and many patients rely on HD to sustain their lives.1 However, HD treatment is not a definitive cure; during the treatment period, patients must strictly follow dietary management to reduce the risk of complications and improve their quality of life.2 Studies have found that the non-adherence rate during treatment in HD patients can be as high as 82.4%, and that improper diet in HD patients can often induce multiple clinical problems.3 Excessive intake of minerals such as sodium and potassium can cause electrolyte disturbances, insufficient protein intake can lead to malnutrition, and neglecting the intake of dietary fiber can cause gastrointestinal disorders, thereby affecting the treatment outcome.4 Therefore, identifying the factors that influence patients’ dietary adherence and intervening early can improve their quality of life. The nomogram model is a tool commonly used in clinical practice to assess prognosis. It is easy to operate and can predict the risk of adverse events, thus assisting clinicians in developing corresponding strategies to reduce the risk of poor outcomes.5,6 Studies have shown that constructing a nomogram prediction model for medication adherence in HD patients identified eight predictive variables, and the AUC, DCA, and calibration curves demonstrated that the model had good discrimination and accuracy.5 Currently, there are few reports on the use of nomograms to study dietary non-adherence in HD patients. Therefore, this study aims to analyze the influencing factors of dietary behavior adherence in HD patients and to construct a predictive nomogram model.
Materials and Methods
General Data
A retrospective collection was made of 236 HD patients treated at our hospital from January 2022 to January 2024 (as the modeling group). Additionally, 121 HD patients treated at our hospital from January 2024 to May 2025 were collected (as the validation group). Patients in the modeling and validation groups were divided into a dietary non-adherence group and a dietary adherence group based on their dietary adherence. The case collection flowchart is shown in Figure 1. Inclusion criteria: (1) dialysis for more than 12 months; (2) age ≥18 years; (3) capable of communication and comprehension; (4) complete clinical data. Exclusion criteria: (1) patients unable to undergo regular dialysis; (2) patients with recent acute complications such as heart failure or cerebral hemorrhage; (3) patients with malignant tumors; (4) women during lactation or pregnancy; (5) patients with multiple organ dysfunction. This study was approved by the ethics committee of our hospital.
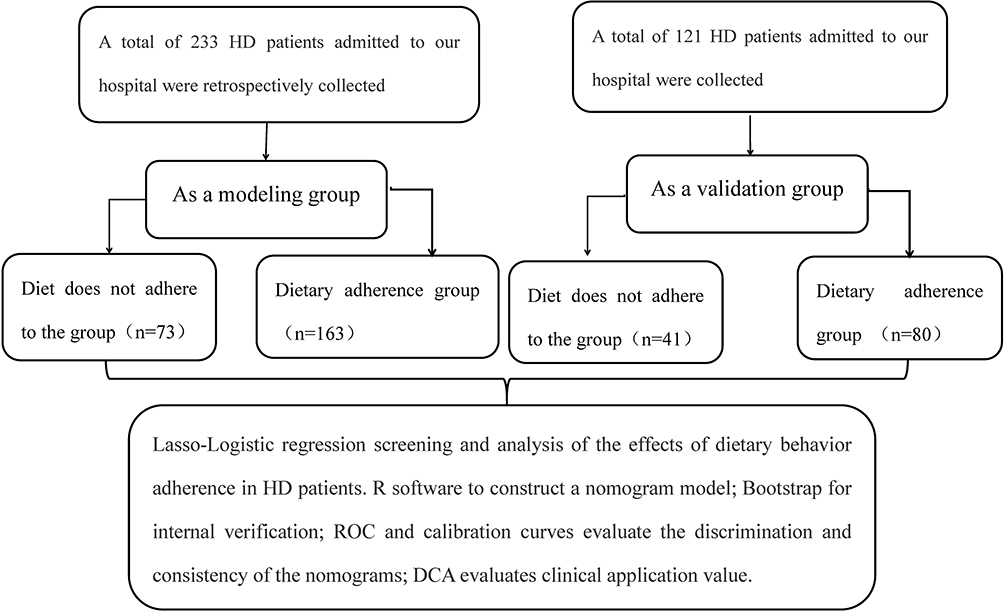 |
Figure 1 Case flow collection diagram. |
Methods
Determination of Dietary Adherence
Patient dietary adherence was assessed using the Dietary Adherence in Kidney Disease Scale, which includes 5 dimensions (salt intake, self-care, potassium intake, fluid restriction, adherence when facing difficulties)7 and 25 items, scored using the Likert 5-point method. A score of ≤25 points was defined as dietary non-adherence, based on which patients were divided into the non-adherence group and the adherence group.
Clinical Data Collection
Electronic medical records of patients in our hospital were collected (The binary classification was based on the median value to facilitate statistical analysis), including age, gender, BMI, monthly household income per capita, duration of dialysis, living alone, education level, place of residence, marital status, primary kidney disease, vascular access type, dietary knowledge (assessed by a self-developed questionnaire, revised by experts, including 13 items on basic knowledge, diet, and medication, with a maximum score of 13; a higher score indicates better knowledge), payment method, social support (including 3 dimensions, 10 items, with a total score of 44; a higher score indicates greater support),8 family support (By asking the patients or their family members), negative emotions (Using a depression scale consisting of 20 items, with 53 as the cutoff value; scores ≥53 indicate the presence of negative emotions),9 self-care ability (assessed using the Barthel Index, with a total score of 100; ≤40 points indicates severe dependence, >40 points indicates mild dependence),10 employment status, dialysis-related complications, and hemodialysis frequency. This study excluded all cases with missing data.
Statistical Processing
Data were processed using SPSS 25.0. Measurement data were analyzed using the t-test and are expressed as (mean ± SD), while categorical data were analyzed using the χ2-test and are presented as n (%). Lasso-Logistic regression was used to screen for and analyze the influencing factors of dietary adherence in HD patients. R software was used to construct the nomogram model. The Bootstrap method was used for internal validation (1000 resamples). ROC and calibration curves were used to evaluate the discrimination and consistency of the nomogram. DCA was used to assess the clinical application value. A P-value < 0.05 was considered statistically significant.
Results
Comparison of Clinical Data Between the Dietary Non-Adherence and Adherence Groups in the Modeling Group
Among the 236 patients in the modeling group, 73 (30.93%) had dietary non-adherence. There were significant differences in age, duration of dialysis, education level, dietary knowledge, social support, family support, and self-care ability between the non-adherence and adherence groups (P < 0.05). There were no significant differences in other clinical data (P > 0.05). See Table 1.
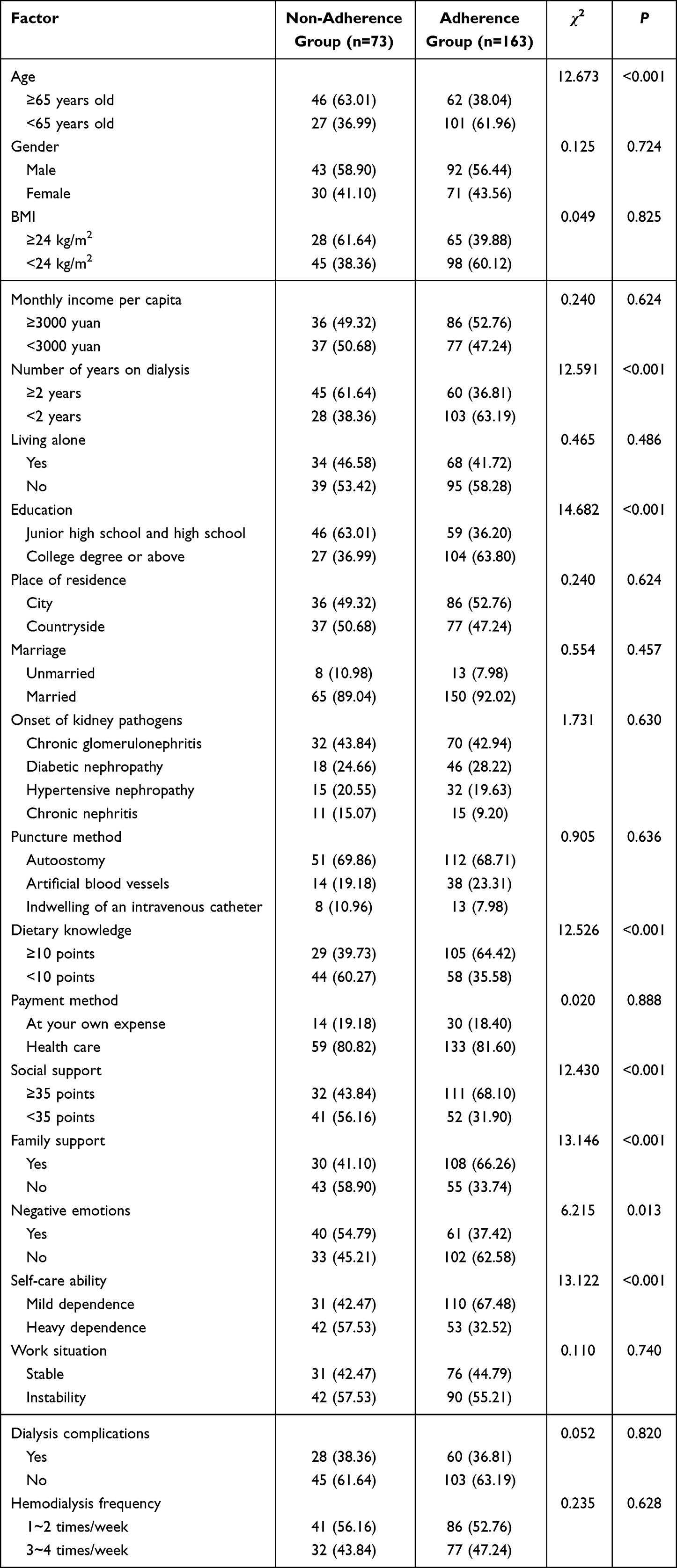 |
Table 1 Comparison of Clinical Data Between the Compliance Group and the Non-Compliance Group in the Modeling Group |
Lasso-Logistic Regression Analysis of Influencing Factors for Dietary Adherence in HD Patients
In the modeling group, with dietary adherence of HD patients as the dependent variable (Yes=1, No=0), and the factors with significant differences from Table 1—age (≥65 years=1, <65 years=0), duration of dialysis (≥2 years=1, <2 years=0), education level (junior high and high school=1, college and above=0), dietary knowledge (≥10 points=0, <10 points=1), social support (≥35 points=0, <35 points=1), family support (Yes=0, No=1), negative emotions (Yes=1, No=0), and self-care ability (severe dependence=1, mild dependence=0)—as independent variables, Lasso analysis was performed using R software. The results showed that when the penalty coefficient λ=0.0265474, the model performance was optimal, and seven predictive factors were selected: age, duration of dialysis, education level, dietary knowledge, social support, family support, and self-care ability. See Figure 2. Variance inflation factors (VIFs) among all factors were analyzed through multicollinearity testing, and all VIFs were <10, indicating no significant interaction effects. The seven independent variables selected by Lasso regression were included in a Logistic analysis (forward stepwise method), which showed that age, duration of dialysis, and self-care ability were risk factors for dietary non-adherence in HD patients (P < 0.05), while education level, dietary knowledge, social support, and family support were protective factors (P < 0.05). See Table 2.
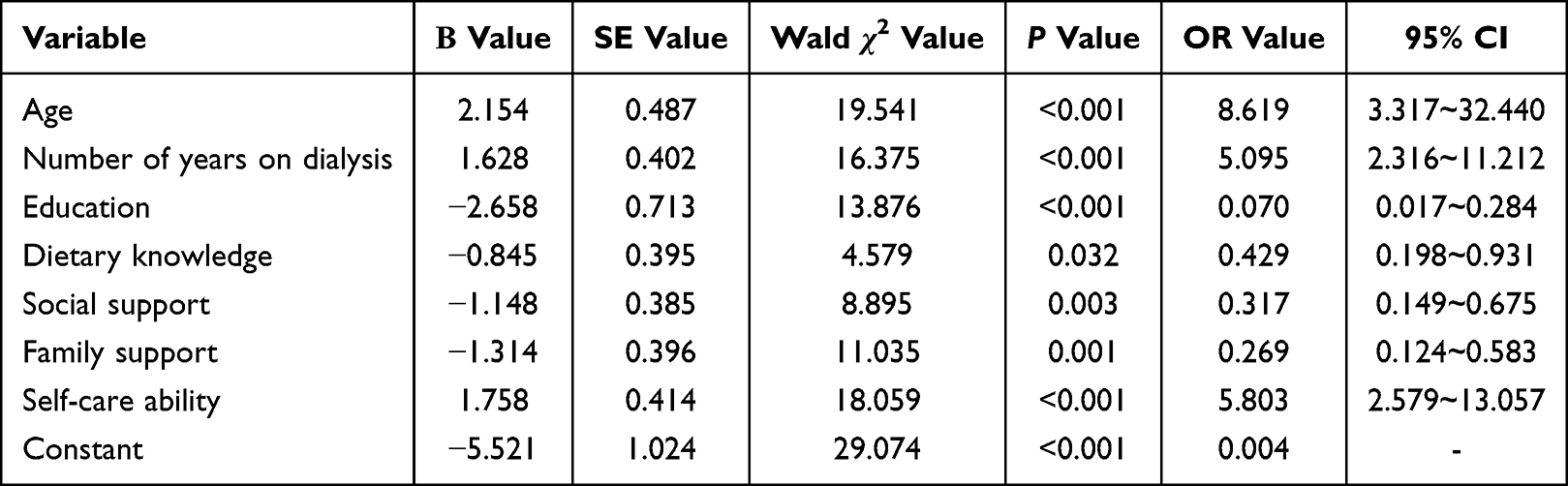 |
Table 2 Analysis of Influencing Factors of Dietary Behavior Compliance in HD Patients |
 |
Figure 2 Analysis of factors influencing dietary behavior adherence in hemodialysis patients using Lasso-logistic regression (A) Relationship diagram of Lasso regression coefficient; (B) Lasso regression 10-fold cross-validation results. |
Construction of a Nomogram Model for Dietary Adherence in HD Patients
A nomogram model was constructed based on the factors selected by the Lasso-Logistic regression analysis, with the formula:  , where x = −5.521 + 2.154×Age + 1.628×Duration_of_Dialysis - 2.658×Education_Level - 0.845×Dietary_Knowledge - 1.148×Social_Support - 1.314×Family_Support + 1.758×Self-care_Ability. In this model, the most important influencing factor was age. For example, a patient aged <60 years (0 points), with a dialysis duration ≥2 years (53.5 points), education level of junior high and high school (86.5 points), dietary knowledge <10 points (29.0 points), social support <35 points (37.5 points), no family support (43.5 points), and mild dependence in self-care (0 points), has a total score of 250 points. A vertical line is drawn down from this total score, yielding a predicted probability of 82%. See Figure 3.
, where x = −5.521 + 2.154×Age + 1.628×Duration_of_Dialysis - 2.658×Education_Level - 0.845×Dietary_Knowledge - 1.148×Social_Support - 1.314×Family_Support + 1.758×Self-care_Ability. In this model, the most important influencing factor was age. For example, a patient aged <60 years (0 points), with a dialysis duration ≥2 years (53.5 points), education level of junior high and high school (86.5 points), dietary knowledge <10 points (29.0 points), social support <35 points (37.5 points), no family support (43.5 points), and mild dependence in self-care (0 points), has a total score of 250 points. A vertical line is drawn down from this total score, yielding a predicted probability of 82%. See Figure 3.
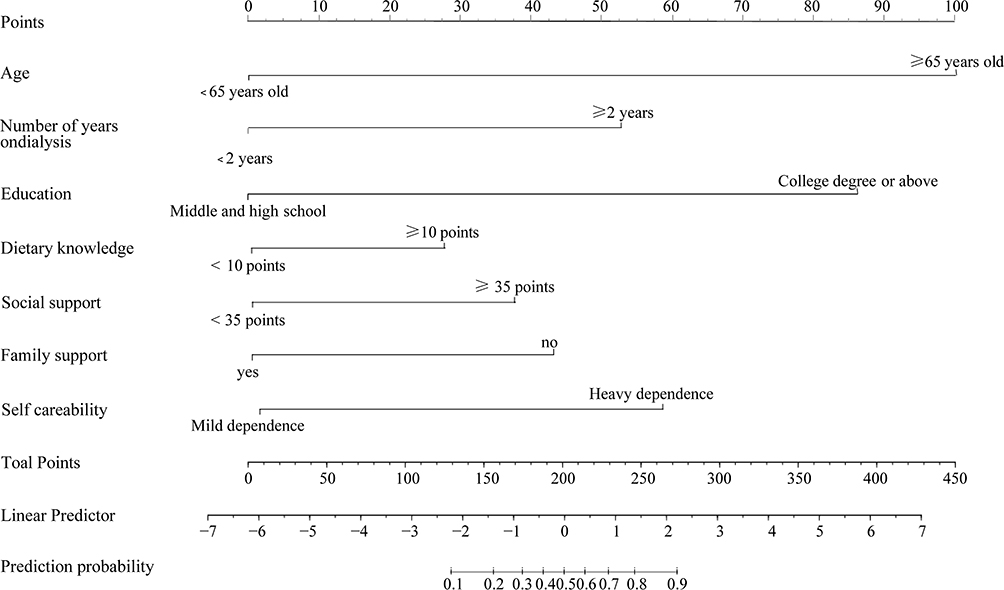 |
Figure 3 A nomogram model of dietary behavior compliance in HD patients was constructed. |
Internal Validation of the Nomogram Model for Dietary Adherence in HD Patients
The AUC of the ROC curve for internal validation was 0.884 (95% CI = 0.838–0.930). The Hosmer-Lemeshow (H-L) test showed good consistency, with χ2=7.346 (P=0.713). See Figure 4.
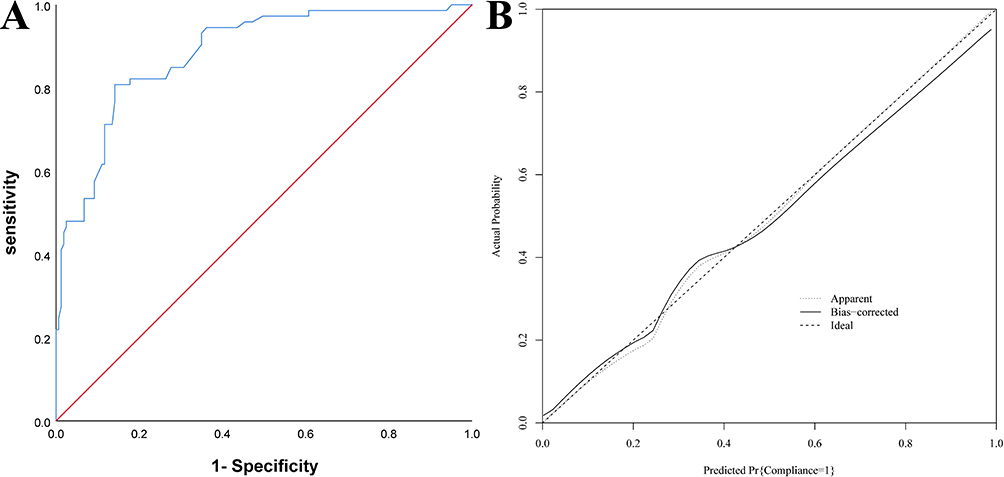 |
Figure 4 Internal validation of the nomogram predicting dietary behavior adherence in hemodialysis (HD) patients (A) ROC curves; (B) Calibration curves. |
Internal Validation of the Nomogram Model’s DCA Curve
The DCA curve results showed that when the threshold probability was between 0.10 and 0.83, the nomogram had high clinical application value for assessing dietary adherence in HD patients. See Figure 5.
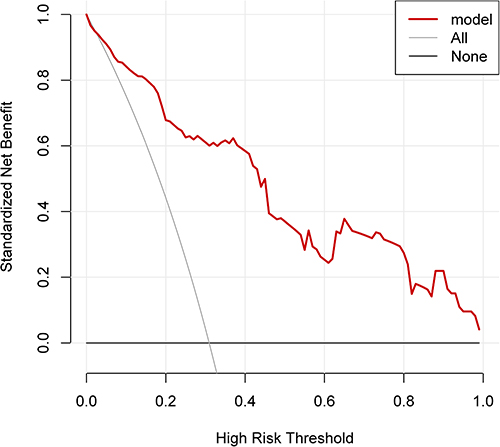 |
Figure 5 DCA curve of the nomogram model in internal validation. |
Comparison of Clinical Data Between the Dietary Non-Adherence and Adherence Groups in the Validation Group
Among the 121 patients in the validation group, 41 (33.88%) had dietary non-adherence. There were significant differences in age, duration of dialysis, education level, dietary knowledge, social support, family support, and self-care ability between the non-adherence and adherence groups (P < 0.05), with no significant differences in other data (P > 0.05). See Table 3.
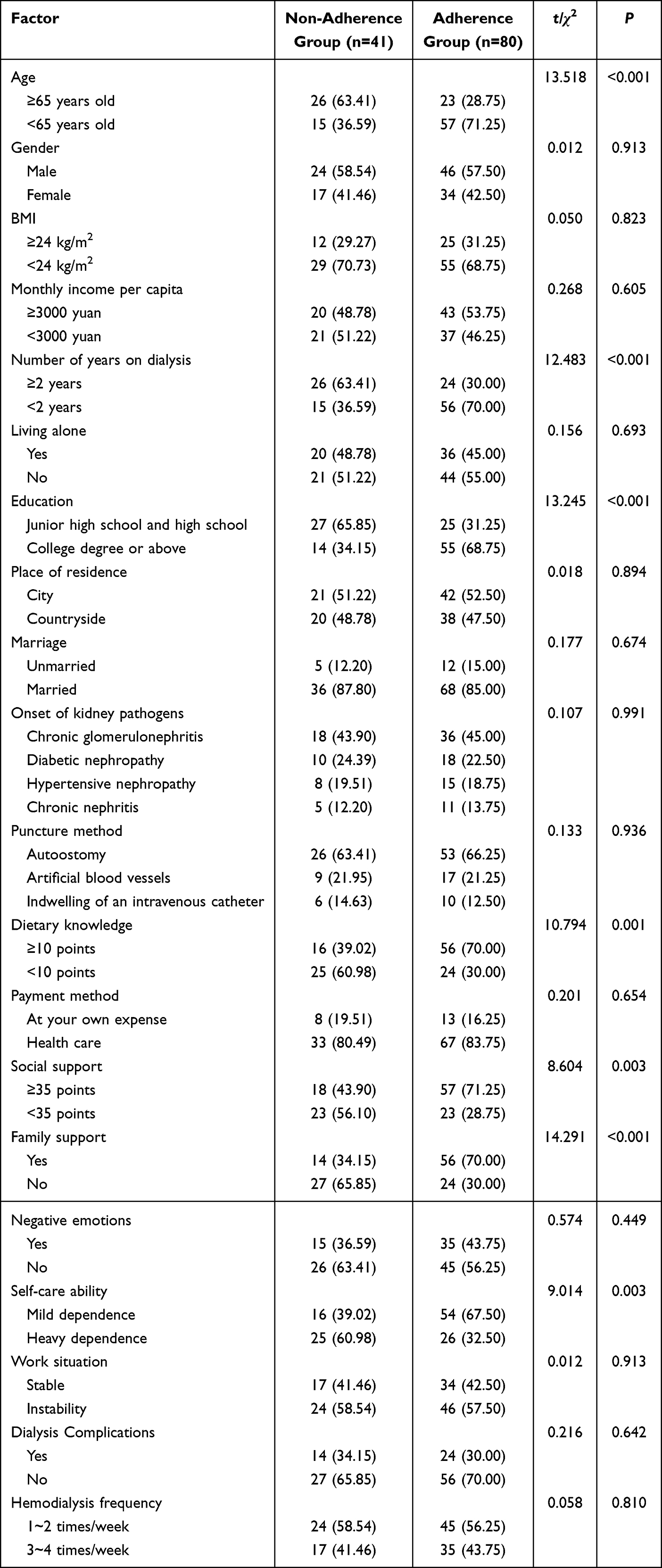 |
Table 3 The Clinical Data of the Validation Group Were Compared Between the Non-Compliance Group and the Compliance Group |
External Validation of the Nomogram Model for Dietary Adherence in HD Patients
The AUC of the ROC curve for external validation was 0.902 (95% CI = 0.839–0.965). The H-L test showed good consistency, with χ2=7.342 (P=0.726). See Figure 6.
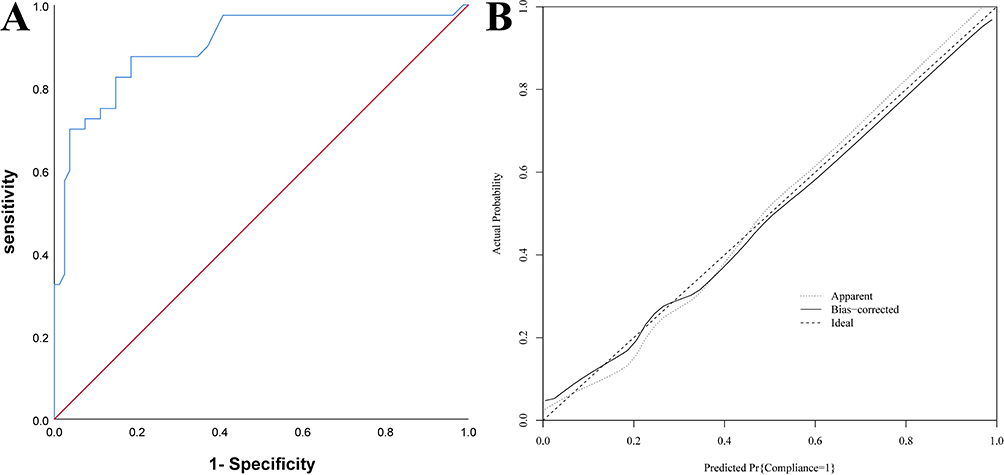 |
Figure 6 External validation of the nomogram model for dietary behavior adherence in hemodialysis (HD) patients (A) ROC curves; (B) Calibration curves. |
External Validation of the Nomogram Model’s DCA Curve
The DCA curve results showed that when the threshold probability was between 0.15 and 0.84, the nomogram had high clinical application value for assessing dietary adherence in HD patients. See Figure 7.
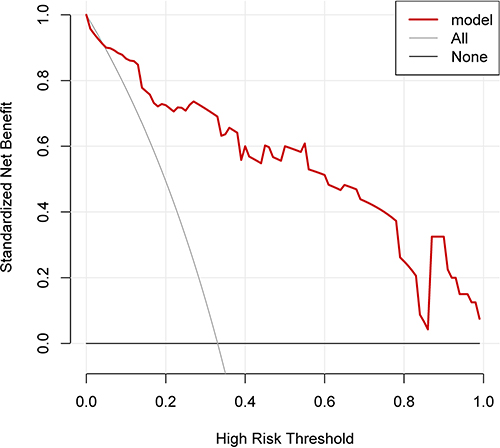 |
Figure 7 DCA curve of the nomogram model in external validation. |
Discussion
HD is a replacement therapy for patients with end-stage kidney disease. Dialysis can substitute for some of the kidney’s filtration function, clearing waste products generated from the metabolism of dietary intake. Due to its limited regulatory function, patients often experience severe problems such as electrolyte disturbances and malnutrition. These dialysis-related complications are closely related to the patient’s dietary intake, so paying attention to the dietary management of dialysis patients is very important.11,12 HD patients need to follow a specific diet to control electrolyte levels in their blood, but worldwide, dietary adherence among HD patients is not ideal. This has been confirmed in various countries, with approximately 50% of patients being non-adherent. Non-adherent patients often suffer from conditions like hyperphosphatemia and hyperkalemia, which seriously threaten their health.13,14 This study found that dietary adherence in both groups was not optimistic; therefore, improving patient dietary adherence is crucial for improving patient prognosis.
The results of this study found that 7 influencing factors were screened out through Lasso-Logistic analysis. The reasons are analyzed as follows: (1) With increasing age, patients may have more health problems, such as memory decline and hearing loss, which can affect their understanding of dietary guidance.15 Therefore, it is important to inform family members about the importance of companionship to supervise the patient’s diet and improve adherence. (2) Long-term dialysis can cause patients to become weary of dietary management. Furthermore, an increased duration of dialysis can lead to a decline in the patient’s physical condition and self-care ability, making it difficult to adhere to dietary restrictions amidst ongoing health challenges, thus affecting their dietary adherence.16 Therefore, nursing staff should strengthen health education for long-term dialysis patients and guide family members to show more care, encouragement, and support to alleviate the patient’s psychological stress and improve adherence. (3) Education level and lack of dietary knowledge also have a significant impact on patient adherence. Patients with higher education levels have a better understanding of their disease and can recognize the importance of dietary control in managing their condition. However, patients with lower education levels lack relevant knowledge and are susceptible to misinformation, leading to cognitive biases. This can also cause them to misunderstand or not follow dietary advice, as they may not be familiar with high-potassium and high-phosphorus foods or know how to meet their nutritional balance needs, affecting dietary adherence.17–19 Therefore, it is recommended that nursing staff popularize relevant knowledge for patients with lower education levels, improve their disease awareness, and assist in creating corresponding dietary plans to enhance dietary adherence. (4) Patients with good social support have access to better social resources, can learn about their disease, and receive external support. However, those with low social support have fewer social resources and find it difficult to get external help, which can affect their motivation and lead them to cope with treatment through avoidance, impacting treatment adherence.20 Therefore, medical staff can broaden patients’ social channels through organized communication sessions to compensate for the lack of social support. (5) Family support can help supervise and encourage patients to follow their dietary plan. A lack of family support can negatively affect patients’ dietary management, reducing dietary adherence.21 Therefore, family members can be encouraged to provide psychological and spiritual support, making patients feel warmth and improving dietary adherence. (6) Patients with poor self-care ability are more likely to develop resistance and avoidance psychology, which may lead to fewer medical visits and reduced motivation for treatment, thereby lowering dietary adherence.22,23 Therefore, medical staff can provide relevant education to family members, instructing them to offer necessary support so that patients can face their disease and establish good, healthy dietary habits under the guidance of doctors and family.
Studies have found that a nomogram model for medication adherence in chronic kidney disease patients, constructed based on five factors, showed good agreement between predicted probabilities and actual observed probabilities by the Hosmer–Lemeshow (H-L) test, and can be incorporated into long-term medication management.24 Another study constructed a nomogram prediction model for non-adherence in patients receiving phototherapy, in which Lasso regression identified seven predictive factors; the nomogram demonstrated good discriminative ability and calibration, and decision curve analysis (DCA) indicated favorable net benefit, supporting its clinical utility.25 In this study, a nomogram model was constructed based on Lasso regression and Logistic analysis. The AUCs for the training set and external validation were 0.884 and 0.902, respectively, and the H-L test showed good consistency. The threshold probabilities of the DCA curves for the modeling and validation groups were in the ranges of 0.10–0.83 and 0.15–0.84, respectively, indicating that this nomogram model demonstrates relatively high clinical value, consistent with previous studies. The nomogram we developed can help clinicians identify HD patients at high risk of non-adherence early. Additionally, this predictive tool can be applied in clinical trials to guide researchers in selecting patients with poor dietary adherence. Furthermore, the nomogram can support early interventions for high-risk non-adherent patients, which may include encouraging the use of automatic reminders and monitoring dietary adherence, thereby assisting healthcare providers in timely management of HD patients’ dietary behaviors and effectively improving their quality of life.
In summary, age, duration of dialysis, education level, dietary knowledge, social support, family support, and self-care ability are influencing factors for dietary adherence in HD patients, and the nomogram model constructed based on these variables demonstrated good discriminative ability and high clinical net benefit. It can assist healthcare providers in identifying HD patients at high risk of non-adherence at the beginning of clinical management, enabling individualized assessment of dietary adherence. This study is a retrospective, single-center study with a relatively small sample size, which may introduce bias, and further studies with larger, multi-center, and prospective designs are warranted for external validation.
Data Sharing Statement
The datasets used during the present study are available from the corresponding author upon reasonable request.
Ethics
The study was approved by the Ethics Committee of Ganzhou People’s Hospital, Jiangxi, China (Approval No. TY-ZKY2025-114-07). All procedures involving human participants were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their inclusion in the study.
Funding
There is no funding to report.
Disclosure
There are no conflicts of interest declared by the authors.
References
1. Loutradis C, Sarafidis PA, Ferro CJ, et al. Volume overload in hemodialysis: diagnosis, cardiovascular consequences, and management. Nephrol Dial Transplant. 2021;36(12):2182–2193. doi:10.1093/ndt/gfaa182
2. Arad M, Goli R, Parizad N, et al. Do the patient education program and nurse-led telephone follow-up improve treatment adherence in hemodialysis patients? A randomized controlled trial. BMC Nephrol. 2021;22(1):119. doi:10.1186/s12882-021-02319-9
3. Bleyer AJ. Factors that lead to dialysis as the preferred treatment modality for patients with chronic kidney disease. Curr Opin Nephrol Hypertens. 2022;31(2):180–184. doi:10.1097/MNH.0000000000000772
4. Tian X, X Xia, Yu H, et al. Cognitive dysfunction and its risk factors in patients undergoing maintenance hemodialysis. Neuropsychiatr Dis Treat. 2022;18:2759–2769. doi:10.2147/NDT.S380518
5. Wang Y, Y Yao, Hu J, et al. Development of a predictive nomogram for estimating medication nonadherence in hemodialysis patients. Med Sci Monit. 2022;28:e934482. doi:10.12659/MSM.934482
6. Chen J, Shen C, H Xue, et al. Development of an early prediction model for vomiting during hemodialysis using LASSO regression and Boruta feature selection. Sci Rep. 2025;15(1):10434. doi:10.1038/s41598-025-95287-1
7. Cicolini G, Palma E, Simonetta C, et al. Influence of family carers on haemodialyzed patients’ adherence to dietary and fluid restrictions: an observational study. J Adv Nurs. 2012;68(11):2410–2417. doi:10.1111/j.1365-2648.2011.05935.x
8. Račić M, Petković N, Bogićević K, et al. Comprehensive geriatric assessment: comparison of elderly hemodialysis patients and primary care patients. Ren Fail. 2015;37(7):1126–1131. doi:10.3109/0886022X.2015.1057459
9. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
10. Mahoney FI, Barthel DW. Functional evaluation: the barthel index. Md State Med J. 1965;14:61–65.
11. Hu EA, Coresh J, Anderson CAM, et al. Adherence to healthy dietary patterns and risk of CKD progression and all-cause mortality: findings from the CRIC (chronic renal insufficiency cohort) study. Am J Kidney Dis. 2021;77(2):235–244. doi:10.1053/j.ajkd.2020.04.019
12. Palmer BF. Potassium binders for hyperkalemia in chronic kidney disease-diet, renin-angiotensin-aldosterone system inhibitor therapy, and hemodialysis. Mayo Clin Proc. 2020;95(2):339–354. doi:10.1016/j.mayocp.2019.05.019
13. Vijay VR, Kaur Kang H. The worldwide prevalence of nonadherence to diet and fluid restrictions among hemodialysis patients: a systematic review and meta-analysis. J Ren Nutr. 2022;32(6):658–669. doi:10.1053/j.jrn.2021.11.007
14. Basaleem HO, Alwan SM, Ahmed AA, et al. Assessment of the nutritional status of end-stage renal disease patients on maintenance hemodialysis. Saudi J Kidney Dis Transpl. 2004;15(4):455–462.
15. Fotaraki Z-M, Gerogianni G, Vasilopoulos G, et al. Depression, adherence, and functionality in patients undergoing hemodialysis. Cureus. 2022;14(2):e21872. doi:10.7759/cureus.21872
16. Tsuruya K, Arima H, Iseki K, et al. Association of dialysis-related amyloidosis with lower quality of life in patients undergoing hemodialysis for more than 10 years: the Kyushu Dialysis-Related Amyloidosis Study. PLoS One. 2021;16(8):e0256421. doi:10.1371/journal.pone.0256421
17. H Kim, Jeong IS, Cho M-K. Effect of treatment adherence improvement program in hemodialysis patients: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022;19(18):11657.
18. Alhamad MA, Almulhim MY, Alburayh AA, et al. Factors affecting adherence to hemodialysis therapy among patients with end-stage renal disease attending in-center hemodialysis in Al-Ahsa Region, Saudi Arabia. Cureus. 2023;15(10):e46701. doi:10.7759/cureus.46701
19. Hussain F, Ashraf S, Arshad M, et al. Knowledge, adherence, and perception of patients on maintenance hemodialysis to treatment regimens at a tertiary care hospital in Pakistan. Cureus. 2023;15(12):e51341. doi:10.7759/cureus.51341
20. Alatawi AA, Alaamri M, Almutary H. Social support and adherence to treatment regimens among patients undergoing hemodialysis. Healthcare. 2024;12(19):1958. doi:10.3390/healthcare12191958
21. Li B, P Cai, Zhao X, et al. Factors associated with stigma in patients undergoing hemodialysis: a meta-analysis and systematic review. Am J Transl Res. 2024;16(8):3498–3509. doi:10.62347/SRIC1173
22. Ma L-C, Liu Y-M, Lin Y-C, et al. Factors influencing self-management behaviors among hemodialysis patients. J Pers Med. 2022;12(11):1816. doi:10.3390/jpm12111816
23. Li J, Lin Y, Wang L, et al. Analysis of the application effect of the Clark comfortable nursing approach in hemodialysis patients with end stage renal failure. Ren Fail. 2024;46(2):2423011. doi:10.1080/0886022X.2024.2423011
24. Wu X, Tang F, Li H, et al. Development and validation of a nomogram model for medication non-adherence in patients with chronic kidney disease. J Psychosom Res. 2023;171:111385. doi:10.1016/j.jpsychores.2023.111385
25. Zhang Y. Predicting risk of treatment non-adherence in patients receiving intense light therapy: development and evaluation of a new predictive nomogram. Lasers Med Sci. 2025;40(1):268. doi:10.1007/s10103-025-04524-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of Prediction Models for All-Cause Mortality and Cardiovascular Mortality in Patients on Hemodialysis: A Retrospective Cohort Study in China
Yang M, Yang Y, Xu Y, Wu Y, Lin J, Mai J, Fang K, Ma X, Zou C, Lin Q
Clinical Interventions in Aging 2023, 18:1175-1190
Published Date: 28 July 2023
Factors related to the occurrence of fetal birth defects and the construction of a Nomogram model
Chen X, Lin L, Zhong Q, Wu H, Zheng Z, Zhang B, Lan L
Pediatric Health, Medicine and Therapeutics 2024, 15:289-298
Published Date: 9 September 2024
Influencing Factors (History of Alcohol Consumption) and Construction of a Nomogram Prediction Model for In-Hospital Gastrointestinal Bleeding Secondary to Acute Cerebral Hemorrhage in a Certain Hospital
Ye P, Luo Y
Risk Management and Healthcare Policy 2025, 18:1557-1568
Published Date: 11 May 2025
Construction of a Nomogram Prediction Model for Individualized Prediction of the Risk of Pulmonary Fungal Infection in Lung Cancer
Lai Q, Liao K, Kuang G, Liao W, Zhang S
Infection and Drug Resistance 2025, 18:3137-3147
Published Date: 26 June 2025
Factors Influencing Cardiac Rehabilitation Compliance in Elderly Myocardial Infarction Patients and the Development of a Nomogram Prediction Model
Zhou B, Yan J, Wang Q, He Q, Ao W, Yang Y, Ren Y
Patient Preference and Adherence 2025, 19:2015-2025
Published Date: 11 July 2025