Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Developing a Core Outcome Set for Herpes Zoster-Associated Neuralgia in Clinical Trials of Traditional Chinese Medicine: A Study Protocol
Authors Wang J, Jutaputthi T, Cheng Y, Ye Z, Xu M ![]() , Wu Y
, Wu Y ![]() , Jin Z
, Jin Z
Received 16 August 2025
Accepted for publication 23 December 2025
Published 14 January 2026 Volume 2026:19 561192
DOI https://doi.org/10.2147/JMDH.S561192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Judith Johnson
Junyi Wang,1 Tanundorn Jutaputthi,1 Yuanyuan Cheng,1 Ziqi Ye,1 Moran Xu,1 Yuanyuan Wu,1,2 Zongda Jin1,2
1The Third Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Yuanyuan Wu, Email [email protected] Zongda Jin, Email [email protected]
Context: Herpes zoster-associated neuralgia (ZAN), the most common symptom across all stages of herpes zoster, significantly impacts patients’ quality of life and emotional well-being. Traditional Chinese Medicine (TCM) treatments have demonstrated unique efficacy in treating ZAN. However, non-standardized outcome reporting remains a significant challenge. Therefore, establishing a core outcome set (COS) is essential for standardizing TCM clinical research on ZAN.
Objective: This study aims to develop a COS for future clinical trials of TCM for ZAN (COS-TCM-ZAN).
Methods: This study determined the list of outcomes measures by systematically searching databases and clinical trial registeres. Subsequently, multiple stakeholder groups from various fields were selected to conduct two rounds of Delphi surveys to assess the importance of each outcome measure. Finally, we will hold a face-to-face consensus conference to approve the final COS-TCM-ZAN.
Timeline: The study will start in April 2025, aiming to finalize the outcomes list by June 2025. Then having stakeholder screening, a Delphi survey (July-Dec 2025), and a consensus conference in early 2026. In line with the COS-STAR (Core Outcome Set–STAndards for Reporting) guidelines, the COS findings will be reported and exchanged at national and international conference.
Conclusion: The standardized COS will enhance the identification of effective evaluation indicators for TCM treatment of ZAN, thereby enhancing the comparability and reproducibility in research and clinical practice for TCM in the field of ZAN treatment.
Trial Registration: This COS has been prospectively registered in the COMET database (registration #3370, available at https://www.comet-initiative.org/studies/details/3370). Clinical trial number: not applicable.
Keywords: herpes zoster-associated neuralgia, traditional Chinese medicine, core outcome set
Introduction
Herpes Zoster (HZ) is a disorder of nerve tissue. The disease is caused by the reactivation of the human varicella-zoster virus (VZV) dormant within the dorsal root ganglia (DRG).1 The course of HZ can be divided into four stages: pre-eruptive, acute exudative, subacute and postherpetic neuralgia (PHN).2 Globally, the incidence of HZ has been increasing over time.3 For the global population aged ≥70, the number of HZ cases increased from 2,189,406 in 1997 to 4,539,519 in 2021. Meanwhile, the incidence rate rose from 888.0 to 918.2 per 100,000 population.4 Herpes zoster-associated neuralgia (ZAN) is a common feature of HZ and is usually described as aching, burning or stinging in quality.5 ZAN is known to have an adverse effect on health-related quality of life, including physical and emotional functioning.6
ZAN appears to occur in each stage. There are roughly three stages of ZAN: acute pain phase, subacute pain phase, and post-herpetic neuralgia(PHN) phase. Pain that appears within a month is the acute pain stage. Any pain that takes 30–90 days for the rash healing is the subacute pain phase. When the pain remains for over three months or even years, the long-term condition is known as PHN.7–9 It is the most common complication of shingles. Greater acute pain severity stands as a risk factor for PHN.10 Adequate pain control is important in HZ. Effective treatment and management of HZ may lessen the risk of the transition to chronic PHN.11 The incidence of PHN in patients with HZ is as high as 29.8%.12 This risk increases sharply with advancing age among the elderly.6,7 China is experiencing a profound demographic shift as its population rapidly ages. Therefore, ZAN is still one of the complicated diseases affecting human health.
Western Medicine treatment of ZAN mainly includes pain management strategies and symptom control. Medications such as antivirals, tricyclic antidepressants, antiepileptic drugs, opioids, and local analgesics are the mainstream therapy for ZAN.13 The effective responses observed in clinical use have been often limited by concerns regarding long-cycles regimens and adverse drug reactions.14–17
Traditional Chinese medicine (TCM) is a well-established medicine with a long history in China.18 TCM has accumulated rich experience in ZAN treatment. Practical approaches involve orally administered medicinal formulas, medicinal powder, acupuncture, and moxibustion therapies. TCM can hasten the resolution of pain and decrease the incidence, duration, and severity of chronic pain. Furthermore, TCM formulas act as an antiviral agent to combat the pathological condition.19–21 At the onset of HZ infection, earlier TCM interventions lead to greater benefits. The use of TCM could achieve the purpose of treating both the symptoms and root causes and improve the prognosis and life quality in patients with ZAN.
The core competitiveness of TCM should reply on solid clinical efficacy evidence. However, high-quality evidence is lacking at present.22 The research finds that the current selection of outcome indicators in similar TCM studies is highly heterogeneous and suffers from a lack of standardization, rationality, and comprehensiveness.23–25 As a method of ZAN treatment, TCM is further supported by the growing number of clinical trials.26 However, there has been a risk of inconsistency and outcome reporting bias in relevant studies. For instance, some outcome indicators appear to be not as important or practical as they could be.27 In particular, the existing studies about PHN suggested a lack of standards to measure changes in TCM syndromes.28 The need for better evidence synthesis and direct comparisons across research studies is a challenge. Systematic evaluations not only fail to accurately reflect the effectiveness of TCM treatment but also cannot effectively guide clinical-decision making.29 Therefore, we need to construct a relatively standardized outcome assessment to minimize the negative impact of these findings. This can be achieved by the development of a core outcome set (COS). This essential set is designed to meet the needs of clinical studies exploring TCM’s approaches to ZAN relief.
A COS is a uniform and standardized minimum set of indicators that must be measured and reported in clinical studies for a specific disease.20,21 A COS is based on consensus to facilitate the synthesis of evidence and improve consistency of outcome reporting in disease management or prevention.19 A COS can provide a reference for clinical research, improve the quality of research and reduce the cost of research design.30 It is widely recognized that the study on COS has been increasing and has been widely recognized.31,32
In China, TCM has been carried out for thousands of years for health maintenance and disease treatment.33 The usage of TCM-related interventions is widespread in the treatment of pain conditions, such as post-surgical pain, neuropathic pain, and musculoskeletal pain.34 TCM relies on unique theories and practices. There is an urgent need for an evaluation system in line with the characteristics and advantages of TCM to improve the value of trials in TCM.
The Core Outcome Measures in Effectiveness Trials (COMET) initiative was founded in 2010 and was devoted to fostering the development of COS.35 Neuropathic pain varies greatly under different conditions. At present, there are two neuropathic pain-related COSs for clinical studies in the COMET database. The COS of diabetic neuropathy is still ongoing and has not yet been published (https://www.comet-initiative.org/Studies/Details/2461). The COS of trigeminal neuralgia recommended 11 mandatory outcome measurements, which respectively addressed pain, side effects, social impact, quality of life, global improvement, and satisfaction with treatment domains.28 No ongoing or completed COS registration information has been identified for TCM in neuropathic pain associated with HZ. The present COS will focus only on TCM interventions for adults with ZAN. Candidate outcomes will be aligned to four disease stages and aggregated into seven core domains: clinical manifestations, TCM-specific syndrome, quality of life, physical and chemical examination, economic assessment, prognosis and side effects. This COS is intended for adults without major comorbidities those who receiving any TCM intervention for ZAN and should be applied in RCTs and observational studies. Therefore, a COS for clinical trials of TCM for ZAN disease is of great value in meeting clinical research demands.
Study Objective
To systematically review the existing literature and clinical trials on the TCM-related intervention of ZAN. To collect additional information from clinicians, patients following ZAN, and caregivers and identify the outcome not reported in the scientific literature. To generate a comprehensive inventory of outcome indicators and undertake a Delphi questionnaire. To reach a consensus on a formal outcome set for ZAN using TCM by a Delphi survey and a face-to-face consensus conference with all key stakeholders. To promote and disseminate the COS in the clinical trials of TCM for ZAN (COS-TCM-ZAN).
Scope
The health condition for this study is ZAN. Patients with ZAN 18 years of age or older will be included without other complications. This COS will cover all TCM-related interventions, including traditional Chinese medicine decoction, proprietary Chinese medicine (with proprietary ingredients), external Chinese medicine, and external Chinese treatment. It is anticipated that the COS-TCM-ZAN will be implemented for all future studies, including randomized controlled trials (RCTs), cohort studies and case-control studies.
Preliminary Preparation
Steering Committee
A steering committee, which will be composed of six experts, three TCM and two Western medicine clinical experts in the field of ZAN and a methodologist, is responsible for decision-making, such as confirming the research plan, providing guidance as well as settling the disagreements during the process.
Working Group
A working group will be composed of ten members, including TCM clinicians, Western medicine clinicians, methodologists, and COS researchers. The main tasks of the working group consist of distributing questionnaires and statistical results and holding meetings to seek advice from the steering committee to resolve the differences.
Methods
This COS has been prospectively registered in the COMET database (registration #3370, available at https://www.comet-initiative.org/studies/details/3370). A comprehensive and systematic review of registered clinical trials and published literature will be conducted.36 Two clinical trial registration databases will be chosen to retrieve (www.chictr.org.cn; Clinicaltrials.gov). Meanwhile, semi-structured interviews with patients and a questionnaire survey with clinicians will be conducted. So a comprehensive outcomes pool will be established. Then, the expert consensus will be formed and the COS is constructed by Delphi. To develop COS, the following interlinked four stages will be sequentially addressed (Figure 1).
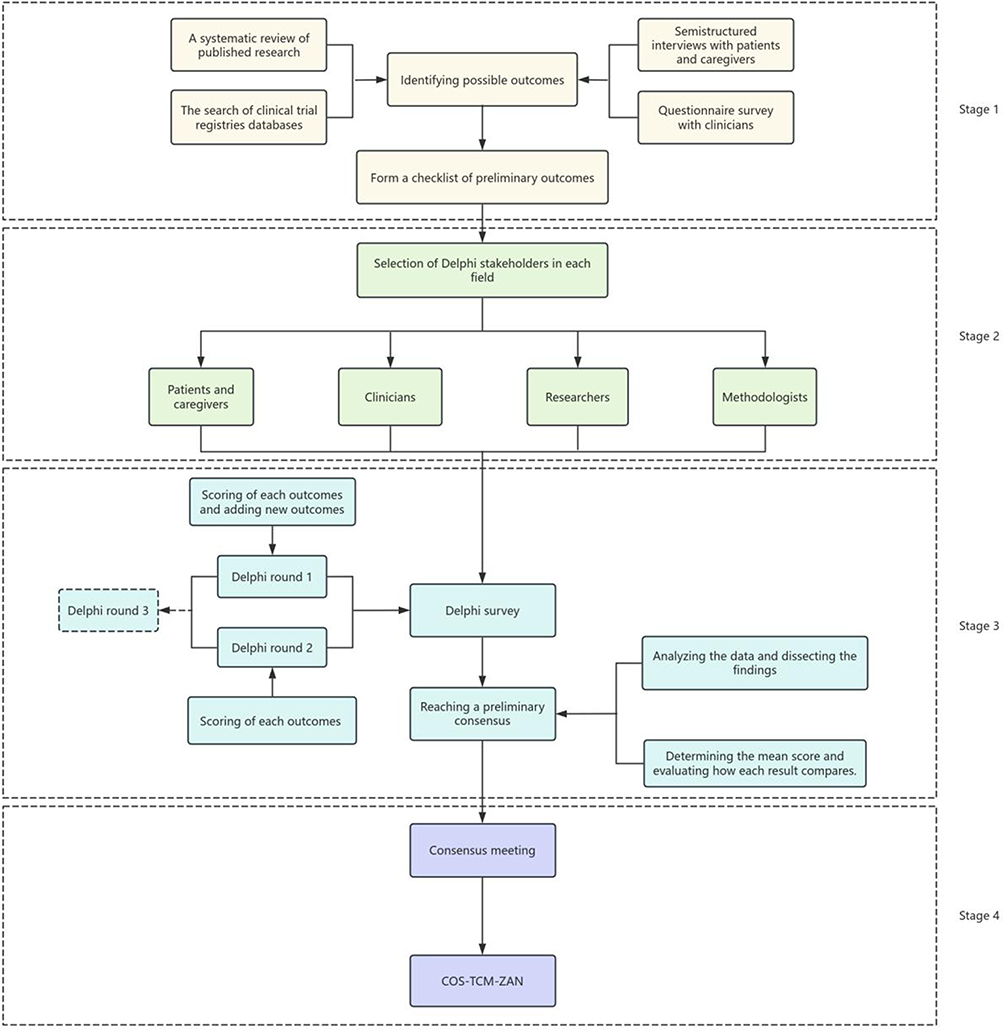 |
Figure 1 Flowchart of developing core outcome set of the clinical trials of TCM for ZAN. Abbreviations: COS, core outcome set; TCM, traditional Chinese medicine; ZAN, Herpes zoster-associated neuralgia. |
Stage 1. Identifying potential outcomes and generating an outcome list.
Stage 2. Screening stakeholder groups in various fields for the Delphi survey.
Stage 3. Conducting two rounds Delphi surveys to determine the importance of outcomes.
Stage 4. Holding a face-to-face consensus conference to approve the final COS-TCM-ZAN.
Stage 1. Identifying Possible Outcomes
We will perform a comprehensive systematic review by exploring both databases and clinical trial registration centers both in China and in other countries. Semi-structured interviews with patients and caregivers will be conducted concurrently with the administration of questionnaire surveys to clinicians.37–39 The reporting indicators will be classified according to the course of HZ, including pre-eruptive, acute, subacute and chronic stage. The number and frequency of outcome indicators will be counted, and duplicates will be eliminated to form a relatively complete index pool for TCM clinical research on ZAN. The working group will standardize and classify the original item pool. Then a preliminary list of outcome indicators will be formed for clinical research of TCM treatment of ZAN.
Step 1. A Systematic Review of Published Research
Search Strategy
The following electronic databases will be searched: China National Knowledge Infrastructure, Wanfang Database, SinoMed and VIP information resource integration service platform database, PubMed, Cochrane Library, EMbase, Web of Science (a total of eight Chinese and English literature databases). The search is restricted to the interval from the database’s completion to 2025 and limited to English and Chinese languages. The search strategy is shown in Supplementary File 1.
Eligibility Criteria
The criteria for including and excluding published articles will be outlined in Table 1.
 |
Table 1 The Inclusion and Exclusion Criteria for Published Articles |
Data Processing and Analysis
Two reviewers will screen the title and abstract of the article according to inclusion and exclusion criteria. Then the full text for another review. If two reviewers disagree, a third reviewer is consulted. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart will be presented, including the number of selected and excluded studies and the reasons for exclusion. The collected data will include: (1) Basic details of the research, including the title, the name of the first author, publication date, author’s field of expertise. (2) Baseline characteristics of the study will consist of age, disease progression, sample size, and types of TCM syndromes (including syndrome, symptoms, tongue, and pulse). (3) Intervention details will cover the name of the intervention, duration of treatment, treatment frequency, and dosage. (4) Outcome names or definitions, measurement techniques, and time points of measurement will all be included.40
The extracted data are categorized according to the stages of ZAN occurrence, that is,pre-eruptive, acute, subacute and chronic stages.
Step 2. The Search of Clinical Trial Registry Databases
Search Strategy
We will search for clinical trials of ZAN that have been registered in the two major clinical trial registries: the Chinese Clinical Trial Registry (www.chictr.org.cn) and the US Clinical Trial Database (clinicaltrials.gov). The search period will span from inception to 2025, with the following keywords as search terms: herpes zoster, zoster-associated neuralgia, postherpetic neuralgia, snake sore, snake Dan, girdling fire cinnabar, girdling snake cinnabar, snake strand sore and waist fire Dan.
Eligibility Criteria
TCM clinical trials for ZAN will be included. The inclusion and exclusion criteria are shown in Table 2.
 |
Table 2 The Inclusion and Exclusion Criteria for Clinical Trial |
Data Processing and Analysis
The collected information will include the country of the registered organization or researcher, the status of the registered trial, ethical clearance, source of funding, phase of the study, intervention details, description of outcomes, methods for measuring outcomes, and specific time points.
The classification for extracted data is the same as that in the previous systematic review.
Step 3. Semi-Structured Interviews with Patients and Questionnaire Surveys with Clinicians
It has become increasingly evident that prioritizing the patient is crucial in the process of defining a COS. Patients possess an inherent ability to perceive their condition, enabling them to more effectively assess the feasibility of evaluation indicators. To make the study more comprehensive, we will adopt a combination of Semi-structured interviews and questionnaires. We will recruit 30 ZAN patients over the age of 18 to conduct semi-structured interviews (patients with severe mental problems, communication difficulties, or other factors that may interfere with the development of the trial will be excluded).41,42 The significance of outcome indicators at the patient level is assessed during semi-structured interviews. To facilitate the understanding and participation of patients, the questionnaire provides guided index items. The questionnaire will be distributed through the website, mobile phone, email, and paper materials. Before the semi-structured interview, the trained members of the working group will explain the purpose of the study and ask if they want to participate in the study. Patients who agree to participate will complete both the informed consent form and the information form. They will be informed of their right to withdraw from the survey at any time. Patients will be asked to focus on what outcome indicators they consider more important at different stages of ZAN. The semi-structured interview outline and guided index items are shown in Table 3. With the completion of the semi-structured interview, the members of the working group will collate and evaluate the relevant data. To improve the validity of the study, all interviews will be conducted anonymously. Any atypical indicators mentioned will be thoroughly examined. These indicators will be reported and included in the results pool after deliberation by the steering committee.
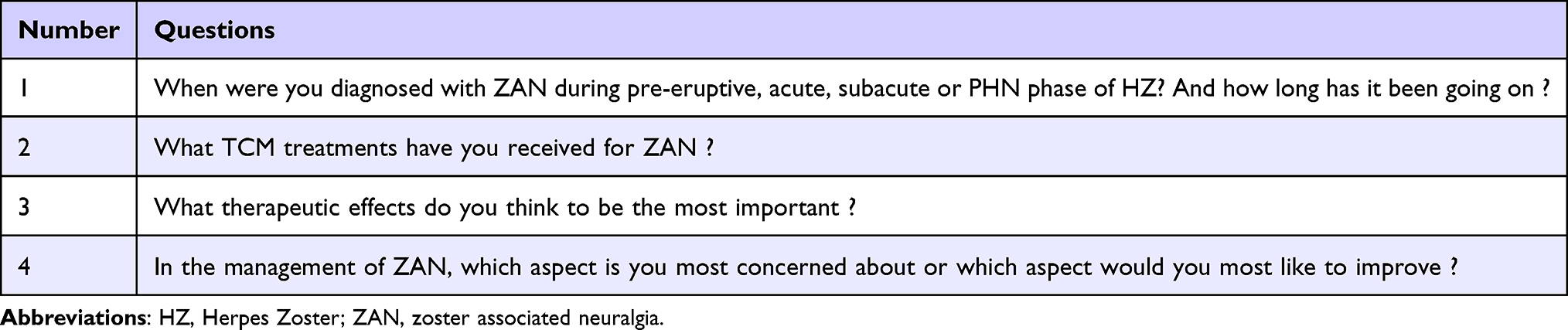 |
Table 3 The Semi-Structured Interviews Outline and Guided Index Items |
The main purpose of the semi-structured interviews is to generate patient-centered outcomes, identify the reason behind their selection, and determine their significance for the clinical assessment of ZAN. The Semi-structured interview is necessary for the establishment of a COS because it aligns with the clinical indicator investigation and helps to strengthen the overall framework.
On the other hand, we will invite 60 clinicians, with at least 3 years of clinical experience specializing in neurology, dermatology, and TCM to participate in the questionnaire survey.41,42 Before the start of the survey, the trained members of the working group will explain the purpose of the study and ask whether they consent to participate in the study. Clinicians who agree will complete the informed consent form and the information form. The questionnaire will be distributed through the website, mobile phone, email, and paper materials. With extensive experience in clinical treatment, clinicians are capable of providing practical clinical indicators based on their ongoing grasp of a patient’s health status and clinical judgment. To identify key clinical indicators and to broaden the scope of clinical outcome indicators, the questionnaire for clinicians is designed in an open format. Clinicians will be requested to list up to 5 outcome indicators that they consider important for each stage of ZAN.
Step 4. Form a Checklist of Preliminary Outcomes
The working group will classify and sort the data, which were collected through the aforementioned three approaches, based on the stages of ZAN. First, outcome indicators with the same definition but different expressions will be standardized. The quantity and frequency of outcome indicators used will be assessed, and any duplicates will be removed. Drawing on the functional attributes of the outcome, the initial outcome items will be categorized into seven outcomes domains: symptoms and signs, TCM disease syndrome, quality of life, physical and chemical examination, economic evaluation, long-term prognosis, and adverse events. The collected outcome indicators will be further classified and sorted to form a preliminary checklist of outcomes. The entries on the checklist will be ultimately reviewed and approved by the steering group for inclusion in the following Delphi.
Stage 2. Selection of Delphi Stakeholders in Each Field
The selection of stakeholders is crucial to establishing a COS. We will engage stakeholders from the following groups: clinicians, patients and caregivers, researchers, and methodologists. The majority of studies on the treatment of ZAN by TCM are domestically focused. Therefore, it is in line with the current research background that the stakeholders recruited in this study are within China. There is no consensus regarding fixed minimum sample size for conducting a Delphi survey. Instead, the sample size is not determined by statistical power calculations.30 For Delphi studies focusing on individual stakeholder groups (such as researchers, clinicians, patients), a sample size of 20 to 30 per group can generate reliable responses.43 With reference to previous Delphi surveys, we aim to enroll 100 participants, 25 from each of the four major stakeholders groups to ensure a balanced representation.44–47 Clinicians, such as experts of western medicine or TCM with specialization in neurology, dermatology and with more than 5 years of clinical experience, will be selected in tertiary hospitals. Patients diagnosed with ZAN having the ability of literacy and communication will be eligible. They come from the Zhejiang Chinese Medical University affiliated hospitals. Caregivers have been taking care of patients. Methodologists will be recruited from Tianjin University of Traditional Chinese Medicine evidence-based medicine center or Zhejiang Chinese Medical University. Researchers, including journal editors, COS developers and other related experts, will be recruited by searching high-impact published studies. An Email will be sent to potential participants explaining the content of the study and the significance of the Delphi survey. The Email also clarifies voluntary participation and that participants have the right to withdraw from the study at any time. A questionnaire link is included, and clicking the link constitutes agreement to the informed content. We expect that there will be a loss of participants across the rounds of the Delphi survey. Based on previous similar Delphi studies, our target retention rate is set at ≥70%. To minimize attrition as much as possible, we will adopt the following strategies: The questionnaire was maintained at an appropriate length. Participants were permitted to save their progress which will be automatically restored when they fill it out next time. Throughout the survey period, automated Email reminders were scheduled and dispatched following the initial invitation, with subsequent reminders sent one week prior to the deadline.
Stage 3. Delphi Survey and Reaching a Preliminary Consensus
The Delphi method is a group facilitation technique that is an iterative, multi-stage process designed to translate individual opinions into a collective consensus through two or three rounds until agreement is reached.48 The structured approach of the Delphi method to reach consensus among group members has gained acceptance in various medical fields.49,50 The Delphi questionnaire utilized in this study will be implemented on the ChiCOS website (https://chicos.org.cn/home). Stakeholders (excluding patients) will receive an electronic questionnaire, while patients will receive a paper questionnaire, and both will rate the outcome.A 9-point Likert Scale has been recommended by the COMET group to be widely used in the development of COS. It will be employed to assess the importance of each outcome.34 Each item on the scale is assigned a score from 1 to 9 and an additional option for “uncertain”. Scores from 1 to 3 denote “not important”, from 4 to 6 “important but not critical”, and from 7 to 9 “critical”, and the choice “uncertain” is for ambiguity (Table 4).
 |
Table 4 The 9-Point Likert Scale |
All submitted responses will be assessed against pre-defined completion criteria. Questionnaires in which participants have completed all the rating are deemed valid and will typically qualify the respondent for inclusion in subsequent round. Responses failing to meet this requirement are excluded from analysis and the individuals will not be re-invited. The investigators will Email participants at the end of the 2nd week, prompting them to finish the survey. To reduce attrition bias, if the response rate is less than 70%, we will offer a brief grace period for one more week. Those still unresponsive after 3 weeks will be classified as having dropped out. These data will be regarded as attrition data. The final study report will document the initial sample size, attrition rates per round, and an analysis of dropout characteristics to evaluate potential systematic bias caused by participant loss.
Pilot Survey
To ensure the clarity of the scale items, we will pilot the questionnaire using convenience sampling with 20 participant representives from Hangzhou, China.51,52 The participants represented four key stakeholder groups: clinicians, patients and caregivers, methodologies, and researchers. After completing the survey, they provided feedback on each item. Items identified as unclear were flagged for review and subsequently referred to a steering committee for discussion and revision.
Round 1
The candidate indicators will be included in the first round of the Delphi survey and will be sent out via a personalized Email through an online platform. For the Delphi round 1 questionnaire, a brief summary of the COS study will be presented to the participants. Both electronic and paper questionnaires are of the same version. All the outcomes must be scored using the Likert Scale provided above. To maintain the integrity of the outcomes, participants will have the opportunity to add other outcomes that they think are important but not on the outcome list. For the stakeholder group of patients, the face-to-face survey will be conducted by the trained members of the working group in the inpatient ward or outpatient department. The first round of the Delphi survey is planned to be completed within three weeks.
The working group will collect all the completed questionnaires and perform a summary analysis. Anonymous feedback will be provided, which includes the following parts: (1) the number of responses and participants, the average score of each item, and the score distribution of each outcome for different stakeholder group; (2) If over 70% of participants score an outcome between 4 and 9, it will be included in the next Delphi round; (3) newly added outcomes which the steering committee will review to determine whether to retain to the next round.
Round 2
All participants who completed the first round will be invited to join the second round of Delphi. Response rate, the own score of the participants, the distribution of score for each outcome as well as supplementary outcome will be presented in the questionnaire. Participants will be asked to prioritize the outcomes using the same scoring criteria as the first round within three weeks.
Data analysis at the end of round 2 will also include the participants’ response rate, the average score of each outcome, and the score of distribution for each item separately by group. If the score of an outcome item shows a significant change between two rounds, the reason will be requested. Consensus criteria will be specified in advance. The definition of consensus is derived from previous COS research, as detailed in Table 5.53 If more than 80% of the outcome indicators meet the consensus standards, they will be directly admitted to the consensus meeting; otherwise, they will proceed to the third round of Delphi.
 |
Table 5 Consensus Definition |
Round 3
Participants completing round 2 will participate in the third and final round of Delphi consultation via an online survey. Summary statistics such as the score distribution of each outcome by stakeholder group will accompany the electronic questionnaire. They will re-rate each item on the list using the same rating scale as the previous rounds for three weeks. The process of summary analysis follows the same pattern as before. The outcome will be classified based on the consensus definition. To maintain data integrity in the survey, the electronic questionnaire cannot be submitted when incomplete.
Stage 4. Consensus Meeting and COS-TCM-ZAN
The last step of developing COS-TCM-ZAN is to organize a face-to-face consensus meeting after the candidate outcomes of the COS are determined through the Delphi survey. The consensus meeting will be held in China for 1–2 days. A total of 20 participants will be invited, including all members of the steering group and participant representatives from each stakeholder group who have completed the Delphi investigations. The working group will report on the research method of the COS-TCM-ZAN and summarize the results of the Delphi survey. According to the consensus definition, outcomes of “consensus in” will be directly included in the final COS, whereas outcomes of “consensus out” will be instantly eliminated. Participants will vote anonymously on the outcomes identified as “no consensus” before full discussion. If these outcomes receive at least 75% of the votes cast, then they will also be recommended to the final COS.54 The procedure will comprise the following steps: (1) Anonymous presentation of the item’s rating distribution.(2) Timed statements from experts with opposing viewpoints.(3) A structured panel discussion.(4) The final decision is made through anonymous voting, and at least 75% of the votes are required for inclusion. Any conflict of view during the process will be addressed and resolved by the steering committee. The final COS-TCM-ZAN will be developed.
Discussion
TCM plays a vital role in healthcare and has certain characteristics and advantages in ZAN. Numerous clinical trials have been widely used and have reported benefits. However, the evidence is heterogeneous. The standardized outcomes will help clarify effectiveness. Non-standardized outcome reporting is a major challenge that compromises the quality of clinical studies. A COS can effectively address this issue.
There is currently no COS available that covers TCM treatment on ZAN. The researchers propose a robust approach to the development of TCM-COS-ZAN. A well-developed COS will standardize the evaluation of therapeutic effects, thereby enhancing the comparability and reproducibility in research and clinical practice for TCM in the field of ZAN treatment. The standardized COS will facilitate the identification of more effective evaluation indicators for TCM treatment of ZAN. By incorporating the insights of various stakeholders this COS ensures the scientific validity and rationality of the minimum outcome set. The COS research not only improves research efficiency and reduces research waste but also strengthens global collaboration aiming to maximize the potential of TCM in clinical practice in the future.
The methodological rigor of our study was strengthened by a clear, pre-defined consensus process. We set a 70% threshold for the Delphi rounds and a 75% voting rule to resolve any “no consensus” items in the consensus meeting. These criteria kept discussions focused, prevented deadlocks or dominance by individuals, and improved the credibility and objectivity of the final core outcome set.
Limitations of this study are acknowledged as detailed blow. First, the literature search and group discussions were conducted primarily in Chinese and English, which may have led to the omission of evidence published exclusively in other languages. To mitigate potential publication bias, we plan to translate the COS into English, circulate it to an international advisory group for review, and incorporate their feedback before initial publication. The scope of this study was confined to the identification of core outcomes, and when to measure lied beyond the scope. Although these time points were systematically recorded during data extraction, their analysis will be pursed in future work. Second, as the consensus meeting will take place in China, the results may be more representative of regional clinical practices than global ones. We acknowledge this potential limitation and will seek international feedback or external validation once the COS is finalized, ensuring its global applicability. Finally, recruiting some key stakeholder groups, such as clinicians with expertise in narrow subspecialties, may be difficult. To mitigate under-representation, we will report response rates by subgroup and actively invite experts from diverse clinical backgrounds to foster inclusive decision-making.
Ethics and Dissemination
The institutional ethics committee of The Third Affiliated Hospital of Zhejiang Chinese Medicine University has reviewed and approved the entire project (ZSLL-KY-2024-071-01). Informed consent will be obtained from all participants in the semi-structured interviews and the Delphi survey. On completion of the COS, we commit to updating the COMET record upon completion, disseminating a one-page checklist of the final COS as supplementary material and notifying all stakeholder groups. The final COS will be shared in peer-reviewed and open-access journals and presented at national and international conference. The publication of our findings will adhere to a predefined minimum data set that includes stage-specific yields, Delphi process details, and consensus meeting results as essential reporting criteria. We also send the publication to all participants of this study. It is hope that the COS will be widely recognized by the relevant fields.
Funding
The study was financially supported by the Program of Sci-research Foundation of the Affiliated Hospital of Zhejiang Chinese Medical University (2023FSYYZY12).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gregg RK, Kapil A, Isoba LG, et al. Herpes zoster in older adults: diagnosis, treatment, and care strategies. Geriatric Dermatol. 2024;13:1–12.
2. Anant P, Mohamad G, Uwe W. Herpes zoster: a review of clinical manifestations and management. Viruses. 2022;14(2):192. doi:10.3390/v14020192
3. Catherina XP, Michelle SL, Vinod EN. Global herpes zoster incidence, burden of disease, and vaccine availability: a narrative review. Therape Adv Vaccines Immunotherapy. 2022;10:1–19.
4. Yang C, Guo Z, Deng X, et al. Global, regional, and national burden of varicella-zoster infections in adults aged 70 years and older from 1997 to 2021: findings from the global burden of disease study. J Infect Public Health. 2025;18(10):102868. doi:10.1016/j.jiph.2025.102868
5. Devor M. Neural basis of pain in herpes zoster and postherpetic neuralgia: the ectopic pacemaker hypothesis. Herpes Zoster. 2017;06:157–187.
6. Albert JMVW, Yannick RA. Pain, itch, quality of life, and costs after herpes zoster. Pain Prac. 2017;17(6):738–746. doi:10.1111/papr.12518
7. Herpes Zoster Expert Consensus Working Group. Chinese medical doctor association dermatologist branch, national clinical research center for skin and immune diseases. Chinese consensus on the diagnosis and management of herpes zoster (2022). Chinese J Dermatol. 2022;55(12):1033–1040.
8. Chinese Medical Doctor Association Pain Medicine Branch. Chinese Medical doctor association neuromodulation professional committee. Expert consensus on the use of transcutaneous short-term nerve stimulation for the treatment of herpes zoster neuralgia in China. Chinese J Pain Med. 2021;27(11):801–805.
9. Robert WJ, Marie JAP, Marc B, et al. Herpes zoster epidemiology, management, and disease and economic burden in Europe: a multidisciplinary perspective. Therapeutic Adv Vaccines. 2015;3(4):109–120. doi:10.1177/2051013615599151
10. Haiou Z, Zhiguang W, Haifei J, et al. A systematic review and meta-analysis of independent risk factors for postherpetic neuralgia. Ann Palliative Med. 2021;10(12):12181–12189. doi:10.21037/apm-21-3028
11. Delwyn ZJL, Hong LT, Brenda MAS, et al. Herpes zoster and post-herpetic neuralgia-diagnosis, treatment, and vaccination strategies. Pathogens. 2024;13(7):596. doi:10.3390/pathogens13070596
12. Fei Y, Shengyuan Y, Bifa F, et al. The epidemiology of herpes zoster and postherpetic neuralgia in china: results from a cross-sectional study. Pain Therapy. 2019;8(2):249–259. doi:10.1007/s40122-019-0127-z
13. Xuelian L, Huaxiang Z, Xu Z, et al. A central and peripheral dual neuromodulation strategy in pain management of zoster-associated pain. Sci Rep. 2024;14(1):24672. doi:10.1038/s41598-024-75890-4
14. Aaron S, Shawn K, Michael M, et al. Herpes zoster and postherpetic neuralgia: prevention and management. Ame Family Physician. 2017;96(10):656–663.
15. Zhujiazi Z, Xinnong L, Luodan S, et al. The incidence of herpes zoster in China: a meta-analysis and evidence quality assessment. Human Vaccines Immunother. 2023;19(2):2228169. doi:10.1080/21645515.2023.2228169
16. Jing C, Page EA, k Y, et al. A systematic literature review of the epidemiology and burden of herpes zoster in selected locales in Asia Pacific. Hum Vaccin Immunother. 2024;20(1):2344983. doi:10.1080/21645515.2024.2344983
17. Priya S, Lisa AD, David PM. Herpes zoster (shingles) and postherpetic neuralgia. Mayo Clinic Proceedings. 2009;84(3):274–280. doi:10.4065/84.3.274
18. Zhanhong W, Danli W, Wen L, et al. Traditional Chinese medicine diagnosis and treatment based on systematics. iLIVER. 2023;2(4):181–187. doi:10.1016/j.iliver.2023.08.004
19. Ruijin Q, Yang S, Changming Z, et al. Methods of developing core traditional Chinese medicine syndromes set. Chinese J Evidence Based Med. 2021;21(11):1353–1357.
20. Lauren EK, Flora S, Sonya M, et al. A core outcome set for neonatal opioid withdrawal syndrome. Pediatrics. 2022;146(1):e20200018.
21. Duffy J, Cairns AE, Richards-D D, et al. A core outcome set for pre-eclampsia research: an international consensus development study. BJOG. 2020;127(12):1516–1526. doi:10.1111/1471-0528.16319
22. Fei F, Shanshan L. Boli zhang: promoting the internationalization of traditional Chinese medicine research with the methodology of evidence-based medicine. Chinese Med Sci. 2015;5(17):1–3.
23. Xinyue D, Mingjie Z, Qiaoning Y, et al. Analysis and reflection on the current situation of outcome indicators in clinical research of traditional chinese medicine based on literature. J Traditional Chinese Med. 2022;63(12):1122–1127.
24. Junhua Z. Research progress and prospect of core outcome set of traditional Chinese medicine. Chinese J Drug Eval. 2022;39(02):101–104.
25. Ruijin Q, Xuxu W, Zhiyue G, et al. Research status and prospect of core outcome sets in the field of traditional Chinese medicine. Chinese J Evidence Based Med. 2023;23(02):211–220.
26. Jianhua C, Chao L, Peijun J, et al. A bibliometric analysis and visualization of acupuncture and moxibustion therapy for herpes zoster and postherpetic neuralgia. Skin Res Technol. 2024;30(6):e13815. doi:10.1111/srt.13815
27. Changhe Y, Ying Z, Ying W, et al. Construction of an outcome-based evaluation system for clinical efficacy of traditional Chinese medicine. China J Traditional Chinese Med. 2021;36(03):1238–1243.
28. Carolina VN, Richeal NR, Sarah RB, et al. An international Delphi survey and consensus meeting to define the core outcome set for trigeminal neuralgia clinical trials. Euro J Pain. 2023;27(1):86–89. doi:10.1002/ejp.2041
29. Li Z, Junhua Z, Jing C, et al. Clinical research of traditional Chinese medicine needs to develop its own system of core outcome sets. Evidence Based Complement Alternat Med. 2013;2013:202703. doi:10.1155/2013/202703
30. Williamson PR, Altman DG, Bagley H, et al. The COMET handbook: version 1.0. Trials. 2017;18(Suppl 3):280. doi:10.1186/s13063-017-1978-4
31. Elizabeth G, Sarah LG, Paula RW. Choosing important health outcomes for comparative effectiveness research: 5th annual update to a systematic review of core outcome sets for research. PLoS One. 2019;14(12):e0225980. doi:10.1371/journal.pone.0225980
32. Paula RW, Heather B, Jane MB, et al. Review finds core outcome set uptake in new studies and systematic reviews needs improvement. J Clin Epidemiol. 2022;150:154–164. doi:10.1016/j.jclinepi.2022.06.016
33. Si-si M, He Y, Yu-qi L, et al. Qualitative research on TCM complex interventions - the experience and cognition of Chinese patients. Euro J Integrat Med. 2023;59:102243. doi:10.1016/j.eujim.2023.102243
34. Xiaoli Z, Zhoulin J, Ye Z, et al. Current advances in the pain treatment and mechanisms of traditional Chinese medicine. Phytother Res. 2024;38(8):4114–4139. doi:10.1002/ptr.8259
35. Elizabeth G. The COMET (core outcome measures in effectiveness trials) initiative. Maturitas. 2016;91:91–92. doi:10.1016/j.maturitas.2016.06.007
36. Alessandro L, Douglas GA, Jennifer T, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339(1):b2700. doi:10.1136/bmj.b2700
37. Karen I, Jemma H, Katie B, et al. Core outcome set for symptomatic uncomplicated gallstone disease. British J Surg. 2022;109(6):539–544. doi:10.1093/bjs/znac095
38. Sarah LK, Shauna LC, Sharleen LO, et al. Pregnancy nutrition core outcome set (PRENCOS): a core outcome set development study. BJOG. 2023;130(10):1247–1257. doi:10.1111/1471-0528.17470
39. Ruijin Q, Siqi W, Changming Z, et al. Core outcome sets for myocardial infarction in clinical trials of traditional Chinese medicine and Western medicine. J Evidence Based Med. 2024;17(1):86–94. doi:10.1111/jebm.12579
40. Guozheng F, Wenlong Y, Dingbang C, et al. Development of a core outcome set of clinical research on the integration of traditional Chinese and Western medicine for spinal metastases: a study protocol. BMJ Open. 2024;14(9):e083315. doi:10.1136/bmjopen-2023-083315
41. Mingyan Z, Chua H, Zhang J, et al. Developing a core outcome set on traditional Chinese medicine (COS-TCM) for chronic heart failure (CHF): a study protocol. BMJ Open. 2021;11(7):e047148. doi:10.1136/bmjopen-2020-047148
42. Xiaodi S, Chao C, Zhaochen J, et al. Development of a core outcome set on traditional Chinese medicine and Western medicine for rheumatic heart disease: a study protocol. BMJ Open. 2022;12(11):e062497. doi:10.1136/bmjopen-2022-062497
43. Manyara AM, Purvis A, Ciani O, et al. Sample size in multistakeholder Delphi surveys: at what minimum sample size do replicability of results stabilize? J Clin Epidemiol. 2024;174:111485. doi:10.1016/j.jclinepi.2024.111485
44. Jill JF, Marie J, Clare R, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychology & Health. 2010;25(10):1229–1245. doi:10.1080/08870440903194015
45. Jamie JK, Sarah G, Douglas GA, et al. Core outcome set-standardised protocol items: the COS-STAP statement. Trials. 2019;20(1):116. doi:10.1186/s13063-019-3230-x
46. Gonçalves AC, Samuel D, Ramsay M, et al. A core outcome set to evaluate physical activity interventions for people living with dementia. Gerontologist. 2020;60(4):682–692. doi:10.1093/geront/gnz100
47. Reynolds KA, Schlessinger DI, Vasic J, et al. Core outcome set for actinic keratosis clinical trials. JAMA Dermatol. 2020;156(3):326–333. doi:10.1001/jamadermatol.2019.4212
48. Hasan FÇ, Aysen A, Lale A, et al. Evaluation of disease burden, patient journey, unmet diagnosis and treatment needs of patients with Hip and knee osteoarthritis in Turkey: a study through Delphi methodology. Osteoarthritis Cartilage Open. 2022;5(1):100332. doi:10.1016/j.ocarto.2022.100332
49. Dilek T, Collette H, Ann WM, et al. Developing consensus in histopathology: the role of the Delphi metho. Histopathology. 2022;81(2):159–167. doi:10.1111/his.14650
50. Diamond IR, Grant RC, Feldman BM. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–409. doi:10.1016/j.jclinepi.2013.12.002
51. Yuxin Z, Mengjuan J, Xiulu X, et al. Development and preliminary validation of the evaluation scale for nurses’ core emergency response abilities in sudden major infectious disease outbreaks. BMC Nurs. 2025;24(1):266. doi:10.1186/s12912-025-02922-3
52. Iezadi S, Gholipour K, Khanijahani A, et al. Development, validation, and pilot implementation of the minimum datasheet for a domestic violence registry system: the case of a developing country. PLoS One. 2021;16(12):e0261460. doi:10.1371/journal.pone.0261460
53. Olga H, Silvie HMJ, Bryce BR, et al. Protocol for the development of a core outcome set (COS) for adolescents and young adults (AYAs) with cancer. BMC Cancer. 2024;24(1):126. doi:10.1186/s12885-023-11716-2
54. Geng L, Ruxue H, Mingjun L, et al. Developing a core outcome set for clinical trials of chinese medicine for hyperlipidemia. Front Pharmacol. 2022;13:847101. doi:10.3389/fphar.2022.847101
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.