Back to Journals » Journal of Pain Research » Volume 16
Determining the Efficacy and Safety of Acupuncture for the Preventive Treatment of Menstrual Migraine: A Protocol for a PRISMA-Compliant Systematic Review and Meta-Analysis
Authors Wu Q ![]() , Wang J
, Wang J ![]() , Lin X, Han D, Hu H
, Lin X, Han D, Hu H ![]() , Gao H
, Gao H
Received 24 October 2022
Accepted for publication 17 December 2022
Published 10 January 2023 Volume 2023:16 Pages 101—109
DOI https://doi.org/10.2147/JPR.S394446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Qiqi Wu,1,* Jiawei Wang,2,* Xiaoqi Lin,2,* Dexiong Han,3 Hantong Hu,3 Hong Gao3
1Department of Acupuncture, Moxibustion and Massage, Wenzhou Central Hospital, Wenzhou City, People’s Republic of China; 2The Third School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China; 3Department of Acupuncture and Moxibustion, the Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hantong Hu; Hong Gao, Department of Acupuncture and Moxibustion, the Third Affiliated Hospital of Zhejiang Chinese Medical University, No. 219 Moganshan Road, Xihu District, Hangzhou City, People’s Republic of China, Email [email protected]; [email protected]
Background: Menstrual migraine (MM), as a common type of headache related to women’s menstrual cycle, currently available treatments do not produce sufficient effectiveness, making it remains difficult to manage. Although acupuncture may be an effective treatment for MM, there is a lack of convincing evidence to recommend acupuncture to patients with MM until more solid evidence is produced. Therefore, the purpose of our systematic review (SR) and meta-analysis protocol is to synthesize up-to-date evidence regarding the clinical efficacy and safety of acupuncture on MM.
Methods: To find qualifying RCTs, nine databases will be searched. RevMan 5.3 will be used to combine the retrieved data for meta-analyses. The Cochrane risk of bias instrument will be used to assess the methodological quality of each included trial. The strength and certainty of the evidence will be evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system. Additionally, we will undertake sensitivity analyses, publication bias, and subgroup analyses if available.
Discussion: Our SR and meta-analysis protocol will contribute to determining acupuncture’s therapeutic effect and safety in the preventive treatment of MM. Based on the up-to-date evidence produced by the subsequent SR and meta-analysis, informed treatment decisions will be made by patients, physicians and policy makers.
Keywords: menstrual migraine, acupuncture, systematic review, meta-analysis
Introduction
Migraine is a common chronic neurovascular disorder. According to the 2013 Global Burden of Disease survey from the World Health Organization (WHO), migraine was identified as the 3rd most common disease and was the 6th most disabling disease.1,2 The International Headache Society defines migraine as an episodic headache that lasts from 4 to 72 h, concomitant with two of the following: throbbing pain, unilateral localization, aggravation by movement, moderate or severe intensity, and at least one of the following: nausea or vomiting, or photophobia and phonophobia.3 The exact pathogenesis of migraine remains unclear, but the disorder may be associated with neurovascular dysfunction.4 Migraine affects 18.9% of women worldwide,5 and menstrual migraine (MM) is a special type of migraine associated with women’s menstrual cycle.
MM attacks often occur before the onset of menstruation, the symptoms are significantly worse during menstruation and are relieved after menstruation, and the frequency and symptoms of outbreaks tend to decrease during pregnancy or after menopause as hormone levels stabilized.6,7 The headache of MM is often more severe than other types of migraine, with recurring attacks, usually lasting for 4~5 days, as long as the duration of menstruation, and is often accompanied by nausea, photophobia, irritability, depression, spontaneous sweating, stiff neck and vomiting.8–10
It has been shown that MM is closely related to the ovarian cycle.11 About 60% of female migraineurs report a link between migraine and menstruation.12 Currently, the pathophysiological mechanisms underlying MM are not fully understood, but many studies suggest that due to the specific physiological cycle and genetic specificity of female migraine patients, the levels of sex hormones, especially estrogen, change periodically, along with changes in the function and morphology structure of nerve cells in the brain, and play an “analgesic” or “pain-causing” role in migraine under the influence of the internal and external environment.13,14
The clinical diagnosis and treatment of MM are inadequate. Current treatment is mainly based on the migraine management model, which mainly includes acute treatment and preventive treatment. Acute treatment focuses on aborting migraine attacks, while preventive treatment focuses on reducing the frequency, duration and severity of migraine attacks. Treatment mainly includes pharmacological treatment (eg, non-steroidal anti-inflammatory drugs, calcium channel blockers, beta-blockers, analgesics, triptans, ergotamines) and non-pharmacological therapies (eg, psychotherapy, physical therapy and surgery).15 However, Western medicine treatment varies greatly among individuals and requires a long treatment period, while a long-term treatment course is prone to recurrence and side effects (such as gastrointestinal reactions). In addition, overuse of analgesics or specific anti-migraine treatments may lead to increased frequency of headaches and medication overuse headaches.16,17 Consequently, one of the main goals of the medical community today is to reduce drug-related side effects and improve the quality of life and symptoms of female patients; hence, complementary and alternative medicine (CAM) is expected to serve as an optional therapy for patients with MM.
Acupuncture therapy has been frequently reported to be a useful CAM therapy for the treatment of MM.18–23 The role of acupuncture on MM includes acute effects for aborting migraine attacks and preventive effects for reducing the frequency, duration and severity of migraine attacks. Notably, there is an increasing number of clinical trials supporting the preventive effect of acupuncture on MM. For example, the study conducted by Liu et al indicated that acupuncture can reduce the number of migraine days in patients with MM21 by performing acupuncture 10 days before menstruation. The other trial conducted by Zhang et al revealed that true acupuncture and sham acupuncture were both helpful in treating MM and could improve emotional symptoms, but true acupuncture had a better effect in reducing the frequency of MM attacks than sham acupuncture.22 Another trial performed by Yu et al showed that both acupuncture and acupressure are significantly effective in reducing the number of MM days and peak pain.23
Despite that a previous systematic review (SR) and meta-analysis24 attempted to evaluate the evidence regarding the therapeutic effect of acupuncture on MM, as concluded by this study, there is no conclusive evidence to support the efficacy of acupuncture in treating MM, thereby making acupuncture cannot yet be recommended to patients with MM until more solid evidence is produced. Moreover, it is notable that only RCTs published before 1 May 2019 were included in this SR and meta-analysis,24 hence, the total amount of the included qualified RCTs was only 13. With the publication of increasing randomized controlled trials (RCTs)21,22,25–29 in the past 3 years, it is critical to integrate these recent potentially eligible RCTs into an up-to-date SR and meta-analysis to update the previous evidence in this field. Therefore, this protocol outlines the rationale, feasibility, and methodological procedure for a SR and meta-analysis that aims to summarize the up-to-date evidence concerning acupuncture’s clinical efficacy and safety on MM.
In addition to the rationale elaborated above, the feasibility of conducting this study is described below. First, with the increasing number of RCTs published in recent years, it is likely to integrate more eligible studies in the subsequent SR and meta-analysis. Second, by referring to previous studies21,30 or SR/meta-analyses,31,32 the methodological procedures (such as trial inclusion criteria and outcome measures of interest) of this study will be scientific and feasible.
Objective
The goal of this SR and meta-analysis protocol is to summarize the up-to-date evidence to verify the efficacy and safety of acupuncture in the preventive treatment of MM.
Methods
While creating this SR and meta-analysis protocol, we consult the globally recognized checklist of the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P, uploaded in Supplementary Table 1).33 Additionally, to promote research transparency, we have registered our protocol in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42022367446.
Eligibility Criteria
The eligibility of the trials will be assessed using the validated ‘PICOS’ establishment for a SR and meta-analysis, which are shown below in further detail.
Study Designs
The eligible research type for our SR and meta-analysis will be limited to RCTs that aim to examine the effect of acupuncture therapy for MM, regardless of the publication language. Additionally, we will only include the results of the two groups prior to crossover in the meta-analysis for crossing over RCTs.34 Reviews, case series, non-RCTs, or other ineligible research types will not be taken into account.
Participants
Participants have a confirmed diagnosis of MM based on the International Headache Society (IHS) diagnostic criteria or other standards that generally matched the IHS diagnostic criteria.35,36 Participants who have been given a diagnosis of tension-type headache, chronic migraine, cluster headache, other primary headaches, secondary headache brought about by otorhinolaryngological illnesses or intracranial pathological alterations will be disqualified from the study. There will be no limitations on participants’ nationality, gender, or age.
Interventions in the Experimental Group
Acupuncture therapy must be used in the test group. Notably, acupuncture can be employed in the test group alone or in conjunction with other positive treatments that are the same as those used in the control arm. For our study, the definition of acupuncture therapy responds to acupuncture modalities involving skin penetrating, such as auricular acupuncture, warming-needle moxibustion, electroacupuncture (EA), manual acupuncture (MA) and so on. The clinical variability among the included studies will be reduced as a result of this prospective definition of acupuncture therapy. Studies using non-penetrating acupuncture methods, such as laser acupuncture and acupressure, are not permitted in such a situation.
Interventions in the Control Group
- Active therapies, such as medication, counseling, physical therapy, and surgery, as recommended by guidelines.37–41
- Sham acupuncture and other placebo measures.
- Waiting list management.
- Blank control (no treatment).
Outcome Measures
To determine the outcomes of interest, we consult previous similar researches.42–44 Accordingly, original studies that will be scrutinized for eligibility must have at least one of the outcome measures as follows.
Primary Outcome Measures
- Frequency of migraine attacks (FM).
- Number of migraine days (NM).
- Pain intensity assessed by the Visual Analog Scale (VAS).
Secondary Outcome Measures
- Duration of migraine (DM).
- Migraine-Specific Quality of Life Questionnaire (MSQ).
- Self-rating Depression Scale (SDS).
- Total effective rate (ER).
- Adverse events (AEs).
Safety Evaluation
The total number of AEs in each group of the original RCT will be extracted and pooled in meta-analysis for the safety evaluation of acupuncture compared with the control treatments. Regarding acupuncture-related AEs, they mainly include fainting or unbearable acupuncture pain during acupuncture treatment, local haematoma, and post-needling discomfort.
Sources for Trial Retrieval
A systematic search will be conducted across 9 representative databases, including 5 English-language databases (ie, Physiotherapy Evidence Database (PEDro), Cochrane Central Register of Controlled Trials, EMBASE, Web of Science, PubMed) and 4 Chinese-language databases (ie, VIP Database for Chinese Technical Periodicals, Wanfang database, Chinese National Knowledge Infrastructure, Chinese Biomedical Literature Database). From the time of creation until December 2022, we will scan each database for possibly qualified RCTs.
Retrieval Strategies
The three components of the search strategies are as follows: subjects (MM), research type (RCT), and treatments (such as warming-needle moxibustion, MA, EA, and auricular acupuncture). The database will be searched using any pertinent phrases related to these 3 elements. Individual or combination search phrases in English will be used for English-language databases, and Chinese-language databases will be retrieved using the appropriate search phrases. Our retrieval strategies will blend free text words and subject headings to achieve the highest degree of retrieval sensitivity and comprehensiveness (eg, Medical Subject Headings [MeSH] for PubMed). The retrieval strategies of PubMed are shown in Table 1, which will be modified for the remaining databases by superseding MeSH with pertinent topic keywords (where available) and maintaining the same free-text phrases.
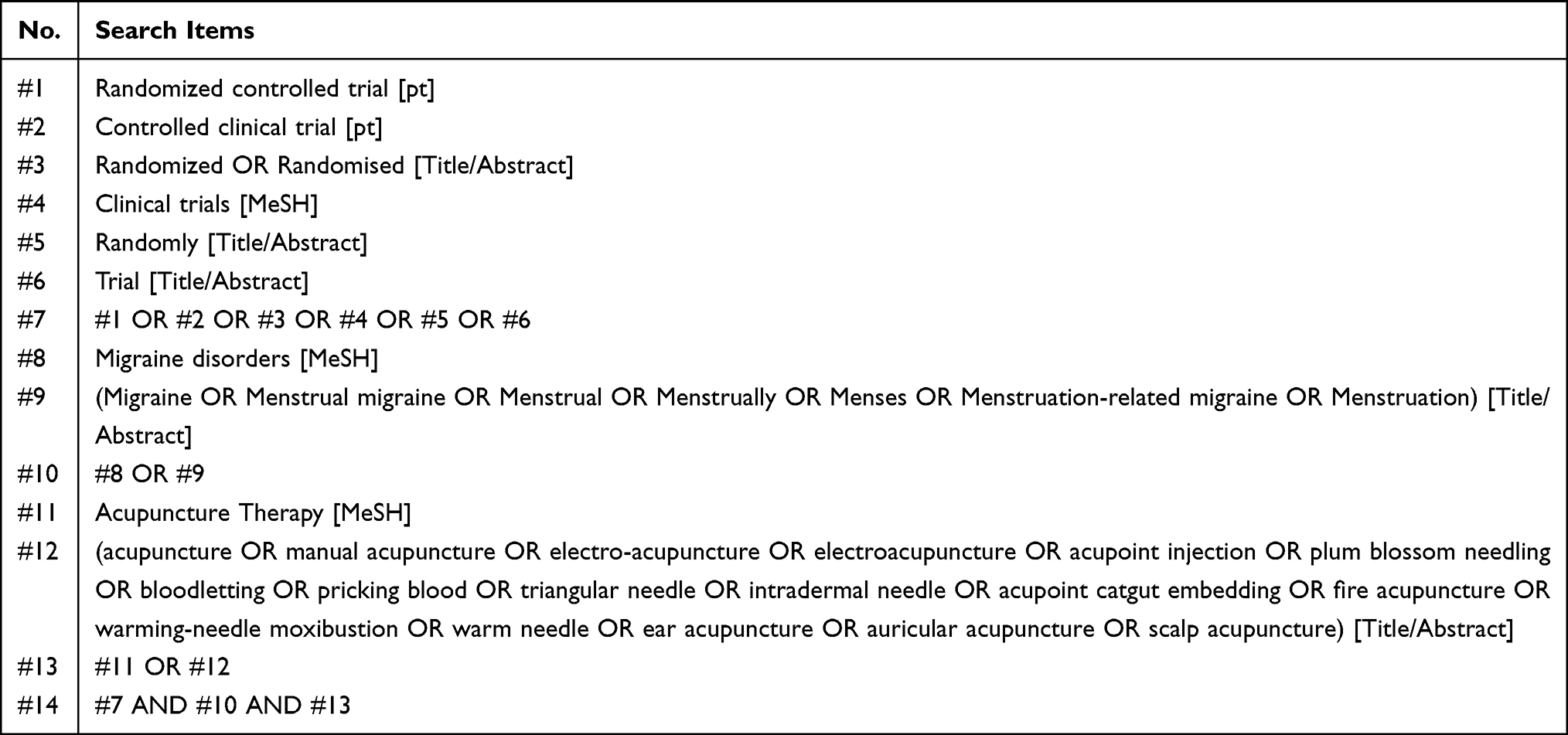 |
Table 1 The Search Strategies for PubMed |
The references of prior relevant SRs and meta-analyses in this clinical topic will also be scanned to avoid the possible omission of eligible RCTs. If this SR is updated in the future, relevant ongoing trials will also be looked up on the Clinical Trials Registry (www.clinicaltrials.gov/), the World Health Organization’s International Clinical Trials Registry Platform (www.who.int/clinical-trials-registry-platform), the Chinese Clinical Trial Registry (www.chictr.org.cn).
Study Selection Process
The total number of retrieval records generated by the 9 databases will be transferred into EndNote (version X9, Clarivate, USA) to delete duplicate publications. First, two reviewers (J.W and Q.W) will independently analyze the titles and abstracts of the imported articles to find any potential studies that could fit the aforementioned qualification requirements and weed out studies that appear to be irrelevant. The complete text of every potential qualifying publication will be studied at the second round of literature screening to eventually confirm validity. The third referee (H.G) will be consulted if there is disagreement among the reviewers as to whether or not to include a particular trial. The selection of the studies is summarized in Figure 1.
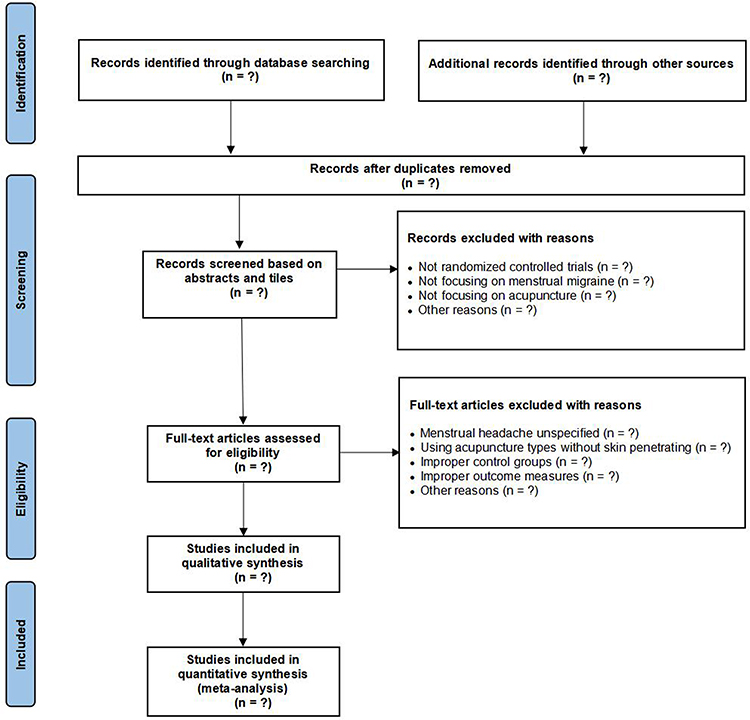 |
Figure 1 The PRISMA-compliant flowchart of study selection. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. Creative Commons. |
Data Extraction and Data Items
To gather relevant information about the included trial, two unbiased reviewers (Q.W and J.W) will use a pre-defined electronic table (Supplementary Table 2) to gather author names, publication years, study designs, participant characteristics, sample sizes, interventions in both groups, the frequency and duration of treatment, and outcome measures. Regarding continuous variables, means and standard deviations (SDs) will be gathered when all eligible RCTs have been identified. When continuous data are given in different ways, The Cochrane Handbook for Systematic Reviews of Interventions45 advises converting them to means (SDs). The total amount of subjects and respondents for each group in a dichotomous variable will be retrieved. Additionally, if pertinent data are missing from the original articles, reviewers will send an email to the relevant authors asking for the missing information. Two reviewers (Q.W and J.W) will refer any disagreements to the senior referee (H.G) to be resolved.
Before entirely extracting data for all included studies, Kappa coefficients will be used to assess the inter-rater agreements on the accuracy of data extraction by comparing between-rater differences for data extracted from 20 randomly chosen studies. If there is insufficient inter-rater consistency and accuracy, reviewers will receive further data extraction training.
Evaluation of the Methodological Quality
Two raters (J.W and Q.W) will assess each enrolled RCT’s methodological quality independently using the risk of bias (RoB) 2.0 tool suggested by the Cochrane Collaboration.46 The risk of bias for each included study will be assessed using the following five critical factors: 1) the randomization procedure; 2) digressions from intended treatments; 3) lacking outcome data; 4) outcomes measuring; and 5) the choice of the reported outcome. Each domain will receive a rating of “low”, “unclear”, or “high”. Furthermore, reviewers will provide a grade of “low” (indicating low ROB in the whole domains), “unclear” (indicating some worries in leastwise one domain), or “high” to each trial’s overall ROB (indicating high ROB in at least one domain, or some worries in several domains). Any dispute between the two raters shall be resolved through mediation with the referee (H.G).
Data Synthesis and Statistical Analysis
For the meta-analysis of pooled trials with extracted data, the effect size and 95% confidence interval (CI) will be determined using the RevMan software (V5.30, Cochrane Collaboration, England). Due to the anticipated heterogeneity resulting from the likely different acupuncture protocols across each trial, meta-analyses will be conducted using the random effects model. The I2 statistic value, which is employed by the χ2 test to gauge heterogeneity among all included studies, is taken to indicate considerably heterogeneous data when it exceeds 50%. When assessing pooled effects, statistical significance is indicated by a two-sided P value less than 0.05. Sensitivity studies utilizing the leave-one-out methodology will also be utilized to assess the dependability of the results of the meta-analysis.
Subgroup Analysis
When they are available, we will undertake subgroup analyses in terms of the aspects as follows.
- Various acupuncture methods (eg, MA, EA).
- Different traits of the control arm (eg, sham controls, active controls).
- Different assessment points for the primary outcome.
Assessment of Evidence Strength and Certainty
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) method by the Cochrane collaboration will be used to evaluate the strength and certainty of the evidence, which will be classified into a total of 4 evidence levels (ie, extremely low, low, moderate, and high).47
Publication Bias
If 10 or more trials are included in the meta-analysis, publication bias will be examined using funnel plots and the Egger test.
Ethics-Related Issues
Due to the absence of any identifiable data, this protocol does not require ethical approval.
Discussion
As a TCM treatment, acupuncture is an important tool in the clinical treatment of MM. A large number of clinical trials have reported that acupuncture can effectively treat MM. Despite that a previous SR and meta-analysis study sought to assess the evidence on the therapeutic impact of acupuncture on MM, this study only concluded that acupuncture cannot yet be recommended to MM patients until more solid evidence is produced. Therefore, to date, there has been a lack of definitive evidence supporting the use of acupuncture in treating MM. Nonetheless, it should be noted that this review24 only included RCTs published before 1 May 2019 for evidence synthesis. Thus, only 2 English publications were included and the total number of the included RCTs is inadequate (only 13). With the emerging publications of RCTs21,22,25–29 in the past 3 years, it is critical to integrate these RCTs into an up-to-date SR and meta-analysis to update the previous evidence in this field. Thus, we conduct this SR and meta-analysis to summarize the up-to-date evidence to verify the efficacy and safety of acupuncture in the preventive treatment of MM.
Although both of our study and a previous similar study24 aim to evaluate the efficacy and safety of acupuncture on MM, nevertheless, one of the main differences between our study and the previous study24 is that our research will include more eligible RCTs, especially those published in recent years, to perform an updated SR and meta-analysis. The other main difference is that the topic of our SR and meta-analysis focus more on the prophylactic treatment of acupuncture on MM, so we partly amend the classification of primary and secondary outcomes for conducting a SR and meta-analysis in relative to the previous SR.24 Thus, the anticipated results of this study will enable a definite conclusion to be drawn. Additionally, by determining a potentially effective and safe therapy for MM, our study will enrich the treatment of MM. Based on the up-to-date evidence produced by the subsequent SR and meta-analysis, will contribute to well-informed treatment decisions made by clinicians, policy makers, and patients. The aforementioned aspect is the primary merit of our study.
In addition, the PRISMA-P guidelines will be fully cited in our SR and meta-analysis protocol.33 To incorporate as many eligible RCTs as possible, 9 typical English and Chinese databases will be exhaustively searched for our study. The Cochrane Collaboration’s GRADE tool will also be adopted to assess the certainty and strength of the generated evidence. When appropriate, publication bias, sensitivity and subgroup analyses will also be carried out.
However, this review has several expected limitations. First, different types of acupuncture may lead to the risk of significant heterogeneity between the included studies in pooled results. Second, it is anticipated that China will host the majority of the included RCTs; however, it is previously revealed that China has published vastly more acupuncture studies with positive results than Western nations.48 Thus, it will potentially arise publication bias, thereby decreasing the robustness of the study results.
Conclusion
In conclusion, this study expounds on the rationale, feasibility, as well as anticipated methodological steps, for an updated SR and meta-analysis. Expected findings will determine the efficacy and safety of acupuncture for the preventive treatment of MM, and verify whether acupuncture can be an evidence-based treatment approach for the preventive treatment of MM.
Author Contributions
All authors contributed significantly to the work that was published, whether it be in the conception, study design, implementation, data collection, analysis, and interpretation, or all of these areas. They also all participated in drafting, revising, or critically evaluating the article, gave their final approval for the version that would be published, agreed on the journal to which the article has been submitted, and agreed to be responsible for all aspects of the work.
Funding
The work was supported by Zhejiang Provincial Famous Traditional Chinese Medicine Experts Inheritance Studio Construction Project (grant number: GZS2021027), the 2021 Special Project for Modernization of Chinese Medicine in Zhejiang Province (grant number: 2021ZX010), the hospital project of the Third Affiliated Hospital of Zhejiang Chinese Medical University (grant number: ZS21ZA01) and the Zhejiang Province Public Welfare Technology Application Research (grant number: LTGY23H270003).
Disclosure
Qiqi Wu, Jiawei Wang, and Xiaoqi Lin are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Zhang Y, Wang H, Liu L. Patent foramen ovale closure for treating migraine: a meta-analysis. J Interv Cardiol. 2022;2022:6456272. doi:10.1155/2022/6456272
2. Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743–800. doi:10.1016/S0140-6736(15)60692-4
3. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
4. Dalkara T, Nozari A, Moskowitz MA. Migraine aura pathophysiology: the role of blood vessels and microembolisation. Lancet Neurol. 2010;9(3):309–317. doi:10.1016/S1474-4422(09
5. GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/S1474-4422(18)30322-3
6. Sacco S, Ricci S, Degan D, Carolei A. Migraine in women: the role of hormones and their impact on vascular diseases. J Headache Pain. 2012;13(3):177–189. doi:10.1007/s10194-012-0424-y
7. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States. Relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267(1):64–69. doi:10.1001/jama.1992.03480010072027
8. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders. Cephalalgia. 2013;33(9):629–808. doi:10.1177/0333102413485658
9. Peck KR, Johnson YL, Smitherman TA. Migraine. Handb Clin Neurol. 2016;138:283–293. doi:10.1016/B978-0-12-802973-2.00016-1
10. Bigal ME, Edvinsson L, Rapoport AM, et al. Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of chronic migraine: a multicentre, randomised, double-blind, placebo-controlled, phase 2b study. Lancet Neurol. 2015;14(11):1091–1100. doi:10.1016/S1474-4422(15)00245-8
11. Uygunoglu U, Siva A. Epidemiology of Headache//Dimos D, Mitsikostas, Koen Paemeleire. Pharmacol Management Headaches. 2016;7:17.
12. Pavlović JM, Stewart WF, Bruce CA, et al. Burden of migraine related to menses: results from the AMPP study. J Headache Pain. 2015;16:24. doi:10.1186/s10194-015-0503-y
13. Peterlin BL, Gupta S, Ward TN, et al. Sex matters: evaluating sex and gender in migraine and headache research. Headache. 2011;51(6):839–842. doi:10.1111/j.1526-4610.2011.01900.x
14. Delaruelle Z, Ivanova TA, Khan S, et al. Male and female sex hormones in primary headaches. J Headache Pain. 2018;19(1):117. doi:10.1186/s10194-018-0922-7
15. Allais G, Chiarle G, Sinigaglia S, et al. Menstrual migraine: a review of current and developing pharmacotherapies for women. Expert Opin Pharmacother. 2018;19(2):123–136. doi:10.1080/14656566.2017.1414182
16. Bigal ME, Lipton RB. Excessive acute migraine medication use and migraine progression. Neurology. 2008;71(22):1821–1828. doi:10.1212/01.wnl.0000335946.53860.1d
17. Bigal ME, Borucho S, Serrano D, et al. The acute treatment of episodic and chronic migraine in the USA. Cephalalgia. 2009;29(8):891–897. doi:10.1111/j.1468-2982.2008.01819.x
18. Chen LN, Zhu W, Lin Y, et al. Balance acupuncture for females with menstrual migraine: a clinical study. J Guangzhou Univ Trad Chine Med. 2011;28:379–381+387.
19. Wang LH, Li DH, Zhang JQ, et al. Clinical effect of Shuitu acupoint transcutaneous electric nerve stimulation combined with acupoint injection on menstrual migraine: a randomized controlled observation. Modern J Integrated Trad Chine Western Med. 2015;24:1829–1831+1834. doi:10.3969/j.issn.1008-8849.2015.17.002
20. Tian LQ, Li L. Acupuncture at the starting and ending points of Liver-Gall bladder meridians for menstrual migraine: a clinical study. J Clin Acupuncture Moxibustion. 2014;30:7–9. doi:10.3969/j.issn.1005-0779.2014.05.003
21. Liu L, Zhang CS, Liu HL, et al. Acupuncture for menstruation-related migraine prophylaxis: a multicenter randomized controlled trial. Front Neurosci. 2022;16:992577. doi:10.3389/fnins.2022.992577
22. Zhang Y, Wang Z, Du J, et al. Regulatory effects of acupuncture on emotional disorders in patients with menstrual migraine without aura: a resting-state fMRI study. Front Neurosci. 2021;15:726505. doi:10.3389/fnins.2021.726505
23. Yu X, Salmoni A. Comparison of the prophylactic effect between acupuncture and acupressure on menstrual migraine: results of a pilot study. J Acupunct Meridian Stud. 2018;11(5):303–314. doi:10.1016/j.jams.2018.04.003
24. Yang M, Du T, Long H, et al. Acupuncture for menstrual migraine: a systematic review. BMJ Support Palliat Care. 2020. doi:10.1136/bmjspcare-2019-002024
25. Liu LY. Treatment of menstrual migraine with warming acupuncture and moxibustion. Shanxi Univ Chine Med. 2020. doi:10.27820/d.cnki.gszxy.2020.000055
26. Du EY, Wang N. Clinical observation of acupuncture treatment of menstrually related migraine. Chine Commun Doctors. 2022;38(09):69–71.
27. Yan JX, Wang Q, Liao ZL, et al. Treatment of menstrual migraine patients with Qi stagnation blood stasis syndrome by acupuncture and medicines: a randomized controlled trial. Chine J Integrated Trad Western Med. 2021;41(12):1511–1513.
28. Xing R, Zhang SX. Observation on acupuncture combined with blood-letting therapy in the treatment of menstrual headache of the liver fire syndrome. Jilin J Chine Med. 2020;40(12):1659–1662. doi:10.13463/j.cnki.jlzyy.2020.12.033
29. Li XF, Yu M. Clinical study on the treatment of menstrual migraine by acupuncture taichong and yongquan points. J Xi’an Jiaotong Univ. 2019;40(05):834–838. doi:10.7652/jdyxb201905033
30. Allais G, Bussone G, Tullo V, et al. Frovatriptan 2.5 mg plus dexketoprofen (25 mg or 37.5 mg) in menstrually related migraine. Subanalysis from a double-blind, randomized trial. Cephalalgia. 2015;35(1):45–50. doi:10.1177/0333102414542290
31. Hu Y, Guan X, Fan L, et al. Triptans in prevention of menstrual migraine: a systematic review with meta-analysis. J Headache Pain. 2013;14(1):7. doi:10.1186/1129-2377-14-7
32. Nierenburg Hdel C, Ailani J, Malloy M, et al. Systematic review of preventive and acute treatment of menstrual migraine. Headache. 2015;55(8):1052–1071. doi:10.1111/head.12640
33. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1
34. Lee CJ, Iyer G, Liu Y, et al. The effect of vitamin D supplementation on glucose metabolism in type 2 diabetes mellitus: a systematic review and meta-analysis of intervention studies. J Diabetes Complications. 2017;31(7):1115–1126. doi:10.1016/j.jdiacomp.2017.04.019
35. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders. Cephalalgia. 2004;24:9–160. doi:10.1111/j.1468-2982.2003.00824.x
36. Headache Classification Committee of the International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia. 1988;8:1–96.
37. Worthington I, Pringsheim T, Gawel MJ, et al. Canadian Headache Society guideline: acute drug therapy for migraine headache. Can J Neurol Sci. 2013;40(5 Suppl 3):S1–S80. doi:10.1017/S0317167100017819
38. American Headache Society. The American Headache Society position statement on integrating new migraine treatments into clinical practice. Headache. 2019;59(1):1–18. doi:10.1111/head.13456
39. Pringsheim T, Davenport W, Mackie G, et al. Canadian Headache Society guideline for migraine prophylaxis. Can J Neurol Sci. 2012;39(2 Suppl 2):S1–S59.
40. Scottish Intercollegiate Guidelines Network (SIGN). Pharmacological management of migraine. 2018. Available from: http://www.sign.ac.uk.
41. National Institute for Health and Care Excellence (NICE). Diagnosis and management of headaches in young people and adults: evidence update October 2014. Available from: https://www.evidence.nhs.uk/search?q=Diagnosis+and+manageme.
42. Ou MQ, Fan WH, Sun FR, et al. A systematic review and meta-analysis of the therapeutic effect of acupuncture on migraine. Front Neurol. 2020;11:596. doi:10.3389/fneur.2020.00596
43. Jiang Y, Bai P, Chen H, et al. The effect of acupuncture on the quality of life in patients with migraine: a systematic review and meta-analysis. Front Pharmacol. 2018;9:1190. doi:10.3389/fphar.2018.01190
44. Xu J, Zhang FQ, Pei J, et al. Acupuncture for migraine without aura: a systematic review and meta-analysis. J Integr Med. 2018;16(5):312–321. doi:10.1016/j.joim.2018.06.002
45. Higgins J, Thomas. J. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Collab. 2011;10:1465.
46. Flemyng E, Dwan K, Moore TH, et al. Risk of bias 2 in Cochrane reviews: a phased approach for the introduction of new methodology. Cochrane Database Syst Rev. 2020;10:Ed000148. doi:10.1002/14651858.ED000148
47. Brozek JL, Akl EA, Alonso-Coello P, et al. Grading quality of evidence and strength of recommendations in clinical practice guidelines. Part 1 of 3. An overview of the GRADE approach and grading quality of evidence about interventions. Allergy. 2009;64(5):669–677. doi:10.1111/j.1398-9995.2009.01973.x
48. Gang WJ, Gong CZ, Jing XH. Acupuncture randomized controlled trials: comparing China-based vs Western-based studies. Zhongguo Zhen Jiu. 2022;42(1):3–7. doi:10.13703/j.0255-2930.20201224-k0001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
The Analgesic Effect and Potential Mechanisms of Acupuncture for Migraine Rats: A Systematic Review and Meta-Analysis
Sun S, Liu L, Zhou M, Liu Y, Sun M, Zhao L
Journal of Pain Research 2023, 16:2525-2542
Published Date: 24 July 2023
Efficacy of Acupuncture in Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Yang C, Tian H, Xu G, Luo Q, Sun M, Liang F
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:707-720
Published Date: 11 March 2024
Acupuncture and Moxibustion in the Treatment of Gynecological Perioperative Anxiety: A Systematic Review and Meta-Analysis
Wang X, Yu Q, Zhu J, Liu J, Gao X, Wang X, Wang L, Xu X
Journal of Pain Research 2024, 17:3515-3538
Published Date: 31 October 2024
Efficacy of Acupuncture Assisted Anesthesia in Laparoscopic Cholecystectomy: A Systematic Review and Meta-Analysis
Lv H, Xu J, Bian Z, Lu Y, Li X, Jiang Y, Fang J, Liu Y
Journal of Pain Research 2025, 18:5567-5585
Published Date: 25 October 2025