")
Back to Journals » Patient Related Outcome Measures » Volume 15
Determinants of Mortality of Patients Admitted to the Intensive Care Unit at Debre Berhan Comprehensive Specialized Hospital: A Retrospective Cohort Study
Authors Melaku EE , Urgie BM , Dessie F, Seid A, Abebe Z , Tefera AS
Received 29 November 2023
Accepted for publication 16 February 2024
Published 22 February 2024 Volume 2024:15 Pages 61—70
DOI https://doi.org/10.2147/PROM.S450502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Ermiyas Endewunet Melaku,1 Besufekad Mulugeta Urgie,1 Firmayie Dessie,1 Ali Seid,1 Zenebe Abebe,2 Aklile Semu Tefera3
1Department of Internal Medicine, School of Medicine, Debre Berhan University, Debre Berhan, Ethiopia; 2Department of Biostatistics, School of Public Health, Debre Berhan University, Debre Berhan, Ethiopia; 3Department of Epidemiology, School of Public Health, Debre Berhan University, Debre Berhan, Ethiopia
Correspondence: Ermiyas Endewunet Melaku, Debre Berhan University, Debre Berhan, Ethiopia, Tel +251912980319, Email [email protected]
Background: The provision of intensive care services is advancing globally. However, in resource-limited settings, it is lagging far behind and intensive care unit mortality is still higher due to various reasons. This study aimed to assess determinants of mortality among medical patients admitted to the intensive care unit.
Methods: A five-year facility-based retrospective Cohort Study was conducted. A total of 546 medical patients admitted to the intensive care unit from March 2017 to February 2022 were included. Document review using a structured questionnaire was implemented to collect data. Data entered into Epi Data were analyzed by STATA and summarized using frequency tables and graphs. Binary and multivariate logistic regression analyses were performed to identify determinants of mortality.
Results: The overall mortality was 35.9%. Approximately half of the deaths were attributed to septic shock, congestive heart failure, severe community-acquired pneumonia, and stroke. The most common immediate cause of death was cardio-respiratory arrest. Source of admission, GCS level at admission, duration of ICU stay, treatment with inotropes, septic shock, and retroviral infection status were found to have a statistically significant association with ICU mortality.
Conclusion and Recommendations: This study revealed a significantly higher mortality rate among patients admitted to the intensive care unit. Early identification and admission of patients to the intensive care unit are important factors that could decrease mortality. Patient selection is essential since some patients with a high likelihood of mortality might not benefit from intensive care unit admission in an area with high resource limitations.
Keywords: intensive care unit, ICU mortality, determinants of ICU mortality
Background
The Intensive Care Unit (ICU) serves as a comprehensive and continuous care setting for patients who require frequent monitoring of vital signs, invasive hemodynamic monitoring, administration of intravenous medications, fluid management, ventilator support, and nutritional assistance. It is a specialized area within the hospital that is staffed by a multidisciplinary team and equipped with specialized resources to ensure the provision of safe and effective care for individuals with life-threatening illnesses.1
Intensive care units (ICUs) have enhanced the quality of care and outcomes for critically ill and injured patients, particularly in high-resource settings. Despite significant advancements in critical care services driven by technological progress and new scientific developments in treatment outcomes for critically ill patients worldwide, the progress of critical care service provision in resource-limited settings has been lagging behind, resulting in higher mortality rates.2,3
The ICU is currently the setting where the highest number of deaths occur in most hospitals. The global burden of ICU mortality has significant implications, leading to substantial losses in productivity and financial costs. The mortality rate varies across the world, depending on factors such as ICU infrastructure, staff availability, and training, as well as the cause of ICU admission. In the United States alone, there are approximately four million annual ICU admissions, with an average death rate ranging from 8% to 19%. Developed continents like North America, Oceania, Asia, and Europe have lower ICU mortality rates, with rates of 9.3%, 10.3%, 13.7%, and 18.7%, respectively. On the other hand, in South America and the Middle East, the mortality rates are higher, at 21.7% and 26.2%, respectively.3–5
In comparison to other developed continents, Africa has a high ICU mortality rate. Studies conducted in Nigeria, Tanzania, and Kenya showed that the ICU mortality rates of 32.9%, 40.1%, and 53.6%, respectively.6–8
Various studies conducted in Ethiopia have revealed that the mortality rate of ICU patients in the country is comparable to other African countries. A study conducted about a decade ago in Jimma and Addis Ababa reported ICU mortality rates of 37.7% and 39%, respectively.9–11 Additionally, recent studies conducted in Mekele, Gondar, and Bahir Dar within the past five years showed ICU mortality rates of 27%, 38.7%, and 29.6%, respectively. Furthermore, a multicentre cohort study conducted in Southern Ethiopia Comprehensive Hospitals revealed an ICU mortality rate of 46.8%.9,10,12–15
Predictors of in-hospital intensive care unit mortality include but are not limited to treatment with vasopressors, the presence of one or more severely deranged vital signs, advanced age, admission diagnosis, need for mechanical ventilation, length of stay in ICU, altered mental status and acute respiratory distress syndrome.8,11,16,17
Limited information is available regarding the factors that contribute to in-hospital mortality among patients admitted to an intensive care unit in the study setting. Thus, the objective of this study was to gather evidence on disease patterns, clinical outcomes, and associated factors among patients admitted to the Intensive Care Unit at Debre Berhan Comprehensive Specialized Hospital in Northeast Ethiopia. The findings of this study will be of significant practical value for healthcare providers, health planners, and researchers in improving patient care and outcomes.
Methods
Study Design and Setting
An institution-based retrospective cohort study was conducted by reviewing all available charts of ICU admitted medical patients at Debre Berhan Compressive Specialized Hospital (DBCSH) from March 2017 to February 2022. The hospital is located in Northeast Ethiopia, which is 130 km away from the capital city, Addis Ababa. The hospital has around 200 inpatient beds and 4 ICU beds that serve close to 3.5 million people in the surrounding area. There is only one common adult ICU serving for all adult patients in the hospital. The ICU has three mechanical ventilator machines and four noninvasive hemodynamic monitoring devices. The service operates within the Department of Internal Medicine and consists of a dedicated specialist (Internist), a general practitioner, and one nurse assigned to each patient. Additionally, anaesthetists are involved in the service when needed. There is no intensivist involved in the care of medical patients admitted to ICU. One nurse is assigned for one patient; however, these nurses are not specialized in ICU or critical care.
Study Subjects
The source population was all patients admitted to ICU of Debre Berhan Comprehensive Specialized Hospital, whereas the study population was all adult medical patients admitted to the ICU during the study period.
Sample Size and Sampling Procedure
A total of 896 patients were admitted to the facility from March 2017 to February 2022. Of these patients, 736 were classified as adult medical patients. However, 190 patients were excluded from the study due to either lost charts in the card room or incomplete data. Consequently, the final sample size for the study consisted of 546 medical patients.
Data Collection Instruments and Procedures
Data were collected through trained data collectors using a predesigned questionnaire that was developed after reviewing different literatures. Relevant medical history and laboratory parameters were obtained from patient records. The ICU admission/discharge logbook was used as an entry point to identify study subjects. Demographics, diagnosis, wards from which they were admitted, vital signs, lab investigations, and interventions received were extracted from the patients’ files. To ensure data quality, a training was given to the data collectors (two medical interns) and supervised by an internist. Before data processing, the information was checked for internal consistency and completeness.
Study Variables
Dependent variable: ICU mortality
Independent Variables:
- Sociodemographic characteristics: age, sex, marital status, educational status, and place of residence.
- Clinical Variables: Admission Diagnosis, vital signs at admission, Glasgow Coma scale at admission, comorbidities
- Interventions at Hospital: Antibiotics, the use of inotropes, treatment with Mechanical ventilators, cardiopulmonary resuscitation
- Miscellaneous Variables: Length of ICU stay, frequency of admission, source of admission, duration of mechanical ventilation
Inclusion and Exclusion Criteria
All adult medical patients admitted to the intensive care unit are included in the study. However, all adult medical patients with incomplete data and unknown outcomes were excluded from this study.
Data Processing and Analysis
Data were coded, recoded, cleaned, and explored to identify missing values and inconsistencies. Data were entered into EpiData V.3.1 and analysed by STATA 14.0. In the descriptive analysis, the mean with standard deviation, frequency, and percentages were calculated. Basic assumptions of logistic regression were checked. Both bivariate and multivariate logistic regression analyses were used to identify factors independently associated with mortality in ICU admitted patients. Those variables with p values of less than 0.2 in bivariate analysis were exported to multivariate analysis to control the possible effect of confounders. Adjusted odds ratio (AOR) with 95% confidence interval (CI) and p value <0.05 were used to select independently associated factors in patient mortality among patients admitted to the intensive care unit at DBCSH.
Results
Socio-Demographic Characteristics of Study Participants
A total of 546 medical patients were included in the study. The age of the study participants ranged from 18 to 97 with a mean age of 45 ±0.81. Two hundred fifty-two (46.2%) patients were males. The majority of the patients, 444 (81.3%), were admitted to the ICU for the first time (Table 1).
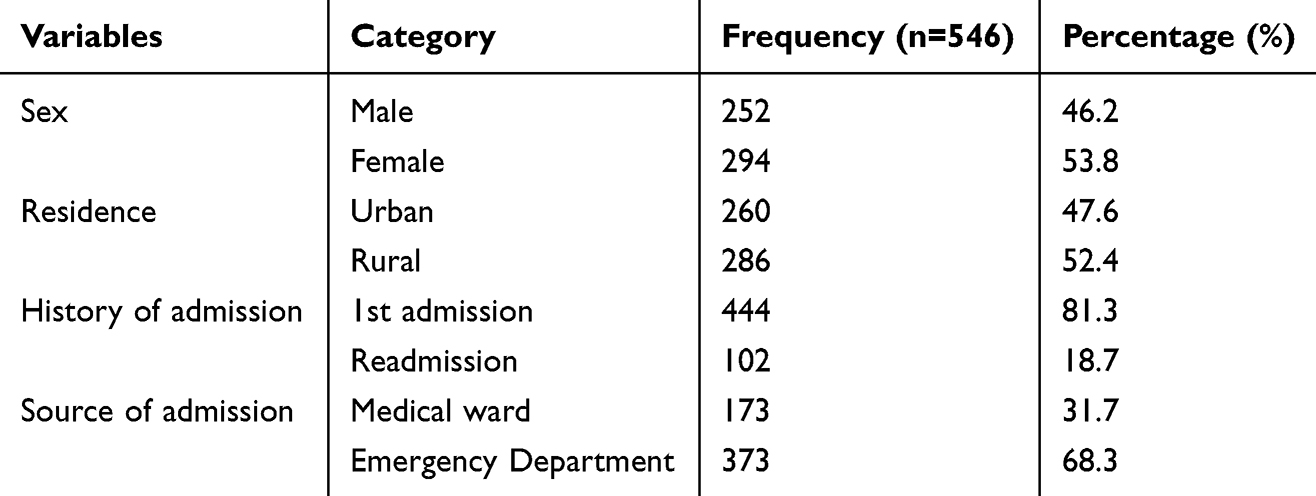 |
Table 1 Socio Demographic Variables of Medical Patients Admitted to ICU of DBCSH, March 2017 to February 2022 |
Primary Admission Diagnosis of Study Participants
When considering the disease categories, cardiovascular diseases, specifically acute coronary syndrome and congestive heart failure, were found to be the most prevalent, accounting for a total of 206 (37.7%) cases. Neurologic diseases, including stroke and meningitis, ranked as the second most common category, with 91 (16.7%) patients. Endocrine diseases, primarily diabetic ketoacidosis, were the third most prevalent, accounting for 70 (12.8%) cases. Respiratory diseases, mainly attributed to severe community-acquired pneumonia, were the fourth leading cause of admission, representing 59 cases or 10.8%. This was followed by infectious diseases, which accounted for 66 (12.1%) cases. Additionally, poisoning, predominantly organophosphate poisoning, accounted for approximately 38 (7%) of ICU admissions (Table 2).
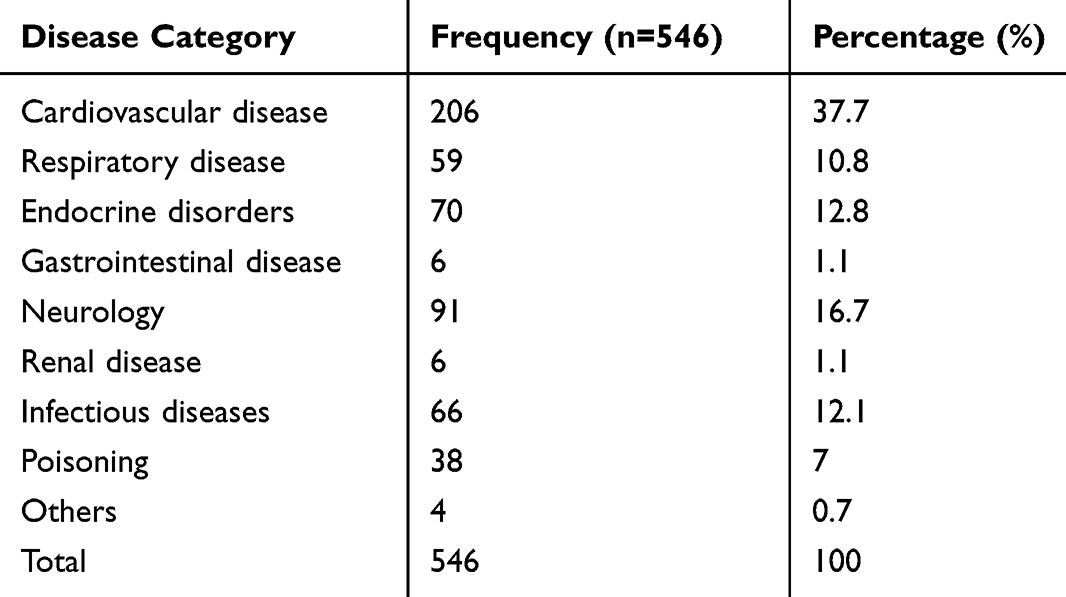 |
Table 2 Distribution of Disease Categories of Medical Patients Admitted to ICU DBCSH, from March 2017 to February 2022 |
Admission Vital Signs of Study Participants
Among the study participants, a significant majority of patients presented with one or more abnormal vital signs upon admission to the Intensive Care Unit (ICU). Specifically, 304 (55.7%) patients had an elevated pulse rate, while 259 (47.4%) exhibited abnormal blood pressure readings. Additionally, the majority of patients displayed elevated respiratory rates (328, 60.1%) and low oxygen saturation levels (272, 49.8%). In terms of consciousness, approximately 123 (22.5%) patients had a Glasgow Coma Scale (GCS) score of less than 8(Table 3).
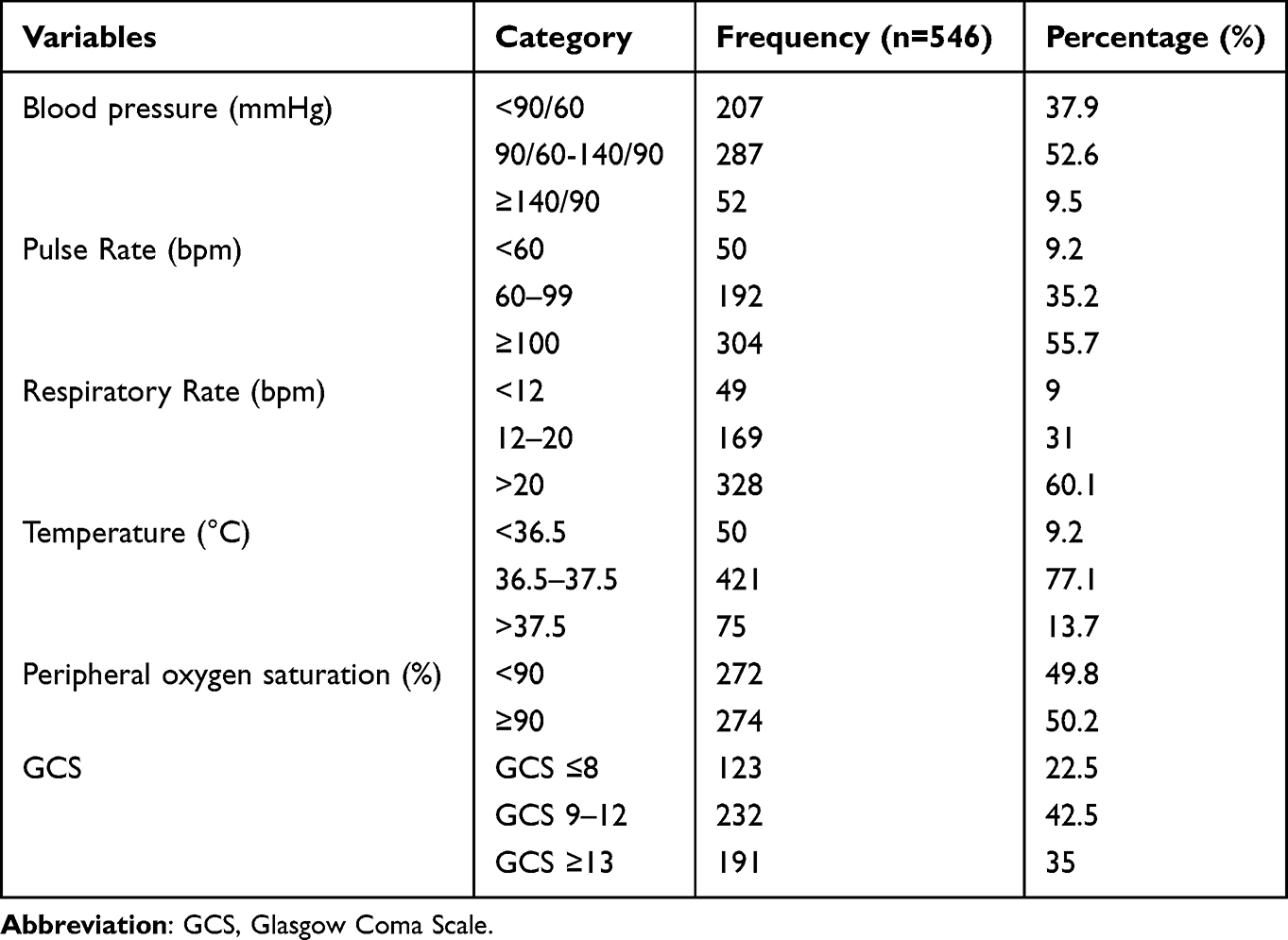 |
Table 3 Admission Vital Signs and GCS of Medical Patients Admitted to ICU DBCSH, from March 2017 to February 2022 |
Treatments and Interventions Given in the ICU
Among the patients admitted to ICU, 49 (9%) patients were put on mechanical ventilation with tracheal intubation, 456 (83.5%), 450 (82.4%), and 367 (67.2%) patients were given antibiotics, intravenous fluid, and analgesics, respectively. The mean duration of treatment of mechanical ventilation was 2.73 ± 0.59. The minimum and maximum lengths of stay in ICU were 1 day and 43 days, respectively, with a mean duration of 4.42 ± 0.18 days (Table 4).
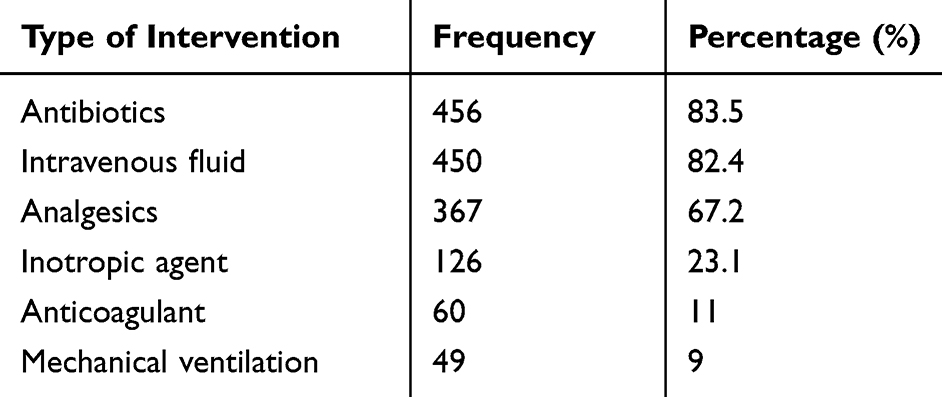 |
Table 4 Interventions Given to Admitted Patients to ICU of DBCSH, March 2017 to February 2022 |
Mortality Status of Patients Admitted to ICU
The overall ICU mortality rate was 35.9% (196 patients). Approximately half of the deaths were attributed to septic shock, congestive heart failure, severe community-acquired pneumonia, and stroke. The most common immediate cause of death was cardio-respiratory arrest. Around 3.1% of patients were found to be retroviral infected. About 68% of patients were directly admitted from medical emergency to ICU, and the rest were transferred from the medical wards. It was observed that only 57.2% of patients admitted from wards to the ICU survived, while approximately 67.3% of patients admitted directly from the medical emergency department survived (Table 5).
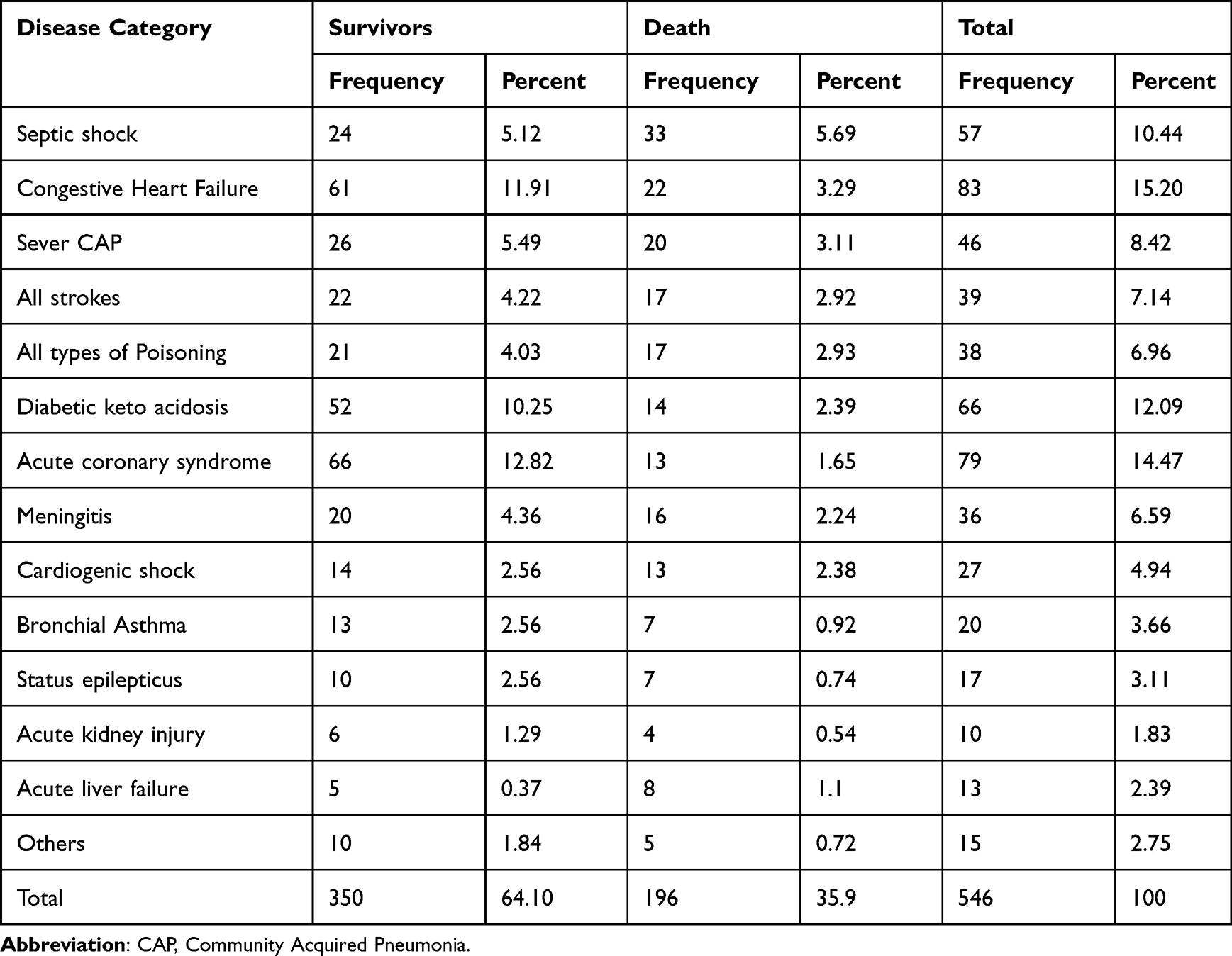 |
Table 5 Admission Diagnosis of Patients Admitted to ICU of DBCSH, March 2017 to February 2022 |
Factors Associated with ICU Mortality
The potential risk variables were checked for possible association using the chi2 test. Those independent variables that showed an association with the outcome variable (ICU mortality) were entered into the bivariate analysis (binary logistic regression) to quantify their association with the dependent variable (ICU mortality). Accordingly, source of admission, GCS level at admission, blood pressure at admission, respiratory rate at admission, body temperature at admission, duration of ICU stay, treatment with mechanical ventilator, treatment with inotropes, treatment with antibiotics, intravenous fluid therapy, diabetic keto acidosis, septic shock, cardiogenic shock, acute coronary syndrome, and RVI status were found to have p values of less than 0.2 and were entered into the multivariate logistic regression.
After computing the multiple logistic regression, source of admission, GCS level at admission, duration of ICU stay, treatment with inotropes, septic shock, and RVI status were found to have a statistically significant association with ICU mortality at P value <0.05 (Table 6).
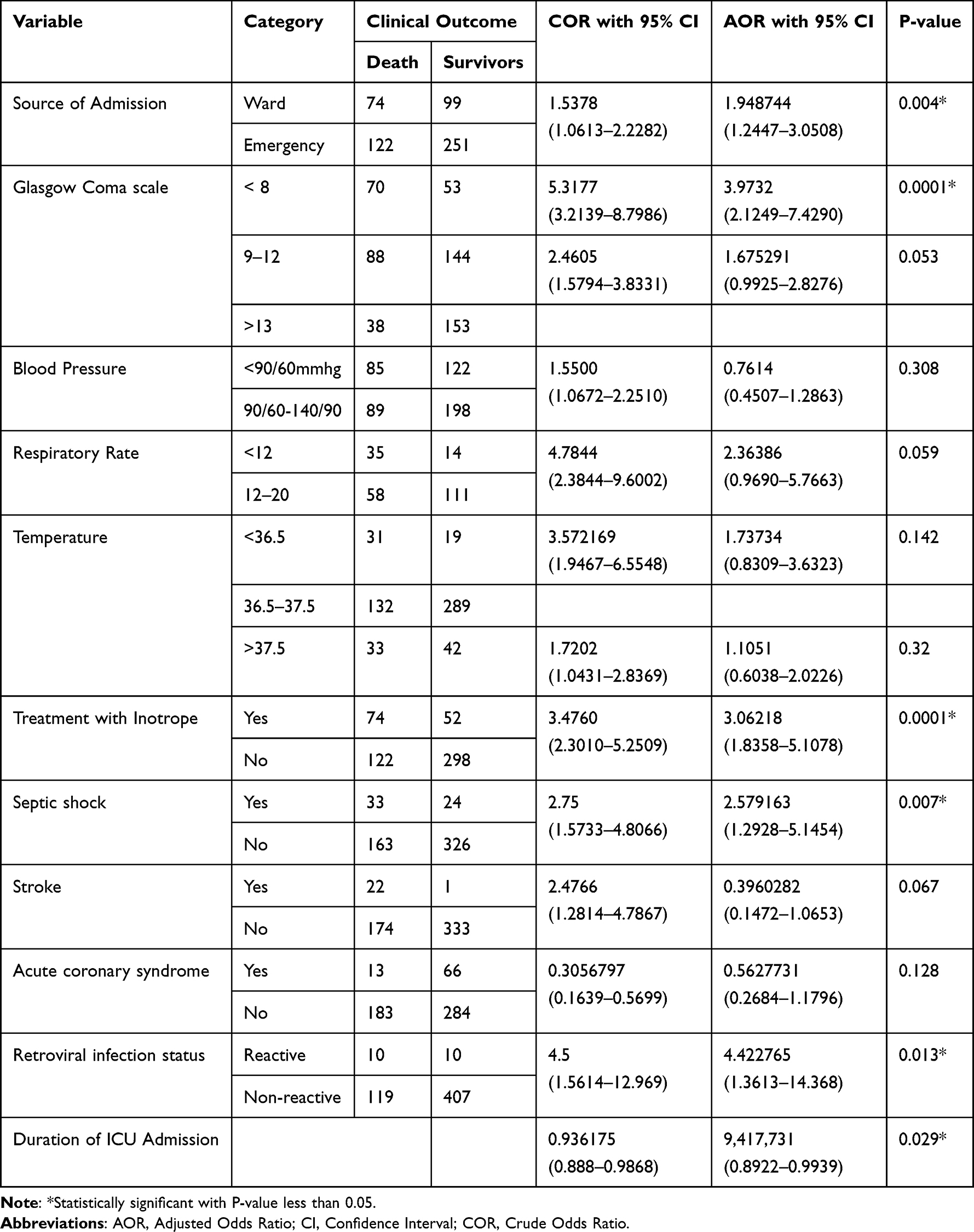 |
Table 6 Multivariate Analysis of Factors Associated with ICU Mortality in DCSH, from March 2017 to February 2022 |
Discussion
This study included a total of 546 medical patients admitted to the ICU. The overall mortality rate among these patients was 35.9%. The study was conducted in a healthcare setup characterized by limited availability and accessibility of resources required for intensive critical care. Additionally, updates or trainings for healthcare professionals in this setting are limited. Despite the presence of a rehabilitation service in the hospital, its focus is primarily on chronic physical therapies, and it does not fully support the needs of the intensive care unit (ICU) care team. Moreover, respiratory therapies are not available within this setup.
A large worldwide study involving 84 countries to assess the worldwide burden of critical illness in the ICU reported an overall mortality rate of 16.2%, suggesting that the current study had a higher rate of ICU mortality. One possible explanation for this difference could be the relatively small sample size and differences in the treatment setup among the patients included in this study.3
In comparison to the cross-sectional study conducted in Brazil from 2017 to 2018, which reported a 21% ICU mortality rate, this study once again found a significantly higher rate of ICU mortality. The difference in mortality rates could potentially be attributed to the differences in treatment setups, as this study was conducted in an area with limited resources and facilities.18
In contrast to the study conducted in Kenya from 2013 to 2015, which reported a 53% ICU mortality rate, the ICU mortality rate in this study is significantly lower. The disparity in mortality rates could potentially be attributed to a time gap between the two studies, which may reflect advancements in medical care and treatment strategies, differences in patient populations, and disparities in healthcare resources and infrastructure.8
This study revealed a similar ICU mortality rate when compared to previous Ethiopian studies conducted in Jimma, Addis Ababa, and Gondar. However, studies conducted in Mekele and Bahir Dar reported lower rates of ICU mortality than the current study. The disparity in mortality rates could potentially be attributed to variations in the setup and availability of human resources between the different study areas.9,12–14,16,19
Patients admitted from medical wards had a 1.95-fold increased likelihood of ICU mortality compared to patients who were directly admitted from a medical emergency (AOR = 1.948744, 95% CI: 1.2447–3.0508). This could be attributed to the delayed admission of patients from medical wards, resulting in a lack of early intervention and the development of complications prior to ICU admission. Other studies conducted in Brazil, Taiwan, United Kingdom, Turkey, and other systematic reviews and meta-analysis also showed a similar association between ICU mortality and delayed admissions.20–24
Patients with a Glasgow Coma Scale (GCS) score of less than 8 had an approximately fourfold higher likelihood of ICU mortality compared with patients with a GCS score of greater than or equal to 13 (adjusted odds ratio = 3.9732, 95% confidence interval: 2.1249–7.4290). Similar associations between GCS and ICU mortality were also observed in studies conducted in USA, Kenya, and Ethiopia.8,16,18,25
Patients who were treated with inotropes had an approximately threefold higher likelihood of dying in the ICU compared to those who were not treated with inotropes (adjusted odds ratio = 3.06218, 95% confidence interval: 1.8358–5.1078). Studies conducted in USA, France, and India also showed similar findings.26–28
Patients admitted to the ICU with an admission diagnosis of septic shock had a 2.5 times higher likelihood of dying in the ICU compared with patients admitted with other diagnoses (adjusted odds ratio = 2.579163, 95% confidence interval: 1.2928–5.1454). This could be explained due to the fact that septic shock is a condition with rapid progression, multiorgan involvement, immune system dysregulation, and treatment challenges compared to other diseases. Other studies conducted in Europe, North America, China, and sub-Saharan Africa also demonstrated that patients admitted with a diagnosis of septic shock had a higher likelihood of ICU mortality compared to patients admitted with other diagnoses.29–31
Patients with HIV comorbidity who were admitted to the ICU had an approximately 4.4 times higher risk of ICU mortality compared to patients without HIV comorbidity (AOR = 4.422765, 95% confidence interval: 1.3613–14.368). This strong association could be due to the fact that HIV infection is associated with an increased risk of severe infections, which in turn can contribute to higher ICU mortality rates. Other studies conducted in Africa also showed similar associations between HIV infection and ICU mortality.32
As the duration of ICU stay increases by one day, the likelihood of a patient dying in the ICU decreases by 6% (adjusted odds ratio = 0.9417731, 95% confidence interval: 0.8922–0.9939). This inverse association might be due to the fact that severely ill patients were more likely to die during the early stages of their illness and patients requiring a more extended stay in the ICU could have received intensive monitoring and treatment. A study conducted in Australia also showed most hospital deaths occurred within the first few days of ICU admission. Increasing length of hospital stay in ICU was not associated with an increased risk of in-hospital mortality.33
Limitations of the Study
This is a retrospective cohort study in which some of the determinant variables could not be accessed and included in the study. The relatively small sample size of the study might not reflect the real figure of ICU mortality. Patients with incomplete charts were not included in this study that could alter the findings.
Conclusions
This study revealed clear evidence of a significantly higher overall mortality rate among medical patients admitted to the ICU. Factors such as septic shock, retroviral infection, low GCS at admission, and the need for inotrope treatment at admission were associated with increased ICU mortality. Moreover, patients who were admitted to the ICU from medical wards had a higher risk of mortality compared to those admitted directly from medical emergencies, which indirectly suggests that delayed admission to the ICU might have contributed to increased ICU mortality rates. Additionally, this study showed that mortality rates are particularly high in the early days following ICU admission.
Recommendations
Early identification and admission of patients to ICU are important factors that could decrease ICU mortality. Patient selection is essential since some patients, like low GCS level, with high likelihood of mortality, might not benefit from ICU admission in an area with high resource and service limitations.
Abbreviations
AOR, Adjusted Odds Ratio, ARDS, Acute Respiratory Distress Syndrome; CHF, Congestive Heart Failure; CI, Confidence Interval; DBCSH, Debre Berhan Comprehensive Specialized Hospital; HIV, Human Immunodeficiency Virus; ICU, Intensive Care Unit.
Data Sharing Statement
The data used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
All methods of this research were done in accordance with the Declaration of Helsinki. Ethical clearance and approval to conduct the research was obtained from Debre Berhan University, Asrat Woldeyes Health Science Campus, Institutional Review Board (IRB) office. Official letters were written from the IRB office to the Debre Berhan Comprehensive Specialized Hospital. Formal letter of permission was obtained from Debre Berhan Comprehensive Specialized Hospital administrative body. Informed consent of study participants was exempted (waived) by the IRB office of the university since the study was a retrospective study based on the chart review of patients admitted to ICU and discharged over the past five years. The identity of the patients was coded and unspecified in the research process.
Acknowledgments
The authors greatly appreciate the cooperation and support of all participants and are grateful to data collectors and supervisors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is, in the conception, study design, execution, acquisition of data, analysis, interpretation, drafting, revising, and critically reviewing the article. All authors gave final approval of the version to be published; have agreed to the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors read and approved the final manuscript and approved its submission for publication.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Nates JL, Nunnally M, Kleinpell R, et al. ICU admission, discharge, and triage guidelines: a framework to enhance clinical operations, development of institutional policies, and further research. Crit Care Med. 2016;44(8):1553–1602. doi:10.1097/CCM.0000000000001856
2. van de Leur JP, van der Schans CP, Loef BG, Deelman BG, Geertzen JH, Zwaveling JH. Discomfort and factual recollection in intensive care unit patients. Critical Care. 2004;8(6):1–7. doi:10.1186/cc2976
3. Vincent J-L, Marshall JC, Ñamendys-Silva SA, et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. 2014;2(5):380–386. doi:10.1016/S2213-2600(14)70061-X
4. Lee PR ICU outcomes (mortality and length of Stay) methods, data collection tool and data, 2010. Institute for health policy studies State of California. Available from: http://healthpolicyucsfedu/content/icu-outcomes.
5. Rhodes A, Moreno RP. Intensive care provision: a global problem. Rev Bras Ter Intensiva. 2012;24(4):322–325. doi:10.1590/S0103-507X2012000400005
6. Kwizera A, Dünser M, Nakibuuka J. National intensive care unit bed capacity and ICU patient characteristics in a low income country. BMC Res Notes. 2012;5(1):1–6. doi:10.1186/1756-0500-5-475
7. Sawe HR, Mfinanga JA, Lidenge SJ, et al. Disease patterns and clinical outcomes of patients admitted in intensive care units of tertiary referral hospitals of Tanzania. BMC Int Health Hum Rights. 2014;14(1):1–8. doi:10.1186/1472-698X-14-26
8. Lalani HS, Waweru-Siika W, Mwogi T, et al. Intensive care outcomes and mortality prediction at a national referral hospital in Western Kenya. Ann Am Thoracic Soc. 2018;15(11):1336–1343. doi:10.1513/AnnalsATS.201801-051OC
9. Demass TB, Guadie AG, Mengistu TB, et al. The magnitude of mortality and its predictors among adult patients admitted to the intensive care unit in Amhara Regional State, Northwest Ethiopia. Sci Rep. 2023;13(1):12010. doi:10.1038/s41598-023-39190-7
10. Abate SM, Assen S, Yinges M, Basu B. Survival and predictors of mortality among patients admitted to the intensive care units in southern Ethiopia: a multi-center cohort study. Ann Med Surg. 2021;65:102318. doi:10.1016/j.amsu.2021.102318
11. Kachingwe M, Kazidule Kayambankadzanja R, Kumwenda Mwafulirwa W, Chikumbanje SS, Baker T, Thanachartwet V. Factors associated with in-hospital mortality of patients admitted to an intensive care unit in a tertiary hospital in Malawi. PLoS One. 2022;17(9):e0273647. doi:10.1371/journal.pone.0273647
12. Agalu A, Woldie M, Ayele Y, Bedada W. Reasons for admission and mortalities following admissions in the intensive care unit of a specialized hospital, in Ethiopia. Int J Med Med Sci. 2014;6(9):195–200. doi:10.5897/IJMMS2013.0883
13. Bayisa T, Berhane A, Kedir S, Wuletaw T. Admission patterns and outcomes in the medical intensive care unit of St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. Ethiopian Med J. 2017;55(1):19–26.
14. Kibreab Gidey MD, Abraha Hailu M. Pattern and outcome of medical intensive care unit admissions to ayder comprehensive specialized hospital In Tigray, Ethiopia. Age. 2018;20(184):15.
15. Tesema HG, Lema GF, Mesfin N, Fentie DY, Arefayne NR. Patterns of admission and clinical outcomes among patients admitted to medical intensive care unit of a teaching and referral hospital, Northwest Ethiopia. Global Adv Health Med. 2021;10:2164956121989258. doi:10.1177/2164956121989258
16. Endeshaw AS, Tarekegn F, Bayu HT, Ayalew SB, Gete BC. The magnitude of mortality and its determinants in Ethiopian adult intensive care units: a systematic review and meta-analysis. Ann Med Surg. 2022;84:104810. doi:10.1016/j.amsu.2022.104810
17. Vosylius S, Sipylaite J, Ivaskevicius J. Determinants of outcome in elderly patients admitted to the intensive care unit. Age Ageing. 2005;34(2):157–162. doi:10.1093/ageing/afi037
18. Soares Pinheiro FG, Santana Santos E, Barreto ID, et al. Mortality predictors and associated factors in patients in the intensive care unit: a cross-sectional study. Crit Care Res Pract. 2020;2020:1–6. doi:10.1155/2020/1483827
19. Demass TB, Guadie AG, Mengistu TB, et al. The Burden of intensive care unit mortality and the predictors in Amhara regional state, Northwest Ethiopia; 2022.
20. Cardoso LT, Grion CM, Matsuo T, et al. Impact of delayed admission to intensive care units on mortality of critically ill patients: a cohort study. Crit Care. 2011;15(1):1–8. doi:10.1186/cc9975
21. Kiekkas P, Tzenalis A, Gklava V, Stefanopoulos N, Voyagis G, Aretha D. Delayed admission to the intensive care unit and mortality of critically ill adults: systematic review and meta-analysis. Biomed Res Int. 2022;2022:1–16. doi:10.1155/2022/4083494
22. Hung S-C, Kung C-T, Hung C-W, et al. Determining delayed admission to the intensive care unit for mechanically ventilated patients in the emergency department. Crit Care. 2014;18(4):1–9. doi:10.1186/s13054-014-0485-1
23. Harris S, Singer M, Rowan K, Sanderson C. Delay to admission to critical care and mortality among deteriorating ward patients in UK hospitals: a multicentre, prospective, observational cohort study. Lancet. 2015;385:S40.
24. Sabaz MS, Asar S, Cukurova Z, Sabaz N, Dog H, Sertcakacilar G. Effect of delayed admission to intensive care units from the emergency department on the mortality of critically ill patients. Iran Red Crescent Med J. 2020;22(6). doi:10.5812/ircmj.102425
25. Rordorf G, Koroshetz W, Efird JT, Cramer SC. Predictors of mortality in stroke patients admitted to an intensive care unit. Crit Care Med. 2000;28(5):1301–1305. doi:10.1097/00003246-200005000-00007
26. Sonawane P, Jagtap BL, Chaudhury S. Inotrope use in critically ill patients: prevalence and effects on mortality. Pravara Med Rev. 2016;8:4.
27. Gao F, Zhang Y. Inotrope use and intensive care unit mortality in patients with cardiogenic shock: an analysis of a large electronic intensive care unit database. Front Cardiovasc Med. 2021;8:696138. doi:10.3389/fcvm.2021.696138
28. Motiejunaite J, Deniau B, Blet A, Gayat E, Mebazaa A. Inotropes and vasopressors are associated with increased short-term mortality but not long-term survival in critically ill patients. Anaesth Crit Care Pain Med. 2022;41(1):101012. doi:10.1016/j.accpm.2021.101012
29. Vincent J-L, Jones G, David S, Olariu E, Cadwell KK. Frequency and mortality of septic shock in Europe and North America: a systematic review and meta-analysis. Critical Care. 2019;23(1):1–11. doi:10.1186/s13054-019-2478-6
30. Zhou J, Qian C, Zhao M, et al. Epidemiology and outcome of severe sepsis and septic shock in intensive care units in mainland China. PLoS One. 2014;9(9):e107181. doi:10.1371/journal.pone.0107181
31. Metogo Mbengono JA, Tochie JN, Ndom Ntock F, et al. The epidemiology, therapeutic patterns, outcome, and challenges in managing septic shock in a sub-saharan African intensive care unit: a cross-sectional study. Hosp Pract Res. 2019;4(4):117–121. doi:10.15171/hpr.2019.24
32. Kwizera A, Nabukenya M, Peter A, et al. Clinical characteristics and short-term outcomes of HIV patients admitted to an African intensive care unit. Crit Care Res Pract. 2016;2016:1–7. doi:10.1155/2016/2610873
33. Williams T, Ho K, Dobb G, Finn J, Knuiman M, Webb S. Effect of length of stay in intensive care unit on hospital and long-term mortality of critically ill adult patients. Br J Anaesth. 2010;104(4):459–464. doi:10.1093/bja/aeq025
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.