Back to Journals » Journal of Inflammation Research » Volume 17
Despite Recovery from Necrotizing Enterocolitis Infants Retain a Hyperinflammatory Response to Injury
Authors Snyder KB ![]() , Calkins CL
, Calkins CL ![]() , Golubkova A, Leiva T, Schlegel C, Hunter CJ
, Golubkova A, Leiva T, Schlegel C, Hunter CJ
Received 13 September 2023
Accepted for publication 19 December 2023
Published 17 January 2024 Volume 2024:17 Pages 331—341
DOI https://doi.org/10.2147/JIR.S436125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam Bachstetter
Katherine B Snyder,1,2 Chase L Calkins,3 Alena Golubkova,1,2 Tyler Leiva,1,2 Camille Schlegel,1 Catherine J Hunter1,2
1Division of Pediatric Surgery, Oklahoma City, OK, 73104, USA; 2Department of Surgery, The University of Oklahoma Health Sciences Center, Oklahoma City, OK, 73104, USA; 3College of Medicine, The University of Oklahoma College of Medicine, Oklahoma City, OK, 73104, USA
Correspondence: Catherine J Hunter, Department of Pediatric Surgery, Oklahoma Children’s Hospital, 1200 Everett Drive, ET NP 2320, Oklahoma City, OK, 73104, USA, Email [email protected]
Background: Necrotizing enterocolitis (NEC) is the leading gastrointestinal cause of death of premature neonates. NEC is associated with prematurity, a hyperinflammatory response, and dysregulation of intestinal barrier function. We hypothesize that patients with NEC will have, and continue to have after recovery, an increased hyperinflammatory intestinal response compared to those patients without NEC.
Methods: Neonates with NEC, those that have recovered from NEC, and those without NEC undergoing intestinal resections had specimens collected and snap frozen or generated into enteroids. The enteroids were treated with 100ug/mL lipopolysaccharide (LPS) and subjected to 24 hr of hypoxia together, then compared with untreated controls. Expression of Tumor Necrosis Factor (TNF-α) and interleukin 8 (IL-8) were evaluated via RT-qPCR and ELISA to measure inflammatory response. ANOVA determined statistical significance (p< 0.05).
Results: There was no difference in inflammatory markers in recovered NEC tissue compared to non-NEC tissue on RTqPCR (p=0.701 TNF-α and 0.861 IL-8). However, recovered NEC enteroids demonstrate elevated levels of inflammatory markers after treatment compared to non-NEC enteroids after treatment on RTqPCR (p=0.0485 TNF-α, p=0.0057 IL-8) and ELISA (p=0.0354 TNF-α, p=0.0011 IL-8). Recovered NEC enteroids that underwent treatment demonstrated increased inflammatory markers compared to recovered NEC enteroids without treatment on RTqPCR (p=0.0045 TNF-α, p=0.0002 IL-8) and ELISA (p=0.034 TNF-α, p=0.0002 IL-8) suggesting a heightened inflammatory response to a second hit.
Conclusion: Intestinal tissue resected from neonates with NEC has an elevated hyperinflammatory response compared to neonates recovered from NEC and neonates without NEC. Enteroids generated from patients that have recovered from NEC have a heightened inflammatory response in response to NEC inducing stimuli compared to controls. This tendency towards an increased hyperinflammatory state may be correlated with an infant’s proclivity to develop NEC and demonstrates the significance of a second hit on this tissue creating a heightened inflammatory response. This could be correlated with the impact and trajectory of an illness post recovery from NEC.
Keywords: necrotizing enterocolitis, recovery, hyperinflammatory, enteroids
Introduction
Necrotizing enterocolitis (NEC) is a devastating disease of premature neonates characterized by significant intestinal injury with severe morbidity and mortality.1,2 There are well-established associations with the disease including prematurity, early enteral feeding with formula feeds, intestinal barrier disruption, and an unregulated hyperinflammatory response.3,4 Despite these known associations and significant advances in care for these neonates, pathogenesis remains incompletely understood.1,4,5
Premature neonates appear to have a heightened inflammatory state as demonstrated through studies of the premature immune response in extrauterine life, this could have implications in NEC development, however this has yet to be fully elucidated.6–8 The inflammatory cascade is recognized to play a significant role in the development of NEC, however the timing and significance of this needs to be further explored.4 To achieve this, our lab has demonstrated that enteroids taken from patients with NEC are more hyperinflammatory at baseline and have a heightened response to additional insult.4,9 We aim to describe this hyperinflammatory response following recovery from NEC and determine its significance.
While there are a paucity of data regarding the two- hit hypothesis specifically for NEC, the idea itself is well described in literature for a variety of disease processes. In regards to the gastrointestinal tract, inflammatory bowel disease (IBD) literature explores the two-hit hypothesis. Even though NEC and IBD are distinct disease processes, we postulate that a similar principle may apply to NEC. In IBD, it is thought that genetic susceptibility mediated by a dysfunctional immune system and commensal bacteria play a role in the development of intestinal inflammation, and a second hit from environmental factors can affect disease development further.10 To explore this two-hit hypothesis in NEC, we investigated the inflammatory cascade using human tissue, and human-derived enteroids from patients with and without NEC and post-recovery from NEC.
Materials and Methods
Human Samples
Following institutional review board approval (IRB #11610-11,611) and parental consent, we collected human neonatal intestinal tissue from patients already undergoing bowel resection at the Oklahoma Children’s Hospital in Oklahoma City, OK. For this study, premature infant patients were included, with one patient with active NEC, one patient without NEC, and one patient that had fully recovered from NEC. Tissue specimens were divided after collection and subsequently snap frozen in liquid nitrogen or washed in cold Dulbecco’s phosphate-buffered saline (DPBS, Sigma Life Science, #D8573, St. Louis, MO) then kept in Roswell Park Memorial Institute media (Gibco, #11875-093, Waltham, MA) for 24 hr or less until processed for enteroid culture. Enteroids were developed from each of the three patients used for this particular set of experiments.
In vitro Human Neonatal Enteroid Cultures
Within 24 hr from collection, intestinal crypts were isolated from the samples and enteroid cultures were generated per our previously described protocol used for crypt isolation and enteroid processing.11 Following this, the enteroid cultures were suspended in basement membrane matrix, Matrigel (Corning, #CB-40230C, Corning, NY) domes and grown in 50% L-WRN conditioned media, which is supplemented with 50 ng/mL epidermal growth factor (Millipore Sigma, #GF144, Burlington, MA), 1 mM N-Acetylcysteine (Millipore Sigma, #A9165-5G, Burlington, MA), 500nM A-83-01 (R&D Systems, #2939/10, Minneapolis, MN), 10uM SB202190 (Millipore Sigma, #S7067-5 MG, Burlington, MA), 10 mM Nicotinamide (Millipore Sigma, #N0636-100G, Burlington, MA), and 10nM [leu] 15-gastrin 1 (Millipore Sigma, #G9145-0.1 MG). All enteroids were passaged every 5–7 days and experimented on when at full maturity, between passages 4 and 10 for all experiments.
Enteroid NEC Experimentation
The enteroid cultures were grown in the basement membrane matrix, Matrigel, with the supplemented media for 7–21 days. For all experiments, the enteroids were mature at the time of experimentation determined by visualization of blebbing and ensuring they were 7 days from the last passage. There were on average, 300 enteroids per well at time of experimentation. Our lab has previously described a protocol for NEC induction in enteroids in vitro, and this protocol was followed for 24 hr.9 For each set of experiments, one set of enteroids underwent treatment consisting of 100 ug/mL lipopolysaccharide injection into the supplemented media along with 24 hr of hypoxia to induce NEC. This time point was chosen per prior published protocols to induce in vitro NEC without causing frank necrosis per previous protocols.11,12 In order to create a translational ex vivo model similar to mammalian model systems of NEC, hypoxia for 24 hr has been chosen to supplement LPS exposure for 24 hr.11,13 The other set of enteroids was untreated and used as control enteroids. Enteroids derived from three different patients were used for all experiments and controls. For each experiment, enteroids from a patient with NEC were compared to enteroids from a patient without NEC for three different sets and age matched to comparable cGA. The following sets were compared: enteroids from a patient with active NEC to enteroids from a patient that has recovered from NEC and enteroids from a patient that has recovered from NEC to enteroids from a patient without NEC. All experiments were performed in triplicate to enhance scientific rigor.
RNA Isolation, Reverse Transcription, and RTqPCR of Enteroids
Total RNA was isolated and extracted using TRIzol (Life Technologies, Carlsbad, CA) RNA was quantified for purity (2.0–2.1 A260/A280 ratio) and quantity using a NanoDrop Lite spectrophotometer (Thermo Scientific, Waltham, MA). RNA was then reverse transcribed to 0.5–2ug of complementary DNA (cDNA) using high capacity cDNA reverse transcription kit (Applied biosystems, #4374966, Waltham, MA). Real-time PCR results were obtained using the CFX Opus 96 system an iQ SYBR Green Supermix (Biorad, Hercules, CA) with 4ng of cDNA template and the final primer concentration was 0.5 uM. Expression levels were quantitated and normalized to GAPDH. The following primers were used for amplification of target cDNA: TNF-α, 5’ TGA GGT ACA GGC CCT CTG AT 3’ and 5’ CTC GAA CCC CGA GTG ACA AG 3’; IL-8, 5’ GGC CGT GGC TCT CTT GGC AG 3’ and 5’ TGT GTT GGC GCA GTG TGG TCC 3’; GAPDH, 5’ TCA AGG CTG AGA ACG GGA AG 3’ and 5’ CGC CCC ACT TGA TTT TGG AG 3’.
Enzyme Linked Immunosorbent Assay
For each set of experiment comparisons, the enteroid media was isolated and enzyme-linked immunosorbent assay was performed for TNF-α (KHC3011) and IL-8 (KHC0081) (Invitrogen, Waltham, MA).
RNA Isolation, Reverse Transcription, and RTqPCR of Tissue
Total RNA isolation was performed from snap frozen tissue beginning with homogenization using the Fisher Brand Pellet Pestle cordless motor (Fisher Scientific, Hampton, NH) and VWR disposable pestles (VWR, Radnor, PA). Samples were then further homogenized using Qiagen QIAshredder homogenization columns (Qiagen, Hilden, Germany) directly before RNA purification using a Qiagen RNeasy mini kit (Qiagen, Hilden, Germany). RNA was quantified for purity (2.0–2.1 A260/A280 ratio) and quantity using a NanoDrop Lite spectrophotometer (Thermo Scientific, Waltham, MA). RNA was reverse transcribed to a concentration of 100 ng/ul of cDNA using an Applied Biosystems (Waltham, MA) High-Capacity cDNA Reverse Transcription Kit with RNase Inhibitor. Quantitative Real-Time Polymerase Chain Reaction was performed using the CFX Opus 96 Real-Time PCR system (BioRad, Hercules, CA) and iQ SYBR Green Supermix (BioRad, Hercules, CA) using 4ng of cDNA template and 0.5uM final primer concentration. Relative gene expression was analyzed using the ΔΔCq method and normalized to GAPDH using the BioRad CFX Maestro software (BioRad, Hercules, CA). The following primer sequences were used for amplification of target cDNA: TNF-α, 5’ TGA GGT ACA GGC CCT CTG AT 3’ and 5’ CTC GAA CCC CGA GTG ACA AG 3’; IL-8, 5’ GGC CGT GGC TCT CTT GGC AG 3’ and 5’ TGT GTT GGC GCA GTG TGG TCC 3’; GAPDH, 5’ TCA AGG CTG AGA ACG GGA AG 3’ and 5’ CGC CCC ACT TGA TTT TGG AG 3’.
Illumina RNA-Sequencing
Stranded RNA-seq libraries were constructed using NEBNext poly(A) mRNA isolation kit with the IDT’s xGen Broad-range RNA Library Prep Kit and the established protocols (New England Biolabs NEBNext, Ipswich MA, and Integrated DNA Technologies IDT, Coralville IA). The library construction was done using 1μg of RNA. Each of the libraries was indexed during library construction in order to multiplex for sequencing. Samples were normalized and pooled onto a 150 paired end run on Illumina’s NextSeq 2000 Platform (Illumina, San Diego, CA). A heat map of the top 30 differentially expressed genes was then generated as an output of the standard pipelines built into the DRAGEN Differential Expression v4.0.3 app in Illumina’s BaseSpace as aligned quant.sf files (Illumina, San Diego, CA).
Statistical Analysis
For all statistical analysis and result graphing, GraphPad Prism 9.4.0 (Graph Pad Software, San Diego, CA) was used. Student’s t-test and analysis of variance were used as appropriate for data within a normal distribution. Statistical significance was accepted if p<0.05.
Results
All of the following specimens were obtained from three patients undergoing a variety of operations including those for active NEC, intestinal atresia repair, and ostomy reversal. For each specimen, we noted the anatomic site obtained (ileum, jejunum, etc.), type of surgical procedure, and surgical histories for each patient. We also noted the age at birth, age at resection, and corrected gestational age. Patients included both male and female patients and all were premature. Corrected gestation age (cGA) of infants at the time of collection ranged from 36 weeks and 1 day to 46 weeks and 6 days. Among these infants, one underwent intestinal resections for active NEC, one underwent resection for an ostomy takedown following recovery from NEC, and one underwent resection for intestinal stricture repair. Recovery from NEC was determined by the patient’s ability to tolerate enteral feeds, have adequate ostomy output, and labs and vital signs within normal limits prior to ostomy reversal. In this study, the operation for the patient that had recovered from NEC was performed over 14 weeks following the active NEC infection and the patient had a full clinical recovery as determined from the criteria above.
Tissue Samples from a Patient with Active NEC Compared to Tissue Samples from a Patient Without NEC
Tissue resected from patients with NEC that was snap frozen immediately following resection expressed significantly higher levels of TNF-α when compared to tissue resected from patients without NEC that was immediately snap frozen following resection seen on RTqPCR (p=0.006). In addition to this, tissue resected from NEC patients expressed significantly higher levels of IL-8 when compared to tissue resected from non-NEC patients (RTqPCR p=0.031). Elevated levels of TNF-α and IL-8 in the tissue resected from patients with NEC at time of resection support our hypothesis that patients with NEC are in an elevated hyperinflammatory state (Figure 1).
 |
Figure 1 Expression of TNF-α and IL-8 in active NEC, recovered NEC, and non-NEC snap frozen tissue samples on RTqPCR. There is a significant difference seen in both TNF-α and IL-8 expression when comparing active NEC tissue to recovered NEC tissue (p=0.014 TNF-α and p=0.049 IL-8) and to non-NEC tissue (p=0.006 TNF-α and p=0.031 IL-8). There is no significant difference seen when comparing recovered NEC tissue to non-NEC tissue (p=0.701 TNF-α and 0.861 IL-8). (*Denotes significance, with increasing number of *Denoting increased significance; ns denotes no significance). |
Tissue Samples from a Patient That Have Recovered from NEC Compared to Tissue Samples from a Patient Without NEC
Tissue resected from patients that have recovered from NEC show no statistically significant difference in levels of TNF-α and IL-8 when compared to tissue resected from patients without NEC and immediately snap frozen. However, there is an upward trend in inflammatory markers seen in the tissue from recovered NEC patients compared to tissue from patients without NEC. This can be seen on RTqPCR (p=0.701 TNF-α and 0.861 IL-8). This suggests that despite clinical recovery from NEC that the tissue response from these patients is not significantly different from patients without NEC, in that they trend towards a greater hyperinflammatory state at baseline (Figure 1).
Tissue Samples from a Patient That Have Recovered from NEC Compared to Tissue Samples from a Patient with Active NEC
Intestinal tissue resected from patients with active NEC show a statistically higher inflammatory cytokine response when compared to tissue resected from patients that have fully recovered from NEC that was immediately snap frozen following resection. This is noted both in TNF-α expression and IL-8 expression by RTqPCR (p=0.014 TNF-α and p=0.049 IL-8). Taken together with the above results, this is supportive of patients with active NEC being in a heightened inflammatory state that trends downward as they recover (Figure 1).
Enteroids Derived from Tissue from a Patient with Active NEC Compared to Enteroids Derived from Tissue from a Patient That Has Recovered from NEC
Enteroids generated from patients with NEC who underwent treatment with LPS and hypoxia demonstrated significantly higher levels of TNF-α when compared to untreated NEC derived enteroids seen on RTqPCR (p=0.0003) and ELISA (p<0.0023). Furthermore, NEC derived enteroids that underwent treatment had significantly higher levels of TNF-α when compared to enteroids developed from tissue without NEC that underwent treatment as seen on RTqPCR (p=0.0039) and ELISA (p=0.0061) (Figure 2).
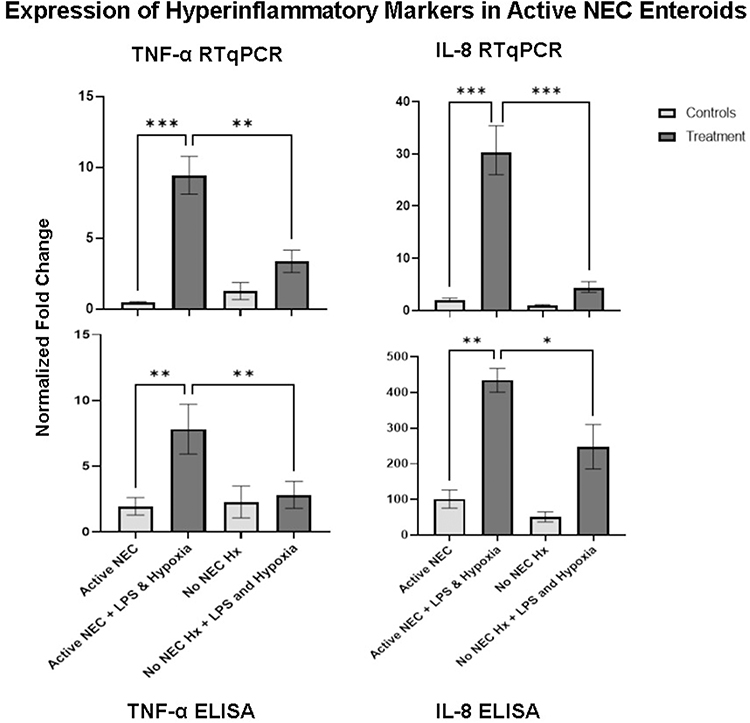 |
Figure 2 Expression of TNF-α and IL-8 in active NEC enteroids and non-NEC enteroids. NEC enteroids that underwent treatment demonstrate elevated levels of both inflammatory markers when compared to untreated NEC enteroids and treated non-NEC enteroids seen on RTqPCR and ELISA. (TNF-α RTqPCR p=0.0003 and p=0.0039 respectively, ELISA p<0.0023 and p=0.0061 respectively) (IL-8 RTqPCR p<0.0001 and p=0.0001 respectively, ELISA p=0.0012 and p=0.0352 respectively). (*Denotes significance, with increasing number of *Denoting increased significance). |
Enteroids generated from patients with NEC who underwent treatment with LPS and hypoxia display significantly higher amounts of RNA and increased protein levels of IL-8 (RTqPCR (p<0.0001) and ELISA (p=0.0012)) when compared to untreated NEC-derived enteroids. A significantly higher level of IL-8 demonstrated in NEC-derived enteroids compared to enteroids from normal control patients following LPS and hypoxia treatment seen on RTqPCR (p=0.0001) and ELISA (P=0.0352). These findings are interesting because they suggest that there is an elevated hyperinflammatory response in response to an insult, the treatment with LPS and hypoxia (Figure 2).
Enteroids Derived from a Patient That Has Recovered from NEC Compared to Enteroids Derived from a Patient Without NEC
Enteroids developed from a patient that has fully recovered from NEC demonstrate significantly elevated levels of inflammatory marker TNF-α when subjected to NEC inducing treatment compared to enteroids developed from a patient without NEC that underwent NEC inducing treatment seen on RTqPCR (p=0.0485) and ELISA (p=0.0354). When comparing recovered NEC enteroids that underwent treatment to recovered NEC enteroids that did not undergo treatment, there was a significant difference in the amount of TNF-α present as well demonstrated with RTqPCR (p=0.0045) and ELISA (p=0.034) (Figure 3).
 |
Figure 3 Expression of TNF-α and IL-8 in recovered NEC enteroids and non-NEC enteroids. Recovered NEC enteroids demonstrate elevated inflammatory markers when compared to non-NEC enteroids that underwent treatment and when compared to recovered NEC enteroids that did not undergo treatment on both RTqPCR and ELISA. (TNF-α RTqPCR p=0.0485 and p=0.0045 respectively, ELISA p=0.0354 and p=0.034 respectively) (IL-8 RTqPCR p=0.0057 and p=0.0002 respectively, ELISA p=0.0011 and p=0.0002 respectively). (*Denotes significance, with increasing number of *Denoting increased significance). |
This was further demonstrated when analyzing IL-8 expression in these enteroids. When comparing recovered NEC enteroids that underwent treatment to non-NEC enteroids that underwent treatment, there was a significant elevation of IL-8 demonstrated on RTqPCR (p=0.0057) and on ELISA (p=0.0011). When comparing recovered NEC enteroids that underwent treatment to recovered NEC enteroids that did not undergo treatment, there again was a significant elevation in IL-8 seen on RTqPCR (p=0.0002) and ELISA (p=0.0002). These results are interesting and show that patients with a history of NEC appear to remain primed for an elevated hyperinflammatory response compared to patients without NEC when subjected to an insult of LPS and hypoxia (Figure 3).
Enteroids Derived from a Patient That Has Recovered from NEC Compared to Enteroids Derived from a Patient with Active NEC
When comparing the enteroids from patients that have both had NEC, one with active NEC and one fully recovered from NEC, RTqPCR continues to demonstrate elevated levels of TNF-α between treated active NEC enteroids and untreated active NEC enteroids on RTqPCR (p=0.002) and ELISA (p=0.0116). Moreover, there is a significant difference when comparing treated recovered NEC enteroids and untreated recovered NEC enteroids on RTqPCR (p=0.002) and ELISA (0.0348). However, there is no significant difference when comparing treated active NEC enteroids to treated recovered NEC enteroids (Figure 4).
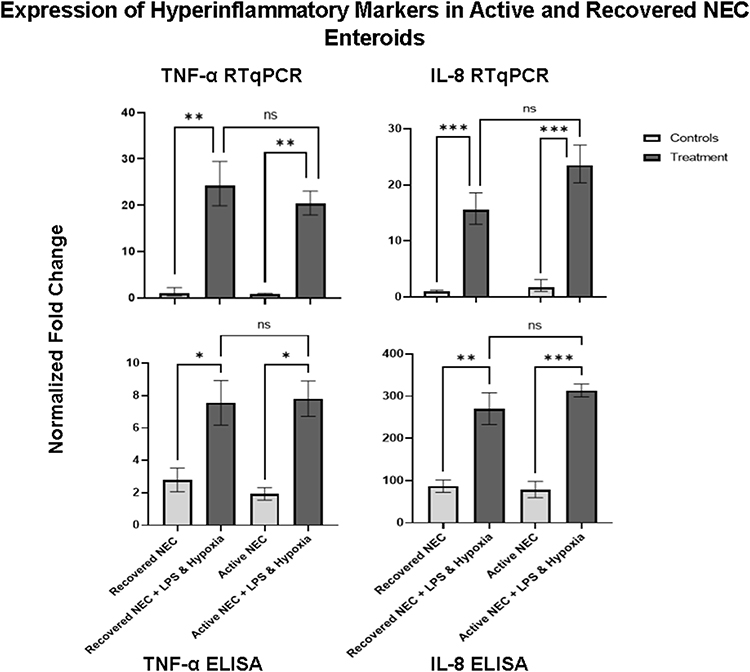 |
Figure 4 Expression of TNF-α and IL-8 in active NEC enteroids and recovered enteroids. Recovered NEC enteroids that underwent treatment demonstrate elevated inflammatory markers when compared to recovered NEC enteroids that did not undergo treatment on both RTqPCR and ELISA. (TNF-α RTqPCR p=0.002, ELISA p=0.0348) (IL-8 RTqPCR p=0.001, ELISA p=0.0027). Active NEC enteroids demonstrate elevated inflammatory markers when compared to active NEC enteroids that did not undergo treatment on RTqPCR and ELISA. (TNF-α RTqPCR p=0.002, ELISA p=0.0116) (IL-8 RTqPCR p=0.001, ELISA p=0.0005). (*Denotes significance, with increasing number of *Denoting increased significance; ns denotes no significance). |
When performing the same comparisons with hyperinflammatory marker IL-8 there are significantly elevated levels of IL-8 between treated active NEC enteroids and untreated active NEC enteroids seen on RTqPCR (p=0.001) and ELISA (p=0.0005). There is also a significant difference when comparing treated recovered NEC enteroids and untreated NEC enteroids on RTqPCR (p=0.001) and ELISA (0.0027). There is no significant difference when comparing treated active NEC enteroids to treated recovered NEC enteroids (Figure 4).
These results showcase an interesting phenomenon in our enteroid model, which allows us to perform a second hit with the LPS and hypoxia treatment. The enteroids from both active NEC and recovered NEC tissue display a robust hyperinflammatory response compared to controls following treatment, indicating that they are primed for an elevated hyperinflammatory response even post recovery from NEC.
RNA-Sequencing of Enteroids Derived from Patients with Active NEC, Recovered from NEC, and a Patient Without NEC
When comparing RNA-sequencing of control active NEC, recovered NEC, and non-NEC enteroids RNA to treated active NEC, recovered NEC, and non-NEC enteroids RNA a total of 60,610 genes were constructed in the library. Within the top 30 differentially expressed genes, 9 are genes involved in the inflammatory response. Of these genes, there was a statistically significant difference seen in the expression when comparing control enteroids versus enteroids that underwent NEC induction with treatment of LPS and hypoxia (p<0.0001) (Figure 5). This is supportive of our hypothesis that patients with NEC and those recovered from NEC have an increased proclivity to a hyperinflammatory state and tend to become even more hyperinflammatory following a second hit insult.
 |
Figure 5 RNA-sequencing genes involved in the inflammatory response within the top 30 differentially expressed genes in control versus experiment NEC enteroids. There are 9 genes within the top 30 of 60,610 genes expressed on RNA sequencing of control (untreated) and experiment (treated) NEC derived enteroids. (*Denotes significance). |
Discussion
The proinflammatory cascade is widely accepted to be activated during NEC. This is supported by an extensive body of prior data, both in animal and human tissue.9,11,13–15 Although infants that develop NEC are typically premature, not all infants who are premature will develop NEC. This makes the identifying those “at risk” infants within the premature subpopulation particularly necessary. Potentially, this may allow for better risk stratification of infants and opportunities for early intervention. Our data supports the idea that certain infants may harbor a tendency towards a hyperinflammatory state, even after recovery. Indeed, these studies may provide insights into why one infant develops NEC over another.9
Until recently, the extent of the hyperinflammatory state that is seen in intestinal injury in NEC had not been fully described.4,16,17 We have demonstrated a significant inflammatory response in an enteroid model of NEC and provided data indicating a persistent proclivity to hyperinflammation.9 In addition to this, we were able to delineate the impact of a “second hit” by analyzing tissue and enteroids that have clinically fully recovered from NEC.
We have previously demonstrated that enteroids derived from premature infants provide an in vitro model for studying NEC that closely mimics clinical NEC.9,12 Enteroids maintain the characteristics from the host from which they were derived at the time of intestinal resection, making them an ideal model for studying clinical conditions in vitro.12 This retained intrinsic memory has allowed us to utilize this human-derived enteroid model to closely mimic the impact of a second hit clinically on a patient that has fully recovered from NEC.
In our prior studies, we have shown that there is a marked increase in hyperinflammatory response demonstrated when comparing enteroids from patients with active NEC to those without NEC, with an even further increase demonstrated after undergoing induction of NEC in vitro.9 This study supported our original hypothesis that NEC patients are more hyperinflammatory at baseline and have a heightened response to additional injury. When studying this same profile of enteroids and inducing NEC in the enteroids as previously described, we were able to reproduce these results with a consistent increase in hyperinflammatory markers demonstrated in those with active NEC and more so following in vitro induction of NEC.
Through further study of this phenomenon, we were able to analyze the second hit that enteroids received when undergoing NEC induction in vitro by comparing enteroids from patients with active NEC to patients that have recovered from NEC more extensively through both tissue and enteroid analysis. When comparing tissue from patients that have reached full clinical recovery to tissue from those with active NEC and tissue from patients without NEC immediately following resection, there is a clear difference in the number of inflammatory markers between active NEC and the recovered NEC, while there is no difference seen between recovered NEC and the control. However, when analyzing enteroids made from this tissue after the treatment of LPS and hypoxia for induction of a second hit, there is a significant increase in the number of inflammatory markers in the recovered NEC enteroids when compared to control enteroids, and now no significant difference is seen between the recovered NEC enteroids and the active NEC enteroids. Representing the impact of a second hit on the underlying hyperinflammatory state in these patients.
NEC is known to have significant morbidity and mortality, and if these infants survive, they often times present with further issues as they age such as failure to thrive, intestinal strictures, intestinal failure, and other gastrointestinal issues.18–22 The two-hit hypothesis has yet to be fully elucidated in regard to necrotizing enterocolitis, however it is well accepted that NEC is associated with prematurity.1,14,23,24 Through our studies involving tissue and enteroids from patients that have clinically recovered from NEC, we believe we are able to expand on the two-hit hypothesis within necrotizing enterocolitis. When analyzing the hyperinflammatory response in tissue and following that with analysis of enteroids from that tissue, we are able to demonstrate the significance of multiple intestinal insults that occur in vivo in patients with necrotizing enterocolitis through an in vitro model. The robust inflammatory response demonstrated by the recovered NEC enteroids supports the theory that a second hit can play a significant role not only in NEC but in intestinal pathology as these patients age. While the inflammatory markers in tissue obtained from patients that had recovered from NEC were no different than those seen in control, we believe we were able to demonstrate that the recovered NEC tissue is already “primed” for an increased hyperinflammatory response when subjected to further insult through the enteroids model.
Limitations and Strengths
Our study is performed utilizing human tissue; therefore, our study is limited by availability of this tissue for clinically indicated resections. This results in us having limited patient numbers. However, our lab has developed a manner to enhance our scientific rigor by utilizing enteroids, which allows us to have thousands of enteroid numbers. We are constantly working towards collecting tissue from individual patients following clinically indicated resections to strengthen our patient numbers.
With that being said, utilizing human tissue is also one of the main strengths of this study. By utilizing human tissue and creating enteroids from the tissue, we are able to create a study design that closely mimics the in vivo conditions seen in patients. Enteroids maintain their host characteristics that were occurring at the time of resection, allowing us to perpetuate this state and study it more closely. We are also able to follow these patients over time, for example following their ostomy takedowns, enhancing our research.
Conclusion
Necrotizing enterocolitis is a devastating disease seen primarily in premature neonates with an unregulated hyperinflammatory response. We have been able to demonstrate inflammatory response seen in NEC previously through our enteroid model. Through expansion of our studies, we have now been able to demonstrate the impact of a second hit on the inflammatory response in previously primed tissue, that of a patient that has recovered from NEC. The persistence of this primed response following full recovery from NEC could not only be an avenue to identify at-risk infants but also to potentially prevent a second hit from occurring, impacting the hyperinflammatory pathology seen as these patients age.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All tissue was collected only after institutional review board approval (IRB #11610-11611) and parental consent for patients. This work complies with the Declaration of Helsinki.
Acknowledgments
We thank the Institutional Research Core Facility at the University of Oklahoma Health Sciences Center for the use of the Core Facility that provided total RNA library construction and sequencing.
Funding
Oklahoma Center for Adult Stem Cell Research (CH). Research reported in this manuscript was supported by the National Institutes of Health NIDDK under award number 1R01DK133207-01A1.
Disclosure
The authors have no conflicts of interest to declare. We are funded by the Oklahoma Center for Adult Stem Cell Research (CH); however, we have no conflicts of interest with this funding.
References
1. Hunter CJ, Upperman JS, Ford HR, Camerini V. Understanding the susceptibility of the premature infant to necrotizing enterocolitis (NEC). Pediatr Res. 2008;63(2):117–123. doi:10.1203/PDR.0b013e31815ed64c
2. Neu J, Walker WA. Necrotizing Enterocolitis. N Engl J Med. 2011;364(3):255–264. doi:10.1056/NEJMra1005408
3. Bein A, Eventov-Friedman S, Arbell D, Schwartz B. Intestinal tight junctions are severely altered in NEC preterm neonates. Pediatr Neonatol. 2018;59(5):464–473. doi:10.1016/j.pedneo.2017.11.018
4. Markel TA, Crisostomo PR, Wairiuko GM, Pitcher J, Tsai BM, Meldrum DR. CYTOKINES IN NECROTIZING ENTEROCOLITIS. Shock. 2006;25(4):329–337. doi:10.1097/01.shk.0000192126.33823.87
5. Thompson AM, Bizzarro MJ. Necrotizing enterocolitis in newborns. Drugs. 2008;68(9):1227–1238. doi:10.2165/00003495-200868090-00004
6. Claud EC. Neonatal Necrotizing Enterocolitis -Inflammation and Intestinal Immaturity. Antiinflamm Antiallergy Agents Med Chem. 2009;8(3):248–259. doi:10.2174/187152309789152020
7. Van Marter LJ, Dammann O, Allred EN, et al. Chorioamnionitis, mechanical ventilation, and postnatal sepsis as modulators of chronic lung disease in preterm infants. J Pediatr. 2002;140(2):171–176. doi:10.1067/mpd.2002.121381
8. Patra A, Huang H, Bauer JA, Giannone PJ. Neurological consequences of systemic inflammation in the premature neonate. Neural Regen Res. 2017;12(6):890–896. doi:10.4103/1673-5374.208547
9. Snyder KB, Golubkova A, Leiva T, et al. Persistent proclivity to a proinflammatory state in a human enteroid model of necrotizing enterocolitis. Surg Infect. 2023;24:606–612. doi:10.1089/sur.2023.123
10. Kaser A, Zeissig S, Blumberg RS. Genes and environment: how will our concepts on the pathophysiology of IBD develop in the future? Dig Dis. 2010;28(3):395–405. doi:10.1159/000320393
11. Buonpane C, Ares G, Yuan C, Schlegel C, Liebe H, Hunter CJ. Experimental modeling of necrotizing enterocolitis in human infant intestinal enteroids. J Invest Surg. 2022;35(1):111–118. doi:10.1080/08941939.2020.1829755
12. Liebe H, Schlegel C, Cai X, et al. Apical-out enteroids as an innovative model for necrotizing enterocolitis. J Surg Res. 2023;283:1106–1116. doi:10.1016/j.jss.2022.11.048
13. Barlow B, Santulli TV. Importance of multiple episodes of hypoxia or cold stress on the development of enterocolitis in an animal model. Surgery. 1975;77(5):687–690.
14. Hackam DJ, Sodhi CP. Toll-Like Receptor-Mediated Intestinal Inflammatory Imbalance in the Pathogenesis of Necrotizing Enterocolitis. Cell Mol Gastroenterol Hepatol. 2018;6(2):229–238.e1. doi:10.1016/j.jcmgh.2018.04.001
15. Kovler ML, Gonzalez Salazar AJ, Fulton WB, et al. Toll-like receptor 4-mediated enteric glia loss is critical for the development of necrotizing enterocolitis. Sci Transl Med. 2021;13(612):eabg3459. doi:10.1126/scitranslmed.abg3459
16. Ford HR, Sorrells DL, Knisely AS. Inflammatory cytokines, nitric oxide, and necrotizing enterocolitis. Semin Pediatr Surg. 1996;5(3):155–159.
17. Frost BL, Jilling T, Caplan MS. The importance of pro-inflammatory signaling in neonatal necrotizing enterocolitis. Semin Perinatol. 2008;32(2):100–106. doi:10.1053/j.semperi.2008.01.001
18. Morgan RL, Preidis GA, Kashyap PC, et al. Probiotics reduce mortality and morbidity in preterm, low-birth-weight infants: a systematic review and network meta-analysis of randomized trials. Gastroenterology. 2020;159(2):467–480. doi:10.1053/j.gastro.2020.05.096
19. Phad N, Trivedi A, Todd D, Lakkundi A. Intestinal strictures post-necrotising enterocolitis: clinical profile and risk factors. J Neonatal Surg. 2014;3(4):44. doi:10.47338/jns.v3.134
20. Gaudin A, Farnoux C, Bonnard A, et al. Necrotizing Enterocolitis (NEC) and the risk of intestinal stricture: the value of C-reactive protein. PLoS One. 2013;8(10):e76858. doi:10.1371/journal.pone.0076858
21. Harpavat S, Pammi M, Gilger M. Novel Treatments for NEC: keeping IBD in mind. Current Gastroenterol Reports. 2012;14(5):373–379. doi:10.1007/s11894-012-0267-3
22. Bazacliu C, Neu J. Necrotizing enterocolitis: long term complications. Curr Pediatr Rev. 2019;15(2):115–124. doi:10.2174/1573396315666190312093119
23. Neu J. Gastrointestinal development and meeting the nutritional needs of premature infants. The American Journal of Clinical Nutrition. 2007;85(2):629S–634S. doi:10.1093/ajcn/85.2.629S
24. Taylor GL, O’Shea TM. Extreme prematurity: risk and resiliency. Curr Probl Pediatr Adolesc Health Care. 2022;52(2):101132. doi:10.1016/j.cppeds.2022.101132
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.