Back to Journals » Journal of Pain Research » Volume 18
Depression as an Independent Predictor of Incident Pain: Longitudinal Evidence From CHARLS
Authors Song W, Wang S ![]() , Cao Z, Lin J
, Cao Z, Lin J ![]()
Received 6 July 2025
Accepted for publication 9 October 2025
Published 17 October 2025 Volume 2025:18 Pages 5481—5491
DOI https://doi.org/10.2147/JPR.S551970
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Wenwen Song,1,2 Shenghan Wang,1,2 Zhijian Cao,1,2 Jiangnan Lin1,2
1Department of Radiology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, People’s Republic of China; 2The First School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
Correspondence: Jiangnan Lin, Department of Radiology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, People’s Republic of China, Email [email protected]
Background: This study employs a longitudinal research design to investigate the impact of depression as an independent risk factor on the incidence of pain among middle-aged and elderly populations, with the objective of providing evidence for early intervention strategies to reduce pain-related disability and improve quality of life in aging populations.
Methods: This study utilized baseline data from the 2011 wave of the China Health and Retirement Longitudinal Study (CHARLS). Participants aged ≥ 45 years without baseline pain were included (n = 4,966), with three follow-up assessments conducted in 2013, 2015, and 2018. Pain occurrence was defined as the first self-reported pain episode during follow-up. Depressive symptoms were assessed using the 10-item Center for Epidemiologic Studies Depression Scale (CESD-10) (score ≥ 10). Multivariable Cox regression was used to assess the impact of depression and various demographic factors on pain occurrence, and stratified analysis was conducted to further clarify the independence of depression as a risk factor.
Results: Among 4,966 participants, depressive symptoms were significantly associated with higher pain incidence (HR = 1.35, 95% CI: 1.25– 1.47). Other predictors included female sex (HR = 1.55), arthritis (HR = 1.61), Activities of Daily Living/ Instrumental Activities of Daily Living (ADL/IADL) dysfunction (HR = 1.23), and chronic diseases (lung/kidney/digestive). Subgroup analyses identified a significant ADL/IADL-pain interaction (P = 0.001), with no other depression-related interactions observed.
Conclusion: Depression serves as an independent predictor of pain onset among middle-aged and elderly populations in China, and this relationship is further complicated by functional decline. Early screening for depressive symptoms and functional decline may help alleviate pain-related disability in elderly populations. Future research should investigate the dynamic relationship between pain and depression across different disease subtypes and treatment contexts.
Keywords: depression, pain, middle-aged and elderly, risk factors, CHARLS
Introduction
Pain affects over 20% of the global population1 and ranks among the leading causes of disability, particularly in middle-aged and older adults. Its high prevalence severely impairs daily functioning2,3 and imposes substantial economic burdens on healthcare systems worldwide. Proactive management of modifiable risk factors for pain onset is thus critical to reducing its societal impact. Notably, pain is not merely a somatic symptom but is intricately intertwined with psychological comorbidities, particularly depression.
Pain and depression show significant comorbidity. The prevalence of depression is markedly higher in pain populations compared to healthy controls, while pain occurrence is also elevated among individuals with depression. Those with both conditions exhibit the highest likelihood of functional impairment in daily life.4 Studies confirm that childhood chronic pain increases the risk of depression in adulthood.5 A recent meta-analysis indicates that approximately 40% of adults with chronic pain suffer from comorbid depression or anxiety.6 The interplay between physical pain and emotional distress exacerbates both conditions, leading to higher disability rates, prolonged disease duration, poorer prognosis, increased treatment complexity, and greater healthcare burdens.
A study based on 14-year follow-up data from the UK Biobank large-scale cohort found that the coexistence of multiple types of pain significantly increases the risk of depression through mechanisms such as inflammation7 The release of pro-inflammatory mediators such as IL-1β, IL-6, TNF-α, activates peripheral immune cells, prompting them to release inflammatory signals. This induces microglial activation and triggers a neuroinflammatory cascade, which impairs synaptic plasticity in brain regions like the prefrontal cortex and amygdala. Ultimately, this process exacerbates pain sensitivity and promotes negative emotions.8,9 Additionally, reduced activity in the dopaminergic pathway from the ventral tegmental area (VTA) to the ventral hippocampus (vHPC) can lead to depression comorbid with chronic pain.10 These findings collectively suggest that neuronal hyperexcitability serves as a key overlapping mechanism underlying the comorbidity of depression and pain.11
Although depression and pain are comorbidities with common regulatory pathways, it is not difficult to see that the above studies have mostly focused on the occurrence of pain after depression, overlooking pain as a multifactorial outcome where depression serves as an independent predictor. Furthermore, few studies have systematically examined how demographic variables and chronic comorbidities interact with depressive symptoms to modulate pain incidence and progression. To address these gaps, this study leverages longitudinal data from the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative cohort of middle-aged and older adults.12 Unlike previous work, we systematically evaluate depression, chronic diseases, and sociodemographic factors as predictors of incident pain. Subgroup analyses further identify risk heterogeneity across gender and age strata, offering insights for targeted prevention.
Our findings aim to inform integrated biopsychosocial interventions, emphasizing early depression screening to mitigate pain-related disability and alleviate healthcare burdens in aging populations.
Methods
Population
This research employed data sourced from the China Health and Retirement Longitudinal Study (CHARLS), a cohort study with national representativeness that centers on Chinese adults aged 45 and over. CHARLS adopted a multi - stage stratified sampling method with probability proportional to size, enrolling participants from both urban and rural areas spanning 28 provinces and 150 counties throughout China, thus ensuring a diverse and thorough sample. Every participant gave written informed consent. CHARLS was carried out in accordance with the Declaration of Helsinki and has obtained ethical approval from the Institutional Review Board at Peking University (IRB00001052 - 11015).
In this research, we utilized data ranging from wave 1 (2011–2012) to wave 4 (2018), taking wave 1 as the baseline. From an initial sample of 17705 participants in the first wave, 12739 were excluded due to baseline pain, age under 45 years, or missing values, resulting in a final analytical sample of 4966 individuals. This final cohort comprised 1146 with depression and 3820 without (Figure 1).
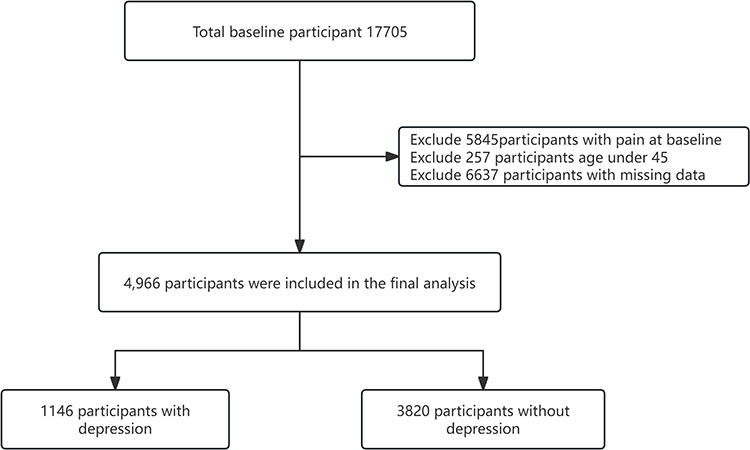 |
Figure 1 Flowchart of the study participants. |
Data Collection
Assessment of Depressive Symptoms
Depressive symptoms were diagnosed using the 10-item Center for Epidemiologic Studies Depression Scale (CESD-10) at baseline. The CESD-10 questionnaire includes 10 questions evaluating feelings and behaviors experienced over the past week. A score of 10 or higher indicated the presence of depressive symptoms.13
Covariates
Data were collected for the following variables: gender, age, education level, grip strength (positive if <18 kg for females and <28 kg for males), ChairRise test (positive if taking >12 seconds to stand up 5 times consecutively), chronic diseases (including hypertension, dyslipidemia, diabetes, cancer, chronic lung diseases, liver disease, heart problems, stroke, kidney disease, digestive disease, memory disease, asthma, arthritis), children’s visits (defined as >1 visit per week), children’s contact (defined as >1 contact per week), hearing status, eyesight status, sleep duration, social activity, cognitive score, health insurance, life satisfaction score, body mass index (BMI), smoking status, drinking status, and Activities of Daily Living/ Instrumental Activities of Daily Living (ADL/IADL) score (positive if any functional abnormality existed in activities of daily living/instrumental activities of daily living). The classification of positive and negative results for grip strength and the ChairRise test were both defined according to the Asian Working Group for Sarcopenia (AWGS) 2019 criteria.
The selection of covariates was informed by previous literature and clinical expertise. We adjusted for a range of potential confounders, including basic demographic factors, socioeconomic status, and health-related measures, as these factors could potentially influence both the exposure and the outcome.
Outcome
Pain data from 2013, 2015, and 2018 were included, with the first reported pain onset time as the outcome.
Statistical Analyses
Continuous variables were described as mean (standard deviation) due to their approximately normal distribution, which appropriately summarizes central tendency and variability, Categorical variables were summarized as number (percentage), as this is conventional for reporting proportions. Baseline characteristics were compared using the Wilcoxon rank-sum test (Mann–Whitney U-test) for continuous variables—since most were non-normally distributed—and Chi-square tests for categorical variables, which are suitable for assessing associations between nominal or ordinal variables.
To analyze time-to-pain-onset, Kaplan-Meier curves were generated to visualize cumulative incidence, and Log rank tests were used to compare survival curves between groups; these are standard methods for time-to-event data that account for censoring. Univariate Cox regression was first performed to identify potential risk factors (using p < 0.1 as an inclusive threshold to avoid overlooking variables that might contribute in adjusted models). Variables meeting this criterion were included in the multivariate Cox regression model to assess independent associations while controlling for confounders. Variables included: gender, education, hypertension, chronic lung diseases, liver disease, heart problems, kidney disease, digestive disease, arthritis, sleep, hearing, eyesight, social activity, cognition, health insurance, life satisfaction, smoking, drinking, ChairRise test result, low muscle strength, and ADL/IADL status. Multicollinearity among these variables was assessed using variance inflation factors (VIF); all VIF values were below 5, indicating that multicollinearity was not a substantial concern in the regression models.
To further confirm the independent predictive role of depression for pain incidence, subgroup analyses were performed for variables that reached statistical significance (p < 0.05) in the multivariate Cox model. This approach helps assess the consistency of the association across key subgroups.
All analyses were performed using R statistical software version 4.5.0, with two-sided P values <0.05 considered statistically significant.
Results
General Characteristics of Participants
The study included a total of 4966 participants. Table 1 presents the baseline clinical and demographic characteristics as well as the occurrence of follow-up pain. We found that depressive symptoms were more concentrated in female participants, who were slightly older and had generally lower educational levels. In terms of chronic diseases, the prevalence of chronic lung diseases, heart-related diseases, digestive diseases, asthma, and arthritis was higher among these individuals. Additionally, the incidence of hearing and vision problems was higher. Furthermore, participants with depressive symptoms had shorter sleep duration, less social activity, lower frequency of contact with children, lower cognitive function, and reduced muscle strength. Conversely, the proportions of smokers and drinkers were lower among those with depressive symptoms. During the follow-up of the two groups, the group with depressive symptoms exhibited a greater risk of pain occurrence.
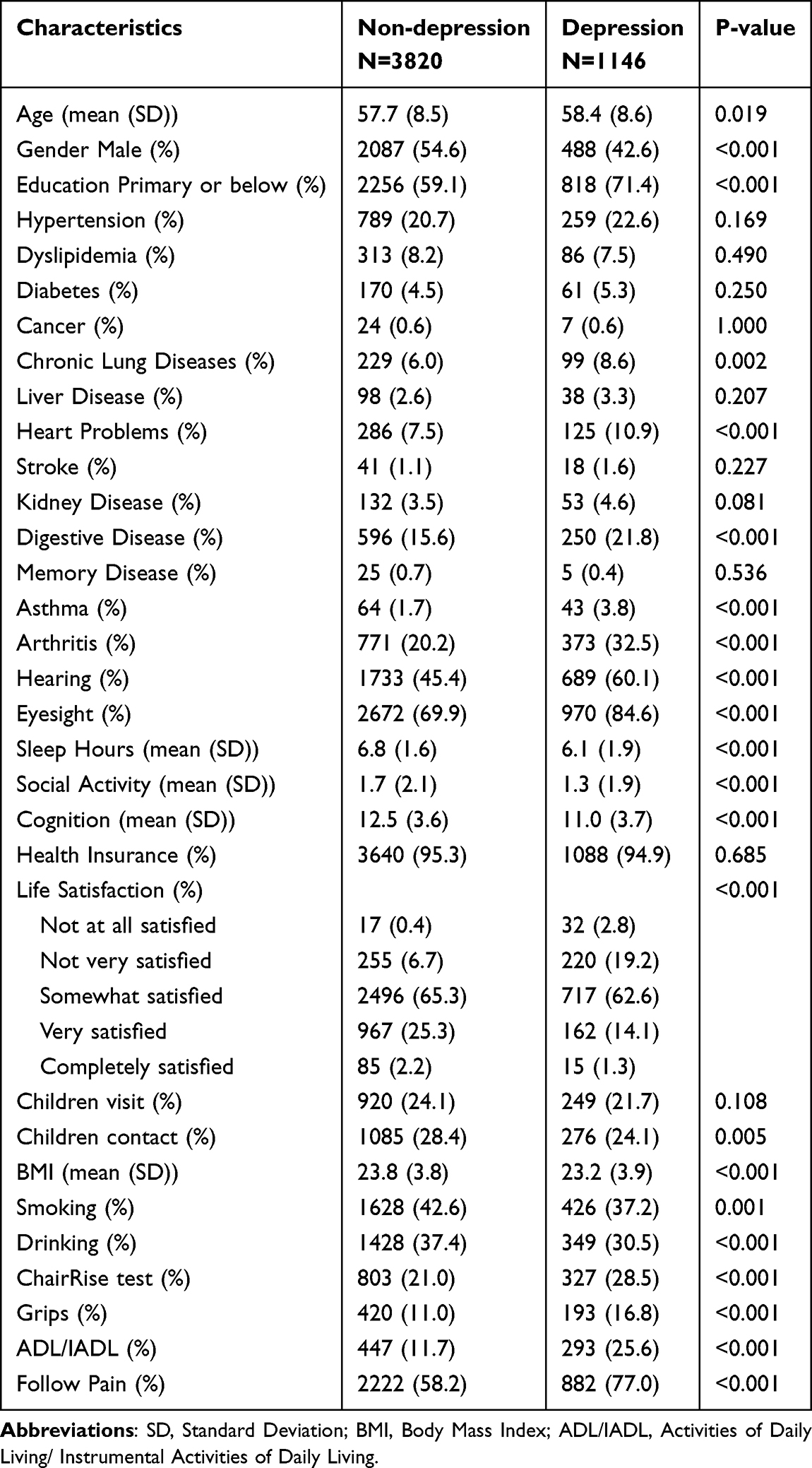 |
Table 1 Baseline Characteristics of Individuals Classified by Depression |
Association Between Depressive Symptoms and the Incidence of New-Onset Pain
The Kaplan-Meier analysis showed a significantly higher cumulative incidence of pain in the depressive symptoms group compared to the non-depressive group (log-rank p<0.0001) (Figure 2). Multivariate Cox regression identified depressive symptoms as a significant risk factor for pain (HR=1.35, 95% CI: 1.25–1.47, p<0.001). Other significant predictors included female gender (HR=1.55, 95% CI: 1.39–1.73, p<0.001), chronic lung diseases (HR=1.18, 95% CI: 1.03–1.35, p=0.020), kidney disease (HR=1.24, 95% CI: 1.05–1.47, p=0.011), digestive disease (HR=1.20, 95% CI: 1.10–1.32, p<0.001), arthritis (HR=1.61, 95% CI: 1.49–1.75, p<0.001), shorter sleep duration (HR=0.96 per hour increase, 95% CI: 0.94–0.98, p<0.001), hearing problems (HR=1.09, 95% CI: 1.01–1.18, p=0.021), health insurance (HR=1.29, 95% CI: 1.08–1.54, p=0.005), lower life satisfaction (HR=0.88 per satisfaction level increase, 95% CI: 0.83–0.93, p<0.001), positive ChairRise test (HR=1.09, 95% CI: 1.01–1.19, p=0.037), and ADL/IADL dysfunction (HR=1.23, 95% CI: 1.12–1.35, p<0.001) (Table 2 and Figure 3).
 |
Table 2 Association Between the Depression and Pain Incidence |
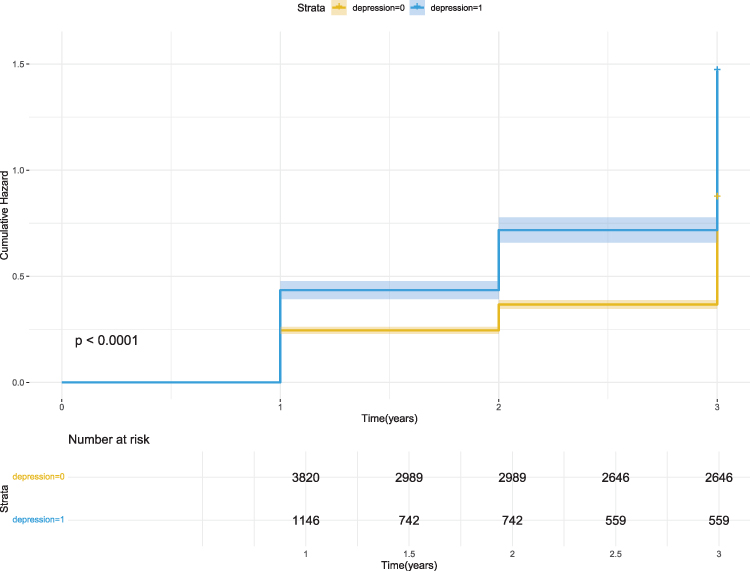 |
Figure 2 Kaplan–Meier analysis for pain was based on depression. |
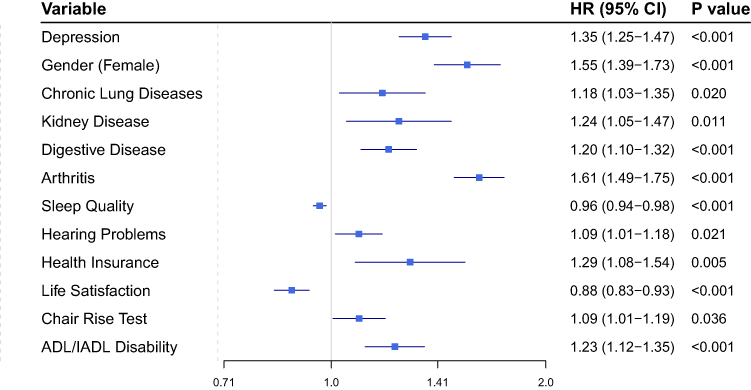 |
Figure 3 Forest plot for significant predictors (p<0.05). Abbreviations: HR, Hazard Ratio; ADL/IADL, Activities of Daily Living/ Instrumental Activities of Daily Living. |
Stratified Analysis
Stratified analyses revealed that depression was consistently associated with an increased incidence of pain across all subgroups categorized by sex, age, education level, ADL/IADL dysfunction, chair stand test results, arthritis, chronic lung disease, digestive diseases, kidney diseases, health insurance status, life satisfaction, and sleep duration. Additionally, besides the significant interaction effect between ADL/IADL dysfunction and depression (interaction p=0.001), no other variables demonstrated statistically significant interaction effects with depression (all interaction p>0.05). (Figure 4).
 |
Figure 4 Forest plot for stratified analyses. Abbreviations: HR, Hazard Ratio; ADL/IADL, Activities of Daily Living/ Instrumental Activities of Daily Living. |
Discussion
This study found that the depression symptom group had a higher risk of pain occurrence. Multivariate Cox regression indicated that depressive symptoms were a significant risk factor for pain. Additionally, factors such as female sex, chronic lung disease, kidney disease, digestive system diseases, arthritis, reduced sleep duration, hearing problems, health insurance, decreased life satisfaction, positive chair stand test results, and ADL/IADL dysfunction were also significantly associated with pain occurrence. Although a certain interaction was observed between ADL/IADL dysfunction and pain occurrence, both subgroups showed significant associations with pain incidence, while other variables did not significantly modify the association. This suggests the independent effect of depression on pain.
Multiple studies have established the comorbidity between depression and pain. Our findings indicate that depression may serve as a relatively independent risk factor. Our findings further support a potential bidirectional association between depression and pain. Although this study focused on the predictive role of depression in pain onset, it is notable that pain may also contribute to depression. A recent large-scale study using UK Biobank data and Mendelian randomization indicated that multisite chronic pain (MCP) has a causal effect on depression, which was not observed for single-site pain, suggesting that pain distribution rather than mere presence plays a critical role. Subtype analyses revealed that chronic pain, particularly in the head and abdomen, was most strongly linked to depression, partially mediated by inflammatory markers such as C-reactive protein, highlighting a role for neuroinflammation.7 Future studies should adopt finer pain subtyping, such as by location, duration, and multisite co-occurrence, thereby informing the development of targeted clinical intervention strategies. Earlier, the Irish Longitudinal Study on Ageing (TILDA) identified physical health as the primary risk factor for pain, with mental health status as a secondary risk factor.14 Another predictive modeling study found that major risk factors for pain included insomnia, high BMI, fatigue, and significant life stress.15 Through follow-ups at multiple time points and stratified analyses of various risk factors, our study confirmed the independence of depression as a risk factor.
Neuroscientific research demonstrates that pain and depression share multiple brain regions, including the amygdala, hippocampus, thalamus, anterior cingulate cortex (ACC), prefrontal cortex, and insular cortex, which are involved in processing pain and depression.16,17 Animal studies have identified several neural circuits, such as the ventral hippocampus-medial prefrontal cortex (mPFC), thalamus-subcortical circuits, and ACC-ventral tegmental area (VTA) pathways, that participate in the comorbidity of pain and depression.18–20 Furthermore, neurotransmitters like serotonin, norepinephrine, and dopamine play crucial roles in regulating mood and pain perception.21 Imbalances in these neurotransmitters in depressed patients may lead to low mood and increased pain sensitivity. Studies have shown that antidepressant treatment in patients with comorbid depression and pain not only reduces depression scores but also effectively alleviates pain.22
Declines in physical function also significantly influence pain occurrence. Several studies suggest an association between ADL/IADL and pain, indicating that pain can predict short-term changes in ADL.23 Disability is also a major risk factor for poor pain prognosis.24 An Indian cohort study of older adults similarly identified pain as a risk factor for impaired functional activity.25 Our study found that middle-aged and older adults with activity limitations had an increased probability of developing pain in subsequent years. Additionally, those with longer chair stand times showed a higher probability of pain in later follow-ups. The chair stand test assesses lower limb strength (particularly quadriceps), balance, and daily functional activity. Abnormalities in these variables are associated with fall risk.26 However, grip strength showed no significant association with pain occurrence, suggesting that lower limb strength may have specificity for pain development. Reduced upper limb strength has been reported in some studies to be associated with the development of upper limb pain.27 Combined with previous research, we propose a vicious cycle between ADL/IADL dysfunction and pain. Therefore, any decline in physical function among middle-aged and older adults should be actively addressed.
Our study identified osteoarthritis, chronic lung disease, kidney disease, and digestive diseases as risk factors for pain. Osteoarthritis mechanically stimulates surrounding tissues and releases pro-inflammatory cytokines, causing pain.28 Chronic lung diseases, such as COPD, may lead to chest wall muscle strain or pleural inflammation due to chronic coughing, resulting in chest/back pain.29 Chronic kidney disease can cause neuropathic pain due to metabolite accumulation.30 Digestive diseases such as gastric ulcers and intestinal spasms directly generate pain signals through mucosal damage and abnormal smooth muscle contractions.31,32 However, no clear associations were found between pain and hypertension, liver disease, heart problems, dyslipidemia, diabetes, cancer, stroke, memory-related diseases, or asthma. This does not necessarily mean these conditions cannot cause subsequent pain, as studies have linked cancer and diabetes to pain.33,34 Potential limitations include sample size biases like low prevalence of certain diseases, insufficient consideration of disease heterogeneity, and lack of detailed classification by subtype/stage, which may obscure underlying associations. The relationships between many diseases and pain remain controversial,35 warranting further optimized longitudinal studies.
We observed significantly higher pain prevalence in women than men, possibly due to sex differences in nociceptive responses. Women show greater susceptibility to certain conditions such as inflammation, osteoarthritis, variable drug responses, and higher emotional sensitivity.36–38 Additionally, higher education levels were associated with lower pain incidence, consistent with prior epidemiological findings.2 Our study found that individuals with less sleep have a higher probability of developing pain in the future, and previous studies have reported similar results.39 Our study shows that individuals with health insurance have a higher incidence of pain. Similarly, a correlational study on the association between insurance and pain in the US population found that those with public insurance face an increased risk of future chronic pain.40 This may be due to high population insurance coverage, where pain-susceptible individuals (such as those with disabilities) are more likely to actively enroll in insurance programs. Additionally, our study failed to subdivide insurance types, which may have introduced bias.
This study has several limitations. First, due to data constraints, we were unable to subclassify pain by type or etiology, which may obscure potential differences in how depression interacts with distinct pain subtypes. Second, potential biases may exist in self-reported variables due to recall bias or social desirability bias. For example, underreporting of depressive symptoms in culturally stigmatized contexts could attenuate observed associations. Additionally, functional assessments such as the ChairRise test and grip strength measurements may lack sensitivity to detect subtle declines, potentially misclassifying physical frailty status. Third, information regarding medications, socioeconomic stress, inflammatory marker was not included in the analysis. This omission limits our ability to account for potential confounding or mediating effects of treatments on the depression-pain relationship.
Conclusion
Despite these limitations, our findings demonstrate that depression serves as an independent and major risk factor for pain onset. Effective management of depression appears crucial for pain prevention. Future research should further investigate the relationships between pain etiology, anatomical location, pain intensity, and the severity of depressive symptoms, as well as potential bidirectional reinforcement of pain and depression comorbidities.
Data Sharing Statement
The datasets generated for this study are available in the China Health and Retirement Longitudinal Study (CHARLS) database at https://charls.pku.edu.cn.
Ethics Approval and Consent to Participate
This study was formally reviewed and granted exemption (Approval No. 2025-YBK-017-01) by the Ethics Committee of Zhejiang Provincial Hospital of Chinese Medicine in accordance with Article 32, Sections 1-2 of China’s Ethical Review Measures for Life Science and Medical Research Involving Human Subjects (2023).
Acknowledgments
We would like to thank all the members of the CHALRS for their contributions and the participants who contributed their data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Medical and Health Science and Technology Project of Zhejiang Province [2023KY849, 2024KY130] and the Research Project of Zhejiang Chinese Medical University [2022FSYYZY06].
Disclosure
The authors declare that the research was conducted without commercial or financial relationships that could create a conflict of interest.
References
1. Cao B, Xu Q, Shi Y, et al. Pathology of pain and its implications for therapeutic interventions. Signal Transduct Target Ther. 2024;9:155. doi:10.1038/s41392-024-01845-w
2. Nahin RL, Feinberg T, Kapos FP, Terman GW. Estimated rates of incident and persistent chronic pain among US adults, 2019–2020. JAMA Network Open. 2023;6:e2313563. doi:10.1001/jamanetworkopen.2023.13563
3. Shi Y, Wu W. Multimodal non-invasive non-pharmacological therapies for chronic pain: mechanisms and progress. BMC Med. 2023;21:372. doi:10.1186/s12916-023-03076-2
4. De La Rosa JS, Brady BR, Ibrahim MM, et al. Co-occurrence of chronic pain and anxiety/depression symptoms in U.S. adults: prevalence, functional impacts, and opportunities. Pain. 2024;165:666–673. doi:10.1097/j.pain.0000000000003056
5. Antoniou G, Lambourg E, Steele JD, Colvin LA. The effect of adverse childhood experiences on chronic pain and major depression in adulthood: a systematic review and meta-analysis. Br J Anaesth. 2023;130:729–746. doi:10.1016/j.bja.2023.03.008
6. Aaron RV, Ravyts SG, Carnahan ND, et al. Prevalence of depression and anxiety among adults with chronic pain: a systematic review and meta-analysis. JAMA Network Open. 2025;8:e250268. doi:10.1001/jamanetworkopen.2025.0268
7. Jiang R, Geha P, Rosenblatt M, et al. The inflammatory and genetic mechanisms underlying the cumulative effect of co-occurring pain conditions on depression. Sci Adv. 2025;11:eadt1083. doi:10.1126/sciadv.adt1083
8. Zhang Y, Ma H, Bai Y, et al. Chronic neuropathic pain and comorbid depression syndrome: from neural circuit mechanisms to treatment. ACS Chem Neurosci. 2024;15:2432–2444. doi:10.1021/acschemneuro.4c00125
9. Arzani M, Jahromi SR, Ghorbani Z, et al. Gut-brain axis and migraine headache: a comprehensive review. J Headache Pain. 2020;21:15. doi:10.1186/s10194-020-1078-9
10. Ji Y, Xiao Y, Bai X, et al. Modulation of comorbid depression of neuropathic pain by dopamine input from VTA to the ventral hippocampus. Theranostics. 2025;15:4101–4123. doi:10.7150/thno.104394
11. Pelzer N, de Boer I, Van den maagdenberg A, Terwindt GM. Neurological and psychiatric comorbidities of migraine: concepts and future perspectives. Cephalalgia. 2023;43:3331024231180564. doi:10.1177/03331024231180564
12. Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. 2014;43:61–68. doi:10.1093/ije/dys203
13. Bai S, Wang J, Liu J, Miao Y, Zhang A, Zhang Z. Analysis of depression incidence and influence factors among middle-aged and elderly diabetic patients in China: based on CHARLS data. BMC Psychiatry. 2024;24:146. doi:10.1186/s12888-023-05473-6
14. O’Neill A, O’Sullivan K, O’Keeffe M, Hannigan A, Walsh C, Purtill H. Development of pain in older adults: a latent class analysis of biopsychosocial risk factors. Pain. 2018;159:1631–1640. doi:10.1097/j.pain.0000000000001251
15. Tanguay-Sabourin C, Fillingim M, Guglietti GV, et al. A prognostic risk score for development and spread of chronic pain. Nature Med. 2023;29:1821–1831. doi:10.1038/s41591-023-02430-4
16. Sezer I, Pizzagalli DA, Sacchet MD. Resting-state fMRI functional connectivity and mindfulness in clinical and non-clinical contexts: a review and synthesis. Neurosci Biobehav Rev. 2022;135:104583. doi:10.1016/j.neubiorev.2022.104583
17. Ashar YK, Gordon A, Schubiner H, et al. Effect of pain reprocessing therapy vs placebo and usual care for patients with chronic back pain: a randomized clinical trial. JAMA psychiatry. 2022;79:13–23. doi:10.1001/jamapsychiatry.2021.2669
18. Lv SS, Lv XJ, Cai YQ, et al. Corticotropin-releasing hormone neurons control trigeminal neuralgia-induced anxiodepression via a hippocampus-to-prefrontal circuit. Sci Adv. 2024;10:eadj4196. doi:10.1126/sciadv.adj4196
19. Deng J, Chen L, Liu CC, et al. Distinct Thalamo-subcortical circuits underlie painful behavior and depression-like behavior following nerve injury. Adv Sci. 2024;11:e2401855. doi:10.1002/advs.202401855
20. Song Q, Wei A, Xu H, et al. An ACC-VTA-ACC positive-feedback loop mediates the persistence of neuropathic pain and emotional consequences. Nat Neurosci. 2024;27:272–285. doi:10.1038/s41593-023-01519-w
21. Zhou W, Jin Y, Meng Q, et al. A neural circuit for comorbid depressive symptoms in chronic pain. Nat Neurosci. 2019;22:1649–1658. doi:10.1038/s41593-019-0468-2
22. Liao HY, Satyanarayanan SK, Lin YW, Su KP. Clinical efficacy and immune effects of acupuncture in patients with comorbid chronic pain and major depression disorder: a double-blinded, randomized controlled crossover study. Brain Behav Immun. 2023;110:339–347. doi:10.1016/j.bbi.2023.03.016
23. van Dalen-Kok AH, Pieper MJC, de Waal MWM, van der Steen JT, Scherder EJA, Achterberg WP. The impact of pain on the course of ADL functioning in patients with dementia. Age Ageing. 2021;50:906–913. doi:10.1093/ageing/afaa247
24. van der Gaag WH, Chiarotto A, Heymans MW, et al. Developing clinical prediction models for nonrecovery in older patients seeking care for back pain: the back complaints in the elders prospective cohort study. Pain. 2021;162:1632–1640. doi:10.1097/j.pain.0000000000002161
25. Muhammad T, Rashid M, Zanwar PP. Examining the association of pain and pain frequency with self-reported difficulty in activities of daily living and instrumental activities of daily living among community-dwelling older adults: findings from the longitudinal aging study in India. J Gerontol B Psychol Sci Soc Sci. 2023;78:1545–1554. doi:10.1093/geronb/gbad085
26. Ishida Y, Maeda K, Ueshima J, et al. The SARC-F score on admission predicts falls during hospitalization in older adults. J Nutr Health Aging. 2021;25:399–404. doi:10.1007/s12603-021-1597-3
27. AlAnazi A, Alghadir AH, Gabr SA. Handgrip strength exercises modulate shoulder pain, function, and strength of rotator cuff muscles of patients with primary subacromial impingement syndrome. Biomed Res Int. 2022;2022:9151831. doi:10.1155/2022/9151831
28. Yu H, Huang T, Lu WW, Tong L, Chen D. Osteoarthritis Pain. Int J Mol Sci. 2022;23. doi:10.3390/ijms23094642.
29. Clarke SY, Williams MT, Johnston KN, Lee AL. The prevalence and assessment of pain and dyspnoea in acute exacerbations of COPD: a systematic review. Chron respir dis. 2022;19:14799731221105518. doi:10.1177/14799731221105518
30. Kalantar-Zadeh K, Lockwood MB, Rhee CM, et al. Patient-centred approaches for the management of unpleasant symptoms in kidney disease. Nat Rev Nephrol. 2022;18:185–198. doi:10.1038/s41581-021-00518-z
31. Zia JK, Lenhart A, Yang PL, et al. Risk factors for abdominal pain-related disorders of gut-brain interaction in adults and children: a systematic review. Gastroenterology. 2022;163:995–1023.e1023. doi:10.1053/j.gastro.2022.06.028
32. Lu J, Chen Y, Shi L, et al. Cognition of abdominal pain and abdominal discomfort in Chinese patients with irritable bowel syndrome with diarrhea. BioPsychoSoc med. 2023;17:31. doi:10.1186/s13030-023-00286-1
33. Calcutt NA. Diabetic neuropathy and neuropathic pain: a (con)fusion of pathogenic mechanisms? Pain. 2020;161:S65–s86. doi:10.1097/j.pain.0000000000001922
34. Zhang H. Cancer pain management-new therapies. Current Oncol Rep. 2022;24:223–226. doi:10.1007/s11912-021-01166-z
35. Argüello E, Bermeo L, Castillo J. Exploring the abilities of peripheral autonomic parameters to describe pain: another dead end? Pain Physician. 2022;25:E1–e14.
36. Templeton KJ. Sex and gender issues in pain management. J Bone Joint Surg. 2020;102(Suppl 1):32–35. doi:10.2106/jbjs.20.00237
37. Li J, Liu F, Liu Z, et al. Prevalence and associated factors of depression in postmenopausal women: a systematic review and meta-analysis. BMC Psychiatry. 2024;24:431. doi:10.1186/s12888-024-05875-0
38. Courties A, Kouki I, Soliman N, Mathieu S, Sellam J. Osteoarthritis year in review 2024: epidemiology and therapy. Osteoarthritis Cartilage. 2024;32:1397–1404. doi:10.1016/j.joca.2024.07.014
39. Meng X, Li D, Wang Y, Han C. Sleep duration and pain during the COVID-19 pandemic with depression and chronic diseases as mediators. Sci Rep. 2024;14:27095. doi:10.1038/s41598-024-78579-w
40. Semaan K, Frech A, Tumin D. Reciprocal association between chronic pain and health insurance type in a population-based longitudinal cohort study. J Pain. 2024;25:104503. doi:10.1016/j.jpain.2024.02.017
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Alleviating Excessive Worries Improves Co-Occurring Depression and Pain in Adolescent and Young Adult Cancer Patients: A Network Approach
Li W, Xu Y, Luo X, Wen Y, Ding K, Xu W, Garg S, Yang Y, Sun H
Neuropsychiatric Disease and Treatment 2022, 18:1843-1854
Published Date: 25 August 2022
Depression and Associated Risk Factors Among Type 2 Diabetic Patients: A Cross Sectional Study on a Convenience Sample from the Diabetic Center, Khamis Mushait; Saudi Arabia
Abuhegazy H, Mujairi A, Banah F, Agdi Y, Elkeshishi H, Kamel A, Abdullah A, Elsheikh M
Neuropsychiatric Disease and Treatment 2022, 18:1975-1984
Published Date: 31 August 2022
Predictive Validity and Patterns of Change Over Time of the Sensitivity to Pain Traumatization Scale: A Trajectory Analysis of Patients Seen by the Transitional Pain Service Up to Two Years After Surgery
Fashler SR, Pagé MG, Svendrovski A, Flora DB, Slepian PM, Weinrib AZ, Huang A, Fiorellino J, Clarke H, Katz J
Journal of Pain Research 2022, 15:2587-2605
Published Date: 31 August 2022
Association Between Breakfast Consumption and Suicidal Attempts in Adolescents
Park H, Lee K
Psychology Research and Behavior Management 2022, 15:2529-2541
Published Date: 13 September 2022