Back to Journals » Journal of Inflammation Research » Volume 16
Decreased Peripheral Blood Lymphocyte Count Predicts Poor Treatment Response in Peritoneal Dialysis-Associated Peritonitis
Authors He Y ![]() , Huang X
, Huang X ![]() , Zhang J, Liao J, Huang H, He Y, Gao M, Liao Y, Xiong Z
, Zhang J, Liao J, Huang H, He Y, Gao M, Liao Y, Xiong Z
Received 5 September 2023
Accepted for publication 10 November 2023
Published 16 November 2023 Volume 2023:16 Pages 5327—5338
DOI https://doi.org/10.2147/JIR.S438674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
YuJian He,1,2 XiaoYan Huang,1 Jingwen Zhang,1 Jinlan Liao,1 Huie Huang,1 Yan He,1 Min Gao,1 Yumei Liao,1 Zibo Xiong1
1Renal Division, Peking University Shenzhen Hospital, Shenzhen, People’s Republic of China; 2Renal Division, PKU-Shenzhen Clinical Institute of Shantou University Medical College, Shenzhen, People’s Republic of China
Correspondence: Zibo Xiong, Renal Division, Peking University Shenzhen Hospital, Shenzhen, People’s Republic of China, Tel +86-13510880599, Fax +86-755-83089011, Email [email protected]
Purpose: Peripheral blood lymphocyte counts is a pivotal parameter in assessing the host’s immune response during maladies and the equilibrium of the immune system which has been found to correlate with various diseases progression and prognosis. However, there was no study on patients with peritoneal dialysis-associated peritonitis (PDAP). We sought to investigate the prognostic value of baseline peripheral blood lymphocyte count in PDAP patients.
Patients and methods: This retrospective study analyzed data from 286 PDAP patients over nine years. Episodes were categorized according to the tertiles of peripheral blood lymphocyte counts (Very Low Lymphocyte Count (VLLC) Group, < 0.72× 106/L; Low Lymphocyte Count (LLC) Group, 0.72– 1.11× 106/L; Normal Lymphocyte Count (NLC) Group, ≥ 1.11× 106/L). Demographic, laboratory, and infection-related variables were analyzed. Cox regression and generalized estimating equation (GEE) models were used to estimate the association between lymphocyte counts and PDAP treatment failure, which included PD catheter removal and death.
Results: After adjusting for other potential predictors, decreased lymphocyte counts exhibited an incremental relationship with the risk of treatment failure. The VLLC group indicated a 270% (95% CI, 1.168– 6.247, P=0.020) and 273% (95% CI, 1.028– 7.269, P=0.044) increased venture of treatment failure in Cox regression and GEE analyses, respectively, compared with the NLC group. As a continuous variable, the restricted cubic spline showed a linear negative correlation between lymphocyte counts and the treatment failure risk (P for overall = 0.026). The multivariate model C (combined lymphocyte count with baseline age, sex, dialysis age, Charlson Comorbidity index (CCI), etiology of kidney failure, hemoglobin, albumin, total bilirubin and infection type) showed an area under the curve of 0.824 (95% CI, 0.767– 0.881, P=0.001) for the prediction of treatment failure.
Conclusion: Lower lymphocyte counts are linked to increased PDAP treatment failure risk. This highlights lymphocyte count’s potential as a prognostic indicator for PDAP.
Keywords: peritoneal dialysis-associated peritonitis, lymphocyte counts, prognosis, treatment failure
Introduction
Peritoneal dialysis-associated peritonitis (PDAP) represents a frequent yet grave complication in peritoneal dialysis (PD) patients, standing as a major cause of technical failure and death.1,2 Hence, the early identification of markers and risk determinants pertaining to peritonitis outcomes, particularly those readily accessible at the onset of peritonitis episodes, assumes paramount significance for precise evaluation, prognostic anticipation, and timely decision-making in clinical practice. Zhou et al conducted a single center retrospective study, revealing associations between numerous inflammatory markers computed from complete blood counts and the outcomes of PDAP,3 including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), hemoglobin-to-lymphocyte ratio (HLR), and systemic immune-inflammation index (SII). While these inflammatory markers provide valuable insights, it is essential to recognize that lymphocyte counts, a clinically obtainable hematological marker, hold a well-established role in immune response assessment. Their simplicity, cost-effectiveness, and ease of interpretation make lymphocyte counts a practical and reliable choice for predicting poor prognosis in peritonitis, surpassing other immune-inflammation indexes.
Lymphocyte count operates as a pivotal gauge for assessing the host’s immune response during maladies and the equilibrium of the immune system, an elemental facet for the body’s defense against foreign pathogens.4 Beyond their principal function as pivotal constituents of the human immune system, safeguarding against foreign invaders, lymphocytes also play a role in modulating immune responses by releasing diverse immunomodulatory agents, encompassing interleukins, tumor necrosis factors, and interferons. Furthermore, lymphocyte-mediated immune reactions are indispensable in fortifying the functional integrity of the intestinal tract and curbing bacterial translocation.5 Over the past few decades, multiple studies have underscored the intimate association between lymphocyte counts and disease progression, prognosis, spanning afflictions like sepsis, acute pancreatitis, bronchitis, pneumonia, malignancies, and chronic kidney disease.6–10 Cueto and Quintana’s investigation has illuminated that lymphocytopenia has emerged as a predictor of poor prognosis among continuous ambulatory peritoneal dialysis (CAPD) patients.10 Likewise, Zahorec’s prospective longitudinal observational study substantiated the correlation between the clinical course’s severity and lymphocytopenia in patients treated for severe sepsis and septic shock within the intensive care unit (ICU).11
Despite multiple studies identifying the influence of lymphocyte counts on disease progression and outcomes, scant evidence exists to conclusively affirm the correlation between lymphocyte counts and adverse prognoses in PDAP. Therefore, we have meticulously reviewed our clinical dataset encompassing peritonitis episodes over the past nine years at the Peritoneal Dialysis Center of Peking University Shenzhen Hospital, which sought to elucidate the connection between baseline peripheral blood lymphocyte counts and treatment failure. We speculate that diminished baseline peripheral blood lymphocyte count is associated with worse outcomes among PDAP patients.
Methods
Study Design and Ethics
A retrospective single-center study was conducted involving PDAP patients from the Peritoneal Dialysis Center at Peking University Shenzhen Hospital. Ethical approval was obtained from the Ethics Committee of Peking University Shenzhen Hospital (No. 2022050). Informed consent was waived because it was a retrospective study and patient confidentiality was maintained. The study adhered to the principles of the Declaration of Helsinki.
Patients
We retrospectively documented PDAP patients treated at our institution between May 2014 and February 2023. All enrolled PDAP patients met the 2022 diagnostic criteria as recommended by the International Society for Peritoneal Dialysis (ISPD). These criteria necessitated the presence of at least two of the following conditions: (i) clinical manifestations indicative of peritonitis, such as abdominal pain and/or cloudy dialysis effluent; (ii) dialysis effluent leukocyte count exceeding 100/μL or 0.1×109 /L after a minimum dwell time of 2 hours, with polymorphonuclear leukocytes constituting over 50%; and (iii) positive dialysis effluent culture. Patients who with 2019 coronavirus infection were excluded.
Basic Demographic and Laboratory Data
The data were sourced from Peking University Shenzhen Hospital’s record system. Fundamental demographic data encompassed gender, age, dialysis age, Charlson Comorbidity Index (CCI) and etiology of kidney failure. The laboratory data included an assortment of blood cell counts, including leukocytes, neutrophils, monocytes, erythrocytes, and hemoglobin. Additionally, the data also included variables such as total protein, albumin, globulin, total bilirubin, blood urea nitrogen, creatinine, uric acid, potassium, sodium, chlorine, calcium and microbiology.
The CCI, established by Charlson et al, is employed to assess the severity of comorbid conditions.12 CCI assigns scores based on the following criteria: One point for a history of myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, connective tissue disorder, peptic ulcer disease, mild liver disease, or diabetes without end-organ damage. Two points for cerebrovascular disease with hemiplegia, moderate to severe renal disease, diabetes with end-organ damage, or the presence of tumors without metastases, leukemia, lymphoma, or myeloma. Three points for moderate or severe liver disease. Six points for metastatic solid tumors or acquired immunodeficiency syndrome (AIDS). Additionally, an extra point is added for every decade beyond the age of 40.
Laboratory Measurements and Therapeutic Schedule
For suspected peritonitis patients, peritoneal dialysis effluent (PDE) was collected using aseptic techniques into blood culture bottles and sterile tubes. The collected PDE samples were subjected to cell counts, Gram staining, microbial culture, and drug sensitivity tests. Following PDE collection, all patients received initial treatment with intraperitoneal first-generation cephalosporin to cover Gram-positive organisms. Additionally, third-generation cephalosporin or aminoglycoside therapy was administered based on the patient’s residual renal function to target Gram-negative organisms. The choice of antibiotics was promptly adjusted once the results of dialysis effluent cultures and antibiotic susceptibility testing became available.
Clinical Outcome
Peritonitis medical cure was defined as the complete resolution of peritonitis, together with the absence of complications such as relapse/recurrent peritonitis, catheter removal, transfer to hemodialysis for ≥ 30 days, or death. Treatment failure included PD catheter removal and death.
Statistics
Statistical analyses were conducted using SPSS version 26.0 and R v. 3.3.1. Study participants divided into three equal subgroups based on the tertiles of the lymphocyte count levels: Very Low Lymphocyte Count (VLLC) Group (Lymphocyte count < 0.72×106/L), Low Lymphocyte Count (LLC) Group (Lymphocyte count: 0.72–1.11×106/L), and Normal Lymphocyte Count (NLC) Group (Lymphocyte count ≥ 1.11×106/L). Continuous variables were presented as mean ± standard deviation (SD) for normally distributed data, and comparisons between groups were performed using one-way ANOVA. Non-normally distributed variables were presented as median and interquartile range (IQR), with differences between groups assessed using the Kruskal–Wallis H-test. Categorical variables were expressed as frequencies and percentages, and inter-group differences were analyzed using the Chi-square or Fisher’s exact test. In order to evaluate the covariate adjusted relationship between peripheral blood lymphocyte counts and treatment failure, Cox regression and generalized estimation equation (GEE) analyses were conducted on the data respectively. GEE, a technique used to control for correlations among clustered records, accounted for multiple peritonitis episodes in the same patient. As a continuous variable, the fitting curve based on restricted cubic spline were performed for mapping the associations between baseline peripheral blood lymphocyte counts and the risk of treatment failure events.
Univariate COX regression assessed the individual covariate association with PDAP treatment failure. Covariates meeting the hypothesis that P ≤ 0.01 and clinically relevant to the outcome were chosen for constructing multivariate models. The fully adjusted model incorporated age, sex, CCI, etiology of kidney failure, dialysis age, peritonitis infection types, hemoglobin, albumin and total bilirubin as adjustment factors. The predictive performance of univariate and multivariate models were assessed by receiver operating characteristic curve (ROC) analyses and corresponding accuracy, including area under the curve (AUC), and 95% confidence intervals (CI).
Ultimately, in the sensitivity analysis, we ensured the robustness of the association between lymphocyte count groups and outcome across 6 subgroups: sex (male or female), age (< 55 or ≥ 55 years), dialysis age (categorized by median into short or long), renal anemia (yes or no), albumin (categorized by median: < 28.50 or ≥ 28.50 g/L), and total bilirubin (categorized by median: < 8.25 or ≥ 8.25 μmol/L). In addition, we reevaluated the enrolled patients, categorizing them into quartiles based on their lymphocyte count levels (Q1, < 0.63 × 106/L; Q2, 0.63–0.88 × 106/L; Q3, 0.88–1.25 × 106/L; and Q4, ≥1.25 × 106/L) to affirm the robustness of the study’s results.
The results were presented as hazard ratios (HR) and odds ratios (OR) with corresponding 95% CI. All figures were generated using Microsoft Visio or GraphPad Prism software. Statistical significance was defined as a P-value of ≤ 0.05.
Results
Baseline Characteristics
Based on the tertile grouping of lymphocyte counts, a total of 286 PDAP patients with an average age of 54.74 years, comprising 48.30% males, were categorized into three distinct groups: the VLLC group, the LLC group, and the NLC group, as shown in Figure 1. Analyzing demographic characteristics, it was observed that the NLC group contained a higher proportion of female patients and those with shorter dialysis age compared to other groups. In terms of the type of PDAP infection, Gram-negative strain infections, with Escherichia coli (E. coli) accounted for 41.9%, were common in the VLLC and LLC groups patients, 31.6% and 24.0% of the total, respectively. Regarding laboratory variables, higher lymphocyte counts corresponded to elevated monocyte counts and sodium levels, while total bilirubin and urea nitrogen levels were comparatively lower. Concerning PDAP prognosis, the treatment failure rates for patients within the VLLC, LLC, and NLC groups stood at 28.4%, 18.8%, and 8.4% respectively. All of these results can be seen in Table 1.
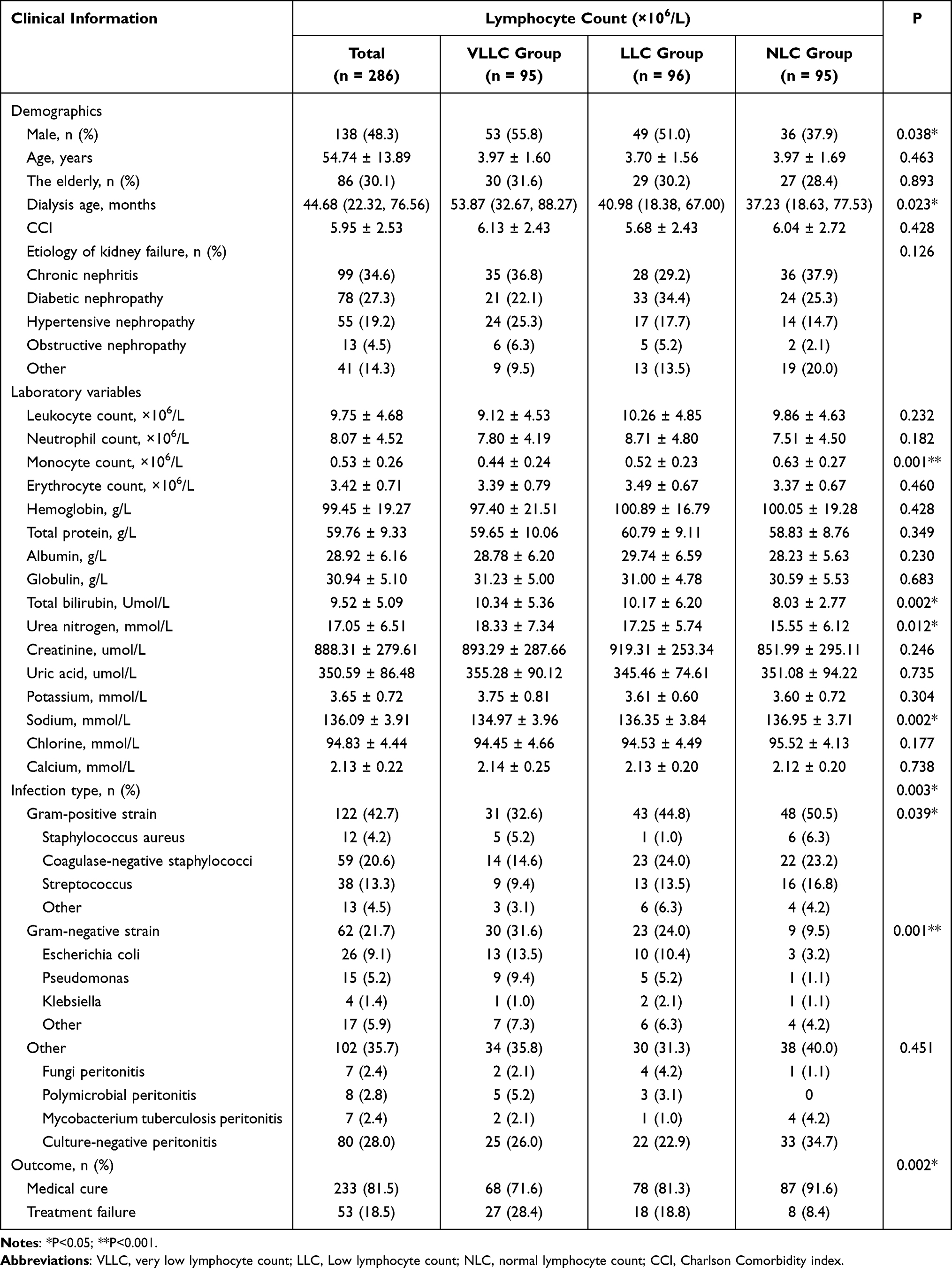 |
Table 1 Demographic and Baseline Clinical Data for Different Lymphocyte Count Group Patients |
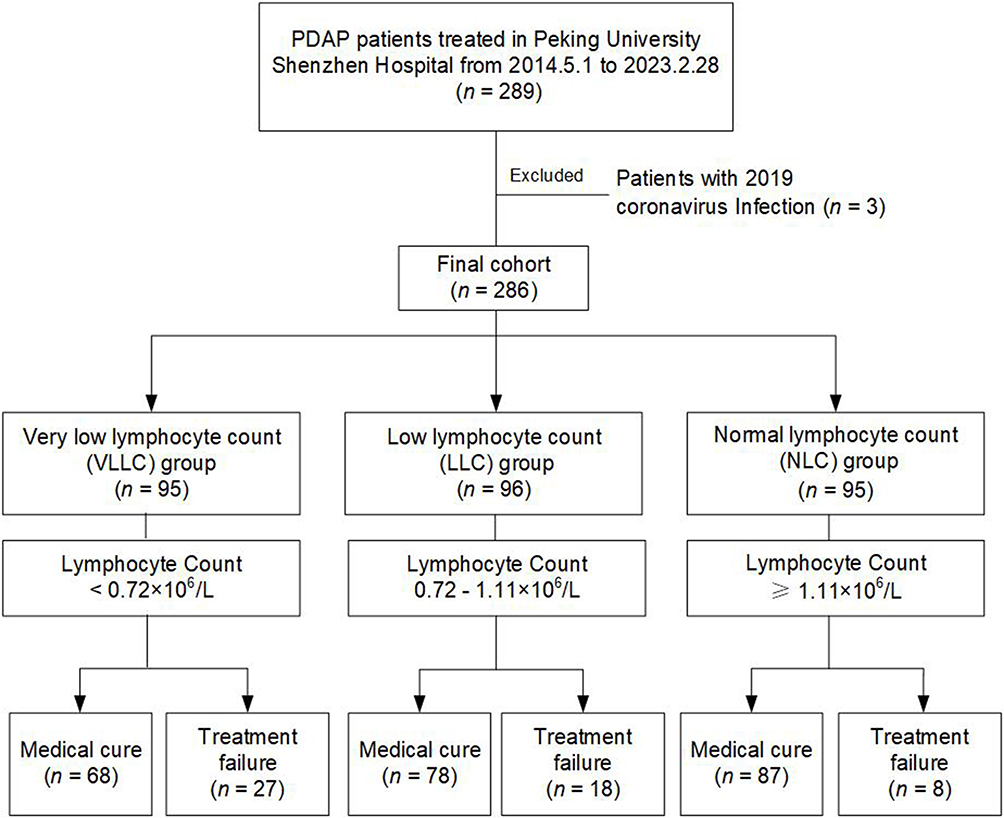 |
Figure 1 Flowchart of participants. |
Independent Predictors for Treatment Failure
The results, as shown in Table 2 and Supplemental Table 1, showed that in both Cox regression and GEE models, multivariate analyses indicated that lymphocytes were an independent protective factor for treatment failure, whereas Gram-negative and other strain infection (eg, fungi, tubercle bacillus, etc.) were independent risk factors for treatment failure.
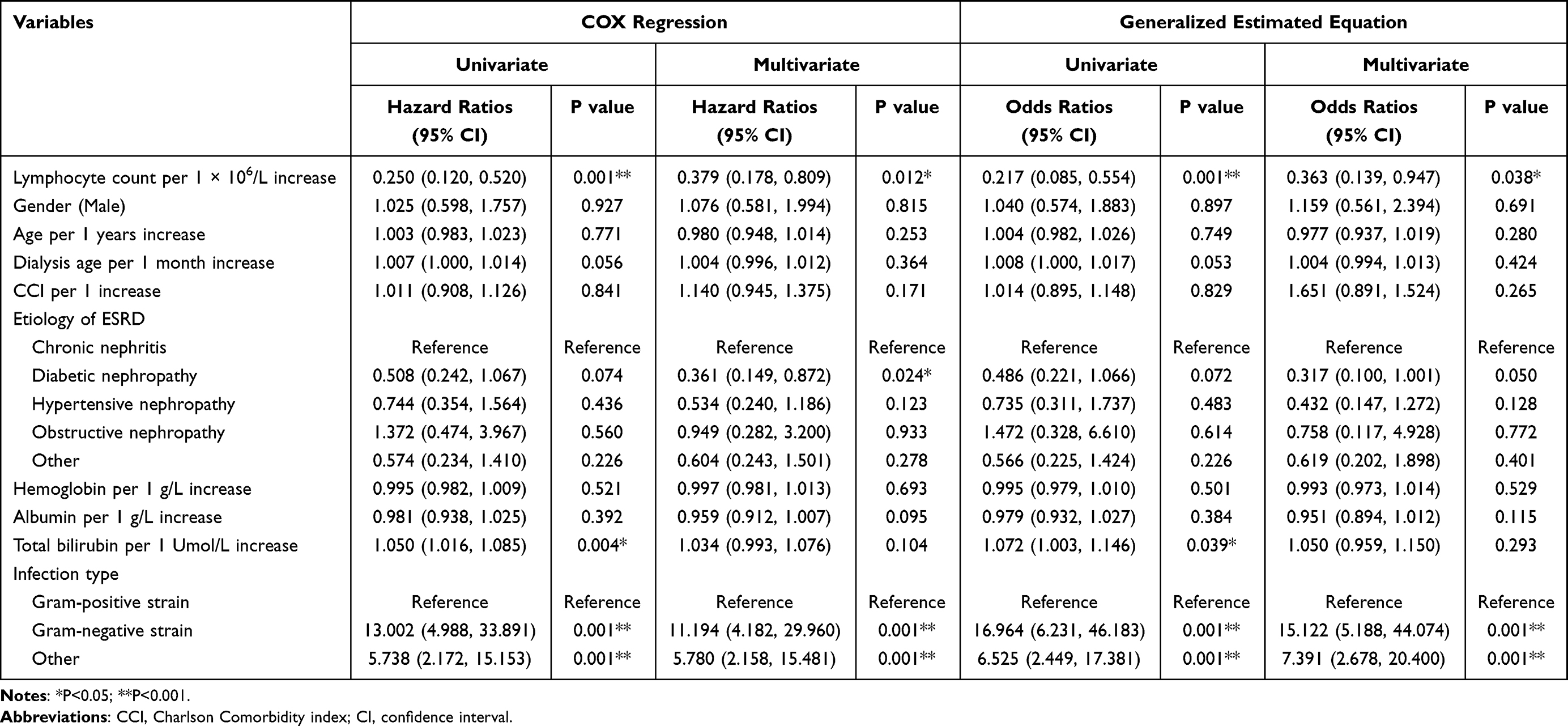 |
Table 2 Cox and Generalized Estimated Equation Analyses Independent Risk Factors Related to Treatment Failure |
Association Between Lymphocyte Count and PDAP Treatment Failure
After adjustment for demographic characteristics (gender, age, dialysis age, CCI and kidney failure etiology), laboratory parameters (hemoglobin, albumin and total bilirubin), and infection type (Gram-positive, Gram-negative, or other strain infection), relative to NLC group, the risk of treatment failure in VLLC group was higher, the hazard ratio was 2.701 in cox proportional hazard model (95% CI, 1.168–6.247; P = 0.020) and the odds ratios was 2.733 in GEE (95% CI, 1.028–7.269; P = 0.044), as shown in Figure 2.
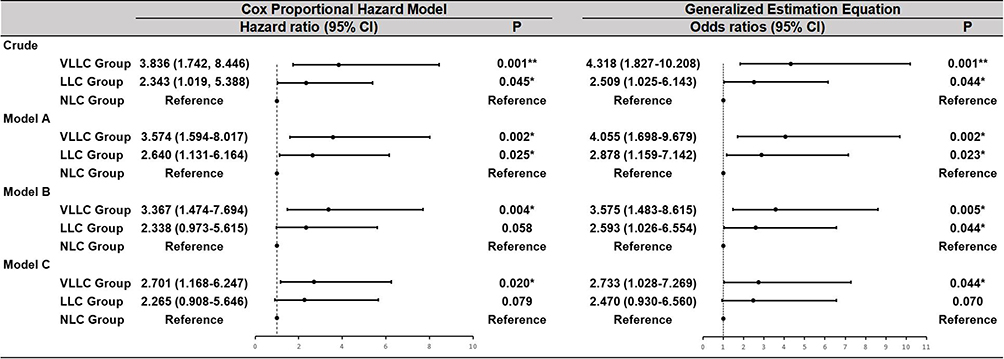 |
Figure 2 Associations between 3-level categorical variable of baseline peripheral blood lymphocyte counts and treatment failure. Crude meant no variable was adjusted; Model A was adjusted for demographic characteristics (age, sex, dialysis age, CCI and etiology of kidney failure); Model B was adjusted for demographic characteristics (age, sex, dialysis age, CCI and etiology of kidney failure) and laboratory variables (hemoglobin, albumin and total bilirubin); Model C was adjusted for demographic characteristics (age, sex, dialysis age, CCI and etiology of kidney failure), laboratory variables (hemoglobin, albumin and total bilirubin) and infection type (Gram-positive strain, Gram-negative strain and other strain infection). *P<0.05; **P<0.001. Abbreviations: PDAP, peritoneal dialysis-associated peritonitis; CCI, Charlson Comorbidity index; VLLC, very low lymphocyte count; LLC, Low lymphocyte count; NLC, normal lymphocyte count; CI, confidence interval. |
Figure 3 depicted the association between lymphocyte counts (as a continuous variable) and the hazard ratios of PDAP treatment failure. After adjustment for other potential predictors, we found that a linear negative correlation between lymphocyte counts and the risk of PDAP treatment failure (P for overall = 0.026, P for nonlinear = 0.663).
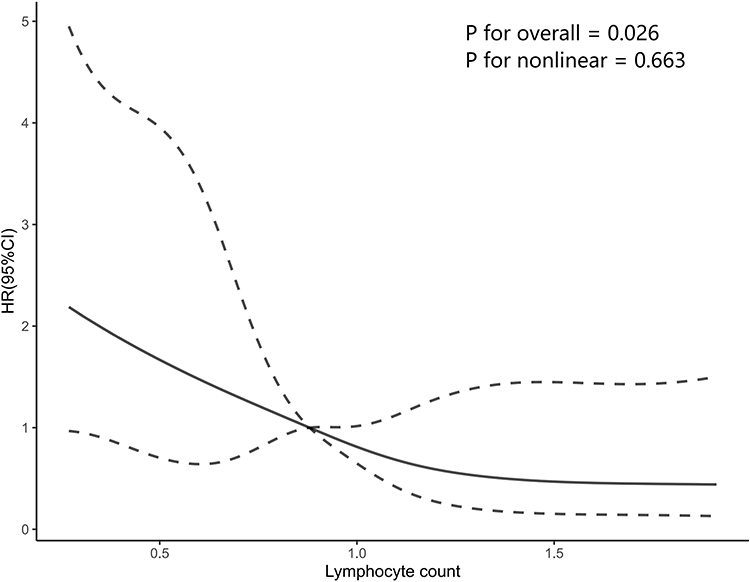 |
Figure 3 Restricted cubic spline curve showing adjusted hazard ratios and 95% confidence intervals for PDAP treatment failure in relation to baseline peripheral blood lymphocyte counts. The solid lines indicated the trend of estimated hazard ratios, the area between 2 dashed lines indicated the 95% confidence intervals. |
Predictive Performance of Univariate and Multivariate Models
As shown in Supplemental Table 2 and Figure 4, the predictive performance of lymphocyte counts (AUC, 0.683; 95% CI, 0.603–0.763; P = 0.001) was significantly higher than other variables in univariate analysis. In multivariate analyses, model A combined lymphocyte counts and demographic characteristics such as age, sex, dialysis age and etiology of kidney failure, with an AUC of 0.705 (95% CI, 0.628–0.783; P = 0.001). The predictive performance was significantly enhanced compared with the lymphocyte counts alone. After the development of model B by included laboratory variables such as hemoglobin, albumin and total bilirubin in model A, we noticed the predictive value further improved (AUC, 0.728; 95% CI, 0.651–0.805; P = 0.001). Furthermore, the predictive value would still be further elevated after the final inclusion of the type of infection into model B to build model C (AUC, 0.824; 95% CI, 0.767–0.881; P = 0.001).
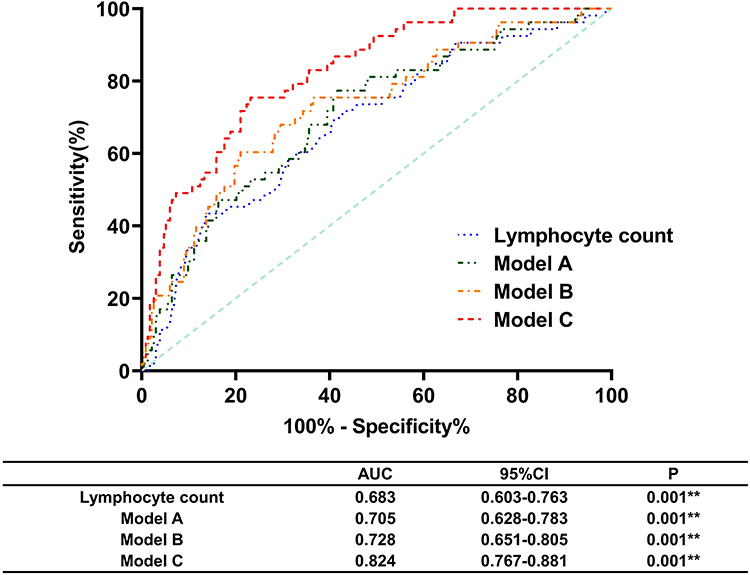 |
Figure 4 Predictive value of peripheral blood lymphocyte counts and multivariate models for treatment failure. Model A was adjusted for demographic characteristics (age, sex, dialysis age, CCI and etiology of kidney failure); Model B was adjusted for demographic characteristics (age, sex, dialysis age, CCI and etiology of kidney failure) and laboratory variables (hemoglobin, albumin and total bilirubin); Model C was adjusted for demographic characteristics (age, sex, dialysis age, CCI and etiology of kidney failure), laboratory variables (hemoglobin, albumin and total bilirubin) and infection type (Gram-positive strain, Gram-negative strain and other strain infection). **P<0.001. Abbreviations: CCI, Charlson Comorbidity index; AUC, area under the receiver operating characteristic curve; CI, confidence interval. |
Sensitivity Analyses
In stratified analyses, after adjusting for all covariates except the subgroup variables, no significant interactions were observed between lymphocyte counts and the individual subgroup variables, as indicated in Supplemental Table 3.
In addition, we employed quartile-based grouping to divide PDAP patients into four equally sized cohorts, aiming to validate the reliability of our findings. As presented in Supplemental Table 4, our results indicate that when compared to the Q4 group, PDAP patients in the Q1 group exhibited a significantly heightened risk of treatment failure in both COX regression and GEE analyses (COX Regression: HR, 4.099, 95% CI, 1.484–11.325, P = 0.007; GEE: OR, 4.571, 95% CI, 1.450–14.411, P = 0.009).
Discussion
To the best of our knowledge, this study marks the inaugural discovery of a correlation between initial peripheral blood lymphocyte counts and treatment failure in episodes of PDAP. Within this study, we formulated two predictive models, comprising lymphocyte count in conjunction with other clinical parameters. Our findings underscore a notable linkage between reduced lymphocyte count and the heightened risk of PDAP treatment failure. Furthermore, subsequent ROC analysis, following adjustments for pertinent confounders, suggests that lymphocyte count exhibits superior predictive efficacy concerning the prognosis of PDAP.
Lymphocytes play an indispensable role in the body’s immune system, participating in both innate and adaptive immunity.4 Their ability to identify specific antigens, activate immune responses, and establish immune memory is crucial for defending against infections and maintaining overall health. Extensive research has highlighted the relationship between lymphopenia and poor prognosis in various diseases.6–10 Several studies have indicated a close association between lymphocyte counts and the recurrence and prognosis of various tumors.13–15 Moreover, Ceccato et al demonstrated lymphopenia as an independent predictor of mortality in patients with ICU-acquired pneumonia.9 Wagner’s retrospective study observed a correlation between lymphocyte counts and clinical progression, as well as disease severity, in patients with Covid-19.16 Similarly, Ding et al established lymphocyte count as a reliable biomarker for predicting disease severity and clinical outcomes in patients with cryptococcal infection.17 Collectively, upon reviewing the aforementioned studies, we gained insights into the significance of lymphocyte counts in disease progression and prognosis. However, the association between peripheral blood lymphocyte counts and the prognosis of PDAP has remained enigmatic, serving as the impetus for our study hypothesis: low baseline peripheral blood lymphocyte levels potentially heighten the risk of treatment failure in PDAP patients.
Regarding lymphocyte count concerning demographic and laboratory indicators, our study results revealed that patients in the NLC group tended to have a greater proportion of females, as well as exhibiting higher levels of sodium and monocyte counts. A previous animal study has found that lymphocyte counts are significantly increased in females, while the opposite is true in males.18 Other research has also found that the capacity of sodium and monocyte counts to orchestrate modifications in lymphocyte function and distribution, often by instigating an inflammatory microenvironment or triggering pathways within the immune system.19,20 Furthermore, higher levels of dialysis age, urea nitrogen, and total bilirubin were observed in the VLLC and LLC groups. Chronic inflammation is a characteristic of patients on long-term PD and those with chronic kidney disease (CKD).21 This inflammatory state may lead to lymphocyte apoptosis.22 Simultaneously, PDAP patients with low lymphocyte counts demonstrated a more robust inflammatory response, which can elevate the body’s protein consumption, subsequently increasing urea nitrogen levels.23 Similar to prior investigations, our results indicate a plausible connection between liver function and immune competence in patients.24
Regarding infection types, our study demonstrated that Gram-negative bacterial infections were predominant in the VLLC and LLC groups, with a predominance of E. coli. Previous studies have found that lymphopenia has the potential to disrupt the intestinal barrier and gut-associated lymphoid tissue (GALT),5,25 thereby facilitating bacterial translocation from the gut to the peritoneal cavity. This phenomenon may contribute to the predominance of E. coli infections in the VLLC group.
In our work, after adjusting for other potential risk factors, low peripheral blood lymphocyte counts exhibited an incremental relationship with the risk of treatment failure. The baseline peripheral blood lymphocyte counts < 0.72×106/L (VLLC) group indicated a 2.70 and 2.73 fold increased venture of treatment failure in cox regression and GEE models, respectively, compared with ≥ 1.11×106/L (NLC) group. As a continuous variable, the restricted cubic spline showed a linear negative correlation between lymphocyte counts and the treatment failure risk. The precise mechanisms underlying the association between lymphocyte counts and PDAP treatment failure remain unclear. However, several potential mechanisms warrant consideration. Firstly, lymphocytes constitute vital components and primary effector cells that uphold the body’s immune function, playing a critical role in effective host defense against invading pathogens.4,26 T cells engage in cellular immunity, recognizing and combating pathogens that infect host cells.27 CD8+ T cells possess the ability to identify and eliminate infected host cells, thereby impeding pathogen propagation.26 Additionally, B cells serve as key agents of humoral immunity.28 Upon binding to recognized antigens, B cells differentiate into plasma cells, which generate substantial quantities of antibodies. These antibodies bind to pathogens, marking them for attack and removal by other immune cells. Furthermore, antibodies can also neutralize pathogen toxins, safeguarding host cells. NK cells exhibit “natural killer” activity against infected or transformed cells, directly recognizing and eliminating these aberrant cells without prior activation.29 NK cells release cytotoxins and chemokines that target and destroy pathogen-infected cells, thereby thwarting pathogen spread. Reduced lymphocyte counts compromise the body’s immune response, potentially impeding timely control and elimination of the infecting pathogen. This prolonged infection duration may trigger persistent peritonitis progression and lead to treatment failure.
Secondly, beyond pathogen clearance, diverse lymphocyte subtypes significantly contribute to immune response regulation, averting excessive inflammation and tissue damage. CD4+ T cells, for instance, enhance humoral immune responses by interacting with antigen-presenting cells and promoting antibody production by B cells.30,31 CD4+ T cells differentiate into subpopulations such as Th1, Th2, Th17, and Treg cells, which respectively govern cellular and humoral immunity. B cells and NK cells secrete cytokines, including IL-10, interferon, and tumor necrosis factor, influencing the activity and function of other immune cells while fostering a coordinated immune response.32,33 Lymphopenia may disrupt the equilibrium between pro-inflammatory and anti-inflammatory signaling, culminating in aberrant inflammatory responses.
Thirdly, as previously mentioned, lymphocyte-mediated immune responses play a crucial role in protecting the intestinal barrier and inhibiting bacterial translocation.5,25 Upon bacterial penetration of the epithelial layer, the body triggers an adaptive immune response to counter bacterial invasion by activating CD4+ T cells and releasing cytokines.34 Lymphopenia can potentially compromise the intestinal barrier and GALT, fostering bacterial transit from the intestines to the abdominal cavity, thus influencing peritonitis prognosis.
There are some limitations in the study. Firstly, the data were gathered exclusively from a solitary medical center, thus rendering the potential influence of center-specific variables indeterminable. The generalizability of the study’s findings to diverse populations across various geographic regions and ethnic backgrounds necessitates additional substantiation. Consequently, the imperative for expansive prospective external validation investigations, encompassing diverse settings, becomes evident, aimed at corroborating the prognostic utility of lymphocyte count. Secondly, this study solely gathered total lymphocyte counts, lacking information on lymphocyte subpopulations, highlighting the need for further research in this area. Lastly, the study solely incorporated baseline lymphocyte data, overlooking the impact of dynamic lymphocyte changes on PDAP prognosis.
Conclusion
In conclusion, our research highlights that lower peripheral blood lymphocyte counts are linked to a higher risk of treatment failure in PDAP patients. Lymphocyte counts could be a practical and reliable marker for evaluating the prognosis of PDAP, with potential implications for clinical practice. Our study suggests that it is essential for clinicians to emphasize the importance of evaluating the lymphocyte counts of patients with PDAP in the management and diagnosis of PDAP patients in order to identify patients at higher risk of treatment failure. This will allow for more targeted and effective treatment strategies to be developed for these patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Disclosure
This retrospective study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Human Investigation Committee (IRB) of the Ethics Committee of Peking University Shenzhen Hospital approved this study.
Patient Consent Statement
Informed consent was waived because it was a retrospective study, and the anonymized processing of patient data was conducted.
Acknowledgments
We are grateful to all our colleagues in the clinical departments and laboratories.
Funding
This work was supported by the General Program for Clinical Research at Peking University Shenzhen Hospital (LCYJ2021004). The authors have no relevant financial or non-financial interests to disclose.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hsieh YP, Chang CC, Wen YK, Chiu PF, Yang Y. Predictors of peritonitis and the impact of peritonitis on clinical outcomes of continuous ambulatory peritoneal dialysis patients in Taiwan--10 years’ experience in a single center. Perit Dial Int. 2014;34(1):85–94. doi:10.3747/pdi.2012.00075
2. Teitelbaum I, Ingelfinger JR. Peritoneal dialysis. N Engl J Med. 2021;385(19):1786–1795. doi:10.1056/NEJMra2100152
3. Zhou D, Yang H, Zeng L, et al. Calculated inflammatory markers derived from complete blood count results, along with routine laboratory and clinical data, predict treatment failure of acute peritonitis in chronic peritoneal dialysis patients. Ren Fail. 2023;45(1):2179856. doi:10.1080/0886022X.2023.2179856
4. Cronkite DA, Strutt TM. The regulation of inflammation by innate and adaptive lymphocytes. J Immunol Res. 2018;2018:1467538. doi:10.1155/2018/1467538
5. Hu J, Kang H, Liu C, Hu P, Yang M, Zhou F. Regulatory T cells could improve intestinal barrier dysfunction in heatstroke. Inflammation. 2019;42(4):1228–1238. doi:10.1007/s10753-019-00983-6
6. de Jager CP, van Wijk PT, Mathoera RB, de Jongh-Leuvenink J, van der Poll T, Wever PC. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit Care. 2010;14(5):R192. doi:10.1186/cc9309
7. Matera L, Nenna R, Frassanito A, et al. Low lymphocyte count: a clinical severity marker in infants with bronchiolitis. Pediatr Pulmonol. 2022;57(7):1770–1775. doi:10.1002/ppul.25919
8. Shen X, Sun J, Ke L, et al. Reduced lymphocyte count as an early marker for predicting infected pancreatic necrosis. BMC Gastroenterol. 2015;15(1). doi:10.1186/s12876-015-0375-2
9. Ceccato A, Panagiotarakou M, Ranzani OT, et al. Lymphocytopenia as a predictor of mortality in patients with ICU-acquired pneumonia. J Clin Med. 2019;8(6):843. doi:10.3390/jcm8060843
10. Cueto-Manzano AM, Quintana-Piña E, Correa-Rotter R. Long-term CAPD survival and analysis of mortality risk factors: 12-year experience of a single Mexican center. Perit Dial Int. 2001;21(2):148–153. doi:10.1177/089686080102100207
11. Zahorec R. Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102(1):5–14.
12. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
13. Feng F, Zheng G, Wang Q, et al. Low lymphocyte count and high monocyte count predicts poor prognosis of gastric cancer. BMC Gastroenterol. 2018;18(1):148. doi:10.1186/s12876-018-0877-9
14. Lee YJ, Chung YS, Lee JY, et al. Pretreatment lymphocytopenia is an adverse prognostic biomarker in advanced-stage ovarian cancer. Cancer Med. 2019;8(2):564–571. doi:10.1002/cam4.1956
15. Gawiński C, Michalski W, Mróz A, Wyrwicz L. Correlation between Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Tumor-Infiltrating Lymphocytes (TILs) in left-sided colorectal cancer patients. Biology. 2022;11(3):385. doi:10.3390/biology11030385
16. Wagner J, DuPont A, Larson S, Cash B, Farooq A. Absolute lymphocyte count is a prognostic marker in Covid-19: a retrospective cohort review. Int J Lab Hematol. 2020;42(6):761–765. doi:10.1111/ijlh.13288
17. Ding Y, Li P, He Q, et al. The CD4(+) T-lymphocyte count is an important predictor for the prognosis of cryptococcosis. Eur J Clin Microbiol Infect Dis. 2017;36(5):897–904. doi:10.1007/s10096-016-2880-9
18. Venkatasubbu GD, Ramasamy S, Gaddam PR, Kumar J. Acute and subchronic toxicity analysis of surface modified paclitaxel attached hydroxyapatite and titanium dioxide nanoparticles. Int J Nanomedicine. 2015;10(Suppl 1):137–148. doi:10.2147/IJN.S79991
19. Jobin K, Müller DN, Jantsch J, Kurts C. Sodium and its manifold impact on our immune system. Trends Immunol. 2021;42(6):469–479. doi:10.1016/j.it.2021.04.002
20. Biswas SK, Mantovani A. Macrophage plasticity and interaction with lymphocyte subsets: cancer as a paradigm. Nat Immunol. 2010;11(10):889–896. doi:10.1038/ni.1937
21. Chiu YL, Shu KH, Yang FJ, et al. A comprehensive characterization of aggravated aging-related changes in T lymphocytes and monocytes in end-stage renal disease: the iESRD study. Immun Ageing. 2018;15(1):27. doi:10.1186/s12979-018-0131-x
22. Han JB, Shu QH, Zhang YF, Yi YX. Predictive Value of Inflammation Biomarkers in Patients with Portal Vein Thrombosis. J Clin Transl Hepatol. 2021;9(3):384–391. doi:10.14218/JCTH.2020.00159
23. Fouque D, Kalantar-Zadeh K, Kopple J, et al. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008;73(4):391–398. doi:10.1038/sj.ki.5002585
24. Huang H, Chen S, Li H, et al. The association between markers of liver injury and clinical outcomes in patients with COVID-19 in Wuhan. Aliment Pharmacol Ther. 2020;52(6):1051–1059. doi:10.1111/apt.15962
25. Powell N, MacDonald TT. Recent advances in gut immunology. Parasite Immunol. 2017;39(6). doi:10.1111/pim.12430
26. Xing S, Shao P, Li F, et al. Tle corepressors are differentially partitioned to instruct CD8(+) T cell lineage choice and identity. J Exp Med. 2018;215(8):2211–2226. doi:10.1084/jem.20171514
27. Crauwels P, Bohn R, Thomas M, et al. Apoptotic-like Leishmania exploit the host’s autophagy machinery to reduce T-cell-mediated parasite elimination. Autophagy. 2015;11(2):285–297. doi:10.1080/15548627.2014.998904
28. Irons EE, Punch PR, Lau JTY. Blood-borne ST6GAL1 regulates immunoglobulin production in B CELLS. Front Immunol. 2020;11:617. doi:10.3389/fimmu.2020.00617
29. Alicata C, Ashouri E, Nemat-Gorgani N, et al. KIR variation in Iranians combines high haplotype and allotype diversity with an abundance of functional inhibitory receptors. Front Immunol. 2020;11:556. doi:10.3389/fimmu.2020.00556
30. Ghosh MK, Chen KE, Dill-Garlow R, et al. Sex differences in the immune system become evident in the perinatal period in the four core genotypes mouse. Front Endocrinol. 2021;12:582614. doi:10.3389/fendo.2021.582614
31. Cui XR, Guo YH, Liu QQ. Cangma Huadu granules, a new drug with great potential to treat coronavirus and influenza infections, exert its efficacy through anti-inflammatory and immune regulation. J Ethnopharmacol. 2022;287:114965. doi:10.1016/j.jep.2021.114965
32. Zhou XL, Zhu WG, Zhu ZJ, et al. Lymphopenia in esophageal squamous cell carcinoma: relationship to malnutrition, various disease parameters, and response to concurrent chemoradiotherapy. Oncologist. 2019;24(8):e677–e686. doi:10.1634/theoncologist.2018-0723
33. Park A, Lee Y, Kim MS, et al. Prostaglandin E2 secreted by thyroid cancer cells contributes to immune escape through the suppression of Natural Killer (NK) cell cytotoxicity and NK cell differentiation. Front Immunol. 2018;9:1859. doi:10.3389/fimmu.2018.01859
34. Fakhoury HMA, Kvietys PR, AlKattan W, et al. Vitamin D and intestinal homeostasis: barrier, microbiota, and immune modulation. J Steroid Biochem Mol Biol. 2020;200:105663. doi:10.1016/j.jsbmb.2020.105663
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Follow-up of Surgical and Nonsurgical Patients With Pulmonary Aspergillosis: A Real-World Study
Chen Z, Shang Y, Wasti B, Ou Y, Gong S, Xiang X, Ouyang R
Infection and Drug Resistance 2025, 18:1059-1070
Published Date: 21 February 2025