Back to Journals » Nature and Science of Sleep » Volume 12
Deciphering Age Differences in Experience-Based Decision-Making: The Role of Sleep
Authors Peng XR ![]() , Liu YR, Fan DQ, Lei X, Liu QY, Yu J
, Liu YR, Fan DQ, Lei X, Liu QY, Yu J ![]()
Received 18 July 2020
Accepted for publication 3 September 2020
Published 29 September 2020 Volume 2020:12 Pages 679—691
DOI https://doi.org/10.2147/NSS.S272176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Steven Shea
Xue-Rui Peng,1 Yun-Rui Liu,1,2 Dong-Qiong Fan,1,3 Xu Lei,1 Quan-Ying Liu,4 Jing Yu1,5
1Faculty of Psychology, Southwest University, Chongqing, People’s Republic of China; 2Department for Cognitive and Decision Sciences, University of Basel, Basel, Switzerland; 3School of Biological Science and Medical Engineering, Beihang University, Beijing, People’s Republic of China; 4Department of Biomedical Engineering, Southern University of Science and Technology, Shenzhen, People’s Republic of China; 5Key Laboratory of Mental Health, Institute of Psychology, Chinese Academy of Sciences, Beijing, People’s Republic of China
Correspondence: Jing Yu
Faculty of Psychology, Southwest University, Tiansheng Road, Beibei District, Chongqing 400715, People’s Republic of China
Email [email protected]
Quan-Ying Liu
Department of Biomedical Engineering, Southern University of Science and Technology, 1088 Xueyuan Avenue, Shenzhen 518055, People’s Republic of China
Email [email protected]
Objective: Recent studies have demonstrated that sleep not only facilitates memory consolidation but also benefits more complex cognitive skills such as decision-making in young adults. Older adults use different decision strategies compared with young adults, which leaves the role of sleep in older adults’ decision-making unclear. We investigated the age-by-sleep effect on decision-making.
Methods: We recruited 67 young adults (ages 18 to 29 years) and 66 older adults (ages 60 to 79 years) and randomly assigned them into the “sleep” or “wake” study condition. They were given a modified Iowa gambling task to perform before and after a 12-hour interval with sleep or wakefulness.
Results: Using the typical model-free analysis, we found that young adults’ between-session performance improved greater than that of older adults regardless of the sleep/wake condition. Furthermore, older adults with longer total sleep time showed a greater improvement in the selection of one “good” deck. To further examine the sleep effect on age-related differences in cognitive processes underlying decision-making, we conducted computational modelling. This more fine-grained analysis revealed that sleep improved feedback sensitivity for both young and older adults while it increased loss aversion for older adults but not for young adults.
Conclusion: These findings indicate that sleep promotes learning-based decision-making performance via facilitating value representation, and such modulation is distinct in young compared to older adults.
Keywords: decision-making, the Iowa gambling task, sleep, aging, computational modelling
Sleep is vital for humans, and we spend about one-third of our lives in sleep. It plays a profound role in a variety of physiological systems that maintain our health and promote cognitive function across domains.1,2 Both sleep and cognitive function of older adults alter with advanced age.3–5 While previous research has extensively focused on age differences in the sleep-related effects on emotion, memory,1,6–8 and executive function,9 little is known about age-related differences in sleep modulation effects on decision-making.
Among the widely used decision-making paradigms, the Iowa gambling task (IGT)10 has been adopted to uncover the relationship between sleep and decision-making, as it involves a feedback learning component that is often influenced by sleep.11,12 Specifically, the IGT requires participants to have reinforcement learning ability to distinguish advantageous and disadvantageous decks. The advantageous decks offer small immediate gains but even smaller losses in the long term, resulting in an overall net gain. While the disadvantageous decks produce large immediate gains but even larger losses in the long term, leading to an overall net loss. To maximize earnings, participants have to consider gains and losses, long-term and short-term payoffs, as well as uncertainty about outcomes. In sleep studies, poor IGT performance was often reported in the context of sleep deprivation13,14 and sleep disorders.15,16 Correspondingly, normal sleep was found to be beneficial to IGT performance in young adults. These studies used the “am-pm” experimental design, in which participants had either a 12-hour interval with sleep (in the sleep condition) or with wakefulness (in the wake condition) between the first test and the re-test. For example, Pace-Schott et al17 found that after a 12-hour interval, participants’ performance, indexed by their net scores, were improved more in the sleep condition compared with that of participants in the wake condition.
Although older adults exhibit cognitive declines and neurobiological impairments with aging, they can still be identified as adaptive decision-makers with the ability to distinguish advantageous decks from disadvantageous decks.18–20 However, to achieve this comparable performance as young adults, older adults may utilize different strategies based on the capacity of their cognitive resources. For instance, young adults had more strengths in learning and memory, while older adults had a more accurate representation of gains and losses.18 Moreover, older adults were more conservative in exploratory behaviour than that of young adults.21 Since these age differences were observed in the cognitive processing underlying the IGT, we speculate that the sleep effect on decision-making could be modulated by age.
The typical analysis for the IGT is usually focused on the comparison of net scores between conditions, which is often averaged by blocks of 20 trials.22–24 However, this traditional analysis approach does not provide detailed trial-by-trial information, therefore, is insufficient for a more thorough examination of decision strategy. Recently, reinforcement learning (RL) models have been adopted to break down the trial-by-trial performance of the IGT into cognitive components, such as feedback learning, memory, sensitivity, and response consistency,25,26 that may enrich our understanding of the cognitive processes underlying decision-making. In this study, we applied the RL models to investigate the sleep effect on decision-making modulated by age.
The overarching aim of the present study is to examine whether sleep contributes to the performance of IGT, and whether and how this potential sleep effect is modulated by age. We conducted both model-free and model-based analysis to examine decision strategies used by young and older adults. Moreover, we investigated the association between IGT performance and sleep characteristics in order to explore the possible mechanisms underlying the age-by-sleep effect.
Methods
Participants
We recruited 68 young adults (aged 18–29) from a university and 70 older adults (aged 60–79) from adjacent communities. Older adults were independent community-dwelling adults with a mean score of 28.9 ±1.13 in the mini-mental state examination (MMSE).27 Participants were all right-handed, had no history of psychiatric, neurological diseases, or sleep disorders, and had normal or corrected-to-normal vision. Five participants were excluded: three older adults with MMSE scores below 25, and two participants (one old and one young) with incomplete data recording. Participants were randomly assigned to the wake or the sleep condition groups. Thus, the sample used for the following analyses included 67 young adults—33 in the sleep condition and 34 in the wake condition—and 66 older adults—32 in the sleep condition and 34 in the wake condition. As shown in Table 1, participants in the wake and sleep conditions were well matched for demographic and neuropsychological characteristics across age groups. With respect to age differences, older adults were generally less educated and more morningness-oriented, and they had generally poorer subjective sleep quality. Considering the significant differences in education and circadian chronotype between the two age groups, we conducted additional analyses to control for these confounding variables. The significance of our results was not affected by these covariates (see Supplementary Tables S1 and S5).
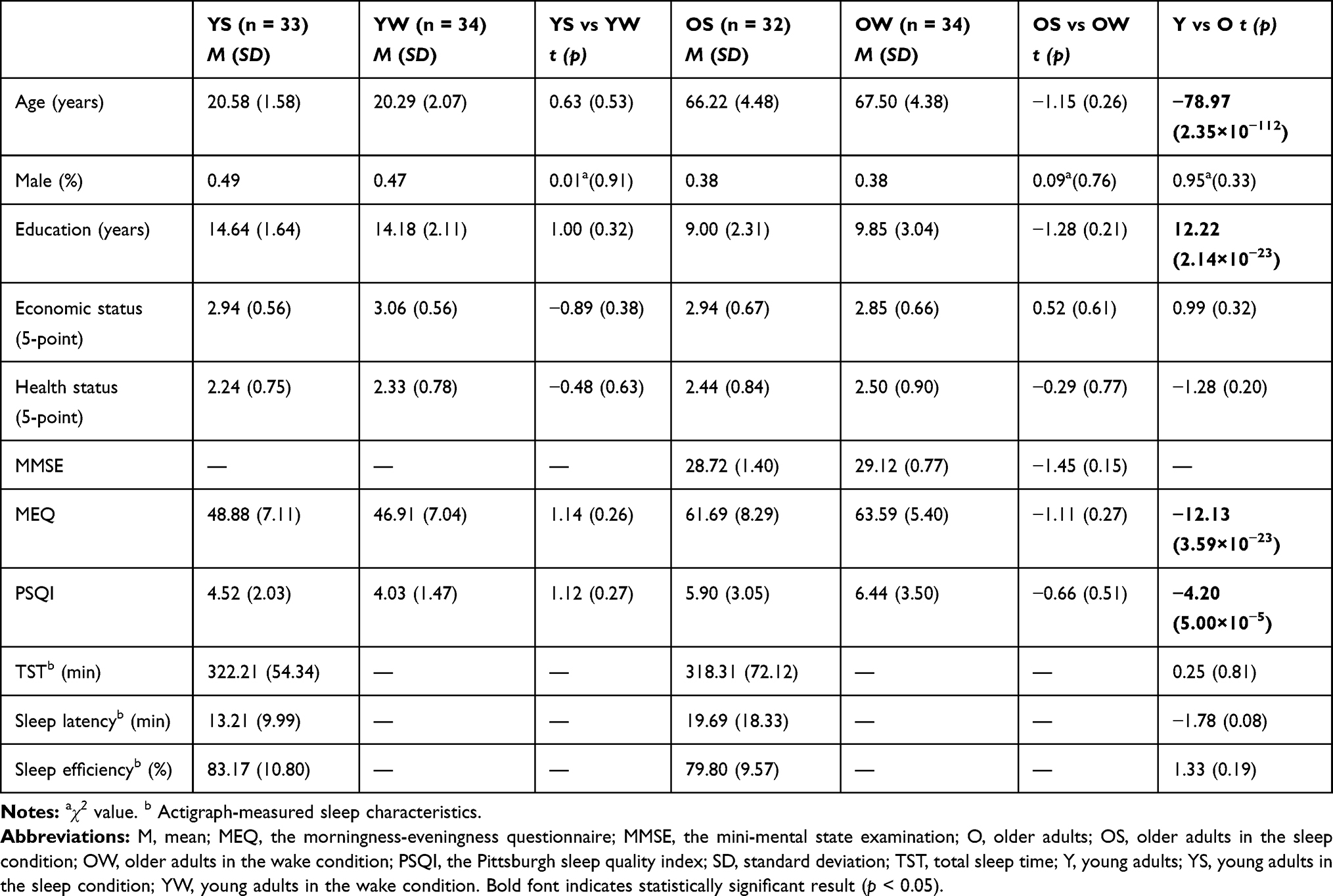 |
Table 1 Participants’ Characteristics and Neuropsychological Data |
This study was approved by the ethics committees of the Faculty of Psychology, Southwest University (H17001), and was conducted in accordance with the Declaration of Helsinki. Participants provided informed consent prior to the experiment. Each participant received 40 CNY (ca. 6 USD) for participation in the study, with the opportunity to earn up to an additional 40 CNY based on their performance in the task.
Materials and Procedure
The experiment consisted of two sessions (Figure 1A). The first session was conducted either in the morning (7:30–9:30 am; wake condition) or in the evening (7:30–9:30 pm; sleep condition), and the second session was conducted 12 hours later (following an interval of wakefulness or sleep). Participants in the wake condition were not allowed to have a nap before the re-test session. All participants were asked to provide a record of their sleep/daily activities of the previous night/daytime prior to each session. To monitor the sleep of participants in the sleep condition, they were asked to wear an actigraph (BodyMedia FIT LINK) on their non-dominant wrist during sleep. Sleep parameters, including total sleep time (TST), sleep latency, and sleep efficiency were obtained from Sense Wear Software 8.1 (BodyMedia LINK).
 |
Figure 1 Experimental procedure and design. (A) Experimental procedure. The first session was conducted either in the morning (7:30–9:30 am; the wake condition) or in the evening (7:30–9:30 pm; the sleep condition), followed by a re-test session 12 hours later. (B) Screenshot of the Iowa gambling task. The green bar shows the amount of money participants gained; the red bar shows the amount of money participants borrowed. In this example, the participant selected deck A and gained 100 CNY. |
The Iowa Gambling Task
In the present study, we adopted a well-known experience-based decision-making task, the Iowa gambling task (IGT)10,28 The computerized version of IGT was written with MATLAB 2018a (MathWorks) based on Psychtoolbox (www.psychtoolbox.org). As shown in Figure 1B, in each trial of the task, participants were asked to choose one of four decks (A, B, C and D) on a screen. Two of the decks (A and B) were disadvantageous decks with net losses in the long term, whereas two of the decks (C and D) were advantageous decks with net gains in the long term. Additionally, losses are more frequent in decks A and C (50%) than in decks B and D (10%). Each deck has up to 60 draws and the net gains/losses increase with every 10 draws.29 Specifically, the net profit of decks A and B in the first 10 draws are −250 CNY, and it is increased by −150 CNY every 10 draws; the net profit of decks C and D in the first 10 draws are 250 CNY, and it goes up by 25 CNY every 10 draws. Participants were only told that sometimes they would gain and sometimes they would lose and that some decks might be better than others; they were not told which decks were good or bad. They were required to gain as much as possible, as total gain in the task would be converted into their monetary recompense for the study. There were two bars at the top of the screen, with the green bar showing the amount of money participants gained and the red bar showing the amount of money participants borrowed. The green bar was updated according to the outcome after each selection. If participants’ amount of gain was less than 0, a load of 2000 CNY was added to the red bar automatically while the green bar was reset accordingly. Participants were informed of their net outcome (ie, the total amount of money gained minus the total amount of money borrowed) at the end of the task. Participants completed 100 trials in each session, and the features of the four decks were kept the same across the two sessions to avoid reversal learning.
Data Analysis
We calculated the net score for each participant in each session, as net scores have been widely used in the IGT studies to quantify participants’ task performance.10,30,31 To examine the feedback learning process, the 100 trials were divided into 5 consecutive blocks with each containing 20 trials. A net score was calculated by subtracting the number of draws of the disadvantageous decks from the number of draws of the advantageous decks [(C + D) – (A + B)] for each block. The net scores were examined using a repeated-measure ANOVA, with age (young, old) and condition (sleep, wake) as between-subject variables, session (test, re-test), and block (1–5) as within-subject variables.
Previous studies identified the decreasing selection of deck B as evidence of sleep beneficial effect on decision-making.22,23 Thus, we calculated the proportional change of each deck selection from session 1 to session 2 in order to examine whether the sleep-related improvement was deck-specific. A repeated-measure ANOVA with age (young, old) and condition (sleep, wake) as between-subject variables and deck (A, B, C, D) as a within-subject variable was performed. Next, we conducted correlation analyses between sleep and decision-performance changes. Statistical analyses were performed using SPSS 26.0 (IBM Corporation, Armonk, NY, USA).
Computational Modelling
The IGT is a complex, experience-based, decision-making task involving multiple cognitive processes such as feedback learning, reward sensitivity, loss aversion, time insight, and exploration. Computational modelling is a useful tool for understanding task performance at a more nuanced level. Three commonly used and validated reinforcement learning models of the IGT were applied: the Prospect Valence Learning (PVL)-Decay model,32 the PVL-Delta model33 and the Value-Plus-Perseverance (VPP) model.34 The main difference between these models is how the expected value of each option updates over time.
The PVL-Decay and PVL-Delta Model
The concepts of PVL models include utility function, learning rule, and choice rule. Outcomes of decisions are evaluated according to the prospect utility function. The utility  of outcome
of outcome  on the
on the  trial is expressed as:
trial is expressed as:
where  is a shape parameter, which determines sensitivity to outcome feedback, while
is a shape parameter, which determines sensitivity to outcome feedback, while  is a loss-aversion parameter, which determines sensitivity to losses versus gains. Higher
is a loss-aversion parameter, which determines sensitivity to losses versus gains. Higher  means greater sensitivity to feedback (i.e., giving higher subjective value to outcomes). A value of
means greater sensitivity to feedback (i.e., giving higher subjective value to outcomes). A value of  indicates higher sensitivity to gains other than losses, whereas
indicates higher sensitivity to gains other than losses, whereas  represents the opposite.
represents the opposite.
These two PVL models are identical in utility function and choice rule but are different in learning rule. In the decay rule, the expected value for all decks is discounted in each trial, and the expected value of the selected deck is updated by its current utility. For example, the expected value of the jth deck in the (t + 1) trial,  , is updated as:
, is updated as:

where  is a decay parameter, which determines how much past expectancy is discounted;
is a decay parameter, which determines how much past expectancy is discounted;  when the jth deck is the selected deck, otherwise
when the jth deck is the selected deck, otherwise  . However, in the delta rule, only the expected value of the selected deck will be updated, and expected values of unselected decks remain unchanged, which is expressed as:
. However, in the delta rule, only the expected value of the selected deck will be updated, and expected values of unselected decks remain unchanged, which is expressed as:

where  is a learning rate, which determines the weight of past experiences versus recent experiences. A high learning rate means recent outcomes have greater influence other than past outcomes on the expected value of the selected deck, whereas a low learning rate means the opposite. In addition,
is a learning rate, which determines the weight of past experiences versus recent experiences. A high learning rate means recent outcomes have greater influence other than past outcomes on the expected value of the selected deck, whereas a low learning rate means the opposite. In addition,  is the prediction error. The softmax function35 was used as a choice rule to calculate the probability of selecting deck
is the prediction error. The softmax function35 was used as a choice rule to calculate the probability of selecting deck in
in  trial:
trial:


where the sensitivity  changes over trials depending on the response consistency parameter
changes over trials depending on the response consistency parameter  . Greater
. Greater  means the continuous selection becomes less random and more determined by expected deck utility. In sum, the PVL models have four free parameters: the feedback sensitivity parameter
means the continuous selection becomes less random and more determined by expected deck utility. In sum, the PVL models have four free parameters: the feedback sensitivity parameter  , the loss-aversion parameter
, the loss-aversion parameter  , the learning rate
, the learning rate  in the PVL-delta model and the decay parameter
in the PVL-delta model and the decay parameter  in the PVL-decay model, as well as the choice sensitivity
in the PVL-decay model, as well as the choice sensitivity  .
.
The VPP Model
The VPP model is an updated version of the PVL-delta model, which consists of the same utility function, learning rule and choice rule but combines an additional psychological process, perseverance (ie, win-stay-loss-switch choice behaviour), and is expressed as:

where  is a perseverance decay rate, which determines participants’ decay of tendency to select the deck
is a perseverance decay rate, which determines participants’ decay of tendency to select the deck  in each trial;
in each trial;  or
or  is the outcome impact parameter, depending on whether the outcome of selected deck
is the outcome impact parameter, depending on whether the outcome of selected deck  in the
in the  trial is positive (i.e., gain) or negative (i.e., loss). Specifically, positive
trial is positive (i.e., gain) or negative (i.e., loss). Specifically, positive  or
or  means a persistent tendency (i.e., to select the same deck in the next trials) while a negative value means a switching tendency (i.e., to select other decks in the next trials). The VPP model also assesses the persistence and maximization of expected utility as two basic but independent psychological processes. A weighted average of these two processes is used in the choice rule to determine the probability of selecting deck
means a persistent tendency (i.e., to select the same deck in the next trials) while a negative value means a switching tendency (i.e., to select other decks in the next trials). The VPP model also assesses the persistence and maximization of expected utility as two basic but independent psychological processes. A weighted average of these two processes is used in the choice rule to determine the probability of selecting deck  in the
in the  trial (i.e., the next trial), which is expressed as:
trial (i.e., the next trial), which is expressed as:


where  determines the weight of expected utilities of deck and
determines the weight of expected utilities of deck and  determines the weight of perseveration process. A value of
determines the weight of perseveration process. A value of  indicates the expected utilities of the deck have more weight while a value of
indicates the expected utilities of the deck have more weight while a value of  indicates the perseveration of the deck has more weight. In sum, the VPP model has eight free parameters: the feedback sensitivity (α), the loss aversion (
indicates the perseveration of the deck has more weight. In sum, the VPP model has eight free parameters: the feedback sensitivity (α), the loss aversion ( ), the learning rate (
), the learning rate ( ), the gain impact (
), the gain impact ( ), the loss impact (
), the loss impact ( ), the perseverance decay rate (
), the perseverance decay rate ( ), the choice sensitivity (
), the choice sensitivity ( ), as well as the reinforcement learning weight (
), as well as the reinforcement learning weight ( ).
).
Model Fits and Comparisons
Model fitting and parameter estimation were performed for each session in each group using a hierarchical Bayesian analysis approach based on the implemented algorithms using the hBayesDM R package (https://cran.rproject.org/web/packages/hBayesDM/index.html). Four chains were used, each of which comprised 2000 iterations; the initial half of each chain was discarded as burn-in (1000 samples × 4 chains = a total of 4000 samples).36 Model fits were assessed using the Widely Applicable Information Criterion (WAIC).37 This index is a “more fully Bayesian approach”38 that uses point-by-point log-likelihood posterior predictive density, and a penalty term is used to control the trade-off between goodness of fit and complexity of the model. Smaller WAIC indicates better model-fit, and the overall fitness is assessed by the sum of WAIC in each group for each model.
Model-based estimates (mean) for parameters were analyzed using repeated-measure ANOVAs with age (young, old), condition (sleep, wake) as between-subject variables, and session (test, re-test) as a within-subject variable. Bonferroni correction with p < 0.05/8 = 0.0063 were applied for multiple comparisons. Moreover, we performed correlation analyses between sleep characteristics and parameters estimation from the winning model to investigate individual differences in the relationship between sleep and cognitive processes underlying IGT.
Results
Model-Free Analyses on the Net Score
The net score was examined using a 2 (age: young, old) × 2 (condition: sleep, wake) × 2 (session: test, re-test) × 5 (block: 1–5) repeated-measure ANOVA, with age and condition as between-subject variables, session and block as within-subject variables. As shown in Figure 2A, all groups showed an increased tendency of net score as a function of learning, resulting in significant main effects of block (F4, 130 = 19.18, p = 2.48 × 10−12, partial η2 = 0.13) and session (F1, 130 = 37.55, p = 1.01 × 10−8, partial η2 = 0.23). In addition, there was a significant interaction of age × session (F1, 130 = 7.78, p = 0.006, partial η2 = 0.06). The Bonferroni-corrected simple effect analyses showed that young adults’ net scores showed greater between-session increases (Msession1 = 0.004, SD = 0.28; Msession2 = 0.25, SD = 0.40; p = 3.73 × 10−9) than those of older adults (Msession1 = 0.06, SD = 0.32; Msession2 = 0.16, SD = 0.25; p = 0.02). No other significant main effects or interactions of net score were observed.
 |
Figure 2 (A) The net score in five 20-trial blocks for four groups in session 1 and session 2, respectively. (B) The proportion change in the selection of each deck (A, B, C and D) from session 1 to session 2. Performance improvement is manifested as the decreased selection of disadvantageous decks (A and B) and increased selection of advantageous decks (C and D). (C) The correlation between total sleep time and the proportion of selection change of advantageous deck D. *** p < 0.001. |
For the proportional change of each deck selection, a 2 (age: young, old) × 2 (condition: sleep, wake) × 4 (deck: A, B, C, D) repeated-measure ANOVA with age and condition as between-subject variables, deck as a within-subject variable was performed. The analysis revealed a significant main effect of deck (F3387 = 17.13, p = 5.83 × 10−9, partial η2 = 0.12) and an interaction of age × deck (F3387 = 9.61, p = 2.20 × 10−5, partial η2 = 0.07). Bonferroni-adjusted pairwise comparisons showed that young adults reduced the selection of the disadvantageous deck B more than older adults (p = 2.56 × 10−4) while increased the selection of the advantageous deck C more compared with older adults (p = 3.40 × 10−5; Figure 2B).
Correlation analyses revealed that the TST was positively correlated with increases in the selection of advantageous deck D in older adults (r = 0.53, p = 0.002; Bonferroni corrected) but not in young adults (r = −0.10, p = 0.57; Figure 2C). The difference between these two correlations was significant (z = 2.65, p = 0.008). No other significant correlation between sleep characteristics and changes in deck selection survived after multiple comparison correction (see Supplementary Table S2 for all correlation results).
Together, the analyses of net scores suggest that young adults experienced a greater feedback learning effect than older adults in general, manifested as greater performance improvements from session 1 to session 2. Specifically, young adults demonstrated a greater decrease in their selections from disadvantageous deck B and greater increases in their selections from advantageous deck C. However, the evidence of an impact based on condition, ie, sleep versus wake, was relatively weak, only manifesting as the positive correlation between the TST and the increased selection of advantage deck D in older adults.
Computational Modelling
Model Fitting and Comparison
As shown in Table 2 and Supplementary Figure S1, model comparisons suggested that the VPP model (WAICsum = 59,244.57) provided the best model-fit relative to the PVL-Decay (WAICsum = 66,136.71) and the PVL-Delta model (WAICsum = 62,746.38) in all 4 groups and 2 sessions. In addition, we performed model simulation for the VPP model for each session of each participant based on their parameter estimates to evaluate model fit.39 Real data and simulated data of the number of each deck selection in each session showed strong correlations (ps < 0.001; Supplementary Figure S2).
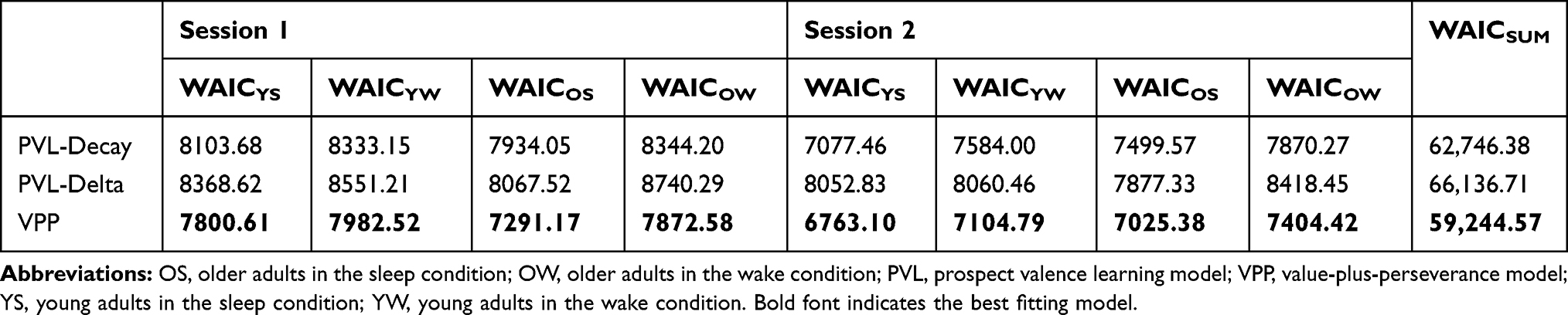 |
Table 2 Widely Applicable Information Criterion (WAIC) Scores of Each Model for Each Group |
Parameter Comparison
We extracted model parameters from the winning model, ie, the VPP model, to compare specific cognitive processes underlying decision-making assumed by the model among groups. Parameter estimates of the VPP model are provided in Supplementary Table S3, and the other two models are summarized in Supplementary Table S4. In the following, we reported the 2 (age: young, old) × 2 (condition: sleep, wake) × 2 (session: test, re-test) repeated-measure ANOVA results of parameter estimates (ie, α, the feedback sensitivity and λ, the loss aversion) that had significant interaction effects of age × condition × session after Bonferroni correction, which reflected the mediation effect of age on the association between sleep and decision-making.
α: Feedback Sensitivity
Feedback sensitivity results yielded the significant main effects of session (F1, 129 = 248.57, p = 7.10 × 10−32, partial η2 = 0.66), condition (F1, 129 = 286.75, p = 1.39 × 10−34, partial η2 = 0.69) and age (F 1129 = 800.62, p = 3.59 × 10−57, partial η2 = 0.86). Moreover, there was a two-way interaction of age × condition (F 1129 = 360.75, p = 3.47 × 10−39, partial η2 = 0.74) and a three-way interaction of age × condition × session (F 1129 = 359.98, p = 3.85 × 10−39, partial η2 = 0.74).
As shown in Figure 3, Bonferroni-adjusted pairwise comparisons showed that feedback sensitivity for young adults increased significantly in the sleep condition (MYS1 = 0.07, SD = 0.01; MYS2 = 0.10, SD = 0.08; p = 0.002), but decreased significantly in the wake condition (MYW1 = 0.56, SD = 0.08; MYW2 =0.09, SD = 0.02; p = 1.12 × 10−77). For older adults, feedback sensitivity increased significantly in the sleep condition (MOS1 = 0.04, SD = 0.02; MOS2 = 0.12, SD = 0.05; p = 7.41 × 10−11), whereas there was no significant difference between two sessions in the wake condition (MOW1 = 0.02, SD = 0.001; MOW2 = 0.02, SD = 0.004; p = 0.94).
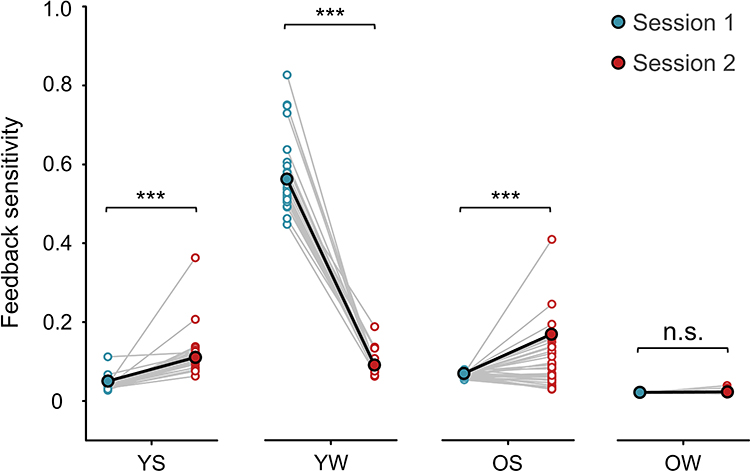 |
Figure 3 Group-level and individual-level feedback sensitivity α changes after sleep or wakefulness interval for young and older adults. *** p < 0.001. |
Loss aversion showed significant main effects with session (F 1,129 = 21.91, p = 7.00 × 10−6, partial η2 = 0.15) and age (F 1129 = 106.36, p = 1.48 × 10−18, partial η2 = 0.45). Moreover, there were a significant two-way interaction of age × condition (F 1129 = 20.56, p = 1.30 × 10−5, partial η2 = 0.14) and a three-way interaction of age × condition × session (F 1129 = 20.73, p = 1.20 × 10−5, partial η2 = 0.14).
As shown in Figure 4, Bonferroni-adjusted pairwise comparisons showed that for young adults, there was no significant difference between two sessions in the sleep condition (MYS1 = 0.32, SD = 0.02; MYS2 = 0.34, SD = 0.17; p = 0.63), whereas loss aversion was decreased significantly in the wake condition (MYW1 = 0.73, SD = 0.46; MYW2 = 0.05, SD = 0.001; p = 4.15 × 10−30). For older adults, loss aversion was increased significantly in the sleep condition (MOS1 = 0.02, SD = 0.001; MOS2 = 0.27, SD = 0.18; p = 1.87 × 10−7), whereas there was no significant difference between sessions in the wake condition (MOW1 = 0.12, SD = 0.005; MOW2 = 0.09, SD = 0.01; p = 0.53). Unfortunately, no correlation between sleep characteristics and model parameters survived after multiple comparison correction.
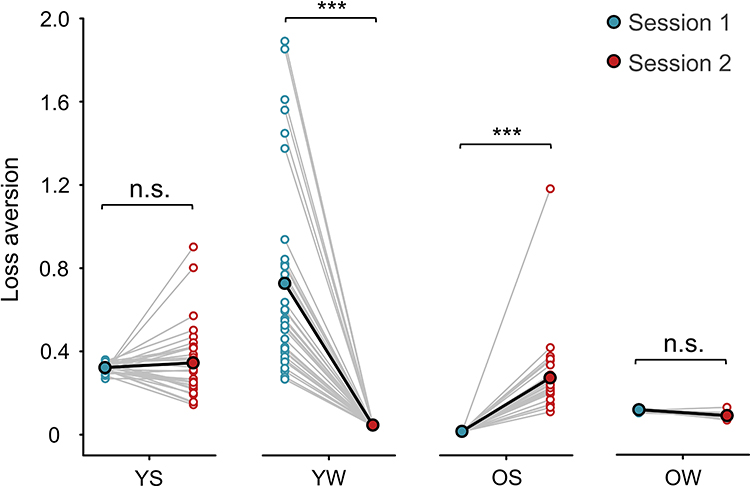 |
Figure 4 Group-level and individual-level loss aversion λ changes after sleep or wakefulness interval for young and older adults.*** p < 0.001. |
Discussion
To the best of our knowledge, this is the first study to investigate age differences in the sleep-related modulation effects on experience-based decision-making. With typical net score analysis, we only found a salient age difference on the feedback learning effect, illustrated as young adults selecting fewer disadvantageous decks and more advantageous decks in the re-test session compared with older adults. Nevertheless, with a more fine-grained analysis considering the underlying cognitive processes, age-by-condition interactions were observed in feedback sensitivity (α) and loss aversion (λ), illustrated by sleep improving feedback sensitivity for both young and older adults (Figure 3) while increasing loss aversion in older adults but not in young adults (Figure 4). Together, these findings indicate that sleep plays a distinct role in the modulation of decision-making in both young and older adults.
Enhancement of Feedback Sensitivity Following Sleep
Due to the complexity of IGT, the behavioural analysis of net scores may not be sufficient to reflect the underlying psychological processes.25,26 Therefore, in the present study, we further conducted computational modelling to break down the decision-making process in the IGT into multiple cognitive components, which could then be assessed and associated with the effects of sleep and aging. Consistent with previous studies,26,32,34,40 we confirmed that the VPP model provided the best model-fit relative to the other two models (ie, the PVL-Delta and PVL-Decay model).
Among model parameters provided by the winning model, an age-by-condition interaction was observed in the feedback sensitivity. Feedback sensitivity is an index of how sensitive an individual is to the changes in monetary outcomes. A closer inspection of data revealed that post-test sleep increased both young and older adults’ feedback sensitivity in the re-test, while the feedback sensitivity decreased in young adults but was retained in older adults who had a wakefulness interval (Figure 3). According to the synaptic homeostatic hypothesis,41,42 the role of sleep is to downscale synaptic strength to a baseline level and allow the organism to learn afresh the next day. In the case of IGT, decision-making is based on information processing of feedback and prior experience. Participants with post-test sleep may have synaptic downscaling to the pre-test level and corresponding promotion of synaptic competition leading to an increase of feedback sensitivity the next morning regardless of age. On the contrary, during wakefulness, individuals interact with the environment and acquire information from it, possibly leading to an increase in synaptic strength in many brain circuits, consuming energy and space; thus, the ability of the brain to acquire new information may be weakened after long-term wakefulness.
Indeed, we found that young adults’ feedback sensitivity decreased after a 12-hour period of wakefulness (Figure 3). According to their daily activity records (Supplementary Table S6), young adults were primarily involved in activities with high cognitive load, such as studying in class, doing homework, or playing video games during post-test wakefulness. These activities occupy cognitive resources and may cumulatively decrease synaptic plasticity, ultimately leading to the declines of feedback sensitivity in the re-test. Using reversal learning paradigms, previous studies found that young adults were less sensitive to feedback under sleep deprivation, showing impairments of adaptive decision-making ability.43,44 Similarly, our results suggested that although a 12-hour wakefulness did not affect young adults’ net scores in the IGT, it made them less sensitive to feedback. Of note, this wakefulness influence on feedback sensitivity was modulated by age. Older adults’ daily activity records showed that they often engaged in relatively low-cognitive-load activities, such as doing housework, walking, and participating in social activities (Supplementary Table S6). These activities may have less impact on cognitive-dependent synaptic plasticity, therefore allowing us to observe retained feedback sensitivity at re-test in older adults. These findings imply that the alterations of feedback sensitivity not only depend on the length of wakefulness but also the content of it (how people spend that time).
Alteration of Loss Aversion Following Sleep
In the VPP model, loss aversion is an index of how much an individual is averse to losses relative to preference toward gains at the same magnitude. Higher loss aversion suggests that an individual is more sensitive to losses than to gains. The value range of loss aversion in this study is consistent with previous studies.32,40 Similar to the findings of feedback sensitivity, our findings showed that loss aversion decreased with post-test wakefulness in young adults but was retained in older adults. On the other hand, sleep sustained young adults’ loss aversion whereas it boosted older adults’ loss aversion in the re-test. Although the negative information leads to an aversion, a higher loss aversion, helping us be alert to losses and danger, plays a vital role in our survival during evolution. Here, our finding supported that sleep facilitates young adults retaining their alertness to negative information.
As for the older adults, according to the socioemotional selectivity theory (SST), older adults attend to prioritize current goal related to emotional satisfaction as they approach the end of life. One aspect of this optimization may involve reducing negative arousal45,46 and a general decrease in sensitivity to negative feedback during information processing.47 With regard to decision-making, in line with the prediction from the SST, older adults exhibited a preserved function of the anticipation of rewards but showed a relative reduction in activation during loss anticipation.48 Similarly, findings were found with a reinforcement learning paradigm that older adults showed more decision-making noises compared to younger counterparts when learning from negative feedbacks.49,50 The increased noises and decreased anticipation of loss may lead older adults to make more high-risk choices, manifested as choosing more disadvantageous decks in the IGT. Importantly, the current study found that sleep could promote older adults’ feedback sensitivity and loss aversion, both of which are essential components of error prediction. Thus, compared with younger counterparts, older adults may need to “sleep on it” more when it comes to an important or difficult decision in daily life.
In addition, the IGT has been used as a testing tool of the somatic marker hypothesis (SMH).28,51 The SMH assumes that in complex and uncertainty environments, emotional reactions (ie, somatic makers) produced by previous experience of the emotional feedback following selection could promote rational decision-making in the long term. Specifically, it helps avoiding disadvantageous selections. However, this hypothesis has been disputed in the field.52,53 Several researches suggested that with the temporary emotion regulation, participants cannot adopt rational strategies to maximize their long-term profits in the IGT.30,54 In line with these findings, we found that sleep facilitated participants’ loss aversion; however, this emotion-related regulation did not translate into performance improvement.
Change of Model-Free Index Following Sleep
Our results showed that sleep might not directly contribute to the performance improvement in the IGT in terms of net score in young adults, which is inconsistent with previous studies.22,24 The inconsistencies may be attributed to the characteristics of IGT and the relatively low monetary amount involved in our study. For example, Abe et al24 used a variant version of IGT with 10-times higher feedback monetary amounts relative to the original version10,28 and fewer trials (reduced from 100 trials to 60 trials). These alterations may increase the task difficulty and correspondingly provide enough room for the subsequent potential post-sleep enhancement. In our study, we adopted the modified version of IGT29 and found there were 6 young adults in the sleep condition reached the highest net score (ie, 1) in the second block of session 2, implying that the ceiling effect of young adults’ performance may lead to a lack of sleep-wake difference in the current study. Indeed, using the original IGT, Pace-Schott et al17 found that sleep protective effect was only observed in the poor performance participants (ie, remained both advantageous decks by 80 selections) but not in the superior performance participants (ie, had emptied one of the advantageous decks by 80 selections). Together, previous sleep-related learning studies suggested that the beneficial effect of sleep could depend on the degree of prior sleep learning.17,55 Although the current study cannot offer direct evidence supporting this hypothesis, the notion of the difficulty of IGT being linked to sleep effect offers a potential avenue for future research aimed at connecting sleep and age interactive effects on decision-making.
We found that older adults with longer TST showed a larger increasing of selection of advantageous deck D, indicating a positive role of sleep in decision-making in older adults. The loss frequency of deck D is lower (10%) compared with another advantageous deck C (90%). Thus, the deck D is a more gain-framed deck. Previous research demonstrated age differences on negative bias in the context of IGT,18 and our results extended it and showed that this age-related bias also existed in the modulation effect of sleep on decision-making. We did not find any association between sleep characteristics and performance change in young adults. One possible reason is that while the actigraph can provide basic sleep parameters such as TST and sleep efficacy, it cannot recognize specific sleep stages (ie, N1, N2, N3, and REM). The improvement in young adults may be stage-dependent. Furthermore, a recent study showed that the theta activity during REM sleep is positively correlated with performance improvement with deck B in young adults.23 It is possible that the cortical activity rather than the sleep quantity could predict young adults’ decision changes.
Limitations
Despite our novel findings on the effects of sleep and aging on decision-making, some potential limitations of this study need to be taken into consideration. First, we instructed participants to keep their regular sleep and avoid any tea, caffeine, or alcohol consumption during the whole experiment period. Indeed, participants reported zero caffeine or alcohol use in their self-report afterwards. Nevertheless, at-home sleep manipulation is less controllable than lab-based sleep studies. Future research could repeat this finding in a laboratory environment. Second, young adults exhibited different circadian rhythms and lifestyles compared to older adults, yet our study required them all to complete the IGT at the same times of the day (ie, 7:30–9:30 am in the morning or 7:30–9:30 pm in the evening). Nevertheless, the significance of the results was not changed when we controlled for participants’ MEQ scores that reflected morningness/eveningness tendencies (Supplementary Table S1 and S5). In order to further eliminate the influence of circadian rhythms, future studies could consider to adopt the “am-pm-am” compared with “pm-am-pm” design7,17 to control the influence of sleep-wake cycle. Third, although older adults’ subjective sleep quality (reflected by PSQI scores) was poorer than that of young adults, objective sleep quality as reflected by the actigraph data did not show any age-related difference. Both groups showed shorter TST than their usual routine. The actigraph-measured short TST may be due to the early time used for the beginning of experiment—7:30 in the morning— which may be different from the habitual wake-up time of participants (especially for young adults). However, participants performed the task more than 30 minutes after getting up, and there was no significant between-session difference in response times for the IGT in sleep groups. Thus, the differences found in the current study might not be attributed to the differences in alertness.
Conclusions
To conclude, as the first study to examine age differences in the sleep-related modulation effect on decision-making, we found that sleep following exposure yielded more optimal decision strategies, reflected as increased feedback sensitivity in both age groups. Of note, this sleep effect was modulated by age such that older adults who had post-test sleep exhibited greater loss aversion, suggesting that, compared with younger counterparts, older adults may need more “sleep on it” time before making decisions in life. Future studies may consider the use of model-based EEG or fMRI to examine the neural mechanisms that potentially underlie the sleep-dependent modulation effect.
Disclosure
Data and MATLAB scripts used in the current study are available from the corresponding authors on reasonable request. This work was supported by the National Natural Science Foundation of China (31971007, 71942004, and 6191101096), the Ministry of Education of Humanities and Social Science project (17YJA190015), and the CAS Key Laboratory of Mental Health, Institute of Psychology (KLMH2019K02). The authors report no conflicts of interest for this work.
References
1. Goldstein AN, Walker MP. The role of sleep in emotional brain function. Annu Rev Clin Psychol. 2014;10:679–708. doi:10.1146/annurev-clinpsy-032813-153716
2. Leproult R, Van Cauter E. Role of sleep and sleep loss in hormonal release and metabolism. Endocr Dev. 2010;17:11–21. doi:10.1159/000262524
3. Skeldon AC, Derks G, Dijk DJ. Modelling changes in sleep timing and duration across the lifespan: changes in circadian rhythmicity or sleep homeostasis? Sleep Med Rev. 2016;28:96–107. doi:10.1016/j.smrv.2015.05.011
4. Yaffe K, Falvey CM, Hoang T. Connections between sleep and cognition in older adults. Lancet Neurology. 2014;13(10):1017–1028. doi:10.1016/S1474-4422(14)70172-3
5. Pace-Schott EF, Spencer RM. Age-related changes in the cognitive function of sleep. Prog Brain Res. 2011;191:75–89. doi:10.1016/B978-0-444-53752-2.00012-6
6. Pace-Schott EF, Spencer RM. Sleep-dependent memory consolidation in healthy aging and mild cognitive impairment. Curr Top Behav Neurosci. 2015;25:307–330. doi:10.1007/7854_2014_300
7. Spencer RM, Gouw AM, Ivry RB. Age-related decline of sleep-dependent consolidation. Learn Mem. 2007;14(7):480–484. doi:10.1101/lm.569407
8. Gui W-J, Li H-J, Guo Y-H, Peng P, Lei X, Yu J. Age-related differences in sleep-based memory consolidation: a meta-analysis. Neuropsychologia. 2017;97:46–55. doi:10.1016/j.neuropsychologia.2017.02.001
9. Wilckens KA, Woo SG, Kirk AR, Erickson KI, Wheeler ME. Role of sleep continuity and total sleep time in executive function across the adult lifespan. Psychol Aging. 2014;29(3):658–665. doi:10.1037/a0037234
10. Bechara A, Tranel D, Damasio H. Characterization of the decision-making deficit of patients with ventromedial prefrontal cortex lesions. Brain. 2000;123(Pt 11):2189–2202. doi:10.1093/brain/123.11.2189
11. Mander BA, Santhanam S, Saletin JM, Walker MP. Wake deterioration and sleep restoration of human learning. Curr Biol. 2011;21(5):R183–R184. doi:10.1016/j.cub.2011.01.019
12. Djonlagic I, Rosenfeld A, Shohamy D, Myers C, Gluck M, Stickgold R. Sleep enhances category learning. Learn Mem. 2009;16(12):751–755. doi:10.1101/lm.1634509
13. Killgore WD, Balkin TJ, Wesensten NJ. Impaired decision making following 49 h of sleep deprivation. J Sleep Res. 2006;15(1):7–13. doi:10.1111/j.1365-2869.2006.00487.x
14. Killgore WDS, Grugle NL, Balkin TJ. Gambling when sleep deprived: don’t bet on stimulants. Chronobiol Int. 2012;29(1):43–54. doi:10.3109/07420528.2011.635230
15. Delazer M, Hogl B, Zamarian L, et al. Decision making and executive functions in REM sleep behavior disorder. Sleep. 2012;35(5):667–673. doi:10.5665/sleep.1828
16. Bayard S, Langenier MC, Dauvilliers Y. Decision-making, reward-seeking behaviors and dopamine agonist therapy in restless legs syndrome. Sleep. 2013;36(10):1501–1507. doi:10.5665/sleep.3044
17. Pace-Schott EF, Nave G, Morgan A, Spencer RM. Sleep-dependent modulation of affectively guided decision-making. J Sleep Res. 2012;21(1):30–39. doi:10.1111/j.1365-2869.2011.00921.x
18. Wood S, Busemeyer J, Koling A, Cox CR, Davis H. Older adults as adaptive decision makers: evidence from the Iowa Gambling Task. Psychol Aging. 2005;20(2):220–225. doi:10.1037/0882-7974.20.2.220
19. Lamar M, Resnick SM. Aging and prefrontal functions: dissociating orbitofrontal and dorsolateral abilities. Neurobiol Aging. 2004;25(4):553–558. doi:10.1016/j.neurobiolaging.2003.06.005
20. MacPherson SE, Phillips LH, Della Sala S. Age, executive function and social decision making: a dorsolateral prefrontal theory of cognitive aging. Psychol Aging. 2002;17(4):598–609. doi:10.1037/0882-7974.17.4.598
21. Ligneul R. Sequential exploration in the Iowa gambling task: validation of a new computational model in a large dataset of young and old healthy participants. PLoS Comput Biol. 2019;15(6):e1006989. doi:10.1371/journal.pcbi.1006989
22. Seeley CJ, Beninger RJ, Smith CT. Post learning sleep improves cognitive-emotional decision-making: evidence for a ‘deck B sleep effect’ in the Iowa Gambling Task. PLoS One. 2014;9(11):e112056. doi:10.1371/journal.pone.0112056
23. Seeley CJ, Smith CT, MacDonald KJ, Beninger RJ. Ventromedial prefrontal theta activity during rapid eye movement sleep is associated with improved decision-making on the Iowa Gambling Task. Behav Neurosci. 2016;130(3):271–280. doi:10.1037/bne0000123
24. Abe T, Inoue Y, Komada Y, Hori T. Effect of post-learning sleep versus wakefulness on advantageous decision-making: a preliminary study. Sleep Biol Rhythms. 2012;10(1):72–74. doi:10.1111/j.1479-8425.2011.00509.x
25. Ahn WY, Dai J, Vassileva J, Busemeyer JR, Stout JC. Computational modeling for addiction medicine: from cognitive models to clinical applications. Prog Brain Res. 2016;224:53–65. doi:10.1016/bs.pbr.2015.07.032
26. Steingroever H, Wetzels R, Wagenmakers E-J. Bayes factors for reinforcement-learning models of the Iowa Gambling Task. Decision. 2016;3(2):115–131. doi:10.1037/dec0000040
27. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
28. Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. 1994;50(1–3):7–15. doi:10.1016/0010-0277(94)90018-3
29. Bechara A, Dolan S, Denburg N, Hindes A, Anderson SW, Nathan PE. Decision-making deficits, linked to a dysfunctional ventromedial prefrontal cortex, revealed in alcohol and stimulant abusers. Neuropsychologia. 2001;39(4):376–389. doi:10.1016/s0028-3932(00)00136-6
30. Steingroever H, Wetzels R, Horstmann A, Neumann J, Wagenmakers EJ. Performance of healthy participants on the Iowa Gambling Task. Psychol Assess. 2013;25(1):180–193. doi:10.1037/a0029929
31. Li X, Lu ZL, D’Argembeau A, Ng M, Bechara A. The Iowa Gambling Task in fMRI images. Hum Brain Mapp. 2010;31(3):410–423. doi:10.1002/hbm.20875
32. Ahn W-Y, Vasilev G, Lee S-H, et al. Decision-making in stimulant and opiate addicts in protracted abstinence: evidence from computational modeling with pure users. Front Psychol. 2014;5:849. doi:10.3389/fpsyg.2014.00849
33. Ahn W-Y, Busemeyer JR, Wagenmakers E-J, Stout JC. Comparison of decision learning models using the generalization criterion method. Cognitive Science: A Multidisciplinary Journal. 2008;32(8):1376–1402. doi:10.1080/03640210802352992
34. Worthy DA, Maddox WT. A comparison model of reinforcement-learning and win-stay-lose-shift decision-making processes: a tribute to W.K. Estes. J Math Psychol. 2014;59:41–49. doi:10.1016/j.jmp.2013.10.001
35. Luce RD. Individual Choice Behavior. Oxford, England: John Wiley; 1959.
36. Ahn W-Y, Haines N, Zhang L. Revealing neurocomputational mechanisms of reinforcement learning and decision-making with the hBayesDM package. Computational Psychiatry. 2017;1:24–57. doi:10.1162/CPSY_a_00002
37. Watanabe S. Asymptotic equivalence of Bayes cross validation and widely applicable information criterion in singular learning theory. J Machine Learn Res. 2010;11:
38. Gelman A, Hwang J, Vehtari A. Understanding predictive information criteria for Bayesian models. Stat Comput. 2014;24(6):997–1016. doi:10.1007/s11222-013-9416-2
39. Aylward J, Valton V, Ahn W-Y, et al. Altered learning under uncertainty in unmedicated mood and anxiety disorders. Nature Human Behaviour. 2019;3(10):1116–1123. doi:10.1038/s41562-019-0628-0
40. Carlisi CO, Norman L, Murphy CM, et al. Shared and disorder-specific neurocomputational mechanisms of decision-making in autism spectrum disorder and obsessive-compulsive disorder. Cereb Cortex. 2017;27(12):5804–5816. doi:10.1093/cercor/bhx265
41. Tononi G, Cirelli C. Sleep function and synaptic homeostasis. Sleep Med Rev. 2006;10(1):49–62. doi:10.1016/j.smrv.2005.05.002
42. Tononi G, Cirelli C. Sleep and synaptic down-selection. Eur J Neurosci. 2020;51(1):413–421. doi:10.1111/ejn.14335
43. Honn KA, Hinson JM, Whitney P, Van Dongen HPA. Cognitive flexibility: a distinct element of performance impairment due to sleep deprivation. Accident Analysis Prevent. 2019;126:191–197. doi:10.1016/j.aap.2018.02.013
44. Whitney P, Hinson JM, Jackson ML, Van Dongen HPA. Feedback blunting: total sleep deprivation impairs decision making that requires updating based on feedback. Sleep. 2015;38(5):745–754. doi:10.5665/sleep.4668
45. Murphy NA, Isaacowitz DM. Preferences for emotional information in older and younger adults: a meta-analysis of memory and attention tasks. Psychology and Aging. 2008;23(2):263–286. doi:10.1037/0882-7974.23.2.263
46. Carstensen LL. The influence of a sense of time on human development. Science. 2006;312(5782):1913–1915. doi:10.1126/science.1127488
47. Sharot T, Garrett N. Forming beliefs: why valence matters. Trends Cogn Sci. 2016;20(1):25–33. doi:10.1016/j.tics.2015.11.002
48. Samanez-Larkin GR, Gibbs SEB, Khanna K, Nielsen L, Carstensen LL, Knutson B. Anticipation of monetary gain but not loss in healthy older adults. Nat Neurosci. 2007;10(6):787–791. doi:10.1038/nn1894
49. Sojitra RB, Lerner I, Petok JR, Gluck MA. Age affects reinforcement learning through dopamine-based learning imbalance and high decision noise—not through Parkinsonian mechanisms. Neurobiol Aging. 2018;68:102–113. doi:10.1016/j.neurobiolaging.2018.04.006
50. Lerner I, Sojitra R, Gluck M. How age affects reinforcement learning. Aging. 2018;10(12):3630–3631. doi:10.18632/aging.101649
51. Damasio A, Descartes RJNYA. Error: Emotion, Reason, and the Human Brain. 1994:350–412.
52. Bechara A, Damasio H, Tranel D, Damasio AR. The Iowa Gambling Task and the somatic marker hypothesis: some questions and answers. Trends Cogn Sci. 2005;9(4):159–162. doi:10.1016/j.tics.2005.02.002
53. Tomb I, Hauser M, Deldin P, Caramazza A. Do somatic markers mediate decisions on the gambling task? Nat Neurosci. 2002;5(11):1103–1104. doi:10.1038/nn1102-1103
54. Chiu Y-C, Lin C-H, Huang J-T, Lin S, Lee P-L, Hsieh J-C. Immediate gain is long-term loss: are there foresighted decision makers in the Iowa Gambling Task? Behavioral and Brain Functions. 2008;4(1):13. doi:10.1186/1744-9081-4-13
55. Creery JD, Oudiette D, Antony JW, Paller KA. Targeted memory reactivation during sleep depends on prior learning. Sleep. 2015;38(5):755–763. doi:10.5665/sleep.4670
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.