Back to Journals » Nature and Science of Sleep » Volume 14
Daytime Sleep Behaviors and Cognitive Performance in Middle- to Older-Aged Adults Living with and without HIV Infection
Authors Li P ![]() , Gao L
, Gao L ![]() , Gao C, Parker RA, Katz IT, Montano MA, Hu K
, Gao C, Parker RA, Katz IT, Montano MA, Hu K ![]()
Received 27 September 2021
Accepted for publication 20 January 2022
Published 9 February 2022 Volume 2022:14 Pages 181—191
DOI https://doi.org/10.2147/NSS.S339230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Peng Li,1,2 Lei Gao,1– 3 Chenlu Gao,1,2 Robert A Parker,4– 6 Ingrid T Katz,5,7,8 Monty A Montano,5,9 Kun Hu1,2
1Medical Biodynamics Program, Division of Sleep and Circadian Disorders, Departments of Medicine and Neurology, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA; 2Division of Sleep Medicine, Harvard Medical School, Boston, MA, USA; 3Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA; 4Biostatistics Center, Massachusetts General Hospital, Boston, MA, USA; 5Harvard Medical School, Boston, MA, USA; 6Center for AIDS Research, Harvard University, Boston, MA, USA; 7Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA; 8Harvard Global Health Institute, Cambridge, MA, USA; 9Boston Claude D. Pepper Older Americans Independence Center, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA
Correspondence: Peng Li, Email [email protected]
Purpose: We investigated whether daytime sleep behaviors (DSBs) such as frequent daytime sleepiness or napping are associated with worse cognitive performance, and whether HIV infection moderates this relationship.
Methods: Among 502,507 participants in the UK Biobank study, we identified 562 people living with HIV infection (PLWH; Mage= 50.51± 7.81; 25.09% female; 78.83% white) and extracted 562 uninfected controls who matched on age, sex, ethnic background, social-economic status, and comorbidities. DSB burden was assessed based on answers to two questions on DSBs. Participants who answered “sometimes” or “often/usually” to one of them were considered to have poor DSB burden, or otherwise were considered not having any. A composite cognition score was computed by averaging the available standardized individual test results from four neurocognitive tests: ie, a reaction time test for information processing speed, a pairs matching test for visual episodic memory, a fluid intelligence test for reasoning, and a prospective memory test. Mixed-effects models with adjustment for the variables used in extracting matched uninfected controls were performed to test the hypotheses.
Results: Having poor DSB burden was associated with a 0.15 – standard deviation (SD) decrease in cognitive performance (p = 0.006). People living with HIV infection (PLWH) also performed worse on the cognitive tasks than uninfected controls, with an effect size similar to that of having poor DSB burden (p = 0.003). HIV infection significantly modified the negative association between DSB burden and cognition (p for interaction: 0.008). Specifically, the association between DSB burden and cognition was not statistically significant in uninfected controls, whereas PLWH who reported having poor DSB burden had a 0.28 – SD decrease in cognitive performance compared to PLWH who did not.
Conclusion: HIV infection significantly increased the adverse association between DSBs and cognitive performance. Further studies are needed to investigate the potential mechanisms that underlie this interaction effect and whether poor DSBs and worse cognitive performance are causally linked.
Keywords: aging, cognition, daytime napping, daytime sleepiness, risk factors, sleep
Plain Language Summary
People living with HIV infection (PLWH) commonly experience daytime somnolence that may adversely synergize to increase comorbidity burden, reduce the quality of life, and reduce adherence to complex medical regimens. PLWH also frequently report cognitive complications such as cognitive decline. We studied whether daytime sleep behaviors, ie, daytime sleepiness or napping, are related to cognitive performance and whether the association is more profound in PLWH. From the UK Biobank cohort, we identified 562 PLWH and extracted 562 demographically similar uninfected people. They reported daytime sleepiness and napping frequencies and completed four cognitive tests. Firstly, among all 1124 participants, those with frequent daytime sleepiness or napping behaviors had worse cognitive functions than those without. Secondly, PLWH had worse cognitive functions than their uninfected counterparts. And thirdly, the association between frequent daytime sleepiness/napping behaviors and worse cognitive performance was much stronger in PLWH than in uninfected people. These results highlight the importance of sleep health in the context of HIV infection and imply complex mechanisms among HIV infection, daytime sleepiness/napping, and cognition, which need to be investigated further. Practitioners may use frequent daytime sleepiness/napping as an early phase signal for potential cognitive complications in PLWH. The current study also helps in identifying potential targets in terms of optimizing daytime sleep for cognitive benefits should a causal link be confirmed in future studies.
Introduction
The advent of effective antiretroviral therapy (ART) has substantially increased the life expectancy of people living with HIV infection (PLWH). As PLWH age, cognitive impairment becomes an increasing clinical concern. Up to 50% of older (ie, aged > 60 years) PLWH experience cognitive impairment,1,2 compromising adherence to complex medical regimens, successful independent living,3,4 and overall quality of life.5,6 It is thereore a critical need to identify mid- to late-life (ie, aged 40–69 years) risk factors predisposing PLWH to cognitive impairment.7
Sleep disturbance is highly prevalent in PLWH, affecting up to 70% of this population.8 Epidemiological studies have demonstrated higher prevalence of insomnia and obstructive sleep apnea syndrome in PLWH than in the general population.8 Prior evidence has also related sleep disturbance to cognitive impairment or dementia in populations such as older adults,9–13 as well as in PLWH.14 Daytime sleepiness and daytime napping, important aspects of the 24-hour sleep-wake cycle, are common in the general older population and particularly in aging PLWH.15 Excessive daytime sleepiness and napping can be a direct consequence of nighttime sleep disturbances, as well as factors separate from nighttime sleep, such as underlying disease processes and mood disorders.16,17 While a link between excessive daytime sleepiness or daytime napping and adverse health consequences including cognitive outcomes in the general population has been reported,16,18–21 such associations in aging PLWH have not been directly addressed.
We aimed to investigate: (1) whether poor daytime sleep behavior (DSB) burden (ie, more frequent daytime sleepiness or napping) is associated with worse cognitive performance in both PLWH and uninfected people, (2) whether PLWH have worse cognitive performance than uninfected people, and (3) whether HIV infection exacerbates the association between DSBs and cognition.
Materials and Methods
Study Design and Participants
This case-control study was based on individual-level data from the UK Biobank cohort.22 More than 500,000 middle- to older-aged participants (ie, aged 40–69 years) were recruited between 2006 and 2010 from 22 assessment centers across the United Kingdom. PLWH were identified at study baseline based on (1) HIV-1 antigen test (if seropositive; the tests cover 9,690 participants), (2) the International Classification of Disease version 10 (ICD-10; if with codes: B20-B24, F02.4, O98.7, R75, Z11.4, Z20.6, Z21, Z71.7, Z83.0, or with the keyword “HIV”; ICD records cover 437,506 participants), or (3) self-reported non-cancer illness (if with code 1439 or with keyword “HIV” or “AIDS”; this self-reported record covers 386,094 participants). The remaining UK Biobank participants who did not meet the above criteria were considered uninfected people. Participants who had missing data for the exposure variable (see details below), did not complete any cognitive tests (see details below), or were diagnosed with dementia were excluded.
At baseline, 502,507 participants were assessed in the UK Biobank. Among them, 2,386 had missing data for the exposure variable, or did not complete any one of the four cognitive tests. They were excluded. Afterwards, 226 participants with dementia were further excluded. In the remaining 499,895 participants, 18 were HIV seropositive; 313 had the ICD-10 codes related to HIV infection; and 465 self-reported themselves infected with HIV. After considering overlapped cases, the total number of unique PLWH participants was 567. Five of them were further excluded because of missing data in the variables used for propensity score (PS) matching (see details in “Extraction of matched uninfected people”), resulting in 562 PLWH included in the following analysis. From the remaining participants without identified infection, 562 matched uninfected people were extracted. Table 1 summarizes the covariates used in the PS model, as well as the exposure, and the outcome variables between the two groups. Supplemental Table 1 summarizes the additional three covariates, ie, education level, smoking behavior, and alcohol consumption behavior between the two groups.
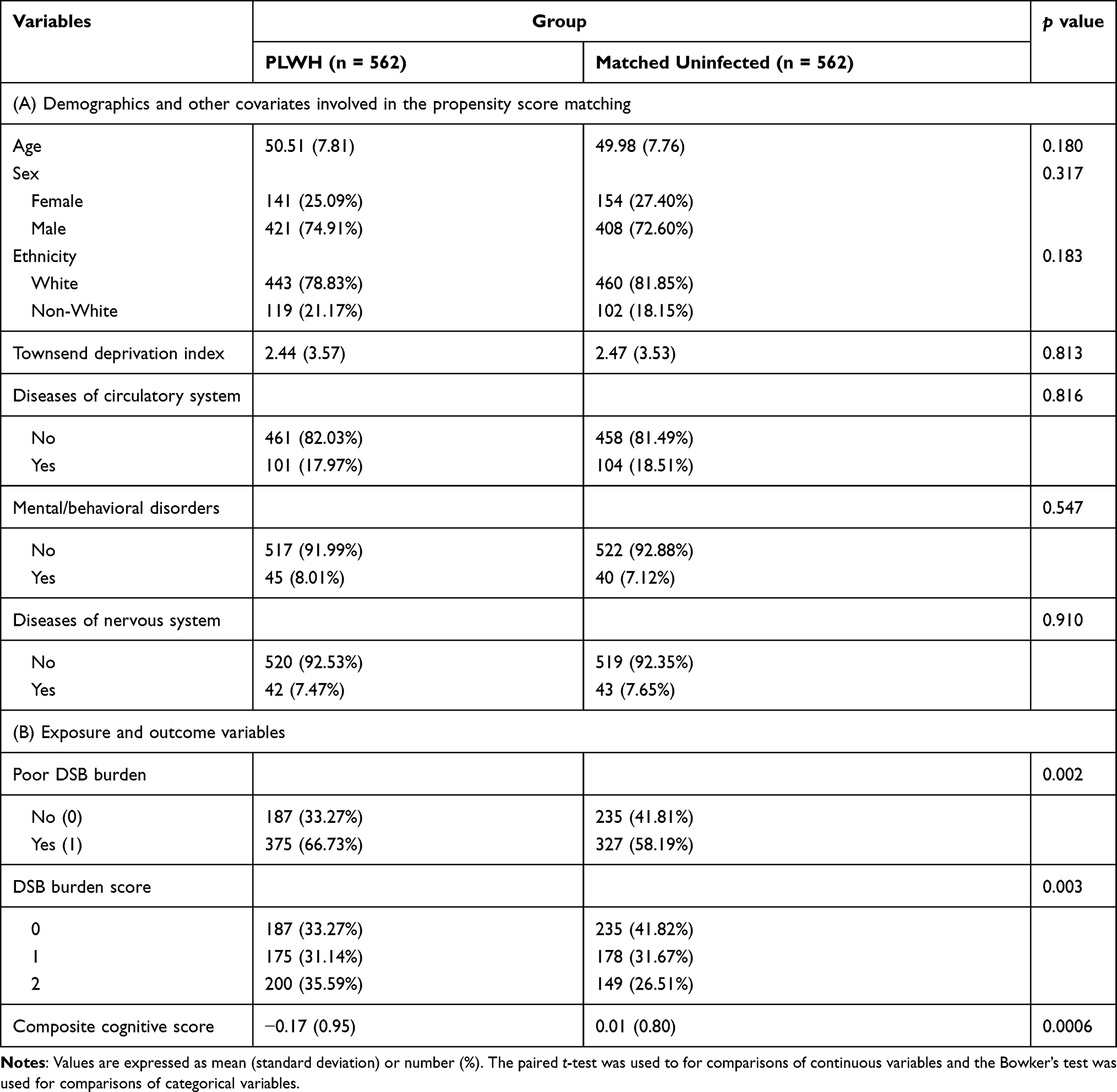 |
Table 1 Demographics and Other Covariates Involved in the Propensity Score Matching, and Exposure and Outcome Variables for PLWH and Matched Uninfected People |
Ethical approval for the UK Biobank study was received from the Northwest Multi-Center Research Ethics Committee. All participants provided written informed consent through electronic signature at study baseline. Data were collected and deidentified by the UK Biobank staff; they were transferred to and analyzed at the Brigham and Women’s Hospital. The Mass General Brigham institutional review board approved this specific study protocol with a final decision of not human subject study.
Extraction of Matched Uninfected People
To extract matched uninfected people, a PS model predicting PLWH based on age, sex, ethnicity, social-economic status, and comorbidities (ie, mental behavioral disorders, diseases of the nervous system, and diseases of the circulatory system) was developed. For each PLWH, an uninfected person was extracted based on the nearest neighbor of PS without replacement.
Ethnicity was dichotomized as white (those who reported “British”, “Irish”, or “any other white background”) or non-white. Social-economic status was based on Townsend deprivation index (TDI)23 at recruitment. The ICD-10 records were parsed to identify diseases of circulatory system (code I00-I99), mental/behavioral disorders (code F00-F99), and diseases of nervous system (code G00-G99). More detailed information regarding the ICD-10 codes and specific diseases within each of the categories can be found in Supplemental Methods. The three conditions were dichotomized as yes or no depending on whether any of these corresponding codes appeared in participants’ ICD-10 records prior to their dates of assessment. Participants who had missing data in any one of these variables were excluded prior to performing the analysis.
Assessment of Cognitive Function
Results from four cognitive tests that covered a majority of the UK Biobank participants24 were used in the current study, namely reaction time (RT) test, pairs matching test (PT), fluid intelligence (FI) test, and prospective memory (PM) test. They were administered at baseline through computerized touchscreen test batteries that were designed specifically for the UK Biobank to allow population-scale testing without examiner supervision.9,24,25
Reaction Time (RT) Test
This test was delivered as a timed test of symbol matching. It requested participants to respond with a button press when they identified the appearance of matching symbols in one pair of cards out of 12 pairs. The test score was the mean response time in milliseconds across four trials. Results under 50 ms (which was considered to be due to anticipation rather than reaction) or over 2,000 ms (since the cards would have already disappeared by then) were excluded when computing the average response time. The RT test is a simple measure of information processing speed.
Pairs Matching Test (PT)
During this test, participants were shown six pairs of cards for five seconds. Cards were then turned over, and participants were asked, from recall, to locate the position of as many matching pairs of cards as possible. The test score was the number of errors that each participant made. The PT assesses the visual episodic memory.
Fluid Intelligence (FI) Test
Participants were presented with 13 logic/reasoning questions with multiple response options during this test. They had to answer as many as they could within two minutes. The score of this test was the total number of correct answers, ranging between 0 and 13, that represents a measure of verbal-numerical reasoning.
Prospective Memory (PM) Test
Participants were asked to engage in a specific behavior after the assessment. Specifically, they were presented with the instruction:
At the end of the games we will show you four colored symbols and ask you to touch the blue square. However, to test your memory, we want you to actually touch the orange circle instead.
The test result was either correct (1) or incorrect (0) depending on whether the participant touched the orange circle on the first attempt or not. PM refers to the ability to carry out future intentions at a specific time or in response to a specific event.
Individual test scores were z-score transformed based on the corresponding mean and standard deviation (SD) of all UK Biobank participants at baseline. The signs of the z-scores for RT and PT were reversed, so that a higher z score for each cognitive task represents better performance. A composite measure for cognitive performance was then constructed by averaging the available z-scores for each participant.26 Therefore, for this score, zero represents the mean and 1 represents 1 SD above the mean of the baseline score of all UK Biobank participants. A negative z-score means that someone has an overall score that is lower than the average of the entire cohort at baseline (ie, worse cognitive performance).
Assessment of Daytime Sleep Behavior Burden
Daytime sleepiness was ascertained through self-report using the questions “How likely are you to doze off or fall asleep during the daytime when you don’t mean to?” with responses “never/rarely”, “sometimes”, “often”, and “all of the time”. To assess daytime napping, participants were asked “Do you have a nap during the day?” with responses “never/rarely”, “sometimes”, and “usually”. We examined DSB burden using two approaches. First, a composite dichotomized measure for DSB burden was constructed by re-coding the answers for the two questions: “Not having poor DSB burden (0)” if participants answered “never/rarely” for both questions, and “Having DSB burden (1)” if otherwise.27,28 It was considered missing when participants did not answer (or prefer not to answer) both questions, or answered one of them whereas answered “never/rarely” for the other question. Additionally, we further divided those who have DSB burden (ie, being scored “1” using the above dichotomized coding approach) into two groups. Specifically, participants who answered “sometimes” for both questions, or answered “often/usually” for at least one of them were scored “2”, otherwise they kept the score “1”. This alternative code approach thus resulted in an ordinal DSB burden score ranging from 0 to 2.
Statistical Analysis
Characteristics of covariates, the exposure variable, ie, DSB burden (0/1) or DSB burden score (0/1/2), and the composite measure for cognitive performance were summarized between PLWH and matched uninfected as percentage for categorical variables and mean ± SD for continuous variables. To examine the differences in these variables between PLWH and matched uninfected, paired t-test was carried out for continuous variables and Bowker’s test was carried out for categorical variables.
To examine whether poor DSB burden is associated with worse cognitive performance in both PLWH and uninfected people (hypothesis 1), a mixed-effect model was performed with the composite measure for cognitive performance as an outcome, DSB burden as a fixed-effect predictor, and the matched flag as a random-effect predictor. To examine whether PLWH have worse cognitive performance than uninfected people (hypothesis 2), a mixed-effect model was performed with the composite measure for cognitive performance as an outcome, group (ie, PLWH or uninfected) as a fixed-effect predictor, and the matched flag as a random-effect predictor. To test whether HIV infection exacerbates this association (hypothesis 3), we augmented the mixed model for hypothesis 1 by including group and an interaction item between group and DSB burden as additional predictors. All models were adjusted for the variables used in the PS matching. Additionally, we also accounted for education level, smoking behavior, and alcohol consumption behavior by adjusting for these variables in the models. Methods to derive these additional covariates are provided in Supplemental Methods. As secondary analysis, we examined domain-specific associations by replacing the outcome variable, the composite cognitive score, with the score from each domain of cognitive performance (ie, RT, PT, FI, and PM). Note that since the PM test resulted in either “yes (1)” or “no (0)”, the link function of the corresponding mixed-effect model was changed to logit function and the distribution was changed to binominal (ie, a logistic regression model). Statistical significance was accepted at alpha level of 0.05 (two-sided). The retrieval of data from the UK Biobank and the PS matching was performed using MATLAB (version R2020a, the MathWorks Inc., Natick, MA, USA). Other statistical analyses were performed using JMP Pro (version 15.1.0, SAS Institute, Cary, NC, USA).
Results
Having poor DSB burden was associated with worse cognitive performance in PLWH and matched uninfected. Specifically, the composite score of cognitive performance was −0.15 (−0.25, −0.04) [estimate (95% CI) unless otherwise indicated] in those who had DSB burden compared with those who did not (p = 0.006; Table 2, Hypothesis 1). Using the alternative coding approach (ie, three levels varying from 0 to 2) for DSB burden, we found that the decrease in the composite cognitive score occurred mainly in the participants whose DSB burden was scored 2 [compared with 0: estimate = −0.22 (-0.35, -0.10), p = 0.0004], then in participants whose DSB burden was scored 1 [estimate = −0.08 (−0.20, 0.04), p = 0.2; Table 3, Hypothesis 1]. A DSB burden of 2 was also significantly worse than a burden of 1 [estimate = −0.14 (−0.28, 0.00), p = 0.03; based on post-hoc test on results shown in Table 3, Hypothesis 1].
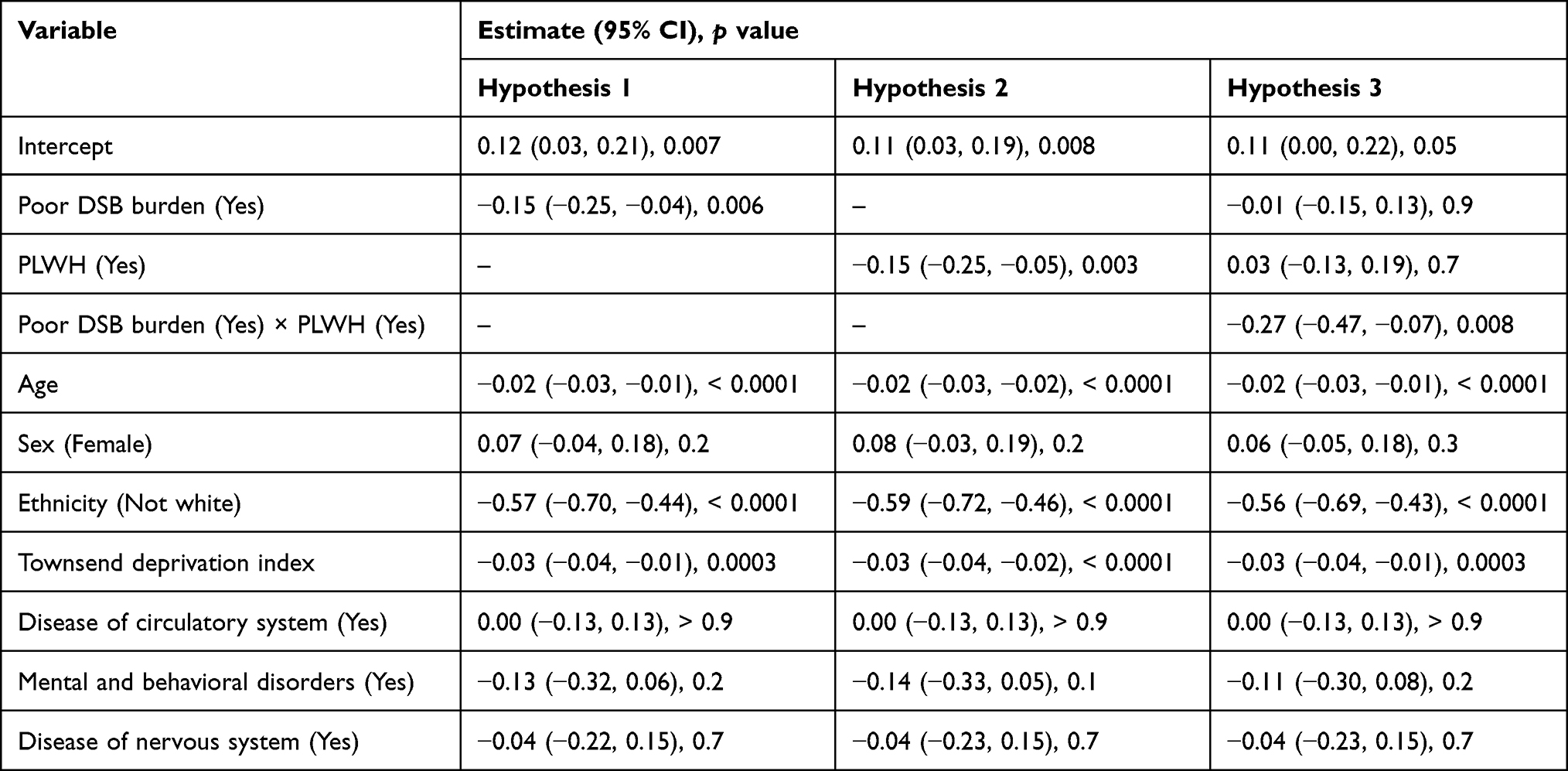 |
Table 2 Poor DSB Burden (Yes/No) and Cognitive Performance in PLWH and Matched Uninfected People |
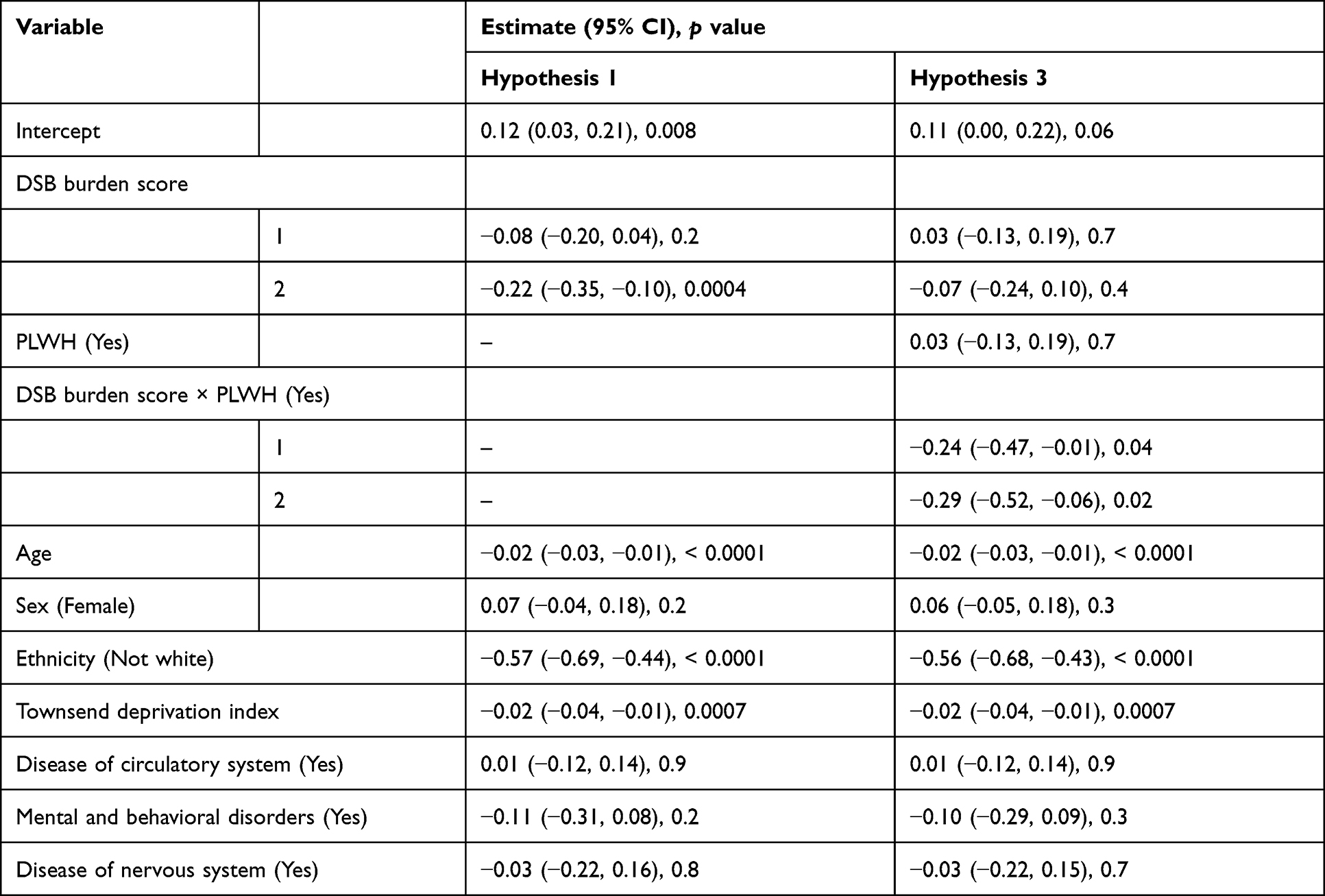 |
Table 3 DSB Burden Score (2/1/0) and Cognitive Performance in PLWH and Matched Uninfected People |
PLWH showed lower cognitive performance than uninfected controls. Specifically, PLWH had a score of −0.15 (−0.25, −0.05) in the composite score for cognition compared with uninfected controls (p = 0.003; Table 2, Hypothesis 2).
The cognitive performance in people who had poor DSB burden was even worse in PLWH. Specifically, in PLWH who had poor DSB burden, the difference was −0.28 (−0.45, −0.11) compared to PLWH without a DSB burden whereas it was only −0.01 (−0.15, 0.13) in uninfected people who had poor DSB burden (p for interaction = 0.008; Table 2, Hypothesis 3; Figure 1A). Using the alternative coding approach, the additional reduction was also observed in PLWH whose DSB burden was scored 1 [compared with uninfected: estimate = −0.24 (−0.47, −0.01), p = 0.04] or 2 [compared with uninfected: estimate = −0.29 (−0.52, −0.06), p = 0.02; Figure 1B].
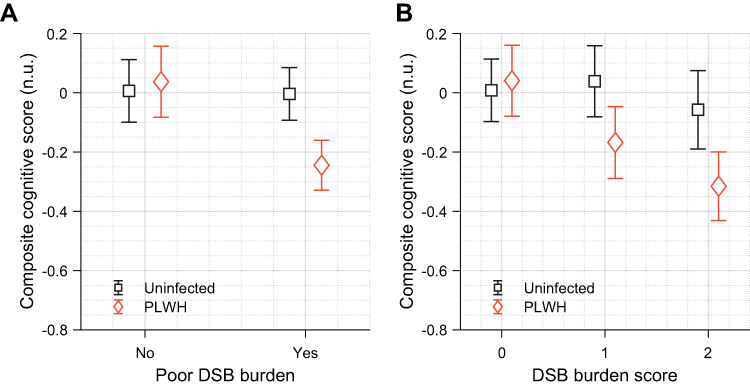 |
Figure 1 HIV infection interacts with poor DSB burden to worsen cognition. Shown are predicted mean values (uninfected: square; PLWH: diamond) and 95% confidence intervals. DSB burden is coded as (A) a dichotomized variable with “Yes” meaning having poor DSB burden and “No” meaning having no poor DSB burden, and (B) a higher score means higher DSB burden. |
All observations above were consistent after we further adjusted for education level, smoking behavior, and alcohol consumption behavior. Detailed results are summarized in Supplemental Tables 2 and 3.
In secondary analyses, we found that having poor DSB burden was significantly associated with increased RT [estimate = 0.05 (0.02, 0.07) (unit, log ms), p = 0.0002] and lower FI score [estimate = −0.50 (−0.96, −0.03), p = 0.04]. The worsened cognitive performance in PLWH is mainly driven by increased RT [estimate = 0.04 (0.01, 0.06), p = 0.002] and potentially also by increased number of incorrect matches in PT [estimate = 0.08 (−0.01, 0.16) (unit: log number)], although not statistically significant (p = 0.07). HIV infection did not interact with DSB burden to affect any individual cognitive test results (all p’s for interaction > 0.1).
Discussion
The current study showed that people who reported poor DSB burden (ie, having “sometimes or frequent daytime napping or sleepiness”) had worse cognitive performance than those who did not. This association was also dose specific as suggested by the monotonic decline in cognitive performance with the increase of DSB burden score. While looking into different cognitive tests, this association was found to be statistically significant for RT and FI. Besides, this study also showed that PLWH had worse cognitive performance than uninfected people, and this association appeared to be mainly driven by RT, and potentially, PT as well. Intriguingly, the association between DSB burden and cognition was considerably stronger in PLWH when compared to uninfected people.
Cognitive impairment is a critical emerging issue in older persons and in the clinical management of aging PLWH.7 Prior studies showed both subcortical and cortical involvements in the clinical neuropsychological presentation of HIV-associated cognitive impairment;4 learning and executive function were found to be the most affected domain in the post ART era.7,29 As a higher level cognitive construct, executive function is associated with a wide range of measurable cognitive functions, including RT, an index of information processing speed.30,31 The current findings that HIV infection adversely affects cognition specially in terms of RT performance expands on observations in previous studies using smaller sample sizes.32,33
However, information processing speed can represent a cognitive construct separate from executive functions. A previous study employing samples from the United States with pre-ART era and post-ART era data reported that slow information processing speed was more commonly found in the PLWH pre-ART rather than post-ART era.29 While lacking information of ART administration in the UK Biobank, it remains unclear whether the observed performance decline in RT was due to a lumped effect of early treatment and infection history (eg, a legacy effect of potential central nervous system damage due to HIV sustained before the administration of ART). Given that therapies for HIV management have continued to evolve in the past decade, further studies are needed to determine whether advancement in treatment attenuates the observed exacerbated association between poor DSB burden and cognition in PLWH.
While the information processing speed is among the seven abilities outlined in the current nosology of HIV-associated neurocognitive disorders,34 the current findings also suggest episodic memory (as assessed by the PT) be potentially added to the repository of potential neurocognitive functions adversely affected by HIV infection. Although episodic memory partially contributes to the integrity of executive functions, there are different neuroanatomical correlates.35 Newly identified evidence may help refine the current criteria for screening HIV-associated neurocognitive impairment, improving particularly the domain specificity that is lacking.36
It is reported that over 55% of PLWH experience daytime sleepiness/drowsiness.15 In this current study, the prevalence of having poor DSB burden was over 60% in PLWH, which is substantially greater than that in uninfected people. Such increase may be a direct effect of disturbance in nocturnal sleep or sleep disorders that is common in PLWH (ie, the prevalence was reported to be >50% in PLWH versus <30% in the general population).37 Prior mechanistic studies have also been conducted. For example, cytokine activity secondary to immune response of HIV infection38 that is involved in induction of non-rapid eye movement sleep may influence nighttime sleep patterns.39 Chronic inflammation in PLWH is another hypothesized mediator of sleep disturbance in PLWH,14 potentially influencing biochemical regulation of sleep patterns.40 As a result, those biological mechanisms may lead to daytime sleepiness and fatigue indirectly through disturbed nocturnal sleep.40 Future studies evaluating the potential role of inflammatory factors and aging in outcomes from this study population are warranted.
The current study replicated and expanded upon previous observations in smaller-scale data that excessive daytime sleepiness and daytime napping were linked to poorer cognitive performance;16,18–21 it also documented this association in PLWH, and perhaps most importantly, suggested that HIV infection adversely moderated this association. While exact mechanisms linking daytime napping and cognitive performance remain unclear, prior studies in the general population have examined several potential pathways. For example, excessive daytime sleepiness and prolonged daytime napping can be secondary to nighttime sleep disturbance or sleep disorders that lead to cognitive impairment; they may also be sequelae to underlying pathophysiological processes (eg, chronic inflammation) that cause cognitive impairments. Notably, direct contributions of these daytime sleep behaviors have also been reported.16,18–21 To test whether nighttime sleep disturbances also interact with HIV infection to influence cognitive performance or whether they mediate the observed association between DSBs and cognition in PLWH, nighttime sleep assessment through, for example, polysomnography, is needed, which is a costly measurement and not feasible for large-scale cohort studies. Luckily, the UK Biobank monitored the rest-activity patterns of around 1/5 of all participants (including around 100 PLWH) using actigraphy that provides a proxy for studying sleep,41 for example, sleep fragmentation,42 which can potentially be studied in the future.
It is worth noting that there is a greater proportion of men living with HIV in our studied cohort. This is consistent with the sex ratio in the UK back to 10 years ago when this cohort was established43 and even now.44 The sex ratio is in keeping with prior PLWH cohorts (for example, The Antiretroviral Therapy Cohort Collaboration conducted a collaborative analysis of 13 HIV cohorts to study prognosis of ART and cause of death, and among total 39,272 participants from the 13 cohorts, male participants made up more than 70%).45,46 Gender disparities in virological outcomes including survival likely contribute to this.47,48 For example, there is a growing evidence showing that HIV+ men live longer than HIV+ women (whereas in the general population, women have longer life expectancy).49 In a PLWH cohort of the UK, findings show consistent poorer virological outcomes in women living with HIV even in the modern ART era.47 Risk factors of death including substance use, psychological and mental health conditions, multimorbidity, and polypharmacy that affect men and women differently may also interact with HIV infection, which may partially explain the different survival rates.47,48,50–52
Future studies are required to identify mechanisms underlying the interaction effect of chronic HIV infection and frequent daytime sleepiness/napping in cognitive performance. It is possible that the pathophysiological processes mentioned above—sleep disturbance, inflamm-aging, and increased comorbid burden—as a result of HIV infection synergize with the effect of sleepiness and napping during daytime. Moreover, sleep behaviors usually worsen over time, underscoring a complex relationship with cognitive decline and dementia.53 In the context of aging PLWH, how to optimize sleep is clinically relevant. Separately, excessive sleepiness and napping may cause poor adherence to complex medical regimens related to comorbidities in PLWH and lack of social engagement, and subsequently increase the propensity of cognitive impairment. Independent influences of excessive sleepiness/napping on cognition and direct modifying effects of HIV infection on these influences are also worth further investigation. Studies that target various candidate drivers of cognitive impairment are also encouraged.
A major limitation of this study is that the UK Biobank is not an HIV-focused cohort, limiting the ability to document the exact history of acquired immunodeficiency syndrome and early treatment information. However, the current study leverages large-scale population level data to answer questions relevant to neurocognitive performance in the context of HIV infection with rich hospital records to reduce potential bias. Potential moderating effects through adherence to ART or the treatment itself should be addressed in future studies. Besides, it also needs further attention whether the observed exacerbated effect of HIV infection on the association between poor DSB and worse cognitive performance depends on the duration of the infection. Methodologically, the ICD-10 codes offered a well-structured system to identify uninfected controls that matched PLWH broadly in terms of the three umbrella comorbid conditions. We did not attempt to match for presence of a specific disease. Future studies using quantitative assessment of daytime sleep are encouraged by observations in this study. In addition, future studies should also investigate whether daytime sleep behaviors are associated with prospective longitudinal cognitive decline and whether sleep interventions can help maintain cognitive status in PLWH.
Abbreviations
ART, antiretroviral therapy; CI, confidence interval; DSB, daytime sleep behavior; FI, fluid intelligence; HIV, human immunodeficiency virus; ICD-10, International Classification of Disease version 10; PLWH, people living with HIV; PM, prospective memory; PT, pairs matching test; PS, propensity score; RT, reaction time; SD, standard deviation; TDI, Townsend deprivation index.
Acknowledgments
This research has been conducted using the UK Biobank Resource under Application Number 33883.
Funding
This research was funded in part by a 2021 developmental grant (to P.L.) from the Harvard University Center for AIDS Research (CFAR), an NIH funded program (P30AI060354) which is supported by the following NIH Co-Funding and Participating Institutes and Centers: NIAID, NCI, NICHD, NHLBI, NIDA, NIMH, NIA, NIDDK, NIMHD, NIDCR, NINR, OAR, and FIC, by a Pilot Grant (to P.L.) sponsored by the AIDS and Aging Research Platform (NIH R33AG067069-02), and in part by NIA grants (RF1AG064312 and RF1AG059867; to K.H.). P.L. is also supported by the BrightFocus Foundation Alzheimer’s Disease Research Program (A2020886S). L.G. is also supported by the National Institute on Aging (NIA) grant (R03AG067985). R.A.P. is supported by the CFAR grant (P30AI060354). M.A.M. is supported by the CFAR grant (P30AI060354) and the Pepper Center, an NIA funded program (P30AG031679). K.H. is supported by NIA grants (RF1AG064312 and RF1AG059867).
Disclosure
Dr Peng Li reports grants from Harvard University Center for AIDS Research, grants from HIV and Aging Research Consortium, grants from The BrightFocus Foundation, during the conduct of the study.
Dr Robert A Parker reports grants from NIH, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. McArthur JC, Steiner J, Sacktor N, Nath A. Human immunodeficiency virus-associated neurocognitive disorders: mind the gap. Ann Neurol. 2010;67(6):699–714. doi:10.1002/ana.22053
2. De Francesco D, Underwood J, Post FA, et al. Defining cognitive impairment in people-living-with-HIV: the POPPY study. BMC Infect Dis. 2016;16(1):617. doi:10.1186/s12879-016-1970-8
3. Gorman AA, Foley JM, Ettenhofer ML, Hinkin CH, van Gorp WG. Functional consequences of HIV-associated neuropsychological impairment. Neuropsychol Rev. 2009;19(2):186–203. doi:10.1007/s11065-009-9095-0
4. Guha A, Brier MR, Ortega M, Westerhaus E, Nelson B, Ances BM. Topographies of cortical and subcortical volume loss in HIV and aging in the cART era. J Acquir Immune Defic Syndr. 2016;73(4):374–383. doi:10.1097/QAI.0000000000001111
5. Alford K, Vera JH. Cognitive impairment in people living with HIV in the ART era: a review. Br Med Bull. 2018;127(1):55–68. doi:10.1093/bmb/ldy019
6. Alford K, Banerjee S, Nixon E, et al. Assessment and management of HIV-associated cognitive impairment: experience from a multidisciplinary memory service for people living with HIV. Brain Sci. 2019;9(2):37. doi:10.3390/brainsci9020037
7. Clifford DB, Ances BM. HIV-Associated Neurocognitive Disorder (HAND). Lancet Infect Dis. 2013;13(11):976–986. doi:10.1016/S1473-3099(13)70269-X
8. Taibi DM. Sleep disturbances in persons living with HIV. J Assoc Nurses AIDS Care. 2013;24(1 Suppl):S72–S85. doi:10.1016/j.jana.2012.10.006
9. Kyle SD, Sexton CE, Feige B, et al. Sleep and cognitive performance: cross-sectional associations in the UK Biobank. Sleep Med. 2017;38:85–91. doi:10.1016/j.sleep.2017.07.001
10. Westwood AJ, Beiser A, Jain N, et al. Prolonged sleep duration as a marker of early neurodegeneration predicting incident dementia. Neurology. 2017;88(12):1172–1179. doi:10.1212/WNL.0000000000003732
11. Blackwell T, Yaffe K, Ancoli-Israel S, et al. Poor sleep is associated with impaired cognitive function in older women: the study of osteoporotic fractures. J Gerontol a Biol Sci Med Sci. 2006;61(4):405–410. doi:10.1093/gerona/61.4.405
12. Blackwell T, Yaffe K, Laffan A, et al. Associations between sleep-disordered breathing, nocturnal hypoxemia, and subsequent cognitive decline in older community-dwelling men: the osteoporotic fractures in Men Sleep Study. J Am Geriatr Soc. 2015;63(3):453–461. doi:10.1111/jgs.13321
13. Chen JC, Espeland MA, Brunner RL, et al. Sleep duration, cognitive decline, and dementia risk in older women. Alzheimers Dement. 2016;12(1):21–33. doi:10.1016/j.jalz.2015.03.004
14. Byun E, Gay CL, Lee KA. Sleep, fatigue, and problems with cognitive function in adults living with HIV. J Assoc Nurses AIDS Care. 2016;27(1):5–16. doi:10.1016/j.jana.2015.10.002
15. Salahuddin N, Barroso J, Leserman J, Harmon JL, Pence BW. Daytime sleepiness, nighttime sleep quality, stressful life events, and HIV-related fatigue. J Assoc Nurses AIDS Care. 2009;20(1):6–13. doi:10.1016/j.jana.2008.05.007
16. Spira AP, An Y, Wu MN, et al. Excessive daytime sleepiness and napping in cognitively normal adults: associations with subsequent amyloid deposition measured by PiB PET. Sleep. 2018;41(10):10. doi:10.1093/sleep/zsy152
17. Wang H, Lane JM, Jones SE, et al. Genome-wide association analysis of self-reported daytime sleepiness identifies 42 loci that suggest biological subtypes. Nat Commun. 2019;10(1):1–12. doi:10.1038/s41467-019-11456-7
18. Foley D, Monjan A, Masaki K, et al. Daytime sleepiness is associated with 3-year incident dementia and cognitive decline in older Japanese-American men. J Am Geriatr Soc. 2001;49(12):1628–1632. doi:10.1111/j.1532-5415.2001.49271.x
19. Tsapanou A, Gu Y, Manly J, et al. Daytime sleepiness and sleep inadequacy as risk factors for Dementia. DEE. 2015;5(2):286–295. doi:10.1159/000431311
20. Leng Y, Stone K, Ancoli-Israel S, Covinsky K, Yaffe K. Who take naps? Self-reported and objectively measured napping in very old women. J Gerontol A. 2018;73(3):374–379. doi:10.1093/gerona/glx014
21. Leng Y, Redline S, Stone KL, Ancoli-Israel S, Yaffe K. Objective napping, cognitive decline, and risk of cognitive impairment in older men. Alzheimers Dement. 2019;15(8):1039–1047. doi:10.1016/j.jalz.2019.04.009
22. Sudlow C, Gallacher J, Allen N, et al. UK Biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015;12(3):e1001779. doi:10.1371/journal.pmed.1001779
23. Townsend P. Deprivation. J Soc Policy. 1987;16(2):125–146. doi:10.1017/S0047279400020341
24. Lyall DM, Cullen B, Allerhand M, et al. Cognitive test scores in UK Biobank: data reduction in 480,416 participants and longitudinal stability in 20,346 participants. PLoS One. 2016;11(4):e0154222. doi:10.1371/journal.pone.0154222
25. Cornelis MC, Wang Y, Holland T, Agarwal P, Weintraub S, Morris MC. Age and cognitive decline in the UK biobank. PLoS One. 2019;14(3):e0213948. doi:10.1371/journal.pone.0213948
26. Wilson RS, Boyle PA, Yu L, et al. Temporal course and pathologic basis of unawareness of memory loss in dementia. Neurology. 2015;85(11):984–991. doi:10.1212/WNL.0000000000001935
27. Li P, Zheng X, Ulsa MC, et al. Poor sleep behavior burden and risk of COVID-19 mortality and hospitalization. Sleep. 2021;44(8):zsab138. doi:10.1093/sleep/zsab138
28. Ulsa MC, Zheng X, Li P, et al. Association of poor sleep burden in middle age and older adults with risk for delirium during hospitalization. J Gerontol A. 2021:glab272. doi:10.1093/gerona/glab272.
29. Heaton RK, Franklin DR, Ellis RJ, et al. HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: differences in rates, nature, and predictors. J Neurovirol. 2011;17(1):3–16. doi:10.1007/s13365-010-0006-1
30. Grudnik JL, Kranzler JH. Meta-analysis of the relationship between intelligence and inspection time. Intelligence. 2001;29(6):523–535. doi:10.1016/S0160-2896(01)00078-2
31. Karalunas SL, Huang-Pollock CL. Integrating impairments in reaction time and executive function using a diffusion model framework. J Abnorm Child Psychol. 2013;41(5):837–850. doi:10.1007/s10802-013-9715-2
32. Hardy DJ, Hinkin CH. Reaction time performance in adults with HIV/AIDS. J Clin Exp Neuropsychol. 2002;24(7):912–929. doi:10.1076/jcen.24.7.912.8391
33. Ettenhofer ML, Foley J, Behdin N, Levine AJ, Castellon SA, Hinkin CH. Reaction time variability in HIV-positive individuals. Arch Clin Neuropsychol. 2010;25(8):791–798. doi:10.1093/arclin/acq064
34. Antinori A, Arendt G, Becker JT, et al. Updated research nosology for HIV-associated neurocognitive disorders. Neurology. 2007;69(18):1789–1799. doi:10.1212/01.WNL.0000287431.88658.8b
35. Cacciaglia R, Molinuevo JL, Sánchez‐Benavides G, et al. Episodic memory and executive functions in cognitively healthy individuals display distinct neuroanatomical correlates which are differentially modulated by aging. Hum Brain Mapp. 2018;39(11):4565–4579. doi:10.1002/hbm.24306
36. Nightingale S, Winsto A, Letendre S, et al. Controversies in HIV-associated neurocognitive disorders. Lancet Neurol. 2014;13(11):1139–1151. doi:10.1016/S1474-4422(14)70137-1
37. Mahmood Z, Hammond A, Nunez RA, Irwin MR, Thames AD. Effects of sleep health on cognitive function in HIV+ and HIV− adults. J Int Neuropsychol Soc. 2018;24(10):1038–1046. doi:10.1017/S1355617718000607
38. Byun E, Gay CL, Portillo CJ, Pullinger CR, Aouizerat BE, Lee KA. Cytokine polymorphisms are associated with daytime napping in adults living with HIV. Sleep Med. 2017;32:162–170. doi:10.1016/j.sleep.2016.12.021
39. Lorton D, Lubahn CL, Estus C, et al. Bidirectional communication between the brain and the immune system: implications for physiological sleep and disorders with disrupted sleep. NIM. 2006;13(5–6):357–374. doi:10.1159/000104864
40. Clinton JM, Davis CJ, Zielinski MR, Jewett KA, Krueger JM. Biochemical regulation of sleep and sleep biomarkers. J Clin Sleep Med. 2011;7(5 Suppl):S38–S42. doi:10.5664/JCSM.1360
41. Smith MT, McCrae CS, Cheung J, et al. Use of actigraphy for the evaluation of sleep disorders and circadian rhythm sleep-wake disorders: an American academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2018;14(7):1231–1237. doi:10.5664/jcsm.7230
42. Gao L, Lim ASP, Wong PM, et al. Fragmentation of rest/activity patterns in community-based elderly individuals predicts incident heart failure. Nat Sci Sleep. 2020;12:299–307. doi:10.2147/NSS.S253757
43. Health Protection Agency. HIV in the United Kingdom: 2011 report. Health Protection Services; 2011.
44. O’Halloran C, Sun S, Nash S, et al. HIV in the United Kingdom: towards zero 2030. Public Health England; 2019.
45. May M, Sterne JAC, Sabin C, et al. Prognosis of HIV-1-infected patients up to 5 years after initiation of HAART: collaborative analysis of prospective studies. AIDS. 2007;21(9):1185–1197. doi:10.1097/QAD.0b013e328133f285
46. Antiretroviral Therapy Cohort Collaboration. Causes of death in HIV-1-infected patients treated with antiretroviral therapy, 1996–2006: collaborative analysis of 13 HIV cohort studies. Clin Infect Dis. 2010;50(10):1387–1396. doi:10.1086/652283.
47. Saunders P, Goodman AL, Smith CJ, et al. Does gender or mode of HIV acquisition affect virological response to modern antiretroviral therapy (ART)? HIV Med. 2016;17(1):18–27. doi:10.1111/hiv.12272
48. Montano M, Bhasin S, D’Aquila RT, et al. Harvard HIV and aging workshop: perspectives and priorities from Claude D. Pepper centers and centers for AIDS research. AIDS Res Hum Retroviruses. 2019;35(11–12):999–1012. doi:10.1089/AID.2019.0130
49. Hogg RS, Eyawo O, Collins AB, et al. Health-adjusted life expectancy in HIV-positive and HIV-negative men and women in British Columbia, Canada: a population-based observational cohort study. Lancet HIV. 2017;4(6):e270–e276. doi:10.1016/S2352-3018(17)30029-2
50. Tuchman E. Women and addiction: the importance of gender issues in substance abuse research. J Addict Dis. 2010;29(2):127–138. doi:10.1080/10550881003684582
51. Salter ML, Lau B, Go VF, Mehta SH, Kirk GD. HIV infection, immune suppression, and uncontrolled viremia are associated with increased multimorbidity among aging injection drug users. Clin Infect Dis. 2011;53(12):1256–1264. doi:10.1093/cid/cir673
52. Justice AC, McGinnis KA, Tate JP, et al. Risk of mortality and physiologic injury evident with lower alcohol exposure among HIV infected compared with uninfected men. Drug Alcohol Depend. 2016;161:95–103. doi:10.1016/j.drugalcdep.2016.01.017
53. Hu K, Li P, Gao L. Sleep, rest-activity rhythms and aging: a complex web in Alzheimer’s disease? Neurobiol Aging. 2021;104:102–103. doi:10.1016/j.neurobiolaging.2021.02.017
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.