Back to Journals » Journal of Pain Research » Volume 19
Data Mining of Acupuncture Prescriptions for Lateral Epicondylitis: A Literature-Based Analysis of Acupoint Patterns and Parameters
Authors Xu Y ![]() , Chen M, Dong Y, Wang F, Lai Q, Ye Y, Huang J, Xu Y, Shi M, Zhan Q
, Chen M, Dong Y, Wang F, Lai Q, Ye Y, Huang J, Xu Y, Shi M, Zhan Q
Received 23 November 2025
Accepted for publication 18 March 2026
Published 31 March 2026 Volume 2026:19 583466
DOI https://doi.org/10.2147/JPR.S583466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yunyun Xu,1 Meilan Chen,1 Yiqi Dong,1 Fangjun Wang,1 Qingzhong Lai,1 Yang Ye,1 Jiayuan Huang,2 Yuanhong Xu,3 Meng Shi,4 Qiang Zhan1
1Department of Tuina, Hangzhou Red Cross Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2The Second School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 3The Third School of Clinical Medicine (School of Rehabilitation Medicine), Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Acupuncture, Hangzhou Red Cross Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Qiang Zhan, Department of Tuina, Hangzhou Red Cross Hospital, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Background: Lateral epicondylitis (LE) is a prevalent musculoskeletal disorder characterized by pain and functional limitations of the elbow. Acupuncture is increasingly employed as an adjunctive therapy for LE, owing to its potential to alleviate symptoms. Significant heterogeneity persists in clinical acupuncture protocols, and the optimal selection of acupoints remains inadequately defined, thereby limiting the generalizability and standardization of treatment approaches.
Objective: This study seeks to identify and synthesize the most frequently used and effective acupoint combinations for LE treatment through the application of data mining techniques to analyze existing clinical literature.
Methods: Eight electronic databases were searched for studies on acupuncture treatments for LE published from January 2015 to March 2025. Randomized controlled trials and clinical controlled trials that reported acupuncture prescriptions for LE were included. Reviews, meta-analyses, protocols, animal experiments, guidelines, and case reports were excluded. Literature screening and data extraction were performed based on predefined criteria. Microsoft Excel 2019 was used for descriptive statistical analysis. Association rule analysis was performed using R Version 4.5.0. A visual association network of acupoints was generated using Cytoscape 3.10.1. OriginPro2024 was used for clustering and correlation analyses of acupoints.
Results: Forty-two articles were included according to the established criteria. Regarding treatment parameters, the most frequently used needle type was 0.30 mm × 40 mm, and a 30-minute retention time was predominant. The most common treatment frequency was 7 days per week, with total duration most commonly being 20 days. Regarding acupoint selection, the most frequently used acupoints were Ashi point, Quchi (LI11), Shousanli (LI10), Hegu (LI4) and Waiguan (TE5). The Large Intestine Meridian of Hand Yangming was the most frequently used meridian. Among specific point categories, five-shu points were the most frequently employed. The frequency of acupoints used was highest in the elbow. The association analysis showed the most supported acupoint pair was LI11 and LI10. Core acupoints identified for LE treatment included Ashi point, LI4, LI11, LI10 and TE5. By hierarchical cluster analysis, the acupuncture points were categorized into four categories.
Conclusion: This review identified 0.30 mm × 40 mm needles, 30‑minute retention, 7 sessions weekly, and 20 days total duration as the predominant treatment parameters for lateral epicondylitis. The core acupoints included Ashi, LI11, LI10, LI4, and TE5. Notably, the combination of LI11 and LI10 constituted the most significant association rule. The Large Intestine Meridian and five‑shu points were most frequently used, and acupoint distribution was highest in the elbow. These findings provide evidence-based support for clinical acupuncture decision-making, yet further prospective trials are needed to confirm the validity of these patterns.
Keywords: acupuncture, lateral epicondylitis, data mining, association rule analysis, cluster analysis
Introduction
Lateral epicondylitis (LE), commonly known as tennis elbow, is characterized by pain over the lateral epicondyle of the humerus when using the arms, especially when grasping and lifting heavy objects.1,2 It is a public health issue with a prevalence of 1%~3% in the general population with higher incidence rates among manual workers and mostly affects persons aged 40~50 years with equal sex distribution.3,4 The condition is associated with several adverse effects, including functional impairment in daily and professional activities, increased psychological stress and prolonged workplace absenteeism.5 Various conservative treatment strategies, including corticosteroid injections, nonsteroidal anti-inflammatory drugs (NSAIDs), and physical therapies, have been commonly employed in the management of LE.6–8 However, such treatments are often reported to increase the risk of adverse events or have poor long-term outcomes.9 Corticosteroid injections may provide short-term pain relief but are associated with high recurrence rates and potential long-term tissue damage.10 NSAIDs can alleviate inflammation and pain but their prolonged use is constrained by gastrointestinal and cardiovascular risks.11 Physical therapies, such as extracorporeal shockwave therapy and eccentric exercises, have demonstrated variable efficacy, with some studies reporting limited benefits compared to placebo.12,13 For refractory cases, surgical interventions, including open or arthroscopic release, may be considered. However, evidence supporting their superiority over conservative management remains inconclusive.14 Given the limitations and inconsistent outcomes associated with current treatment options, there is increasing interest in complementary approaches.15
As a form of Traditional Chinese Medicine, acupuncture has been increasingly employed as an adjunctive therapy of musculoskeletal pain owing to its complementary and alternative consequences in improving symptoms evidently and harmlessly.11 Previous systematic reviews have demonstrated that acupuncture treatment was both tolerable and effective in reducing pain and alleviating pain-related disability in patients with LE.16–18 Recent evidence has further clarified the therapeutic benefits of acupuncture for LE. Beyond its mechanistic advantages in providing rapid pain relief by modulating local microcirculation and activating endogenous opioid pathways,19,20 acupuncture is also distinguished by its safety. Unlike nonsteroidal anti-inflammatory drugs or corticosteroid injections, which carry risks of gastrointestinal, cardiovascular, and local tissue complications, acupuncture is associated with minimal adverse effects.21 Furthermore, studies have suggested that acupuncture may facilitate short-term functional recovery.22 However, several limitations regarding acupuncture for LE should be acknowledged. The overall quality of the evidence remains limited, largely attributed to methodological shortcoming, including small sample sizes, lack of blinding, and considerable heterogeneity in acupuncture treatment.17,23 While short-term benefits have been well-documented, evidence regarding long-term efficacy remains inconsistent.24 A recent review concluded that acupuncture may be ineffective compared to other interventions, highlighting ongoing controversies in the literature.25 Additionally, improper acupoint selection or stimulation parameters may lead to adverse events, such as needling pain, hematoma, or transient symptom exacerbation.21,26 These limitations highlight the need for rigorous, large-scale trials with standardized interventions to establish the therapeutic role of acupuncture in LE management.
Acupuncture therapy works by prescription, which is a combination of acupoints, stimulation methods and treatment course. There have been alternative studies evaluating the efficacy of acupuncture prescriptions in the treatment of LE. However, due to the considerable variation in acupuncture treatments, determining the optimal acupoint selection and combination for LE remains challenging. Some studies also indicated that improper acupoints parameter selection may induce negative outcomes for LE.23,26 Consequently, it’s crucial to explore the regularity of clinical acupuncture prescription to provide a reference for standardization and clinical practice of LE with acupuncture. Despite the increasing published research on acupuncture for LE, a comprehensive acupoint selection patterns and treatment parameters remains lacking. While previous systematic reviews have provided valuable insights into the efficacy of acupuncture, they have not systematically analyzed the underlying rules underlying acupoint combinations or stimulation parameters. By analyzing previous studies, these methods can reveal associations and clusters that may not be readily discernible through narrative synthesis or conventional meta-analysis.27,28 Indeed, data mining has been increasingly utilized in acupuncture research to extract and analyze treatment parameters, facilitating the identification of potential acupoints for the effective management of various diseases.29,30 Therefore, this study employed data mining techniques, including association rule mining, network analysis and hierarchical cluster analysis, to systematically examine acupuncture prescriptions for LE, with the objective of summarizing the characteristics and patterns of acupoint selection and treatment parameters in clinical practice. Therefore, this study focused on analyzing the acupuncture prescription for LE through data mining techniques, such as association rule mining and hierarchical cluster analysis, summarizing characteristics and patterns of acupuncture for LE.31–33
By analyzing treatment parameters, our findings are expected to provide clinicians with an evidence-based reference for optimizing acupuncture treatment for LE, thereby helping to reduce variability in clinical practice. For researchers, this analysis provides a methodological framework for future investigations. Patients may also benefit from greater transparency regarding commonly used acupuncture approaches. Overall, this study contributes to the standardization of acupuncture practice and promotes consistent, high-quality care for individuals with LE.
Methods
Retrieval Strategy
We searched electronic databases including PubMed, Embase, Web of Science, Cochrane Library, Chinese Biomedical Literature Database, Wanfang Data, Chongqing VIP Database and China National Knowledge Infrastructure to retrieve research literature on acupuncture treatment for LE published between January 2015 and March 2025 without language limitation. The following search keywords were mainly used and modified according to different databases: (a) “tennis elbow”, “tennis elbows”, “lateral epicondylitis”, “epicondylitis lateral”, “epicondylitis lateral humeral”; and (b) “Acupuncture”, “acupuncture therapy”, “acupuncture treatment”, “eletro-acupuncture”, “eletroacupuncture”, “manual acupuncture”, “needle”, “needling”, “warm needle” (Supplementary Material 1). Chinese characters with the same meaning were used for literature retrieval in Chinese databases. Further relevant studies were manually searched. This article is based on previously conducted studies and does not include any new research involving human participants or animals conducted by any of the authors.
Literature Screening
Two reviewers (CML and YY) independently screened all the titles and abstracts of the eligible articles based on the criteria. After reading the titles and abstracts, we removed duplicate and irrelevant articles. Subsequently, the screening was performed by reading the remaining articles in full text. If there was disagreement between the two researchers regarding an article, it was then resolved by discussion between the two reviewers or consultation with a third reviewer (WFJ).
Types of Studies
This study aimed to explore the effects of acupuncture on parameters related to LE, including randomized control trials (RCTs) and clinical control trials (CCTs). Reviews, meta-analyses, protocols, animal experiments, guidelines and case reports were excluded. Studies that did not report any of the relevant parameters were excluded. All qualifying studies included a control group as a minimum requirement. Compared to controls, patients who underwent acupuncture in the included studies had positive outcomes. Furthermore, the sample size was more than ten. Two reviewers (CML and YY) independently assessed the risk of bias of all included trials using the Cochrane Risk of Bias tool (RoB 1) implemented in RevMan5.4. This tool evaluates seven domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other bias. Any disagreements were resolved through discussion with a third reviewer (WFJ).
Types of Participants
The patients described in the studies met one of the following diagnostic criteria for LE: Clinical diagnosis and treatment guidelines: Orthopedics volume,34 Standards for Diagnosis and Therapeutic Effect of TCM Diseases and Syndromes,35 Practical Orthopedics.36 No restrictions based on the side of the lesion (unilateral or bilateral), duration and severity of illness, age, sex, race or geographic region imposed.
Intervention and Control Group
Interventions were acupuncture or a combination of acupuncture with other treatments, such as mobilization with movement, Tuina or extracorporeal shock wave. Acupuncture treatment was defined as manual acupuncture, electroacupuncture and warm needle. Studies that solely involved unconventional acupuncture types such as wrist and ankle acupuncture, auricular acupuncture, abdominal acupuncture, moxibustion and laser stimulating were excluded. Additionally, studies were excluded if they had ambiguous acupoint prescriptions, unreportable outcomes, or showed no significant efficacy in the intervention group.
Types of Outcome Measures
As the study focused on data mining of acupuncture prescriptions for LE, inclusion in the analysis required the use of at least one of the following clinical efficacy indicators: Visual Analog Scoring (VAS), Mayo Elbow Performance Score (MEPS), Tennis Elbow Rating Scale (TERS), or Pain-Free Grip Strength (PFG). Studies that reported only chemical and physical examinations were excluded.
Data Collection and Extraction
The collected studies were input into Endnote X9 by two reviewers (DYQ and XYH), who then independently and manually extracted comprehensive data from the eligible trials using a pre-defined data extraction form. Any discrepancies were resolved through discussion with the third reviewer (SM). Given that all extracted data were objective factual information explicitly reported in the original studies, formal inter-reviewer reliability testing was not applicable to this data mining analysis. Nevertheless, the independent extraction and cross-checking procedures described above ensured data accuracy. The characteristics of the included studies encompassed title, needle type, treatment frequency, stimulation duration, total treatment duration, acupoint selection and adverse effects. Finally, we established a dataset of acupuncture treatment for LE and entered all the data into a Microsoft Excel 2019 workbook. Missing data were obtained by contacting the corresponding or relevant authors. If the missing data could not be retrieved, the study was excluded from the specific analysis requiring that parameter but was retained for other analyses where data were complete. All acupoint prescriptions from the included literature were compiled into a novel Excel table, which was used to conduct descriptive statistical analyses on the frequency of acupoint usage, meridian attribution, point locations and the classification of specific acupoints. The above results were illustrated using various graphs and diagrams. The radar diagram and Circular strip diagram were plotted by applying “ggplot2” of the R software (version 4.5.0). Circular diagram of meridians was plotted by https://www.bioinformatics.com.cn, an online platform for data analysis and visualization. The names of all the acupoints involved in the prescription were standardized according to the World Health Organization’s Standard Acupuncture Point Location in the Western Pacific Region and the China National Standard “Naming and Positioning of Acupoints” (GB/T 12346–2006).
Association Rule Analysis
The association rule analysis of the Apriori algorithm in this study were performed using R software (version 4.5.0). This scheme was properly adapted by applying “arules” of the R package. Visualization of association rules could be perfectly matched by applying “arulesViz” of the R package. To capture clinically meaningful acupoint combinations, the minimum support threshold was set at 10%, ensuring sufficient frequency across studies; the minimum confidence threshold was set at 80% to guarantee that only strong and reliable associations between acupoints were included. The lift was used to verify that two itemsets were dependent on one another, which made the rule valuable when the lift’s value is larger than 1. We used the support level to determine the probability that A and B occurred simultaneously.
Complex Network Analysis
To obtain the core acupoint prescriptions of the acupuncture treatments for LE, the interconnection network of acupoints in all the included prescriptions was analyzed using IBM SPSS Modeler 18.0. The acupuncture prescriptions were transformed into a vector format, and the vectors were entered into a prescription table in a T/F format. These standardized vectors were then imported into IBM SPSS Modeler 18.0, resulting in an association rule stream that included acupoint nodes and their weights. Subsequently, a visual association network of effective acupoints was generated using Cytoscape 3.10.1. Acupoints (defined as the “nodes” of the network) were connected by “lines” in the network. Thicker connecting lines represented more frequently used acupoints.
Clustering and Correlation Analysis of Acupoints
The literature selecting acupoints based on pattern identification was initially reviewed, and a matrix was constructed to link each pattern identification with its corresponding acupoints. OriginPro 2024 was utilized to conduct clustering and correlation analyses of the acupoints mentioned in the text. Clustering and correlation heatmap analyses were performed using the Phi correlation coefficient, which measured the strength and direction of associations between binary variables.
Results
Study Selection
A total of 1,765 relevant studies were identified. Among these, 953 were identified as duplicates, and 590 were excluded after screening the titles and abstracts. A total of 180 articles were excluded following full-text evaluation, while 42 articles were retained for further analysis. The study screening process is represented through a flowchart in Figure 1.
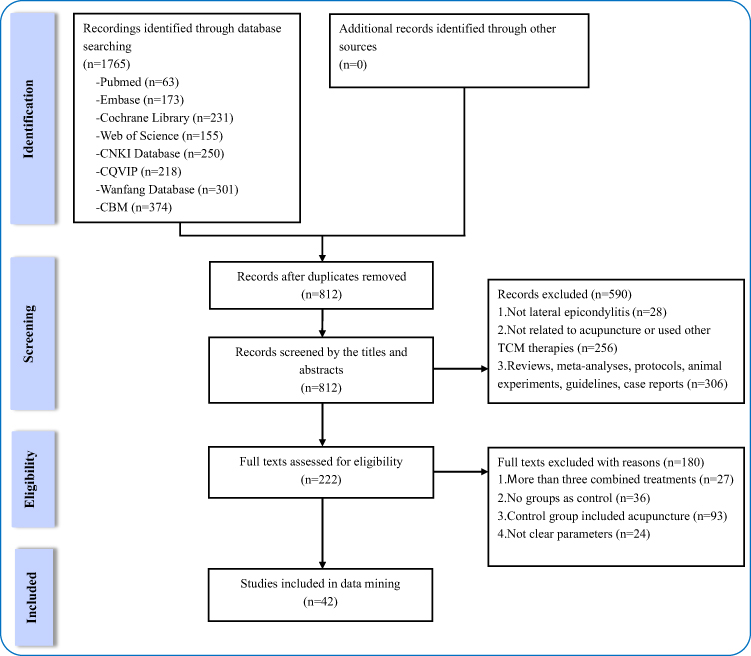 |
Figure 1 Study flow diagram. |
Risk of Bias Assessment
All 42 included studies reported randomization. However, 5 studies had unclear risk due to insufficient description of methods, and 2 studies using registration order were rated as high risk. Allocation concealment was unclear in 36 studies, with only 6 studies describing adequate methods rated as low risk. Due to the nature of acupuncture, blinding of participants and personnel was not implemented in most studies; only 3 studies reported adequate blinding (low risk), while the remaining were high risk. For blinding of outcome assessment, 5 studies reported blinded evaluators (low risk), with the remainder unclear. Incomplete outcome data was unclear in 2 studies. Selective reporting and other biases were low risk across all studies. Details are shown in Supplementary Material 2.
Frequency of Needle Type
Eleven types of needles were analyzed across 42 studies, with a total of 32 recorded uses. However, ten studies did not specify the needle type, which may have impacted the replication of the RCT. The most commonly used needle type in these studies was 0.30 mm × 40 mm, used nine times and accounting for 28.13% of the total frequency, as demonstrated in Table 1.
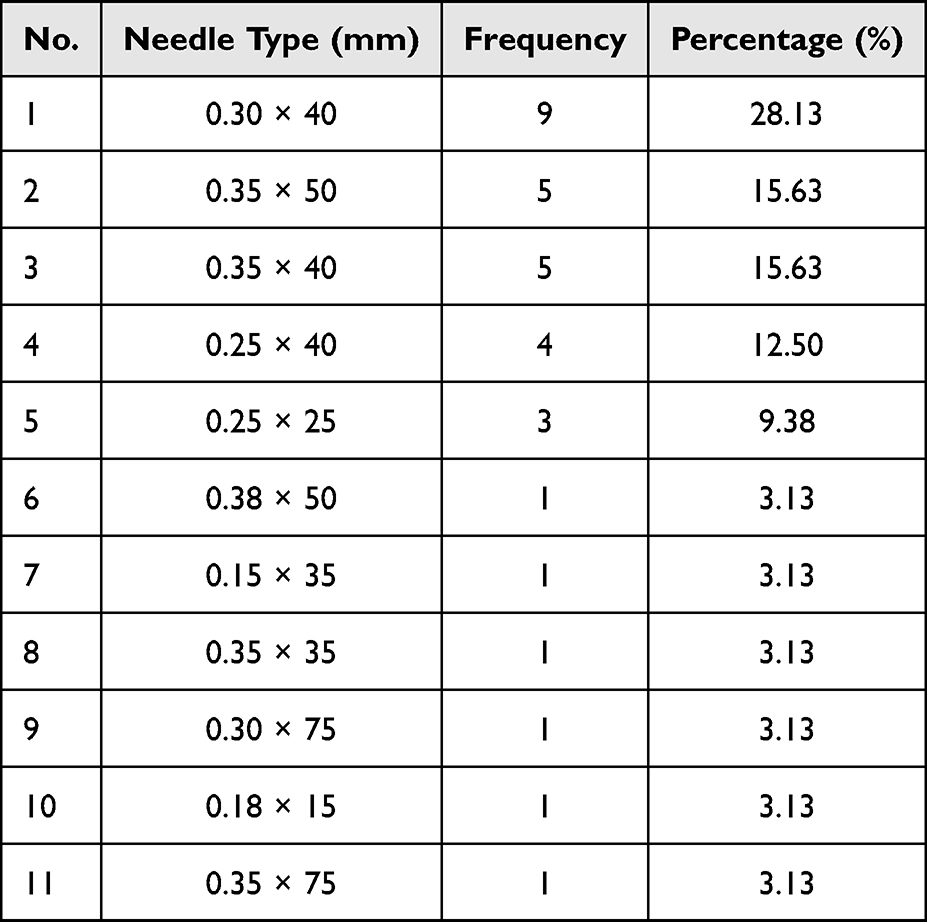 |
Table 1 Frequency of Needle Type |
Retention Time, Treatment Frequency and Total Treatment Duration
Six needle retention times were reported in thirty-four studies, with the longest being 30 minutes. The 30-minute retention time was most frequently employed, appearing in twenty instances and constituting over half of all documented cases. This suggests that a 30-minute acupuncture intervention may be the preferred clinical practice for LE to achieve the intended therapeutic effect, as shown in Table 2. Five treatment frequencies were mentioned in 35 studies, including 7, 4, 5, 3, and 1 day(s) per week, as demonstrated in Table 3. Twelve kinds of total treatment durations were mentioned in 34 studies and the top three were 20, 10 and 14 days, as shown in Table 4.
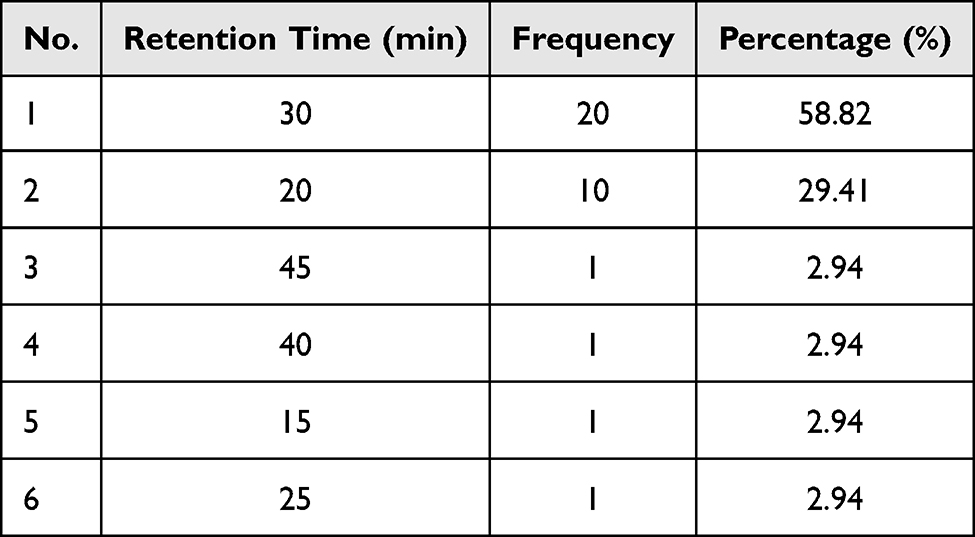 |
Table 2 Frequency of Retention Time |
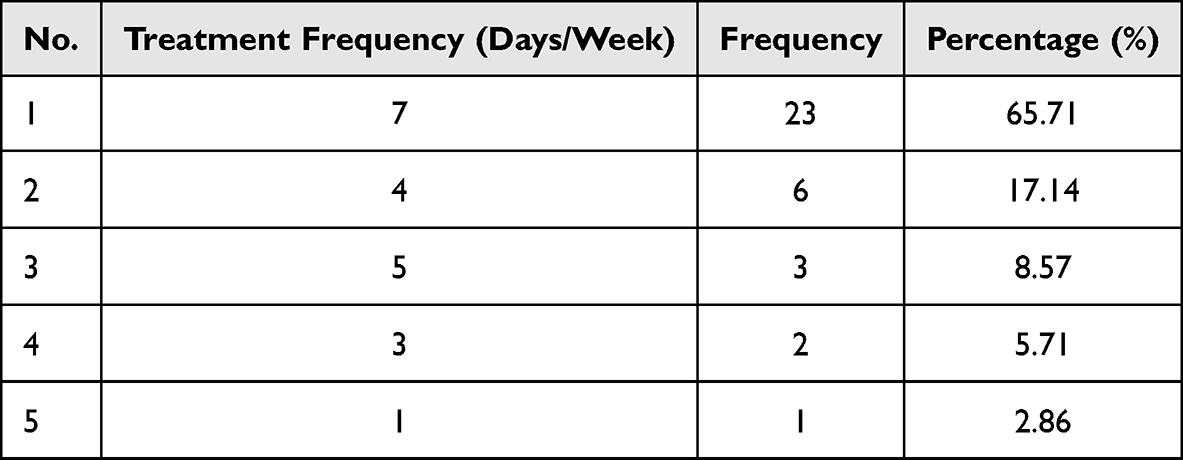 |
Table 3 Frequency of Treatment Frequency |
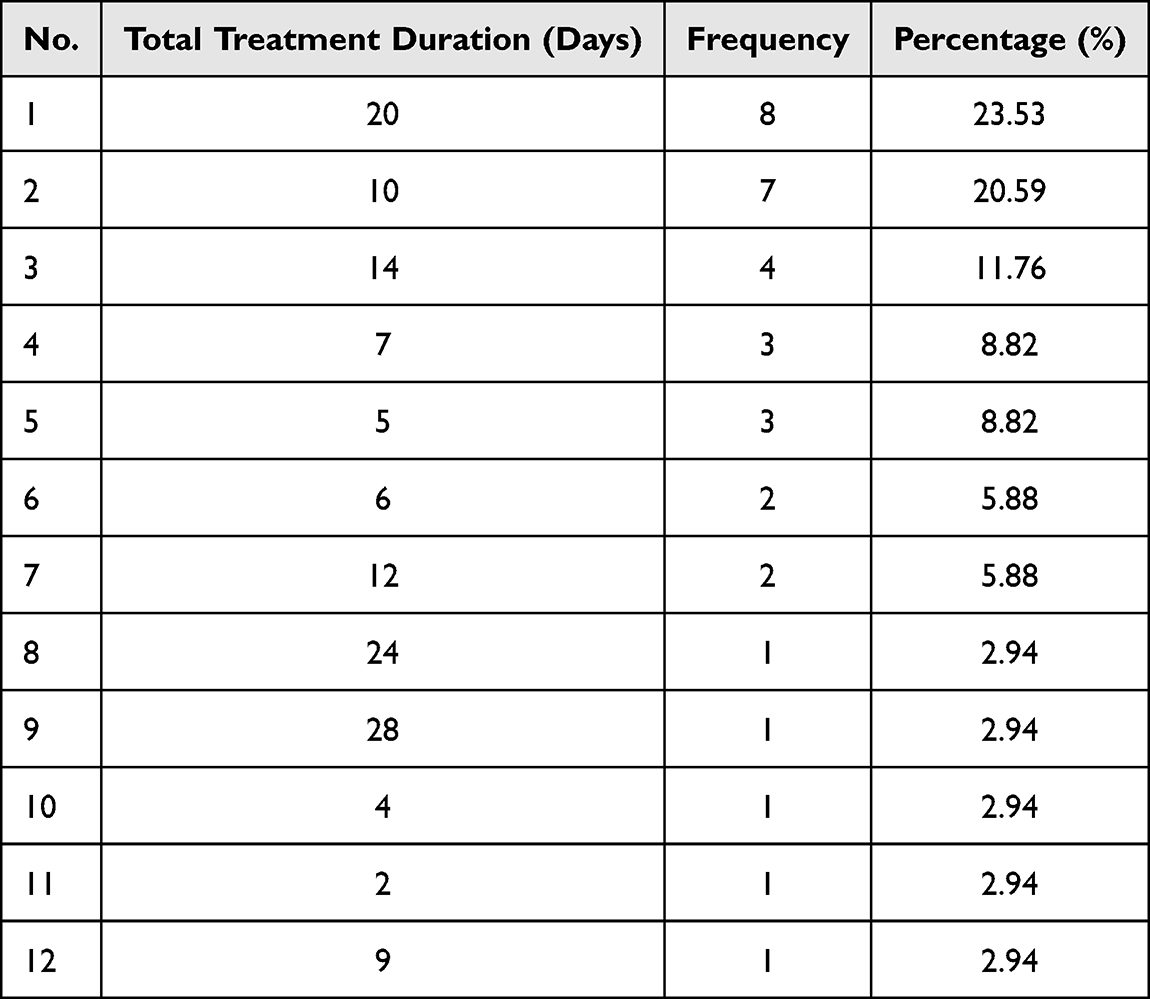 |
Table 4 Frequency of Total Treatment Duration |
Application of Acupoints
Forty-two eligible intervention prescriptions, 40 acupoints, and 196 occurrences were extracted from 42 studies. The most frequently selected acupoints are presented in Table 5, which include Ashi point, Quchi (LI11), Shousanli (LI10), Hegu (LI4), Waiguan (TE5), Chize (LU5), Zhouliao (LI12), Yanglinquan (GB34), Shouwuli (LI13), Jiaji (EX-B2), Zusanli (ST36) and Jianjin (GB21). Ashi point was the most frequently used, with a frequency of 15.82% appearing in 31 of 42 prescriptions. LI11 was the second most frequently used, with a frequency of 14.80% appearing in 29 prescriptions, followed by LI10 with a frequency of 13.27% in 26 prescriptions, LI4 with a frequency of 9.18% in 18 prescriptions, and TE5 with a frequency of 8.16% in 16 prescriptions.
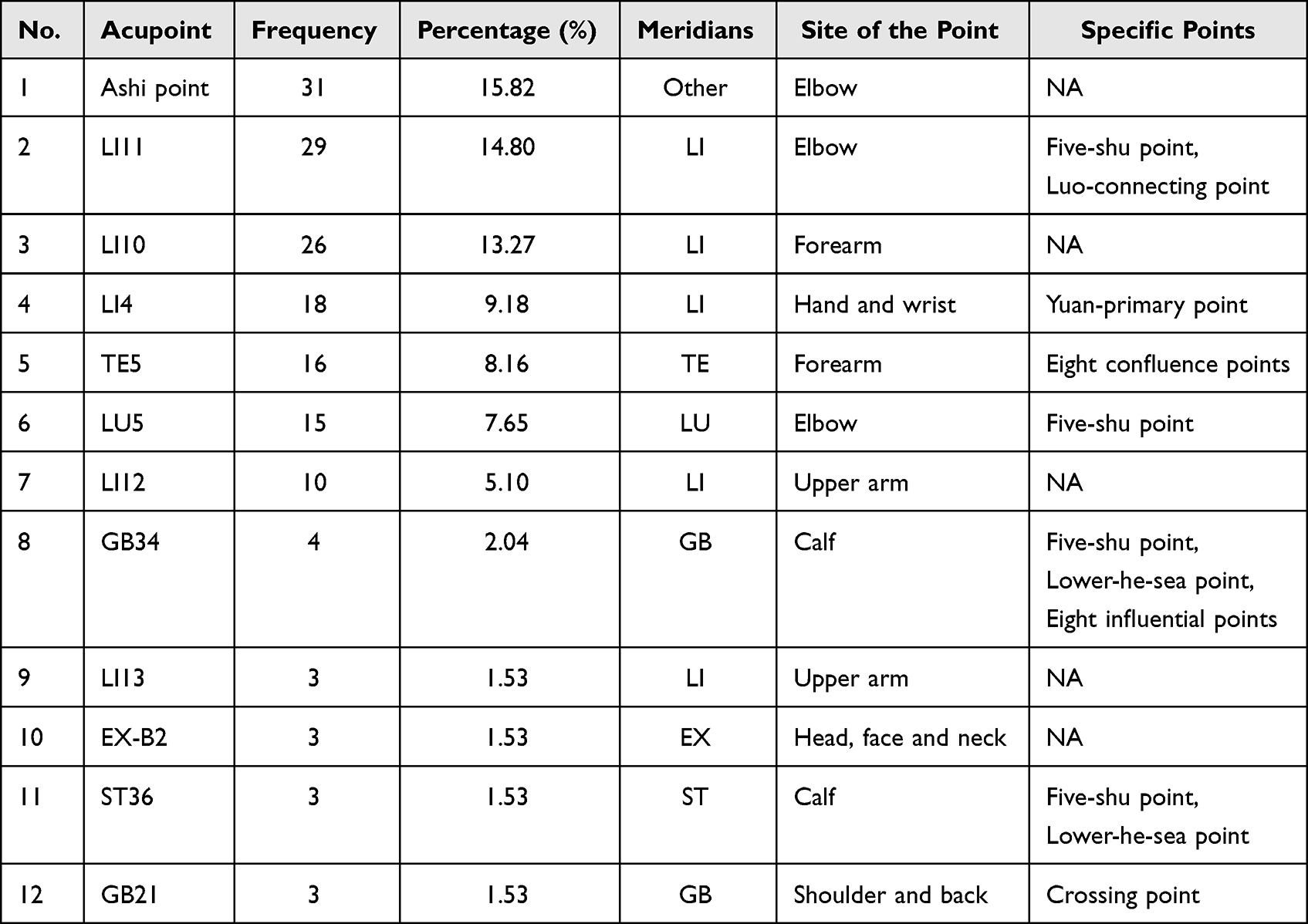 |
Table 5 The Top 12 Acupoints for LE Treatment |
Application of Meridians
After screened all acupoint prescriptions, we found that 38 acupoints were used by 11 conventional meridians, 1 acupoint was used by the Extraordinary meridian and 1 acupoint was used by the Nonconventional meridian. The frequency and percentage of meridians, the number and frequency of acupoints used in each meridian were demonstrated in Table 6. Figure 2A shows the frequency of all meridians involved in acupuncture prescriptions of LE. Notably, the Large Intestine Meridian of Hand Yangming (LI) acupoints accounted for the highest number of acupoints and were used as frequently as 94 times, representing 47.96% of total acupoint occurrences, while the Pericardium Meridian of Hand Jueyin (PC) and the Heart Meridian of Hand Shaoyin (HT) meridians were used only once. Although the Nonconventional meridian had only one acupoint, the frequency accounted for 15.82%, indicating that Ashi point may be potentially valuable for acupuncture interventions in LE. Of the eleven meridian acupoints, 84.57% (137/162) were Yang meridian acupoints and 15.43% (25/162) were Yin meridian acupoints. Additionally, Figure 2B directly shows relationship between acupoints and meridians.
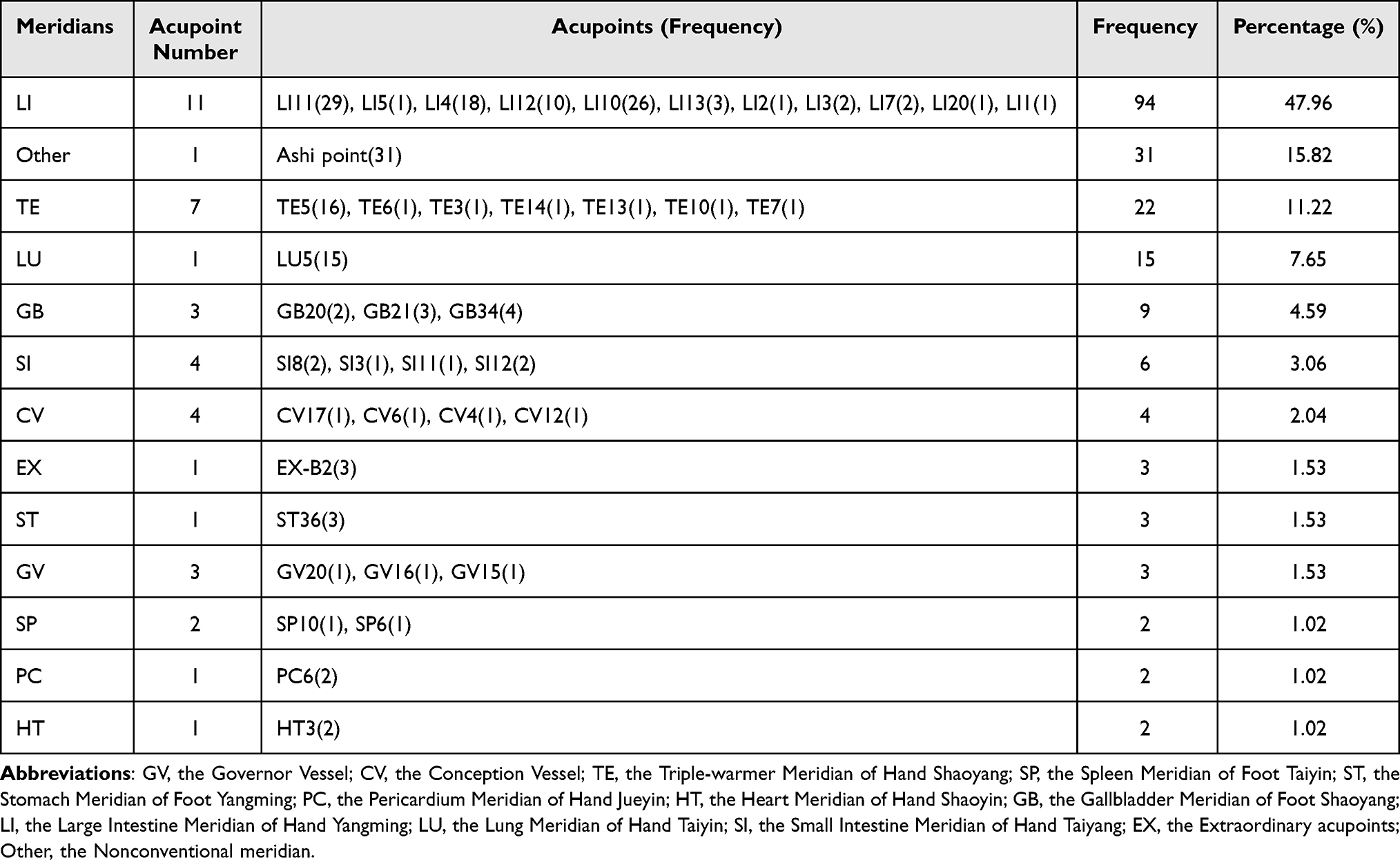 |
Table 6 Frequency of Meridian Application for LE Treatment |
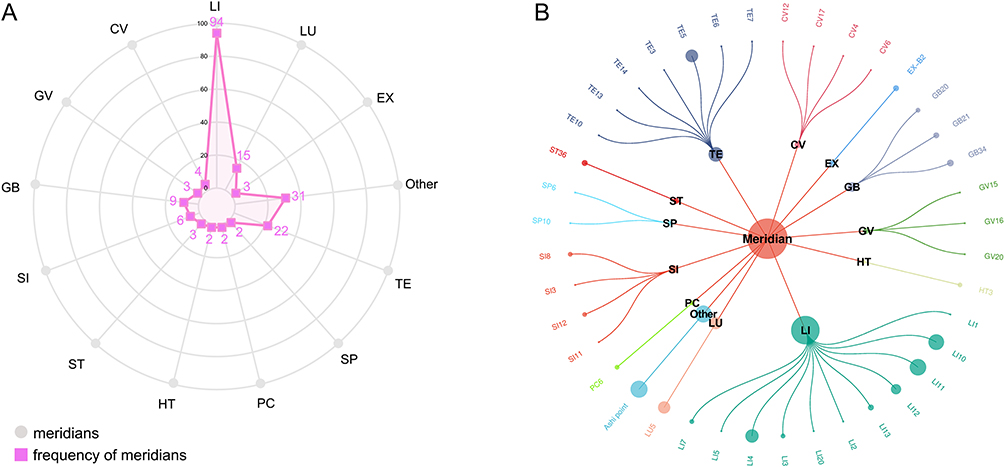 |
Figure 2 (A) Radar diagram of the frequency of meridians. Gray dots represent individual meridians, and concentric circles from the innermost to the outermost indicate usage frequency ranging from 0 to 100. Pink squares represent the frequency of meridians. Specific frequency values are also displayed in the diagram. (B) Circular diagram of the relationship between acupoints and meridians. The central node represents meridians, the second-layer nodes represent specific meridians, and the outermost nodes represent individual acupoints. Acupoints belonging to the same Meridian are depicted in consistent colors to indicate their meridian affiliation. Node size reflects usage frequency: larger circles indicate higher frequency of acupoints or meridians. |
Application of Specific Acupoints
The results demonstrated the use of specific acupoints in the acupuncture prescription, including frequency, amount of acupoints, selected acupoints and percentage. Of the 40 acupoints, 29 were specific acupoints, accounting for 72.50% of the total number of acupoints, and 8 acupoints contained more than one attribute. Overall, a total of nine types of specific acupoints were involved. Besides, the most used specific acupoints were Five-shu points. The frequency, percentage and number of acupoints used as Five-shu points in the specific points analysis were 64, 42.38% and 14, respectively. Eight confluence points had a moderate frequency as 19 times (Table 7). Notably, the percentage of the Front-mu points and Xi-cleft points were both 1.99%, implying that acupuncturists seldom considered these specific acupoints for therapeutic LE. Additionally, the frequency of nine specific acupoints were visualized with in Figure 3.
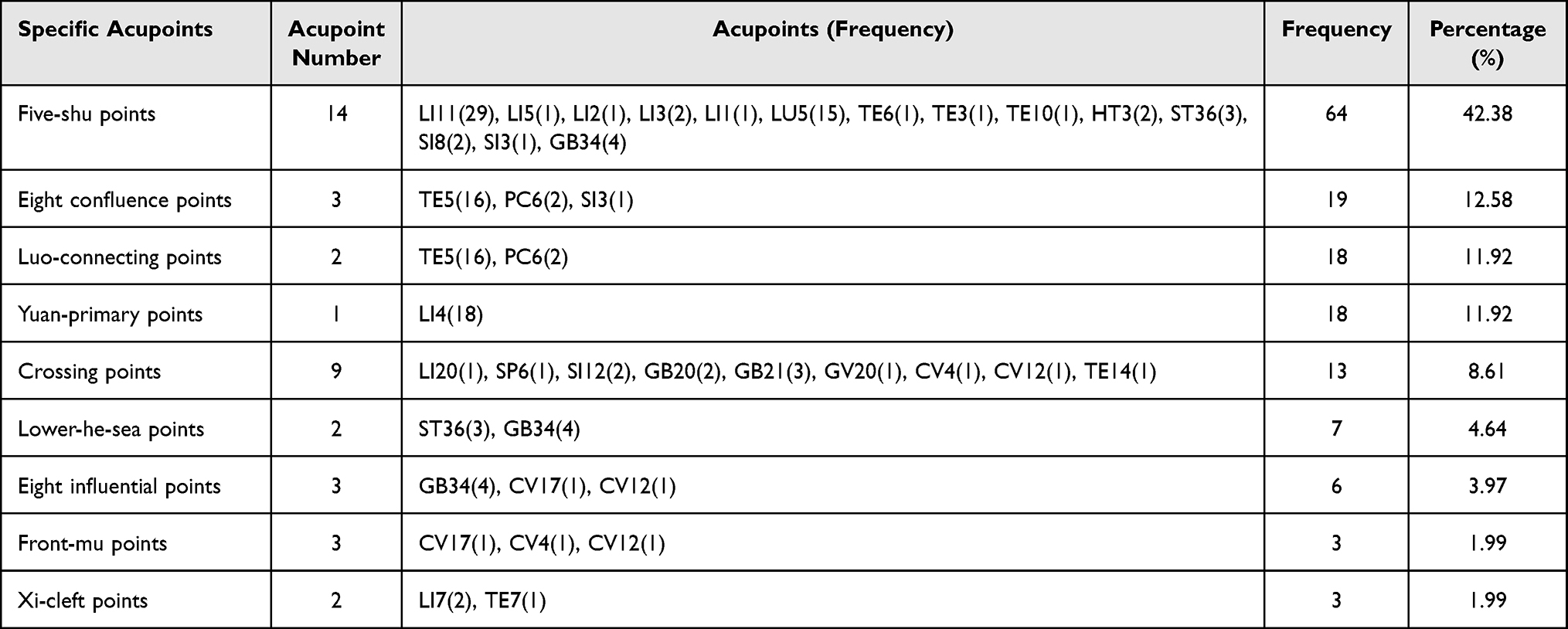 |
Table 7 Frequency of Special Point Application for LE Treatment |
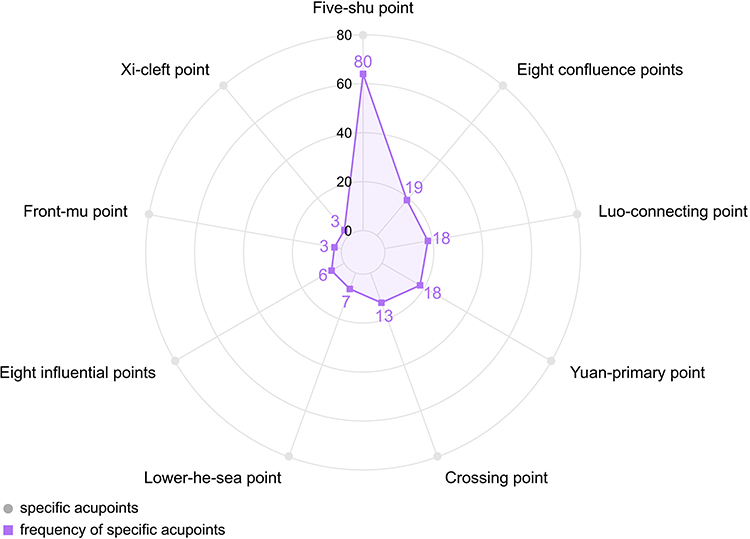 |
Figure 3 Radar diagram of the frequency of specific acupoints. Gray dots represent specific acupoints, and concentric circles from the innermost to the outermost indicate usage frequency ranging from 0 to 80. Purple squares represent the frequency of specific acupoints. Specific frequency values are also displayed in the diagram. |
Application of Acupoints on Different Body Parts
The frequency and percentage of acupoint distribution were analyzed and presented in Table 8. In the acupoint distribution analysis, the elbow was the most selected area, with 6 acupoints used a total of 80 times, accounting for 40.82% of total acupoint occurrences. This area corresponds with the clinical symptoms of patients with LE, indicating that acupuncturists tend to consistently select these acupoint locations. While the thigh had the fewest acupoints, one in total, and this location was not considered, possibly because of disease specificity. Besides, the frequency of different body parts was visualized with in Figure 4.
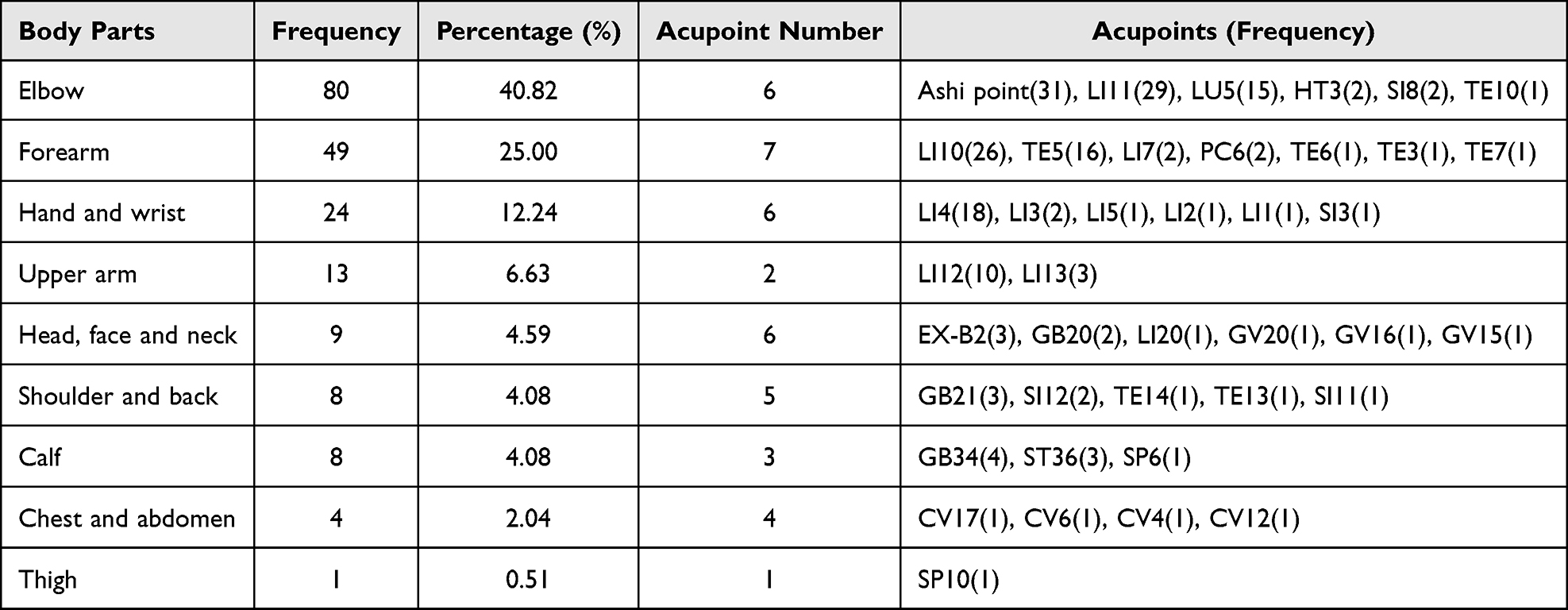 |
Table 8 Frequency of Body Parts and Acupoints Used for LE Treatment |
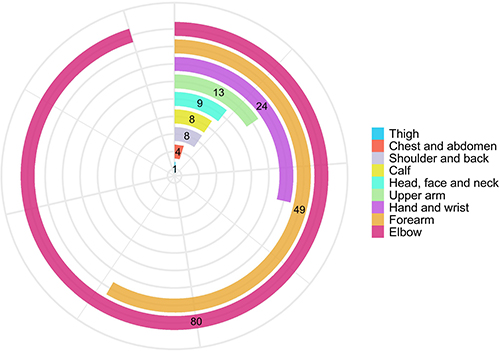 |
Figure 4 Circular strip diagram of the frequency of different body parts. Different colors represent distinct body parts, and strip lengths indicate the frequency of acupoint usage in each region. |
Association Rules of Acupoints for LE
In this study, we performed association rule analysis using the Apriori algorithm, and the resulting 59 association rules were visualized in a grouped matrix, as shown in Figure 5. This method utilizes color and size encoding to show the characteristics of grouped rules, offering a clear and structured overview of the associations. In this matrix, rows represent antecedent item groups (LHS) and columns represent consequent item groups (RHS). Labels such as “{LI10, Ashi point, +3 items}” follow the standard output format of the association rule mining software, indicating that the LHS group contains five acupoints, with LI10 and Ashi point as the two representative items and three additional acupoints. These five acupoints can form various combinations. Multiple association rules exist between each LHS and RHS group, but due to space limitations, each circle represents only one representative rule in Figure 5. The complete list of all association rules is provided in Supplementary Material 3. In addition, association rules with support exceeding 20% were summarized and presented in Table 9, along with their confidence, support, and lift values. The top five supported pairs included {LI10} ≧ {LI11} (support: 57.14%, confidence: 92.31%, lift: 1.34), {LI11} ≧ {LI10} (support: 57.14%, confidence: 82.76%, lift: 1.34), {Ashi point, LI10} ≧ {LI11} (support: 40.48%, confidence: 94.44%, lift: 1.37), {Ashi point, LI11} ≧ {LI10} (support: 40.48%, confidence: 80.95%, lift: 1.31), and {TE5} ≧ {LI10} (support: 33.33%, confidence: 87.50%, lift: 1.41). Furthermore, all 19 pairs of acupoint combinations had lift values > 1. Figure 6 presents a scatter plot illustrating the distribution of support and confidence for the association rules. Each point corresponds to a specific rule. The vertical axis (support) represents the frequency of rules, with higher values indicating more common combinations. The horizontal axis (confidence) represents rule reliability, with points positioned farther to the right indicating stronger predictive relationships. Some rules are distributed in the upper region of the plot, indicating relatively high support, while numerous points are concentrated in the right region, indicating high confidence. Outliers in the lower-central region represent infrequent yet clinically significant patterns. The color gradient indicates lift, with darker points representing stronger positive associations. The results were consistent with the results in the correlation matrix of acupoints (Figure 7).
 |
Table 9 The Top 19 Acupoint Association Rules for LE Treatment |
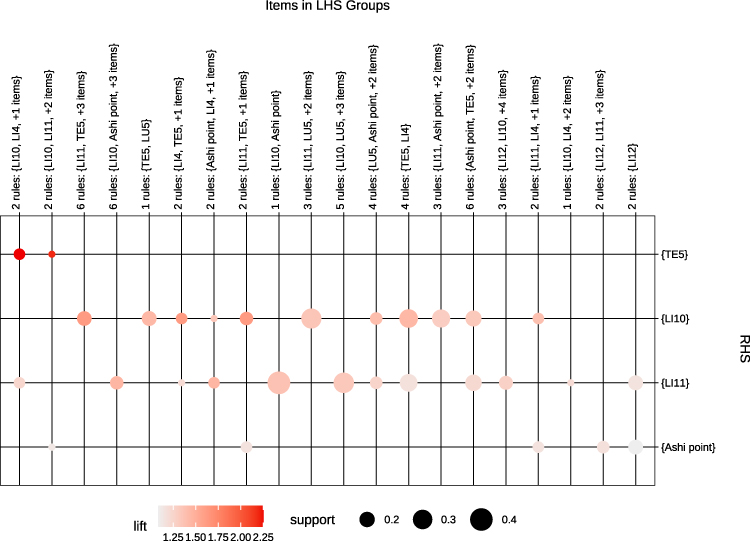 |
Figure 5 Grouping matrix of 59 association rules for acupuncture intervention. This color grid illustrates the relationship between groups of LHS and RHS within the association rules. Larger circles represent higher support and darker red circles indicate higher lift. “+n items”: n additional acupoints in LHS group; “n rules”: total rules between groups. |
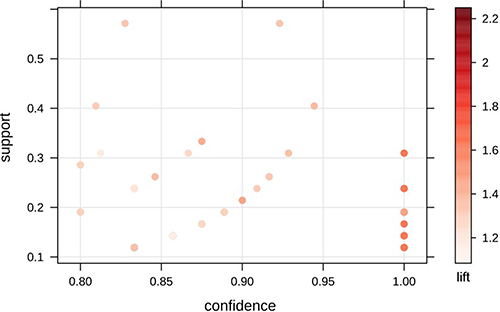 |
Figure 6 Scatter plot of 59 association rules for acupoint combinations. Each point represents an individual rule. The horizontal axis represents confidence, and the vertical axis represents support. Color intensity represents lift, with darker points indicating stronger associations between acupoints. |
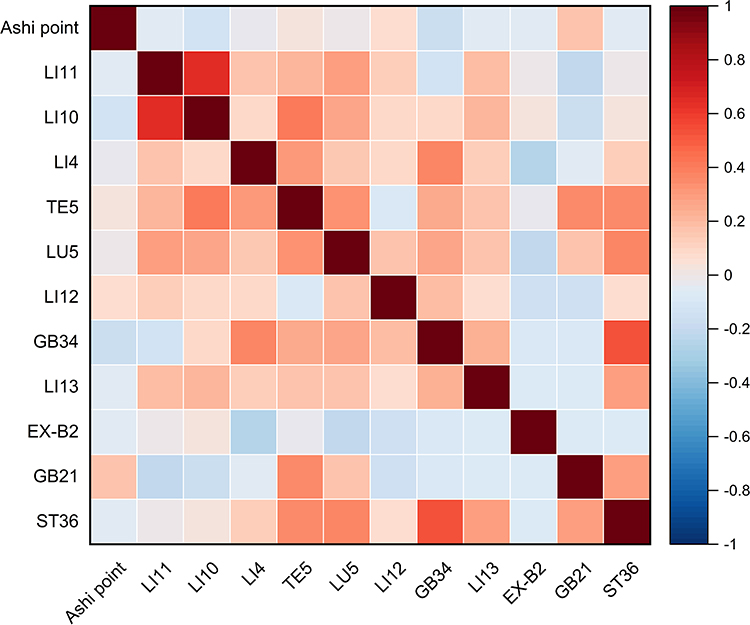 |
Figure 7 Correlation of the top 12 frequently used acupoints. The color scale indicates correlation coefficients from −1 (blue, negative) to +1 (red, positive), with white representing near-zero correlations. |
Network of Acupoints for LE
A complicated network was established using Cytoscape to derive 40 acupoints (nodes) and 456 edges, which were classified by degree scores: the darker the color and the higher the frequency, as shown in Figure 8A. The average degree of the network was 11.4, suggesting that each acupoint can coexist with 11.4 other acupoints on average. A total of seven acupoints had degrees of 20 or above and Ashi point was the most frequently used among these acupoints. The average path length of network was 1.68. When degree ≥10, the top 5 core acupoints were Ashi point, LI4, LI11, LI10 and TE5, as shown in Figure 8B. Notably, these acupoints were consistent with the results of association rule analysis.
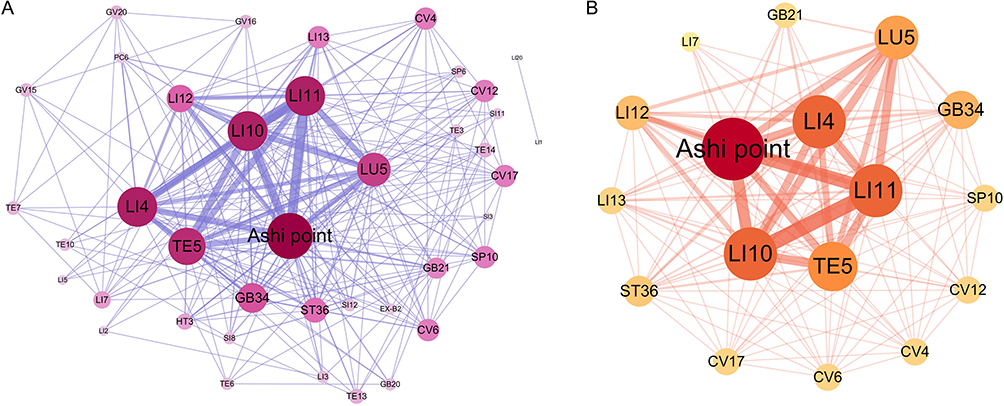 |
Figure 8 (A) Acupoints association network of acupuncture; (B) Core acupoints network of acupuncture. Nodes represent individual acupoints; larger node size and darker color indicate higher frequency of use. Edges represent co-occurrence relationships between acupoints; thicker edges indicate higher degree of co-occurrence. |
Hierarchical Cluster Analysis of Acupoints for LE
A hierarchical cluster analysis was performed on the acupoint prescriptions using OriginPro2024. By hierarchical cluster analysis, the top 12 selected acupoints were categorized into four categories: Cluster 1 contained TE5, GB21, LU5, GB34, ST36, LI13 and LI4; Cluster 2 contained LI10, LI11 and LI12; Cluster 3 contained Ashi point; Cluster 4 contained EX-B2 (Figure 9).
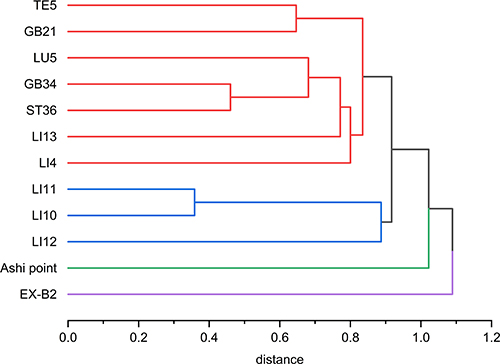 |
Figure 9 Cluster analysis of top 12 selected acupoints for LE. The distance metric used is Pearson correlation distance, defined as 1-r, where r is the Pearson correlation coefficient. |
Adverse Effects of Acupuncture for LE
Four publications mentioned adverse effects (AEs) of the trials and five types of AEs were mentioned in the intervention group (Table 10). The AEs that occurred in the intervention group were mainly from acupuncture, such as acupuncture pain or acupuncture numbness.
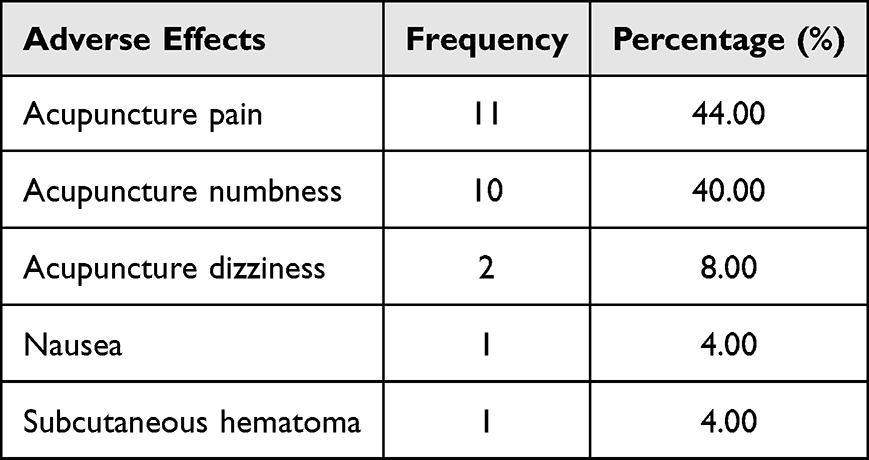 |
Table 10 Adverse Effects of Acupuncture for LE |
Discussion
Our study applied data mining techniques to perform a secondary analysis of literary studies to summarize the parameters related to acupuncture treatment for LE and to develop guidance for future clinical studies. Data mining, as an exploratory analytical method, systematically extracts hidden patterns, associations, and clusters from published data that may not be readily discernible through narrative synthesis.37 Unlike traditional review methods that depend on subjective summarization, data mining techniques employ computational algorithms to objectively quantify frequencies, identify statistical associations, and uncover hierarchical structures within the extracted data.38 This methodological approach facilitates the conversion of diverse and heterogeneous literature into structured, evidence-based references for clinical practice. Specifically, we combined 42 clinical studies of acupuncture intervention for LE and obtained needling parameters (needle type, retention time, treatment frequency and total treatment duration) and acupoint parameters (acupoints frequency, meridians, specific acupoints and acupoints on different body parts). Furthermore, association rules, complex network and hierarchical cluster were evaluated. These results have positive implications for clinical practice, providing acupuncturists with an evidence-based reference for optimizing prescription decisions for LE.
In clinical practice, although diverse types of needles may lead to different outcomes, it is challenging to establish standardized needle specifications owing to several factors, including inconsistent practice backgrounds of acupuncturists, physical condition of patients, needling tolerance and disease duration.39,40 Our study identified the three most commonly used needling types, 0.30mm × 40 mm, 0.35mm × 50 mm and 0.35mm × 40 mm, suggesting an overall trend in needling types for LE. Previous studies have found that needles with larger diameters may produce stronger effects, but the sensation was more painful and less acceptable.41,42 Therefore, the use of medium-sized needles is generally recommended. We found that the stimulation duration of acupuncture for LE ranged from 20 to 30 minutes, with 30 minutes being the most frequently applied, which was consistent with clinical practice.43 In addition, many studies have suggested that a 30-minute retention time was optimal for managing pain originating from bone and joint diseases.44–47 The results indicated that seven times per week was the most commonly used treatment frequency in previous studies. According to some studies, both excessively low and high acupuncture frequencies may fail to achieve the optimal therapeutic outcomes, potentially reducing treatment efficacy.48 However, high-quality evidence is still lacking to define the optimal acupuncture frequency specifically for LE. Furthermore, based on the available evidence, a total treatment duration of twenty days was identified as optimal for patient recovery. The application of appropriate acupuncture treatment is crucial for ensuring therapeutic efficacy. Although treatment duration is influenced by objective factors such as the disease course and treatment methodology, research specifically examining its correlation with treatment outcomes remains limited.49 Therefore, further studies are needed to establish quantitative standards for optimal treatment duration.
Among the articles included, acupoints used for LE were found to involve eleven conventional meridians, one extraordinary meridian and one nonconventional meridian, indicating that the condition is associated with multiple meridians. Acupoints on the Large Intestine Meridian of Hand Yangming accounted for the greatest number of points.50 Inner Canon of the Yellow Emperor, the foundational text of TCM, stated that “Yangming is abundant in qi and blood.” This suggested that the Yang-ming meridian can nourish the tendons and promote movement of the joints.51 Other frequently used meridians included the Triple-warmer Meridian of Hand Shaoyang, the Lung Meridian of Hand Taiyin and the Nonconventional meridian. The meridian analysis indicated that clinical acupuncture treatments for LE emphasized the selection of acupoints along the affected meridians. Most of the aforementioned meridians traverse the elbow region, which is consistent with the theory that “the channel can treat wherever it passes.”
The frequency analysis of acupoints identified Ashi point, LI11, LI10, LI4 and TE5 as those with a usage frequency greater than 15. The results indicated that Ashi point is the most central acupoint and could theoretically serve as a key point for treating LE, based on the theory of “taking the painful area as acupoint” from Inner Canon of the Yellow Emperor. Numerous clinical studies also have demonstrated the significant efficacy of this acupuncture theory in managing pain disorders.52–55 Researchers reported that stimulating Ashi point can produce local analgesia by downregulating inflammatory mediators at the pain site and centrally increase the pain threshold by inhibiting the expression of neurons in posterior horn of the spinal cord.29 LI11 is located on the Large Intestine Meridian of Hand Yangming and is categorized as one of the Five-Shu Points, with functions including clearing heat, dispersing wind, reducing swelling and relieving pain.56 LI11 lies in a region with a rich neurovascular supply, neighbored by the superficial branch of the radial nerve and the median nerve. Given this anatomical relationship, stimulation at this site is considered to modulate the function of these major nerves.57 LI4 is the Yuan-primary point of the Hand Yangming Meridian. The anatomical region of LI4 contains a high density of muscles, blood vessels, nerves and peripheral receptors.58–60 This anatomical foundation facilitates key physiological effects of acupuncture, such as improved local circulation, regulation of nerve function and an elevated pain threshold, which collectively contribute to analgesia.61,62 LI10 is the source point of the Large Intestine Meridian of Hand Yangming, which is an important point for treating pain. Previous studies have shown that acupuncture at LI10 has a significant analgesic effect and can increase the pain threshold.63,64 Its mechanism is mainly related to increase levels of serotonin or dopamine in the brain, thereby exerting analgesic effects.65,66 TE5 belongs to the Triple-warmer Meridian of Hand Shaoyang and is one of the Luo-connecting points and one of the Eight confluence points. It regulates Qi and blood to alleviate pain. Supporting this, a study provided scientific evidence by demonstrating that electroacupuncture stimulation at TE5 significantly reduced serum concentrations of TNF-α and IL-6, leading to pain reduction in a rat model.67 The analysis of acupoint selection strategies revealed a frequent combination of predominantly local points with distal points, particularly those farther from the elbow. This methodology originates from meridian theory, which proposes that stimulating distal points can remotely modulate Qi circulation.68,69 Empirical support for this principle is provided by modern neuroimaging, which has identified functional connections between distal body surfaces and the brain.70 Furthermore, evidence indicates that acupuncture signals from these distal regions ascend to superior brain centers such as the brainstem, hypothalamus and limbic system. The subsequent activation of the endogenous analgesic system engages a descending inhibitory pathway, culminating in the release of neurotransmitters including serotonin and norepinephrine. This subsequently attenuates pain signal transduction at the spinal level, thereby inducing systemic analgesia.71,72
This study utilized association rule mining to uncover core acupoint combinations for LE. A key finding was the strong association between the local points LI10 and LI11, recognized in traditional theory for their ability to tonify Qi, activate blood, unblock the meridians and alleviate pain. A study demonstrated that acupuncture was efficacious in improving the function of the arm associated with lateral elbow tendinosis.73 Subsequently, network diagrams derived from association rule mining identified core acupuncture points with the strongest associations, including Ashi point, LI4, LI11, LI10 and TE5. This reveals a potentially effective acupoint prescription for the treatment of LE. The identified acupoint combinations likely alleviate pain through distinct mechanisms. Local stimulation within the affected C5–C8 dermatomes may induce segmental analgesia through spinal gate control mechanisms.74 In contrast, distal points can activate extrasegmental descending pathways that involve the periaqueductal gray and rostral ventromedial medulla, resulting in the release of neurotransmitters such as serotonin, norepinephrine, and endogenous opioids.71,72 This supraspinal response elicits widespread analgesic effects beyond the stimulated region, thereby supporting the clinical application of distal points in LE treatment. Therefore, the observed integration of local and distal points may represent an optimized therapeutic strategy that engages both segmental and extrasegmental pain modulation.75
The selection and combination of acupoints based on pattern identification are essential for the efficacy of acupuncture treatment. Our hierarchical cluster analysis of acupoints for Le identified four distinct clusters, each exhibiting a unique therapeutic focus based on their co-occurrence patterns in clinical prescriptions. Cluster 1 comprised seven acupoints (TE5, GB21, LU5, GB34, ST36, LI13, LI4), which are distal points on the upper extremities and shoulders traditionally used to regulate Qi circulation and provide analgesic effects through extrasegmental pathways.76 These points are located in different spinal segments from the elbow, suggesting their therapeutic effects may be mediated through supraspinal mechanisms involving the descending pain modulatory system.77 Notably, Clusters 1 and 4 contained distal points located farther from the elbow, which were associated with pain attenuation around the elbow, with points in Cluster 1 being more prevalent. Cluster 2 comprised three acupoints (LI10, LI11, LI12), all local points from the Large Intestine Meridian of Hand Yangming near the elbow region, which may provide segmental analgesia through spinal inhibitory mechanisms.78 These points share similar spinal innervation with the elbow joint, thereby supporting their traditional use in treating disorders along the Meridian pathway. Cluster 3 consisted exclusively of the Ashi point, highlighting its unique role as a direct tender point targeting the pathological site. Ashi point stimulation has been demonstrated to induce local analgesia by downregulating inflammatory mediators and centrally elevating the pain threshold.79 Cluster 4 comprised EX-B2 exclusively, representing extra-meridian points employed as adjunctive therapy tailored to individual patient presentation.
Regarding safety, the intervention group experienced a wider range of adverse events, primarily minor acupuncture-related reactions including pain, numbness, dizziness, nausea and hematoma. All events were well-tolerated and resolved spontaneously with appropriate management or rest.
Several limitations of this study should be acknowledged when interpreting the findings. First, the quality and completeness of the included studies directly influence the reliability of our results; heterogeneity in study design, outcome measures, and acupuncture techniques across the 42 studies may have introduced bias and affected the generalizability of the findings. Second, as a data mining study, our analysis identifies patterns of acupoint selection but cannot establish causal relationships or directly infer clinical efficacy. Third, the lack of patient sub-classification based on traditional Chinese medicine pattern differentiation may have obscured condition-specific acupoint preferences. Fourth, the relatively small number of included studies may constrain the stability and generalizability of the identified acupoint patterns. A greater number of studies would provide stronger evidence for association rules and cluster analyses. Future updates of this study, incorporating a broader range of research, are necessary to validate and refine the findings. Finally, the cluster analysis was limited to acupoint frequencies derived from published literature and did not incorporate clinical variables such as disease severity, duration, or individual patient characteristics. Additionally, study setting information (eg., geographic location, clinical environment) was not extracted, which may affect the generalizability of our findings. Future research could explore variations in acupuncture practices across different settings or regions. Therefore, the acupoint prescriptions identified in this study require further validation through well-designed clinical trials, animal experiments, and investigations incorporating objective biomarkers to confirm their therapeutic efficacy and strengthen the evidence base.
Conclusion
Through data mining of 42 studies, we identified the predominant acupuncture parameters for lateral epicondylitis: 0.30 mm × 40 mm needles, 30-minute retention, seven sessions weekly, and 20 days total duration. The most frequently used acupoints were Ashi point, LI11, LI10, LI4, and TE5. The Large Intestine Meridian and five-shu points were most commonly employed, with LI11-LI10 as the strongest acupoint pair. Core acupoints comprised Ashi point, LI4, LI11, LI10, and TE5. Hierarchical cluster analysis revealed four distinct acupoint clusters, each with a specific therapeutic focus. These findings provide a foundational reference for acupuncture treatment. Future research should include well-designed randomized controlled trials to confirm the clinical efficacy of the core acupoint combination (Ashi point, LI4, LI11, LI10, and TE5) and to determine the optimal treatment parameters for lateral epicondylitis.
Patient and Public Involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Acknowledgments
We thank Mingjie Chen (Shanghai NewCore Biotechnology Co., Ltd.) for providing data analysis and visualization support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This article was financially supported by The Construction Fund of Key Medical Disciplines of Hangzhou (No.2025HZPY02) and The Zhejiang Provincial TCM Administration Science and Technology Program-Youth Talent Project (No.2025ZR058).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kholinne E, Singjie LC, Anastasia M, et al. Comparison of clinical outcomes after different surgical approaches for lateral epicondylitis: a systematic review and meta-analysis. Orthop J Sports Med. 2024;12(5):23259671241230291. doi:10.1177/23259671241230291
2. Blonna D, Hoxha N, Greco V, et al. When lateral epicondylitis is not lateral epicondylitis: analysis of the risk factors for the misdiagnosis of lateral elbow pain. Am J Sports Med. 2025;53(5):1195–20. doi:10.1177/03635465251319545
3. Hung CC, Chen HS, Chang CH, et al. Evaluation and surveillance of lateral elbow tendinopathy in manual workers: identifying elbows at risk. J Med Ultrasound. 2024;33(1):47–53. doi:10.4103/jmu.jmu_22_24
4. Simental-Mendía M, Vilchez-Cavazos F, Álvarez-Villalobos N, et al. Clinical efficacy of platelet-rich plasma in the treatment of lateral epicondylitis: a systematic review and meta-analysis of randomized placebo-controlled clinical trials. Clin Rheumatol. 2020;39(8):2255–2265. doi:10.1007/s10067-020-05000-y
5. Kizilkurt T, Aydin AS, Yagci TF, et al. Platelet-rich plasma provides superior clinical outcomes without radiologic differences in lateral epicondylitis: randomized controlled trial. Medicina. 2025;61(5):894. doi:10.3390/medicina61050894
6. Thanasas C, Papadimitriou G, Charalambidis C, et al. Platelet-rich plasma versus autologous whole blood for the treatment of chronic lateral elbow epicondylitis: a randomized controlled clinical trial. Am J Sports Med. 2011;39(10):2130–2134. doi:10.1177/0363546511417113
7. Alizadehkhaiyat O, Fisher AC, Kemp GJ, et al. Pain, functional disability, and psychologic status in tennis elbow. Clin J Pain. 2007;23(6):482–489. doi:10.1097/AJP.0b013e31805f70fa
8. Lowdon H, Chong HH, Dhingra M, et al. Comparison of interventions for lateral elbow tendinopathy: a systematic review and network meta-analysis for patient-rated tennis elbow evaluation pain outcome. J Hand Surg Am. 2024;49(7):639–648. doi:10.1016/j.jhsa.2024.03.007
9. Nambi G, Alghadier M, Verma A, et al. Clinical and radiological effects of Corticosteroid injection combined with deep transverse friction massage and Mill’s manipulation in lateral epicondylalgia-A prospective, randomized, single-blinded, sham controlled trial. PLoS One. 2023;18(2):e0281206. doi:10.1371/journal.pone.0281206
10. Hohmann E, Tetsworth K, Glatt V. Corticosteroid injections for the treatment of lateral epicondylitis are superior to platelet-rich plasma at 1 month but platelet-rich plasma is more effective at 6 months: an updated systematic review and meta-analysis of level 1 and 2 studies. J Shoulder Elbow Surg. 2023;32(9):1770–1783. doi:10.1016/j.jse.2023.04.018
11. Parrey JA, Bari MA, Khan AQ, Ajhar A, Singh S. Evaluating the impact of NSAIDs and exercise therapy versus sole exercise therapy on joint mobility, pain levels, grip strength, and muscle activity in lateral epicondylitis patients. Retos. 2025. 69: 512–526.
12. Özmen T, Koparal SS, Karataş Ö, et al. Comparison of the clinical and sonographic effects of ultrasound therapy, extracorporeal shock wave therapy, and Kinesio taping in lateral epicondylitis. Turk. J Med Sci. 2021;51(1):76–83.
13. Syed AU, Darain H, Rana M. The effects of the addition of Mulligan mobilization with movement to exercise on elbow pain and function associated with lateral elbow tendinopathy. J Bodyw Mov Ther. 2024;40:872–879. doi:10.1016/j.jbmt.2024.06.007
14. Muir D, Blakeway H, Morris R, et al. Surgical management of lateral epicondylitis: a scoping review of published literature. JSES Rev Rep Tech. 2024;5(1):79–85. doi:10.1016/j.xrrt.2024.08.008
15. Mazzocca AD, McCarthy MB, Intravia J, et al. An in vitro evaluation of the anti-inflammatory effects of platelet-rich plasma, ketorolac, and methylprednisolone. Arthroscopy. 2013;29(4):675–683. doi:10.1016/j.arthro.2012.12.005
16. Ang L, Song E, Choi TY, et al. Effects of acupuncture on musculoskeletal pain: an evidence map. Front Med. 2025;12:1575226. doi:10.3389/fmed.2025.1575226
17. Navarro-Santana MJ, Sanchez-Infante J, Gómez-Chiguano GF, et al. Effects of manual acupuncture and electroacupuncture for lateral epicondylalgia of musculoskeletal origin: a systematic review and meta-analysis. Acupunct Med. 2021;39(5):405–422. doi:10.1177/0964528420967364
18. Chang WD, Lai PT, Tsou YA. Analgesic effect of manual acupuncture and laser acupuncture for lateral epicondylalgia: a systematic review and meta-analysis. Am J Chin. 2014;42(6):1301–1314. doi:10.1142/S0192415X14500815
19. Wang Z, Qin P, Chen Y, et al. Exploring the spatial effects of acupuncture analgesia. Neuroscience. 2025;573:300–314. doi:10.1016/j.neuroscience.2025.03.053
20. Li Y. Cao Q. application of acupuncture in cervical spondylotic radiculopathy: an in-depth analysis and outlook on pathophysiological basis and therapeutic mechanisms. Int J Gen Med. 2025;18:5717–5730.
21. Huang CC, Kotha P, Tu C-H, et al. Acupuncture: a review of the safety and adverse events and the strategy of potential risk prevention. Am J Chin Med. 2024;52(6):1555–1587. doi:10.1142/S0192415X24500617
22. Picelli A, Di Censo R, Zuccher P, et al. Therapeutic ultrasound versus acupuncture for lateral epicondylitis: a pilot case-control observational study. Minerva Orthopedics. 2025;76(4):275–281. doi:10.1146/annurev-psych-021524-110810
23. Zhou Y, Guo Y, Zhou R, et al. Effectiveness of Acupuncture for lateral epicondylitis: a systematic review and meta-analysis of randomized controlled trials. Pain Res Manag. 2020;2020:8506591. doi:10.1155/2020/8506591
24. Zhu F, Chen Y, Zhu Y, et al. Acupuncture therapy for extremity musculoskeletal pain: a clinically focused evidence synthesis with therapeutic implications. J Pain Res. 2025;18:5541–5554. doi:10.2147/JPR.S551446
25. Bonczar M, Ostrowski P, Plutecki D, et al. Treatment options for tennis elbow - an umbrella review. Folia Med Cracov. 2023;63(3):31–58.
26. Tang H, Fan H, Chen J, et al. Acupuncture for Lateral Epicondylitis: a Systematic Review. Evid Based Complement Alternat Med. 2015;2015:861849. doi:10.1155/2015/861849
27. Wu WT, Li YJ, Feng AZ, et al. Data mining in clinical big data: the frequently used databases, steps, and methodological models. Mil Med Res. 2021;8(1):44. doi:10.1186/s40779-021-00338-z
28. Xu H, Miao FR, He YJ, et al. Data mining-based analysis to explore the application of an animal model of diabetic gastroparesis. Front Endocrinol. 2025;16:1612473. doi:10.3389/fendo.2025.1612473
29. Li QY, Yang WX, Liu H, et al. Research on electroacupuncture parameters for cancer pain based on data mining. Integr Cancer Ther. 2023;22:15347354231192017. doi:10.1177/15347354231192017
30. Yu F, Li S, Li Z, et al. Usage, anti-inflammatory effect and safety of adjunctive acupuncture for cerebral infarction: an Apriori algorithm-based data mining and meta-analysis. Front Neurol. 2025;16:1546194. doi:10.3389/fneur.2025.1546194
31. Wang J, Yang F, Wang X, et al. Acupoint selection in postoperative ophthalmic pain management: a data mining protocol. J Pain Res. 2024;17:903–909. doi:10.2147/JPR.S449175
32. He Y, Li L, Zhou M, et al. Analysis of acupoint selection and combinations in acupuncture treatment of trigeminal neuralgia: a protocol for data mining. J Pain Res. 2025;18:3373–3381. doi:10.2147/JPR.S533617
33. He Y, Miao F, He C, et al. A data mining study for analysis of acupoint selection and combinations in acupuncture treatment of carpal tunnel syndrome. J Pain Res. 2024;17:1153–1170. doi:10.2147/JPR.S452618
34. Chinese Medical Association. Clinical Diagnosis and Treatment Guidelines: Orthopedics Volume. Beijing: The People’s Health Press Co. Ltd; 2009:65.
35. National Administration of Traditional Chinese Medicine. Standards for Diagnosis and Therapeutic Effect of Traditional Chinese Medicine Diseases and Syndromes. Beijing: China Medical Science and Technology Press; 2012:195.
36. Xu ST, Ge BF, Xu YK. Practical Orthopedics.
37. You TY, Zhang HY, Ma T-M. Ma TM. Current status, challenges and countermeasures of acupuncture data mining literature researches. Zhen Ci Yan Jiu. 2022;47(11):1036–1040. doi:10.13702/j.1000-0607.20220570
38. Wang Z, Chen QX, Dong ZH, et al. Construction and application of acupuncture data mining algorithms within an evidence-based framework. Chin J Evid Based Med. 2024;24(9):1070–1078.
39. Wang JL, Li YM, Ren L, et al. Standardization of acupuncture needles and safe insertion depth: towards enhanced clinical safety and global consensus. Chin Archiv Tradit Chin Med. 2025;43(10):202–207.
40. Wu JL, Yu ZS, Wei QS, et al. Influence of ‘combining medicine and engi‑neering’ on reform of acupuncture and moxibustion’s needles. China J Tradit Chin Med Pharm. 2018;33(12):5409–5411.
41. Gan Y, Xiong YY. A comparative study of thick and thin filiform needles for acupuncture treatment of acute frozen shoulder. J Extern Ther TCM. 2017;26(05):38–39.
42. Wang YN, Qiu LL, Liu XQ. Influence of thick‑thin filiform on pain threshold of patients with sciatica. West J Tradit Chin Med. 2012;25(01):79–80.
43. Zhang YH, Wang B, Yang JH. Research progress and thoughts on the relationship between needle retention time and curative effect of acupuncture. China J Tradit Chin Med Pharm. 2024;39(08):4229–4234.
44. Dai YX, Wang K, Wang JW, et al. A comparative study of different needle retention times in warm needling therapy for knee osteoarthritis. J Pract Tradit Chin Med. 2023;39(06):1201–1203.
45. Lin YZ, Wu Y, Li L, et al. Influence of different needle retention time on the efficacy of warm needling moxibustion for knee osteoarthritis. Shanghai J Acu-Mox. 2022;41(02):149–153.
46. Peng KS, Guo XQ, Huang ZJ, et al. Observations on the analgesic effect of electroacupuncture of different duration on knee osteoarthritis. Shanghai J Acu-Mox. 2022;41(10):1011–1015.
47. Xue XJ, Liu ZB, Wang YY, et al. Correlations of curative effect with time interval of acupuncture and moxibustion. J Clin Acupunct Moxibust. 2018;34(01):1–4.
48. Luo Q, Sun MS, Tian H, et al. Research status and dose-effect relationship of acupuncture frequency and treatment course in past decade. World Chin Med. 2025;20(02):266–274.
49. Zhang LJ, Wang YJ, Song K. The impact of course on the therapeutic effect of acupuncture and moxibustion. Clin J Tradit Chin Med. 2018;30(04):754–757.
50. Li S, Li JS, Yan W. Analysis of clinical acupoint selection rules in acupuncture treatment of knee osteoarthritis based on data mining technology. Chin Imaging J Integr Tradit West Med. 2021;19(03):210–216.
51. Geng QD, Jiang YD, Gao SH, et al. Study on the correlation between pain of supraspinatus tendon injury and its influencing factors and meridian circulation of shoulder. J Liaon Univer TraditChin Med. 2025;27(02):166–175.
52. Li X, Zhang Y, Gao T, et al. Effect of oblique insertion at Ashi point with long needle on joint function in female patients with knee osteoarthritis of early and middle stages. Chin Acupunct Moxibust. 2024;44(9):1017–1022. Chinese.
53. Zhao L, Cheng K, Wang L, et al. Effectiveness of moxibustion treatment as adjunctive therapy in osteoarthritis of the knee: a randomized, double-blinded, placebo-controlled clinical trial. Arthritis Res Ther. 2014;16(3):R133. doi:10.1186/ar4590
54. Mitidieri AMS, Baltazar MCDV, da Silva APM, et al. Ashi acupuncture versus local anesthetic trigger point injections in the treatment of abdominal myofascial pain syndrome: a randomized clinical trial. Pain Physician. 2020;23(5):507–518.
55. Li X, Zhang YW, Gao TC, et al. Effect of oblique insertion at Ashi point with long needle on joint function in female patients with knee osteoarthritis of early and middle stages. Chin Acupunct Moxibust. 2024;44(09):1017–1022.
56. Sheng RR, Zhang W. A review of clinical applications and experimental studies of the quchi acupuncture point. Guide Chin Med. 2013;11(20):81–82.
57. Li L, Huang Y, An C, et al. Acupuncture in the treatment of chemotherapy-induced peripheral neuropathy: a meta-analysis and data mining. Front Neurol. 2024;15:1442841. doi:10.3389/fneur.2024.1442841
58. Dong QS, Zhang RT, Dong XM, et al. Exploring the material basis of acupoints in electroacupuncture analgesia by examining the relationship among analgesic effect, needle sensation, and sensory function. J Sichuan TCM. 2008;(11):117–121.
59. Li MZ, Qi HT, Qi YD, et al. Anatomical structure of Hegu acupoint. Shandong Medical Journal. 2023;63(09):3–7.
60. Sun W, Liu Y. Anatomic found of hegu acupuncture. Heilongjiang Med J. 2011;35(08):570–572.
61. Dong QS, Wang XQ, Zhang RT, et al. Investigating the material basis of acupoints in manual acupuncture needle sensation: insights from the interaction with sensory function. J Sichuan TCM. 2007;(01):92–97.
62. Huang SZ, Wu TA, Deng N, et al. Research progress on the clinical application and mechanism of action of the siguan acupuncture points. Hunan J TCM. 2025;41(05):161–165.
63. Zhang YX, Feng X, Wei W, et al. Observation of pain-temperature evoked potential produced by pressing method on shousanli (LI10) of normal people and analysis of nerve conduction effect of meridian theory. J Liaoning Univer Tradit Chin Med. 2020;47(09):150–152.
64. Zhang YX, Feng X, Wei W, et al. Discussion on patterns of small fiber neurosensory transmission along meridians based on pain-temperature evoked potentials of finger-pressing and acupuncture on shousanli. Chin J Informat TCM. 2020;27(04):23–27.
65. Jiang YY, Chen YF. Analysis on the clinical application of shousanli (LI10) in Zhenjiu Dacheng. GuangMing J Chin Med. 2023;38(02):232–234.
66. Xiao J, Tang ZY, Qin Y, et al. A clinical exploration of the shousanli point (LI10) in treating postoperative pain and dysfunction. J Emerg TCM. 2024;33(02):336–339.
67. Zhang H, He SD, Pan XY, et al. Effect of electroacupuncture on the expression of serum inflammatory factors in rats with migraine. Hunan J TCM. 2018;34(07):170–171.
68. Gao YJ, Qiao HF, Wang Q, et al. Discussion on the clinical significance of distant acupoints on Meridian-tendon disease based on the correlation between body surface-body surface. China J Tradit Chin Med Pharm. 2022;37(10):5730–5734.
69. Li QP, Zhang XW. Treatment of lateral epicondylitis by remote needling based on the theory of “Tongqi Xiangqiu”. J Shanxi Univer Chin Med. 2024;25(10):1135–1139.
70. Padberg J, Franca JG, Cooke DF, et al. Parallel evolution of cortical areas involved in skilled hand use. J Neurosci. 2007;27(38):10106–10115. doi:10.1523/JNEUROSCI.2632-07.2007
71. Xia YF, Wang YY, Li RR, et al. Research progress on the central mechanisms underlying the cumulative effect of acupuncture analgesia. Zhejiang J Integrat Tradit Chin West Med. 2022;32(06):585–588.
72. Lv GW. Basic and clinical studies of acupoint afferentation and acupuncture analgesia. Chin J Neuroanatomy. 2016;32(01):119–123.
73. Gadau M, Zhang SP, Wang FC, et al. A multi-center international study of acupuncture for lateral elbow pain - results of a randomized controlled trial. Eur J Pain. 2020;24(8):1458–1470. doi:10.1002/ejp.1574
74. Bingel U, Tracey I. Imaging CNS modulation of pain in humans. Physiology. 2008;23:371–380. doi:10.1152/physiol.00024.2008
75. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
76. Zhang R, Lao L, Ren K, et al. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
77. Xu WD, Zhu B, Rong PJ, et al. The pain-relieving effects induced by electroacupuncture with different intensities at homotopic and heterotopic acupoints in humans. Am J Chin Med. 2003;31(5):791–802. doi:10.1142/S0192415X03001478
78. Mao WC, Liu BY, He LY, et al. Discussion on existing problems of placebo acupuncture design based on acupuncture analgesia. Zhen Ci Yan Jiu. 2013;38(2):163–167.
79. Li T, Xie YQ, Li SC, et al. Effect of bloodletting at Ashi point on peripheral pain mediators in a rat model of acute gouty arthritis. Zhongguo Zhen Jiu. 2006;26(3):215–217.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of Acupoint Selection and Combinations in Acupuncture Treatment of Carpal Tunnel Syndrome: A Protocol for Data Mining
He Y, Miao F, Fan Y, Zhang F, Yang P, Zhao X, Wang M, He C, He J
Journal of Pain Research 2023, 16:1941-1948
Published Date: 7 June 2023
Analysis of Acupoint Selection and Combinations in Acupuncture Treatment of Piriformis Syndrome: A Protocol for Data Mining
He Y, Miao F, Fan Y, He J, Zhang F, Wang Z, Wu Y, Zhao Y, Yang P
Journal of Pain Research 2023, 16:3265-3272
Published Date: 28 September 2023
Analysis of Traditional Chinese Medicine Symptoms in Children with Spastic Cerebral Palsy, a Protocol for Data Mining
Wang X, Pang F, Du XG
Journal of Multidisciplinary Healthcare 2023, 16:3143-3149
Published Date: 25 October 2023
A Data Mining Study for Analysis of Acupoint Selection and Combinations in Acupuncture Treatment of Carpal Tunnel Syndrome
He Y, Miao F, He C, Fan Y, Zhang F, Yang P, Wang M, He J
Journal of Pain Research 2024, 17:1153-1170
Published Date: 18 March 2024
Exploration of the Application Rules and Clinical Significance of Acupoints in Acupuncture Treatment of Migraine Based on Data Mining
He Y, Wang X, Liu M, Li L, Han T, Wu Y, Li X
Journal of Pain Research 2025, 18:3049-3067
Published Date: 18 June 2025