Back to Journals » Clinical Epidemiology » Volume 8
Danish Palliative Care Database
Authors Groenvold M, Adsersen M, Hansen MB
Received 11 November 2015
Accepted for publication 18 February 2016
Published 25 October 2016 Volume 2016:8 Pages 637—643
DOI https://doi.org/10.2147/CLEP.S99468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Mogens Groenvold,1,2 Mathilde Adsersen,1 Maiken Bang Hansen1
1The Danish Palliative Care Database (DPD) Secretariat, Research Unit, Department of Palliative Medicine, Bispebjerg Hospital, 2Department of Public Health, University of Copenhagen, Copenhagen, Denmark
Aims: The aim of the Danish Palliative Care Database (DPD) is to monitor, evaluate, and improve the clinical quality of specialized palliative care (SPC) (ie, the activity of hospital-based palliative care teams/departments and hospices) in Denmark.
Study population: The study population is all patients in Denmark referred to and/or in contact with SPC after January 1, 2010.
Main variables: The main variables in DPD are data about referral for patients admitted and not admitted to SPC, type of the first SPC contact, clinical and sociodemographic factors, multidisciplinary conference, and the patient-reported European Organisation for Research and Treatment of Cancer Quality of Life Questionaire-Core-15-Palliative Care questionnaire, assessing health-related quality of life. The data support the estimation of currently five quality of care indicators, ie, the proportions of 1) referred and eligible patients who were actually admitted to SPC, 2) patients who waited <10 days before admission to SPC, 3) patients who died from cancer and who obtained contact with SPC, 4) patients who were screened with European Organisation for Research and Treatment of Cancer Quality of Life Questionaire-Core-15-Palliative Care at admission to SPC, and 5) patients who were discussed at a multidisciplinary conference.
Descriptive data: In 2014, all 43 SPC units in Denmark reported their data to DPD, and all 9,434 cancer patients (100%) referred to SPC were registered in DPD. In total, 41,104 unique cancer patients were registered in DPD during the 5 years 2010–2014. Of those registered, 96% had cancer.
Conclusion: DPD is a national clinical quality database for SPC having clinically relevant variables and high data and patient completeness.
Keywords: specialized palliative care, cancer, quality indicator, patient-reported outcomes, multidisciplinary conference, EORTC QLQ-C15-PAL
Aim for database
The Danish Board of Health has defined a clinical quality database as:
[…] a register containing quantitative indicators, which are based on the individual patient trajectory and can elucidate the overall quality or parts of the overall quality of the health care system’s activity and results for a defined group of patients.1
The aim of the Danish Palliative Care Database (DPD) is to monitor, evaluate, and improve the clinical quality of specialized palliative care (SPC) (ie, the activity of hospital-based palliative care teams/departments and hospices) in Denmark.2
Study population
The study population for DPD is all patients in Denmark who
- have been referred to SPC and/or
- have been admitted to SPC.
Patients who have been referred to or have been admitted to SPC prior to the opening of DPD (January 1, 2010) are not part of the study population and are not included in the database.
The reason for including referred patients who have not been admitted to SPC is that access to SPC was judged to be an important aspect of quality: at the time when the DPD was designed, it was often reported in media that particularly the hospices had to decline access due to insufficient capacity.
“Being admitted to SPC” requires the initiation of palliative care, ie, at least one consultation between the patient and the SPC unit in any location (the patient’s home, the SPC unit, a non-SPC hospital department, etc). A patient who has only had contact with the SPC unit via telephone or who has only been evaluated with regard to eligibility is not regarded as having been admitted to SPC.
Each patient is registered once in DPD by each SPC unit receiving a referral of or admitting the patient. Thus, a patient having had contact with more than one SPC unit will appear with one registration for each of these SPC units. The same is the case for a patient who has been referred to more than one SPC unit but was not admitted to any of these units.
Between 2010 and 2014, 41,104 cancer patients were registered in DPD (2010: 6,041; 2011: 7,904; 2012: 8,743; 2013: 8,982; and 2014: 9,434). In addition, patients with other diagnoses such as respiratory, cardiovascular, and neurological diseases (in 2014: 4% of all patients) are registered.
According to the rules for clinical quality databases approved by the Danish Board of Health, registration of patients in DPD is mandatory for the SPC units.
Main variables
Table 1 lists all variables and their categories and indicates the variables that are used to estimate the following five quality indicators:
- Proportion of referred, relevant patients who were actually received in SPC.
- Proportion of patients who waited <10 days before admission to SPC.
- Proportion of patients who died from cancer and who obtained contact with a SPC.
- Proportion of patients screened with European Organisation for Research and Treatment of Cancer Quality of Life Questionaire-Core-15-Palliative Care (EORTC QLQ-C15-PAL)3 questionnaire at admission to SPC.
- Proportion of patients discussed at a multidisciplinary conference.
 | Table 1 Variables in the Danish Palliative Care Database (DPD): variable name, categories, purpose, data completeness, and data quality |
In addition to the variables needed for the quality indicators, the DPD includes clinical and sociodemographic variables and patient-reported outcomes at baseline (EORTC QLQ-C15-PAL scores). The first two quality indicators focus on access and waiting time. Problems related to these issues were often publicly debated before the creation of the DPD, and there was no national data available. The third indicator is a bit untypical by being a measure of access at the regional level. When developing the DPD, there was no knowledge as to whether the proportion of cancer patients who were admitted to SPC was similar in different parts of the country or whether this proportion corresponded to figures in other countries. This indicator will be subdivided into different types of contact (in-patient, out-patient, home visit, and consultation at non-SPC hospital department) when linking with the Danish National Patient Register has been established (work in progress).
There is evidence that not all the patients’ symptoms and problems are detected if a systematic assessment is not conducted.4–6 This motivates the fourth quality indicator, which requests that the patient has completed the EORTC QLQ-C15-PAL questionnaire at the day of first contact with SPC or up to 3 days before. The EORTC QLQ-C15-PAL3 is an abbreviated version of the internationally most widely used instrument assessing health-related quality of life in cancer patients, the EORTC QLQ-C30, which was developed by the European Organization for Research and Treatment of Cancer.7,8 To develop an instrument with minimal patient burden while preserving the advantages of (and comparability with) a well-validated instrument used in thousands of studies, the QLQ-C15-PAL was established by reducing the QLQ-C30 from 30 to 15 items by shortening scales and by deleting the items that were not important for patients in palliative care.3 The content of the ten scales is shown in Table 1.
Patient-reported outcomes may be very important variables in clinical databases, and data from the EORTC QLQ-C15-PAL can be used to describe the baseline levels of symptoms and problems in the patients admitted to SPC and for other purposes.
SPC is defined as a multiprofessional and interdisciplinary approach.9 Therefore, the fifth quality indicators measures whether it is documented in the medical record that the patient has been discussed at a multidisciplinary conference with representation from at least four disciplines (medical secretaries not included) present.
Most of the variables in DPD are entered by the SPC units in a web-based data entry system called Clinical Measurement System (in Danish: Klinisk Målesystem [KMS]). The following two paper-based forms are used for this: a data form consisting of 18 items and the patient-completed questionnaire EORTC QLQ-C15-PAL.3 The information for completion of the data form is extracted from the medical record, including documents relating to referral. This typically takes place after the patient’s death or after contact has been stopped. The variables in DPD have a high level of data completeness, with completeness ~100% for several variables, reflecting that these fields are mandatory in the reporting (Table 1).
Follow-up
As all data for each patient are entered at a single point of time, there is no subsequent follow-up.
The DPD Board is planning two expansions of the DPD related to follow-up. First, detailed data about all SPC activity subsequent to the first contact will be added to the DPD via linking with the Danish National Patient Register (using the unique personal registration number), which contains all hospital and hospice contacts.
Second, it is planned to add a second assessment with the EORTC QLQ-C15-PAL questionnaire,3 in addition to the first, which is completed by the patient at the first contact. The second assessment will take place ~1–4 weeks later and will allow evaluation of change in each of the scores after initiation of SPC, ie, “response to treatment.”
Examples of research
Two ongoing PhD projects are based on DPD data and take place in the DPD Secretariat at Bispebjerg Hospital (Table 2). In the first, data from DPD are linked with other national registers in Denmark, the Danish Register of Causes of Death,10 the Danish Civil Registration System,11 the Danish Cancer Registry,12 and Statistics Denmark to investigate social inequality in admittance to SPC. In the second project, the data from the EORTC QLQ-C15-PAL are analyzed in order to better understand the epidemiology of symptoms and problems in the patients admitted to SPC.
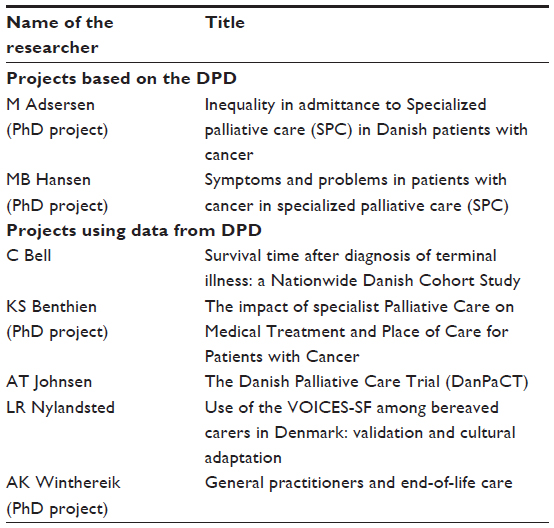 | Table 2 Examples of research with data from the Danish Palliative Care Database (DPD) |
Data from the DPD play an important role in several other projects (Table 2).
Administrative issues and funding
The DPD Secretariat supports the 43 SPC institutions, which report data to DPD, at a daily basis concerning questions and problems in relation to the mandatory entering of data in DPD, and carries out analyses of and validation of data. Data from DPD are continuously validated against the Danish National Patient Register to ensure that all patients are entered in DPD: it is checked whether all patients registered in the Danish National Patient Register as having a contact with an SPC unit are registered in DPD, and whether there is agreement about the date of admission. To clarify any discrepancies, the DPD Secretariat contacts the SPC units if there is disagreement between the two data sources. Any errors detected are corrected. This ensures a high completeness of patients in the database: in 2014, the patient completeness was 100%, ie, all patients registered with an SPC contact in the Danish National Patient Register were also registered in the DPD. The DPD Secretariat, in collaboration with the DPD Board, produces an Annual Report in Danish showing the results of the indicators overall and at the SPC unit level and at the regional level.2
The SPC institutions have access to their own data, and the DPD Secretariat offers courses in handling and analyzing their own data.
DPD is funded by the Danish Regions (who are the owners and administrators of the public hospitals) via The Danish Clinical Registries (RKKP).
Conclusion
Prior to the establishment of DPD, there was no knowledge about the quantity or quality of SPC at the national level. The past years of work with the DPD have shown that it is possible to establish a national clinical quality database with a high level of completeness even in a newly established, very busy, and very heterogeneous part of the health care system. This positive development probably reflects the perceived importance of the data produced by the DPD (both about quantity and quality), the high level of professional motivation in the SPC units and the DPD Board, the relatively modest registration burden, the availability of support from a dedicated Secretariat, and the fact that registration in the clinical databases, which are officially approved by the Danish Board of Health, is mandatory.
Acknowledgments
This paper was funded by the Program for Clinical Research Infrastructure (PROCRIN) established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions. We thank all SPC institutions in Denmark for their contribution and collaboration. Further, we thank the DPD Board, representing the five regions in Denmark, for their work in the development of DPD and the continuing work to improve the database with clinically relevant data. The current members of the DPD Board are Lise Pedersen, Thomas Feveile, Helle Tingrupp, Per Sjøgren, Thor Schmidt, Mogens Grønvold, Bettina Kotasek, Lars Michael Clausen, Anne Marie Olsen, Mette Asbjørn Neergaard, Dorit Simonsen, Helle Bjørn Larsen, and Anette Agerbæk.
Disclosure
Mogens Groenvold is chairman of the DPD Board and Mathilde Adsersen and Maiken Bang Hansen, PhD students, work part time in the DPD Secretariat. The authors report no other conflicts of interest in this work.
References
National Board of Health (Sundhedsstyrelsen). [Clinical Quality Databases]. Copenhagen: National Board of Health (Sundhedsstyrelsen); 2001:1–40. [In Danish]. | |
Hansen MB, Adsersen M, Groenvold M. [Danish Palliative Care Database. Annual Report 2014]. Copenhagen: DMCG-PAL; 2015. [In Danish]. | |
Groenvold M, Petersen MA, Aaronson NK, et al. The development of the EORTC QLQ-C15-PAL: a shortened questionnaire for cancer patients in palliative care. Eur J Cancer. 2006;42:55–64. | |
Stromgren AS, Groenvold M, Pedersen L, Olsen AK, Spile M, Sjogren P. Does the medical record cover the symptoms experienced by cancer patients receiving palliative care? A comparison of the record and patient self-rating. J Pain Symptom Manage. 2001;21:189–196. | |
Stromgren AS, Groenvold M, Sorensen A, Andersen L. Symptom recognition in advanced cancer. A comparison of nursing records against patient self-rating. Acta Anaesthesiol Scand. 2001;54:1080–1085. | |
Homsi J, Walsh D, Rivera N, et al. Symptom evaluation in palliative medicine: patient report vs systematic assessment. Support Care Cancer. 2006;14:444–453. | |
Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85:365–376. | |
Fayers PM, Aaronson N, Bjordal K, et al. The EORTC QLQ-C30 Scoring Manual. 3rd ed. Brussels: European Organization for Research and Treatment of Cancer; 2001. | |
Radbruch L, Payne S. White paper on standards and norms for hospice and palliative care in Europe: part 1. Recommendations from the European Association for Palliative Care. Eur J Palliat Care. 2009;16:278–289. | |
Helweg-Larsen K. The Danish Register of Causes of Death. Scand J Public Health. 2011;39:26–29. | |
Pedersen CB. The Danish Civil Registration System. Scand J Public Health. 2011;39:22–25. | |
Gjerstorff ML. The Danish Cancer Registry. Scand J Public Health. 2011;39:42–45. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.